

Abstract
Introduction:
Suicide is a leading cause of death. One challenge to prevention efforts is the wide phenomenological heterogeneity in suicidal urges, thoughts, and behaviors across individuals at risk. Despite this heterogeneity, most suicide research estimates group-level effects by averaging across people as if they were the same, preventing detection of person-specific factors that may modulate risk and be key to effective prevention. The goal of the present study is to illustrate the idiographic (i.e., person-specific) approach and highlight its utility for suicide research.
Methods:
We implemented a case series approach using three cases from a sub-set of psychiatrically hospitalized adolescents who provided intensive longitudinal data on daily urges and coping behavior after discharge following a suicide attempt. For illustration, person-specific, bidirectional links between suicidal urges and coping behavior were modeled across a series of cases using a vector autoregression approach.
Results:
The relationship between suicidal urges and coping differed across the three individuals, who were presented to exhibit the range of this variability in the presence/absence and magnitude of effects.
Conclusions:
Individuals who report similar suicidal risk levels likely respond in individualized ways to suicidal urges (e.g., use different coping strategies), necessitating personalized assessment and treatment. We discuss implications for future suicide research.
Keywords: developmental psychopathology, ecological momentary assessment, idiographic methods, precision medicine, suicide
INTRODUCTION
Suicide is the 2nd leading cause of death among the United States youth ages 12–19 (CDC, 2020), and the 2nd leading cause of death globally among individuals ages 15–29 years (World Health Organization, 2018). From 2000 to 2017, the rate of suicide deaths among U.S. youth ages 15–19 increased by 47% (Miron et al., 2019). Although the initial reports on the mental health consequences of the COVID-19 pandemic and associated public health measures are mixed (Bryan et al., 2020), there is some emerging evidence suggesting further increases in the rate of suicidal ideation for young adults 18–24 years old (Czeisler et al., 2020). These increasing rates of mortality and ideation are despite decades of research aimed at identifying risk factors and a growing body of research aimed at decreasing the prevalence of suicidal thoughts and behaviors (STBs).
Suicidal thoughts and behaviors vary across people in their phenomenology (i.e., frequency, duration, and intensity; Bryan & Rudd, 2015; Huang et al., 2017) and appear to be multiply determined (Kuehn et al., 2019), with no clear evidence of a single causal pathway. Recent analyses have highlighted variability in the group-level trajectories of both STB phenomena and their risk factors over time (Allan et al., 2019; Bagge et al., 2017; Czyz & King, 2015; King, Brent, et al., 2019; Kleiman et al., 2017). Identifying and reducing risk for specific individuals across this heterogeneous group necessitates insight about not only individual-level variation in phenomenology but in the predictive associations that may account for that variation (i.e., person-specific effects).
Unfortunately, most statistical procedures employed across these studies and in suicide research more broadly, apply a common cause approach by estimating average, group-level (i.e., nomothetic) effects that draw single inferences intended to apply to the entire population under study (Molenaar, 2004; Molenaar & Campbell, 2009). A nomothetic inference, for example, could involve testing whether the use of a specific coping strategy predicts reduction in suicidal urge, on average. Yet, person-to-person differences (i.e., individual-level heterogeneity) in the presence, magnitude, and direction of the association between STBs and their risk factors are also important to consider.
The most common approaches to considering individual-level heterogeneity in STBs are individual differences models, including multilevel models with random effects. These are intended to capture group-level, phenomenological differences (i.e., who has more risk or what modulates risk at what level). Yet, group-level approaches like these retain assumptions of inter-individual homogeneity (e.g., ergodicity). For example, multilevel models with random effects are routinely expected to account for individual-level variation in group-level effects. Even when random effects are estimated, primary inferences are most often derived from the average/fixed effects. Mathematically, random effects parameterize the between-person variance in an effect under the assumption that both the probability of detecting the effect and the degree of measurement error is equally for all individuals. Furthermore, as they derive variance from group-level estimation procedures, random effects do not estimate patterns of person-specific heterogeneity most needed for applying evidence to the individual patient in crisis.
A growing body of idiographic work—along with the suicide risk-specific case illustrations we present here—demonstrates that person-to-person differences in the presence of many psychological effects limit the individual-level generalizability of nomothetic research (Borkenau & Ostendorf, 1998; Fisher et al., 2018; Wright et al., 2015). Some individuals simply do not exhibit some effects that are relevant to others. Consequently, person-specific models of predictive relationships (i.e., whether the same level of risk is more likely to have the same potency for different people) may be especially valuable for improving the individual-level precision of nomothetic research (Wright et al., 2015; Wright & Woods, 2020).
While idiographic methods are broadly applicable to psychological research, they could be especially important for suicide research where individual phenomenological differences in STBs are observed (e.g., some individuals may report more frequent STBs while others have less frequent but more intense STBs). For example, if distraction is found to reduce suicidal urge on average, the corresponding nomothetic inference suggests that all, or at least most, individuals should experience a reduction in urge when using distraction to cope. Yet, this research does not provide a strong test of whether this effect is either true or meaningful for all individuals sampled. Even when including a covariate that attempts to account for phenomenological variation (e.g., average intensity or frequency), the covariate effects are also assumed to have a uniform influence in all individuals.
Expanding the repertoire of STB methods to include idiographic approaches also has translational import for defining actionable targets for people in crisis. A nomothetic framework—even one that accounts for random between-person effects—provides solutions with uncertain value for understanding or predicting the behavior of the individual in crisis (i.e., to what degree does response to a coping strategy vary across people?) while an idiographic one affords a shift to something more personalized (e.g., which coping strategies are effective for this person?). Study of suicide risk using nomothetic approaches may highlight the person-specific nature of its causes or yield person-specific solutions needed to address individuals in crisis.
A better understanding of what works for whom (Norcross & Wampold, 2011), and how individuals vary in their proximal risk of suicide and responsiveness to core components of treatment, is a critical step forward for streamlining and tailoring interventions and maximizing their effectiveness across individuals. Coping strategies are thought to play an essential role in mitigating risk for suicide and are, consequently, a common target of many suicide-related interventions (Linehan, 1993; Neacsiu et al., 2010; Stanley et al., 2009). For example, safety planning, a brief evidence-based intervention (Stanley & Brown, 2012), emphasizes identifying suicide warning signs, increasing capacity for effective coping, and restricting access to lethal means (Stanley & Brown, 2012). Although the decision about which coping strategies are incorporated into safety planning for whom is a collaborative process driven by individual clients’ needs, there is limited evidence regarding the extent to which coping strategies typically incorporated into safety planning work effectively for everyone. Recent nomothetic findings from intensive longitudinal data (ILD) highlight the strong association between coping and STBs, with certain strategies (i.e., distraction and positive activities) associated with a lower risk of STBs at the next time point (Stanley et al., 2021).
On the other hand, applying idiographic methods to the same type of data would allow for the understanding of both (1) individual-level variability in the population (i.e., for what proportion of people are certain coping strategies helpful?) and (2) what is helpful for the person presenting at the clinic for services. Answers to these questions would enable greater personalization of safety plans. For example, clinicians often suggest youth distract themselves to manage high-risk periods; however, this strategy is not likely effective for all youth and in all contexts (i.e., some youth may use distraction as an avoidance technique, leading to increases in mental health symptoms and subsequent suicide risk). Nomothetic models ignore these nuances and assume findings generalize down to the individual level (i.e., a specific strategy is helpful for all high-risk youth). In circumstances such as the example just presented, this could be an iatrogenic assumption.
The overarching aim of the present paper is to illustrate one application of the idiographic approach in the context of STB research. To achieve this study objective, we focus on person-specific variability in associations between STBs, coping strategies, and ability to refrain from suicidal action in a sample of adolescents at elevated suicide risk in the month following a psychiatric hospitalization. We focused on self-efficacy to refrain from suicidal action in addition to coping strategies as a function of prior nomothetic research linking self-efficacy to prospective suicide risk (Czyz, Horwitz, Arango, et al., 2016). Critically, we use an especially phenomenologically homogenous sample to provide an especially strong test of person-specific heterogeneity (i.e., where it would not be expected). We first present a case series analysis of idiographic models, highlighting person-specific effects for three exemplar individuals. Second, we discuss how these methods can guide future STB research directions.
METHOD
To illustrate the application of nomothetic approaches, we use data from participants who are phenomenologically similar in their high degree of risk and examine associations between STBs and coping behavior. The analytic approach and results are reviewed in the style typical of a research report to model how these methods can be discussed in a traditional format.
Participants
Participants were psychiatrically hospitalized youth ages 13–17 years old and recruited to participate in a brief psychosocial intervention pilot trial (Czyz et al., 2019). Eligible participants were hospitalized due to suicidal ideation in the past week or a suicide attempt in the past month. Individuals were excluded from the pilot study based on the presence of cognitive impairment or altered mental status (mania, psychosis), transfer to a more intensive form of care (e.g., medical unit or residential facility), unavailability of a guardian (ward of state), or not owning a cell phone with text messaging capabilities. Out of the 47 eligible adolescents, 36 (76.6%) agreed to participate in the pilot trial. Thirty-four participants took part in the ILD portion of the study (1 participant withdrew from the study, and 1 did not complete any ILD assessments).
Eleven of the 34 individuals provided data for more than 50% of the days and experienced more than five suicidal urges over the course of the 28-day observation period. Three of these participants are highlighted below and were chosen to ensure idiographic heterogeneity in effects. Given the high degree of homogeneity in STB phenomenology across these individuals (i.e., all recently hospitalized for suicide risk, high compliance with daily surveys, and similar STB frequency in the same period), it is reasonable to assume—consistent with traditional approaches—that variability in person-specific effects would be low. More specifically, using an ostensibly homogenous set of individuals reduces the chances that the heterogeneity in effects detected would be attributable to phenomenological differences.
Procedures
Following discharge from the psychiatric unit, participants responded to daily surveys, using an online link sent via text messages, regarding their STBs and coping styles over a 28-day period. Participants were given up to 1.5 h to respond to the surveys. Additional details about the daily survey protocol are described elsewhere (Czyz et al., 2018). All procedures were approved by an institutional review board.
Measures
Suicidal urges: Participants who each day responded affirmatively to the question assessing presence of suicidal thoughts (“At any point in the last 24 hours, did you have any thoughts of killing yourself?”) were asked to rate the intensity of their suicidal urge (“How strong was the urge to act on your thoughts of suicide?”) using a 7-point scale ranging from 1 (low) to 7 (high). Participants who denied thoughts of suicide in the past 24 hours were not asked about suicidal urges. Thus, the suicidal urge variable was scored 0 through 7 where 0 represented the absence of suicidal urge. This item was modeled after an item assessing urge to engage in self-injurious behaviors in another ILD study (Nock et al., 2009).
Coping strategies: Participants who reported thoughts of suicide were asked, “When you had thoughts of killing yourself in the last 24 hours, did you do any of these things to deal or cope with your thoughts?” Participants who did not report any suicidal ideation in the past 24 hours were asked about coping in reference to coping with feelings or stressful events (i.e., “In the last 24 hours, did you do any of these things to deal or cope with your feelings or any stressful situations?). The coping behaviors assessed were consistent with internal and external coping strategies typically included on safety plans (King et al., 2013; Stanley & Brown, 2012). Thus, we identified coping behaviors that mapped onto recommended strategies for coping with suicidal urges or warning signs.
The eight coping behaviors measured were as follows: (1) talked to a family member; (2) talked to a friend or another support person; (3) talked to a therapist, counselor, or doctor; (4) contacted a crisis line; (5) tried to distract self with something else; (6) tried to relax or do something comforting; (7) tried to tell self-something calming or positive; and (8) tried a cognitive strategy that involved either (a) thinking about reasons for living (on days suicidal ideation was endorsed) or (b) thinking differently about the situation (on days when ideation was not endorsed). Responses were dichotomized (0 = No, 1 = Yes) to reflect whether a coping strategy was used. The distraction and relaxation items (5 & 6) were combined and dichotomized to reflect emotion-focused coping due to the strong correlation between the two items. We also calculated two variables based on these responses: (1) Sum of coping strategies, calculated by summing across all strategies to reflect the range of strategies tried each day; and (2) a 3-day average of summed strategies to reflect an individual’s consistent efforts to cope using multiple strategies.
Self-efficacy to refrain from suicidal action: Participants were asked, “How confident are you that you will be able to keep yourself from attempting suicide” with response options ranging from 0 (Not at all confident) to 10 (Completely confident). This item was adapted from the Self-Assessed Expectations of Suicide Risk Scale (Czyz, Horwitz, & King, 2016).
Analytic strategy
We used within-person vector autoregression, a foundational component of many idiographic methods to examine person-specific associations between coping strategies, coping self-efficacy, and suicidal urges. In modeling person-specific effects, data from each person were analyzed separately. Vector autoregression simultaneously models autoregressive effects (Xt−1 → Xt; Yt−1 → Yt) as well as bidirectional lagged associations between two variables (Xt−1 → Yt; Yt−1 → Xt). VAR models thus estimate the prospective influence of one time series variable on another after accounting for the stability in both factors (i.e., consistency in one factor from one day to the next). Multiple models were fit to test for Granger causality (Shukur & Mantalos, 2000) between suicidal urge and each coping strategy and between suicidal urge and efficacy. Granger causality is a forecasting tool that tests for the predictive utility of one variable (X) on another (Y) and therefore useful in determining whether previous values of X provide useful information in estimating future values of Y.
To account for missing data, we used a full imputation approach (Ji et al., 2016).1 Of the three participants analyzed, the average dataset was missing 2.67 responses (compliance rate = 96.43%; range = 82–100%). Following imputation, splines were used to interpolate values and detrend as per convention for ensuring stationarity (Fisher et al., 2017; Piccirillo et al., 2019). Standardized residuals from the detrended models were used in final analyses. We used the “mice” package in R (R Core Team, 2013) for full imputation and the “vars” package (Pfaff, 2008) for VAR models. Randomly generated data based on the present study and tutorial R scripts to run these models are available online (https://github.com/kskuehn/Idiographic-VAR.git).
RESULTS
To provide an illustration of the idiographic analytic approach, we examined bidirectional relations between suicidal urge and coping behavior on the same day. See Table 1 for full results from these models. Three individual-level models (i.e., Person 1, 2, and 3) are described in detail below to highlight between-person heterogeneity in the pattern of associations between suicidal urge and coping behaviors and suicidal urge and self-efficacy to refrain from suicidal behavior. Trajectories in suicidal urge over the course of the study for each of the participants are plotted in Figure 1. An abbreviated selection of models for these three individuals is presented in Figure 2 to facilitate understanding of both the model and the heterogeneity in effects.
TABLE 1.
Idiographic results from vector autoregressive (VAR) models of urge predicting immediate coping
| Person # | Coping variable | F-test (df) | Granger causality p-valuea | SI urge predicting copingb | Coping ARb | Constantc | Coping predicting SI urge | SI urge AR | Constantc |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Talk Family | 5.37 (1,102) | 0.02* | 0.38* | −0.08 | 0.02 | −0.24* | 0.57*** | −0.01 |
| Talk MH | 13.60 (1,102) | <0.001*** | 0.67*** | −0.19 | 0.02 | −0.25** | 0.63*** | 0.01 | |
| Thought | 1.75 (1,102) | 0.19 | −0.21 | −0.04 | 0.05 | 0.07 | 0.52*** | 0.01 | |
| Thinking | 0.61 (1,102) | 0.44 | −0.14 | −0.04 | −0.04 | 0.03 | 0.51*** | −0.01 | |
| Talk Friend | 6.98 (1,102) | <0.01** | 0.49* | −0.04 | −0.03 | −0.17* | 0.54*** | 0.01 | |
| Emotionc | 0.20 (1,102) | 0.66 | −0.07 | 0.01 | −0.04 | −0.01 | 0.50*** | −0.01 | |
| Coping sum | 15.30 (1,102) | <0.001*** | 0.43*** | 0.12 | −0.02 | −0.44** | 0.65*** | 0.01 | |
| Efficacy | 5.77 (1,102) | 0.02* | 0.31* | 0.57*** | −0.05 | −0.40** | 0.43*** | 0.02 | |
| 3 Day Avg. | 0.05 (1,102) | 0.81 | −0.02 | −0.06 | −0.04 | −0.02 | 0.50*** | −0.01 | |
| 2 | Talk Family | 6.97 (1,102) | <0.01** | −0.34* | −0.04 | −0.01 | 0.12 | 0.38** | 0.02 |
| Talk MH | 0.58 (1,102) | 0.45 | −0.15 | −0.02 | 0.00 | 0.06 | 0.38** | 0.01 | |
| Thought | 2.57 (1,102) | 0.11 | −0.23 | 0.00 | 0.04 | 0.21 | 0.37** | 0.01 | |
| Thinking | 2.60 (1,102) | 0.11 | −0.31 | 0.01 | −0.01 | 0.19* | 0.35** | 0.02 | |
| Talk Friend | 0.17 (1,102) | 0.68 | −0.08 | 0.00 | −0.02 | 0.00 | 0.37** | 0.01 | |
| Emotionc | 1.02 (1,102) | 0.32 | −0.16 | −0.01 | −0.03 | 0.09 | 0.37** | 0.02 | |
| Coping sum | 8.25 (1,102) | <0.01** | −0.31** | 0.41** | 0.02 | 0.26 | 0.36** | 0.01 | |
| Efficacy | 0.52 (1,102) | 0.47 | 0.10 | 0.22 | 0.00 | 0.00 | 0.37** | 0.01 | |
| 3 Day Avg. | 0.17 (1,102) | 0.68 | −0.03 | −0.09 | −0.01 | 0.14 | 0.37** | 0.01 | |
| 3 | Talk Family | 0.75 (1,102) | 0.39 | −0.24 | 0.02 | −0.05 | 0.09 | 0.38** | −0.03 |
| Talk MH | 0.25 (1,102) | 0.62 | −0.12 | 0.00 | −0.04 | 0.03 | 0.40** | −0.03 | |
| Thought | 0.04 (1,102) | 0.84 | 0.00 | 0.04 | −0.02 | 0.17 | 0.39** | −0.03 | |
| Thinking | 0.61 (1,102) | 0.44 | 0.14 | 0.01 | −0.04 | −0.07 | 0.40** | −0.03 | |
| Talk Friend | 3.43 (1,102) | 0.07 | 0.37 | −0.04 | −0.01 | −0.07 | 0.42*** | −0.03 | |
| Coping sum | 0.04 (1,102) | 0.86 | −0.03 | 0.40*** | −0.01 | −0.03 | 0.39** | −0.01 | |
| Efficacy | 3.90 (1,102) | 0.051 | −0.28 | 0.28* | −0.01 | 0.35*** | 0.44*** | −0.01 | |
| 3 Day Avg | 1.46 (1,102) | 0.23 | −0.21 | −0.15 | −0.06 | 0.21* | 0.45*** | −0.02 |
Granger Causality Test results with suicidal urge modeled as the cause and coping strategy as the dependent variable.
Coefficients are standardized.
Emotion-focused coping: Distraction and relaxation variables are combined.
p < .05;
p < .01;
p < .001.
FIGURE 1.
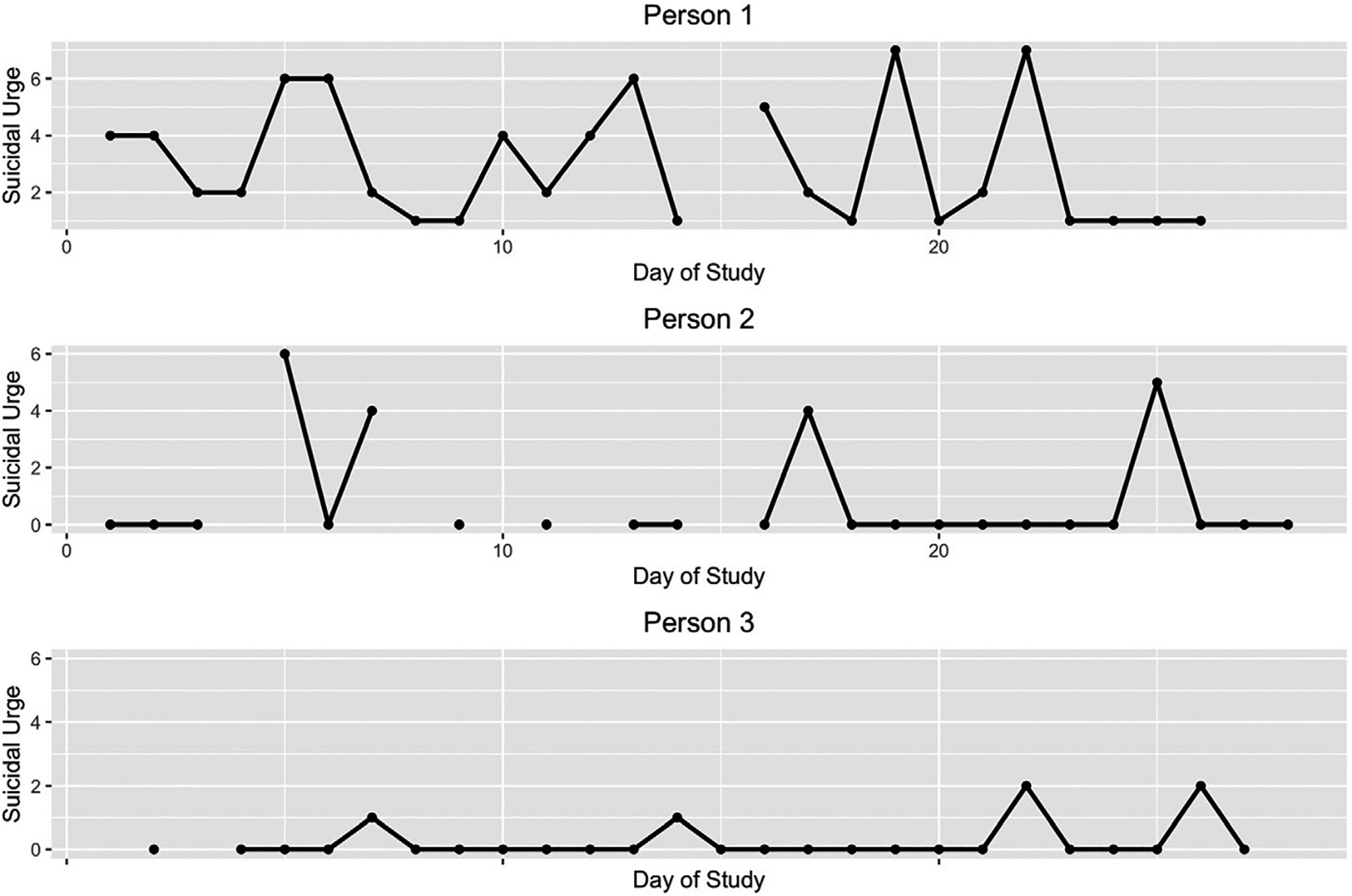
Suicidal urges over the duration of the 28-day study period for each of the three individuals. *Notes: Missing values are deleted. VAR models include imputed and interpolated values which are not depicted in these graphs
FIGURE 2.
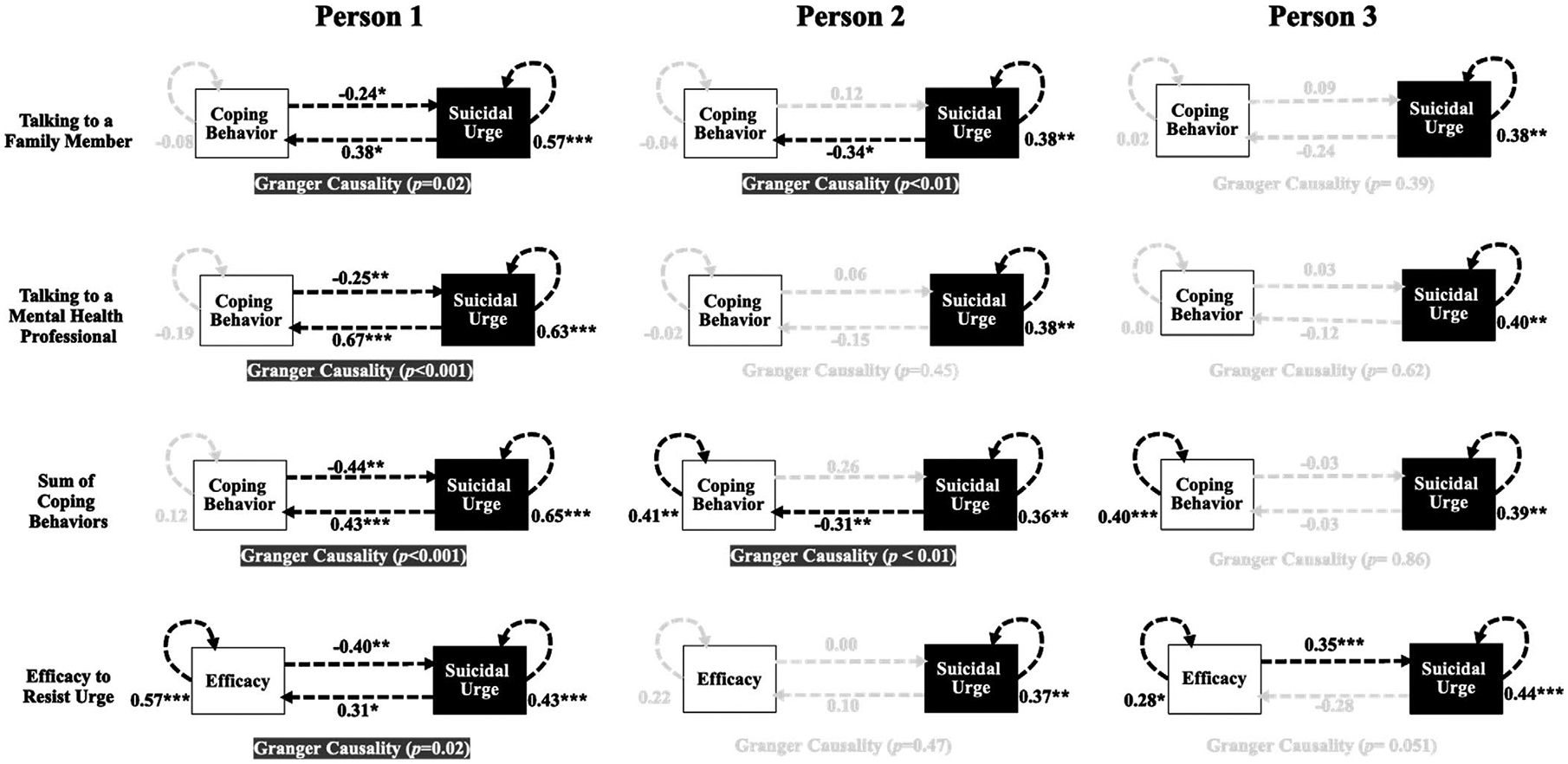
Exemplary vector autoregressive (VAR) models for three individuals with standardized coefficients
For Person 1, same day suicidal urge was related to reaching out to a mental healthcare provider (F = 13.60 (df = 1,102), β = 0.67, p < 0.001, R2 = 0.18). Specifically, a one standard deviation increase in Person 1’s suicidal urge was associated with a 0.67 standard deviation increase in the likelihood of Person 1 reaching out to a mental healthcare provider that same day, after accounting for the stability in both urge and this strategy use. Variation in suicidal urge explained 18% of the variance in Person 1 reaching out to a mental healthcare provider. Additionally, a bidirectional effect was present for Person 1 such that reaching out to a mental health provider on one day predicted a lower likelihood of them experiencing a suicidal urge thereafter (F = 13.22 (df = 2,51), β = −0.25, p < 0.001, R2 = 0.32). That is, when Person 1 reached out to their mental healthcare provider, they experienced a corresponding 0.25 standard deviation decrease (on average) in subsequent suicidal urge. Engagement with a mental health provider explained 32% of the variance in Person 1’s subsequent suicidal urge. Other details of Person 1’s specific results are reported in Table 1.
In terms of the total number of daily coping strategies, Person 1 also had a significant prospective association between the level of suicidal urge and a subsequent increase in the number of coping strategies tried (F = 15.30 (df = 1,102, β = 0.43, p < 0.001, R2 = 0.27). A one standard deviation increase in Person 1’s suicidal urge led to a corresponding 0.43 standard deviation increase (on average) in the total number of coping strategies Person 1 used thereafter. Efficacy was also associated with earlier suicidal urge for Person 1 (F = 5.77 (df = 1,102), β = 0.31, p < 0.05, R2 = 0.27), such that a one standard deviation increase in suicidal urge was associated with a 0.31 standard deviation increase in the efficacy to resist suicidal urges thereafter. After accounting for strong stability in efficacy from one day to the next, suicidal urge explained 27% of the variance in efficacy.
By contrast, Person 2 exhibited distinct effects. A prospective association was detected between suicidal urge and subsequent reaching out to a family member (F = 6.97 (df = 1,102), β = −0.34, p < .01, R2 = 0.09), such that a one standard deviation increase in urge led to a 0.34 standard deviation decrease (on average) in the likelihood that Person 2 reached out to a family member. Urge explained 9% of the variance in reaching out to a family member. Person 2 also had an association between suicidal urges and the number of coping strategies the next day (F = 8.25 (df = 1,102), β = −0.31, p < 0.001, R2 = 0.24), such that a one standard deviation increase in suicidal urge was associated with 0.31 standard deviation decrease in the number of strategies they used the next day. Urge explained 24% of the variance in the breadth of coping strategies used.
Distinct person-specific effects were also detected for Person 3, for whom no association was detected between suicidal urge and next day forms of coping, breadth of coping strategies used, or self-efficacy. Despite this, Person 3 exhibited positive autoregressive effects of suicidal urge (β’s ranged from 0.38 to 0.45 across models) and breadth of coping strategies tried (β = 0.40, p < 0.001) and efficacy (β = 0.28, p < 0.05), such that reports of each were highly consistent from one occasion to the next. Specifically, a one standard deviation in Person 3’s suicidal urge on one day predicted between a 0.38 and 0.45 standard deviation increase in their suicidal urge on the next day depending on the coping or self-efficacy covariate under examination. For breadth of coping strategies, a one standard deviation increase in Person 3’s sum of coping strategies predicted a 0.40 standard deviation increase in the number of coping strategies Person 3 tried on the next day.
DISCUSSION
The primary aim of the present study was to illustrate the utility of idiographic methods in suicide research using a case series approach. We achieved this aim by highlighting person-specific heterogeneity in the associations between coping strategies, self-efficacy to refrain from suicidal action, and STBs among an ostensibly homogeneous set of individuals (i.e., similar STB profiles). Noteworthy heterogeneity distinguished coping responses to suicidal urges across individuals (as illustrated by the three show-cased here), with links between urge, efficacy, and coping detected for some individuals but not others. Specifically, links between suicidal urge and coping behaviors varied from person to person, as illustrated in the three individuals discussed, highlighting that individual-level heterogeneity may be important to consider when studying STBs. When effects were present between urges and coping, associations varied in both magnitude and direction across individuals. Overall, we show the potential richness that idiographic approaches may add alongside nomothetic inferences, provide readers with more information about idiographic methods, and demonstrate the potential for further applications of idiography in suicide research.
In our three case examples, even efficacy to refrain from suicidal action, which has previously been associated with cross-sectional and prospective suicide risk in nomothetic analyses (Czyz et al., 2014; King, Brent, et al., 2019; King, Grupp-Phelan, et al., 2019), exhibited person-specific variation. Specifically, efficacy to refrain from suicidal action was negatively correlated with next-day suicidal urge for Person 1, not related at all for Person 2, and positively correlated for Person 3. When taken together, these results highlight that (1) assumptions of homogeneity that traditional, nomothetic analyses may be insufficient for explaining individual-level variation in suicide risk—even when individuals appear phenomenologically similar—and (2) nomothetic approaches that pool information across individuals to draw a single inference are likely to provide incomplete information with weak correspondence to the experiences of individuals. There are likely many reasons for heterogeneity in person-specific effects, including but not limited to (1) individual differences in biological, cognitive, and affective factors making some strategies more effective for some youth but not for others and (2) environmental differences which either reinforce or punish specific coping strategies (e.g., support seeking met with a validating and helpful response is likely to show a positive correlation between STBs and this strategy over time).
Future studies are needed to further characterize and replicate the full extent of person-specific links in STB etiological factors. As we have refrained from conducting between-person analyses due to small sample size, we recommend that this work be extended in the future studies through use of a larger sample size to permit elaboration on between-person processes from the person-specific models through analysis techniques that leverage idiographic information to detect nomothetic effects (e.g., GIMME; Gates & Molenaar, 2012). Doing so could permit comparison of prevalent effects across people to effects unique to specific people and support the identification of more personalized intervention targets (Rodebaugh et al., 2020). For example, depending on the individuals’ person-specific correlates, one participant could receive a treatment targeting the increase of cognitive reap-praisal, while another participant may be encouraged to first reach out to supportive friends and family members. Single-subject case–control designs could be used to determine the acceptability, feasibility, and efficacy of this approach. Idiographic methods have the potential to identify personalized psychological treatment targets, possibly leading to more effective and efficient interventions.
There are a few notable limitations to this case series analysis. First, participants were not sampled at the highest possible level of granularity compared to those intensive longitudinal studies that have focused on moment-to-moment temporal resolution (e.g., 5+ times per day over a two week or a month-long window). While use of ILD has permitted estimation of short-term prospective effects that are expected to match the time scale of the association between urge and coping, it will be important for future work to conduct more specific investigations of variation in effects due to timescale. This will be especially important if there is person-specific heterogeneity in the time between urge and initiation of coping behavior for some youth, or if there is heterogeneity in the sequencing of coping efforts (i.e., trying one coping strategy unsuccessfully followed by the initiation of a second strategy in an attempt to further downregulate).
Second, vector autoregressive (VAR) models assume stationarity (i.e., links between coping and suicidal urges are expected to generalize across time) and so any benefits of coping practice or treatment (person-specific effects or otherwise) during this limited observation period are not reflected in these results. However, routine outcome monitoring (Lambert et al., 2018)—for both the purpose of assessing personalized targets and tracking personalized improvement—would be especially important to use in tandem with these models. Third, we imputed missing values for the two individuals who missed a few observations as a complete dataset was necessary to run VAR models. Imputation allowed us to account for missing observations post hoc, but imputation is certainly less preferable to a dataset with no missing reports as the underlying reason for unanswered responses can never be known for certain.
Idiographic analyses of the case series presented here illustrate the critical necessity of incorporating these approaches into future research focused on understanding risk pathways for youth at high risk for suicide. Although it has long been observed that suicidal individuals are phenomenologically heterogeneous (i.e., not all individuals with frequent urges ultimately act on thoughts of suicide), the degree and nature of both phenomenological and predictive heterogeneity have been obfuscated by use of nomothetic approaches. To increase the dissemination of idiographic methods, we have made the analysis scripts available so that researchers can incorporate these methods in other datasets. The current results provide evidence that heterogeneity is present in suicide risk, even among ostensibly homogenous groups of individuals at the same point in care. While the inference that heterogeneity is present in predictive links between suicidal urge and coping is expected to generalize to the population more broadly, more work is needed to integrate this observation with group-level approaches that aim to characterize which person-specific effects are most prevalent in the population and to further quantify their rates of expression across diverse individuals.
The case illustrations presented here are designed to showcase the types of inferences that may be gained from implementing idiographic approaches in the study of suicidal urge. However, these data were collected using a traditional approach, consistent with many intensive longitudinal protocols investigating suicide risk (for review of intensive longitudinal studies in suicide research, see Kuehn et al., Under Review), which are often limited in the number of planned assessments and observations of momentary suicide risk, even in especially high-risk samples like this one. Strategic shifts in these protocols are necessary to ensure adequate statistical power is retained for person-specific models, which draw power from the number of observations (vs. number of individuals; Cattell, 1988). Simulation work generally recommends applying idiographic work to ILD with no fewer than 40 time points (Beltz & Gates, 2017; Foster & Beltz, 2018; Liu, 2017). However, these studies consider constructs with a Gaussian distribution rather than the zero-inflated one more typical of momentary suicidal urge observed in these ILD. Consequently, careful attention in the future intensive longitudinal studies of STBs should be devoted to maximizing the typical number of planned assessments, and, perhaps more importantly, the number of observations of reported suicide risk, owing to the fact that 40 time points are very likely far from sufficient to provide a mathematically meaningful account of STBs.
Finally, our sample was composed of youth at very high risk for suicide who experienced frequent and recurring STBs, which allowed us to model these within-person processes over a relatively long period of time. In line with previous studies documenting heterogeneity in suicide risk and protective factors (Czyz & King, 2015; King, Brent, et al., 2019), these results further highlight that coping patterns and STBs are also likely highly heterogeneous both within and between people. This likely means that nomothetic approaches to predicting STBs, which focus on highlighting general processes for all people, are likely obscuring important differences across individuals. It is likely that focusing on subgroups of people (Kleiman et al., 2017; Czyz & King, 2015; King, Brent, et al., 2019) and/or creating personalized risk models for individuals will lead to more accurate and efficient prediction models, which has the potential to strengthen the tailoring and effectiveness of our treatment paradigms for individuals with STBs. Future studies using idiographic methods to complement nomothetic inferences are needed to optimize the information gained from studies collecting ILD with individuals at high risk for suicide, and to ensure that no person is excluded from our intervention efforts.
Funding information
The research reported in this manuscript was supported by training grants from the National Institute of Mental Health (F31MH117827; PI - Kuehn, and K23MH113776; PI - Czyz), a grant from the American Foundation of Suicide Prevention (PDF-0-028-14; PI - Czyz), and by the Michigan Institute for Clinical and Health Research’s Postdoctoral Translational Scholar Program.
Footnotes
CONFLICT OF INTEREST
None.
For this imputation strategy, we lagged each of the covariates (coping strategies and self-efficacy) as well as the dependent variable (suicidal urge) and used either a logistic regression, in the case of binary coping variables, or predictive mean matching, for continuous suicide urge and self-efficacy variables. As we planned to analyze the data idiographically, each person’s dataset was imputed separately.
REFERENCES
- Allan NP, Gros DF, Lancaster CL, Saulnier KG, & Stecker T (2019). Heterogeneity in short-term suicidal ideation trajectories: Predictors of and projections to suicidal behavior. Suicide and Life-Threatening Behavior, 49(3), 826–837. 10.1111/sltb.12480 [DOI] [PubMed] [Google Scholar]
- Bagge CL, Littlefield AK, & Glenn CR (2017). Trajectories of affective response as warning signs for suicide attempts: An examination of the 48 hours prior to a recent suicide attempt. Clinical Psychological Science, 5(2), 259–271. 10.1177/2167702616681628 [DOI] [Google Scholar]
- Beltz AM, & Gates KM (2017). Network mapping with GIMME. Multivariate Behavioral Research, 52(6), 789–804. 10.1080/00273171.2017.1373014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borkenau P, & Ostendorf F (1998). The Big Five as states: How useful is the five-factor model to describe intraindividual variations over time? Journal of Research in Personality, 32(2), 202–221. 10.1006/jrpe.1997.2206 [DOI] [Google Scholar]
- Bryan CJ, Bryan AO, & Baker JC (2020). Associations among state-level physical distancing measures and suicidal thoughts and behaviors among US adults during the early COVID-19 pandemic. Suicide and Life-Threatening Behavior, 50(6), 1223–1229. 10.1111/sltb.12653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryan CJ, & Rudd MD (2015). Demographic and diagnostic differences among suicide ideators, single attempters, and multiple attempters among military personnel and veterans receiving outpatient mental health care. Military Behavioral Health, 3(4), 289–295. 10.1080/21635781.2015.1093978 [DOI] [Google Scholar]
- Cattell RB (1988). The data box. In Nesselroade JR & Cattell RB (Eds.), Handbook of multivariate experimental psychology (pp. 69–130). Springer. [Google Scholar]
- CDC (2020). Web-based Injury Statistics Query and Reporting System (WISQARS). Retrieved from https://www.cdc.gov/injury/wisqars/index.html
- Czeisler MÉ, Lane RI, Petrosky E, Wiley JF, Christensen A, Njai R, & Rajaratnam SM (2020). Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States. Morbidity and Mortality Weekly Report, 69(32), 1049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czyz EK, Bohnert AS, King CA, Price AM, Kleinberg F, & Ilgen MA (2014). Self-efficacy to avoid suicidal action: Factor structure and convergent validity among adults in substance use disorder treatment. Suicide and Life-Threatening Behavior, 44(6), 698–709. 10.1111/sltb.12101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czyz EK, Horwitz AG, Arango A, Cole-Lewis Y, Berona J, & King CA (2016). Coping with suicidal urges among youth seen in a psychiatric emergency department. Psychiatry Research, 241, 175–181. 10.1016/j.psychres.2016.04.118 [DOI] [PubMed] [Google Scholar]
- Czyz EK, Horwitz AG, Arango A, & King CA (2019). Short-term change and prediction of suicidal ideation among adolescents: A daily diary study following psychiatric hospitalization. Journal of Child Psychology and Psychiatry, 60(7), 732–741. 10.1111/jcpp.12974 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czyz EK, Horwitz AG, & King CA (2016). Self-rated expectations of suicidal behavior predict future suicide attempts among adolescent and young adult psychiatric emergency patients. Depression & Anxiety, 33, 512–519. 10.1002/da.22514 [DOI] [PubMed] [Google Scholar]
- Czyz EK, & King CA (2015). Longitudinal trajectories of suicidal ideation and subsequent suicide attempts among adolescent inpatients. Journal of Clinical Child & Adolescent Psychology, 44(1), 181–193. 10.1080/15374416.2013.836454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czyz EK, King CA, & Biermann BJ (2019). Motivational interviewing-enhanced safety planning for adolescents at high suicide risk: A pilot randomized controlled trial. Journal of Clinical Child and Adolescent Psychology, 48(2), 250–262. 10.1080/15374416.2018.1496442 [DOI] [PubMed] [Google Scholar]
- Czyz EK, King CA, & Nahum-Shani I (2018). Ecological assessment of daily suicidal thoughts and attempts among suicidal teens after psychiatric hospitalization: Lessons about feasibility and acceptability. Psychiatry Research, 267, 566–574. 10.1016/j.psychres.2018.06.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher AJ, Medaglia JD, & Jeronimus BF (2018). Lack of group-to-individual generalizability is a threat to human subjects research. Proceedings of the National Academy of Sciences of the United States of America, 115(27), E6106–E6115. 10.1073/pnas.1711978115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher AJ, Reeves JW, Lawyer G, Medaglia JD, & Rubel JA (2017). Exploring the idiographic dynamics of mood and anxiety via network analysis. Journal of Abnormal Psychology, 126(8), 1044. 10.1037/abn0000311 [DOI] [PubMed] [Google Scholar]
- Foster KT, & Beltz AM (2018). Advancing statistical analysis of ambulatory assessment data in the study of addictive behavior: A primer on three person-oriented techniques. Addictive Behaviors, 83, 25–34. 10.1016/j.addbeh.2017.12.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gates K, & Molenaar P (2012). Group Iterative Multiple Model Estimation (GIMME). Quantitative Developmental Systems Methodology. [Google Scholar]
- Hallensleben N, Glaesmer H, Forkmann T, Rath D, Strauss M, Kersting A, & Spangenberg L (2019). Predicting suicidal ideation by interpersonal variables, hopelessness and depression in real-time. An ecological momentary assessment study in psychiatric inpatients with depression. European Psychiatry, 56(1), 43–50. [DOI] [PubMed] [Google Scholar]
- Huang X, Ribeiro JD, Musacchio KM, & Franklin JC (2017). Demographics as predictors of suicidal thoughts and behaviors: A meta-analysis. PLoS One, 12(7), e0180793. 10.1371/journal.pone.0180793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ji L, Chow SM, Schermerhorn AC, Jacobson NC, & Cummings EM (2016). Handling missing data in the modeling of intensive longitudinal data. Structural Equation Modeling, 25(5), 715–736. 10.1080/10705511.2017.1417046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- King CA, Brent D, Grupp-Phelan J, Shenoi R, Page K, Mahabee-Gittens EM, & Littlefield A (2019). Five profiles of adolescents at elevated risk for suicide attempts: Differences in mental health service use. Journal of the American Academy of Child & Adolescent Psychiatry, 59(9), 1058–1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King CA, Foster CE, & Rogalski KM (2013). Teen suicide risk: A practitioner guide to screening, assessment, and management. Guilford Press. [Google Scholar]
- King CA, Grupp-Phelan J, Brent D, Dean JM, Webb M, Bridge JA, Spirito A, Chernick LS, Mahabee-Gittens EM, Mistry RD, Rea M, Keller A, Rogers A, Shenoi R, Cwik M, Busby DR, & Casper TC (2019). Predicting 3-month risk for adolescent suicide attempts among pediatric emergency department patients. Journal of Child Psychology and Psychiatry, 60(10), 1055–1064. 10.1111/jcpp.13087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kleiman EM, Turner BJ, Fedor S, Beale EE, Huffman JC, & Nock MK (2017). Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. Journal of Abnormal Psychology, 126(6), 726. 10.1037/abn0000273 [DOI] [PubMed] [Google Scholar]
- Kuehn KS, Wagner A, & Velloza J (2019). Estimating the magnitude of the relation between bullying, E-bullying, and suicidal behaviors among United States youth, 2015. Crisis, 40(3), 157–165. 10.1027/0227-5910/a000544 [DOI] [PubMed] [Google Scholar]
- Lambert MJ, Whipple JL, & Kleinstäuber M (2018). Collecting and delivering progress feedback: A meta-analysis of routine outcome monitoring. Psychotherapy, 55(4), 520. 10.1037/pst0000167 [DOI] [PubMed] [Google Scholar]
- Linehan MM (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford. [Google Scholar]
- Liu S (2017). Person-specific versus multilevel autoregressive models: Accuracy in parameter estimates at the population and individual levels. British Journal of Mathematical and Statistical Psychology, 70(3), 480–498. [DOI] [PubMed] [Google Scholar]
- Miron O, Yu KH, Wilf-Miron R, & Kohane IS (2019). Suicide rates among adolescents and young adults in the United States, 2000–2017. JAMA, 321(23), 2362–2364. 10.1001/jama.2019.5054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molenaar PCM (2004). A manifesto on psychology as idiographic science: Bringing the person back into scientific psychology, this time forever. Measurement: Interdisciplinary Research and Perspectives, 2(4), 201–218. [Google Scholar]
- Molenaar PCM, & Campbell CG (2009). The new person-specific paradigm in psychology. Current Directions in Psychological Science, 18(2), 112–117. 10.1111/j.1467-8721.2009.01619.x [DOI] [Google Scholar]
- Neacsiu AD, Rizvi SL, & Linehan MM (2010). Dialectical behavior therapy skills use as a mediator and outcome of treatment for borderline personality disorder. Behaviour Research and Therapy, 48(9), 832–839. 10.1016/j.brat.2010.05.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK, Prinstein MJ, & Sterba SK (2009). Revealing the form and function of selfinjurious thoughts and behaviors: A real-time ecological assessment study among adolescents and young adults. Journal of Abnormal Psychology, 118(4), 816–827. 10.1158/2159-8290.CD-16-0307.PD-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norcross JC, & Wampold BE (2011). What works for whom: Tailoring psychotherapy to the person. Journal of Clinical Psychology, 67(2), 127–132. 10.1002/jclp.20764 [DOI] [PubMed] [Google Scholar]
- Pfaff B (2008). VAR, SVAR and SVEC models: Implementation within R package vars. Journal of Statistical Software, 27(4), 1–32. [Google Scholar]
- Piccirillo ML, Beck ED, & Rodebaugh TL (2019). A clinician’s primer for idiographic research: Considerations and recommendations. Behavior Therapy, 50(5), 938–951. 10.1016/j.beth.2019.02.002 [DOI] [PubMed] [Google Scholar]
- R Core Team (2013). R: A language and environment for statistical computing.Vienna, Austria: R Foundation for Statistical Computing. https://www.r-project.org/ [Google Scholar]
- Rodebaugh TL, Frumkin MR, & Piccirillo ML (2020). The long road from person specific models to personalized mental health treatment. BMC Medicine, 18(1), 1–2. 10.1186/s12916-020-01838-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shukur G, & Mantalos P (2000). A simple investigation of the Granger-causality test in integrated-cointegrated VAR systems. Journal of Applied Statistics, 27(8), 1021–1031. 10.1080/02664760050173346 [DOI] [Google Scholar]
- Stanley B, Martínez-Alés G, Gratch I, Rizk M, Galfalvy H, Choo TH, & Mann JJ (2021). Coping strategies that reduce suicidal ideation: An ecological momentary assessment study. Journal of Psychiatric Research, 133, 32–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanley B, & Brown GK (2012). Safety planning intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioral Practice, 19(2), 256–264. 10.1016/j.cbpra.2011.01.001 [DOI] [Google Scholar]
- Stanley B, Brown G, Brent DA, Wells K, Poling K, Curry J, Kennard BD, Wagner A, Cwik MF, Klomek AB, Goldstein T, Vitiello B, Barnett S, Daniel S, & Hughes J (2009). Cognitive-behavioral therapy for suicide prevention (CBT-SP): Treatment model, feasibility, and acceptability. Journal of the American Academy of Child & Adolescent Psychiatry, 48(10), 1005–1013. 10.1097/CHI.0b013e3181b5dbfe [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (2018). Suicide data. 2017. http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/
- Wright AG, Beltz AM, Gates KM, Molenaar P, & Simms LJ (2015). Examining the dynamic structure of daily internalizing and externalizing behavior at multiple levels of analysis. Frontiers in Psychology, 6, 1914. 10.3389/fpsyg.2015.01914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright AG, & Woods WC (2020). Personalized models of psychopathology. Annual Review of Clinical Psychology, 16. 10.1146/annurev-clinpsy-102419-125032 [DOI] [PubMed] [Google Scholar]