

Abstract
Study Design:
Cohort study. Retrospective analysis of uniform billing discharge data (UB-04).
Objectives:
To compare and contrast the primary and secondary causes of hospitalization by type of admission, emergency department (ED) versus inpatient only (IP), during the first five years after the traumatic spinal cord injury (SCI).
Setting:
Academic Medical University in the Southeastern USA.
Methods:
2569 adults with traumatic SCI were identified from a population-based registry and matched to billing data. The main outcome measures were primary and secondary diagnoses associated with hospital admissions in non-federal, state hospitals.
Results:
Overall, there were 9733 hospital admissions in the five years after SCI onset, not including the initial hospitalization; 53% were admissions through the ED. The primary causes of hospitalizations after SCI varied by year post injury and admission type (ED versus IP). The top 15 secondary diagnoses included several secondary health conditions associated with SCI, as well as chronic health conditions.
Conclusions:
Rehabilitation diagnoses were much more prominent during the first year, compared with subsequent years. Septicemia was the leading cause of admissions through the ED, whereas chronic ulcer of the skin were prominent for IP only admissions. This is consistent with the acute nature of septicemia compared with more planned hospitalization for rehabilitation and skin ulcers. These conditions should be targeted for prevention strategies that include patient/family education and early and appropriate access to primary care.
Keywords: diagnoses, hospitalization, spinal cord injuries
Introduction:
Individuals with spinal cord injury (SCI) experience high rates of rehospitalization, including admissions through the emergency department (ED) or direct inpatient (IP) admissions, often for potentially preventable health conditions. Hospitalizations are not only financially costly, but they undermine the individual’s ability to participate in society, maintain employment, and preserve quality of life. Several studies have focused on identifying the causes of and risk factors for hospitalization after SCI. However, there is a disproportionate focus within the first year, there are few longitudinal analyses, and most research is based on self-report.
In the United States (US), an estimated 36% to 45% of individuals with SCI are rehospitalized within the first year.1–4 Based on data from the National Spinal Cord Injury Database, in the first year the mean total days hospitalized is 23 days.3 After the first year of injury, there is more limited data, though the number of hospitalizations and days hospitalized are reported to significantly decrease with increasing injury duration.5 Among those with chronic SCI, roughly 30% are rehospitalized yearly, and the average length of stay is 18 days.3
Based on self-report studies, 26%6 - 37%7 of individuals report at least one hospitalization in the previous year. In one study, an average of two hospitalizations and 7 days per hospitalization were reported.7 In another study of 5,146 individuals with SCI who received rehabilitation at one of the SCI Model Systems, at one-year post-injury, 30.6% of participants reported at least one hospitalization in the past year, 23.6% reported a hospitalization at 5 years post-injury, and 26.1% reported a hospitalization at 10 years post-injury.8 To date, there are limited data from administrative sources documenting hospital utilization by Americans with SCI, specifically after the first year post injury.
A considerable number of studies have assessed risk factors of utilization, finding that race/ethnicity,7–9 injury severity,2,7,10 education,7 employment,9 income,4,7 and aging7,8 are associated with hospitalizations after SCI. Recent population-based analyses of hospitalization among adults with SCI living in the US have identified other predictors of hospitalization, including prior year hospitalizations, chronic health conditions, ambulatory ability, and quality of life indicators, as well as differences in predictors based on utilization status.11–13 In an analysis of high utilizers of healthcare services, men, minorities, those with severe SCI, frequent pressure ulcers, and low income were more likely to be high utilizers.13 Clusters of conditions occurred simultaneously, rather than in isolation.
There are more limited data on the causes of hospitalization after SCI, and they are typically more grossly described as related to certain systems or conditions, rather than specific diagnoses. Furthermore, there is limited study of acute versus chronic SCI, and there has not yet been distinction between admissions through the ED versus planned or less urgent inpatient hospitalization. The most commonly reported causes include genitourinary conditions (e.g. urinary tract infections), respiratory conditions (e.g. pneumonia), musculoskeletal issues (e.g. pressure ulcers), and digestive issues.1–4,13–17 In the analysis of a small group of high utilizers, Krause et. al13 presented the primary and secondary diagnoses associated with discharges in years 2–11 post injury, noting patterns of high utilization for septicemia, other urinary tract disorders, mechanical complication of device, implant, or graft, and chronic ulcer of skin over the 10 year study period. There is a clear gap in the literature and vital need for better understanding the specific causes and patterns of hospitalization in the years after SCI onset, notably a more in-depth analysis of the primary and secondary hospital diagnoses.
Objective
Our purpose was to identify the leading primary and secondary causes of hospital admissions by type - admissions through the emergency department (ED) versus inpatient only (IP) - during the first five years after SCI.
Methods:
Participants.
Institutional review Board (IRB) approval was obtained prior to data collection and analysis. The initial cohort (n=3,995) included all state residents added to the South Carolina SCI Surveillance and Registry System (SCISRS) prior to January 1, 2015, who survived at least 1 year after the date of their earliest hospital admission for SCI. Persons who lived out of state or who may have moved from South Carolina were excluded (people with an out-of-state address on the hospital record and people with no record of South Carolina hospital utilization in the 10 years after initial injury). This left a study sample of 3,739. We focused on admission diagnoses, and we excluded those younger than 18 years old, and those with no admission during years 1–5, leaving a sample of 2,569.
Data Sources.
The South Carolina SCISRS is a population-based registry of SCI occurring in the state. All non-federal hospitals are mandated to report discharge data on hospitalizations involving SCI to the South Carolina Office of Revenue and Fiscal Affairs, Division of Health and Demographics (RFAHD) through the uniform billing discharge data (UB-04); military and VA hospitals are not included in this data. The initial SCI hospitalization record forms the basis for data contained in the SCISRS. Data are validated through verification of randomly selected medical charts and have been shown to be 99% accurate and complete. International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes of 806 [.0–.9] and 952 [.0–.9] were used to identify incident cases of SCI as defined by the Centers for Disease Control and Prevention for surveillance of SCI. Duplicate admissions were eliminated using personal identifiers. Hospitalization data (UB-04) were obtained from RFAHD.
Outcomes.
The main outcomes were primary and secondary diagnoses using the ICD-9-CM codes, condensed to the three-digit level. For several of the diagnoses, the full ICD-9-CM codes were examined to provide more detail about the diagnosis. For example, for “599” (Other disorders of urethra and urinary tract), we examined the frequency of all 599.X codes to determine that 599.0 was the most frequently used code, thus we state “Other disorders of urethra and urinary tract, primarily urinary tract infections” as a leading cause. After preliminary analysis, the causes of hospitalization in each year 2 through 5 were condensed into years 2–5.
Demographic (age, race/ethnicity, and gender) characteristics were also obtained from the SCISRS.
Data Analyses.
All data analyses were conducted using SPSS Statistics Version 27 (IBM Corp. Armonk, NY, USA). Descriptive characteristics of participants and hospitalizations are presented. Frequencies (n, %) were computed for primary and secondary diagnoses.
Results:
Over the five-year study period, there were a total of 9,733 hospital admissions, 53% of admissions occurred through the ED (n=5,220) and 46.4% were IP only (n=4,513). Among those hospitalized the average age at injury was 49.5±18.8, and the majority were male (71%) and white (57.6%). There were no significant differences in the characteristics of those admitted through the ED versus IP only. Across the study period, the total number of hospital admissions decreased, though the percentage of admissions through the ED increased. In year 1, there were 3,915 admissions, 63.2% of which were IP only. There was a total of 5,818 admissions in years 2–5, 65% of which were ED admissions.
Primary diagnoses.
In year 1, the top ten primary diagnoses accounted for 44% of all admissions (Table 1). The most frequently coded diagnosis was Care involving use of rehabilitation procedures, followed by Septicemia, and Chronic ulcer of skin. In years 2–5, the top ten diagnoses accounted for 57.5% of all admissions; the frequency of admissions for rehabilitation decreased significantly, and other conditions such as osteomyelitis, cellulitis, and episodic mood disorders entered the leading causes of admission.
Table 1.
Top 10 Primary Diagnoses for all hospitalizations (n=9,733).
| Year 1 | Years 2–5 | ||||
|---|---|---|---|---|---|
| N=3,915 | N=5,818 | ||||
| ICD-9 Diagnosis Codes | N | % | N | % | |
| V57 | Care involving use of rehabilitation procedures | 1028 | 26.3 | 131 | 2.3 |
| 038 | Septicemia | 268 | 6.8 | 613 | 10.5 |
| 707 | Chronic ulcer of skin (primarily pressure ulcers) | 162 | 4.1 | 332 | 5.7 |
| 518 | Other diseases of lung (primarily acute respiratory failure) | 131 | 3.3 | 110 | 1.9 |
| 599 | Other disorders of urethra and urinary tract (primarily urinary tract infection) | 129 | 3.3 | 340 | 5.8 |
| 996 | Complications peculiar to certain specified procedures (primarily infection and inflammatory reaction due to indwelling urinary catheter) | 121 | 3.1 | 408 | 7 |
| 721 | Spondylosis and allied disorders | 98 | 2.5 | -- | -- |
| 952 | Spinal cord injury without evidence of spinal bone injury | 91 | 2.3 | -- | -- |
| 806 | Fracture of vertebral column with spinal cord injury | 89 | 2.3 | -- | -- |
| 486 | Pneumonia, organism unspecified | 83 | 2.1 | 189 | 3.2 |
| 730 | Osteomyelitis periostitis and other infections involving bone | -- | -- | 144 | 2.5 |
| 682 | Other cellulitis and abscess | -- | -- | 103 | 1.8 |
| 296 | Episodic mood disorders | -- | -- | 102 | 1.8 |
| All other diagnoses | 1715 | 43.9 | 3346 | 57.5 | |
Notes: The top 10 diagnoses accounted for 56.1% of all primary codes listed for hospital admissions in Year 1 and 42.5% of all diagnoses in Years 2–5.
Dashes (--) are shown for diagnoses that are not in the top 10 for the given year(s); these diagnoses may still appear, however, they were not frequent enough to be included in the main diagnoses.
There were differences in the relative frequencies of diagnoses by both year and by admission type. The most frequent diagnoses associated with ED admissions in year 1 were: Septicemia, Other disorders of urethra and urinary tract, and Pneumonia (Table 2). Comparatively, the most frequent diagnoses for IP only admissions in year 1 were: Care involving use of rehabilitation procedures, Other diseases of lung, and Chronic ulcer of skin. Within the IP only admission group, rehabilitation accounted for 41.5% of admissions (Table 3).
Table 2.
Top 10 Primary Diagnoses for ED Admissions (n=5,220).
| Year 1 | Years 2–5 | ||||
|---|---|---|---|---|---|
| N= 1,439 | N= 3,781 | ||||
| ICD-9 Diagnosis Codes | N | % | N | % | |
| 038 | Septicemia | 223 | 15.5 | 544 | 14.4 |
| 599 | Other disorders of urethra and urinary tract (primarily urinary tract infection) | 99 | 6.9 | 282 | 7.5 |
| 486 | Pneumonia, organism unspecified | 67 | 4.7 | 157 | 4.2 |
| 996 | Complications peculiar to certain specified procedures (primarily infection and inflammatory reaction due to indwelling urinary catheter) | 60 | 4.2 | 313 | 8.3 |
| 707 | Chronic ulcer of skin (primarily pressure ulcers) | 58 | 4 | 135 | 3.6 |
| 560 | Intestinal obstruction without mention of hernia | 37 | 2.6 | 66 | 1.7 |
| 780 | Symptoms | 36 | 2.5 | 79 | 2.1 |
| 507 | Pneumonitis due to solids and liquids | 30 | 2.1 | -- | -- |
| 415 | Acute pulmonary heart disease | 29 | 2 | -- | -- |
| 584 | Acute kidney failure | 27 | 1.9 | -- | -- |
| 518 | Other diseases of lung (primarily acute respiratory failure) | -- | -- | 77 | 2.0 |
| 786 | Symptoms involving respiratory system and other chest symptoms | -- | -- | 68 | 1.8 |
| 682 | Other cellulitis and abscess | -- | -- | 67 | 1.8 |
| All other diagnoses | 773 | 53.6 | 1,993 | 52.7 | |
Notes: The top 10 diagnoses accounted for 46.4% of all primary ED diagnoses in Year 1 and 47.3% of all diagnoses in Years 2–5.
Dashes (--) are shown for diagnoses that are not in the top 10 for the given year(s); these diagnoses may still appear, however, they were not frequent enough to be included in the main diagnoses.
Table 3.
Top 10 Primary Diagnoses for IP only Admissions (n=4,513).
| Year 1 | Years 2–5 | ||||
|---|---|---|---|---|---|
| N= 2,476 | N= 2,037 | ||||
| ICD-9 Diagnosis Codes | N | % | N | % | |
| V57 | Care involving use of rehabilitation procedures | 1028 | 41.5 | 131 | 6.4 |
| 518 | Other diseases of lung (primarily acute respiratory failure) | 107 | 4.3 | -- | -- |
| 707 | Chronic ulcer of skin (primarily pressure ulcers) | 104 | 4.2 | 197 | 9.7 |
| 721 | Spondylosis and allied disorders | 95 | 3.8 | -- | -- |
| 952 | Spinal cord injury without evidence of spinal bone injury | 88 | 3.6 | -- | -- |
| 806 | Fracture of vertebral column with spinal cord injury | 83 | 3.4 | -- | -- |
| 996 | Complications peculiar to certain specified procedures (primarily infection and inflammatory reaction due to indwelling urinary catheter) | 61 | 2.5 | 95 | 4.7 |
| 723 | Other disorders of cervical region | 51 | 2.1 | -- | -- |
| 722 | Intervertebral disc disorders | 48 | 1.9 | 44 | 2.2 |
| 038 | Septicemia | 45 | 1.8 | 69 | 3.4 |
| 730 | Osteomyelitis periostitis and other infections involving bone | -- | -- | 89 | 4.4 |
| 296 | Episodic mood disorders | -- | -- | 79 | 3.9 |
| 599 | Other disorders of urethra and urinary tract | -- | -- | 58 | 2.8 |
| 304 | Drug dependence | -- | -- | 39 | 1.9 |
| 715 | Osteoarthrosis and allied disorders | -- | -- | 38 | 1.9 |
| All other diagnoses | 766 | 30.9 | 1,198 | 58.8 | |
Notes: The top 10 diagnoses accounted for 69.1% of all primary IP diagnoses in Year 1 and 41.2% of all diagnoses in Years 2–5.
Dashes (--) are shown for diagnoses that are not in the top 10 for the given year(s); these diagnoses may still appear, however, they were not frequent enough to be included in the main diagnoses.
In years 2–5, the percentage of ED admissions increased, and there were differences in diagnoses by admission type (Tables 2 and 3). The most frequent primary diagnoses associated with ED admissions were Septicemia, Complications peculiar to certain specified procedures, and Other disorders of urethra and urinary tract. Other diagnoses emerged in the top 10, including Other diseases of lung, Symptoms involving respiratory system and other chest symptoms, and Other cellulitis and abscess. For IP admissions, the most frequent diagnoses were Chronic ulcer of skin, Care involving use of rehabilitation procedures, and Complications peculiar to certain specified procedures.
Secondary diagnoses.
There are also notable differences in secondary diagnoses by year and admission type (Figure 1). When reviewing the secondary diagnoses, it is important to acknowledge that up to 14 diagnoses could be listed per admission (as opposed to only one primary diagnosis), therefore, the results present the percentage of ED or IP hospitalizations that included the given secondary diagnosis in the given timeframe.
Figure 1.
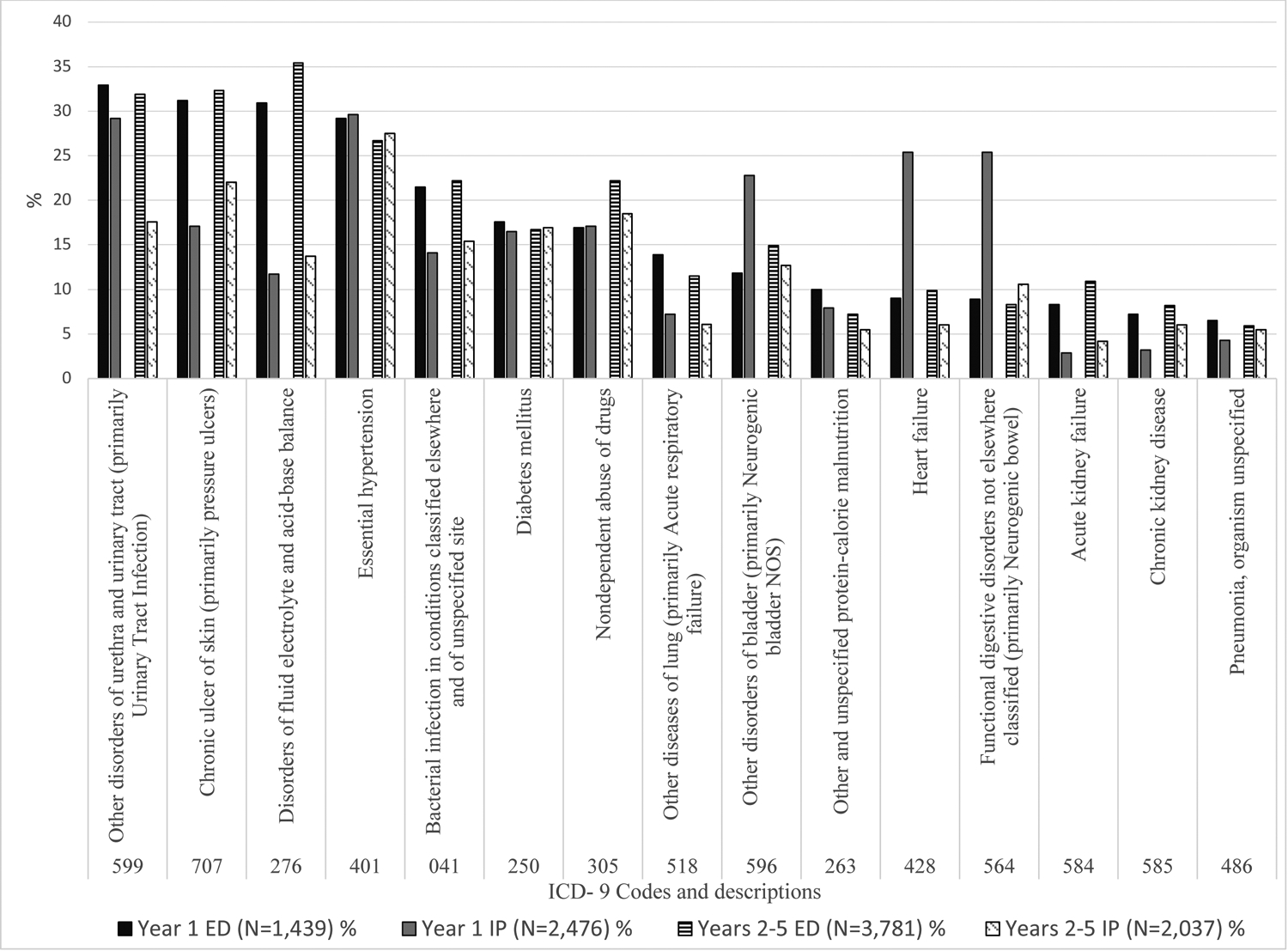
Most frequent secondary diagnoses for ED admissions and IP admissions, by year post injury (%).
Notes: Excludes secondary diagnoses specific to SCI, including 344, 806, 952, and 907.
The column percentages will not sum to equal zero, as each admission could list up to 14 secondary diagnoses. The percentages shown are percent for each category (ED admissions or IP admissions). For interpretation, “Other disorders of urethra and urinary tract” was listed as a secondary diagnosis in 33% of Year 1 ED admissions.
For ED hospitalizations across all years, the most frequent secondary diagnoses were: Other disorders of urethra and urinary tract (31.9% and 31.9%), Chronic ulcer of skin (31.2% and 32.3%), and Disorders of fluid electrolyte and acid-base balance (30.9% and 35.4%). For IP admissions, the most frequent secondary diagnoses in year 1 included essential hypertension (29.6%), other disorders of urethra and urinary tract (29.2%), heart failure and functional digestive disorders (25.4%). In years 2–5, the leading secondary diagnoses were essential hypertension (27.5%), chronic ulcer of skin (22%), and Nondependent abuse of drugs (18.5%).
Discussion:
These unique contributions are threefold: (1) presentation of specific ICD-9 diagnosis codes related to hospitalizations in the first five years after SCI, (2) distinction between hospital admission through the ED versus IP only, and (3) the use of billing data that allows for the identification of the primary and up to 14 secondary diagnoses.
By examining hospitalizations in year 1 separately from years 2–5, we are able to highlight important differences and the unique medical needs of individuals with acute and chronic SCI. Additionally, by differentiating between type of admissions, we are able to obtain a clearer picture of the medical conditions necessitating admission through the ED as opposed to IP only. By increasing our understanding of hospitalizations after SCI, we will be able to better develop strategies for treatment, management and prevention.
The first year after SCI is often considered within the acute phase after injury, in which distinct differences in neurorecovery, secondary complications, and health outcomes, including hospitalization have been observed.1 Based on data from the SCI Model Systems, the causes of rehospitalization in the first year after injury have been broadly defined as related to the genitourinary system, respiratory system, and skin and subcutaneous tissue.1,4 Our findings generally support these findings, though we also highlight rehabilitation and septicemia as key causes. In addition, we reveal differences in the primary diagnoses by admission type. In year 1, septicemia, other disorders of urethra and urinary tract (primarily urinary tract infections), and pneumonia were the leading causes of ED admissions, while rehabilitation, diseases of the lung (primarily acute respiratory failure), and chronic ulcers of the skin (primarily pressure ulcers) were the leading causes of IP admissions.
There is little published data on the causes of hospitalizations among those with chronic SCI living in the United States, and our findings provide a unique glimpse into health conditions affecting these individuals. The finding of an increase in the ED admissions in subsequent years raises concerns about the medical needs management of those with chronic SCI, as most ED admissions are for acute causes, many of which are preventable. While the data from the SCI Model Systems3,4 show the causes of hospitalization over time in 5-year increments, up to 45 years post injury, the causes are broadly classified, lacking the specific hospital billing diagnoses that may provide medical professionals, caregivers, and those with SCI with more information about the specific health conditions that may result in costly hospital utilization.
For example, diseases of the genitourinary system are reported as the leading cause of hospitalization, representing 28% of 3,227 hospitalizations in year 5 post injury,3 but the specific medical needs are not well known. In our analysis, we found that admissions associated with the genitourinary system are frequent in years 2–5, but are not the leading cause of utilization. Specifically, we found that “Complications peculiar to certain specified procedures,” which were primarily coded as “infection and inflammatory reaction due to indwelling urinary catheter” accounted for 8.3% of ED admissions, and “Other disorders of urethra and urinary tract,” primarily “urinary tract infection” diagnoses accounted for 7.5% of ED admissions; both of these increased as relative percentages of ED admissions from year 1 to years 2–5. Contrarily, these diagnoses were much less frequent causes of IP admissions.
By assessing ED related hospitalizations, which are generally related to urgent conditions that necessitate further care separately from IP hospitalizations, which may be planned for a less severe medical needs, we reveal different sets of health conditions and ultimately underscore the importance of coordinated care. These findings may bring awareness to individuals with SCI, caregivers, and providers to better manage and monitor symptoms to avert an ED admission.
Rather than just assessing the primary causes of hospitalization, as has been done in the previous literature, we also examined the secondary causes. Although we present only frequencies of individual secondary diagnoses per admission and did not examine clusters of concurrent primary and secondary diagnoses, we highlight some important medical conditions that may frequently co-exist. To our knowledge, there is no other study that has summarized secondary diagnoses, and the findings help to highlight important co-existing conditions and the medical needs of those with SCI. Notably, we found two chronic conditions, essential hypertension and diabetes mellitus, were consistently coded as secondary diagnoses, both over time and by admission type. In both year 1 and years 2–5, the greatest difference between secondary diagnoses coded for ED versus IP admissions was observed in the relative frequency of disorders of fluid electrolyte and acid-base balance. A much larger percentage of those admitted through the ED presented with this condition. Overall, there was less change over time in the relative frequency of secondary diagnoses associated with ED hospitalizations; several of the secondary diagnoses associated with IP admissions were found to decrease in years 2–5 compared to year 1.
Taken together, the findings provide a better understanding of the health conditions necessitating hospitalization, and may be helpful for developing prevention strategies, management techniques, and determining appropriate avenues of care for those with SCI. For example, we found that individuals with SCI are presenting to the ED and being admitted for potentially preventable conditions including septicemia, urinary tract infections, complications related to catheters, and pneumonia, all serious health issues that may be avoided with proper care or education. The ED related hospitalizations suggest a lack of successful management these expected sequelae. Focused care coordination or enhanced rehabilitation services that might result in improved disease management in years 2–5, just as the percentage of ED admissions increases.
Limitations
The current study is a retrospective analysis of UB-04 discharge data and several limitations should be acknowledged. We assessed diagnoses for admissions that occurred in South Carolina non-federal hospitals in years 1–5 after injury, not individual clinical data. The data included admission records from rehabilitation and long-term acute hospitals in SC. While this provided a more complete picture of hospital utilization, inclusion of rehabilitation might obscure more acute or emergent needs. Data for admissions to hospitals in federal (e.g., VA hospitals), or nearby states are not captured. To minimize selection bias, we focused on the relative frequency of diagnoses, assuming that SCI patients with a particular diagnosis might not be more likely to seek care (especially ED care) from an out-of-state hospital. Additionally, although we present the most frequent primary and secondary diagnoses for hospital admissions, there are considerably more diagnoses that could be considered. It is important to note that in the United States healthcare system, reported diagnoses may be influenced by payer reimbursement policies. Our findings may not be generalizable outside of the US, where differences in healthcare systems, insurance, and access, just to name a few, may affect the course of treatment and management, and ultimately need for emergent or planned hospitalization.
Future directions
There are several considerations for future research or care that may mitigate the risk of rehospitalizations after SCI. First, it is important to understand the diagnoses related to hospitalization, including syndromes or clusters of health conditions that may impact those with SCI, as well as the associated risk factors. Further study of the causes of hospital utilization, including assessment of personal, demographic, and injury characteristics associated with the leading causes may enable providers, caregivers, and individuals with SCI to better monitor and manage health conditions that are associated with the need for hospitalization. Building on our findings, the field would benefit from more focused study of the most common diagnoses – for example, an analysis of the factors associated with ED septicemia admissions or IP pressure injury admissions for among those with chronic SCI. More detailed cost analyses would also add to the body of literature and facilitate a better understanding of the true burden of these health conditions. Future study excluding rehabilitation causes of admissions (which may obscure other causes of IP admissions) or focused solely on rehabilitation admissions and outcomes may provide a clearer picture of the needs of these individuals.
In terms of clinical implications, the relationship between access to primary care or improved disease management at the primary care level and these admissions needs to be explored. Also, the role of care coordination and rehabilitation services in improving patient/caregiver education and disease management should be considered.
Conclusions
There were differences in the causes of ED admissions and IP admissions within the first 5 years after SCI. Notably, the causes of ED visits were frequently for acute, potentially preventable secondary health conditions. IP admissions varied more by time since injury and were more often related to rehabilitation and chronic secondary health conditions. To mitigate the risk and burden of future hospitalization, these conditions should be targeted for prevention strategies that include patient/family education as well as early and appropriate access to care.
Funding
The contents of this publication were developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) grant numbers 90IFRE0028 and 90IF0119, and the South Carolina Spinal Cord Injury Research Fund (SCIRF) grants SCIRF 2017 SI-02. NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this publication do not necessarily represent the policy of NIDILRR, ACL, HHS, or the SCIRF, and you should not assume endorsement by the Federal Government or the state of South Carolina.
List of Abbreviations
- SCI
Spinal cord injury
- SCISRS
SCI Surveillance and Registry System
- RFAHD
Office of Revenue and Fiscal Affairs, Health, and Demographics
- UB-4
Uniform billing discharge data
- US
United States
Footnotes
Data Archiving
The data sets generated and/or analyzed during the current study are not publicly available due to the privacy concerns of study participants and are not standardized to be in a publicly interpretable format.
Statement of Ethics
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Conflicts of Interest
The authors have no conflict of interest to disclose.
References:
- 1.DeJong G, Tian W, Hsieh CH, Junn C, Karam C, Ballard PH, et al. Rehospitalization in the first year of traumatic spinal cord injury after discharge from medical rehabilitation. Arch Phys Med Rehabil. 2013;94(4 Suppl):S87–97. [DOI] [PubMed] [Google Scholar]
- 2.Skelton F, Hoffman JM, Reyes M, Burns SP. Examining health-care utilization in the first year following spinal cord injury. J Spinal Cord Med. 2015;38(6):690–695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.National Spinal Cord Injury Statistical Center. 2020 Annual Statistical Report for the Spinal Cord Injury Model Systems Public Version. Birmingham, AL: University of Alabama at Birmingham;2020. [Google Scholar]
- 4.Cardenas DD, Hoffman JM, Kirshblum S, McKinley W. Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil. 2004;85(11):1757–1763. [DOI] [PubMed] [Google Scholar]
- 5.Charlifue S, Lammertse D, Adkins R. Aging with spinal cord injury: changes in selected health indices and life satisfaction. Arch Phys Med Rehabil. 2004;85:1848–1853. [DOI] [PubMed] [Google Scholar]
- 6.Noonan VK, Fallah N, Park SE, Dumont FS, Leblond J, Cobb J, et al. Health care utilization in persons with traumatic spinal cord injury: the importance of multimorbidity and the impact on patient outcomes. Top Spinal Cord Inj Rehabil. 2014;20(4):289–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Krause JS, Saunders LL. Risk of hospitalizations after spinal cord injury: relationship with biographical, injury, educational, and behavioral factors. Spinal Cord. 2009;47(9):692–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mahmoudi E, Meade MA, Forchheimer MB, Fyffe DC, Krause JS, Tate D, et al. Longitudinal analysis of hospitalization after spinal cord injury: variation based on race and ethnicity. Arch Phys Med Rehabil. 2014;95(11):2158–2166. [DOI] [PubMed] [Google Scholar]
- 9.January AM, Zebracki K, Czworniak A, Chlan KM, Vogel LC. Predictive factors of hospitalization in adults with pediatric-onset SCI: a longitudinal analysis. Spinal Cord. 2015;53(4):314–319. [DOI] [PubMed] [Google Scholar]
- 10.Eastwood E, Hagglund K, Ragnarsson K, Gordon W, Marino R. Medical rehabilitation length of stay and outcomes for persons with traumatic spinal cord injury. Arch Phys Med Rehabil. 1999;80:1457–1463. [DOI] [PubMed] [Google Scholar]
- 11.DiPiro ND, Murday D, Corley B, Krause JS. The association between participation and quality of life indicators with hospitalizations in ambulatory adults with spinal cord injury. Spinal Cord, 2020. Nov;58(11):1150–1157. doi: 10.1038/s41393-020-0461-3. Epub 2020 Apr 27. [DOI] [PubMed] [Google Scholar]
- 12.DiPiro ND, Murday D, Corley EH, Krause JS. Prevalence of chronic health conditions and hospital utilization in adults with spinal cord injury: an analysis of self-report and South Carolina administrative billing data. Spinal Cord. 2019;57(1):33–40. [DOI] [PubMed] [Google Scholar]
- 13.Krause JS, Murday D, Corley EH, DiPiro ND. Concentration of Costs Among High Utilizers of Health Care Services Over the First 10 Years After Spinal Cord Injury Rehabilitation: A Population-based Study. Arch Phys Med Rehabil. 2019;100(5):938–944. [DOI] [PubMed] [Google Scholar]
- 14.Hammond FM, Horn SD, Smout RJ, Chen D, DeJong G, Scelza AJ, et al. Acute rehospitalizations during inpatient rehabilitation for spinal cord injury. Arch Phys Med Rehabil. 2013;94(4 Suppl):S98–105. [DOI] [PubMed] [Google Scholar]
- 15.Savic G, Short DJ, Weitzenkamp D, Charlifue S, Gardner BP. Hospital readmissions in people with chronic spinal cord injury. Spinal Cord. 2000;38(6):371–377. [DOI] [PubMed] [Google Scholar]
- 16.Dorsett P, Geraghty T. Health-related outcomes of people with spinal cord injury--a 10 year longitudinal study. Spinal Cord. 2008;46(5):386–391. [DOI] [PubMed] [Google Scholar]
- 17.Jaglal SB, Munce SE, Guilcher SJ, Couris CM, Fung K, Craven BC, et al. Health system factors associated with rehospitalizations after traumatic spinal cord injury: a population-based study. Spinal Cord. 2009;47(8):604–609. [DOI] [PubMed] [Google Scholar]