

Abstract
Background:
Studies on endoscopic calcaneal spur resection (CSR) without plantar fascial release (PFR) are limited. This study aimed to review the data of patients who underwent fluoroscopic and endoscopic CSR without PFR for plantar fasciitis with a calcaneal spur to assess the effectiveness of CSR.
Methods:
Medical records of consecutive patients with plantar fasciitis with ≥2 mm calcaneal spur who underwent endoscopic CSR without PFR from November 2017 to December 2019 were reviewed. Patients with ≥2 years of follow-up were included, whereas those who underwent another surgery on the operated foot were excluded. Age, body mass index (BMI), follow-up duration, calcaneal spur length, duration to full weightbearing postoperatively, Japanese Society for Surgery of the Foot (JSSF) score, visual analog scale (VAS) score for pain, and complications were assessed.
Results:
The mean follow-up duration was 2.7 years. A total of 47 patients (31 female, 16 male; mean age, 56.4 years; mean BMI, 25.5) were included. The mean calcaneal spur length was 5.7 mm. The VAS score improved from 79.6 ± 12.9 mm preoperatively to 5.3 ± 7.3 mm postoperatively. The JSSF score improved from 54.0 ± 19.1 points preoperatively to 97.5 ± 5.7 points postoperatively (Wilcoxon signed-rank test, P < .001, respectively). The mean duration to full weightbearing postoperatively was 4.4 ± 4.2 days. Two patients presented with tenderness, and one presented with hypesthesia at the portal site.
Conclusion:
Endoscopic CSR without PFR resulted in good outcomes, early return to full weightbearing, and few complications in patients with plantar fasciitis with ≥2 mm calcaneal spur. The results suggested that CSR was sufficient to relieve symtoms and improve function. PFR may not be necessary for treating plantar fasciitis with calcaneal spur.
Level of Evidence:
Level IV, retrospective case series.
Keywords: minimally invasive surgery, Japanese Society for Surgery of the Foot score, visual analog scale score, heel pain, pathology, vertical stress, tensile loads
Introduction
Plantar fasciitis is defined as plantar heel pain at the insertion of the plantar fascia to the calcaneus due to degenerative changes. Conservative treatment, such as the use of heel pads or night splints, stretching exercise, local anesthetic injection, and extracorporeal shock wave therapy, may be applied initially. 22 However, after the failure of appropriate conservative management for >9-12 months, surgery may be the next option. 9 Operative treatments include endoscopic plantar fascial release (PFR), open plantar release with the release of the first branch of the lateral plantar nerve, and gastrocnemius recession.1,9,14
Among these procedures, endoscopic surgeries for plantar fasciitis have become increasingly common. 25 A randomized controlled trial study reported that endoscopic surgery was more effective than conservative treatment for patients with plantar fasciitis for >3 months. 17 Endoscopic procedures for plantar fasciitis include PFR without calcaneal spur resection (CSR) and PFR with CSR.2,3,5,6,8,11 -13,16,17,20,29,34 -37 Both procedures are reported to have good outcomes, suggesting that CSR might not be necessary for plantar fasciitis treatment.
On the contrary, many studies have indicated that the calcaneal spur is one of the causes of plantar fasciitis. 19 Pathologic studies have reported that the calcaneal spur was located on, not in, the plantar fascia, and its trabeculae are perpendicular to the plantar fascia, suggesting that the calcaneal spur receives vertical stress from the ground rather than tensile stress from the plantar fascia.21,24 Epidemiologic studies have suggested that the strongest point of tenderness for patients with heel pain was just beneath the spur, and people with calcaneal spur experienced them 4.6 times higher than those without the spur.7,27 Moreover, the occurrence rate of osteophytes in people with heel pain is higher than that in those without heel pain.28,38 According to meta-analyses, calcaneal spurs were associated with heel pain.15,26 These findings may support the hypothesis that endoscopic CSR can provide good outcomes. To date, only 1 study on endoscopic CSR without PFR reported good outcomes, 8 with the American Orthopaedic Foot & Ankle Society (AOFAS) score improving from 51.3 points preoperatively to 89.9 points postoperatively, and the visual analog scale (VAS) score for pain improving from 89 mm preoperatively to 13 mm postoperatively. However, the CSR in the study was performed in combination with platelet-rich plasma injection; therefore, whether the good outcome resulted from endoscopic CSR or platelet-rich plasma injection was unclear. If endoscopic CSR without PFR is effective, it would be better than endoscopic PFR combined with CSR, because the plantar fascia is preserved.
This study aimed to review a case series of plantar fasciitis with calcaneal spur that was treated with fluoroscopic and endoscopic CSR without PFR to assess the effectiveness of CSR.
Materials and Methods
Inclusion and Exclusion Criteria
With approval from the institutional review board of our hospital, we reviewed the medical records of patients with plantar fasciitis who underwent endoscopic surgery from November 2017 to December 2019. 30 Informed consent for the use of medical record data was obtained from all patients before surgery. 31 The diagnosis of plantar fasciitis was based on tenderness at the medial insertion of the plantar fascia to the calcaneus and the thickness of >4.0 mm on magnetic resonance imaging (MRI).10,17 After failing to respond to >6 months of conservative treatment, the patients with plantar fasciitis underwent endoscopic CSR with or without PFR. Patients with a calcaneal spur ≥2 mm underwent endoscopic CSR alone, and those with a calcaneal spur <2 mm underwent endoscopic PFR combined with CSR. The calcaneal spur length was measured preoperatively using computed tomography (CT) in the sagittal plane, which showed the longest calcaneal spur. The MRI findings of the plantar fascia were not considered when determining the application of surgical procedures. In this study, patients who underwent endoscopic CSR alone and were followed up for >2 years were included, and those who had previously undergone other surgeries on the same foot and were followed up for <2 years were excluded. 31 All procedures, data measurement, collection, and analyses were performed by the first author.
Surgical Technique
Preoperatively, a 3-dimensional CT of the calcaneus was conducted, and the surgeon confirmed the shape of the calcaneal spur when planning CSR.
The patient was placed supine on the operating table. The lower leg was sustained with a leg holder, and traction was applied to stabilize the operated foot (Figure 1). The fluoroscopy, fluoroscopy monitor, and arthroscopy monitor were placed on the unoperated side, and the surgeon stood at the end of the operating table. The C-arm was placed under the table to obtain a perfect lateral view of the calcaneus. The tip of the calcaneal spur was marked on the medial and lateral sides of the foot using the lateral view during fluoroscopy. When the line between the medial and lateral marks was not perpendicular to the axis of the foot, the position of the C-arm was adjusted to obtain a perfect lateral view, and the tip of the calcaneal spur was identified.
Figure 1.
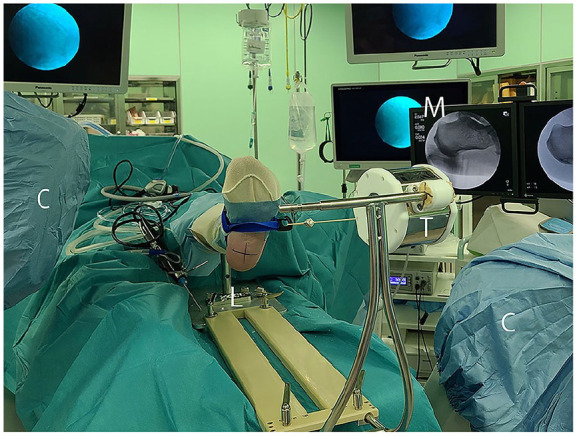
Photograph of the operating room. The cross mark on the plantar aspect of the foot shows that the line between the medial and lateral portals is perpendicular to the axis of the foot. C, C-arm; L, leg holder; M, monitors; T, traction device.
A 5-mm skin incision was made on the planned medial portal, and a straight mosquito forceps was introduced through the skin incision. The medial edge of the plantar fascia was palpated using the tip of the mosquito forceps, and the forceps was advanced on the plantar fascia to reach the calcaneal spur, where blunt dissection was performed (Figure 2A). The spur was on, not in, the plantar fascia; thus, separation of the spur and plantar fascia was possible.21,24 The mosquito forceps was extracted, and a 3.0-mm hooded abrasion bur (Formula, Stryker, Kalamazoo, MI, USA) was introduced from the medial portal.
Figure 2.

Overview of fluoroscopic procedures of the left calcaneus. The instruments were introduced from the medial portal. (A) Blunt dissection around the spur using a mosquito forceps. (B) Resection of the spur using a 3.0-mm hooded abrasion bur (Stryker). The hood of the bur is directed to the flexor digitorum brevis muscle to avoid damaging it.
The bur palpated the tip of the spur, and fluoroscopic resection was performed (Figure 2B). The hood of the bur was directed to the flexor digitorum brevis muscle to avoid damaging it. Both the medial and lateral edges of the spur were resected with internal and external rotations of the foot. The spur-resected space became the working space for endoscopy. After spur resection, the bur was extracted.
A 5-mm skin incision was made on the planned lateral portal. Blunt dissection was performed on the plantar fascia using straight mosquito forceps. The forceps was extracted, and a 2.3-mm, 30-degree arthroscope (Stryker) was introduced through the lateral portal and advanced on the plantar fascia to reach the spur-resected space (Figure 3A). An infusion pump (FloSteady, Stryker) was set to the autocalibration mode. 30 A 3.5-mm cutter (Formula, Stryker) was introduced through the medial portal and advanced to the arthroscopic view, and the debris was cleared. The plantar fascia remained attached to the calcaneus (Figure 3B). When the unresected spur was visible, it was removed using a cutter. The skin incisions were sutured using 4-0 nylon. A postoperative radiograph was obtained to confirm successful spur resection (Figure 4).
Figure 3.

Endoscopic view of the left calcaneus and plantar fascia from the lateral portal using a 2.3-mm 30-degree arthroscope. (A) Before endoscopic debridement. The plantar fascia was identified, but the calcaneus was difficult to identify due to the debris. (B) After endoscopic debridement. The plantar fascia was preserved and attached to the calcaneus. C, calcaneus; P, plantar fascia.
Figure 4.

Radiographs of the lateral view of the left calcaneus. (A) Preoperative. (B) Postoperative.
Postoperative Care
Full weightbearing without an orthosis was initiated 1 day after surgery, as tolerated. The nylon suture was removed 2 weeks postoperatively. Participation in sports activities was allowed 1 month after surgery, as tolerated. 31
Data Collection
Data included sex, age, body mass index (BMI), calcaneal spur length, VAS (0-100 mm) score for pain, Japanese Society for Surgery of the Foot (JSSF) scale score (0-100 points),32,33 duration to full weightbearing after surgery, and complications. 30 Preoperative data for review included data recorded within 1 month before surgery, and postoperative data included data recorded at the last outpatient visit. The VAS score represented the worst pain felt when performing activities of daily living and sports. 30
Statistical Analyses
The Wilcoxon signed-rank test was used to assess improvements in the VAS and JSSF scores. All tests were 2-tailed, and differences were considered significant when the P value was <.05. Post hoc power analyses were also performed.
All statistical analyses were performed using EZR (easy R) version 1.54 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), 18 which is a modified version of R version 4.0.3 commander (The R Foundation for Statistical Computing, Vienna, Austria), which was designed to add statistical functions for biostatistics.18,30
Results
Demographics
A total of 47 patients (31 females and 16 males) were included in this study. The mean patient age was 56.4 years (range, 35-84), and the mean BMI was 25.5 (range, 17.6-35.5). The mean follow-up duration was 2.7 (range, 2.0-7.9) years. The average calcaneal spur length was 5.7 (range, 2.0-11.0) mm (Table 1). None of the patients underwent reoperation.
Table 1.
Demographics (N = 47).
| Factor | n or Mean ± SD | Range |
|---|---|---|
| Sex, n | ||
| Female | 31 | |
| Male | 16 | |
| Age, y | 56.4 ± 9.8 | 35-84 |
| BMI | 25.5 ± 4.1 | 17.6-35.5 |
| Calcaneal spur length, mm | 5.7 ± 2.1 | 2-11 |
| Follow-up duration, y | 2.7 ± 0.5 | 2.0-4.1 |
Abbreviation: BMI, body mass index.
Preoperative and Postoperative Measurements
The VAS score improved from 79.6 ± 12.9 (median, 82; range, 48-100) mm preoperatively to 5.3 ± 7.3 (median, 2; range, 0-30) mm postoperatively (Wilcoxon signed-rank test, P < .001). The JSSF score improved from 54.0 ± 19.1 (median, 60; range, 24-85) points preoperatively to 97.5 ± 5.7 (median, 100; range, 70-100) points postoperatively (Wilcoxon signed-rank test, P < .001) (Table 2, Figure 5). Additionally, post hoc power analyses were performed. The required sample size calculated using α = 5%, power = 80%, difference of the mean = 74, and SD = 13 in terms of the VAS score was 3, and the required sample size calculated using α = 5%, power = 80%, difference of the mean = 43, and SD = 19, in terms of the VAS score was 4. Therefore, this study was sufficiently powered to detect improvements in outcomes. The mean duration to full weightbearing after surgery was 4.4 ± 4.2 days (median, 3; range, 1-19).
Table 2.
Preoperative and Postoperative Measures in Patients Treated With Endoscopic Calcaneal Spur Resection Without Plantar Fascia Release.
| Factor | Mean ± SD | Median | Range |
|---|---|---|---|
| Preop. VAS (mm) | 79.6 ± 12.9 | 82 | 48-100 |
| Postop. VAS (mm) | 5.3 ± 7.3 | 2 | 0-30 |
| Preop. JSSF (point) | 54.0 ± 19.1 | 60 | 24-85 |
| Postop. JSSF (point) | 97.5 ± 5.7 | 100 | 70-100 |
Abbreviations: JSSF, Japanese Society for Surgery of the Foot; postop., postoperative; preop., preoperative; VAS, visual analog scale.
Figure 5.

Preoperative and postoperative visual analog scale and Japanese Society for Surgery of the Foot score.
Complications
Two patients presented with tenderness, and 1 presented with hypesthesia at the portal site. No infection and injury of the first branch of the lateral plantar nerve occurred.
Discussion
In this study, fluoroscopic and endoscopic CSR without PFR for plantar fasciitis with calcaneal spur achieved good outcomes (Table 2, Figure 5). These results were similar to those of previous reports on endoscopic PFR combined with CSR.5,8,11,17,20,37 El Shazly et al 11 analyzed 24 patients with a follow-up duration of 24 months and reported that the VAS score improved from 82 to 6 mm. Komatsu et al 20 investigated 10 patients 24 months after surgery and found that their AOFAS score improved from 64 to 92 points. Tang et al 37 reported that the AOFAS score of 45 patients improved from 55 to 96 points. Moreover, the duration to full weightbearing in this study (4.4 days) was earlier than those in previous reports (Komatsu et al, 13.9 days 20 ; Tang et al, 14.2 days 37 ). Therefore, we believe that endoscopic CSR was sufficient and PFR may not be necessary for treating plantar fasciitis with calcaneal spur.
In this study, the good outcomes of endoscopic CSR without PFR indicated that a calcaneal spur was one of the causes of plantar fasciitis. Considering the pathologic findings of calcaneal spur described in the Introduction,21,24 vertical stress on the calcaneal spur from the plantar fascia may be a cause of pain. Additionally, Li and Muehleman reported in a pathological study where the plantar aponeurosis was attached to 46% of the calcaneal spur. 24 Considering this, the partial release of the plantar fascia attached to the calcaneal spur may be associated with pain alleviation. The pain resolution using endoscopic PFR without CSR2,3,6,12,13,16,29,34 -36 can be explained by a similar mechanism described above. Because of the PFR, the plantar fascia was released from the tensile loads, and the calcaneal spur avoided stresses from the plantar fascia. However, many other causes of plantar fasciitis have been advocated for, including nerve trap, bone bruise of the calcaneus, plantar fascia tightening, gastrocnemius contracture, neurogenesis, chronic degenerative changes in the plantar fascia origin,3,4 microtears of the plantar fascia, and collagen necrosis. 23 Moreover, in the case of plantar fasciitis without calcaneal spur, the causes of pain may differ from those of plantar fasciitis with calcaneal spur. Further studies are necessary to understand how these causes are related.
Our technique of creating a working space for endoscopy was different from the techniques used in previous reports on endoscopic PFR combined with CSR.5,8,11,17,20,37 In our method, the void left after spur resection was used as the working space for endoscopy. With the minimally invasive technique, we believe that the complication rate was low (6%) compared with that in previous reports (15%-30%5,8,11,20,37), and no injury occurred to the first branch of the lateral plantar nerve. Previous studies on endoscopic PFR combined with CSR have reported that a working space was created by resecting the plantar fascia and calcaneal spur, 5 fat tissue and plantar portion of the flexor digitorum brevis muscle, 20 or soft fibrous tissue.8,37 We believe that creating a working space under poor endoscopic view is more invasive and dangerous than our fluoroscopic technique because the endoscope will often move in the wrong direction in a poor endoscopic view, and many soft tissues must be destroyed to ensure a sufficient view.
This study had some limitations. First, this study had a small sample size; thus, subgroup analyses, such as those classified by sex, age, or BMI, were not performed. Second, the study had a relatively short follow-up. Third, the rate of spur regeneration was unknown because postoperative roentgenograph follow-up was not performed. Finally, there was no comparison group as this was a case series.
In conclusion, in patients with plantar fasciitis and a ≥2-mm calcaneal spur, endoscopic CSR without PFR resulted in good outcomes, early return to full weightbearing, and few complications.
Acknowledgments
The author would like to thank Elsevier and Enago (www.enago.jp) for the English language review.
Footnotes
Ethical approval: Ethical approval for this study was obtained from the Institutional Review Board of Yashio Central General Hospital (Approval number: YIHCE2021-01).
Declaration of Conflicting Interests: The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding: The author received no financial support for the research, authorship, and/or publication of this article.
ORCID iD: Kenichiro Nakajima, MD,  https://orcid.org/0000-0002-8649-2346
https://orcid.org/0000-0002-8649-2346
References
- 1. Arshad Z, Aslam A, Razzaq MA, Bhatia M. Gastrocnemius release in the management of chronic plantar fasciitis: a systematic review. Foot Ankle Int. 2022;43(4):568-575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Bader L, Park K, Gu Y, O’Malley M. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012;33(1):37-43. [DOI] [PubMed] [Google Scholar]
- 3. Bazaz R, Ferkel RD. Results of endoscopic plantar fascia release. Foot Ankle Int. 2007;28(5):549-556. [DOI] [PubMed] [Google Scholar]
- 4. Benjamin M, Toumi H, Ralphs J, Bydder G, Best T, Milz S. Where tendons and ligaments meet bone: attachment sites (‘entheses’) in relation to exercise and/or mechanical load. J Anatomy. 2006;208:471-490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Blanco CE, Leon HO, Guthrie TB. Endoscopic treatment of calcaneal spur syndrome: a comprehensive technique. Arthroscopy. 2001;17:517-522. [DOI] [PubMed] [Google Scholar]
- 6. Boyle RA, Slater GL. Endoscopic plantar fascia release: a case series. Foot Ankle Int. 2004;24(2):176-179. [DOI] [PubMed] [Google Scholar]
- 7. Brody B. Progressive changes in the pathology of a heel spur. J Am Podiatry Assoc. 1962;52:754-755. [PubMed] [Google Scholar]
- 8. Cottom JM, Maker JM, Richardson P, Baker JS. Endoscopic debridement for treatment of chronic plantar fasciitis: an innovative technique and prospective study of 46 consecutive patients. J Foot Ankle Surg. 2016;55:748-752. [DOI] [PubMed] [Google Scholar]
- 9. DiGiovanni BF, Dawson LK, Baumhauer JF. Plantar heel pain. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann’s Surgery of the Foot and Ankle. 9th ed. Elsevier Saunders; 2004;1910-1922. [Google Scholar]
- 10. Drake C, Whittaker GA, Kaminski MR, et al. Medical imaging for plantar heel pain: a systematic review and meta-analysis. J Foot Ankle Res. 2022;15(1):4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. El Shazly O, El Beltagy A. Endoscopic plantar fascia release, calcaneal drilling and calcaneal spur removal for management of painful heel syndrome. Foot. 2010;20:121-125. [DOI] [PubMed] [Google Scholar]
- 12. El Shazly O, El Hilaly R, El Soud M, El Sayed M. Endoscopic plantar fascia release by hooked soft-tissue electrode after failed shock wave therapy. Arthroscopy. 2010;26:1241-1245. [DOI] [PubMed] [Google Scholar]
- 13. Feng SM, Song RL, Wang AG, Sun QQ, Zhang SC. Endoscopic partial plantar fasciotomy via 2 medial portals vs mini-open procedure for refractory plantar fasciitis. Foot Ankle Int. 2021;42(4):458-463. [DOI] [PubMed] [Google Scholar]
- 14. Gamba C, Serrano-Chinchilla P, Ares-Vidal J, Solano-Lopez A, Gonzalez-Lucena G, Ginés-Cespedosa A. Proximal medial gastrocnemius release versus open plantar fasciotomy for the surgical treatment in recalcitrant plantar fasciitis. Foot Ankle Int. 2020;41(3):267-274. [DOI] [PubMed] [Google Scholar]
- 15. Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: a systematic review. J Sci Med Sport. 2006;9:11-22. [DOI] [PubMed] [Google Scholar]
- 16. Jerosch J, Schunck J, Liebsch D, Filler T. Indication, surgical technique and results of endoscopic fascial release in plantar fasciitis (EFRPF). Knee Surg Sports Traumatol Arthrosc. 2004;12:471-477. [DOI] [PubMed] [Google Scholar]
- 17. Johannsen F, Konradsen L, Herzog R, Krogsgaard MR. Endoscopic fasciotomy for plantar fasciitis provides superior results when compared to a controlled non-operative treatment protocol: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2020;28:3301-3308. [DOI] [PubMed] [Google Scholar]
- 18. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013;48:452-458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Kirkpatrick J, Yassaie O, Mirjalili SA. The plantar calcaneal spur: a review of anatomy, histology, etiology and key associations. J Anat. 2017;230:743-751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Komatsu F, Takao M, Innami K, Miyamoto W, Matsushita T. Endoscopic surgery for plantar fasciitis: application of a deep-fascial approach. Arthroscopy. 2011;27:1105-1109. [DOI] [PubMed] [Google Scholar]
- 21. Kumai T, Benjamin M. Heel spur formation and the subcalcaneal enthesis of the plantar fascia. J Rheumatol. 2002;29:1957-1964. [PubMed] [Google Scholar]
- 22. Landorf KB, Menz HB. Plantar heel pain and fasciitis. BMJ Clin Evid. 2008;2008:1111. [PMC free article] [PubMed] [Google Scholar]
- 23. Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J Am Podiatr Med Assoc. 2003;93:234-237. [DOI] [PubMed] [Google Scholar]
- 24. Li J, Muehleman C. Anatomic relationship of heel spur to surrounding soft tissues: greater variability than previously reported. Clin Anat. 2007;20:950-955. [DOI] [PubMed] [Google Scholar]
- 25. Malahias M, Cantiller E, Kadu V, Müller S. The clinical outcome of endoscopic plantar fascia release: a current concept review. Foot Ankle Surg. 2020;26:19-24. [DOI] [PubMed] [Google Scholar]
- 26. McMillan AM, Landorf KB, Barrett JT, Menz HB, Bird AR. Diagnostic imaging for chronic plantar heel pain: a systematic review and meta-analysis. J Foot Ankle Res. 2009;2:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Menz HB, Zammit GV, Landorf KB, Munteanu S. Plantar calcaneal spurs in older people: longitudinal traction or vertical compression? J Foot Ankle Res. 2008;1:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Moroney PJ, O’Neill BJ, Khan-Bhambro K, O’Flanagan SJ, Keogh P, Kenny PJ. The conundrum of calcaneal spur: do they matter? Foot Ankle Spec. 2014;7:95-101. [DOI] [PubMed] [Google Scholar]
- 29. Morton T, Zimmerman J, Lee M, Schaber J. A review of 105 consecutive uniport endoscopic plantar fascial release procedures for the treatment of chronic plantar fasciitis. J Foot Ankle Surg. 2013;52:48-52. [DOI] [PubMed] [Google Scholar]
- 30. Nakajima K. Arthroscopic sesamoidectomy for hallux sesamoid disorders. J Foot Ankle Surg. 2022;61:175-180. [DOI] [PubMed] [Google Scholar]
- 31. Nakajima K. Sliding oblique metatarsal osteotomy fixated with a K-wire without cheilectomy for hallux rigidus. J Foot Ankle Surg. 2022;61:279-285. [DOI] [PubMed] [Google Scholar]
- 32. Niki H, Aoki H, Inokuchi S, et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders I: development of standard rating system. J Orthop Sci. 2005;10:457-465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Niki H, Aoki H, Inokuchi S, et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders II: interclinician and intraclinician reliability and validity of the newly established standard rating scales and Japanese Orthopaedic Association rating scale. J Orthop Sci. 2005;10:466-474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Othman AM, Ragab EM. Endoscopic plantar fasciotomy versus extra corporeal shock wave therapy for treatment of chronic plantar fasciitis. Arch Orthop Trauma Surg. 2010;130:1343-1347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Radwan YA, Mansour AMR, Badawy WS. Resistant plantar fasciopathy: shock wave versus endoscopic plantar fascial release. Int Orthop. 2012;36:2147-2156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Saxena A. Uniportal endoscopic plantar fasciotomy: a prospective study on athletic patients. Foot Ankle Int. 2004;25(12):882-889. [DOI] [PubMed] [Google Scholar]
- 37. Tang Y, Deng P, Wang G, Yao Y, Luo Z, Xu Y. The clinical efficacy of two endoscopic surgical approaches for intractable plantar fasciitis. J Foot Ankle Surg. 2020;59:280-285. [DOI] [PubMed] [Google Scholar]
- 38. Vyce SD, Addis-Thomas E, Mathews EE, Perez SL. Painful prominences of the heel. Clin Podiatr Med Surg. 2010;27:443-462. [DOI] [PubMed] [Google Scholar]