

PURPOSE
Local researchers must be engaged in research conducted in their populations. However, local authors from low- and middle-income countries are often under-represented in global health journals. This report aims to assess and describe the representation of authors in the Journal of Clinical Oncology Global Oncology (JCO GO).
METHODS
This retrospective cross-sectional study describes data from JCO GO articles published between October 2015 and March 2020. Data were collected on studied countries, authorship position, classified as first, middle, or last, and country of authors' institutional affiliations. Countries were then categorized on the basis of their World Bank region and income classifications. We describe aggregate authorship distribution and distribution by region and income classification. Additionally, we explore the relationships between author's country and studied country.
RESULTS
Of the 608 articles identified, 420 (69.1%) studied a single country population. Although articles represented studies from all World Bank regions, the sub-Saharan Africa (SSA) region accounted for the highest number (n = 145; 34.5%). In all other regions except SSA, most of the first (66.7%-100%) and last authors (56.6%-95.2%) had primary institutional affiliations based in the same region as the studied country. However, among articles about SSA countries, SSA first authors (n = 65; 44.8%) and last authors (n = 59; 40.7%) were under-represented. In fact, there were more North American first (n = 74; 51.0%) and last authors (n = 72; 49.6%) than SSA authors. There was higher SSA representation among middle authors (n = 97; 68.8%) in studies from the region. A similar trend was also noted with the under-representation of authors from low-income compared with high-income countries.
CONCLUSION
SSA authors are under-represented in global oncology articles. Concerted strategies are needed to build local capacity, promote meaningful engagement, and foster equity.
INTRODUCTION
In global health, the pursuit of equity and inclusion is imperative in ensuring that research is impactful and locally applicable. However, the consequences of disparate power dynamics in global health research have been widely documented in history.1-6 Although there is greater recognition of the need for significant local engagement and a movement away from predatory research practices, true equity in global research remains elusive.
CONTEXT
Key Objective
African authors are often under-represented in global health journals. This report examines the distribution of authors in the Journal of Clinical Oncology Global Oncology (JCO GO), and describes representation by region and country income level.
Knowledge Generated
Although sub-Saharan Africa (SSA) was the most studied region, SSA first and last authors were under-represented, including on articles about SSA countries. Authors from low-income countries (LICs) were the minority overall, as well as on publications about LICs.
Relevance
Although there are ongoing efforts in research training and capacity building in SSA and other LICs, continued concerted work and accountability are needed from stakeholders, including academic journals, high-income country academic institutions, global funders, and LIC institutions, to increase engagement and representation of local researchers.
In 2009, the WHO Commission on Social Determinants of Health made recommendations for increasing health equity in research; one of these recommendations is to tackle the persistent inequitable distribution of power, money, and resources within health research.7 Analysis of authorship is an observational lens for examining inequities in medical academia. Assessing the composition of authors can be a window into several important metrics of equity, including the primary parties who conducted the research, the source of funding, level of engagement of the local studied population, and research capacity of the local research team. Several studies in many global health subdisciplines have examined authorship trends and have described imbalances in regional representation and country-income classification distribution.6,8,9
Persistent regional authorship disparities may partly reflect a country's economic resources and its corresponding ability to invest in health services and health care research. Authors from high-income countries (HICs), mainly English-speaking countries, are frequently more dominant contributors in global health literature. For example, Cash-Gibson et al10 observed that the United States, the United Kingdom, Canada, and Australia combined contributed approximately 70% of global health inequity research between 1966 and 2015. Conversely, authors from low-income countries (LICs) and particularly from sub-Saharan Africa (SSA) are substantially under-represented across global health literature even among studies conducted in their countries. For instance, Mbaye et al8 found that of 1,109 studies on six infectious diseases conducted in Africa in varied intervals between 1980 and 2016, < 50% had African first authorship. This under-representation has also been reported more recently among studies related to the COVID-19 pandemic. In an analysis of 94 articles related to COVID-19 in Africa published in 10 top-tier medical journals, Naidoo et al9 observed that 20% of the articles had no African authors, and 66.1% of authors were from outside Africa. These findings highlight persistent disparities in global health research on the basis of country of origin and income level.
Although these authorship trends have been described in other medical specialties, to our knowledge, there have been no comprehensive assessments of regional or income-based authorship representation, including of African representation in global oncology reported in the literature. Global oncology is a relatively newly recognized academic field. Therefore, it has the opportunity to learn lessons from the broader global health community.11 In this study, we describe geographic authorship distribution, representation, and equity in global oncology publications. We also focus on the SSA region, describing the degree of under-representation and exploring trends.
METHODS
This retrospective cross-sectional study describes publication data from the Journal of Clinical Oncology Global Oncology (JCO GO) published between the launch of the journal in October 2015 and March 2020. JCO GO was selected because it is a premier global oncology journal published by ASCO. The journal is open-access, with an international reach, and highlights research from resource-constrained settings.12 Publications are also made affordable through tiered charges for article processing, with the article-processing charges waived for authors from LICs.13
Articles were sourced through a PubMed search in April 2020. We identified 645 publications, of which 608 matched the inclusion criteria for article types. Included article types were original report, editorial, commentary, case report, special article, and review article. Correspondences, responses to the editor, and other miscellaneous articles were excluded. Forms coded using Research Electronic Data Capture were used to collect data from each article.14,15 Author information data collected included authorship position (first, middle, or last author), institutional author affiliation, location of authors' institution, and identification as a corresponding author. The primary country affiliation for the first and last author country was defined as the country of the individual author's primary affiliated institution. For the middle authors, it was defined as the country with the most affiliations among the middle authors. Data about an article included article type, date of publication, topic area, studied country or countries, country region and income classification according to the World Bank, and the total number of authors. The studied country or countries were assigned using the article content.
Countries were categorized on the basis of standard World Bank regions (East Asia and Pacific, Europe and Central Asia, Latin America and Caribbean, Middle East and North Africa, North America, South Asia, and SSA) and income classifications [LICs, lower-middle-income countries (LMICs), upper-middle-income countries (UMICs), and HICs].16
Through a dual data entry approach, H.T. and P.H. individually collected data from 65 (10%) randomly selected articles. The dual data entry approach yielded a discrepancy percentage of 7.5%, below a pre-established threshold of 10%. Discrepancies were discussed to further standardize the data collection protocol before proceeding with single data entry. Data were collected and analyzed data from April 2020 to April 2021.
Analysis and Visualization
Descriptive statistics were used to summarize aggregate data and proportions in groups. Relevant proportions and trends are presented in bar graphs and pie charts, where appropriate. Maps were generated with ArcMap 10.8 (Esri, Redlands, CA) using the Esri World Countries (Generalized) shapefile.17
Reporting and Ethical Considerations
The analysis was conducted on the basis of a priori protocol, designated as exempt by the Dana-Farber Cancer Institute Institutional Review Board. The report follows the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cross-sectional studies.18
RESULTS
We identified 608 articles that met the inclusion criteria. An aggregate summary of the publication profile is presented in the Data Supplement. Original reports constituted the highest number of articles (n = 377; 62.0%), whereas the remaining breakdown was as follows: special articles (n = 80; 13.2%), commentaries (n = 65; 10.7%), review articles (n = 43; 7.1%), case reports (n = 27; 4.4%), and editorials (n = 16; 2.6%).
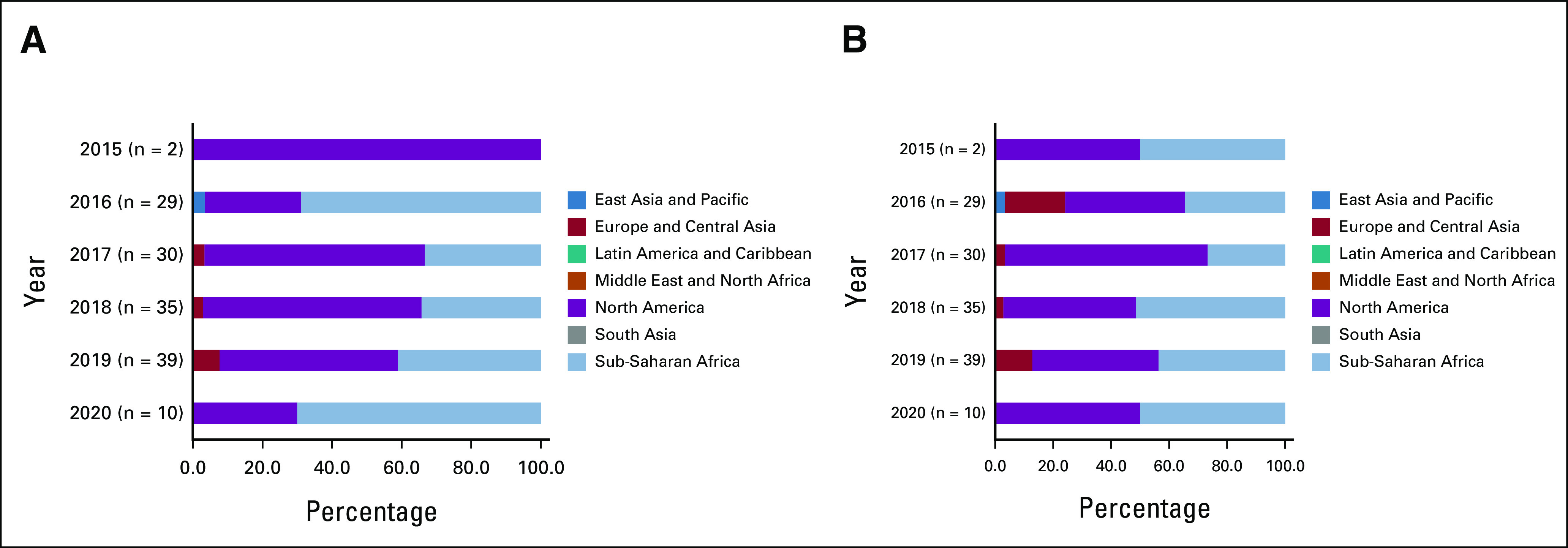
The geographic and regional distribution of articles is shown in Figure 1. The five countries with the highest number of publications included India (70), Brazil (43), and Nigeria (25), the United States (19), and Kenya, tied with South Africa (17). Although 66 countries were represented overall, most 40 (60.6%) had fewer than five publications (Data Supplement). SSA was the most studied region with 145 (34.5%) publications, followed by Latin America and the Caribbean with 90 (21.4%), and South Asia with 84 (20.0%; Data Supplement; Fig 2). The least studied regions were Europe and Central Asia, North America, and the Middle East and North Africa, with 9 (2.1%), 22 (5.2%), and 34 (8.1%) publications, respectively. When categorized on the basis of income level, the distribution of publications was 67 LICs (16.0%), 155 LMICs (36.9%), 135 UMICs (32.1%), and 63 HICs (15.0%). The yearly trends in studied articles by region and country income level are presented in Figure 3. The proportion of studies in LICs and LMICs exceeded 50% for each year from 2015 to 2019 but was 36.1% among the articles from early 2020.
FIG 1.
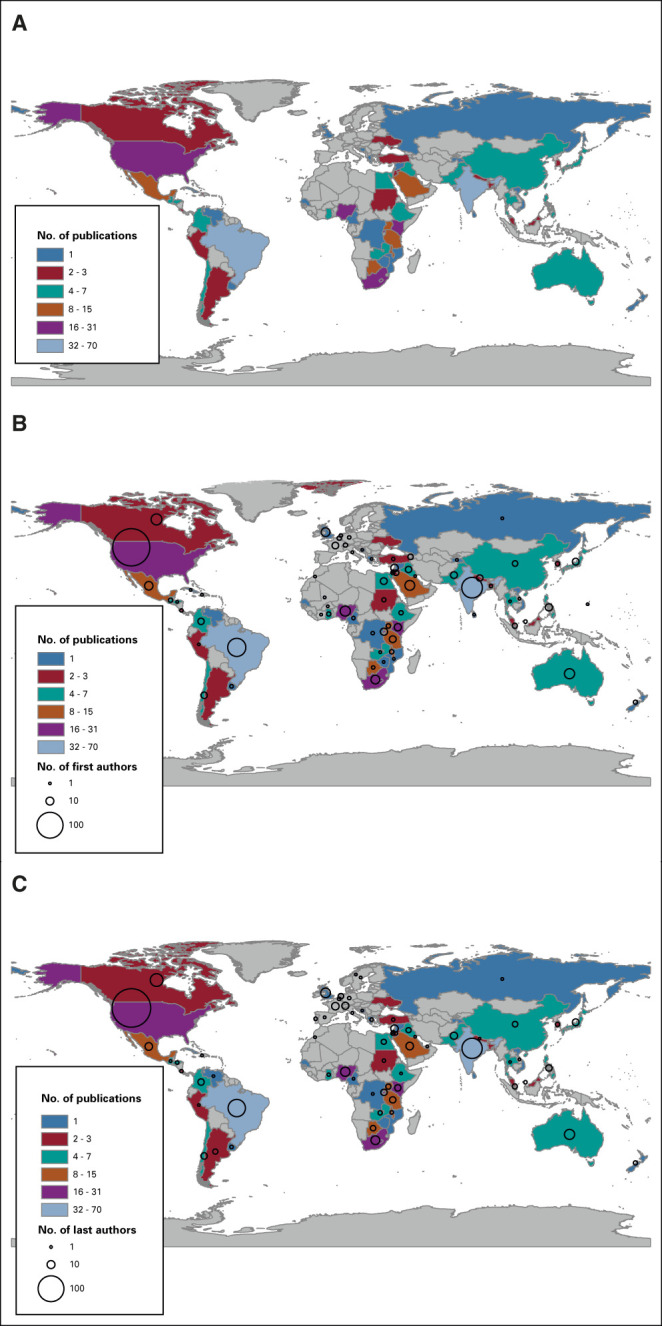
Study and author representation by number of (A) publications per country, (B) first authors per country, and (C) last authors per country. Includes only articles that studied a single country.
FIG 2.
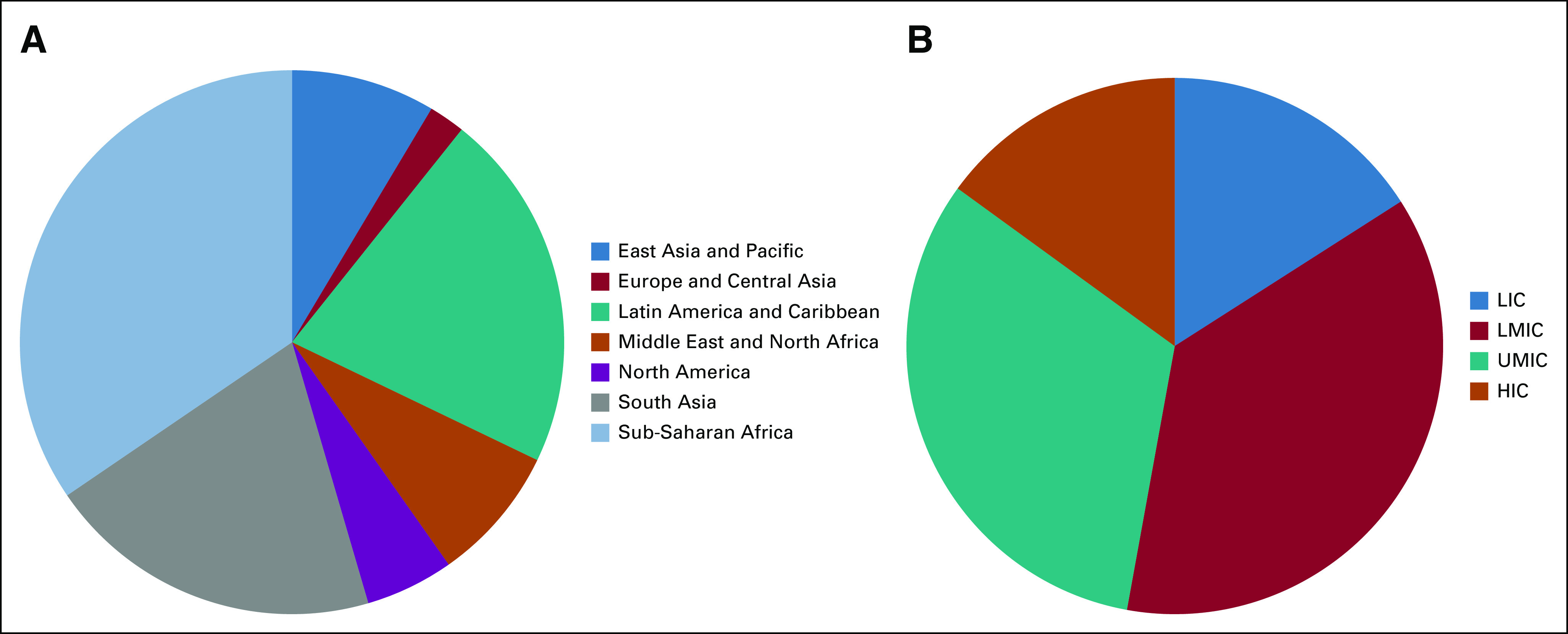
Number of publications by studied country on the basis of (A) region and (B) income (n = 420). Includes only articles that studied a single country. HIC, high-income country; LIC, low-income country; LMIC, lower-middle-income country; UMIC, upper-middle-income country.
FIG 3.
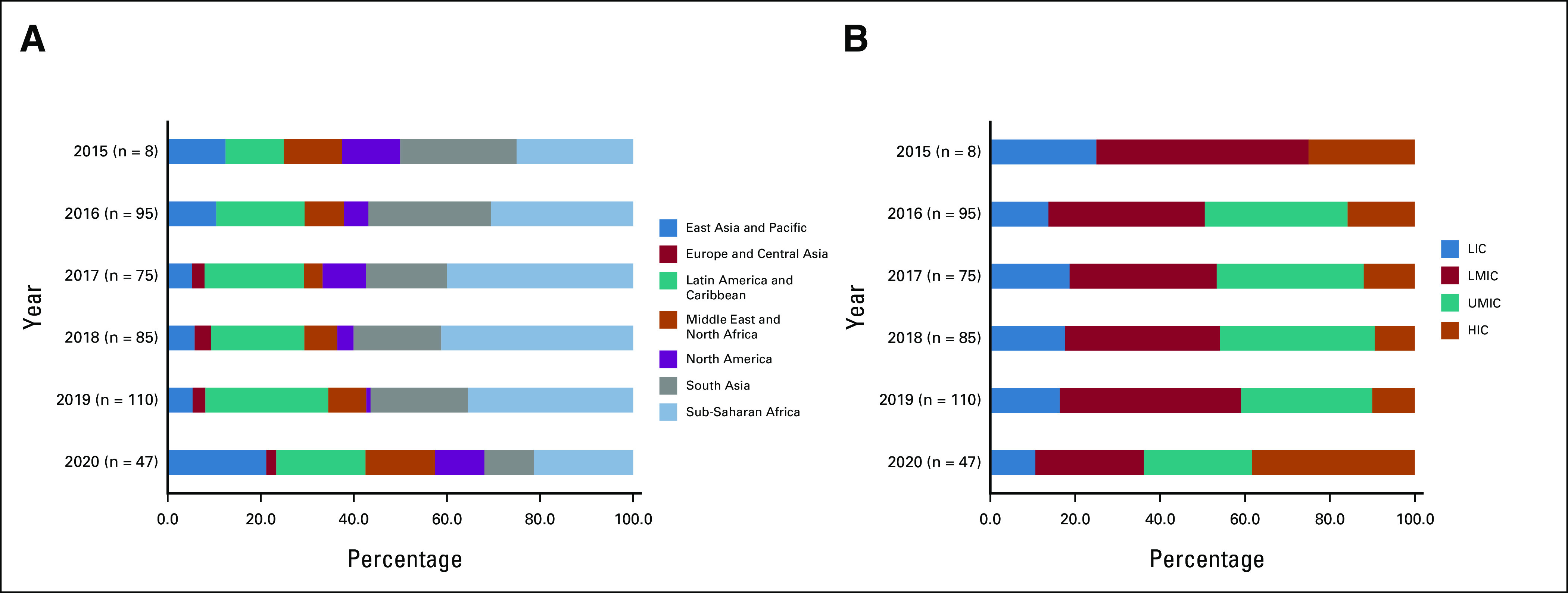
Yearly breakdown of percentage of articles by year on the basis of (A) region and (B) income. Includes only articles that studied a single country. HIC, high-income country; LIC, low-income country; LMIC, lower-middle-income country; UMIC, upper-middle-income country.
The geographic and regional distribution of authors is also shown in Figure 1. In aggregate, there were authors from 85 countries; first authors had primary institutional affiliations in 71 countries, whereas last authors had primary affiliations in 67 countries (Data Supplement). The countries with the highest number of first authors were the United States (n = 208; 34.2%), India (n = 63; 10.4%), and Brazil (n = 50; 8.2%). The same countries had the most last authors with 218 (36.8%), 60 (10.1%), and 44 (7.4%), respectively. Regional authorship distribution is presented in Figure 4. North American first authors accounted for the highest number (n = 226; 37.2%), whereas the contributions from other regions were Latin America and Caribbean (n = 89; 14.6%), South Asia (n = 79; 13.0%), SSA (n = 78; 12.8%), East Asia and Pacific (n = 52; 8.6%), Middle East and North Africa (n = 48; 7.9%), and Europe and Central Asia (n = 36; 5.6%; Fig 4A). Breakdown by country income level in the first author position revealed under-representation of LIC authors; HICs made up the majority of the first authors (n = 318; 52.3%), whereas LICs had the least (n = 37; 6.1%; Fig 4B). A similar trend was noted in the distribution of last authors by region and income level; HICs (n = 347; 58.6%)—particularly North America—accounted for the highest proportion, whereas LICs had the least (n = 22; 3.7%; Fig 4D).
FIG 4.
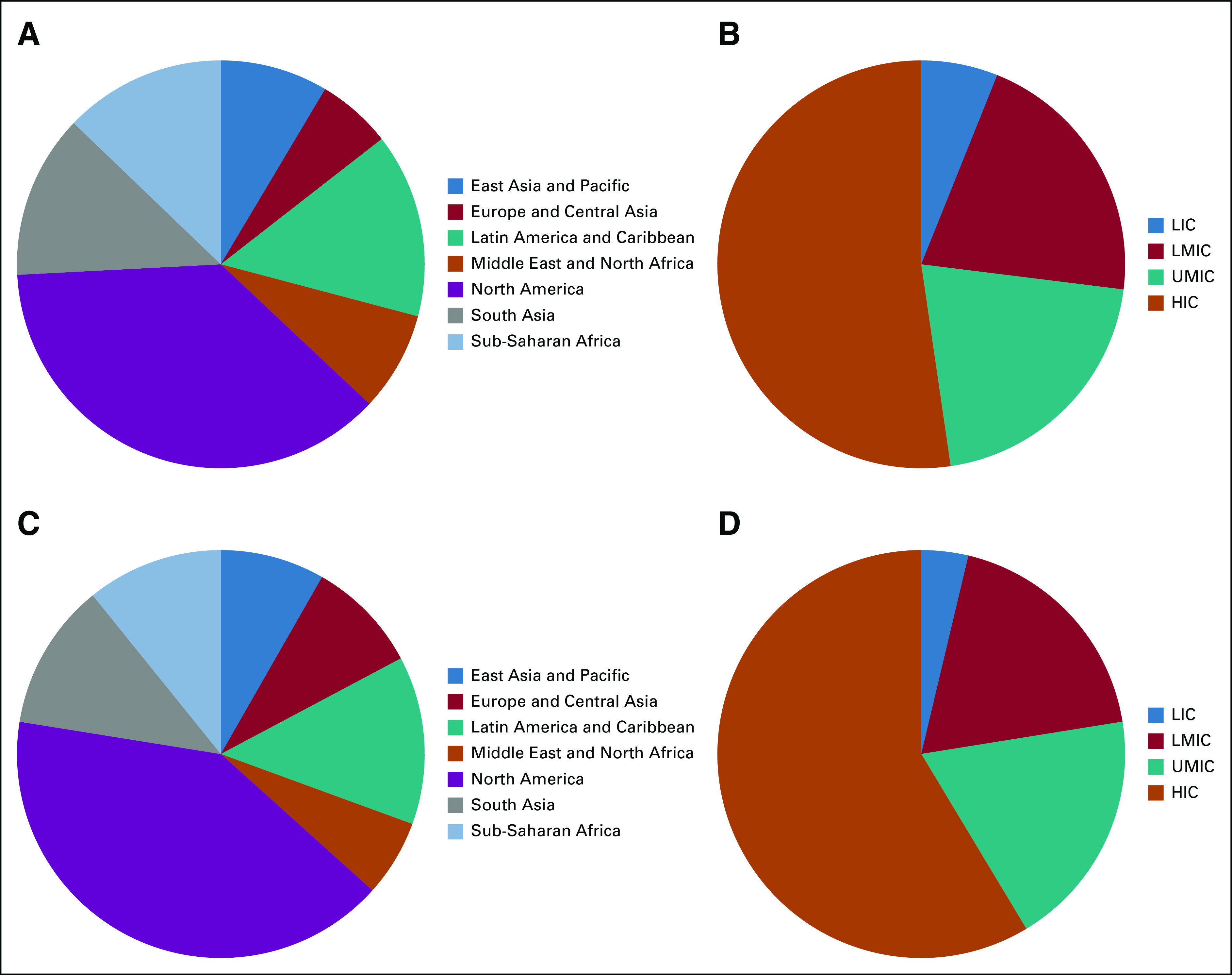
Number of authors by primary country: (A) first authors by primary country region, (B) first authors by primary country income, (C) last authors by primary country, and (D) last authors by primary country income. HIC, high-income country; LIC, low-income country; LMIC, lower-middle-income country; UMIC, upper-middle-income country.
A closer look at authorship distribution by author's region compared with the region of studied countries highlighted the under-representation of SSA authorship (Tables 1 and 2). Excluding SSA articles, there was a very close overlap between the region of the first authors and that of studied countries; first authors from the same region as the article were consistent in the majority, ranging from 66.7% to 100.0% (Table 1). However, there was a higher number of first authors from North America (n = 74; 51.0%) than SSA first authors (n = 65; 44.8%) on publications about SSA countries. We also observed a similar trend for the last authors. Excluding SSA articles, the proportion of last authors from the same region ranged from 55.6% to 95.2%; however, SSA last authors were a minority (n = 59; 40.7%) on SSA articles (Table 2). Again, there were more North American (n = 72; 49.6%) last authors on SSA articles than SSA last authors. Of note, SSA studies having an SSA last author were more likely to have an SSA first author compared with those with HIC last authors, 55.9% versus 36.5% (Data Supplement). There was a greater representation of SSA authors in the middle author position with higher concordance (n = 97; 68.8%) with the studied country region (Data Supplement).
TABLE 1.
First Author Distribution by Region Compared With Studied Country Region

TABLE 2.
Last Author Distribution by Region Compared With Studied Country Region

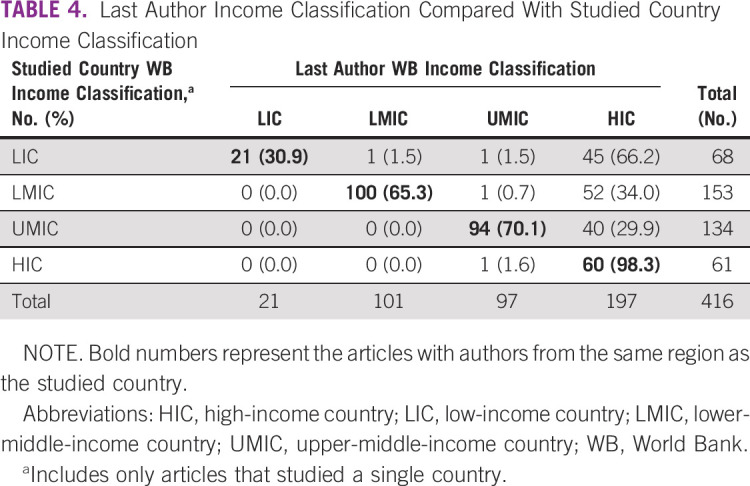
Similarly, the results comparing studied country income level and author country income level reveal under-representation of LIC and LMIC authors. In studies conducted in LICs, LIC first authors (n = 29; 43.3%) were in the minority compared with HIC first authors (n = 38; 56.7%; Table 3). LIC last authors were also in the minority on LIC studies, making up 21 (30.9%) compared with 45 (66.2%) from HICs (Table 4). Moreover, we observed a higher concordance of LIC middle authors (n = 39; 60.1%) with LIC publications (Data Supplement).
TABLE 3.
First Author Income Classification Compared With Studied Country Income Classification
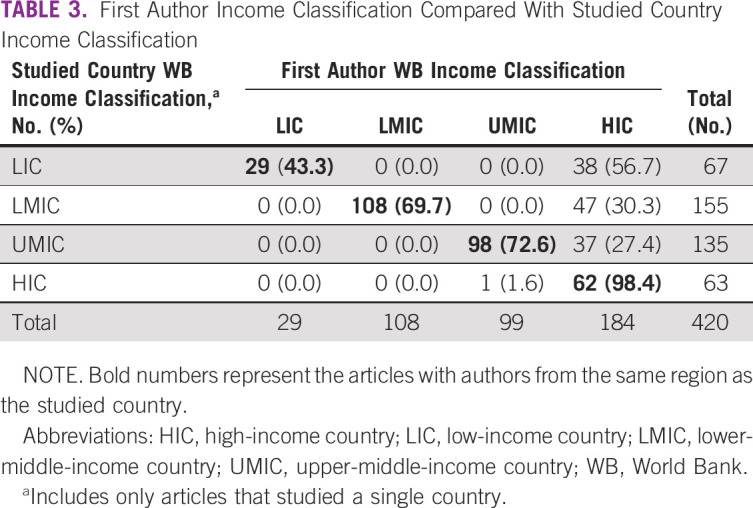
TABLE 4.
Last Author Income Classification Compared With Studied Country Income Classification
Yearly trends in authorship on studies on SSA countries are shown in Figure 5. There were only two eligible articles on SSA countries in 2015, both of which had North American first authors. The percentage of SSA first authors for the other years ranged from 33.3% to 70.0%, with no clear pattern. For the last authors, there appears to be a higher proportion of SSA last authors on SSA articles among articles published from 2018 to 2020 (n = 40; 47.6%), compared with articles from 2015 to 2017 (n = 19; 31.2%).
FIG 5.
Author region on studies from SSA by year: (A) first author region and (B) last author region. SSA, Sub-Saharan Africa.
DISCUSSION
This report describes the under-representation of first and last authors from SSA and LICs in JCO GO. The results show the global reach of the journal articles representing 66 countries and authors from 85 countries. Although SSA was the most studied region, first and last authors from North America accounted for a higher proportion than SSA authors on SSA studies. Every other region had more concordant representation with majority of the authors representing studied regions. Correspondingly, our results also highlight that authors from LICs are under-represented, with first and last authors from HICs comprising a higher proportion of authorship on articles about LICs. However, yearly trends indicate that some progress is being made with greater representation of SSA last authors in the more recent years of publication.
To our knowledge, this report is the first to highlight authorship disparities in global oncology by region and income classification. Although the proportion of SSA authors in global oncology may be rising, SSA authors remain markedly under-represented. These findings are similar to the results from studies that have quantified SSA authorship more broadly within global health. For example, a recent bibliometric analysis published in October 2021 analyzed the concept of authorship parasitism, when none of the study authors were affiliated with the LMIC in which a study took place.19 This paper observed that 14.8% of 32,061 published studies in SSA indexed in PubMed between 2014 and 2018 fell into this category. SSA authorship under-representation has also been described in SSA studies in other specific fields such as infectious disease,8 geoscience,20 COVID-19 pandemic research,9 and collaborative research.21 Authors from SSA are frequently stuck in the middle, which raises concerns about tokenism rather than true equitable engagement.21
There are numerous reasons that contribute to the continued under-representation of SSA authors, including factors associated with limited research infrastructure in many SSA countries, and those related to factors external to the region. Limited research infrastructure manifests as lack of local financial resources dedicated to research and administration of grants; lack of research training and professional incentives to pursue research; and competing professional responsibilities for researchers such as teaching, administrative, or clinical responsibilities. The persistence of HIC versus LIC power differentials are evident in establishing research priorities, which are often linked to HIC sources of funding even when the study is being conducted in LIC and LMIC settings. In addition, academic productivity expectations on HIC investigators may lead to perverse incentives. The value HIC institutions place on the numbers of first and last authorships may lead HIC investigators to deprioritize collaborative activities and capacity building, which can be more nebulous to quantify. Additionally, many high-impact global health journals are based in HICs. Although there has been significant effort with diversifying journal editorial boards to be more inclusive of researchers from LICs and SSA, there remains much room for improvement in ensuring broader perspective among the academic gatekeepers. There is also the need to restructure academic expectations and critically reflect on criteria for promotion in HICs, as well as in LICs and LMICs.22 For instance, developing and valuing metrics of community impact, clinical care innovation, and capacity building may foster more engagement of local researchers.
Deliberate and concerted efforts are required to expand global oncology research training opportunities in SSA. Local governments, health ministries, and partner research organizations need to invest in increasing awareness and incentives to pursue existing opportunities for research training in SSA. These opportunities include repositories of lectures, remote or live participatory sessions, and conferences. For example, there have been workshop-training opportunities in conjunction with the biannual African Organization for Research and Training in Cancer (AORTIC) conference, which have provided training in areas such as implementation science research and clinical trials. AORTIC also established the African Cancer Leaders Institute as a community to foster mentorship of the next generation of leaders in cancer research.23 Regional opportunities such as those coordinated by the African Academy of Sciences could also further avenues for capacity building.24 Furthermore, there are also opportunities to pursue research training and mentorship organized by institutions outside SSA, including the Fogarty International Center e-learning resources for global health researchers25 and the International Development and Education Award through ASCO.26 The combination of local and international opportunities for oncology research training represent important steps in building oncology research capacity. Some gaps remain, especially in access to longitudinal mentorship such as postdoctoral fellowships for young SSA investigators. Building a local cadre of researchers, who become future senior authors and mentors, has the potential to inspire the next generations.
Besides research training, fostering representation of SSA will require increasing research funding opportunities for local investigators. Some existing awards include the Beginning Investigator Grant for Catalytic Research, administered through a partnership between AORTIC and the American Association for Cancer Research, to foster exploratory data collection in Africa by African scientists27,28; the ASCO International Innovation Grant, which supports novel projects with impact on cancer control in LMICs29; Wellcome Early Career Grants, which offer funding for a broad array of disciplines for early-career researchers30; and the American Society of Hematology's Global Research Award, which supports prospective future international scientific leaders in hematology.31 Although there have been efforts to increase funding opportunities, it is crucial to ensure that SSA and LIC investigators are empowered to apply for these grants, including mentorship on grantsmanship and having requisite local institutional administrative backing to manage the grants.
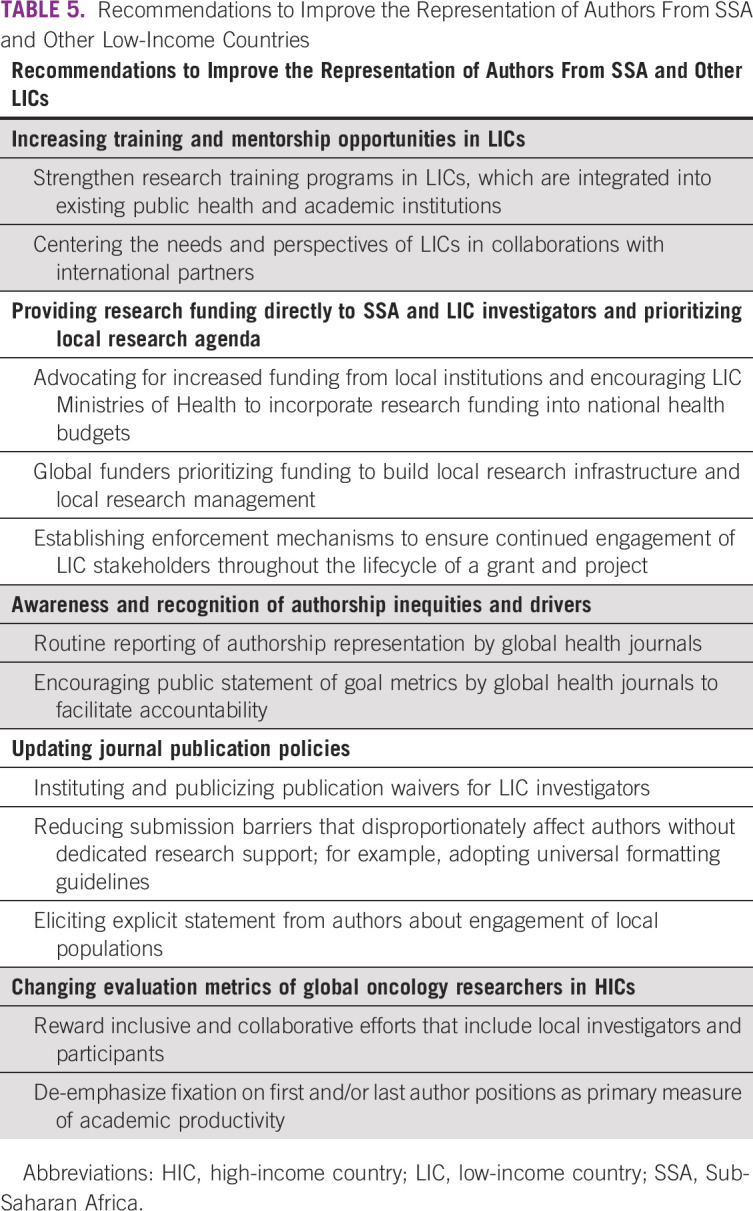
Moreover, policy changes and interventions at journals can reduce barriers to publications for LIC and LMIC authors. For instance, a recent commentary analyzed authorship in 272 journals and concluded that article-processing charge waivers for LIC and LMIC authors could lead to greater representation.32 Some journals also now require explicit statements on the engagement of communities and local populations, which can be expanded to include statements on engagement of local researchers and contributions to capacity building. We recommend systematic self-tracking by global journals, and periodic publication of authorship representation reports to facilitate transparency, accountability, and comparisons across different specialties. A summary of recommendations to improve the representation of authors from SSA and other LICs is outlined in Table 5.
TABLE 5.
Recommendations to Improve the Representation of Authors From SSA and Other Low-Income Countries
There are some limitations to this study. The study is based on one journal with a North American publisher. Hence, the findings may not be generalizable. However, we also show that JCO GO has a vast geographic base where published studies occur. Although the balance of authors from a publisher in a different region may differ, the overarching principles encouraging engagement and representation from local authors still apply. Another limitation is that JCO GO is published solely in English, reflecting the geographic distribution of articles and authors; the findings may not be generalizable to countries and regions with different official languages. Of note, this study was designed before the beginning of the COVID-19 pandemic and includes articles published through March 2020. Therefore, the findings do not reflect the potential differential impact of the COVID-19 pandemic on academic productivity with regard to a country region or income level. Future studies may explore regional collaboration and authorship equity changes in global oncology during the ongoing COVID-19 pandemic.
In conclusion, this study shows persistent under-representation of SSA and LIC authors in global oncology publications. Although there are ongoing efforts in research training and capacity building in SSA and other LICs, more needs to be done by academic journals, HIC academic institutions, funders, and LIC institutions to facilitate representation of local authors. Tracking and periodic reporting can facilitate accountability and ensure continued progress to greater equity in the future.
ACKNOWLEDGMENT
The authors acknowledge the contribution of Kayleigh Bhangdia, MS, of the Institute for Health Metrics and Evaluation, who assisted with preparing the maps. The authors are also grateful to Christine Brown, MBA, and Scott Triedman, MD, of the Center for Global Cancer Medicine at Dana-Farber Cancer Institute, who provided editorial input while preparing the manuscript.
Miriam Mutebi
This author is a member of the JCO Global Oncology Editorial Board. Journal policy recused the author from having any role in the peer review of this manuscript.
Temidayo Fadelu
Research Funding: Celgene (Inst), Cepheid (Inst)
No other potential conflicts of interest were reported.
Footnotes
H.T. and P.H. contributed equally to this work.
AUTHOR CONTRIBUTIONS
Conception and design: Hubert Tuyishime, Paula Hornstein, Nwamaka Lasebikan, Miriam Mutebi, Temidayo Fadelu
Administrative support: Hubert Tuyishime
Collection and assembly of data: Hubert Tuyishime, Paula Hornstein, Nwamaka Lasebikan, Miriam Mutebi, Temidayo Fadelu
Data analysis and interpretation: All authors
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/go/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Miriam Mutebi
This author is a member of the JCO Global Oncology Editorial Board. Journal policy recused the author from having any role in the peer review of this manuscript.
Temidayo Fadelu
Research Funding: Celgene (Inst), Cepheid (Inst)
No other potential conflicts of interest were reported.
REFERENCES
- 1.Shiffman J: Knowledge, moral claims and the exercise of power in global health. Int J Health Policy Manag 3:297-299, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shiffman J: Global health as a field of power relations: A response to recent commentaries. Int J Health Policy Manag 4:497-499, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Walsh A, Brugha R, Byrne E: “The way the country has been carved up by researchers”: Ethics and power in north–south public health research. Int J Equity Health 15:204, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Busse C, August E: Addressing power imbalances in global health: Pre-Publication Support Services (PREPSS) for authors in low-income and middle-income countries. BMJ Glob Health 5:e002323, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abimbola S, Asthana S, Montenegro C, et al. : Addressing power asymmetries in global health: Imperatives in the wake of the COVID-19 pandemic. PLoS Med 18:e1003604, 2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Odjidja EN: What is wrong with global health? So-called glorified data collectors in low-income regions. Lancet Glob Health 9:e1365, 2021 [DOI] [PubMed] [Google Scholar]
- 7.Östlin P, Schrecker T, Sadana R, et al. : Priorities for research on equity and health: Towards an equity-focused health research agenda. PLoS Med 8:e1001115, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mbaye R, Gebeyehu R, Hossmann S, et al. : Who is telling the story? A systematic review of authorship for infectious disease research conducted in Africa, 1980–2016. BMJ Glob Health 4:e001855, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Naidoo AV, Hodkinson P, Lai King L, et al. : African authorship on African papers during the COVID-19 pandemic. BMJ Glob Health 6:e004612, 2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cash-Gibson L, Rojas-Gualdrón DF, Pericàs JM, et al. : Inequalities in global health inequalities research: A 50-year bibliometric analysis (1966-2015). PLoS One 13:e0191901, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Global oncology: Formalizing a career path in building a better World. ASCO Connection, September 18, 2019. https://connection.asco.org/magazine/features/global-oncology-formalizing-career-path-building-better-world [Google Scholar]
- 12.About|JCO Global Oncology. https://ascopubs.org/go/about/about-go [Google Scholar]
- 13.Open Access Terms. JCO Global Oncology. https://ascopubs.org/go/authors/open-access [Google Scholar]
- 14.Harris PA, Taylor R, Thielke R, et al. : Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42:377-381, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Harris PA, Taylor R, Minor BL, et al. : The REDCap consortium: Building an International Community of Software Platform Partners. J Biomed Inform 95:103208, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.World Bank Country and Lending Groups—World Bank Data Help Desk. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups [Google Scholar]
- 17.World Countries (Generalized). https://hub.arcgis.com/datasets/esri::world-countries-generalized/about [Google Scholar]
- 18.Vandenbroucke JP, von Elm E, Altman DG, et al. : Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int J Surg Lond Engl 12:1500-1524, 2014 [DOI] [PubMed] [Google Scholar]
- 19.Rees CA, Ali M, Kisenge R, et al. : Where there is no local author: A network bibliometric analysis of authorship parasitism among research conducted in sub-Saharan Africa. BMJ Glob Health 6:e006982, 2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.North MA, Hastie WW, Hoyer L: Out of Africa: The underrepresentation of African authors in high-impact geoscience literature. Earth Sci Rev 208:103262, 2020 [Google Scholar]
- 21.Hedt-Gauthier BL, Jeufack HM, Neufeld NH, et al. : Stuck in the middle: A systematic review of authorship in collaborative health research in Africa, 2014–2016. BMJ Glob Health 4:e001853, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hedt-Gauthier B, Airhihenbuwa CO, Bawah AA, et al. : Academic promotion policies and equity in global health collaborations. Lancet 392:1607-1609, 2018 [DOI] [PubMed] [Google Scholar]
- 23.ACLI : AORTIC 2019 Conference. 2019. http://2019.aorticconference.org/acli/ [Google Scholar]
- 24.The AAS Mentorship Scheme. The AAS. https://www.aasciences.africa/mentorship-scheme#about-the-aas [Google Scholar]
- 25.E-Learning Resources for Global Health Researchers—Fogarty International Center @ NIH. Fogarty International Center. https://www.fic.nih.gov:443/Global/Pages/training-resources.aspx [Google Scholar]
- 26.International Development & Education Award. ASCO, 2019. https://www.asco.org/career-development/grants-awards/funding-opportunities/international-development-education-award [Google Scholar]
- 27.Admin. Beginning Investigator Grant for Catalytic Research. AORTIC AFRICA. https://aortic-africa.org/big-cat/ [Google Scholar]
- 28.New AACR Partnership Supports BIG Cat Grants for Young Investigators in Africa. American Association for Cancer Research (AACR), 2021. https://www.aacr.org/blog/2021/11/17/new-aacr-partnership-supports-big-cat-grants-for-young-investigators-in-africa/ [Google Scholar]
- 29.International Innovation Grant. ASCO, 2019. https://www.asco.org/career-development/grants-awards/funding-opportunities/international-innovation-grant [Google Scholar]
- 30.Early-Career Awards—Grant Funding. Wellcome. https://wellcome.org/grant-funding/schemes/early-career-awards [Google Scholar]
- 31.ASH Global Research Award. https://www.hematology.org:443/awards/career-enhancement-and-training/global-research-award [Google Scholar]
- 32.Gardner UG, Thompson PS, Burton J, et al. : Article processing charge waiver policies as a barrier to oncology scholarship in low- and lower-middle-income countries. JCO Glob Oncol 7:1413-1417, 2021 [DOI] [PMC free article] [PubMed] [Google Scholar]