

Abstract
BACKGROUND:
Family income is known to affect child health, but this relationship can be bidirectional. We sought to characterize this relationship by quantifying forgone family employment (FFE) due to a child’s health condition in families of children with special health care needs (CSHCN) with updated figures.
METHODS:
We conducted a secondary data analysis from the 2016–2017 National Survey of Children’s Health. CSHCN with previously employed caregivers were included (N = 14 050). FFE was defined as any family member having stopped work and/or reduced hours because of their child’s health or health condition. Child, caregiver, and household characteristics were compared by FFE status. Logistic regression analysis was conducted to evaluate the association between hours of medical care provide by a family member and FFE. US Bureau of Labor Statistics reports were used to estimate lost earnings from FFE.
RESULTS:
FFE occurred in 14.5% (95% confidence interval [CI] 12.9%–16.1%) of previously employed families with CSHCN and was 40.9% (95% CI 27.1%–54.7%) for children with an intellectual disability. We observed disproportionately high FFE among CSHCN who were 0 to 5 years old and of Hispanic ethnicity. We found a strong association between FFE and increasing hours of family-provided medical care, with an adjusted odds ratio (aOR) of 1.72 (95% CI 1.25–2.36) for <1 hour per week (compared with 0 hours), an aOR of 5.96 (95% CI 4.30–8.27) for 1 to 4 hours per week, an aOR of 11.89 (95% CI 6.19–22.81) for 5 to 10 hours per week, and an aOR of 8.89 (95% CI 5.26–15.01) for >10 hours per week. Lost earnings for each household with FFE were estimated at ~$18000 per year.
CONCLUSIONS:
With our findings, we highlight the need to implement programs and policies that address forgone income experienced by families of CSHCN.
The role that social influencers of health, such as family income, play in influencing child health is increasingly recognized.1,2 For example, financial hardships, such as low income or parental incarceration, have been shown to exacerbate a child’s unmet health care needs3 and health outcomes.4–7 However, the relationship between social factors and child health is thought to be bidirectional, whereby children’s health affects their surrounding environments.8,9 Previous research has revealed that the presence of a health condition increases the likelihood of a family caregiver experiencing emotional and financial stressors and having a child with poor health status is associated with reduced family employment and overall financial hardship.9–17
Children with special health care needs (CSHCN), defined as those who have “one or more chronic physical, developmental, behavioral, or emotional conditions and who also require health and related services of a type or amount beyond that required by children generally,”18 are a group of children whose health needs have been shown to negatively impact family finances.9 How health care providers, health care system leaders, policy makers, and payers conceptualize and quantify the relationship between children’s health and their families’ circumstances continues to influence how related programs and policies are developed and even funded. As such, the impact of families having CSHCN must be continually understood and quantified, if we are to build effective interventions to address child health care needs and that of their families.
The National Survey of Children’s Health (NSCH) offers an opportunity to study the connection between CSHCN and their families’ ability to work outside of home. In this study, we examined whether there were child and household characteristics associated with forgone family employment (FFE). We also investigated the association between hours of medical care provided by a family member and FFE as well as the association between FFE and the use of government programs (eg, cash assistance, Special Supplemental Nutrition Program for Women, Infants, and Children [WIC], etc). Lastly, we quantified the loss of earnings associated with FFE due to a child’s health to better describe the impact of child health on the family economy.
METHODS
Data Source
The NSCH is a nationally representative survey funded and directed by the Maternal and Child Health Bureau.19 It is the largest national and state-level survey on the health and health care needs of children and their families. Specifically, the NSCH includes noninstitutionalized children 0 to 17 years old living across all 50 states and the District of Columbia. The survey is administered online and by mail to randomly selected households in the United States.20 The NSCH topics include child physical and mental health as well as factors related to child wellbeing, including family interactions, health care access, and community information.
Study Design and Sample
We combined NSCH data from 2016 and 2017 to ensure adequate sample size (N = 71 811). We narrowed the study population to include only CSHCN on the basis of screening questions (n = 16 304). We removed 385 children (0.2%) who had missing data for questions related to caregiver employment. To describe families of children who experienced FFE, we excluded 1869 children (11%) who did not have at least 1 caregiver who was employed, defined by the NSCH as employment in 50 of the last 52 weeks, for a final primary analytic sample of 14 050. We also conducted a supplemental analysis comparing the already unemployed caregivers (n = 1869) with those families who experience new unemployment (stop work), to understand how characteristics among these unemployed groups might differ.
Our institutional review board deemed this study exempt from human subjects review on the basis of its use of publicly available deidentified data.
Variables
FFE Definition
FFE status (yes or no) was defined by using 2 survey question items: “During the past 12 months, have you or other family members stopped working because of this child’s health or health conditions?” and “during the past 12 months, have you or other family members cut down on the hours you work because of this child’s health or health conditions?”
Participation in Government Assistance Programs
We defined participation in a government assistance program as the family self-report of receiving any one of the following in the past 12 months: cash assistance from a government welfare program; food stamps and/or Supplemental Nutrition Assistance Program (SNAP) benefits; free or reducedcost breakfasts or lunches at school; and WIC Program benefits.
Child and Caregiver Characteristics
Child characteristics in our analyses included: child age by NSCH grouping, biological sex, insurance coverage, and health rating. We recognize that race and ethnicity is a social construct; however, categorization of race and ethnicity may capture shared experiences of specific groups.21 Therefore, in our analyses, we examined race and ethnicity to assess disparate FFE outcomes to inform programs and policies that could decrease identified inequities. The child’s special health care need type, level of medical complexity, and receipt of care within a medical home were identified by using predefined NSCH categories.22,23 Current health conditions collected by the NSCH were also examined.
Primary caregiver and household characteristics were examined to include caregiver age, biological sex, highest level of education, marital status, and household size. Primary caregiver race and ethnicity were not available. Primary caregiver self-reported mental health and physical health were dichotomized between fair or poor versus excellent, very good, or good.24
Given the high number of missing values, the family poverty level (FPL) ratio was imputed by using the NSCH sequential regression imputation methods.25 Household spending out-of-pocket on health care in the past 12 months was also reported.
Hours spent by family providing direct medical care as well as the separate number of hours they spent arranging or coordinating were examined by using predefined NSCH categories.
Analysis
In our data analysis, we accounted for the complex sampling design using SAS 9.4 (SAS Institute, Inc, Cary, NC). χ2 tests were conducted to compare categorical child, caregiver, and household characteristics by FFE status. A 2-sided t test was used to evaluate caregiver mean age by FFE status. Because each of the variables used in this study had only <2% missing data, we treated missing data with a listwise deletion method. A primary multivariable logistic regression analysis was conducted to estimate the odds of FFE associated with weekly hours of medical care spent by a family. A secondary separate regression was conducted to estimate the odds of participation in any government programs associated with FFE. To control for anticipated confounding with sociodemographic factors, we included adjustments in the models for covariates on the basis of known literature and then refined them by the bivariate analysis, avoiding covariates with collinearity. With this selection process, we adjusted for caregiver sex, age, marital status, education, child age and race and ethnicity, and family FPL, except for the model of government program participation because income levels are used to determine program eligibility.
All results are presented with weighted percentages and 95% confidence intervals (CIs).
Forgone (Lost) Earnings Analysis
To estimate lost earnings associated with FFE on the basis of previously described methods,26,27 we used the US Bureau of Labor Statistics (BLS)28 reports of average hourly wages by year, state, race, sex, age, and full- and part-time employment status, in addition to the NSCH data. We generated several estimates that, in combination, account for core demographic characteristics of CSHCN caregivers reported in the NSCH and specified (un)employment circumstances. Given the NSCH does not include extensive employment details, we estimated forgone earnings using the “polar” cases (ie, upper and lower possible bounds), specifically assuming that either all parents who stopped working worked full-time (upper bound) or worked part-time (lower bound). For families indicating work stoppage, we calculate their forgone earnings as the BLS-reported average full- and part-time wages times 2080 work hours in a year. For families indicating cut work hours, we calculated the lost income using time reportedly spent on child care.26 For this group, forgone earnings were calculated as full- or part-time hourly wage rate per hour times the hours spent on child care (weekly) times 52 weeks in a year. We further enhance our estimates by merging wages data with individual NSCH data by the relevant demographic characteristics (age, race, and education) to produce family-specific estimates. The final, national-level estimates are produced by using survey weights. All wages were Consumer Price Index adjusted to 2020 US dollars, so the results are relevant to current day.
RESULTS
Characteristics of CSHCN Experiencing FFE
Overall, we found that 14.5% (95% CI 12.9%–16.1%) of families of CSHCN who were employed in the last 12 months experienced FFE because of the child’s health status or health condition. Among types of FFE, cutting hours because of a child’s health occurred the most frequently (Table 1).
TABLE 1.
Prevalence of FFE Attributed by Family Caregivers to a Child’s Health or Health Condition in Households With CSHCN With at Least 1 Employed Caregiver
| Unweighted n | Forgone Employment |
||
|---|---|---|---|
| Among All Households With CSHCN Who Had an Employed Caregiver Within the Past 12 mo, Weighted % (95% CI) | Among Households With FFE, Weighted % (95% CI) | ||
| No FFE | 12 327 | 85.5 (83.9–87.1) | — |
| With any FFE | 1723 | 14.5 (12.9–16.1) | — |
| Cut hours only | 1169 | 8.6 (7.6–9.6) | 59.3 (53.0–65.6) |
| Stopped work and cut hours | 411 | 4.2 (3.3–5.0) | 28.7 (23.5–34.0) |
| Stopped work only | 143 | 1.7 (0.7–2.8) | 12.0 (5.4–18.6) |
—, not applicable.
Compared with CSHCN in employed households without FFE, in CSHCN in households with FFE, the youngest age group (0–5 years) were overrepresented (Table 2). Similarly, CSHCN affected by FFE were disproportionately likely to have public versus private insurance and be of Hispanic ethnicity. CSHCN affected by FFE also had lower health status ratings, were more likely to have special health care needs because of functional limitations, and were more medically complex compared with CSHCN in employed households without FFE.
TABLE 2.
Characteristics of Children, Their Primary Caregivers, and Households With and Without FFE
| All CSHCN Who Had an Employed Caregiver Within the Past 12 mo (Unweighted N = 14050), Weighted % (95% CI) | Subgroups |
|||
|---|---|---|---|---|
| No Forgone Employment (Unweighted n = 12 327), Weighted % (95% CI) | Any Forgone Employment (Unweighted n = 1723), Weighted % (95% CI) | P | ||
| Child age, y | ||||
| 0–5 | 18.0 (16.5–19.4) | 16.3 (14.9–17.8) | 27.6 (22.7–32.5) | <.01 |
| 6–11 | 38.3 (36.3–40.3) | 38.1 (36.0–40.1) | 39.9 (33.7–46.2) | — |
| 12–17 | 43.7 (41.7–45.6) | 45.6 (43.5–47.7) | 32.5 (27.6–37.3) | — |
| Child sex | ||||
| Male | 57.6 (55.6–59.6) | 56.9 (54.8–59.0) | 61.6 (56.2–67.1) | .12 |
| Female | 42.4 (40.4–44.4) | 43.1 (40.9–45.2) | 38.4 (32.9–43.8) | — |
| Child race and/or ethnicity | ||||
| Non-Hispanic white | 54.5 (52.5–56.6) | 56.1 (53.9–58.3) | 45.0 (39.4–50.6) | .01 |
| Hispanic | 22.6 (20.5–24.8) | 20.9 (18.7–23.1) | 32.8 (25.9–39.7) | — |
| Non-Hispanic Black | 13.9 (12.3–15.5) | 14.0 (12.2–15.8) | 13.4 (9.8–16.9) | — |
| Other | 9.0 (8.0–9.9) | 9.0 (7.9–10.0) | 8.8 (6.7–11.0) | — |
| Child insurance coverage | ||||
| Private only | 55.3 (53.2–57.4) | 58.1 (55.8–60.3) | 38.7 (33.6–43.8) | .01 |
| Any public | 40.9 (38.3–43.1) | 38.0 (35.7–40.2) | 58.6 (53.2–63.9) | — |
| No coverage | 3.8 (2.9–4.6) | 3.9 (3.0–4.9) | 2.7 (0.6–4.9) | — |
| Child health status | ||||
| Excellent or very good | 73.5 (71.4–75.7) | 77.0 (74.7–79.3) | 53.2 (47.1–59.3) | .01 |
| Good, fair, or poor | 26.5 (24.3–28.6) | 23.0 (20.7–25.3) | 46.8 (40.7–52.8) | — |
| Child’s special health care need type | ||||
| Functional limitations (any) | 25.3 (23.2–27.4) | 20.9 (18.7–23.0) | 51.6 (45.7–57.5) | .01 |
| Prescription medications (only) | 32.2 (30.4–33.9) | 35.7 (33.7–37.7) | 11.0 (7.6–14.4) | — |
| Above-routine service use or specialized services (only) | 16.7 (15.3–18.1) | 16.9 (15.4–18.3) | 15.6 (11.3–19.9) | — |
| Prescription medication and above-routine service use | 25.8 (24.3–27.4) | 26.5 (24.8–28.2) | 21.8 (17.5–26.0) | |
| Child’s level of special health care need complexity | ||||
| Less complex health needs | 32.1 (30.4–33.9) | 35.7 (33.8–37.7) | 11.0 (7.6–14.4) | .01 |
| More complex health needs | 67.9 (66.1–69.6) | 64.3 (62.3–66.2) | 89.0 (85.6–92.4) | — |
| Child was reported as receiving care in medical home | ||||
| Care met medical home criteria | 45.1 (43.2–47.1) | 48.7 (46.6–50.7) | 24.2 (19.8–28.6) | .01 |
| Care did not meet medical home criteria | 54.8 (52.9–56.8) | 51.3 (49.2–53.4) | 75.8 (71.4–80.2) | — |
| Caregiver age in years, mean | 42.5 (42.1–42.9) | 42.9 (42.5–43.3) | 40.3 (39.5–41.2) | .01 |
| Caregiver sex | ||||
| Male | 23.6 (22.1–25.1) | 24.5 (22.8–26.2) | 18.4 (14.7–22.1) | .01 |
| Female | 76.4 (74.9–77.9) | 75.5 (73.8–77.2) | 81.6 (77.9–85.3) | — |
| Highest level of education | ||||
| Less than high school | 24.7 (22.5–26.9) | 23.4 (21.1–25.6) | 32.5 (25.6–39.4) | .01 |
| More than high school | 75.3 (73.1–77.5) | 76.6 (74.4–78.8) | 67.5 (60.6–74.4) | — |
| Marital status | ||||
| Married or living with partner | 77.0 (75.3–78.7) | 77.3 (75.5–79.1) | 75.3 (70.8–79.8) | .41 |
| Never married, divorced, separated, or widowed | 23.0 (21.3–24.6) | 22.7 (20.8–24.5) | 24.7 (20.2–29.2) | — |
| Caregiver mental health | ||||
| Fair or poor | 7.6 (6.2—8.9) | 7.2 (5.6–8 7) | 9.9 (7.3–12.5) | .07 |
| Excellent, very good, or good | 92.4 (91.1–93.8) | 92.8 (91.2–94.4) | 90.1 (87.5–92.7) | — |
| Caregiver physical health | ||||
| Fair or poor | 10.0 (8.5–11.5) | 9.9 (8.1–11.6) | 10.8 (7.9–13.6) | .60 |
| Excellent, very good, or good | 90.0 (88.5–91.5) | 90.1 (88.4–91.9) | 89.2 (86.4–92.1) | — |
| Flousehold Size | ||||
| ≤4 persons | 58.0 (55.9–60.1) | 57.9 (55.7–60.1) | 58.6 (52.3–64.9) | .84 |
| >4 persons | 42.0 (39.9–44.1) | 43.1 (39.9–44.2) | 41.4 (35.1–47.7) | — |
| Household FPL ratio, % | ||||
| <100 | 16.5 (14.6–18.4) | 15.0 (13.2–16.8) | 25.4 (18.5–32.2) | .01 |
| 100–199 | 22.5 (20.6–24.5) | 22.2 (20.0–24.3) | 24.4 (19.5–29.4) | — |
| 200–399 | 30.2 (28.5–31.9) | 30.6 (28.7–32.4) | 28.2 (23.7–32.7) | — |
| >400 | 30.8 (29.2–32.3) | 32.2 (30.5–33.9) | 22.0 (18.5–25.6) | — |
| Participation in government assistance program | ||||
| Any | 43.6 (41.5–45.7) | 41.6 (39.3–43.7) | 56.0 (50.4–61.6) | .01 |
| Government cash assistance | 4.7 (3.2—6.2) | 4.1 (2.8–5.4) | 8.3 (1.6–15.0) | .10 |
| Use of food stamps or SNAP | 20.2 (18.1–22.2) | 18.4 (16.3–20.4) | 31.0 (24.1–37.9) | .01 |
| Free or reduced lunch | 38.6 (36.4–40.7) | 36.7 (34.5–39.0) | 49.5 (43.4–55.5) | .01 |
| WIC | 11.0 (9.6–12.5) | 10.2 (8.6–11.7) | 16.1 (11.8–20.5) | .01 |
| Annual spending on child’s health care, $ | ||||
| 0 (no health care-related expenses) | 29.1 (27.0–31.2) | 28.1 (25.9–30.3) | 35.2 (28.7–41.8) | .01 |
| 1–999 | 47.0 (45.0–49.0) | 49.6 (47.5–51.7) | 31.6 (26.5–36.7) | — |
| 1000–5000 | 19.5 (18.2–20.9) | 18.9 (17.5–20.3) | 23.4 (19.0–27.8) | — |
| >5000 | 4.4 (3.6—5.0) | 3.4 (2.7–4.1) | 9.8 (7.6–12.0) | — |
| No. hours per week spent on child’s medical care | ||||
| 0 | 69.7 (67.8–71.7) | 75.0 (73.1–76.9) | 38.3 (32.7–42.8) | .01 |
| <1 | 13.0 (11.8–14.2) | 13.4 (12.0–14.6) | 11.4 (8.7–14.1) | — |
| 1–4 | 9.0 (8.0–10.1) | 6.8 (5.9–14.6) | 22.1 (17.4–26.8) | — |
| 5–10 | 3.5 (2.3–4.7) | 1.8 (1.1–2.6) | 13.1 (6.7–19.7) | — |
| ≥11 | 4.8 (3.6—5.9) | 3.0 (1.8–4.3) | 15.1 (11.9–18.5) | — |
| No. hours per week spent on care coordination | ||||
| 0 | 68.3 (66.5–70.2) | 73.4 (71.6–75.3) | 38.0 (31.7–44.4) | .01 |
| <1 | 20.4 (18.9–21.8) | 19.8 (18.3–21.3) | 23.9 (20.0–27.9) | — |
| 1–4 | 9.0 (7.8–10.2) | 5.5 14.4–6.5) | 29.7 (24.7–34.8) | — |
| 5–10 | 1.2 (0.9,16) | 0.6 (0.4–0.9) | 4.7 12.7–6.5) | — |
| ≥11 | 1.1 (0.2–2.1) | 0.7 (0.0–1.8) | 3.7 (2.1–5.2) | — |
—, not applicable.
The weighted proportion of children with specific health conditions whose family reported FFE is presented in Fig 1. Households of CSHCN with intellectual disability, cerebral palsy, and brain injury had the highest proportions of reported FFE.
FIGURE 1.
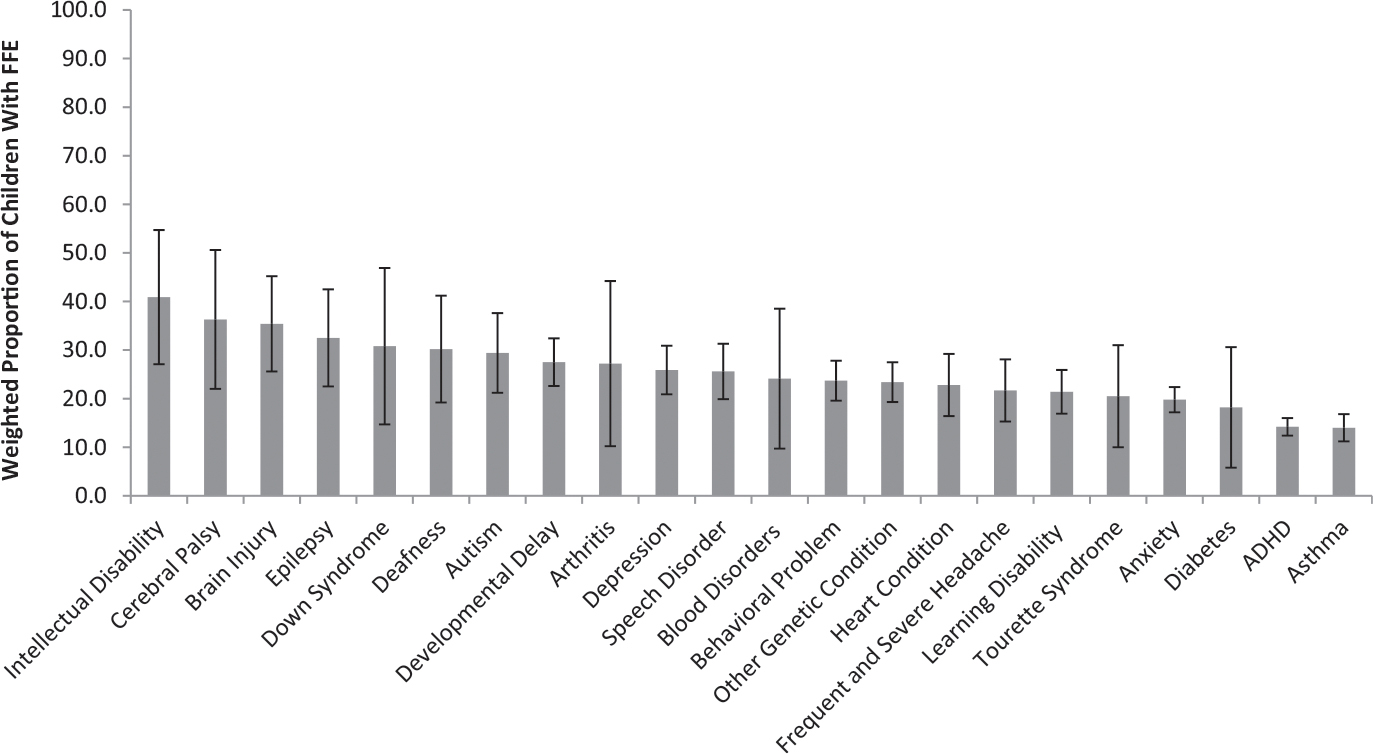
Weight proportion of children with health conditions whose families reported FFE. Bars indicate 95% CIs. The results reveal the weighted proportion of children of families with FFE among families with at least 1 employed caregiver in the past 12 months. ADHD, attention-deficit/hyperactivity disorder.
Characteristics of Caregivers and Households Experiencing FFE
Caregivers of CSHCN with FFE were more likely to be younger and female and less likely to have more than a high school education, compared with caregivers of CSHCN not affected by FFE (Table 2). In addition, affected households were disproportionately likely to live in poverty and participate in a government assistance program. In a U-shaped distribution, families affected by FFE were more likely to not spend money on a child’s health care but were also more likely to spend >$5000 per year on a child’s health care, compared with unaffected families.
Association Between Hours of Medical Care and Odds of FFE
We found a strong association between the adjusted odds of FFE due to a child’s health or health condition and increasing hours of medical care spent per week by a family member caring for the child. Specifically, the adjusted odds ratio (aOR) for FFE was 1.72 (95% CI 1.25–2.36) for families spending <1 hour per week on medical care for their CSHCN, compared with families with CSHCN that required no hours for medical care. These adjusted odds of FFE increased as the hours of medical care per week typically increased, with an aOR of 5.96 (95% CI 4.30–8.27) when families spent 1 to 4 hours per week on care, an aOR of 11.89 (95% CI 6.19–22.81) when families spent 5 to 10 hours per week on care, and an aOR of 8.89 (95% CI 5.26–15.01) when families spent >10 hours per week on care.
Association Between FFE and Government Program Use
We found that, when adjusting for a variety of family and patient characteristics, employed families of CSHCN who experienced FFE because of their child’s health condition were more likely to use a government program (aOR of 1.34 [95% CI 1.01–1.77]), compared with unaffected families of CSHCN.
Forgone (Lost) Earnings Estimate
The estimated earnings lost are presented in Table 3. They are presented by age and sex, race and sex, and education attainment and sex. Except by state of residence, data are reported separately for full-and part-time employees.
TABLE 3.
Estimated Forgone (Lost) Earnings for FFE Because of Their Child’s Health or Health Condition
| Annualized Cost |
Annual Aggregate National Estimate for Households With CSHCN, 95% CI, $ (billions) | |||
|---|---|---|---|---|
| Lost Earnings | Cost per Hour of Caregiving, $ | Mean, $ | 95% CI, $ | |
| Accounting for state of residence | 18.89 | 18 051 | 15 556–20 547 | 12.3–16.3 |
| Full-time | ||||
| Accounting for age and sex | 22.47 | 21 427 | 18 588–24 265 | 14.7–19.2 |
| Accounting for race and sex | 21.65 | 20 689 | 18 1 19–23 258 | 14.3–18.4 |
| Accounting for education and sex | 23.81 | 21 265 | 19 024–23 506 | 15.1 –18.6 |
| Part-time | ||||
| Accounting for age and sex | 16.26 | 15 483 | 13 460–17 507 | 10.7–13.9 |
| Accounting for race and sex | 13.73 | 13105 | 11 410–14 800 | 9.0–11.7 |
| Accounting for education and sex | 13.75 | 13 063 | 1 1 372–14 753 | 9.0–11.7 |
Annualized costs and the annual aggregate national estimate across households with CSHCN with different caregiver characteristics are shown. All results are shown in 2020 US dollars. Estimates are based on the upper and lower bounds of forgone employment (assuming full-time versus part-time previous employment) assuming 2080 work hours per year in 52-week year. Estimates are merged with NSCH respondent-specific characteristics of age, race, and education. Lost earnings are shown with full-time and part-time wage rates. FFE estimates calculated on the basis of the state of residence are lower because these estimates average full- and part-time employment earnings in the absence of a separate report from the BLS.
Lost earnings for each household with FFE were estimated at ~$18000 per year when accounting for state of residence. Annual aggregate national estimates of FFE were similar across different caregiver characteristics, averaging $14.3 to $19.2 billion per year for caregivers of CSHCN assuming full-time work and $9.0 to $13.9 billion for caregivers assuming part-time work.
Unemployed Families Comparison
The comparison of already unemployed caregivers (n = 1869) with those families who experienced new unemployment (ie, stop work [n = 554]) is shown in Supplemental Table 4. Children in families experiencing new unemployment because of their health condition were more likely to be younger, Hispanic, and privately insured. The family caregivers who newly stopped work because of their child’s health were younger, were more likely to be married or partnered, reported better health, and had lower participation in government assistance programs than those already unemployed.
DISCUSSION
We found that ~15% of families of CSHCN with at least 1 continuously employed caregiver in the previous year experienced FFE because of their children’s health conditions and that the prevalence of FFE varied significantly with child age, ethnicity, and health condition. Altogether, FFE accounted for an estimated $18 000 in annual lost earnings per affected US household in 2016–2017.
With these findings, we reinforce a body of literature evaluating the financial impacts of childhood health conditions within families.12–15,29–32 Specifically, with our study, we add to the existing literature that examines general associations between children’s health care needs and family employment by evaluating the NSCH questions that specifically link family’s employment status to the child’s condition.9,17 FFE does remain, however, only part of the larger financial impact of a child’shealth condition on families, including out-of-pocket health expenses,14,33,34 transportation and meal costs for appointments,35,36 and higher living expenses needed for the child’scare (eg, electricity and adaptive home renovations).37,38
We found that FFE was not experienced proportionally. Hispanic families were disproportionately affected, as were families of CSHCN whose caregivers who had lower education and income levels. Of particular concern, families experiencing FFE because of their child’s condition were disproportionately likely to pay the highest amount (>$5000 per year) in out-of-pocket health expenses. Notably, for families with employer-sponsored health care coverage that does not adequately meet their child’s needs, given the family’s wages, the insurance itself may not remain affordable, so families may face either descent into poverty or modify their income so that their child is eligible for Medicaid benefits. Overall, with these results, we underscore that policies created to ameliorate FFE and insure families against the costs of health care needs must carefully consider how to mitigate lost income across varying family financial circumstances, to avoid widening wealth disparities. Notably, however, families experiencing new unemployment because of their child’s health condition had proportionally higher financial stability and health than those who were already generally unemployed.
Currently the United States lacks a national paid family leave program, and although some private companies may provide paid family medical leave benefits, they remain primarily focused on short-term leave (eg, postpartum care) and not on the longitudinal, chronic health needs of employees’ dependents. Although the US Social Security Income (SSI) program does provide financial assistance to some families of CSHCN, SSI requires that the child have marked and severe impairment that is expected to result in death or last for no less than 12 months.39 Our results suggest that these strict criteria may not reach the full scope of families of CSHCN whose employment is impacted by children’s health, including those with mental and behavioral health conditions.
Maintaining financial support for families through the challenges of a child’s health condition has clear implications for society as a whole as well. Although government budget allocation and hospital funding priorities are organized into separate sectors (eg, education, health, etc), our work and others’ highlight how investments in health have consequences across sectors. Specifically, we found that families with FFE associated with children’s health had an increased likelihood of participating in government assistance programs, even after adjusting for other social factors. Creating cross-cutting approaches to address health needs and economic stability in families, therefore, promises to have a broader impact beyond the individual family economy.
Similar to previous analyses based on the 2009–2010 national survey data, our results indicated that CSHCN with poorer health ratings and functional impairment who required increasing hours of medical care were more likely to have caregivers who reported affected employment. Specifically, children with neurologic conditions that typically impact a child’s activities of daily living, especially those involving global brain functioning, continue to have a higher reported prevalence of impact on family employment.
With these findings in mind, in addition to considering the expansion of paid family leave and health-related economic assistance policies, the expansion of caregiving programs may prove important to mitigating FFE. Likely, no single program will meet the needs of all affected CSHCN, with researchers of previous literature indicating a difference in families’ knowledge and preferences regarding family leave.40–42 However, additional considerations include improving the availability of child care programs that serve children with serious neurologic, behavioral, or device-dependent needs, expanding the availability of a high-quality home health care workforce,43 and increasing the option of paid family caregiving models across states.44 Although a better understanding of the presence and scope of such programs is needed, one can imagine that for a select group of children with high in-home medical care needs, paid family caregiving and/or high-quality home health care may alleviate some health-related caregiving needs that lead to family underemployment.
Because of the cross-sectional nature of the NSCH, this study design cannot be used to examine causality between FFE and the variables examined, only their association with each other. Because of the phrasing of the survey questions, this analysis lacks sensitivity for capturing short-term lost family earnings that may have occurred because of episodic acute illness or routine health care visits. However, the selected questions have unique specificity at attributing the FFE to the child’s health or health condition, which likely accounts for forgone earnings of a larger magnitude. In addition, we do not know what kind of cash assistance families may have received within a government program and whether it could have been because of the child’s health condition itself (ie, SSI). Among children with multiple conditions, it is unknown which specific condition listed was the condition that led to the FFE. Our working definition of employment, as 50 of 52 weeks, may also have excluded seasonal workers or intermittent workers, thereby underestimating the FFE impact. Lastly, with the survey, we did not gather information on family caregiver race or ethnicity, limiting the evaluation of that variable on the outcome.
CONCLUSIONS
The connection between child health and family employment is quantifiable and substantial. With our findings, we suggest that more policies and programs that address the impact of CSHCN health on their families’ economic stability are needed. The expansion of paid family leave policies, day care centers able to serve CSHCN, pediatric home health care services, and paid family caregiving may be considered at the local, state, and national levels to bolster families. Given the disproportionate impact of CSHCN-related FFE on families of color, such interventions may also foster greater health equity.
Supplementary Material
WHAT’S KNOWN ON THIS SUBJECT:
Social factors, such as family income, are strongly associated with child health outcomes. However, child health also has effects on the family, which, if quantified, can aid in developing effective health care policies that maximize both child and family well-being.
WHAT THIS STUDY ADDS:
With this study, we update our understanding of the relationship between child health conditions and forgone family employment and discusses the related policy implications and opportunities to improve the well-being of families affected by childhood disease.
FUNDING:
Dr Heard-Garris’s efforts were supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health (grant K01HL147995). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Dr Kan is supported by grant K12 HS026385 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. Funded by the National Institutes of Health (NIH).
ABBREVIATIONS
- aOR
adjusted odds ratio
- BLS
US Bureau of Labor Statistics
- CI
confidence interval
- CSHCN
children with special health care needs
- FFE
forgone family employment
- FPL
family poverty level
- NSCH
National Survey of Children’s Health
- SNAP
Supplemental Nutrition Assistance Program
- SSI
Social Security Income
- WIC
Special Supplemental Nutrition Program for Women, Infants, and Children
Footnotes
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
FINANCIAL DISCLOSURE: Dr Foster received compensation for medical record consultation and/or expert witness testimony; the other authors have indicated they have no financial relationships relevant to this article to disclose.
COMPANION PAPER: A companion to this article can be found online at www.pediatrics.org/cgi/doi/10.1542/peds.2021-050448.
REFERENCES
- 1.Council on Community Pediatrics. Poverty and child health in the United States. Pediatrics. 2016;137(4):e20160339. [DOI] [PubMed] [Google Scholar]
- 2.Trent M, Dooley DG, Dougé J; Section on Adolescent Health; Council on Community Pediatrics; Committee on Adolescence. The impact of racism on child and adolescent health. Pediatrics. 2019;144(2):e20191765. [DOI] [PubMed] [Google Scholar]
- 3.Karpur A, Lello A, Frazier T, Dixon PJ, Shih AJ. Health disparities among children with autism spectrum disorders: analysis of the National Survey of Children’s Health 2016. J Autism Dev Disord. 2019;49(4):1652–1664 [DOI] [PubMed] [Google Scholar]
- 4.Heard-Garris N, Sacotte KA, Winkelman TNA, et al. Association of childhood history of parental incarceration and juvenile justice involvement with mental health in early adulthood. JAMA Netw Open. 2019;2(9):e1910465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lin YC, Seo DC. Cumulative family risks across income levels predict deterioration of children’s general health during childhood and adolescence. PLoS One. 2017;12(5):e0177531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Victorino CC, Gauthier AH. The social determinants of child health: variations across health outcomes - a population-based cross-sectional analysis. BMC Pediatr. 2009;9:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yoshikawa H, Aber JL, Beardslee WR. The effects of poverty on the mental, emotional, and behavioral health of children and youth: implications for prevention. Am Psychol. 2012;67(4):272–284 [DOI] [PubMed] [Google Scholar]
- 8.Witt WP, Gottlieb CA, Hampton J, Litzelman K. The impact of childhood activity limitations on parental health, mental health, and workdays lost in the United States. Acad Pediatr. 2009;9(4):263–269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kuhlthau K, Hill KS, Yucel R, Perrin JM. Financial burden for families of children with special health care needs. Matern Child Health J. 2005;9(2): 207–218 [DOI] [PubMed] [Google Scholar]
- 10.Kish AM, Newcombe PA, Haslam DM. Working and caring for a child with chronic illness: a review of current literature. Child Care Health Dev. 2018; 44(3):343–354 [DOI] [PubMed] [Google Scholar]
- 11.National Alliance for Caregiving. Rare disease caregiving in America. Available at: https://www.caregiving.org/rare/. Accessed July 31, 2018
- 12.Saunders BS, Tilford JM, Fussell JJ, Schulz EG, Casey PH, Kuo DZ. Financial and employment impact of intellectual disability on families of children with autism. Fam Syst Health. 2015;33(1):36–45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ghandour RM, Hirai AH, Blumberg SJ, Strickland BB, Kogan MD. Financial and nonfinancial burden among families of CSHCN: changes between 2001 and 2009–2010. Acad Pediatr. 2014;14(1): 92–100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goudie A, Narcisse MR, Hall DE, Kuo DZ. Financial and psychological stressors associated with caring for children with disability. Fam Syst Health. 2014; 32(3):280–290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Thomson J, Shah SS, Simmons JM, et al. Financial and social hardships in families of children with medical complexity. J Pediatr. 2016;172: 187–193.e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Simpser E, Hudak ML; Section on Home Care; Committee on Child Health Financing. Financing of pediatric home health care. Pediatrics. 2017;139(3):e20164202. [DOI] [PubMed] [Google Scholar]
- 17.Kuhlthau KA, Perrin JM. Child health status and parental employment. Arch Pediatr Adolesc Med. 2001;155(12): 1346–1350 [DOI] [PubMed] [Google Scholar]
- 18.McPherson M, Arango P, Fox H, et al. A new definition of children with special health care needs. Pediatrics. 1998;102(1 pt 1):137–140 [DOI] [PubMed] [Google Scholar]
- 19.The Child and Adolescent Health Measurement Initiative. The National Survey of Children’s Health. Available at: https://www.childhealthdata.org/learn-about-the-nsch/NSCH. Accessed April 8, 2020
- 20.The Child and Adolescent Health Measurement Initiative. 2017. National Survey of Children’s Health (NSCH): sampling and survey administration. Available at: https://www.childhealthdata.org/docs/default-source/default-document-library/2017-nsch-sampling-administration_finaladba3af3c0266255aab2ff00001023b1.pdf?sfvrsn=989c5817_0. Accessed November 20, 2020
- 21.Heard-Garris N, Williams DR, Davis M. Structuring research to address discrimination as a factor in child and adolescent health. JAMA Pediatr. 2018; 172(10):910–912 [DOI] [PubMed] [Google Scholar]
- 22.Child and Adolescent Health Measurement Initiative. 2016–2017 National Survey of Children’s Health. Available at: https://www.childhealthdata.org/docs/default-source/nsch-docs/spss-code-book_-2016-2017nsch_drcv1_01-11-19.pdf. Accessed December 28, 2020
- 23.Bethell CD, Blumberg SJ, Stein RE, Strickland B, Robertson J, Newacheck PW. Taking stock of the CSHCN screener: a review of common questions and current reflections. Acad Pediatr. 2015;15(2):165–176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. a meta-analysis. J Gen Intern Med. 2006;21(3):267–275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.US Census Bureau. Imputation data guide. Available at: https://www.census.gov/content/dam/Census/programssurveys/nsch/tech-documentation/methodology/2017-NSCH-Analysis-with-Imputed-Data-Guide.pdf. Accessed October 1, 2018
- 26.Romley JA, Shah AK, Chung PJ, Elliott MN, Vestal KD, Schuster MA. Family-provided health care for children with special health care needs. Pediatrics. 2017; 139(1):e20161287. [DOI] [PubMed] [Google Scholar]
- 27.Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM. Monetary costs of dementia in the United States. N Engl J Med. 2013;368(14): 1326–1334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.US Bureau of Labor Statistics. Databases, tables & calculators by subject. Available at: https://data.bls.gov. Accessed June 1, 2020 [Google Scholar]
- 29.Kuo DZ, Cohen E, Agrawal R, Berry JG, Casey PH. A national profile of caregiver challenges among more medically complex children with special health care needs. Arch Pediatr Adolesc Med. 2011;165(11):1020–1026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Perrin JM, Fluet CF, Honberg L, et al. Benefits for employees with children with special needs: findings from the collaborative employee benefit study. Health Aff (Millwood). 2007; 26(4):1096–1103 [DOI] [PubMed] [Google Scholar]
- 31.Ouyang L, Grosse SD, Riley C, et al. A comparison of family financial and employment impacts of fragile X syndrome, autism spectrum disorders, and intellectual disability. Res Dev Disabil. 2014;35(7):1518–1527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Pagano E, Baldi I, Mosso ML, et al. The economic burden of caregiving on families of children and adolescents with cancer: a population-based assessment. Pediatr Blood Cancer. 2014;61(6):1088–1093 [DOI] [PubMed] [Google Scholar]
- 33.Shattuck PT, Parish SL. Financial burden in families of children with special health care needs: variability among states. Pediatrics. 2008;122(1):13–18 [DOI] [PubMed] [Google Scholar]
- 34.Chang LV, Shah AN, Hoefgen ER, et al. ; H2O Study Group. Lost earnings and nonmedical expenses of pediatric hospitalizations. Pediatrics. 2018;142(3):e20180195. [DOI] [PubMed] [Google Scholar]
- 35.Hensley C, Heaton PC, Kahn RS, Luder HR, Frede SM, Beck AF. Poverty, transportation access, and medication nonadherence. Pediatrics. 2018;141(4):e20173402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Flores G, Abreu M, Olivar MA, Kastner B. Access barriers to health care for Latino children. Arch Pediatr Adolesc Med. 1998;152(11):1119–1125 [DOI] [PubMed] [Google Scholar]
- 37.Aplin T, de Jonge D, Gustafsson L. Understanding the dimensions of home that impact on home modification decision making. Aust Occup Ther J. 2013;60(2):101–109 [DOI] [PubMed] [Google Scholar]
- 38.Glendinning C, Kirk S, Guiffrida A, Lawton D. Technology-dependent children in the community: definitions, numbers and costs. Child Care Health Dev. 2001;27(4):321–334 [DOI] [PubMed] [Google Scholar]
- 39.Byers E, Valliere FR, Houtrow AJ, eds. National Academies of Sciences Engineering and Medicine; Health and Medicine Division; Board on Health Care Services; Committee on Improving Health Outcomes for Children With Disabilities. Opportunities for Improving Programs and Services for Children With Disabilities. Washington, DC: National Academies Press; 2018 [PubMed] [Google Scholar]
- 40.Schuster MA, Chung PJ, Elliott MN, Garfield CF, Vestal KD, Klein DJ. Awareness and use of California’s Paid Family Leave Insurance among parents of chronically ill children. JAMA. 2008;300(9):1047–1055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chung PJ, Lui CK, Cowgill BO, Hoffman G, Elijah J, Schuster MA. Employment, family leave, and parents of newborns or seriously ill children. Acad Pediatr. 2012;12(3):181–188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Chung PJ, Garfield CF, Elliott MN, Carey C, Eriksson C, Schuster MA. Need for and use of family leave among parents of children with special health care needs. Pediatrics. 2007;119(5). Available at: www.pediatrics.org/cgi/content/full/119/5/e1047 [DOI] [PubMed] [Google Scholar]
- 43.Foster CC, Agrawal RK, Davis MM. Home health care for children with medical complexity: workforce gaps, policy, and future directions. Health Aff (Millwood). 2019;38(6): 987–993 [DOI] [PubMed] [Google Scholar]
- 44.Colorado Department of Public Health & Environment. Parents as their child’s certified nursing aide (CNA). Available at: https://www.colorado.gov/pacific/cdphe/parents-their-childs-certified-nursingaide-cna. Accessed October 8, 2019
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.