

ABSTRACT
Primary colorectal lymphoma is a rare neoplasm. We report the case of a fistula between a diffuse large B-cell lymphoma of the sigmoid colon and an ovarian teratoma. An emergent laparotomy for an acute abdomen in a 90-year-old woman was performed. A pelvic mass of 12 × 9 cm fistulized in the left colon was found with the presence of gas and free liquid within the abdomen. This is an extremely rare condition, and as far as we know, no cases of a fistula between a large B-cell colonic lymphoma and an ovarian teratoma are present in the literature.
INTRODUCTION
Primary colorectal lymphoma is a rare neoplasm, accounting for only 0.2%–0.6% of all colon cancers and 15%–20% of gastrointestinal lymphomas.1 Of note, perforation due to B-cell lymphoma is more common in gastric and splenic forms, whereas, in colonic forms, bleeding rather than perforation is the most common complication.2 We present a rare case of an acute abdomen caused by a fistula between a diffuse large B-cell lymphoma (DLBCL) of the sigmoid colon and an ovarian teratoma.
CASE REPORT
A 90-year-old woman was referred to the emergency department of our institute for severe abdominal pain associated with nausea and fever. However, no relevant comorbidities were reported. On physical examination, she presented with tachycardia (120 beats per minute) and hypotension with a blood pressure of 90/62 mm Hg. Signs of diffuse peritonitis with marked wall rigidity were appreciable on examination of the abdomen. Digital rectal examination was unremarkable, and during the laboratory examinations, a leukocytosis was noticed (15.4 × 109/L). Assuming there was intestinal perforation, an abdominopelvic computed tomography scan was promptly performed. The scan revealed the presence of gas and free liquid within the abdomen. In addition, a pelvic mass of 12 × 9 cm was found, raising the possibility of a dermoid cyst with possible fistulization to the sigmoid colon (Figures 1 and 2). Owing to the septic status of the patient, an emergent laparotomy was performed quickly. A ruptured left ovarian cyst measuring 16 × 10 cm fistulized within the colon with fecal peritonitis was found intraoperatively (Figure 3). The cyst contained hair and teeth, and part of the cystic wall was adherent to the rectosigmoid junction (Figure 4). Excision of the cyst en bloc with the left colon, left ovary, and left tube was performed (Hartmann procedure and left salpingo-oophorectomy).
Figure 1.
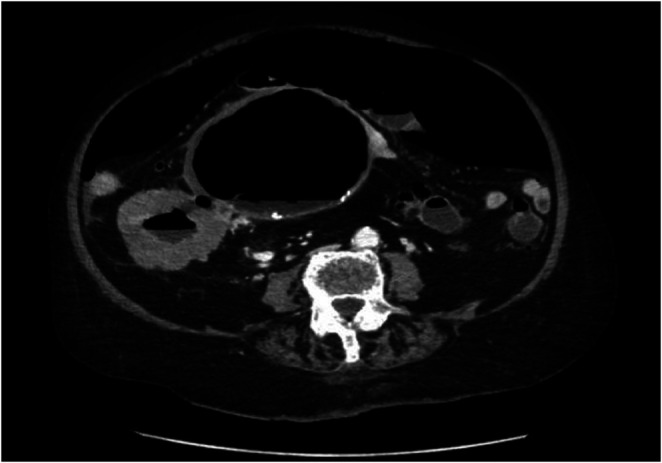
Transverse computed tomography scan image: pneumoperitoneum and close adhesion of the colon and the ovarian cyst.
Figure 2.

Coronal computed tomography scan image: fistulization between the dislocated sigmoid colon and the ovarian teratoma.
Figure 3.

Intraoperative findings.
Figure 4.

Histological specimens.
The postoperative course with the administration of fluids and antibiotic therapy was free of relevant complications, blood tests returned to normal, and the patient restarted the oral intake on the second postoperative day, with colostomy canalization on the third postoperative day.
During the macroscopic examination, a whitish and soft mass involving the colonic wall with mucosal ulceration and serosal involvement was described. Microscopic examination showed a neoplastic lesion constituted by a lymphoid population, medium-to-large in size, in a diffuse pattern of growth, with necrosis and frequent mitosis involving the colonic wall. Immunohistochemical investigation showed immunoreactivity for CD20, BCL-2, BCL6, and CD10 and negative staining for ALK, CD30, MUM1, CD138, and CiclinD1 (Figure 5). The cellular nuclei were positive for c-Myc (10%–15%), and the Ki67 proliferation index was 80%. In addition, histological diagnosis was DLBCL originating from the follicular germinal center. Regarding the ovarian lesion, a 15 cm mass was described. It constituted a fibrotic wall without an epithelial layer filled with adnexal and sebaceous material. The definitive diagnosis was of a mature cystic teratoma associated with edema and vascular congestion of the salpinx infiltrating a sigmoid colon affected by a primitive large B-cell lymphoma. The patient was discharged on the sixth postoperative day in a good clinical condition and reported to the oncologist. The patient was diagnosed as stage I lymphoma, and at a later colonoscopy, no other localizations were founded.
Figure 5.

Hematoxylin & eosin staining shows the neoplastic lesion involving the colonic wall. The other image shows the Ki67 proliferation index (magnification 400×).
DISCUSSION
DLBCL constitutes 30%–58% of non-Hodgkin lymphoma cases.3 Non-Hodgkin lymphoma can affect any organ; however, extranodal forms are predominantly detected in the gastrointestinal tract. A systematic review by Lightner et al found that the most frequent localization of non-Hodgkin lymphoma cases is the ileocecal region.4 The primary involvement of the gastrointestinal tract was defined according to Lewin et al, namely, the presence of gastrointestinal symptoms related to lymphoma with exclusive or predominant intestinal localization.5
To distinguish a primary colonic lymphoma from a diffuse form that secondarily involves the colon, Dawson criteria has also been established: (i) No palpable superficial enlarged lymph nodes at presentation, (ii) no enlargement of mediastinal nodes, (iii) a normal white cell count, (iv) exclusive regional nodes involvement at surgical exploration, and (v) the liver and spleen should not be involved.6
The case presented here is an exceptionally rare case of a complication involving 2 different synchronous tumors: A B-cell lymphoma of the colon, which is the third most common malignancy of the colon after carcinoma and carcinoid, and an ovarian teratoma, which accounts for approximately 1%–2% of ovarian cancer diagnoses.7 In their natural history, ovarian teratomas can develop different complications: Infection, torsion, rupture, and eventually fistulization; fistula formation between a benign ovarian dermoid cyst and the large bowel and/or the rectum has been reported in few cases.8,9
Surgery is the primary option for palliation of pain or in case of clinical condition that require emergency intervention, namely perforation, such in this case, obstruction and bleeding as well. In our case, owing to the septic condition, urgent surgery was performed. Cai et al published a case series, where in more than half of the patients, urgent surgical treatment was needed.10
In consideration of the possibility of a malignant tumor, an extended surgery could be performed, although because the literature allows us to say that the most frequent pathogenesis underlying fistulization is inflammation, sparing surgery may be more suitable.9 Nevertheless, in our clinical case, en bloc resection became necessary in lieu of the unclear diagnosis at the time of surgery.
Both perforations of a colonic primitive B-cell lymphoma and a teratoma with subsequent fistulization are extremely rare conditions, and as far as we know, no cases of a fistula between a large B-cell colonic lymphoma and an ovarian teratoma are present in the literature at the moment. Further reports are needed on these pathologies and above all on the complications, which, although rare, can be extremely serious.
DISCLOSURES
Author contributions: C. Accardo wrote the article and revised the literature. M. Ardu and FD Candido edited the article, revised the article for intellectual content, and approved the final article. M. Ardu is the article guarantor. G. Epifani, D. Cassini, F. Bono, and G. Baldazzi revised the article for intellectual content and approved the final article.
Financial disclosure: None to report. The authors declare that they have no conflict of interest.
Informed consent was obtained for this case report.
Contributor Information
Caterina Accardo, Email: accardocaterina@gmail.com.
Francesca Di Candido, Email: francescadicandido@gmail.com.
Gabriele Epifani, Email: ag.epifani@gmail.com.
Diletta Cassini, Email: diletta_cassini@yahoo.it.
Francesca Bono, Email: polletta.79@libero.it.
Gianandrea Baldazzi, Email: gbaldazzi@hotmail.com.
REFERENCES
- 1.Wong MT, Eu KW. Primary colorectal lymphomas. Colorectal Dis. 2006;8(7):586–91. [DOI] [PubMed] [Google Scholar]
- 2.Skube SJ, Arsoniadis EG, Sulciner ML, et al. Colorectal lymphoma: A contemporary case series. Dis Colon Rectum. 2019;62(6):694–702. [DOI] [PubMed] [Google Scholar]
- 3.Sant M, Allemani C, Tereanu C, et al. HAEMACARE working group. Incidence of hematologic malignancies in europe by morphologic subtype: Results of the HAEMACARE project. Blood. 2010;116(19):3724–34. [DOI] [PubMed] [Google Scholar]
- 4.Lightner AL, Shannon E, Gibbons MM, Russell MM. Primary gastrointestinal non-Hodgkin's lymphoma of the small and large intestines: A systematic review. J Gastrointest Surg. 2016;20(4):827–39. [DOI] [PubMed] [Google Scholar]
- 5.Lewin KJ, Ranchod M, Dorfman RF. Lymphomas of the gastrointestinal tract: A study of 117 cases presenting with gastrointestinal disease. Cancer. 1978;42(2):693–707. [DOI] [PubMed] [Google Scholar]
- 6.Dawson IM, Cornes JS, Morson BC. Primary malignant lymphoid tumours of the intestinal tract. Report of 37 cases with a study of factors influencing prognosis. Br J Surg. 1961;49:80–9. [DOI] [PubMed] [Google Scholar]
- 7.Veneris JT, Mahajan P, Frazier AL. Contemporary management of ovarian germ cell tumors and remaining controversies. Gynecol Oncol. 2020;158(2):467–75. [DOI] [PubMed] [Google Scholar]
- 8.Srisajjakul S, Prapaisilp P, Bangchokdee S. Imaging features of unusual lesions and complications associated with ovarian mature cystic teratoma. Clin Imaging. 2019;57:115–23. [DOI] [PubMed] [Google Scholar]
- 9.Kim JH, Chong GO, Chun DS, Park SY, Lee YH, Hong DG. Laparoscopic repair of a rectal fistula due to a benign ovarian dermoid cyst. Obstet Gynecol Sci. 2017;60(4):383–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cai S, Cannizzo F, Jr, Bullard Dunn KM, Gibbs JF, Czuczman M, Rajput A. The role of surgical intervention in non-Hodgkin's lymphoma of the colon and rectum. Am J Surg. 2007;193(3):409–12. discussion 412. [DOI] [PubMed] [Google Scholar]