

Abstract
Background and Objectives
The relationship between smoking, long-term brain atrophy, and clinical disability in patients with multiple sclerosis (MS) is unclear. Here, we assessed long-term effects of smoking by evaluating MRI and clinical outcome measures after 10 years in smoking and nonsmoking patients with relapsing-remitting MS (RRMS).
Methods
We included 85 treatment-naive patients with RRMS with recent inflammatory disease activity who participated in a 10-year follow-up visit after a multicenter clinical trial of 24 months. Smoking status was decided for each patient by 2 separate definitions: by serum cotinine levels measured regularly for the first 2 years of the follow-up (during the clinical trial) and by retrospective patient self-reporting. At the 10-year follow-up visit, clinical tests were repeated, and brain atrophy measures were obtained from MRI using FreeSurfer. Differences in clinical and MRI measurements at the 10-year follow-up between smokers and nonsmokers were investigated by 2-sample t tests or Mann-Whitney tests and linear mixed-effect regression models. All analyses were conducted separately for each definition of smoking status.
Results
After 10 years, smoking (defined by serum cotinine levels) was associated with lower total white matter volume (β = −21.74, p = 0.039) and higher logT2 lesion volume (β = 0.22, p = 0.011). When defining smoking status by patient self-reporting, the repeated analyses found an additional association with lower deep gray matter volume (β = −2.35, p = 0.049), and smoking was also associated with a higher score (higher walking impairment) on the log timed 25-foot walk test (β = 0.050, p = 0.039) after 10 years and a larger decrease in paced auditory serial addition test (attention) scores (β = −3.58, p = 0.029).
Discussion
Smoking was associated with brain atrophy and disability progression 10 years later in patients with RRMS. The findings imply that patients should be advised and offered aid in smoking cessation shortly after diagnosis, to prevent long-term disability progression.
Smoking is a known negative prognostic factor in patients with multiple sclerosis (MS), associated with higher disability1 and higher risk of conversion to progressive disease phenotypes.1,2 The causal relationship between these associations is not clear, and several pathophysiologic mechanisms have been proposed, for example: cigarette smoke triggering a proinflammatory cascade, inducing autoimmunity and heightened inflammatory activity; facilitating entry of immune cells to the CNS by disruption of the blood-brain barrier (BBB); epigenetic changes; and direct neurotoxicity due to mitochondrial damage.3,4
Studies examining the relation between smoking and inflammatory disease activity have reported inconsistent findings. Although some studies found smoking to be associated with higher relapse rates5 and lesion loads,1,6,7 2 studies using cotinine, an alkaloid metabolite of nicotine,8 to define smoking status, did not.9,10
In MS, smoking has cross-sectionally been shown to be associated with lower total brain volume,1,6,11-13 but longitudinal relationships have been less well studied and with varying results.1,7,9 Furthermore, few studies have considered the relation between smoking and gray matter (GM) atrophy, again with conflicting results.6,11,13
To better understand the possible adverse prognostic effects of smoking in MS, we aimed to investigate the relation between smoking and long-term brain lesion load, atrophy, and clinical outcome measures, first by comparing smokers and nonsmokers, defined by both patient self-reporting and cotinine levels, and second by studying a possible dose effect, using mean cotinine levels in smoking patients with MS.
Methods
Participants
The patients included in this study participated in a 10-year follow-up visit, after a multicenter trial on ω-3 fatty acids in MS (the OFAMS-study). In the original trial, a total of 92 patients with relapsing-remitting MS (RRMS) were followed up for 24 months; a detailed description of the study is provided elsewhere.14 During the OFAMS study period, patients attended regular follow-up visits at their local study site, undergoing biochemical, radiologic, and clinical examinations, including the Expanded Disability Status Scale (EDSS), timed 25-foot walk test (T25FW), the dominant hand and nondominant hand 9-hole peg test, and the paced auditory serial addition test (PASAT). Ten years after the trial concluded, all available (87) participants were invited to a follow-up visit, of which 85 accepted.15 At the 10-year follow-up visit, the patients repeated the radiologic and clinical examinations. Between the OFAMS-study and the 10-year follow-up visit, the participants had received routine clinical treatment and care.
Standard Protocol Approvals, Registrations, and Patient Consents
The OFAMS-study and the 10-year follow-up were approved by the Regional Committee for Medical and Health Research Ethics in Western Norway Regional Health Authority (OFAMS-study: clinicaltrials.gov, Identifier: NCT00360906). All participants gave their written informed consent.
Cotinine Measurement
Serum samples were stored at −80°C until analysis and performed simultaneously for all samples from each patient. As previously described,10 serum cotinine levels were measured by liquid chromatography tandem mass spectrometry at Bevital AS (Bergen, Norway). Laboratory technicians were blinded to patient clinical status. Serum cotinine levels were analyzed from samples collected during the OFAMS-study at baseline (BL) and months 6, 12, 18, and 24.
Definitions of Smokers and Nonsmokers
The effect of smoking status on long-term MRI and clinical outcome measures was analyzed using 2 definitions (described below) of smoking status separately: by (1) serum cotinine levels, with the findings presented in the main text and (2) patient self-reporting, with the findings presented in the supplemental material.
Smoking Defined by Cotinine Levels
Cotinine levels >85 nmol/L indicate recent tobacco use16 and are regarded to distinguish tobacco users from nontobacco users in the general population.17 Patients were categorized into 2 groups according to serum cotinine level: smokers were defined as patients with serum cotinine level >85 nmol/L in ≥60% of the samples and nonsmokers were defined as patients with serum cotinine levels ≤85 nmol/L in ≥60% of the samples. Based on previous studies not finding nicotine or smokeless tobacco to be associated with MS disease progression,18,19 patients who at the 10-year follow-up visit reported “snuff” use (oral tobacco), but no smoking for the past 10 years, were defined as nonsmokers (Figure 1).
Figure 1. Flowchart Illustrating the Classification Process According to the 2 Definitions of Smoking.

Smoking Defined by Patient Self-Reporting
At the 10-year follow-up visit, patients answered a questionnaire about habits of tobacco use, including smoking and snuff use. Patients who reported to have smoked regularly within the past 10 years were defined as smokers while patients who did not report regular smoking, or reported only snuff use (6 patients), were defined as nonsmokers (Figure 1).
Risk Factors and Presence of Peripheral, Cardiovascular, or Cerebrovascular Disease
Vascular risk factors and established peripheral, cardiovascular, and cerebrovascular disease are independently associated with brain imaging changes.20 As smoking is a known risk factor for such conditions,21 patient-reported hypertension, dyslipidemia, hypercoagulable disorder, and symptomatic cardiovascular or cerebrovascular disease and/or events was designated as a dichotomous vascular disease (VD) factor and included as a covariate in the final analyses.
MRI Data and Analysis
The 10-year Follow-up Visit
Imaging was performed at the different study sites, on a 3 Tesla (T) MRI scanner if available, alternatively using a 1.5T MRI scanner, with a standard head coil. The acquisition protocol included the following MRI sequences: a T2-weighted 3D sagittal fluid attenuated inversion recovery (FLAIR) (resolution: 1 × 1 × 1 mm3, echo time (TE)/repetition time (TR)/inversion time (TI) = 386/5000/1.65–2.2 ms) and a postcontrast T1-weighted 3D sagittal magnetization-prepared rapid gradient echo sequence (resolution: 1 × 1 × 1mm3, TE/TR/TI = 2.28/1800/900 ms, flip angle 8°). Acquisition details across sites are presented in eTable 1, links.lww.com/NXI/A728.
Lesion Segmentation
Lesion segmentation was performed on FLAIR images using lesion segmentation tool (version 2.0.15; applied-statistics.de/lst.html).22 To optimize lesion filling, gadolinium-enhancing regions (both lesions and other regions) were first removed, by applying an upper intensity threshold at the 98th percentile. Next, the FMRIB Software Library (version 5.0.1023) was used to fill in abnormal voxels in these preprocessed T1-weighted images using the lesion_filling tool.24 Then, only the filled lesion voxels were pasted back into the original postcontrast 3D T1-weighted images to create the final lesion filled images.
Morphological Reconstruction
Cortical reconstruction and parcellation for (local) cortical volume and thickness measurement and subcortical segmentation were performed with FreeSurfer version 7.1.1, a freely available software package for academic use, available through online download.25 The technical details of FreeSurfer procedures have been previously described.26,27 The use of FreeSurfer on postcontrast 3D T1-weighted images as applied here, was recently validated.28
Quality control was performed by visual inspection, discarding cases with large segmentation errors. Minor to moderate segmentation errors of specific anatomic regions were found in all scans and are previously shown to occur more frequently and to a more severe degree in postcontrast images.28 As these errors were so commonly occurring, mostly with the same effect (overestimation of GM volume/cortical thickness28), we chose to not apply any manual corrections for these errors in our analyses.
The Desikan-Killiany atlas29 was used to extract cortical thickness measures. The mean cortical thickness of the left and right hemisphere was averaged to calculate the overall mean cortical thickness. Furthermore, total cerebral GM and white matter (WM) volume and total deep GM and thalamus volume (average of left and right hemisphere) were obtained. Because of frequent suboptimal segmentation of the temporal pole (previously found in a minor to moderate degree in almost 50% of postcontrast scans28), this region was excluded when calculating the total GM volume.
Statistical Analysis
Statistical analyses were performed using Statistical Product and Service Solutions (SPSS) for macOS (Version 25; SPSS, Chicago, IL) and R software (V.4.0.5).
Kolmogorov-Smirnov tests and visual inspection of the histograms were used to assess the normality of the variables.
The primary outcome measures were MRI and clinical measurements obtained cross-sectionally at the 10-year follow-up visit and the difference in clinical measurements from month 24 to the 10-year follow-up.
As a first exploratory analysis, the difference in outcome measures between smokers and nonsmokers was analyzed by 2-sample t tests for normally distributed variables; otherwise, Mann-Whitney tests were used.
The relationship of smoking status and mean cotinine level with MRI and clinical outcome measures was then further investigated by a linear mixed-effect regression model, correcting for age, sex, vascular disease, estimated total intracranial volume (eTIV) (eTIV included as a covariate in analyses regarding brain volume measurements), BL EDSS, and time from diagnosis. To correct for scanner variability, MRI scanner was entered as a random effect. Assumptions for linear regression were checked for each final model; if the assumptions were not satisfied, log-linear transformation was performed (e.g., logT2 lesion volume). For variables with values below 1, a constant was added before log transformation.
Data Availability
Data not provided within this article may be shared (anonymized) by request from a qualified investigator.
Results
Patient Characteristics
We included the 85 patients who participated in the 10-year follow-up. Each patient was classified as a smoker or nonsmoker, by the 2 different definitions of smoking: (1) by cotinine levels measured during the OFAMS-study and (2) by retrospective patient self-reporting at the 10-year follow-up (Figure 1). Samples available for cotinine analyses were missing for one patient, and another patient did not complete the questionnaire concerning tobacco use, leaving 84 patients to be classified as smoker or nonsmoker by each definition. Including the 2 patients missing either cotinine measurements or the questionnaire, 9 patients were classified differently based on the 2 definitions. Forty-seven patients were smokers and 37 nonsmokers defined by cotinine levels. By patient self-reporting, 48 patients were smokers and 36 nonsmokers. Of the 48 smokers defined by patient self-reporting, 47 reported to smoke 10 years ago. Additional patient self-reported smoking habits are listed in supplemental eTable 2, links.lww.com/NXI/A728.
The mean follow-up time from the BL and month 24 visit to the 10-year follow-up visit was 12.0 (±0.6) and 10.0 (±0.6) years, respectively. Table 1 summarizes the clinical characteristics of the included patients.
Table 1.
Demographic and Clinical Characteristics

Difference in MRI and Clinical Outcome Measures Between Smokers and Nonsmokers
The results of the exploratory t tests are shown in Table 2 (smoking defined by cotinine levels) and supplemental eTable 3, links.lww.com/NXI/A728 (smoking defined by patient self-reporting). In brief, total WM (p = 0.015) and deep GM (p = 0.017) volumes were significantly smaller, and total T2 lesion volumes were significantly larger (p = 0.014) in smokers defined by cotinine level (figure 2). For the clinical measures, smokers had a higher score (more disability) on the T25FW test (p = 0.031) after 10 years and a larger decrease in attention scores measured by the PASAT test (p = 0.042) between month 24 and the 10-year follow-up visit (figure 3). The results were similar for smoking defined by patient self-reporting (eTable 3).
Table 2.
MRI and Clinical Measures in Smokers and Nonsmokers (Defined by Cotinine Level) at the 10-Year Follow-up Visit and Change in Clinical Measures Between Month 24 and the 10-Year Follow-up Visit

Figure 2. Distribution Plots of MRI Measurements at the 10-Year Follow-up Visit in Nonsmokers and Smokers.
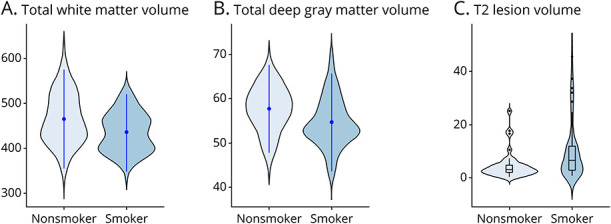
The width of the shaded area represents the proportion of observations for (A) total white matter volume (mL) and (B) total deep gray matter volume (mL) (point range represents the mean and SD), and (C) T2 lesion volume (mL) (box plots represent the median and IQR, with the whiskers representing the distribution of observations within x1.5 of the IQR). IQR = interquartile range.
Figure 3. Distribution Plots of Clinical Measurements in Nonsmokers and Smokers.
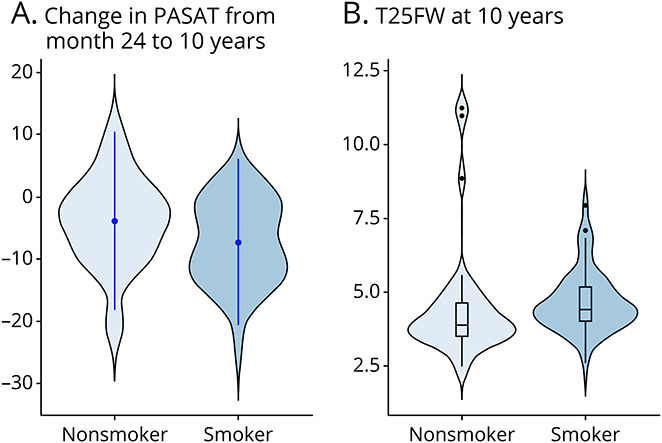
The width of the shaded area represents the proportion of observations for (A) change in PASAT score from month 24 to 10 years (point range represents the mean and SD) and (B) T25FW test score at 10 years (box plots represent the median and IQR, with the whiskers representing the distribution of observations within x1.5 of the IQR). IQR = interquartile range; PASAT = paced auditory serial addition test; T25FW = timed 25-foot walk.
Smoking Status and Long-term MRI and Clinical Outcome Measures
The results from the linear mixed-model investigating the relationship between smoking and long-term MRI and clinical measures are shown in Table 3 (smoking defined by cotinine levels) and supplemental eTable 4, links.lww.com/NXI/A728 (smoking defined by patient self-reporting). Smoking defined by cotinine level was associated with lower total WM volume (β = −21.74, p = 0.039) after 10 years and with higher total logT2 lesion volume (β = 0.22, p = 0.011). Similar results were found for smoking defined by patient self-reporting (eTable 4), additionally associated with lower deep GM volume (β = −2.35, p = 0.049) after 10 years. There were no significant associations between smoking and clinical disability when defined by cotinine levels (Table 3), but when defined by patient self-reporting, smoking was associated with a higher score on the logT25FW test (β = 0.050, p = 0.039) after 10 years and a larger decrease in PASAT scores (β = −3.58, p = 0.029) (eTable 4).
Table 3.
Effect of Smoking Status (Defined by Cotinine Level) on MRI and Clinical Measures at the 10-Year Follow-up Visit and Change in Clinical Measures Between Month 24 and the 10-Year Follow-up Visit

Dose-Effect Relationship on Long-term MRI and Clinical Outcome Measures
The results from the mixed-effect model assessing the relation between mean cotinine levels in smokers (defined by cotinine level) and MRI and clinical outcome measures are shown in supplemental eTable 5, links.lww.com/NXI/A728. In a bivariate model, higher cotinine levels were significantly associated with lower mean cortical thickness, but not after adjusting for age, sex, VD, BL EDSS, and time from diagnosis.
Discussion
We found that patients with MS who smoked had lower total WM and deep GM volumes and higher T2 lesion volumes after 10 years. Smokers also accumulated more disability and incurred a larger decrease in attention scores measured by the T25FW and PASAT test, respectively. The results obtained by defining smokers by cotinine levels collected during the initial 2-year period were highly comparable with those obtained when defining smokers by retrospective patient self-reporting. Furthermore, the associations were still significant when correcting for vascular risk factors and established cardiovascular disease. These findings suggest that smoking has a negative long-term influence on prognosis and disease progression in patients with MS.
The association between smoking and higher lesion load is partly in line with previous research,1,7 supporting the notion that smoking could heighten inflammatory activity.3 However, smoking and increased lesional activity have not been consistently related,9,10 as also shown in a previous study investigating the same patient cohort as in this current work. In the previous study, no association was found between tobacco use (defined by cotinine levels) and the occurrence of new or enlarging lesions during the trial period of 24 months.10 The discrepant findings in this same study population may be a result of the different outcome measures used, that is, lesion volumes vs the less sensitive dichotomous measure of new or expanding lesions present or not present, especially considering the more limited follow-up time of 2 years. Moreover, it is unknown how smoking may affect pathologic processes within the occurring lesions. Lesions with persistent subtle inflammation, called chronic active or smoldering lesions, are associated with low-grade BBB leakage,31 higher atrophy rates,32 and have been shown to develop in patients with RRMS and slowly expand over years.33 In this study, we were unable to investigate whether smokers had a higher fraction of smoldering lesions, but testing that hypothesis could provide insight to the discrepant associations found for the occurrence of new lesions and total lesion volume and to the overall worse prognosis seen in smoking patients with MS.3
After 10 years, we found that deep GM and total WM volume were lower in patients who smoked. Previous longitudinal studies on smoking/nonsmoking patients with MS have mainly assessed whole-brain atrophy and have not reported consistent results.1,7,9 Cross-sectional studies assessing GM atrophy showed a similar lack of consensus.6,11,13 In studies investigating non-MS populations, smoking is associated with atrophy most evidently in the frontal and temporal lobe, cingulate gyrus, and the cerebellum33,34 while the associations with subcortical GM are more variable.33,34 Furthermore, neither studies on MS nor those on non-MS populations have found smoking to be related to lower WM volume.6,7,11,13,33,34 In early MS, atrophy in the deep GM has previously been shown to develop at a relatively high rate35,36 compared with other GM regions, and to be closely related to WM lesions.36,37 Although the causal mechanisms are still not sufficiently clear, a spatiotemporal relationship between WM lesions and subsequent deep GM atrophy progression through neuroaxonal degradation38 seems likely, explaining at least part of the neurodegenerative process. Together with the higher lesion volume, our findings of lower deep GM and total WM volumes in smoking patients with MS may suggest that the pathologic changes are driven by increased inflammatory damage in the WM, followed by secondary degeneration in regions either consisting of WM or highly connected through WM tracts.39 The hypothesis that the main neurodegenerative pathway in MS is driven by neuroaxonal injury has also been proposed in a recent study, which observed higher levels of neurofilament light chain in smokers.40
Although not significant after correcting for age, sex, vascular risk factors, BL EDSS, and time since diagnosis, our initial bivariate analysis found that higher cotinine levels in smokers were associated with lower cortical thickness after 10 years. This is similar to previous literature on non-MS populations, finding a dose-dependent relationship between smoking and cortical atrophy.34,41 The different smoking-associated atrophy patterns seen when comparing smoking and nonsmoking patients with MS (lower deep GM and total WM volume), and cotinine levels in smoking patients (lower cortical thickness), may suggest that smoking affects atrophy progression both through MS-specific disease mechanisms and directly in a dose-dependent manner. It is, however, important to highlight that our sample size for the dose-effect analyses was small and that the current data did not allow us to investigate these possible mechanisms directly.
At the 10-year follow-up visit, smokers had a higher degree of walking impairment measured by the T25FW test, indicating higher risk of disability accrual. The lack of association between smoking defined by cotinine levels and change in EDSS score over the follow-up has previously been reported in this current patient population.15 In our study, we confirmed this finding, for both definitions of smoking. The results are partly in line with previous research, much of which reported a relation between smoking and higher EDSS or Multiple Sclerosis Severity Score in cross-sectional analyses,1,6 but more variably longitudinally.1,9,40,42,43 A possible cause of the inconsistent results for EDSS is the known low sensitivity to change for this measurement,44 suggesting that more targeting tests should be used to capture disability progression in specific functions. Overall, the associations with disability accrual were modest in our study, and after correcting for relevant covariates, it was only found for one of the 2 definitions of smoking (patient self-reporting). In future studies, these longitudinal relations should be further investigated in larger patient populations.
In our study, patients who smoked also had a higher decrease in the PASAT score from month 24 to the 10-year follow-up. This finding is in line with previous studies, where smokers tended to perform worse cognitively.40,45 Attention, information processing, and working memory are cognitive domains commonly affected in patients with MS,46 but impairment on these domains has also been shown in smoking non-MS populations.34 This may imply that smoking patients with MS are at additive risk of developing cognitive impairment, through mechanisms specific to both MS and smoking. This suggests an important clinical consequence to minimize long-term GM atrophy and clinical decline; people with MS who smoke should be encouraged and assisted to quit smoking.
Our study is not without limitations. Brain atrophy and lesion load were measured cross-sectionally at the 10-year follow-up visit. In future research, long-term measurements should be corrected for values at baseline if available, or be investigated by longitudinal analyses, to conclude on atrophy progression in smoking patients with MS.
Obtaining volume and cortical thickness measures in postcontrast images by FreeSurfer is not the standard approach. Recent work using data from a subgroup of this patient cohort has demonstrated excellent consistency between values obtained from precontrast and postcontrast 3D T1-weighted images,28 although minor to moderate segmentation errors, especially in the temporal lobe were more common in postcontrast images. In this current study, we did not apply manual corrections for these errors, and the volume of the temporal lobe was excluded from the total GM volume to limit the possible bias introduced by the larger variability in measurements extracted from this region. In future studies, corrections of these segmentation errors should be considered, especially if evaluating regional atrophy measures.
Owing to its stability in plasma over time (half-life of approximately 20 hours), cotinine has become the preferred biomarker to quantify long-term nicotine exposure.8 However, the use of cotinine levels as a proxy for smoking is potentially biased by other sources of nicotine. This is an important limitation because neither nicotine nor smokeless tobacco have shown to induce inflammation in MS19 or increase the risk of the disease.18 In our study, patients who at the 10-year follow-up reported use of smokeless tobacco (e.g., snuff) exclusively (4 patients) were, therefore, classified as nonsmokers, regardless of their measured cotinine levels. Furthermore, the results obtained by defining smoking by cotinine levels were comparable with those using patient self-reporting to define smoking habits. The associations with MRI atrophy and clinical measures were somewhat stronger when using the definition based on patient self-reporting, most notably for clinical disability. This may be explained by this definition also capturing patients who smoked regularly in time periods during the follow-up, after the 2 years of the clinical trial. In this study, serum cotinine measurements were not available after the first 2 years of follow-up or at the 10-year follow-up visit. In future works, the effect of cotinine levels measured regularly over a longer follow-up period should be explored, especially to determine the effect of smoking duration and cessation. Nevertheless, the overall comparable results suggest that serum cotinine levels provide an objective and reliable option for defining smoking habits and especially to investigate dose-dependent relationships.
Several comorbid conditions may independently influence brain tissue changes (including gray and WM atrophy and localized WM hyperintensities)20 and can be caused or exacerbated by smoking.21 We attempted to limit the effect of these complex interrelations by correcting for vascular risk factors and established cardiovascular and cerebrovascular disease. MS disease–related factors, such as disease-modifying therapies, are also likely to affect brain atrophy. In this data set, however, this was not possible to statistically consider because the patients had used a variety of therapies at different times and duration over the follow-up.
Smoking was associated with lower deep GM and total WM volume and higher T2 lesion volume after 10 years in patients with RRMS. Patients who smoked had higher physical and cognitive disability accrual, measured by the T25FW and PASAT test, respectively. The findings suggest that smoking patients with MS should be advised and offered aid in smoking cessation as early as possible in the disease course.
Acknowledgment
The authors thank the OFAMS study group and the patients who participated in the study.
Glossary
- BBB
blood-brain barrier
- BL
baseline
- EDSS
Expanded Disability Status Scale
- eTIV
estimated total intracranial volume
- GM
gray matter
- MS
multiple sclerosis
- PASAT
paced auditory serial addition test
- RRMS
relapsing-remitting MS
- SPSS
Statistical Product and Service Solutions
- T25FW
timed 25-foot walk test
- VD
vascular-disease
- WM
white matter
Study Funding
The authors report no targeted funding.
Disclosure
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. I.A. Lie has received research grants from the Meltzer Research Fund, Gerda Meyer Nyquist Guldbrandson & Gert Meyer Nyquists Legat, and the Independent Order of Odd Fellows; K. Wesnes has received unrestricted research grants from Novartis and Biogen, research grant from the Independent Order of Odd Fellows, and speaker honoraria from Biogen; S.S. Kvistad has received unrestricted research grants from Novartis and Biogen; I. Brouwer has received research support from Merck KGaA, Novartis, and Teva; S. Wergeland has received speaker honoraria from and served on scientific advisory boards for Biogen, Janssen-Cilag, Sanofi, and Novartis; T. Holmøy has received speaker honoraria, research support/grants and participated in clinical trials for Biogen, Merck, Sanofi, Bristol Myers Squibb, Roche and Novartis, is member of the scientific board of the Norwegian MS society, and has received financial support from the Research Council of Norway (grant #250864); R. Midgard has served on scientific advisory boards for Novartis Norway and Merck and received travel funding and/or speaker honoraria from Biogen, Novartis, and Sanofi Genzyme; A. Bru reports no disclosures relevant to the manuscript; A. Edland has received speaker honoraria from Biogen, Merck, Sanofi, and Novartis; R. Eikeland has received speaker honoraria from Novartis; S. Gosal reports no disclosures relevant to the manuscript; H.F. Harbo has received speaker honoraria from Biogen, Sanofi-Aventis, Merck, Novartis, and Roche; G. Kleveland reports no disclosures relevant to the manuscript; Y.S. Sørenes reports no disclosures relevant to the manuscript; N. Øksendal has received speaker honoraria from Biogen, participated in clinical trials for Biogen and Sanofi-Aventis and has served on a scientific advisory board for Novartis; F. Barkhof has received compensation for steering/safety committee, activities and consulting services from Roche, Biogen, Merck, Combinostics, Janssen, and IXICO. He is cofounder and shareholder of Queen Square Analytics LTD; H. Vrenken has received research grants from Pfizer, Merck Serono, Novartis and Teva, speaker honoraria from Novartis, and consulting fees from Merck Serono. All funds were paid directly to his institution; K.M. Myhr has received unrestricted research grants to his institution, scientific advisory board, and speaker honoraria from Biogen, Sanofi, Merck, Novartis, and Roche and has participated in clinical trials organized by Biogen, Merck, Novartis, and Roche; L. Bø has received unrestricted research grants to his institution and/or scientific advisory board or speaker honoraria from Almirall, Biogen, Genzyme, Merck, Novartis, Roche, and Teva and has participated in clinical trials organized by Biogen, Merck, Novartis, Roche, and Genzyme; Ø. Torkildsen has received research grants and speaker honoraria from Biogen, Roche, Novartis, Merck, and Sanofi and has participated in clinical trials organized by Merck and Sanofi. Go to Neurology.org/NN for full disclosures.
References
- 1.Healy BC, Ali EN, Guttmann CR, et al. Smoking and disease progression in multiple sclerosis. Arch Neurol. 2009;66(7):858-864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Degelman ML, Herman KM. Smoking and multiple sclerosis: a systematic review and meta-analysis using the Bradford Hill criteria for causation. Mult Scler Relat Disord. 2017;17:207-216. [DOI] [PubMed] [Google Scholar]
- 3.Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: a review. JAMA Neurol. 2020;77(2):245-253. [DOI] [PubMed] [Google Scholar]
- 4.Wingerchuk DM. Smoking: effects on multiple sclerosis susceptibility and disease progression. Ther Adv Neurol Disord. 2011;5(1):13-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Petersen ER, Søndergaard HB, Laursen JH, et al. Smoking is associated with increased disease activity during natalizumab treatment in multiple sclerosis. Mult Scler. 2018;25(9):1298-1305. [DOI] [PubMed] [Google Scholar]
- 6.Zivadinov R, Weinstock-Guttman B, Hashmi K, et al. Smoking is associated with increased lesion volumes and brain atrophy in multiple sclerosis. Neurology. 2009;73(7):504-510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Horakova D, Zivadinov R, Weinstock-Guttman B, et al. Environmental factors associated with disease progression after the first demyelinating event: results from the multi-center SET study (P05.134). Neurology. 2013;80(7 suppl):P05134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Florescu A, Ferrence R, Einarson T, Selby P, Soldin O, Koren G. Methods for quantification of exposure to cigarette smoking and environmental tobacco smoke: focus on developmental toxicology. Ther Drug Monit. 2009;31(1):14-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Munger KL, Fitzgerald KC, Freedman MS, et al. No association of multiple sclerosis activity and progression with EBV or tobacco use in BENEFIT. Neurology. 2015;85(19):1694-1701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kvistad S, Myhr KM, Holmøy T, et al. No association of tobacco use and disease activity in multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. 2016;3(4):e260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kappus N, Weinstock-Guttman B, Hagemeier J, et al. Cardiovascular risk factors are associated with increased lesion burden and brain atrophy in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2016;87(2):181-187. [DOI] [PubMed] [Google Scholar]
- 12.Durhan G, Diker S, Has AC, et al. Assessment of the effect of cigarette smoking on regional brain volumes and lesion load in patients with clinically isolated syndrome. Int J Neurosci. 2016;126(9):805-811. [DOI] [PubMed] [Google Scholar]
- 13.Graetz C, Groger A, Luessi F, et al. Association of smoking but not HLA-DRB1*15:01, APOE or body mass index with brain atrophy in early multiple sclerosis. Mult Scler. 2019;25(5):661-668. [DOI] [PubMed] [Google Scholar]
- 14.Torkildsen O, Wergeland S, Bakke S, et al. omega-3 fatty acid treatment in multiple sclerosis (OFAMS Study): a randomized, double-blind, placebo-controlled trial. Arch Neurol. 2012;69(8):1044-1051. [DOI] [PubMed] [Google Scholar]
- 15.Wesnes K, Myhr KM, Riise T, et al. Low vitamin D, but not tobacco use or high BMI, is associated with long-term disability progression in multiple sclerosis. Mult Scler Relat Disord. 2021;50:102801. [DOI] [PubMed] [Google Scholar]
- 16.Connor Gorber S, Schofield-Hurwitz S, Hardt J, Levasseur G, Tremblay M. The accuracy of self-reported smoking: a systematic review of the relationship between self-reported and cotinine-assessed smoking status. Nicotine Tob Res. 2009;11(1):12-24. [DOI] [PubMed] [Google Scholar]
- 17.Biochemical verification of tobacco use and cessation. Nicotine Tob Res. 2002;4(2):149-159. [DOI] [PubMed] [Google Scholar]
- 18.Hedström AK, Bäärnhielm M, Olsson T, Alfredsson L. Tobacco smoking, but not Swedish snuff use, increases the risk of multiple sclerosis. Neurology. 2009;73(9):696-701. [DOI] [PubMed] [Google Scholar]
- 19.Jiang W, St-Pierre S, Roy P, Morley BJ, Hao J, Simard AR. Infiltration of CCR2+Ly6Chigh proinflammatory monocytes and neutrophils into the central nervous system is modulated by nicotinic acetylcholine receptors in a model of multiple sclerosis. J Immunol. 2016;196(5):2095-2108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Friedman JI, Tang CY, de Haas HJ, et al. Brain imaging changes associated with risk factors for cardiovascular and cerebrovascular disease in asymptomatic patients. JACC Cardiovasc Imaging. 2014;7(10):1039-1053. [DOI] [PubMed] [Google Scholar]
- 21.Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: an update. J Am Coll Cardiol. 2004;43(10):1731-1737. [DOI] [PubMed] [Google Scholar]
- 22.Schmidt P, Gaser C, Arsic M, et al. An automated tool for detection of FLAIR-hyperintense white-matter lesions in Multiple Sclerosis. NeuroImage. 2012;59(4):3774-3783. [DOI] [PubMed] [Google Scholar]
- 23.FMRIB Software Library. fmrib.ox.ac.uk/fsl. [Google Scholar]
- 24.Battaglini M, Jenkinson M, De Stefano N. Evaluating and reducing the impact of white matter lesions on brain volume measurements. Hum Brain Mapp. 2012;33(9):2062-2071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.FreeSurfer. surfer.nmr.mgh.harvard.edu/. [Google Scholar]
- 26.Fischl B. FreeSurfer. Neuroimage. 2012;62(2):774-781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. NeuroImage. 1999;9(2):179-194. [DOI] [PubMed] [Google Scholar]
- 28.Lie IA, Kerklingh E, Wesnes K, et al. The effect of gadolinium-based contrast-agents on automated brain atrophy measurements by FreeSurfer in patients with multiple sclerosis. Eur Radiol. 2022;32(5):3576-3587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Desikan RS, Ségonne F, Fischl B, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. NeuroImage. 2006;31(3):968-980. [DOI] [PubMed] [Google Scholar]
- 30.Hochmeister S, Grundtner R, Bauer J, et al. Dysferlin is a new marker for leaky brain blood vessels in multiple sclerosis. J Neuropathol Exp Neurol. 2006;65(9):855-865. [DOI] [PubMed] [Google Scholar]
- 31.Absinta M, Sati P, Masuzzo F, et al. Association of chronic active multiple sclerosis lesions with disability in vivo. JAMA Neurol. 2019;76(12):1474-1483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dal-Bianco A, Grabner G, Kronnerwetter C, et al. Long-term evolution of multiple sclerosis iron rim lesions in 7 T MRI. Brain. 2021;144(3):833-847. [DOI] [PubMed] [Google Scholar]
- 33.Elbejjani M, Auer R, Jacobs DR, et al. Cigarette smoking and gray matter brain volumes in middle age adults: the CARDIA Brain MRI sub-study. Transl Psychiatry. 2019;9(1):78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gallinat J, Meisenzahl E, Jacobsen LK, et al. Smoking and structural brain deficits: a volumetric MR investigation. Eur J Neurosci. 2006;24(6):1744-1750. [DOI] [PubMed] [Google Scholar]
- 35.Eshaghi A, Prados F, Brownlee WJ, et al. Deep gray matter volume loss drives disability worsening in multiple sclerosis. Ann Neurol. 2018;83(2):210-222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bergsland N, Horakova D, Dwyer MG, et al. Subcortical and cortical gray matter atrophy in a large sample of patients with clinically isolated syndrome and early relapsing-remitting multiple sclerosis. AJNR Am J Neuroradiol. 2012;33(8):1573-1578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Henry RG, Shieh M, Amirbekian B, Chung S, Okuda DT, Pelletier D. Connecting white matter injury and thalamic atrophy in clinically isolated syndromes. J Neurol Sci. 2009;282(1-2):61-66. [DOI] [PubMed] [Google Scholar]
- 38.Klaver R, De Vries HE, Schenk GJ, Geurts JJ. Grey matter damage in multiple sclerosis: a pathology perspective. Prion. 2013;7(1):66-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Dendrou CA, Fugger L, Friese MA. Immunopathology of multiple sclerosis. Nat Rev Immunol. 2015;15(9):545-558. [DOI] [PubMed] [Google Scholar]
- 40.Cortese M, Munger KL, Martínez-Lapiscina EH, et al. Vitamin D, smoking, EBV, and long-term cognitive performance in MS. Neurology. 2020;94(18):e1950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Karama S, Ducharme S, Corley J, et al. Cigarette smoking and thinning of the brain's cortex. Mol Psychiatry. 2015;20(6):778-785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Manouchehrinia A, Tench CR, Maxted J, Bibani RH, Britton J, Constantinescu CS. Tobacco smoking and disability progression in multiple sclerosis: United Kingdom cohort study. Brain. 2013;136(pt 7):2298-2304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Koch M, van Harten A, Uyttenboogaart M, De Keyser J. Cigarette smoking and progression in multiple sclerosis. Neurology. 2007;69(15):1515-1520. [DOI] [PubMed] [Google Scholar]
- 44.Meyer-Moock S, Feng YS, Maeurer M, Dippel FW, Kohlmann T. Systematic literature review and validity evaluation of the expanded disability status scale (EDSS) and the multiple sclerosis functional composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014;14:58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ozcan ME, Ince B, Bingöl A, et al. Association between smoking and cognitive impairment in multiple sclerosis. Neuropsychiatr Dis Treat. 2014;10:1715-1719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Chiaravalloti ND, DeLuca J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008;7(12):1139-1151. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data not provided within this article may be shared (anonymized) by request from a qualified investigator.