

Abstract
Radiation dosimetry is central to virtually all radiation safety applications, optimization, and research. It relates to various individuals and population groups and to miscellaneous exposure situations—including planned, existing, and emergency situations. The International Commission on Radiological Protection (ICRP) has developed a new computational framework for internal dose estimations. Important components are more detailed and improved anatomical models and more realistic biokinetic models than before. The ICRP is currently producing new organ dose and effective dose coefficients for occupational intakes of radionuclides (OIR) and environmental intakes of radionuclides (EIR), which supersede the earlier dose coefficients in Publication 68 and the Publication 72 series, respectively. However, the ICRP only publishes dose coefficients for a single acute intake of a radionuclide and for an integration period of 50 years for intake by adults and to age 70 years for intakes by pre-adults. The new software, IDAC-Bio, performs committed absorbed dose and effective dose calculations for a selectable intake scenario, e.g., for a continuous intake or an intake during x hours per day and y days per week, and for any selected integration time. The software uses the primary data and models of the ICRP biokinetic models and numerically solves the biokinetic model and calculates the absorbed doses to organs and tissues in the ICRP reference human phantoms. The software calculates absorbed dose using the nuclear decay data in ICRP publication 107. IDAC-Bio is a further development and an important addition to the internal dosimetry program IDAC-Dose2.1. The results generated by the software were validated against published ICRP dose coefficients. The potential of the software is illustrated by dose calculations for a nuclear power plant worker who had been exposed to varying levels of 60Co and who had undergone repeated whole-body measurements, and for a hypothetical member of the public subject to future releases of 148Gd from neutron spallation in tungsten at the European Spallation Source.
Key words: dosimetry, internal; International Commission on Radiological Protection; medical exposure; occupational safety
INTRODUCTION

Radiation dosimetry is central to virtually all radiation safety applications, optimization, and research. It is the basis for estimates of impact and risk from exposure to ionizing radiation. This paper focuses on internal radiation dose assessments for humans in connection with planned or accidental exposure situations and different modes of intake (inhalation, ingestion, and injection). Ionizing radiation and radioactive materials occur naturally, and human activities may also increase the exposure of people to ionizing radiation. Many uses of ionizing radiation, e.g., in health care and in the nuclear industry, are of benefit to society but also present increased risks of radiation exposure that must be estimated and controlled. In connection with potential nuclear and radiological accidents and disasters, projected dose estimates will be decisive for the planning of countermeasures such as evacuation and remediation. New accelerators, spallation sources, nuclear power plants, decommissioning of old reactors, and waste management require planning based on estimates of absorbed and effective dose to occupationally exposed persons and to the public—often with a long-term perspective covering future generations.
Most of the associated exposure scenarios for these situations, and for many other situations that we cannot predict, will require authorities to provide dose limits, dose constraints, restrictions, and reference guidance levels aimed at protecting the public and the environment. Many of these cases deal with acute exposures and will be covered by internal dose coefficients published by the ICRP in their new framework for internal dose assessment for occupational exposure and in the coming series of reports for members of the public. For many actual or potential exposure conditions, however, additional tools are needed to perform dose calculations from the primary data and models with the option of choosing an arbitrarily selectable dose-integration period instead of a fixed period as in the ICRP methodology. This paper describes new dosimetry software designed to derive dose estimates based on either acute or continuous intake, or on intermittent intake of x hours a day and y days per week, where x and y are supplied by the user. Intake parameter values including the level of activity and the time (s) of intake can be estimated by fitting the parameters of the model to the measured data points.
The ICRP computational framework for internal dose assessment
During the last decade, the ICRP has developed a new computational framework for dose estimations, using more detailed anatomical models and more physiologically realistic biokinetic models than before. New software is needed to derive dose estimates for internally deposited radionuclides based on these new models. The ICRP updated and extended its basic anatomical and physiological data for reference persons in 2002 (ICRP 1975, 2002). New models of the corresponding reference persons have been created. Reference anatomical models for adults based on CT and MR images from a real adult male and female, rather than mathematical models, were later published (ICRP 2009). These were in accordance with the description of the reference adult male and female, e.g., the basic anatomical and physiological data of organs and tissues are in agreement with the specifications given in Publication 89 (ICRP 2002).
In 2007, ICRP updated its general recommendations and published a new set of tissue weighting factors for calculation of effective dose, and a modified set of organs and tissues were assigned specific weighting factors (ICRP 1991, 2007). In the new reference phantoms, all the organs and tissues needed for the revised effective dose calculations were included, and the anatomical models were also created to conform to the new human alimentary tract (HAT) model, describing the transfer of materials within this region (ICRP 2006). A revised version of the Human Respiratory Tract Model (HRTM) (ICRP 2016a) was developed for calculation of absorbed doses for inhaled radionuclides, replacing the original HRTM introduced in Publication 66 (ICRP 1994a).
Furthermore, an updated nuclear decay database intended for radiation dosimetry was published in 2008. The database includes information on the physical half-lives, decay chains, yields, and energies of various types of radiation emitted in nuclear transformations of each of 1,252 radionuclides of 97 elements (ICRP 2008). Based on the reference phantoms (ICRP 2009), monoenergetic sex specific absorbed fractions (SAF) were published (ICRP 2016a). Corresponding SAF values for adolescents have been completed but have not yet been published. Previously, only contributions from photons were included in the SAF-values and particles (except at walled regions) were assumed to be locally absorbed within the source tissue. In the calculations deriving the new adult SAF-values, monoenergetic photons, electrons, and alphas for 79 source regions and 43 sex-specific target regions are included. The decay database includes nuclide-specific beta spectra instead of using the mean beta energies.
Based on the above, ICRP has defined a new computational framework of internal dose assessment for reference adults (ICRP 2016a) for the application with the refined biokinetic models. The revised models are now based on the transfer of radionuclides following the circulating blood in systemic compartment models instead of using the previous descriptive models assuming a direct uptake in different organs and an excretion without realistic connections between different parts of the body. For the “Occupational Intakes of Radionuclides” (OIR) publication series, four out of five publications have already been published (ICRP 2015, 2016b, 2017, 2019). These publications will replace the ICRP Publication 30 series and the Publications 54, 68, and 78 (ICRP 1989, 1994b, 1997). Replacement of the dose coefficients for members of the public in the “Dose coefficients for intakes of radionuclides by members of the public” series is currently underway.
Acute, continuous and protracted intake
Occupational exposure can often be categorized into three different types of exposure: acute intake, continuous intake over a limited time interval, or protracted intake over a working life or a lifetime. The ICRP dose coefficients covers the first case for acute exposure. The types of intakes are shown in Fig. 1.
Fig. 1.
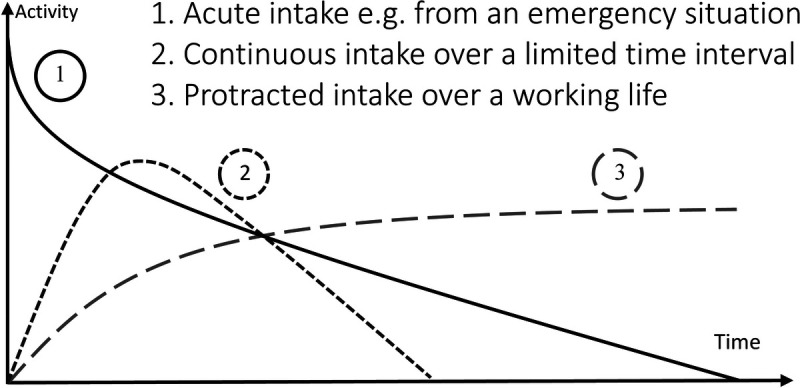
Schematic time activity curves for different types of intake.
Dosimetry based on series of measurements
Workers occupationally exposed to radionuclides are typically undergoing routine activity measurements. From repeated measurements, the type of exposure shown in Fig. 1 can be determined. It is obvious from Fig. 1 that a single measurement alone is not enough to differentiate various types of exposure. By calculating either acute or continuous intake from different exposure scenarios, organ activity can be estimated in the following way: (a) Estimate intake and exposure scenario by fitting solution of biokinetic models to experimental data; (b) Refine scenario parameters until a good fit is achieved; (c) Solve biokinetic model for the best selected scenario parameters. D) Use solution to calculate numbers of decays; and (e) Use S-coefficients to calculate doses, i.e., apply ICRP Publication 133 Methodology (ICRP 2016a).
The aim of this paper is to use the most recent primary data and models in the form of SAF-values, decay data, biokinetic rate constants, etc., from the ICRP dosimetric and biokinetic computational frameworks to estimate the dose contribution for acute or continuous exposure of humans. To do this, it is necessary to numerically solve the different mathematical equations that express the biokinetic model and calculate the absorbed dose to the ICRP reference phantom for selectable exposure times.
MATERIALS AND METHODS
A computer code in MATLAB (MathWorks, Natick, MA) has been developed. It assesses absorbed dose to different organs and tissues using the biokinetic models and data presented within the new ICRP computational framework.
Biokinetics
The purpose of a biokinetic model is to estimate the spatial and temporal distribution for the decays associated with an intake of a specific radionuclide. A biokinetic model is created by determining the most important regions of accumulation or concentration of the radionuclide in the body, the time course of uptake and retention in the different regions, and the rates of excretion along different pathways. The ICRP provides element-specific systemic biokinetic models to quantify organ and tissue activity and their time course. These models, accounting for transfer between organs, so-called compartmental models, are constructed mathematically by defining transfer rates of the radionuclide between different regions of the body. There are several parameters that determine the total number of disintegrations in the total body or the specific organs: the administered activity, the physical half-life of the radionuclide, the residence time of the substance, and its excretion rate via different pathways. If a biokinetic model can be constructed, that model can be used to estimate the contribution of each disintegration to the absorbed dose of the organs.
The general principle is to calculate the distribution of radionuclides in the identified parts of the human body stepwise in time. Over each time step, the transfer of the radionuclide to and from each compartment will be calculated. If there are progenies included in the decay chain, these are also taken into account in each time step. Each progeny is assumed to migrate at a specified rate from the preceding members of the chain and follow its own characteristic biokinetic model, but its initial distribution is dependent on the kinetics of the preceding members of the chain. For biokinetic modeling of infants, children or adolescents, the biokinetic transfer coefficients will also be interpolated between bounding ages specified in the age-specific biokinetic model for each time step; six basic ages are specified in each age-specific biokinetic model: infant, 1 y, 5 y, 10 y, 15 y, and adult. The calculations consider that the adolescent is constantly growing until reaching 20 years of age (or 25 years of age for a bone-seeking radionuclide as the skeleton is not fully mature by age 20 years). After adulthood is reached, the biokinetic transfer parameters remain unchanged in ICRP applications. From a biokinetic point of view, this is one of the differences between the calculations for the general public and workers. For workers, who are assumed to be adults from the start, no age interpolation is necessary.
For continuous intake, activity will be added to the biokinetic model at predefined time steps, e.g., x hours a day, y days a week. For long-lived radionuclides there may be activity left in the human body at age 70. Nevertheless, the committed effective dose is integrated only over 50 years for intake by an adult and only to age 70 years for intake at a pre-adult age.
The graphical interface of the software is shown in Fig. 2 and illustrates a calculation of dose estimates for an oral intake of 1 Bq of 148Gd per day during a 10-y period and with an integration time of 50 years. For more details, see the examples of dose calculations for 60Co and 148Gd intake below.
Fig. 2.
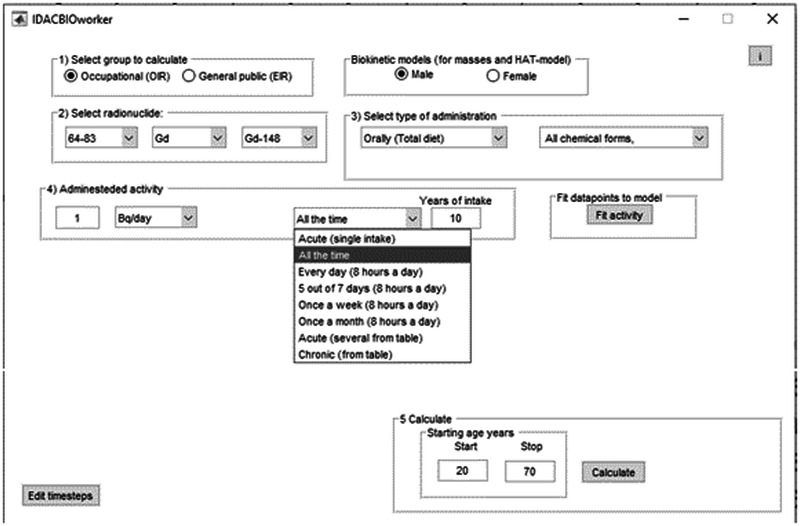
The graphical interface of the software for a 148Gd calculation for an orally ingested activity of 1 Bq per day over 10 years and an integration time of 50 years.
Dosimetry
The absorbed dose is calculated by using a dedicated version of IDAC-Dose2.1 (Andersson et al. 2017) generated for this specific project. The graphical interface is shown in Fig. 2. IDAC-Dose2.1 follows the computational framework of internal dose assessment given for reference adults in ICRP Publication 133 (ICRP 2016a). The program uses the radionuclide decay database of ICRP Publication 107 (ICRP 2008) and considers 79 different source regions irradiating 43 target tissues, defining the effective dose as presented in ICRP Publications 60 and 103 (ICRP 1991, 2007). The computer program IDAC-Dose2.1 has been validated against another ICRP dosimetry program, Dose and Risk Calculation (DCAL, United States Environmental Protection Agency). IDAC-Dose2.1 is written in MATLAB which enables a direct integration when creating absorbed dose calculations for occupationally exposed workers and members of the public. Currently, a new version of IDAC-Dose is under development which will also include absorbed dose calculations for pre-adult ages.
Absorbed dose and effective dose
To estimate the radiation risk, the mean absorbed dose D (J kg−1 or Gy) in target region rT is calculated over the time period TE (s) assuming at time zero the activity A (Bq) was administered (Bolch et al. 2009):
| (1) |
where S(rT ⟵ rs) [Gy (Bq s)−1] is the mean absorbed dose in target rT per nuclear transformation within source region rs and a(rs, t) is the fraction of the administered activity in source region rs at time t. The S values are based on the radiations emitted by the administered radionuclide and their specific absorbed fractions that were derived in Monte Carlo simulations of the source-target geometry in reference mathematical phantoms. The S values are computed as
| (2) |
where Φ(rT ← rs, Ei) is the specific absorbed fraction (kg−1) of the energy of the ith radiation emitted within source region rs that is absorbed per mass in target region rT and Δi = EiYi is the emitted energy per nuclear transformation [J (Bq s)−1]. Here, Yi (Bq s)−1 is the yield of the ith radiation per nuclear transformation and Ei is the emitted energy (J). Each type of emitted radiation is considered, that is the summation extends over electrons, alpha particles, photons and an integral over the beta spectrum.
The effective dose (E) is the sum of sex-averaged, radiation-weighted equivalent dose over radiosensitive organs and is calculated by:
where wRis the radiation weighting factor of radiation R, wTis the tissue weighting factor representing the relative detrimental effects to organs and tissues. D(rT, TD)Male and D(rT, TD)Female are the absorbed doses to target region T of the reference male and female, respectively. For the summation over each type of radiation, D(rT, TD)Male and D(rT, TD)Female are calculated as separate entities.
Validation of the code under ICRP reference exposure scenarios
To verify that the code is developing accurate results, comparisons have been made with the current ICRP effective dose coefficents under the established exposure senarious. The validation was perfomed on 5,080 different ICRP effective dose coefficents, including 90 elements, 886 different nuclides, and 3 different routes of intake (injection, ingestion, and inhalation with particle size of 5 μm) and different material.
Examples of the importance of the software for some current dose calculations for 60Co and 148Gd dose and effective dose
The use of the new software is illustrated by two examples of current dose estimates.
Dose estimation of 60Co intake from monitoring a nuclear power plant worker
Activated corrosion products, especially 60Co, are, under normal operating conditions, the main source of radiation exposure of the staff at Swedish nuclear power reactors. Cobalt-60 is formed by neutron irradiation of cobalt, which is used as a component in stainless steel to make it harder. The material is called stellite and is common in valve surfaces, which typically are made largely (up to 60%) of cobalt. Due to the presence of cobalt, workers at power plants are routinely monitored by whole body counting, often with an HPGe-detector in a low-background chamber to measure the body burden of 60Co.
The absorbed dose contribution for a nuclear power plant worker has been estimated using long term measurements of the body content. In Sweden a nuclear power plant worker is subject to measurements of the body burden of radionuclides at least each 90 days. To estimate the time dependent lung activity, five source organs were used: alveolar-interstitial, bronchiolar surface, bronchial surface, bronchiolar sequestered region, and bronchial sequestered region. In this study, such measurements have been used to estimate the absorbed dose contribution by fitting the parameters of the ICRP biokinetic model to the results from the measurements of a worker who has undergone 27 whole body measurements of 60Co during the last 20 years. The results of the series of measurements indicate a dominating single acute intake.
Dose estimations of continuous ingestion of 148Gd
Gadolinium-148 is produced during proton-induced spallation reactions in tungsten. Both the European Spallation Source (ESS) in Lund, Sweden, and the upgraded second target station at the Spallation Neutron Source (SNS) in Oak Ridge, TN, use tungsten as targets. It is estimated that during a 5-year operation of the ESS, more than 1014 Bq of 148Gd will be produced (Barkauskas and Stenström 2020). Gadolinium-148 is a pure alpha emitter with a physical half-life of 74.6 years. This could be a long-time radiation protection problem if 148Gd is accidently released with resulting contamination of air, agricultural land, and groundwater. It will also be an important component for the ESS’s radioactive waste management.
RESULTS AND DISCUSSION
The code was validated against all published dose coefficients given in ICRP Publications 134, 137, 141, and 151 (ICRP 2016b, 2017, 2019, 2022). The comparisons showed that, of 5,080 calculations, 95% were precise reproductions of the ICRP published values and 5% of the calculations differed by ± 1 unit, in the last significant figure. As the source code was the same for all calculations with only different input parameters, this difference is probably due to rounding errors. This validation for the reference exposure geometries indicates the validity of the code in situations not covered by the ICRP, e.g., the applications given in this paper.
Dose estimation of the absorbed dose from an acute intake of 60Co
The results of the long-term measurements have been used to estimate the 60Co intake for the exposure case described earlier. The fit of the biokinetic model to the measured data points is shown in Fig. 3. As the equipment was recalibrated in 2010 (using more careful calibration, anthropomorphic phantoms, and certified 60Co, 241Am, and 152Eu solutions) and longer measurement times were used. The data points generated after this date were given a higher weight than the earlier measurement. The goodness of fit using a normalized mean squared error was 0.2, where 0 is a perfect fit. The curve fit indicates a high activity intake before the initial measurements were carried out. Due to lack of earlier data points, other exposure scenarios could not be ruled out.
Fig. 3.
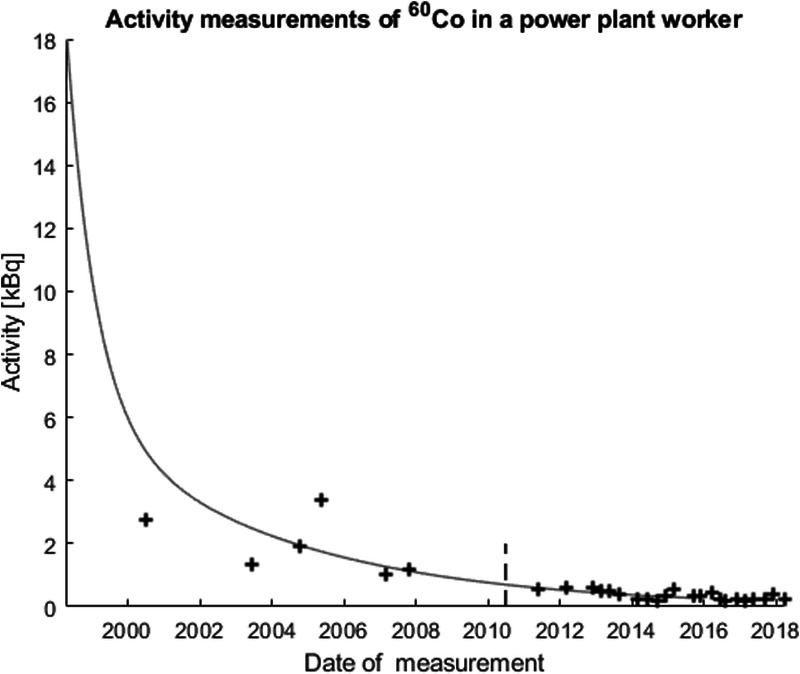
Curve fit of an acute uptake in lung of 350 kBq inhaled 2 years before first measurement. The dashed line shows when the system was recalibrated.
Assuming that most of the activity is present in the lung tissue and inhaled 2 years before the first measurement gives an estimate of the acute single inhalation in lungs of 350 kBq for 60Co (AMAD of 5 μm, Type S—cobalt oxide, FAP and PSL) resulting in an effective dose of 10 mSv (ICRP effective dose coefficient 3.1 × 10−8 Sv Bq−1). The absorbed doses and the effective dose are shown in Fig. 4. The repeated measurements of this worker indicate that this was not an exposure generated during the regular working condition but an acute accidental intake.
Fig. 4.
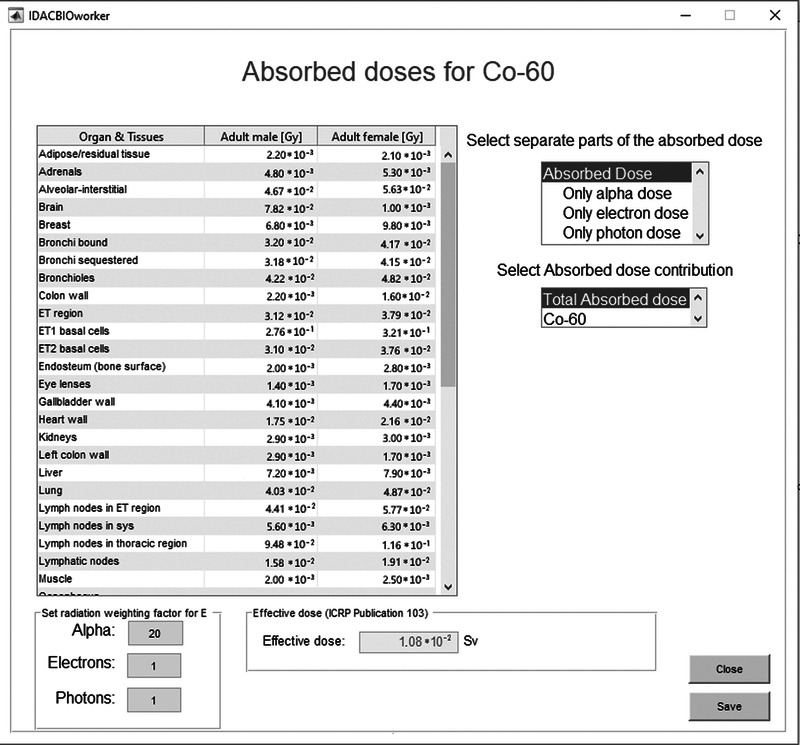
Absorbed dose calculations from repeated lung activity measurements of 60Co from a Swedish power plant worker.
In the process of decommissioning a power plant there are restrictions related to the radiation exposure to workers and members of the public. Radiation Safety Authorities sometimes demand effective dose estimates to a representative person from the general public. Some authorities demand that the dose estimations should be performed on annual exposures due to air and water discharges of radioactive substances and that the calculations should be integrated over a period of at least 100 years (e.g., Swedish Radiation Safety Authority (2017)). If the effective dose to a member of the general public is estimated to 0.01 mSv or more per calendar year, a realistic calculation of radiation dose should be performed. In such cases more detailed absorbed dose calculations to various sub-groups of the population and even to specific individuals will be demanded. There may be exposure scenarios that are not covered well by the published ICRP dose coefficients for workers or members of the public. Calculations of the committed effective dose from primary data and models are expected to provide more realistic estimates of the absorbed dose and effective dose for these scenarios.
Dose estimations of continuous ingestion of 148Gd
For 148Gd, the committed effective dose coefficient for acute intake via ingestion is 0.02 μSv Bq−1 (ICRP 2019). The committed effective dose E(50) for continuous ingestion of 1 Bq per day of 148Gd during 10, 30, and 50 years is 69 μSv, 190 μSv, and 260 μSv, respectively. As the physical half-life of 148Gd is 74.6y, the 50-year integration time is about two-thirds of the physical half-life. However, for ingestion, the fractional uptake of 148Gd from the alimentary tract is only about 0.0005. Thus, only a small fraction of the ingested activity will be transferred into the circulating blood and even less will deposit in bone. The rest will leave the body through fecal excretion over the next few days. Fig. 5 shows the whole body, gastrointestinal tract, and the bone activity over 50 years and for the three different exposure periods. Fig. 6 shows the absorbed dose (Gy) and effective dose (Sv) for continuous ingestion of 1 Bq 148Gd per day over 10 years and integrated for a period of 50 years. Release into the water and contamination of food of 148Gd could be a problem if not monitored. A regulatory annual dose constraint of 0.1 mSv corresponds to a daily intake of 14 Bq. Recent dose estimates (Rääf et al. 2020) use dose coefficients from ICRP Publication 68 (ICRP 1994b), now outdated, and give dose coefficients that are a factor of 3 higher for ingestion and a factor of 9 higher for inhalation type F than the new values.
Fig. 5.
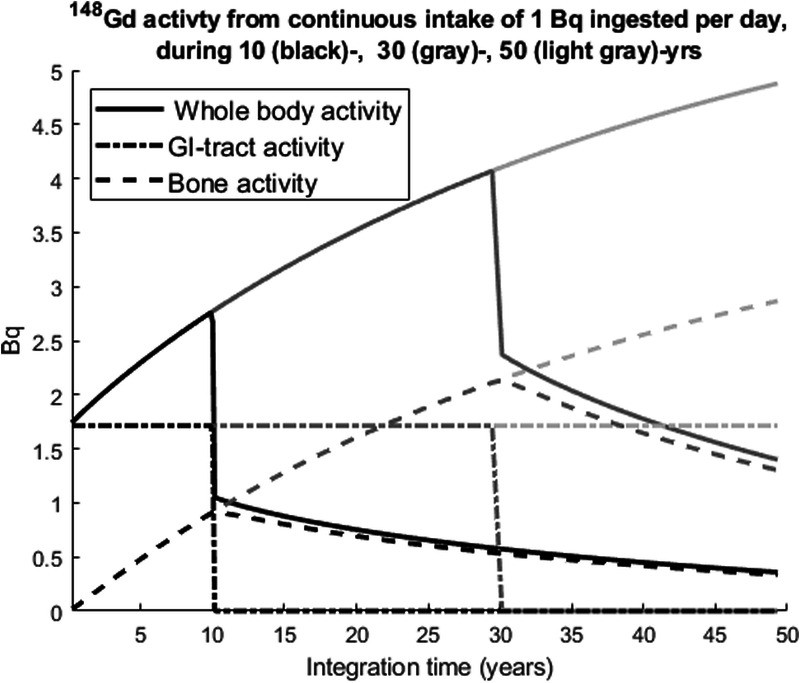
Biokinetic calculations of continuous ingestion of 1 Bq per day of 148Gd during 10, 30 and 50 year, respectively, calculated over an integration time of 50 year.
Fig. 6.
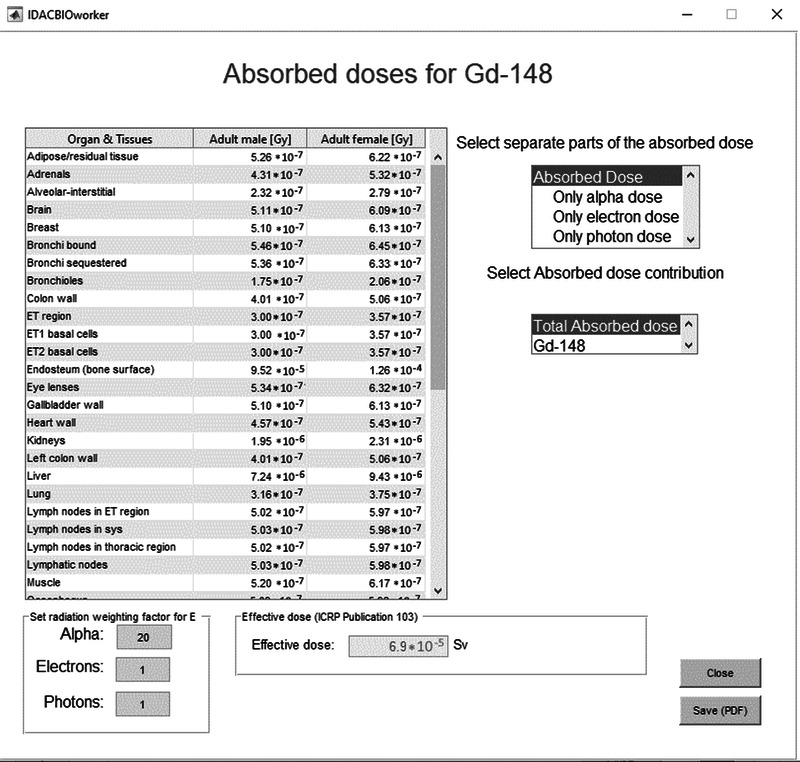
The graphical interface of the result from the software with the continuous intake of 1 Bq per day of 148Gd during 10 year.
SUMMARY AND CONCLUSION
The ICRP is currently producing new organ absorbed dose and effective dose coefficients for occupational intakes of radionuclides (OIR) and environmental intakes of radionuclides (EIR), which supersede the earlier dose coefficients in Publication 68 and in the Publication 72 series, respectively. However, the ICRP has only published information for single acute intake of radionuclides and for a committed period of 50 years for intake by an adult and to age 70 years for intake at a pre-adult age. The new software, IDAC-Bio, performs committed absorbed dose and effective dose calculations for selected chronic intake scenarios and for a user-specified commitment period. The software uses the primary data and models of the ICRP biokinetic models and numerically solves the biokinetic model and calculates the absorbed doses to the reference human phantoms. The software calculates absorbed dose using the nuclear decay data in ICRP Publication 107—radiation weighting factors of ICRP 130 are applied if the user requests equivalent dose.
IDAC-Bio is a further development and an important addition to the internal dosimetry program IDAC-Dose2.1. The software has been validated using the published dose coefficients for workers in ICRP Publication 134, 137, and 141 (ICRP 2016b, 2017, 2019). In a future work the code will be validated through calculations using information in Part 5 of the ICRP OIR publication and the coming ICRP publications for members of the public. The results of this research can be used for radiation protection dosimetry directed toward occupationally exposed individuals and for members of the general public. The potential of the software for dose estimates for time varying intake is illustrated by calculations for a nuclear power plant worker who had undergone repeated whole-body measurements of 60Co and for a hypothetical member of the public subject to future releases of 148Gd from neutron spallation in tungsten at the European Spallation Source, when operational.
In summary, IDAC-Bio can be used to calculate bioassay functions (retention/excretion) and dose coefficients for virtually any scenario. These bioassay functions can then be applied in the dose assessment process for the evaluation of monitoring data.
An online version of the software IDAC-Bio is available at www.idac-dose.org.
Acknowledgments
This project was funded by Swedish Radiation Safety Authority (grant number: SSM2020-642).
Footnotes
Conflict of interests: MA has created a webpage www.idac-dose.org and a distribution channel IDAC-Dose AB to be able to distribute the software generated in this article. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Contributor Information
Richard W. Leggett, Email: leggettrw@ornl.gov.
Keith Eckerman, Email: eckermank@bellsouth.net.
Anja Almén, Email: anja.almen@med.lu.se.
Sören Mattsson, Email: soren.mattsson@med.lu.se.
REFERENCES
- Andersson M, Johansson L, Eckerman K, Mattsson S. IDAC-Dose 2.1, an internal dosimetry program for diagnostic nuclear medicine based on the ICRP adult reference voxel phantoms. EJNMMI Res 7:88; 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barkauskas V, Stenström K. Prediction of the radionuclide inventory in the European Spallation Source target using FLUKA. Nucl Instrum Methods Phys Res B 471:24–32; 2020. [Google Scholar]
- Bolch WE, Eckerman KF, Sqouros G, Thomas SR. MIRD pamphlet no. 21: a generalized schema for radiopharmaceutical dosimetry—standardization of nomenclature. J Nucl Med 50:3:477–484; 2009. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Report of the Task Group on Reference Man. Oxford: Pergamon Press; ICRP Publication 23; 1975. [Google Scholar]
- International Commission on Radiological Protection . Individual monitoring for intakes of radionuclides by workers. Oxford: Pergamon Press; ICRP Publication 54; Ann ICRP 19:(1–3); 1989. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Recommendations of the International Commission on Radiological Protection. Oxford: Pergamon Press; ICRP Publication 60; Ann ICRP 21:(1–3); 1991. [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Human respiratory tract model for radiological protection. Oxford: Pergamon Press; ICRP Publication 66; Ann ICRP 24:(1–3); 1994a. [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Dose coefficients for intakes of radionuclides by workers. Oxford: Pergamon Press; ICRP Publication 68; Ann ICRP 24:4; 1994b. [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Individual monitoring for internal exposure of workers. Oxford: Pergamon Press; ICRP Publication 78; Ann ICRP 27:(3–4); 1997. [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Basic anatomical and physiological data for use in radiological protection reference values. Oxford: Pergamon Press; ICRP Publication 89; Ann ICRP 32:(3–4); 2002. [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Human alimentary tract model for radiological protection. Oxford: Pergamon Press; ICRP Publication 100; Ann ICRP 36:(1–2); 2006. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . The 2007 Recommendations of the International Commission on Radiological Protection. Oxford: Pergamon Press; ICRP Publication 103; Ann ICRP 37:(2–4); 2007. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Nuclear decay data for dosimetric calculations. Oxford: Pergamon Press; ICRP Publication 107; Ann ICRP 38:3; 2008. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Adult reference computational phantoms. Oxford: Pergamon Press; ICRP Publication 110; Ann ICRP 39:2; 2009. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Occupational intakes of radionuclides: Part 1. Oxford: Pergamon Press; ICRP Publication 130; Ann ICRP 44:2; 2015. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . The ICRP computational framework for internal dose assessment for reference adults: specific absorbed fractions. Oxford: Pergamon Press; ICRP Publication 133; Ann ICRP 45:2; 2016a. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection - Occupational intakes of radionuclides: Part 2. Oxford: Pergamon Press; ICRP Publication 134; Ann ICRP 45:(3–4); 2016b. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Occupational intakes of radionuclides: Part 3. Oxford: Pergamon Press; ICRP Publication 137; Ann ICRP 46:(3–4); 2017. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Occupational intakes of radionuclides: Part 4. Oxford: Pergamon Press; ICRP Publication 141; Ann ICRP 48:(2–3); 2019. [DOI] [PubMed] [Google Scholar]
- International Commission on Radiological Protection . Occupational intakes of radionuclides: Part 5. Oxford: Pergamon Press; ICRP Publication 151; Ann ICRP 51; 2022. [Google Scholar]
- Rääf C, Barkauskas V, Eriksson Stenström K, Bernhardsson C, Pettersson HBL. Internal dose assessment of 148Gd using isotope ratios of gamma-emitting 146Gd or 153Gd in accidently released spallation target particles. Scientific Reports 10:21887; 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swedish Radiation Safety Authority . Tillståndsvillkor för avveckling av kärnkraftsreaktorer. Stockholm: Swedish Radiation Safety Authority; Diarienr: SSM2016-5866; 2017. (in Swedish). [Google Scholar]