

Abstract
Following the healing of venous leg ulcers, the primary problems for nursing and patients are adhering to compression therapy and preventing ulcer recurrence. As a result, it is important that patients comprehend their situation. The purpose of this study is to see how an educational nursing intervention affected compression therapy adherence and recurrence of venous leg ulcers in patients with chronic venous leg ulcers. A quasi-experimental design was used, including an intervention, a control group, and before and after assessments. This study was conducted in one of Egypt's largest teaching hospitals associated with Menoufia University. The 20-month study included 80 adult patients with healed venous leg ulcers. Each participant was randomized to either a control (got regular leg ulcer information) or study (received educational interventions) group. The following tools were used in the study: bio-sociodemographic variables, knowledge evaluation, compression therapy adherence scale, and recurrence follow-up, after 3, 6, and 12 months of implementation. Furthermore, there is a statistically significant difference between the study groups during the pretest (r = 0.885, 0.774, and 0.477, p = 0.002). The use of nursing education increased patients' understanding and adherence to compression treatment substantially. As a consequence, those with chronic venous leg ulcers may be able to avoid recurrent venous leg ulcers.
Keywords: Educational nursing intervention, Venous leg ulcer, Compression therapy, Adherence, Recurrence
Introduction
Venous leg ulcer (VLU) affects approximately 0.9% of the global population [1, 2]. A chronic leg ulcer affects approximately 1.0–1.3% of the adult population, and it affects approximately 75% of all people with leg ulcers. The prevalence of chronic leg ulcers ranges between 60% and 70% [3]. Compression treatment is a critical component of recurrence prevention and management. To avoid ulcers, it must be preserved for the rest of one's life [4, 5]. A VLU recurrence is described as a lesion that has reached 100% epithelialization, has relapsed along the same leg as the previously treated VLU, and has been recognized by the treating clinician as mainly venous in origin [6].
Nelson et al. [7] and White-Chu et al. [8] found that without maintenance compression therapy, ulcer recurrence can reach 67%, whereas adherence to compression therapy reduces the reported recurrence rate. However, among VLU patients, the predicted percentage of adherence to compression treatment is poor. According to Heyer et al. [9], compression treatment was used on only 40.6% of VLU patients. Nonadherence can be brought on by a number of causes, including discomfort and pain associated with compression therapy, difficulties applying and removing it, or conflicting instructions from healthcare professionals, and, most commonly, a failure to grasp the basic causes of VLU or recognize the need for self-care activities like resting as well as walking [1]. According to the literature, a lack of patient education and treatment, as well as varied approaches to variables impacting compression therapy adherence, is commonly a cause of the development of a first VLU or recurrence [10, 11]. Stewart et al. [12] emphasized the necessity to explain patients VLU pathophysiology and highlighted the fact that it is a chronic condition rather than a simple wound. As a result, VLU patients must engage in preventive behavior and view the condition in a different way, as well as knowledge gaps and patient education must be addressed in order to increase adherence and prevent the recurrence of VLU. Brown [3] stated that nurses are the best people to give this information in this setting.
Several studies show that nurses have created a variety of personalized educational treatments [13, 14, 15, 16, 17]. However, several systematic reviews indicate a scarcity of high-quality randomized controlled trials (RCTs) examining the effect of various therapies on compression stocking adherence [18, 19].
Training modules can be provided in a variety of ways, such as spoken and written patient information booklets, brochures, multimedia formats, computer-aided formats, and others [20]. A nurse who is involved in delivering educational intervention should be responsible for ensuring patients' comprehension and best, sufficient, delivered information, in an appropriate format, with the patient's preferred learning style to help improve patients' knowledge and adherence to compression therapy [21].
Furthermore, Protz et al. [22] recommended that written educational information, such as pamphlets, be provided in the educational context to allow patients to ask questions and provide opportunities for nurses to reply. As a result, according to Clarke et al. [23], the bulk of the information was delivered verbally, with some utilizing written material and others producing images to illustrate what was happening within the leg. When giving the education, the degree and tactics used were considered to change based on the nurse's experience and expertise.
Adherence to therapy is still a problem with chronic illnesses. VLU is the most common chronic form of lower limb extremity ulceration that affects older adults for the rest of their lives. The disease's underlying chronicity poses a clinical difficulty that both health providers and patients find concerning. According to the current study, VLU patients have additional comorbidities, and concomitant knowledge deficiencies and unmet educational requirements increase with age [24]. Furthermore, despite the fact that it is suggested in at least one set of worldwide recommendations on VLU treatment, measuring patient understanding is not routine practice for healthcare practitioners [25, 26]. Nurses play an important role in influencing patient adherence to treatment by giving required instructions that enhance patient knowledge of the nature of chronic diseases and ongoing disease monitoring. As a result, educational nursing intervention is being sought to improve adherence to compression treatment and avoid the recurrence of VLU. As a result, the purpose of this study was to determine the effect of educational nursing interventions on compression therapy adherence and the recurrence of VLU in patients with chronic venous leg ulcers (CVLUs).
Methodology and Assumptions
Assumptions
Three assumptions were developed in order to achieve this study's goal:
1. The knowledge test score in the study group that receives educational nursing interventions is considerably higher than that in the control group that receives conventional VLU treatment.
2. The research group that received educational nursing interventions had significantly higher compression treatment adherence than the control group that received conventional VLU care.
3. The research group that received educational nursing interventions had a significantly lower recurrence rate of VLUs than the control group that received conventional VLU treatment.
Design of the Research
To achieve the study's goal, a quasi-experimental design comprising intervention, control group, and before and after assessments were used. Figure 1 shows the schematic diagram of the methodology steps in the current study.
Fig. 1.

Schematic diagram of the methodology steps.
Configuration, Participation, and Sample Size
This study was carried out in the vascular surgery clinic of one of Egypt's largest teaching hospitals connected with Menoufia University in the Menoufia Governorate. Purposive sampling was used to choose 80 VLU participants, including men and women. Participants who met the inclusion criteria were asked to take part in the study for 20 months (from the beginning of July 2018 to the end of February 2020). Patients were selected if they were 18 years or older, able to communicate well, oriented, able to follow instructions, and had a previous VLU that had fully cured at the time of collection. Recovery was described as full epithelialization that was maintained for at least 2 weeks [27] and had an ankle-brachial pressure index (ABPI) value of 0.8.
Participants who satisfied any of the following criteria were ineligible:
1. A previous history of congestive heart failure, any type of malignancy, any skin diseases or pruritus, and any arterial insufficiency.
2. Being completely bed-bound.
3. Being unable to mobilize.
4. Those who have mixed-origin ulcers.
5. Being unable to apply their compression stockings independently.
6. Those who have cognitive impairment.
The research sample was determined using the following method based on a pilot study of 10 patients with r = 1 (equal sample size for each group) = 5%, and power at 90%:
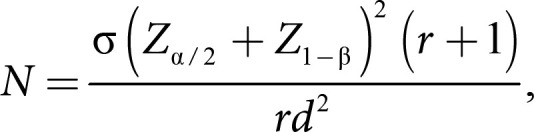
where α and d represent the standard deviation and difference in means of 2 groups, respectively, N = (1 + 1) (1.96 + 0.84)2 (1.2)2/[1 × (1.6 − 1.4)2]. The sample size for each group would thus be 32 for 90% statistical power. The study raised the number of participants to 40 to allow for statistical comparisons between the 2 groups and to boost the study's power. An additional 10–20% of participants were necessary to account for withdrawals, incomplete data, and individuals lost to follow-up [28]. After determining the needed sample size, patients were allocated to one of two groups at random, control (got routine leg ulcer information) or study (received educational treatments), each with 40 patients to maintain a tight balance of group sizes [29]. This approach was employed to guarantee that each patient had an equal chance of being allocated to one of the two groups, as well as to keep the groups impartial.
Procedures
Measures for Intervention
Following a study of the related literature, the researchers created an educational nursing intervention. The educational intervention included a brochure and a pictorial board that covered relevant parts of illness expansion and progression, as well as an overview of preventive strategies needed to facilitate treatment adherence and reduce recurrences, such as topical care, handling, cleaning, and the importance of compression stockings in the management and prevention of recurrence, leg elevation, and pinning. To ensure uniformity in the administration of the intervention, all instructional sessions were delivered by one of the researchers. The educational intervention sessions were carried out by the researcher by interviewing each member of the study group individually in the vascular surgery clinic's waiting room for 45 min. Discussion, demonstration, and explanation were provided using colorful developed pictures on a pictorial board to increase participant understanding of the problem and compression therapy. A color written brochure was created with the outcome criteria in mind; it includes information regarding venous ulcer development, compression stockings, how to work, fitting, and practical skills for its use to complement the researcher's explanation of instructions.
Outcome measures included the following:
1. Total knowledge level scores for the pretest, participants in the study and control groups (baseline), 1 month after intervention, and at 3, 6, and 12 months of follow-up.
2. Adherence to compression therapy scores for the pretest, participants in the study and control groups (baseline), 1 month after intervention, and at 3, 6, and 12 months of follow-up.
3. The emergence of a new ulcer at the same location was operationally characterized as an ulcer recurrence.
Allocation Procedures
Over a 20-month period, the Vascular Surgery Clinic was used for this study for 2 days each week (Tuesday and Thursday) from 9:00 a.m. to 2:00 p.m. The researchers had to pull a lot of strings to figure out which day would be for the study group and which would be for the control group.
Every day, participant lists were verified for participation in the study or control group. Throughout the study period, the researchers evaluated potential individuals on a daily basis as shown in Figure 2.
Fig. 2.

Flowchart of the current study.
Research Instrument
To accomplish the aim of the current study, four instruments were used as given in the following.
Instrument I: Bio-Sociodemographic Characteristics
A systematic interviewing questionnaire was used. It was created by the researchers after they reviewed the relevant literature. It had the following components:
1. Sociodemographic data: used to collect data related to sociodemographic characteristics like the patient's age, gender, employment, and so on.
2. Medical data: included medical data such as smoking status, BMI, prior surgeries, other concomitant illnesses, and so on.
3. Assessment of leg and vascular-related factors: included data such as CEAP classification of VLU, current use of compression therapy, and related data.
Instrument II: Knowledge Assessment Sheet
A systematic interviewing questionnaire was used. It was created by the researchers after they reviewed the relevant literature. It was utilized in the study to assess participants' knowledge of venous ulcers and their management, including pathophysiology, causes or dangers, necessity of compression therapy, handling, cleanliness, its utility in prevention, and reasons to seek care between visits. It consisted of twenty items, seventeen out of them were scored, and each scored from one to three. A score one was given if the answer was poor. A score two was given if the answer was fair and three if the answer was denoted as good, and then all scores were summed. The total score ranged from poor (<50%) (20–41), fair (50%–75%) (42–52), to good (>75%) (53–63), and the patients were categorized into three groups based on their scores. Three items out of twenty were scored, and each scored from one to four. The internal consistency (Cronbach α coefficient) of the knowledge assessment tool was 0.811 in the current study.
Instrument III: Compression Therapy Adherence Scale
It was developed by academics based on a study of the relevant literature and is used to measure patients' adherence to the prescribed compression treatment. It consisted of seven questions concerning adherence to the prescribed compression therapy, such as how often you wore stockings (hours/day), how you wore stockings, and so on. Each scale's item was assigned a score ranging from one to four. If the response indicated low adherence, a score of one was assigned. A score of two was assigned if the response indicated moderate adherence, a score of three if the answer indicated strong adherence, and a score of four if the answer indicated full adherence. All scores were then added together. The overall score ranged from low (25%) (8–15), moderate (25%–50%) (16–23), to good (50%–75%) (24–31) to full (>75%) (32). Based on their ratings, the patients were divided into four groups. In this study, the internal consistency (Cronbach coefficient) of the adherence scale tool was 0.825.
Instrument IV: Recurrence Follow-Up Data Sheet
The recurrent follow-up datasheet utilized in this study was created and updated by Finlayson et al. [6]. It consisted of 4 questions, with no and yes receiving scores of 0 and 1, respectively. After 12 months of educational treatments, it was evaluated using a personalized interview questionnaire. The internal consistency of the recurrence follow-up tool in the prior study was 0.73, whereas it was 0.825 in the current study.
General Procedures
This study was carried out according to the procedures defined below. After receiving official approval from the hospital's director and the head nurses of the outpatient clinics after explaining the purpose of the current study, the researcher began data collection with a preparatory phase in which all eligible patients attending the vascular surgery outpatient clinic during the defined period and treatment routine were asked to participate in the present study after describing the purpose of the investigation; all participants who agreed to participate in the study and met the inclusion criteria signed a written permission form.
Following that, all patients who met the inclusion criteria and agreed to participate were split into two groups: the research group and the control group. The researcher questioned each participant individually in the waiting room of the vascular surgery outpatient clinic. Instruments I, II, and III were used to gather sociodemographic information, medical data, knowledge evaluation, and adherence level. The interview lasted between 30 and 45 min. During this session, each research group participant's specific educational requirements were identified.
Following the pretest as a baseline, the researcher displayed and explained venous ulcer pathophysiology, causes, dangers, and nature of the illness in a personalized session with each participant in the study group using colorful visual graphical representations within the leg. The researcher also discussed compression stocking fitting and application, handling, cleaning, and usage in the management and prevention of venous ulcer recurrence, as well as the necessity of follow-up. Following the first session, the researcher gave a colorful printed pamphlet to each participant in the study group. The researcher reinforced the information every 3 months, and at the conclusion of the session, the researcher showed all supplied knowledge before revising and reinforcing it based on the needs of the participants. In addition, the researcher rectified incorrect performance and answered questions. The control group, on the other hand, got traditional treatment from outpatient clinic nurses and medical personnel. Following that, the patients were followed up through the assessment phase, during which all study participants from both the study and control groups were assessed five times over the course of the study.
The first time was a pretest as a baseline using instruments I, II, and III, respectively; the second time was 1 month after the first session using instruments II and III, respectively; the third time was after 3 months using instruments II and III, respectively; the fourth time was after 6 months using instruments II and III, respectively; and the fifth and final evaluation was after 12 months from the administration. A comparison of the study and control groups was performed to assess the influence of nursing educational interventions on patient understanding, compression treatment adherence, and the recurrence rate of leg ulcers among CVLU patients.
Ethical Consideration and Data Examination
The Ethics Committee of Menoufia University's Faculty of Nursing authorized this study (Approval No. 797). After describing the purpose of the investigation, all participants provided written agreement to participate in the study, and they were guaranteed that all gathered data would be kept strictly secret and used solely for the purpose of the study. Participation in the study was totally optional and anonymous, according to the researchers. Participants were also advised that refusing to participate in the study would not have any impact on their care and, as a result, their health.
The gathered data were organized, tabulated, and statistically analyzed using SPSS software (Statistical Package for the Social Sciences, version 19; SPSS Inc., Chicago, IL, USA). The quantitative data's range, mean, and standard deviation were calculated. The χ2 (2) test was used to compare two groups and more for qualitative data, which defines a categorical collection of data by the frequency, percentage, or proportion of each category.
To compare the means of two sets of parametric data from independent samples, the Student's t test was employed. The Mann-Whitney test's Z value was used to compare the means of two sets of nonparametric data from independent samples. To compare more than two means of parametric data, the F value of the ANOVA test was determined. To compare proportions and percent of change, proportion testing was employed (Z test). To evaluate the link between variables, Pearson's correlation coefficient was employed (r). The significance level for interpreting the results of tests of significance was fixed at p 0.05 [30].
Pilot Study
Prior to the commencement of the main research data collection, a pilot study on 10 patients was conducted to assess recruitment feasibility and tool use and estimate the required sample size. Because there was no variation in the recruitment method, participants who took part in the pilot study were included in the main study sample. The results of the pilot study proved that the investigation was viable.
Results
Description of the Study's Patient Sample
Concerning the characteristics of the entire studied sample (n = 80), the age ranged from 40 to 57 years, males were a high percentage of participants (61.3%), single (92.5%), educated (70.1), employed, and working (75.1%), BMI ranged from 22.10 to 30.50, wore compression stockings below the knee, and had diabetes (52.5%). At baseline, there was no significant difference between the study and control groups in terms of all sociodemographic and medical parameters (p value >0.05), as shown in Table 1.
Table 1.
Sociodemographic and medical characteristics of the studied patients with CVLU
| Variables | The studied patients with CVLU (n = 80) |
χ2 p value | ||||||
|---|---|---|---|---|---|---|---|---|
| Study group (n = 40) |
Control group (n = 40) |
Total (n = 80) |
||||||
| n | % | n | % | n | % | |||
| Sex | ||||||||
| Male | 26 | 65.0 | 23 | 57.5 | 49 | 61.3 | 0.474 | |
| Female | 14 | 35.0 | 17 | 42.5 | 31 | 38.8 | 0.491 | |
| Age, years | ||||||||
| Range | 40–57 | 40–57 | 40–57 | |||||
| Mean ± SD | 47.65±3.61 | 48.85±4.31 | 48.25±3.99 | |||||
| t test | 1.350 | |||||||
| p value | 0.181 | |||||||
| Marital status | ||||||||
| Single | 36 | 90.0 | 38 | 95.0 | 74 | 92.5 | 0.721 | |
| Widowed | 4 | 10.0 | 2 | 5.0 | 6 | 7.5 | 0.396 | |
| Occupation | ||||||||
| Worker | 16 | 40.0 | 13 | 32.5 | 29 | 36.3 | ||
| Employee | 14 | 35.0 | 17 | 42.5 | 31 | 38.8 | 1.653 | |
| Not working | 9 | 22.5 | 10 | 25.0 | 19 | 23.8 | 0.647 | |
| Retired | 1 | 2.5 | 0 | 0 | 1 | 1.3 | ||
| Educational level | ||||||||
| Illiterate | 12 | 30.0 | 12 | 30.0 | 24 | 30.0 | ||
| Primary | 14 | 35.0 | 11 | 27.5 | 25 | 31.3 | 2.78 | |
| Secondary | 7 | 17.5 | 13 | 32.5 | 20 | 25.0 | 0.395 | |
| High education | 7 | 17.5 | 4 | 10.0 | 11 | 13.8 | ||
| BMI | ||||||||
| Range | 22.10–30.30 | 22.10–30.50 | 22.10–30.50 | |||||
| Mean±SD | 24.92±1.98 | 25.06±2.08 | 24.99±2.02 | |||||
| t test | 0.295 | |||||||
| p value | 0.769 | |||||||
| Presence of comorbidities | ||||||||
| Diabetes | 24 | 60.0 | 18 | 45.0 | 42 | 52.5 | 2.590 | |
| Hypertension | 14 | 35.0 | 21 | 52.5 | 35 | 43.8 | 0.274 | |
| DVT | 2 | 5.0 | 1 | 2.5 | 3 | 3.8 | ||
| Type of compression | ||||||||
| Stocking | 38 | 95.0 | 35 | 87.5 | 73 | 91.3 | 1.409 | |
| Bandage | 2 | 5.0 | 5 | 12.5 | 7 | 8.8 | 0.235 | |
| Compression level | ||||||||
| Thigh | 0 | 0 | 3 | 7.5 | 3 | 3.8 | 3.117 | |
| Below the knee | 40 | 100 | 37 | 92.5 | 77 | 96.3 | 0.077 | |
Comparison between the Study Findings and Control Groups before and after Intervention
Table 2 shows that virtually all of the individuals in the study and control groups had inadequate knowledge levels before the pretest and after 1 month (95%, 97.5%, 100%, and 100%, respectively). Furthermore, there was no statistically significant difference between the two groups at the pretest level of knowledge and after 1 month (p value >0.05). At 3, 6, and 12 months, there was a substantial difference between the two groups (p value 0.05). Furthermore, a substantial change in the mean value of overall knowledge scores was detected among the study group after 12 months compared to the pretest. However, the control group's mean value changed only a little. As a consequence, in terms of general knowledge scores 12 months after the pretest, there was a substantial difference between the study and control groups (p value 0.05).
Table 2.
Comparison of level of total knowledge scores between study and control groups before and after intervention during follow-up (n = 80)
| Total knowledge level at different times of assessment | Total knowledge level among the studied patients with chronic venous leg ulcer (n = 80) |
χ2 | p value | |||
|---|---|---|---|---|---|---|
| study group (n = 40) |
control group (n = 40) |
|||||
| n | % | n | % | |||
| Pretest | ||||||
| Poor (20–41) | 38 | 95.0 | 40 | 100 | ||
| Fair (42–52) | 1 | 2.5 | 0 | 0 | 2.051 | 0.359 |
| Good (53–63) | 1 | 2.5 | 0 | 0 | ||
| After 1 month | ||||||
| Poor | 39 | 97.5 | 40 | 100 | ||
| Fair | 1 | 2.5 | 0 | 0 | 1.013 | 0.314 |
| Good | 0 | 0 | 0 | 0 | ||
| After 3 months | ||||||
| Poor | 31 | 77.5 | 40 | 100 | ||
| Fair | 8 | 20.0 | 0 | 0 | 10.141 | 0.006* |
| Good | 1 | 2.5 | 0 | 0 | ||
| After 6 months | ||||||
| Poor | 1 | 2.5 | 40 | 100 | ||
| Fair | 36 | 90.0 | 0 | 0 | 76.098 | 0.0001 * |
| Good | 3 | 7.5 | 0 | 0 | ||
| After 12 months | ||||||
| Poor | 0 | 0 | 40 | 100 | ||
| Fair | 32 | 80.0 | 0 | 0 | 80.000 | 0.0001 * |
| Good | 8 | 20.0 | 0 | 0 | ||
| χ2 = 179.567 | χ2 = − | |||||
| p value = 0.0001* | p value = − | |||||
|
| ||||||
| Change of total knowledge scores after 12 months vs. pretest | −3.00: 36.00 29.58±8.50 |
2.00: 18.00 10.45±3.45 |
Z test 6.540 |
0.0001 * | ||
Statistically significant.
Adherence Scores between Study and Control Groups before and after the Test during Follow-Up
Table 3 shows that there was no significant difference between the study and control groups in terms of adherence during the pretest (p value > 0.05). However, there was a significant difference between the study and control groups after 1, 3, 6, and 12 months (p value 0.05). Over 12 months, there was a substantial shift in the mean value of overall adherence ratings to compression therapy among the study group compared to the pretest. However, the control group had a poor adherence score. As a result, there was a significant difference between the study and control groups in terms of overall adherence scores 12 months after the pretest (p value 0.05).
Table 3.
Comparison of adherence scores between study and control groups before and after test during follow-up (n = 80)
| Total adherence level at different times of assessment | Total adherence level among the studied patients with CVLU (n = 80) |
χ2 | p value | |||
|---|---|---|---|---|---|---|
| study group (n = 40) |
control group (n = 40) |
|||||
| n | % | n | % | |||
| Pretest | ||||||
| Low adherence | 1 | 2.5 | 0 | 0 | ||
| Moderate adherence | 36 | 90.0 | 40 | 100 | 4.211 | 0.122 |
| Good adherence | 3 | 7.5 | 0 | 0 | ||
| After 1 month | ||||||
| Low adherence | 0 | 0 | 24 | 60.0 | ||
| Moderate adherence | 30 | 75.0 | 15 | 37.5 | 36.364 | 0.000* |
| Good adherence | 10 | 25.0 | 1 | 2.5 | ||
| After 3 months | ||||||
| Moderate adherence | 10 | 25.0 | 38 | 95.0 | 40.833 | 0.0001 * |
| Good adherence | 30 | 75.0 | 2 | 5.0 | ||
| After 6 months | ||||||
| Moderate adherence | 1 | 2.5 | 28 | 70.0 | ||
| Good adherence | 21 | 52.5 | 12 | 30.0 | 45.592 | 0.0001 * |
| Full adherence | 18 | 45.0 | 0 | 0 | ||
| After 12 months | ||||||
| Moderate adherence | 0 | 0 | 27 | 67.5 | ||
| Good adherence | 16 | 40.0 | 13 | 32.5 | 51.310 | 0.0001 * |
| Full adherence | 24 | 60.0 | 0 | 0 | ||
|
| ||||||
| χ2 = 167.924 | χ2 = 138.40 | |||||
| p value = 0.0001 * | p value = 0.0001* | |||||
|
| ||||||
| Change of total adherence scores | 1: 16 | −1: 10 | Z test | 0.0001* | ||
| after 12 months vs. pretest | 11.60±3.41 | 4.80±2.63 | 6.629 | |||
Total adherence levels: low (<25%) (8–15), moderate (25%–50%) (16–23), good adherence (50%–75%) (24–31), and full adherence (>75%) (≥32).
Statistically significant.
Table 4 shows that there was a good relationship between total knowledge scores and adherence in individuals suffering from CVLUs in the study group, with a high significant statistical difference between the study groups during pretest and after 1 and 3 months (r = 0.885 at p = 0.0001, r = 0.774 at p = 0.0001, and r = 0.477 at p = 0.002). Figure 3 shows the assessment of the correlation coefficient of adherence scores at different times.
Table 4.
Correlation between total scores of knowledge and adherence of the study group patients with CVLU before and after intervention (n = 80)
| Total adherence scores at different times of assessment | Correlation of total scores among the study group patients with CVLU (n = 80) |
|
|---|---|---|
| total knowledge scores of the study group (n = 40) |
||
| r | p value | |
| Pretest | 0.885 | 0.0001* |
| After 1 month | 0.774 | 0.0001* |
| After 3 months | 0.477 | 0.002* |
| After 6 months | 0.296 | 0.063 |
| After 12 months | 0.290 | 0.069 |
Study group = patients attended educational intervention on compression therapy adherence. Control group = patients did not attend educational intervention on compression therapy adherence. r = correlation coefficient.
Statistically significant.
Fig. 3.

Assessment of the correlation coefficient of adherence scores at different times.
Recurrence of Leg Ulcers in the Research and Control Groups after 12 Months of Educational Interventions
Figure 4 demonstrates that in terms of recurrence of leg ulcers, the occurrence of a new ulcer in the same leg as the previous ulcer was 5.0% and 15.0% in the study and control groups, respectively. Furthermore, the frequency of a new ulcer at the same place as the previous ulcer was 2.5% and 12.5% in the study and control groups, respectively.
Fig. 4.

Comparison of leg ulcer recurrence between study and control groups after 12 months of educational interventions (n = 80).
Discussion
The majority of the respondents in this study varied in age from 40 to 57 years, with a mean of 48.253.99, and male was the dominating gender. This conclusion is similar to the findings of Mahmoud et al. [31], who discovered that the majority of their investigated patients were men between the ages of 40 and 60. Also, Žulec et al. [32] and Kirsner et al. [33] found that VLU occurred among the elderly and verified that the majority of their cases were men.
This was in contrast to previous findings by Kreft et al. [34] and Jeanmonod et al. [35] who reported that the majority of their sample was composed of elderly females. The comparison of the study and control groups' sociodemographic characteristics indicated no significant differences at baseline that might have influenced the findings; this implies that the two study groups were homogeneous. This finding demonstrated that the patient characteristics of both groups were comparable to those in prior studies that assessed educational intervention in VLU patients [36].
Furthermore, the study's findings revealed that there were no statistical differences in terms of medical features between the two groups, with the majority of them wearing compression stockings below the knee. Cataldo et al. [37] conducted prior research in which they examined the medical reasons for and the usage of elastic compression stockings to measure patient adherence to therapy. Similarly, the majority of patients were found to be wearing compression stockings. This could be explained by the fact that in the current study, compression stockings were the most readily available and cost-effective type of compression treatment. This finding is consistent with the findings of Nelson et al. [38], who found that participants may choose the type of compression based on clinical preferences, cost, and compliance.
In terms of knowledge, the present study found that virtually all of both groups had a low level of understanding at the start. However, there was a significant statistical difference between them at 3, 6, and 12 months after the educational intervention was delivered, with a decent degree of knowledge within the research group. This finding is consistent with the findings of Mahmoud et al. [31], who stated that the majority of the studied subjects had a satisfactory level of knowledge following nursing instructions, with a highly statistically significant difference between the study and the control group in terms of patient knowledge. Gonzalez [39] observed that while evaluating the impact of a patient education intervention on knowledge and venous ulcer recurrence, the patient's knowledge levels during assessment were greater than those at baseline. One probable explanation is that the researcher presented information using a graphical board, which has been rigorously shown by Clarke-Moloney et al. [40] to enhance VLU information delivery with the exclusion of individuals with cognitive impairment. Another possible explanation is that the researcher reinforces information every 3 months and distributes brochures, as investigated by Protz et al. [22] for improving VLU patient understanding. This was emphasized throughout the approach, and the researcher only showed these procedures to the study group. This discovery backed up the original research idea.
In terms of adherence, the findings of this study show that there was a significant increase in total adherence scores to compression therapy in both groups over 12 months compared to the pretest, with highly statistical differences between study and control groups at 1, 3, 6, and 12 months after intervention. In line with the current findings, Heinen et al. [14] discovered that there was an increase in adherence in both groups after 18 months of developing and evaluating a counseling program aimed at improving adherence to compression therapy and physical activity for patients with VLUs (from 27% to 45% in the intervention group and from 37% to 46% in the control group).
One of the most plausible explanations for this is that the baseline profile of both groups in the current research was homogeneous. These findings are consistent with those of Edwards et al. [41], who discovered that only 27% of VLU patients utilize compression stockings and related this to the patients' lack of awareness. These data provide credence to the second study hypothesis.
The current study discovered a positive relationship between total knowledge scores and study group adherence, with a highly significant statistical difference between study samples during the pretest and 1 and 3 months later (r = 0.885 at p = 0.0001, r = 0.774 at p = 0.0001, and r = 0.477 at p = 0.002). This conclusion is consistent with findings in the literature by Moffatt et al. [42] that showed nonadherence to treatment is related to the patient's lack of awareness and comprehension of his or her illness and the function of compression therapy treatment.
In terms of leg ulcer recurrence, the current study found that at 12 months after the educational intervention, the ulcer recurrence rate in the study group was lower than that in the control group. This finding is consistent with the findings of the Health Quality Ontario Series (2019), which discovered that in one RCT, people assigned to the compression stocking group had a significantly lower recurrence rate at 12 months than people assigned to the control group (risk ratio 0.43, 95% CI: 0.27–0.69; p = 0.001). Similar to prior findings, O'Brien et al. [43] showed in an RCT that by teaching the patient, the recurrence rate was decreased from 36% to 4% within 1 year (log rank test = 8.28, p = 0.004). In contrast to previous findings, Finlayson et al. [44] found that almost half of the patients (44%) suffered an ulcer recurrence within a year of healing. This finding might be explained by participants in the research group becoming more aware of condition development and advancement in terms of educational intervention. These data provide credence to the third theory.
The current investigation demonstrates that adherence to compression treatment is related to a lower risk of recurrence of leg ulcers. These findings appear to be consistent with previous research [45, 46], which discovered that patients exposed to a structured concordance program delivered by nurses were nine times less likely to develop a leg ulcer within a year than patients who received usual care. In line with the current study's findings, Clarke-Moloney et al. [40] reported in their study comparing compression stockings for ulcer recurrence and patient compliance that the recurrence rate was 16% at 1 year with 89% reported adherence and nonadherence associated with a higher risk of recurrence (p 0.0001), with the lowest recurrence seen in the highest compliancy. Furthermore, these findings are consistent with those of previous research. One RCT by Ontario [47] discovered, for example, that the risk of recurrence was six times higher in those who did not wear compression stockings than in those who did. Furthermore, a single-arm cohort study discovered that the recurrence rate was much higher in those who did not wear or wore compression stockings (79%) compared to those who did (40%).
Nursing Implications
The study's findings have consequences for doctors and nursing research. Every vascular surgery clinic should have dedicated nurse-led teaching and follow-up services. A professional nurse is required for VLU patients to participate in intervention. Education on leg ulcers should be included into nursing practice, raising nurses' understanding of the nature of leg ulcers as a chronic illness and the skills needed for preventative treatment methods. It will also be useful to raise awareness of VLUs as a chronic illness and establish services that offer patients adequate follow-up during ulcer-free times. In addition, family and caregivers should be involved in the patient's instructional session. More focus should be made in future studies on patients' self-efficacy and quality of life. Further research should look into different intervention techniques for preventing VLU recurrence and overcoming nonadherence to therapy. This study needs to be repeated with a bigger sample from diverse settings in numerous clinics in order to generalize the findings.
Conclusion
The current study revealed that patients with CVLU had a lack of understanding of their illness as a result of their treatment. The findings of this study demonstrated the need for educational nurse intervention for patients with CVLUs, as well as the relevance of patient education in terms of adherence to compression therapy. Using compression stockings and wearing them regularly in patients who have healed VLUs may help to reduce their risk for recurrence. Finally, the outcomes of the study lend support to the three research hypotheses that were tested.
Statement of Ethics
This study was approved by the Ethical Committee for Scientific Research Review No. 797 (24/6/ 2018)/Menoufia University Faculty of Nursing. Also, individuals have given their written informed consent to participate in this study.
Conflict of Interest Statement
We have no conflicts of interest to disclose.
Funding Sources
No external funding was received.
Author Contributions
Amoura Soliman Behairy conceived and designed the analysis, collected the data, performed the analysis, and wrote the paper. Samah E. Masry collected the data and performed the analysis.
Data Availability Statement
All data generated or analyzed during this study are included in the article. Further enquiries can be directed to the corresponding author.
Acknowledgments
The authors thank the patients for their participation in the study.
References
- 1.Bobbink P, Larkin PJ, Probst S. Experiences of venous leg ulcer persons following an individualised nurse-led education: protocol for a qualitative study using a constructivist grounded theory approach. BMJ Open. 2020;10((11)):e042605. doi: 10.1136/bmjopen-2020-042605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nussbaum SR, Carter MJ, Fife CE, DaVanzo J, Haught R, Nusgart M, et al. An economic evaluation of the impact, cost, and medicare policy implications of chronic nonhealing wounds. Value Health. 2018;21((1)):27–32. doi: 10.1016/j.jval.2017.07.007. [DOI] [PubMed] [Google Scholar]
- 3.Brown A. Recurrent venous leg ulcers: management in general practice. Practice Nursing. 2021;32((6)):220–5. [Google Scholar]
- 4.Finlayson K, Edwards H, Parker C. Preventing recurrence of venous leg ulcers in older adults: a longitudinal, randomised trial. Innov Aging. 2017;1((Suppl 1)):969. [Google Scholar]
- 5.Milic DJ, Zivic SS, Bogdanovic DC, Golubovic MD, Lazarevic MV, Lazarevic KK. A randomized trial of class 2 and class 3 elastic compression in the prevention of recurrence of venous ulceration. J Vasc Surg Venous Lymphat Disord. 2018;6((6)):717–23. doi: 10.1016/j.jvsv.2018.06.009. [DOI] [PubMed] [Google Scholar]
- 6.Finlayson KJ, Parker CN, Miller C, Gibb M, Kapp S, Ogrin R, et al. Predicting the likelihood of venous leg ulcer recurrence: the diagnostic accuracy of a newly developed risk assessment tool. Int Wound J. 2018;15((5)):686–94. doi: 10.1111/iwj.12911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nelson EA, Bell-Syer SE. Compression for preventing recurrence of venous ulcers. Coch Database Sys Rev. 2014;((9)):CD002303. doi: 10.1002/14651858.CD002303.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.White-Chu EF, Conner-Kerr TA. Overview of guidelines for the prevention and treatment of venous leg ulcers: a US perspective. J Multidiscip Healthc. 2014;7:111. doi: 10.2147/JMDH.S38616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Heyer K, Protz K, Augustin M. Compression therapy − cross-sectional observational survey about knowledge and practical treatment of specialised and non-specialised nurses and therapists. Int Wound J. 2017;14((6)):1148–53. doi: 10.1111/iwj.12773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Meulendijks AM, Welbie M, Tjin EPM, Schoonhoven L, Neumann HAM. A qualitative study on the patient's narrative in the progression of chronic venous disease into a first venous leg ulcer: a series of events. Br J Dermatol. 2020;183((2)):332–9. doi: 10.1111/bjd.18640. [DOI] [PubMed] [Google Scholar]
- 11.Probst S, Séchaud L, Bobbink P, Skinner MB, Weller CD. The lived experience of recurrence prevention in patients with venous leg ulcers: an interpretative phenomenological study. J Tissue Viability. 2020;29((3)):176–9. doi: 10.1016/j.jtv.2020.01.001. [DOI] [PubMed] [Google Scholar]
- 12.Stewart A, Edwards H, Finlayson K. Reflection on the cause and avoidance of recurrent venous leg ulcers: an interpretive descriptive approach. J Clin Nurs. 2018;27((5–6)):e931–9. doi: 10.1111/jocn.13994. [DOI] [PubMed] [Google Scholar]
- 13.Kapp S, Miller C, Sayers V, Donohue L. The leg ulcer prevention program: effectiveness of a multimedia client education package for people with venous leg ulcers. Wound Prac Res J. 2010;18((2)):38. [Google Scholar]
- 14.Heinen M, Borm G, van der Vleuten C, Evers A, Oostendorp R, van Achterberg T. The lively legs self-management programme increased physical activity and reduced wound days in leg ulcer patients: results from a randomized controlled trial. Int J Nurs Stud. 2012;49((2)):151–61. doi: 10.1016/j.ijnurstu.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 15.González A. Education project to improve venous stasis self-management knowledge. J Wound Ost Continen Nurs. 2014;41((6)):556–9. doi: 10.1097/WON.0000000000000088. [DOI] [PubMed] [Google Scholar]
- 16.O'Brien J, Finlayson K, Kerr G, Edwards H. Evaluating the effectiveness of a self‐management exercise intervention on wound healing, functional ability and health‐related quality of life outcomes in adults with venous leg ulcers: a randomised controlled trial. Int Wound J. 2017;14((1)):130–7. doi: 10.1111/iwj.12571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Domingues EAR, Kaizer UAO, Lima MHM. Effectiveness of the strategies of an orientation programme for the lifestyle and wound‐healing process in patients with venous ulcer: a randomised controlled trial. Int Wound J. 2018;15((5)):798–806. doi: 10.1111/iwj.12930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Weller CD, Buchbinder R, Johnston RV. Interventions for helping people adhere to compression treatments for venous leg ulceration. Cochrane Database Syst Rev. 2016;3((3)):CD008378. doi: 10.1002/14651858.CD008378.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Probst S, Allet L, Depeyre J, Colin S, Skinner MB. A targeted interprofessional educational intervention to address therapeutic adherence of venous leg ulcer persons (TIEIVLU): study protocol for a randomized controlled trial. Trials. 2019;20((1)):1–8. doi: 10.1186/s13063-019-3333-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tandler SF. Challenges faced by healthcare professionals in the provision of compression hosiery to enhance compliance in the prevention of venous leg ulceration. EWMA J. 2016;16((1)):56. [Google Scholar]
- 21.Hughes G, Green J. Factors that impact compression hosiery concordance post healing. Int Wound J. 2019;15((5)):386. [Google Scholar]
- 22.Protz K, Dissemond J, Seifert M, Hintner M, Temme B, Verheyen‐Cronau I, et al. Education in people with venous leg ulcers based on a brochure about compression therapy: a quasi‐randomised controlled trial. Int Wound J. 2019;16((6)):1252–62. doi: 10.1111/iwj.13172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Clarke C, Whitmore L, Webb A. Patient education pictorial boards: improving patients' understanding of venous leg ulcer and compression therapy. Wounds UK. 2020;16((2)):e044604. [Google Scholar]
- 24.Taylor JO, Hartzler AL, Osterhage KP, Demiris G, Turner AM. Monitoring for change: the role of family and friends in helping older adults manage personal health information. J Am Med Inform Assoc. 2018;25((8)):989–99. doi: 10.1093/jamia/ocy037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Weller CD, Team V, Probst S, Gethin G, Richards C, Sixsmith J, et al. Health literacy in people with venous leg ulcers: a protocol for scoping review. BMJ open. 2021;11((5)):e044604. doi: 10.1136/bmjopen-2020-044604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gethin G, Probst S, Stryja J, Christiansen N, Price P. Evidence for person-centred care in chronic wound care: a systematic review and recommendations for practice. J Wound Care. 2020;29((Suppl 9b)):S1–S22. doi: 10.12968/jowc.2020.29.Sup9b.S1. [DOI] [PubMed] [Google Scholar]
- 27.Stewart AM. Investigation of predictors of recurrent venous leg ulcers and validation of a recurrence risk assessment tool [Doctoral dissertation] Queensland University of Technology; 2019. [Google Scholar]
- 28.Suresh K, Chandrashekara S. Sample size estimation and power analysis for clinical research studies. J Hum Reprod Sci. 2012;5((1)):7. doi: 10.4103/0974-1208.97779. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 29.Kim J, Shin W. How to do random allocation (randomization) Clin Orthop Surg. 2014;6((1)):103–9. doi: 10.4055/cios.2014.6.1.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dawson B, Trapp RG, Greive A. Basic & clinical biostatistics. New York: Lange Medical Books/McGraw-Hill; 2004. pp. p. 1–438. [Google Scholar]
- 31.Mahmoud SI, El-Sayed ZM, AboDeif HI. Effect of nursing instructions on patient's knowledge and venous leg ulcer healing. 2019. [Google Scholar]
- 32.Žulec M, Rotar-Pavlič D, Puharić Z, Žulec A. “Wounds home alone”: why and how venous leg ulcer patients self-treat their ulcer: a qualitative content study. Int J Env Res Pub Health. 2019;16((4)):559. doi: 10.3390/ijerph16040559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kirsner RS, Vivas AC. Lower‐extremity ulcers: diagnosis and management. Br J Dermatol. 2015;173((2)):379–90. doi: 10.1111/bjd.13953. [DOI] [PubMed] [Google Scholar]
- 34.Kreft D, Keiler J, Grambow E, Kischkel S, Wree A, Doblhammer G. Prevalence and mortality of venous leg diseases of the deep veins: an observational cohort study based on German health claims data. Angiology. 2020;71((5)):452–64. doi: 10.1177/0003319720905751. [DOI] [PubMed] [Google Scholar]
- 35.Jeanmonod DJ, Suzuki K. We are IntechOpen, the world's leading publisher of open access books built by scientists, for scientists TOP 1% control of a proportional hydraulic system. Intech Open. 2018;2:64. [Google Scholar]
- 36.Baquerizo Nole KL, Yim E, Van Driessche F, Lamel SA, Richmond NA, Braun LR, et al. Educational interventions in venous leg ulcer patients. Wound Repair Regen. 2015;23((1)):137–40. doi: 10.1111/wrr.12247. [DOI] [PubMed] [Google Scholar]
- 37.Cataldo JL, de Godoy JM, De Barros N. The use of compression stockings for venous disorders in Brazil. Phlebology. 2012;27((1)):33–7. doi: 10.1258/phleb.2011.010088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nelson EA, Bell-Syer SE. Compression for preventing recurrence of venous ulcers. Coch Database Sys Rev. 2014;((9)):CD002303. doi: 10.1002/14651858.CD002303.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gonzalez A. The effect of a patient education intervention on knowledge and venous ulcer recurrence: results of a prospective intervention and retrospective analysis. Ostomy Wound Manage. 2017;63((6)):16–28. [PubMed] [Google Scholar]
- 40.Clarke‐Moloney M, Keane N, O'Connor V, Ryan MA, Meagher H, Grace PA, et al. Randomised controlled trial comparing European standard class 1 to class 2 compression stockings for ulcer recurrence and patient compliance. Int Wound J. 2014;11((4)):404–8. doi: 10.1111/j.1742-481X.2012.01108.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Edwards LM, Moffatt CJ, Franks PJ. An exploration of patients' understanding of leg ulceration. J Wound Care. 2002;11((1)):35–9. doi: 10.12968/jowc.2002.11.1.26138. [DOI] [PubMed] [Google Scholar]
- 42.Moffatt C, Murray S, Keeley V, Aubeeluck A. Non‐adherence to treatment of chronic wounds: patient versus professional perspectives. Int Wound J. 2017;14((6)):1305–12. doi: 10.1111/iwj.12804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.O'Brien JA, Finlayson KJ, Kerr G, Edwards HE. Testing the effectiveness of a self-efficacy based exercise intervention for adults with venous leg ulcers: protocol of a randomised controlled trial. BMC Dermatol. 2014;14((1)):1–9. doi: 10.1186/1471-5945-14-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Finlayson KJ, Courtney MD, Gibb MA, O'Brien JA, Parker CN, Edwards HE. The effectiveness of a four‐layer compression bandage system in comparison with class 3 compression hosiery on healing and quality of life in patients with venous leg ulcers: a randomised controlled trial. Int Wound J. 2014;11((1)):21–7. doi: 10.1111/j.1742-481X.2012.01033.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Franks PJ, Oldroyd MI, Dickson D, Sharp EJ, Moffatt CJ. Risk factors for leg ulcer recurrence: a randomized trial of two types of compression stocking. Age Ageing. 1995;24((6)):490–4. doi: 10.1093/ageing/24.6.490. [DOI] [PubMed] [Google Scholar]
- 46.Moffatt C, Kommala D, Dourdin N, Choe Y. Venous leg ulcers: patient concordance with compression therapy and its impact on healing and prevention of recurrence. Int Wound J. 2009;6((5)):386–93. doi: 10.1111/j.1742-481X.2009.00634.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Health Quality Ontario Compression stockings for the prevention of venous leg ulcer recurrence: a health technology assessment. Ont Health Technol Assess Ser. 2019;19((2)):1. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are included in the article. Further enquiries can be directed to the corresponding author.