

Abstract
Background
In pancreaticoduodenectomy, the pancreas-visceral fat CT value ratio and serrated pancreatic contour on preoperative CT have been revealed as risk factors for postoperative pancreatic fistulas. We aimed to evaluate whether they could also serve as risk factors for postoperative pancreatic fistulas after distal pancreatectomy.
Methods
A total of 251 patients that underwent distal pancreatectomy at our department from 2006 to 2020 were enrolled for the study. We retrospectively analyzed risk factors for postoperative pancreatic fistulas after distal pancreatectomy using various pre and intraoperative factors, including preoperative CT findings, such as pancreas-visceral fat CT value ratio and serrated pancreatic contour.
Results
The study population included 147 male and 104 female participants (median age, 68 years; median body mass index, 21.4 kg/m2), including 64 patients with diabetes mellitus (25.5%). Preoperative CT evaluation showed a serrated pancreatic contour in 80 patients (31.9%), a pancreatic thickness of 9.3 mm (4.0–22.0 mm), pancreatic parenchymal CT value of 41.8 HU (4.3–22.0 HU), and pancreas-visceral fat CT value ratio of − 0.41 (− 4.88 to − 0.04). Postoperative pancreatic fistulas were developed in 34.2% of the patients. Univariate analysis of risk factors for postoperative pancreatic fistulas showed that younger age (P = 0.005), high body mass index (P = 0.001), absence of diabetes mellitus (P = 0.002), high preoperative C-reactive protein level (P = 0.024), pancreatic thickness (P < 0.001), and high pancreatic parenchymal CT value (P = 0.018) were significant risk factors; however, pancreas-visceral fat CT value ratio (P = 0.337) and a serrated pancreatic contour (P = 0.122) did not serve as risk factors. Multivariate analysis showed that high body mass index (P = 0.032), absence of diabetes mellitus (P = 0.001), and pancreatic thickness (P < 0.001) were independent risk factors.
Conclusion
The pancreas-visceral fat CT value ratio and serrated pancreatic contour evaluated using preoperative CT were not risk factors for postoperative pancreatic fistulas after distal pancreatectomy. High body mass index, absence of diabetes mellitus, and pancreatic thickness were independent risk factors, and a close-to-normal pancreas with minimal fat deposition or atrophy is thought to indicate a higher risk of postoperative pancreatic fistulas after distal pancreatectomy.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12893-022-01650-8.
Keywords: Distal pancreatectomy, Postoperative pancreatic fistula, CT value, Serrated pancreas, Visceral fat, Diabetes mellitus
Background
The postoperative pancreatic fistula (POPF) is the most clinically problematic complication of pancreatectomy. The incidence of POPF depends on the type of pancreatectomy. Distal pancreatectomy (DP), pancreatoduodenectomy (PD) with pancreaticojejunal anastomosis, and PD with pancreatic duct occlusion have reported POFP incidences of 16.0–28.2% [1–5], 10.3–18.5% [6, 7], and 11.8% [8], respectively. Thus, there is a higher incidence of POPF after DP than that after PD [9]. Various risk factors for POPF after DP have been reported thus far, including obesity, younger age, malnutrition, pancreatic thickness, and soft pancreatic texture (i.e., soft pancreas) [10–13]. Although most of these factors can be evaluated preoperatively, pancreatic texture can be determined only by intraoperative findings. Recently, fat deposition in pancreatic parenchyma—related to soft pancreas—has been reported to be strongly associated with POPF after PD, and it is represented by a low pancreatic parenchymal CT value [14, 15]. In addition, preoperative CT images have reportedly been useful in hepatobiliary and pancreatic surgery [16, 17]. In this regard, we have recently reported that the pancreas-visceral fat CT value ratio (PVFR) and serrated pancreatic contour, which can be obtained by preoperative CT images, were associated with fat deposition of the pancreatic parenchyma, and that these factors were selected as strong risk factors of POPF after PD [6]. However, these factors have not been examined for patients that underwent DP.
Thus, the aim of this study was to elucidate the risk factors for POPF after DP and to verify whether PVFR and serrated pancreatic contour could also serve as risk factors for POPF after DP, as they did for POPF after PD.
Methods
Patients
Of the 259 patients who underwent DP at the Department of Hepatobiliary Pancreatic and Transplant Surgery of Mie University Hospital with a high volume of pancreatic resection during the 15-year period from January 2006 to December 2020, we excluded three patients whose preoperative CT images could not be referenced and five patients whose pancreatic parenchyma evaluations were difficult (two patients with remnant pancreatic duct stent after pancreaticoduodenectomy, two patients with severe atrophy/calcification, and one patient with pancreatic blastoma). The remaining 251 patients were identified as the study population (Additional file 1: Fig. S1).
The protocol for this research was approved by a suitably constituted Ethics Committee at the institution (Committee of the Institutional Review Board at Mie University of Japan, Approval No. H2021-024), and the study conformed to the provisions of the Declaration of Helsinki. Informed consents were obtained from all the participants through an opt-out form. Participants were explained that they could opt out of participation by filling out an opt-out form. The study received ethical approval for the anonymization of patient data, the absence of risks to the patient, and the potential benefit for the adequate management of POPF based on unbiased information. All data were fully anonymized before we accessed them.
Risk factor analysis for postoperative pancreatic fistula
Perioperative information and CT images were retrospectively extracted from medical records; univariate and multivariate analyses of risk factors for POPF after DP were performed. Preoperative factors that were evaluated in this study included age, sex, body mass index (BMI), history of preoperative diabetes mellitus (DM), diagnosis, history of preoperative chemoradiotherapy, and the hematologic examinations. Additionally, the preoperative nutritional scores evaluated included the prognostic nutritional index (PNI), neutrophil-to-lymphocyte ratio (NLR), and platelet-to-neutrophil ratio (PNR).
Intraoperative factors that were evaluated included operation time, intraoperative blood loss, surgical procedure (laparotomy or laparoscopy), combined splenectomy, combined portal vein resection, combined celiac axis resection, and simultaneous resection of the alimentary tract. Pancreatic texture could not be confirmed by laparoscopic surgery, and the description of pancreatic texture was omitted in the surgical records in some open surgery cases; therefore, this factor was not evaluated in the present study.
POPF was defined and graded according to the International Study Group on Pancreatic Surgery (ISGPS) in 2016 [18], with Grades B and C set as clinically relevant POPF (CR-POPF). The Clavien-Dindo classification (CD classification) was used for severity classification of postoperative complications [19].
Evaluation of pancreatic fat deposition and pancreatic morphology on preoperative CT
CT examinations were performed using a multidetector CT scanner; Aquilion ONE (Canon medical systems, Otawara, Tochigi, Japan) or LightSpeed 16VCT (GE Healthcare, Milwaukee, WI, USA) between 2006 and 2011, Aquilion ONE or Discovery 750 HD (GE Healthcare) between 2012 and 2014, Discovery 750 HD or SOMATOM Force (Siemens Healthineers, Erlangen, Bayern, Germany) between 2015 and 2018, and SOMATOM Force or Revolution EVO (GE Healthcare) between 2019 and 2020. After the non-contrast CT scan, a triple-phase contrast-enhanced CT scan was performed with a 1.25-mm slice thickness, including an arterial phase, a portal venous phase, and an equilibrium phase. Contrast material was administered intravenously by a power injector. The arterial phase was obtained using a bolus-tracking technique. The scanning delays of the portal phase were approximately 60–70 s, and those of the equilibrium phase were 130–180 s after the start of the contrast material injection.
To represent pancreatic fat deposition, the PVFR was determined from preoperative CT by using the method described in our previous report [6]. The CT values were measured at the future remnant pancreatic head for the pancreatic parenchyma and the left side of the stomach for visceral fat (Fig. 1). The CT values (mean values) were measured at four different locations with regions of interest (ROIs) of 15–30 mm2 at sites where the vessels did not overlap while comparing the non-contrast CT with the contrast-enhanced CT; the mean CT values of the four measurements was calculated and adopted. The PVFR was calculated as the mean pancreatic parenchymal CT value / mean visceral fat CT value.
Fig. 1.

Measurement of the CT value of the remnant pancreatic parenchyma (a) and visceral fat (b). HU Hounsfield units, PVFR pancreas-visceral fat ratio
Pancreatic morphology was categorized as normal with a smooth margin (smooth type) or an irregular serrated pancreatic contour with protrusions of 3 mm or more (serrated type) (Fig. 2). The pancreatic parenchymal thickness was measured as previously reported [20–22]. It was the value in the direction perpendicular to the long axis of the pancreas on the pancreatic dissection line in the horizontal section of the preoperative CT, identified prior to postoperative CT on postoperative day (POD) 2–17 or according to their operation records.
Fig. 2.

Classification of pancreatic morphology. a Smooth type: smooth interlobular border. b Serrated type: feathery, irregular interlobular border, and a protrusion of more than 3 mm
Surgical procedure and postoperative management
A total of 34 surgeons performed DP during the study period. Pancreatic stump closure for open surgery was performed using hand-sewn or stapled closure technique. In the case of hand-sewn occlusion of the pancreatic cut end, the pancreatic parenchyma was transected using an ultrasonic coagulation cutting device (SonoSurg; Olympus Optical Co. Ltd., Tokyo, Japan) followed by either main pancreatic duct ligation and suture ligation using the fish-mouth method. Regarding the staple closure technique, pancreatic parenchyma was divided with a bare or mesh-reinforced triple-row stapler (Endo GIA Tri-Staple™ or NEOVEIL Endo GIA Reinforced Reload, Covidien, North Haven, CT, USA) using a purple (3 mm) or black (4 mm) cartridge, selected by the surgeon according to the thickness of the transection line. In laparoscopic surgery, pancreatic stump was closed using a linear stapler or endoscopic hand-sewn technique as well as open surgery. None of the cases involved gastrointestinal anastomosis with the remnant pancreas or pancreatic duct occlusion [23]. A closed suction drain was placed at the pancreatic stump and/or left subphrenic space based on the surgeon’ judgement.
The basic postoperative and POPF management used in this study has been described in our previous report [24]. Prophylactic antibiotics (second-generation cephalosporin) were administered through POD 2. The amylase content of the discharge from the closed-suction drain was evaluated at POD 1, 3, and until drain removal. In the absence of high amylase values more than thrice the upper limit of normal, drains were removed after POD 3. Postoperative CT was routinely performed on POD 6–8 to evaluate peripancreatic fluid collections. Prophylactic somatostatin analogs were not used. A therapeutic antibiotic was immediately initiated when patients showed signs of clinical infection after DP. Regimens of therapeutic antibiotics, which include carbapenem, piperacillin/tazobactam, cephalosporins, ampicillin/sulbactam, and quinolone, were determined by the surgeon empirically or according to the result of bacterial cultures. Postoperative drainage was performed when a peripancreatic fluid collection was detected on postoperative CT and considered to be the source of inflammation.
Statistical analysis
The normality of data distribution was investigated using the Shapiro–Wilk test; parametric continuous variables were analyzed using Student’s t-test, and the non-parametric continuous variables were analyzed using a Mann–Whitney U test. Categorical variables were analyzed using a χ2 test. The significance level was set to P < 0.05; multivariate analysis was conducted using multiple logistic analysis, with variables showing significant differences in univariate analysis set as independent variables. The optimal cut-off value was determined using the Youden index from the receiver operating characteristic (ROC) curve. All statistical analyses were conducted using SPSS (version 26; IBM Japan, Tokyo Japan).
Results
We retrospectively collected data from 259 patients who underwent DP at the Department of Hepatobiliary Pancreatic and Transplant Surgery of Mie University Hospital from January 2006 to December 2020. The institution is known to have a high volume of pancreatic resections. Three patients were excluded because their preoperative CT images could not be referenced. Another five were excluded due to difficulty in the evaluation of pancreatic parenchyma, and the remaining 251 patients were included in the present study.
Characteristics of the patients and preoperative CT evaluation
Table 1 presents the data for patient characteristics and intraoperative factors. The median patient age was 68 years (3–89 years), and the study population included 147 male (58.7%) and 104 female (41.3%) patients. The median BMI was 21.4 kg/m2 (13.6–34.7 kg/m2), and 64 patients had preoperative DM (25.5%); the most common diagnosis was pancreatic ductal adenocarcinoma (PDAC; 105 cases, 41.8%). Preoperative therapy was performed in 67 patients (26.7%): chemoradiotherapy (CRT) was performed in 54 patients and chemotherapy in 13 patients. Thirteen PDAC patients received gemcitabine-based CRT between January 2006 and October 2011. Forty-one patients received S-1 + GEM (GS)-based CRT between November 2011 and December 2020, and the remaining 13 patients received GS chemotherapy. Our preoperative treatment strategies for pancreatic ductal adenocarcinoma have been described in a previous report [25]. The median operation time was 322 min (132–830 min), and the median blood loss was 404 mL (0–5,033 mL). Laparoscopic surgery was performed in 87 patients (34.7%).
Table 1.
Characteristics of 251 patients that underwent distal pancreatectomy
| Characteristics | Value |
|---|---|
| Age, years | 68 (3–89) |
| Sex, male / female | 147 / 104 |
| Body mass index, kg/m2 | 21.4 (13.6–34.7) |
| Diabetes mellitus, n | 64 (25.5%) |
| Diagnosis, n | |
| Pancreatic ductal adenocarcinoma | 105 (41.8%) |
| Intraductal papillary mucinous neoplasm | 51 |
| Pancreatic neuroendocrine tumor | 31 |
| Solid pseudopapillary neoplasm | 10 |
| Mucinous cystic neoplasm | 9 |
| Metastatic tumor | 8 |
| Serous cystic neoplasm | 6 |
| Others | 31 |
| Preoperative therapy, n | 67 (26.7%) |
| Chemoradiotherapy, n | 54 |
| Chemotherapy, n | 13 |
| Intraoperative characteristics | |
| Operation time, min | 322 (132–830) |
| Blood loss, ml | 404 (0–5033) |
| Laparoscopic surgery, n | 87 (34.7%) |
| Without splenectomy, n | 25 (10.0%) |
| Combined PV resection, n | 8 (3.2%) |
| Combined CA resection, n | 10 (4.0%) |
| Stapler closer of pancreatic cut end, n | 66 (26.3%) |
| Simultaneous resection of alimentary tract, n | 27 (10.8%) |
Data are expressed as number (percentage), median (range), PV portal vein, CA celiac axis
Preoperative CT evaluation revealed a serrated type pancreas in 80 patients (31.9%) (Table 2). The median pancreatic thickness was 9.3 mm (4.0–22.0 mm), median CT value of the pancreatic parenchyma was 41.8 HU (4.3–73.2 HU), and median PVFR value was -0.41 (-4.88 to -0.04).
Table 2.
Preoperative CT evaluation before distal pancreatectomy
| CT findings | Value |
|---|---|
| Morphology | |
| Smooth type | 171 (68.1%) |
| Serrated type | 80 (31.9%) |
| Pancreas thickness, mm | 9.3 (4.0–22.0) |
| CT value | |
| Pancreas, HU | 41.8 (4.3–73.2) |
| Visceral fat, HU | − 102.1 (− 8.3–-202.2) |
| PVFR | − 0.41 (− 4.88–-0.04) |
Data are expressed as number (percentage), median (range), HU Hounsfield units, PVFR pancreas-visceral fat CT value ratio
Incidence and severity of postoperative pancreatic fistula
CR-POPF developed in 86 patients (34.3%), including Grade B in 83 patients (33.1%) and Grade C in three patients (1.2%) (Table 3). Among the patients with Grade B, 30 improved with therapeutic antibiotics alone (CD classification II), while 53 required drain tube replacement and/or additional interventions (CD classification IIIa). Of these 53 patients, 33 (62.3%) required percutaneous drainage. Grade C was observed in three patients, of which one patient underwent additional resection of the residual pancreas at the splenic hilum using the Warshaw technique (CD classification IIIb), one underwent a transverse colon resection and splenic artery stent placement due to puncture of the splenic artery pseudoaneurysm (CD classification IVa), and one developed septic shock and required intensive care in the intensive care unit (CD classification IVb).
Table 3.
Details of POPF according to Clavien–Dindo classification
| POPF | Cases | Clavien–Dindo classification | |||||
|---|---|---|---|---|---|---|---|
| II | IIIa | IIIb | IVa | IVb | V | ||
| BL | 28 (11.2%) | ||||||
| CR-POPF | 86 (34.2%) | ||||||
| Grade B | 83 (33.1%) | 30a | 53b | ||||
| Grade C | 3 (1.2%) | 1c | 1d | 1e | – | ||
BL biochemical leak, CR-POPF clinically relevant-postoperative pancreatic fistula
aRequired antibiotic therapy
bRequired drain tube replacement and/or additional interventions
cResidual pancreas resection at the splenic hilum after Warshaw operation
dTransverse colon resection for penetration of splenic artery pseudoaneurysm
eRequired ICU managements (septic shock)
Risk factors of clinically relevant postoperative pancreatic fistula
Univariate analysis of the risk factors for CR-POPF identified younger age (P = 0.005), high BMI (P = 0.001), absence of DM (P = 0.002), high preoperative CRP value (P = 0.024), pancreatic thickness (P < 0.001), and high pancreatic parenchymal CT value (P = 0.018) as risk factors (Table 4). However, a serrated type pancreas (P = 0.122) and PVFR (P = 0.373) were not identified as risk factors. The duration of hospital stay was significantly longer in the CR-POPF group (P < 0.001).
Table 4.
Risk factors of CR-POPF using the univariate and multivariate analyses
| Factors | Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|---|
| None POPF / BL (n = 165) | CR-POPF (n = 86) | P-value | β | Odds ratio | CI | P-value | |
| Preoperative factors | |||||||
| Sex, male / female | 90 / 75 | 57 / 29 | 0.073 | ||||
| Age, years | 70 (3–87) | 64 (20–89) | 0.005 | ||||
| BMI, kg/m2 | 21.0 (14.0–30.4) | 22.9 (13.6–34.7) | 0.001 | 0.105 | 1.111 | 1.009–1.223 | 0.032 |
| DM, n | 52 (31.5%) | 12 (14.0%) | 0.002 | − 1.33 | 0.265 | 0.123–0.567 | 0.001 |
| PDAC, n | 75 (45.5%) | 30 (34.9%) | 0.069 | ||||
| Preoperative chemoradiotherapy, n | 41 (24.8%) | 13 (15.1%) | 0.075 | ||||
| Blood examination | |||||||
| White blood count, /μl | 5,140 (2,410–12,430) | 5,310 (2,530–12,910) | 0.35 | ||||
| Albumin, g/dl | 4.1 (2.5–5.0) | 4.1 (2.9–5.2) | 0.802 | ||||
| Creatinine, mg/dl | 0.7 (0.4–2.6) | 0.8 (0.4–1.7) | 0.454 | ||||
| BUN, mg/dl | 15.0 (6.0–37.0) | 14.0 (5.0–32.0) | 0.302 | ||||
| Cholesterol, mg/dl | 187 (103–321) | 191 (104–528) | 0.135 | ||||
| Triglyceride, mg/dl | 94 (30–328) | 109 (34–426) | 0.106 | ||||
| AMY, U/l | 75.0 (9.0–1553.0) | 74.0 (38.9–275.0) | 0.667 | ||||
| CRP, mg/dl | 0.07 (0.01–8.02) | 0.11 (0.00–3.38) | 0.024 | ||||
| NLR | 2.2 (0.7–12.5) | 2.3 (0.8–18.0) | 0.978 | ||||
| PNR | 151 (44–667) | 153 (54–4,233) | 0.996 | ||||
| PNI | 48.0 (30.9–62.1) | 48.7 (32.9–60.1) | 0.412 | ||||
| Intraoperative factors | |||||||
| Operation time, min | 311 (138–830) | 337 (132–754) | 0.237 | ||||
| Blood loss, ml | 356 (0–5033) | 515 (0–3520) | 0.086 | ||||
| Laparoscopic surgery, n | 59 (35.8%) | 28 (32.6%) | 0.359 | ||||
| without splenectomy, n | 13 (7.9%) | 12 (14.0%) | 0.098 | ||||
| Combined PV resection, n | 5 (3.0%) | 3 (3.5%) | 0.556 | ||||
| Combined CA resection, n | 6 (3.6%) | 4 (4.7%) | 0.467 | ||||
| Stapler closer of pancreatic cut end, n | 47 (28.5%) | 19 (22.1%) | 0.126 | ||||
| Simultaneous resection of AT, n | 17 (10.3%) | 10 (11.6%) | 0.451 | ||||
| CT evaluation | |||||||
| Morphology, smooth / serrated | 117 / 48 | 54 / 32 | 0.122 | ||||
| Pancreas thickness, mm | 8.8 (4.0–22.0) | 10.1 (4.6–20.7) | < 0.001 | 0.199 | 1.22 | 1.092–1.363 | < 0.001 |
| CT value | |||||||
| Pancreas, HU | 41.0 (4.5–73.2) | 44.2 (4.3–61.8) | 0.018 | ||||
| PVFR | -0.41 (-4.88–-0.05) | -0.42 (-1.19–-0.04) | 0.373 | ||||
| Hospital stays, days | 16 (7–99) | 36 (7–248) | < 0.001 | ||||
Data are expressed as number (percentage), median (range), CR-POPF: clinically relevant - postoperative pancreatic fistula, BL biochemical leak, BMI body mass index, DM diabetes mellitus, PDAC: pancreatic ductal adenocarcinoma, BUN blood urea nitrogen, AMY amylase, CRP C-reactive protein, NLR neutrophil-to-lymphocyte ratio, PNR platelet-to-neutrophil ratio, PNI prognostic nutritional index, PV portal vein, CA celiac axis, AT alimentary tract, HU Hounsfield units, PVFR pancreas-visceral fat CT value ratio
Multivariate analysis revealed that high BMI (odds ratio: 1.111; 95% CI: 1.709–1.223; P = 0.032), absence of DM (odds ratio: − 1.330; 95% CI: 0.123–0.567; P = 0.001), and pancreatic thickness (odds ratio: 1.220; 95% CI: 1.092–1.363; P < 0.001) were independent risk factors for CR-POPF (Table 4). The optimal cut-off values by ROC analysis were 22.4 kg/m2 (AUC: 0.632; sensitivity: 0.581; specificity: 0.697) for BMI and 12.4 mm (AUC: 0.662; sensitivity: 0.372; specificity: 0.927) for pancreatic thickness (Fig. 3).
Fig. 3.

ROC analysis of the risk factors for POPF after DP. ROC receiver operating characteristic, BMI body mass index, AUC area under the curve, PPV positive predictive value, NPV negative predictive value, POPF postoperative pancreatic fistula, DP distal pancreatectomy
Discussion
The present study is the first to show that PVFR and serrated pancreatic contour, which are risk factors for POPF after PD, do not increase the risk of POPF after DP. However, high BMI, absence of DM, and pancreatic thickness were shown to be independent risk factors of POPF after DP.
The incidence of POPF after DP differs between reports, but the results of a large-scale, multi-center, joint study in Japan in 2015 [1] reported an incidence of 28.2% with open surgery and 18.4% with laparoscopic surgery. Several DP-related randomized controlled trials after 2016 [2–4] reported POPF incidence rates of 16.0–18.9%, and a recent meta-analysis [5] reported an incidence of 20.4%, indicating that this complication has a relatively high frequency of occurrence regardless of advancements in surgical techniques. The incidence of CR-POPF in the present study was 34.3%, higher than that in previous reports. In the present study, the incidence of CR-POPF did not differ significantly according to pancreatic stump closure method (hand-sewn closure vs. stapler). Furthermore, the hand-sewn closure method in the laparoscopic surgery—previously adopted in our department—was performed for 33 patients, but CR-POPF was observed in only 10 cases (30.3%); thus, incidence of CR-POPF in our department was not particularly high. Although various reports have evaluated the optimal pancreatic stump closure method for POPF reduction, no consensus has been established, and further studies are needed to identify a closure method that reduces the incidence of CR-POPF. Furthermore, based on our previous report [24], a consideration from the perspectives of intraoperative and postoperative management indicated that the inappropriate drainage tube placement and/or number of drain tubes in our department may have increased the number of cases requiring additional intervention and may have also resulted in excessive use of postoperative therapeutic antibiotics. If the drainage is appropriate, the drain can be removed at an early stage; furthermore, if the indication for therapeutic antibiotic use is judged more strictly, then it would not result in Grade B CR-POPF, and there may be more cases that would heal with a biochemical leak (BL). Although these are all speculations, further improvements are needed in the future both for intraoperative drain tube placement and the postoperative antibiotic usage method.
The previously reported representative risk factors for POPF after DP include obesity, younger age, malnutrition, and soft pancreas [10–13], but many reports have indicated that pancreatic thickness is the most important risk factor [26]. As the global population ages, the demand for pancreatic surgery in elderly patients has increased [27, 28]. Such patients also have a higher incidence of frailty [29], which has been associated with higher morbidity in HBP surgery [30]. Conversely, younger age has been reported as a risk factor for POPF after DP. We consider this as one of the notable features of POPF after DP that differ from other HPB surgery. Univariate analysis in the present study showed that, among the above-mentioned factors, high BMI (obesity), younger age, and pancreatic thickness were detected as risk factors, and multivariate analysis showed that high BMI (obesity) and pancreatic thickness were detected as independent risk factors; these results are similar to those in previous reports. The present study also indicated absence of DM as an independent risk factor in multivariate analysis. Although few report have indicated absence of DM as a risk factor, a recent meta-analysis [5] reported that DM was a significant protective factor for CR-POPF after DP. Exocrine function as well as endocrine function was reduced in DM patients [31], therefore this may have increased the incidence of POPF.
Several reports have performed risk factor analysis of POPF after pancreatic resection by using preoperative CT values, as we have focused on in the present study. In particular, a frequently used value is the pancreas/spleen CT value ratio (P/S ratio), obtained by dividing the pancreatic parenchymal CT value by the spleen CT value; it is based on the liver/spleen CT value ratio commonly used for evaluating fatty liver [32]. The P/S ratio has been reported to represent pancreatic fat deposition and is an index of a soft pancreas in both patients who underwent PD [14] and DP [21], and a significant risk factor of POPF. Furthermore, we had previously discovered that the PVFR, which is based on the P/S ratio and serrated pancreatic contour could be used to predict the fat deposition of the pancreatic parenchyma, and that these findings are risk factors of POPF in PD [6]. Therefore, in the present study, we calculated the PVFR and identified the serrated type pancreas to verify if they could also serve as risk factors of POPF after DP. Specifically, we initially hypothesized that the PVFR and serrated type pancreas, which represent pancreatic fat deposition and a soft pancreas, reflect the fragility of the pancreas, and that a fragile pancreatic stump would be prone to collapse and be more likely to induce POPF. However, our univariate and multivariate analysis showed that the PVFR and serrated type pancreas did not serve as risk factors. Rather, the pancreatic parenchymal CT value was significantly higher in the CR-POPF group, indicating that pancreas fat deposition in this group might be milder than in the non POPF/BL group. Furthermore, an investigation on POPF after DP by Mori et al. [15] indicated that patients with a high pancreatic parenchymal CT value or P/S ratio had mild pancreatic fat deposition and maintained pancreatic exocrine function, and showed a significantly higher POPF incidence than those who do not; these results are similar to the findings of the present study. It is clear that a soft pancreas is a risk factor for POPF after PD, but whether it is a risk factor for POPF after DP, is still controversial [21, 33, 34]. However, the present results seem to indicate that the risk of POPF after DP is higher among patients with less pancreas fat deposition, maintained pancreatic endocrine/exocrine function, less atrophy, and thicker pancreas compared to those with a fragile pancreas with fat deposition. The present results contradict our hypothesis, but to our knowledge, there have been no previous studies that investigated PVFR and morphological characteristics of the pancreas (i.e., serrated type pancreas) as risk factors of POPF after DP; therefore, the present study can provide valuable investigative data in this regard.
The following aspects can be considered as limitations of the present study: (i) this was a retrospective study with a small sample size from a single facility; (ii) the study period was long, potentially introducing various biases related to changes in postoperative management policies, surgical techniques, and pancreatic stump closure method; (iii) the evaluation of pancreatic morphology and CT value measurement method lacked objectivity; although criteria have been set for evaluation of pancreatic morphology, the influence of the evaluator’s subjectivity cannot be excluded; (iv) furthermore, CT value measurements were conducted so as not to overlap with the blood vessels and ducts in comparison with contrast-enhanced CT, but this process was not conducted mechanically, and there were problems with its accuracy. The conclusions drawn from the results of the present study should be interpreted in the light of these limitations and evaluated further in future studies.
Conclusion
PVFR and serrated pancreatic contour evaluated with preoperative CT did not constitute risk factors of POPF after DP, unlike the findings for PD. High BMI, absence of DM, and pancreatic thickness have been shown to be independent risk factors, and the risk of POPF after DP is thought to be higher among those with a closer-to-normal pancreas with minimal fat deposition or atrophy.
Supplementary Information
{kind=link}
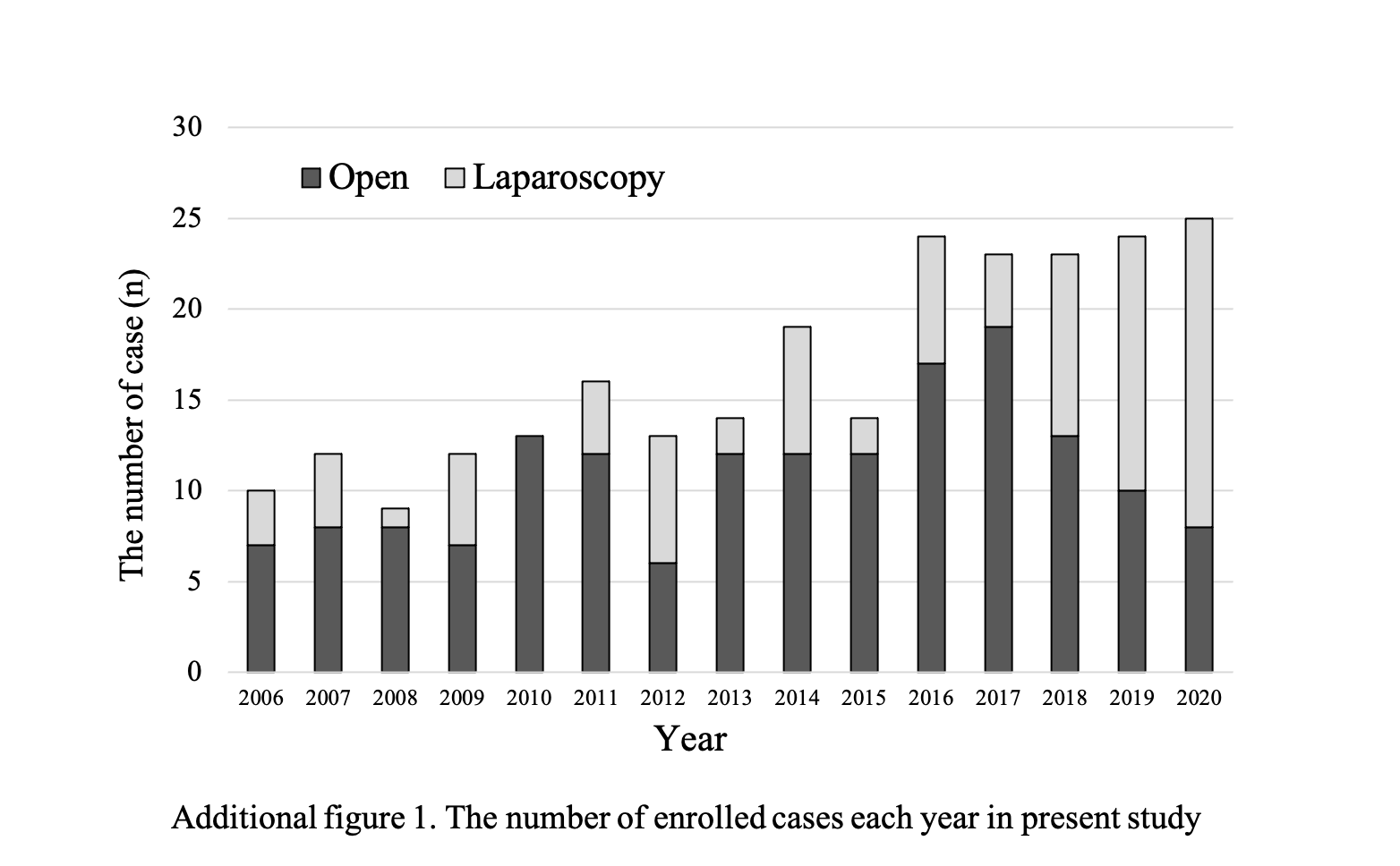
Additional file 1: Fig. S1. The number of enrolled cases each year in present study.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Abbreviations
- BL
Biochemical leak
- BMI
Body mass index
- CR
Clinically relevant
- CRP
C-reactive protein
- DM
Diabetes mellitus
- DP
Distal pancreatectomy
- ISGPS
International Study Group on Pancreatic Surgery
- NLR
Neutrophil-to-lymphocyte ratio
- PD
Pancreaticoduodenectomy
- PNI
Prognostic nutritional index
- PNR
Platelet-to-neutrophil ratio
- POPF
Postoperative pancreatic fistulas
- PVFR
Pancreas-to-visceral fat ratio
- ROC
Receiver operating characteristic
- ROI
Regions of interest
Author contributions
Study design: MK and KN. Data analysis: MK. Data acquisition: YT, IT, GK, HA, FT, IY, MY, TA, KM and SH. Draft and revision of the manuscript: MK, KN. Critical revision and accountability of the study: MS. All authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available as they consist of confidential patient data; however, data will be made available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The protocol for this research was approved by a suitably constituted Ethics Committee at the institution (Committee of the Institutional Review Board at Mie University of Japan, Approval No. H2021-024), and the study conformed to the provisions of the Declaration of Helsinki. Informed consents were obtained from all the participants through an opt-out form. Participants were explained that they could opt out of participation by filling out an opt-out form. This consent procedure was approved by the Committee of the Institutional Review Board at Mie University of Japan. The study received ethical approval for the anonymization of patient data, the absence of risks to the patient, and the potential benefit for the adequate management of POPF based on unbiased information. All data were fully anonymized before we accessed them.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Nakamura M, Wakabayashi G, Miyasaka Y, Tanaka M, Morikawa T, Unno M, et al. Multicenter comparative study of laparoscopic and open distal pancreatectomy using propensity score-matching. J Hepatobil Pancreat Sci. 2015;22:731–736. doi: 10.1002/jhbp.268. [DOI] [PubMed] [Google Scholar]
- 2.Kawai M, Hirono S, Okada K, Sho M, Nakajima Y, Eguchi H, et al. Randomized controlled trial of pancreaticojejunostomy versus stapler closure of the pancreatic stump during distal pancreatectomy to reduce pancreatic fistula. Ann Surg. 2016;264:180–187. doi: 10.1097/SLA.0000000000001395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Uemura K, Satoi S, Motoi F, Kwon M, Unno M, Murakami Y. Randomized clinical trial of duct-to-mucosa pancreaticogastrostomy versus handsewn closure after distal pancreatectomy. Br J Surg. 2017;104:536–543. doi: 10.1002/bjs.10458. [DOI] [PubMed] [Google Scholar]
- 4.Wennerblom J, Ateeb Z, Jönsson C, Björnsson B, Tingstedt B, Williamsson C, et al. Reinforced versus standard stapler transection on postoperative pancreatic fistula in distal pancreatectomy: multicentre randomized clinical trial. Br J Surg. 2021;108:265–270. doi: 10.1093/bjs/znaa113. [DOI] [PubMed] [Google Scholar]
- 5.Chong E, Ratnayake B, Lee S, French JJ, Wilson C, Roberts KJ, et al. Systematic review and meta-analysis of risk factors of postoperative pancreatic fistula after distal pancreatectomy in the era of 2016 International Study Group pancreatic fistula definition. HPB (Oxford) 2021;23:1139–1151. doi: 10.1016/j.hpb.2021.02.015. [DOI] [PubMed] [Google Scholar]
- 6.Kusafuka T, Kato H, Iizawa Y, Noguchi D, Gyoten K, Hayasaki A, et al. Pancreas-visceral fat CT value ratio and serrated pancreatic contour are strong predictors of postoperative pancreatic fistula after pancreaticojejunostomy. BMC Surg. 2020;20:129. doi: 10.1186/s12893-020-00785-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Maggino L, Malleo G, Bassi C, Allegrini V, McMillan MT, Borin A, et al. Decoding grade B pancreatic fistula: a clinical and economical analysis and subclassification proposal. Ann Surg. 2019;269:1146–1153. doi: 10.1097/SLA.0000000000002673. [DOI] [PubMed] [Google Scholar]
- 8.Mazzaferro V, Virdis M, Sposito C, Cotsoglou C, DrozDitBusset M, et al. Permanent pancreatic duct occlusion with neoprene-based glue injection after pancreatoduodenectomy at high risk of pancreatic fistula: a prospective clinical study. Ann Surg. 2019;270:791–798. doi: 10.1097/SLA.0000000000003514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.McMillan MT, Christein JD, Callery MP, Behrman SW, Drebin JA, Hollis RH, et al. Comparing the burden of pancreatic fistulas after pancreatoduodenectomy and distal pancreatectomy. Surgery. 2016;159:1013–1022. doi: 10.1016/j.surg.2015.10.028. [DOI] [PubMed] [Google Scholar]
- 10.Zhou Y, Drake J, Deneve JL, Behrman SW, Dickson PV, Shibata D, et al. Rising BMI is associated with increased rate of clinically relevant pancreatic fistula after distal pancreatectomy for pancreatic adenocarcinoma. Am Surg. 2019;85:1376–1380. doi: 10.1177/000313481908501232. [DOI] [PubMed] [Google Scholar]
- 11.Ecker BL, McMillan MT, Allegrini V, Bassi C, Beane JD, Beckman RM, et al. Risk factors and mitigation strategies for pancreatic fistula after distal pancreatectomy: analysis of 2026 resections from the International, Multi-institutional Distal Pancreatectomy Study Group. Ann Surg. 2019;269:143–149. doi: 10.1097/SLA.0000000000002491. [DOI] [PubMed] [Google Scholar]
- 12.Kawaida H, Kono H, Watanabe M, Hosomura N, Amemiya H, Fujii H. Risk factors of postoperative pancreatic fistula after distal pancreatectomy using a triple-row stapler. Surg Today. 2018;48:95–100. doi: 10.1007/s00595-017-1554-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kollár D, Huszár T, Pohárnok Z, Cselovszky É, Olah A. A review of techniques for closure of the pancreatic remnant following distal pancreatectomy. Dig Surg. 2016;33:320–328. doi: 10.1159/000445017. [DOI] [PubMed] [Google Scholar]
- 14.Yardimci S, Kara YB, Tuney D, Attaallah W, Ugurlu MU, Dulundu E, et al. A simple method to evaluate whether pancreas texture can be used to predict pancreatic fistula risk after pancreatoduodenectomy. J Gastrointest Surg. 2015;19:1625–1631. doi: 10.1007/s11605-015-2855-7. [DOI] [PubMed] [Google Scholar]
- 15.Mori N, Sakurai N, Iizawa H. Predicting postoperative pancreatic fistula after distal pancreatectomy by measuring the CT value ratio of future pancreas remnant to spleen (P/S ratio) in preoperative unenhanced CT images. Jpn J Gastroenterol Surg. 2019;52(9):485–493. doi: 10.5833/jjgs.2017.0181. [DOI] [Google Scholar]
- 16.Rocca A, Brunese MC, Santone A, Avella P, Bianco P, Scacchi A, et al. Early diagnosis of liver metastases from colorectal cancer through CT radiomics and formal methods: a pilot study. J Clin Med. 2021;11:31. doi: 10.3390/jcm11010031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rossi G, Altabella L, Simoni N, Benetti G, Rossi R, Venezia M, et al. Computed tomography-based radiomic to predict resectability in locally advanced pancreatic cancer treated with chemotherapy and radiotherapy. World J Gastrointest Oncol. 2022;14:703–715. doi: 10.4251/wjgo.v14.i3.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bassi C, Marchegiani G, Dervenis C, Sarr M, Hilal MA, Adham M, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161:584–591. doi: 10.1016/j.surg.2016.11.014. [DOI] [PubMed] [Google Scholar]
- 19.Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213. doi: 10.1097/01.sla.0000133083.54934.ae. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sugimoto M, Gotohda N, Kato Y, Takahashi S, Kinoshita T, Shibasaki H, et al. Risk factor analysis and prevention of postoperative pancreatic fistula after distal pancreatectomy with stapler use. J Hepatobiliary Pancreat Sci. 2013;20:538–544. doi: 10.1007/s00534-013-0596-0. [DOI] [PubMed] [Google Scholar]
- 21.Fukuda Y, Yamada D, Eguchi H, Iwagami Y, Noda T, Asaoka T, et al. A novel preoperative predictor of pancreatic fistula using computed tomography after distal pancreatectomy with staple closure. Surg Today. 2017;47:1180–1187. doi: 10.1007/s00595-017-1495-9. [DOI] [PubMed] [Google Scholar]
- 22.Yoshino J, Ban D, Ogura T, Ogawa K, Ono H, Mitsunori Y, et al. The clinical implications of peripancreatic fluid collection after distal pancreatectomy. World J Surg. 2019;43:2069–2076. doi: 10.1007/s00268-019-05009-8. [DOI] [PubMed] [Google Scholar]
- 23.Giuliani A, Avella P, Segreto AL, Izzo ML, Buondonno A, Coluzzi M, et al. Postoperative outcomes analysis after pancreatic duct occlusion: a safe option to treat the pancreatic stump after pancreaticoduodenectomy in low-volume centers. Front Surg. 2021;8:804675. doi: 10.3389/fsurg.2021.804675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Maeda K, Kuriyama N, Nakagawa Y, Ito T, Hayasaki A, Gyoten K, et al. Optimal management of peripancreatic fluid collection with postoperative pancreatic fistula after distal pancreatectomy: significance of computed tomography values for predicting fluid infection. PLoS ONE. 2021;16:e0259701. doi: 10.1371/journal.pone.0259701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ichikawa K, Mizuno S, Hayasaki A, Kishiwada M, Fujii T, Iizawa Y, et al. Prognostic nutritional index after chemoradiotherapy was the strongest prognostic predictor among biological and conditional factors in localized pancreatic ductal adenocarcinoma patients. Cancers (Basel) 2019;11:514. doi: 10.3390/cancers11040514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Miyasaka Y, Mori Y, Nakata K, Ohtsuka T, Nakamura M. Attempts to prevent postoperative pancreatic fistula after distal pancreatectomy. Surg Today. 2017;47:416–424. doi: 10.1007/s00595-016-1367-8. [DOI] [PubMed] [Google Scholar]
- 27.Giuliani A, Ceccarelli G, Rocca A. The role of laparoscopic distal pancreatectomy in elderly patients. Minerva Chir. 2018;73:179–187. doi: 10.23736/S0026-4733.18.07594-6. [DOI] [PubMed] [Google Scholar]
- 28.Yamashita M, Adachi T, Ono S, Matsumura N, Adachi T, Natsuda K, et al. Pancreaticoduodenectomy can be indicated for elderly patients: risk prediction using the Estimation of Physiologic Ability and Surgical Stress (E-PASS) system. J Hepatobiliary Pancreat Sci. 2021;28:165–173. doi: 10.1002/jhbp.840. [DOI] [PubMed] [Google Scholar]
- 29.Yamada M, Nishiguchi S, Fukutani N, Aoyama T, Arai H. Mail-based intervention for sarcopenia prevention increased anabolic hormone and skeletal muscle mass in community-dwelling Japanese older adults: The INE (Intervention by Nutrition and Exercise) study. J Am Med Dir Assoc. 2015;16:654–660. doi: 10.1016/j.jamda.2015.02.017. [DOI] [PubMed] [Google Scholar]
- 30.Komici K, Cappuccio M, Scacchi A, Vaschetti R, Delli Carpini G, Picerno V, et al. The prevalence and the impact of frailty in hepato-biliary pancreatic cancers: a systematic review and meta-analysis. J Clin Med. 2022;11:1116. doi: 10.3390/jcm11041116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Saisho Y. Pancreas volume and fat deposition in diabetes and normal physiology: consideration of the interplay between endocrine and exocrine pancreas. Rev Diabet Stud. 2016;13:132–147. doi: 10.1900/RDS.2016.13.132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Piekarski J, Goldberg HI, Royal SA, Axel L, Moss AA. Difference between liver and spleen CT numbers in the normal adult: its usefulness in predicting the presence of diffuse liver disease. Radiology. 1980;137:727–729. doi: 10.1148/radiology.137.3.6934563. [DOI] [PubMed] [Google Scholar]
- 33.Ridolfini MP, Alfieri S, Gourgiotis S, Di Miceli D, Rotondi F, Quero G, et al. Risk factors associated with pancreatic fistula after distal pancreatectomy, which technique of pancreatic stump closure is more beneficial? World J Gastroenterol. 2007;13:5096–5100. doi: 10.3748/wjg.v13.i38.5096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kah Heng CA, Salleh I, San TS, Ying F, Su-Ming T. Pancreatic fistula after distal pancreatectomy: incidence, risk factors and management. ANZ J Surg. 2010;80:619–623. doi: 10.1111/j.1445-2197.2010.05337.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Fig. S1. The number of enrolled cases each year in present study.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available as they consist of confidential patient data; however, data will be made available from the corresponding author on reasonable request.