

Abstract
Objectives:
Some older drivers choose to avoid certain situations where they do not feel confident driving. Little is known about the process by which older drivers may use avoidance in transitioning to non-driving.
Methods:
We analyzed 2015 ConsumerStyles data for 1198 drivers aged 60+. Driving patterns were examined by sociodemographic and driving characteristics. Avoidance classes were characterized by latent class analysis.
Results:
Among drivers 60+, 79% reported driving 3+ days/week and 84% reported good to excellent health. We identified four driving avoidance classes (low, mild, moderate, and high). High- (versus low-) avoidance drivers were more likely female, 75+, not White/non-Hispanic, and to have income <$25,000/year.
Discussion:
Avoidance of selected driving behaviors may be one component of a multi-step process supporting the transition to non-driving. Drivers displaying avoidance behaviors may be receptive to resources to prepare for this transition and minimize negative health and quality of life outcomes that accompany driving cessation.
Keywords: older drivers, aging, driving avoidance, driving self-regulation, driving cessation, motor vehicle safety
Introduction
As has been well documented, the population is aging, with the global proportion of people aged 65+ expected to grow from 9% in 2020 to 16% in 2050 (United Nations Department of Economic and Social Affairs, 2020). In the United States (U.S.), the number of Americans aged 65+ has grown from 38.8 million in 2008 to 54.1 million in 2019, and these older people are living longer than those from previous generations (Administration for Community Living, 2021). For adults, including older people, the primary means of getting around in the U.S. is by driving passenger vehicles (Shen et al., 2017).
As one ages, the risk of chronic health conditions (e.g., diabetes, heart disease, and vision loss) increases as does the risk of being diagnosed with more than one condition (World Health Organization, 2015). These age-related conditions and the biological process of aging itself may lead to declines in physical, cognitive, or visual function that impact the ability to drive and reduce mobility (Fabbri et al., 2015; World Health Organization, 2015). Transportation, including driving, is an instrumental activity of daily living, facilitating the ability to access goods and services in the community (Marfeo et al., 2021; Marottoli et al., 2000). Reduced mobility also negatively affects the size of people’s social networks and number of social activities (Chihuri et al., 2016; Curl et al., 2014; Edwards et al., 2009).
Some people stop driving due to changes in health and functional status (Choi et al., 2012; Dickerson et al., 2007). However, driving cessation imposes challenges for maintaining mobility and health, having been associated with adverse health outcomes, reduced quality of life, and increased mortality (Chihuri et al., 2016; Edwards et al., 2009; Fonda et al., 2001). Others choose to reduce their amount and types of driving with an approach known as self-regulation (Ang et al., 2019; Molnar et al., 2015). Self-regulation is generally understood to take place over time to retain some mobility and independence in an effort to minimize risks that may be associated with age-related functional declines (Ang et al., 2019; Molnar et al., 2015). Environmental, interpersonal, and personal (e.g., confidence in driving) considerations are other important factors that can influence self-regulation as well (Molnar et al., 2015). Three levels of self-regulation—life-goal, tactical, and strategic—have been conceptualized (Molnar et al., 2015). Briefly, the life-goal level encompasses decisions that affect driving, including vehicle purchases and where to live. Tactical self-regulation takes place during a driving trip with behaviors such as leaving a larger distance between one’s vehicle and those ahead. Strategic self-regulation includes avoidance of selected driving situations (e.g., driving at night) and cutting back on the amount of driving (Molnar et al., 2015). Self-regulation may be a step in the process by which older people transition from driving to non-driving; yet this complex process remains poorly understood (Gwyther & Holland, 2012; Wong et al., 2016). It is also important to note that some drivers may make driving decisions that are not for self-regulation purposes. Driving avoidance, for example, may be undertaken for other reasons, such as not driving during rush hour because of personal preference to avoid congestion (Molnar et al., 2015).
The purpose of the current study was to describe patterns of driving avoidance behaviors among a general population of older drivers aged 60+ and to use latent class analysis to classify older drivers by these patterns. For study purposes, the terms “older people” and “older drivers” comprise people aged 60+. While older people are commonly defined as people aged 65+, we included those aged 60+ to capture a broader range of driving behaviors that might not have been observed with an older sample. Identification of driving avoidance patterns—and the characteristics of drivers in different avoidance classes—could contribute to a better understanding of the process by which older drivers transition to non-driving.
Methods
Study Design and Data Collection Methods
This study analyzed data from Porter Novelli’s 2015 ConsumerStyles survey series (Porter Novelli, n.d.). Respondents were part of Ipsos’ KnowledgePanel, a nationally representative online panel, randomly recruited using probability-based, address-based sampling techniques. Ipsos obtained consent electronically during the recruitment process and maintained a confidentiality agreement with participants to protect personally identifiable information. Participation was voluntary; respondents could leave the panel or refuse to answer any questions on any survey at any time. Respondents without internet access prior to joining the panel were provided with it. Data were collected in three seasonal waves. Driving data were collected during September 10–29, 2015, during the third wave (FallStyles). Of 11,018 adults aged 18+ selected for the first wave (SpringStyles), 6836 completed that survey. Of those respondents, 4432 were randomly selected for the FallStyles survey, and 3529 people completed it. Survey completion took a median of 25 minutes. Participants received reward points with an approximate cash value of $5. Full details of the ConsumerStyles methodology are available from Porter Novelli (n.d.). The Centers for Disease Control and Prevention (CDC) licensed 2015 ConsumerStyles survey data for health-related analyses. Because CDC analyzed de-identified secondary data, the study was exempt from Institutional Review Board review.
Of 3529 respondents, we excluded 2209 adults aged <60 years, 121 older people who reported that they did not drive, and one who did not report their driving status, resulting in a final sample size of 1198. All analyses were conducted using data weighted to approximate 2015 U.S. Current Population Survey estimates. Data were weighted on gender, age, household income, race/ethnicity, household size, education, census region, metropolitan status, and whether the household had internet access prior to panel participation (Porter Novelli, n.d.).
Study Variables
13 driving- and transportation-related variables were used for this study. Respondents were asked whether they were current drivers (yes, no) and their primary means of transportation (driving, riding as passenger with family or friends, walking, bicycling, taxi or private service such as Uber, public transportation, or other transportation). For analysis, we combined walking and bicycling (labeled “walking or bicycling”) and taxi or other private service, public transportation, and other (labeled “other”) due to small number of responses for individual categories. Current drivers reported how often they usually drove (<1, 1–2, or 3+ days/week) and how often (never, sometimes, always) they avoided nine driving situations: driving at night, making left turns across oncoming traffic, driving in bad weather, driving alone, highway driving, driving on high traffic roads, driving during rush hour, driving in unfamiliar areas, and driving long distances. Finally, current drivers reported how often (never, sometimes, always) they “pass up opportunities to go shopping, visit friends, etc. because of concerns about driving.”
Selected sociodemographic, geographic, and health-related variables were included in the study. We converted the continuous age variable into categories (60–74 years, 75+ years) to facilitate comparisons and ease interpretation of results. Categories for other variables were combined as needed to account for small cell sizes and/or to ease interpretation of results. Gender was reported as male or female. Race/ethnicity was reported as non-Hispanic White, non-Hispanic Black, non-Hispanic other, non-Hispanic multiple races, and Hispanic. We combined non-Hispanic other and non-Hispanic multiple races into one category for analysis. Marital status was reported as married, living with a partner (“married or living with partner”), widowed, divorced, separated, or never married (“not married”). Education was reported as highest grade completed up to and including high school degree (“high school or less”), some college, associate’s degree (“some college”), bachelor’s degree, master’s degree, or professional/doctorate degree (“bachelor’s degree or higher”). Employment status was reported as working as paid employee, self-employed (“working”), laid off, looking for work, not working/other (“not working: laid off, looking for work, other”), retired, or disabled (“not working: retired or disabled”). Annual household income was reported in categories ranging from <$5000 to $175,000+. We collapsed groups into < $25,000 and ≥ $25,000. Census region was classified as Northeast, Midwest, South, and West.
Self-reported health status was reported as good, very good, excellent (“good to excellent”), fair, or poor (“fair/poor”). Number of self-reported medical conditions was calculated from the sum of conditions that respondents reported having currently or in the past year: anxiety, arthritis, asthma, chronic pain, depression, diabetes, emphysema or chronic obstructive pulmonary disease, epilepsy or other seizure disorder, high cholesterol, insomnia or other sleep disorder, irritable bowel syndrome, migraine headaches, osteoporosis, overactive bladder or incontinence, high blood pressure, atrial fibrillation, congestive heart failure, other heart disease such as angina or heart attack, lung cancer, or some other cancer (not lung or skin).
Descriptive Data Analysis
Descriptive analyses were conducted to determine prevalence and 95% confidence intervals (CIs) of sociodemographic, geographic, and health-related characteristics of current drivers aged 60+. Prevalence and 95% CIs were also calculated for driving- and transportation-related variables. We compared the ConsumerStyles sample to selected U.S. bridged-race population estimates for 2015 (United States Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, 2020). We calculated number and prevalence of adults aged 60+ in the U.S. by age group, gender, and race/ethnicity.
Latent Class Analysis and Modeling
Driving avoidance classes were characterized by latent class analysis (LCA) using 10 indicators (driving frequency and nine driving avoidance situations). The LCA model estimated the proportion of older people in each class (class membership probabilities) and the distribution of responses to each of the 10 items within each class (item-response probabilities conditional on class membership). The optimal number of latent classes was determined based on a balance of fit, parsimony, and interpretability using the deviance statistic G2, the Akaike Information Criterion (AIC), and the Bayesian Information Criterion (BIC) to assess model fit (Lanza et al., 2003, 2007). Although 19 of the 1198 respondents from the final sample had missing data for at least one but not all 10 driving variables, the number of observations used in the LCA was still 1198 because LCA does not require an observation to have values in all indicators.
After the optimal number of latent classes was determined, a table was created showing the proportion of respondents by class for each of the nine driving avoidances for answers of never, sometimes, or always. Prevalence and 95% CIs for selected transportation variables (primary means of transportation, driving frequency, and passing up opportunities to go out) were calculated by driving avoidance class. Then the covariates analysis was conducted to predict class membership. Demographic variables gender, age, and race/ethnicity were included in the model. Additional variables considered were those that were significant in the covariates list: region, marital status, education level, employment status, annual household income, and health status. A variable from this list was retained in the model if it was significant (p < .05) in the bivariate analysis. PROC LCA and Statistical Analysis Software (SAS) version 9.3 (SAS Institute, Inc., Cary, North Carolina) were used to conduct all analyses (Lanza et al., 2007, 2015). The weight variable was used to generate estimates and draw inference for the U.S. older adult population.
Results
Descriptive Results
Among current drivers aged 60+, 77.7% were 60–74 years of age and 22.3% were 75+ (Table 1). Our sample of current drivers was slightly younger than the U.S. population of all adults aged 60+, 69.7% of whom were aged 60–74. The sample was similar to the U.S. population of people aged 60+ in terms of gender and race/ethnicity (Table 1).
TABLE 1.
Prevalence of Selected Characteristics Among Adults Ages 60+ Years, ConsumerStyles Sample and U.S. Population, 2015.
| Current Drivers, ConsumerStyles | U.S. Population Estimatea | |||
|---|---|---|---|---|
|
|
|
|||
| (N = 1198) | (N = 66,661,997) | |||
|
|
|
|||
| Variable | Sample Nb | Weightedc % (95% CI) | N | % |
|
| ||||
| Age Group | ||||
| 60–74 years | 950 | 77.7 (74.4–81.1) | 46,496,415 | 69.7 |
| 75+ years | 248 | 22.3 (18.9–25.6) | 20,165,582 | 30.3 |
| Gender | ||||
| Male | 592 | 46.1 (42.4–49.9) | 30,122,169 | 45.2 |
| Female | 606 | 53.9 (50.1–57.6) | 36,539,828 | 54.8 |
| Race/Ethnicity | ||||
| White, non-Hispanic | 1018 | 77.6 (73.9–81.3) | 51,339,123 | 77.0 |
| Black, non-Hispanic | 80 | 9.0 (6.5–11.5) | 6,352,134 | 9.5 |
| Other or multiple races, non-Hispanic | 29 | 4.9 (2.5–7.2) | 3,429,323 | 5.1 |
| Hispanic | 71 | 8.6 (6.2–11.0) | 5,541,417 | 8.3 |
| Marital status | ||||
| Married or living with partner | 762 | 67.8 (64.3–71.3) | ||
| Not married | 436 | 32.2 (28.7–35.7) | ||
| Education level | ||||
| High school or less | 475 | 45.9 (42.1–49.8) | ||
| Some college | 352 | 24.8 (21.8–27.7) | ||
| Bachelor’s degree or higher | 371 | 29.3 (25.9–32.6) | ||
| Annual household income | ||||
| Less than $25,000 | 184 | 16.0 (13.0–19.0) | ||
| $25,000 or more | 1014 | 84.0 (81.0–87.0) | ||
| Employment status | ||||
| Working | 315 | 26.5 (23.1–30.0) | ||
| Not working (laid off, looking for work, or other) | 47 | 3.9 (2.4–5.3) | ||
| Not working (retired or disabled) | 836 | 69.6 (66.0–73.2) | ||
| Region | ||||
| Northeast | 202 | 19.1 (15.8–22.4) | ||
| Midwest | 303 | 22.1 (19.2–24.9) | ||
| South | 428 | 36.6 (32.9–40.3) | ||
| West | 265 | 22.2 (19.1–25.3) | ||
| Health statusd | ||||
| Good to excellent | 1018 | 83.6 (80.4–86.8) | ||
| Fair or poor | 178 | 16.4 (13.2–19.6) | ||
| Total number of selected medical conditionse | ||||
| None | 239 | 21.1 (18.0–24.2) | ||
| 1–2 | 525 | 43.0 (39.2–46.8) | ||
| 3+ | 434 | 35.9 (32.2–39.5) | ||
Note. CI=confidence interval.
Bridged-race population estimates compiled by the CDC, National Center for Health Statistics.
Sums may not equal total sample N because of missing data.
Data weighted on gender, age, household income, race/ethnicity, household size, education, census region, metropolitan status, and household internet access prior to panel participation.
Self-reported health status.
Self-reported medical conditions, present currently or during the past year.
About two-thirds (67.8%) were married or living with a partner. Almost half (45.9%) had no more than a high school education, and 16.0% had annual household income <$25,000. More than two-thirds (69.6%) were retired or disabled. More than four-fifths (83.6%) reported their overall health as good to excellent, while most also reported having at least one medical condition (43.0% reported 1–2, 35.9% reported 3+).
Among current drivers aged 60+, 94.6% reported driving as their primary means of transportation, and more than three-fourths (79.0%) reported driving 3+ days/week (Table 2). Overall, more than half of drivers reported sometimes or always avoiding driving at night, in bad weather, in unfamiliar areas, and during rush hour. Driving situations most commonly “never avoided” were driving alone (83.5%), highway driving (67.3%), and making left turns (66.8%). Driving situations most commonly “always avoided” were driving during rush hour (11.3%), for long distances (11.1%), and at night (10.3%). One-fourth of drivers reported sometimes (23.0%) or always (1.3%) passing up opportunities to go out because of driving concerns.
TABLE 2.
Prevalence of Transportation and Driving Characteristics Among Current Drivers Age 60+ Years, ConsumerStyles 2015, United States, Sample N = 1198.
| Variable | Sample Na | Weightedb % (95% CI) |
|---|---|---|
|
| ||
| Primary means of transportation | ||
| Drive a passenger vehicle (e.g., car, truck, van, motorcycle) | 1136 | 94.6 (92.6–96.5) |
| Ride in passenger vehicle with family or friend as driver | 31 | 2.6 (1.4–3.7) |
| Other | 18 | 2.1 (0.7–3.5) |
| Walk or bicycle | 8 | 0.7 (0.0–1.5) |
| Current driving frequency | ||
| Less than 1 day per week | 64 | 5.9 (3.9–7.9) |
| 1–2 days per week | 175 | 15.1 (12.3–17.9) |
| 3 or more days per week | 952 | 79.0 (75.8–82.2) |
| Avoid driving at night | ||
| Never | 522 | 43.4 (39.6–47.2) |
| Sometimes | 557 | 46.3 (42.5–50.1) |
| Always | 117 | 10.3 (7.8–12.8) |
| Avoid highway driving | ||
| Never | 819 | 67.3 (63.7–70.9) |
| Sometimes | 328 | 27.4 (24.1–30.8) |
| Always | 45 | 5.3 (3.1–7.5) |
| Avoid making left turns across oncoming traffic | ||
| Never | 813 | 66.8 (63.1–70.5) |
| Sometimes | 336 | 27.6 (24.2–31.0) |
| Always | 45 | 5.7 (3.4–7.9) |
| Avoid driving in bad weather | ||
| Never | 379 | 32.9 (29.3–36.5) |
| Sometimes | 724 | 58.2 (54.4–62.0) |
| Always | 93 | 8.9 (6.6–11.2) |
| Avoid driving alone | ||
| Never | 1013 | 83.5 (80.4–86.6) |
| Sometimes | 161 | 13.8 (11.1–16.6) |
| Always | 19 | 2.7 (1.0–4.4) |
| Avoid driving on high traffic roads | ||
| Never | 672 | 53.6 (49.8–57.4) |
| Sometimes | 462 | 39.5 (35.7–43.3) |
| Always | 60 | 6.9 (4.6–9.1) |
| Avoid driving in unfamiliar areas | ||
| Never | 599 | 48.4 (44.6–52.2) |
| Sometimes | 517 | 43.3 (39.5–47.0) |
| Always | 79 | 8.3 (5.9–10.7) |
| Avoid driving during rush hour | ||
| Never | 406 | 33.5 (29.9–37.1) |
| Sometimes | 666 | 55.2 (51.4–59.0) |
| Always | 123 | 11.3 (8.7–13.8) |
| Avoid driving long distances | ||
| Never | 630 | 50.7 (46.9–54.5) |
| Sometimes | 454 | 38.2 (34.4–41.9) |
| Always | 112 | 11.1 (8.5–13.8) |
| Pass up opportunities to go out because of concerns about driving | ||
| Never | 925 | 75.7 (72.3–79.2) |
| Sometimes | 259 | 23.0 (19.5–26.4) |
| Always | 14 | 1.3 (0.5–2.1) |
Note. CI=confidence interval.
Sums may not equal total sample N because of missing data.
Data weighted on gender, age, household income, race/ethnicity, household size, education, census region, metropolitan status, and household internet access prior to panel participation.
Latent Class Analysis and Modeling Results
As the number of classes sequentially increased from two to three to four, the deviance statistic G2, the AIC, and the BIC all kept falling, suggesting a better model fit as the number of classes increased. The BIC started rising and the AIC fell marginally as the number of classes increased from four to five, indicating an uncertainty of benefit of increasing the number of classes (see Supplemental Table). Furthermore, consideration of parsimony and interpretability favored four over five classes. Therefore, a four-class model was selected, and the classes were labeled as low, mild, moderate, and high driving avoidance.
Among older drivers, 30.8% were expected to belong to the low-avoidance class, 34.3% to the mild-avoidance class, 28.7% to the moderate-avoidance class, and 6.3% to the high-avoidance class. Drivers in the high-avoidance class were less likely than those in the low-avoidance class to report driving as their primary mode of transportation (76.6%, 95% CI = 65.2%, 88.1%; and 97.5%, 95% CI = 95.6%, 99.4%; respectively) and were less likely to drive 3+ days/week (36.5%, 95% CI = 23.5%, 49.5%, and 87.9%, 95% CI = 83.9%, 91.9%; respectively).
The low-avoidance class had very high probabilities (>95%) in answering “never” in six out of nine driving questions (avoiding highway driving, making left turns, driving alone, driving on high traffic roads, driving in unfamiliar areas, and driving long distances) (Figure 1). Both the low- and mild-avoidance classes had very low probabilities (<5%) in answering “always” in all nine driving questions. In contrast, the high-avoidance class had far higher probabilities in answering “always” in all nine driving questions than other avoidance classes.
Figure 1.
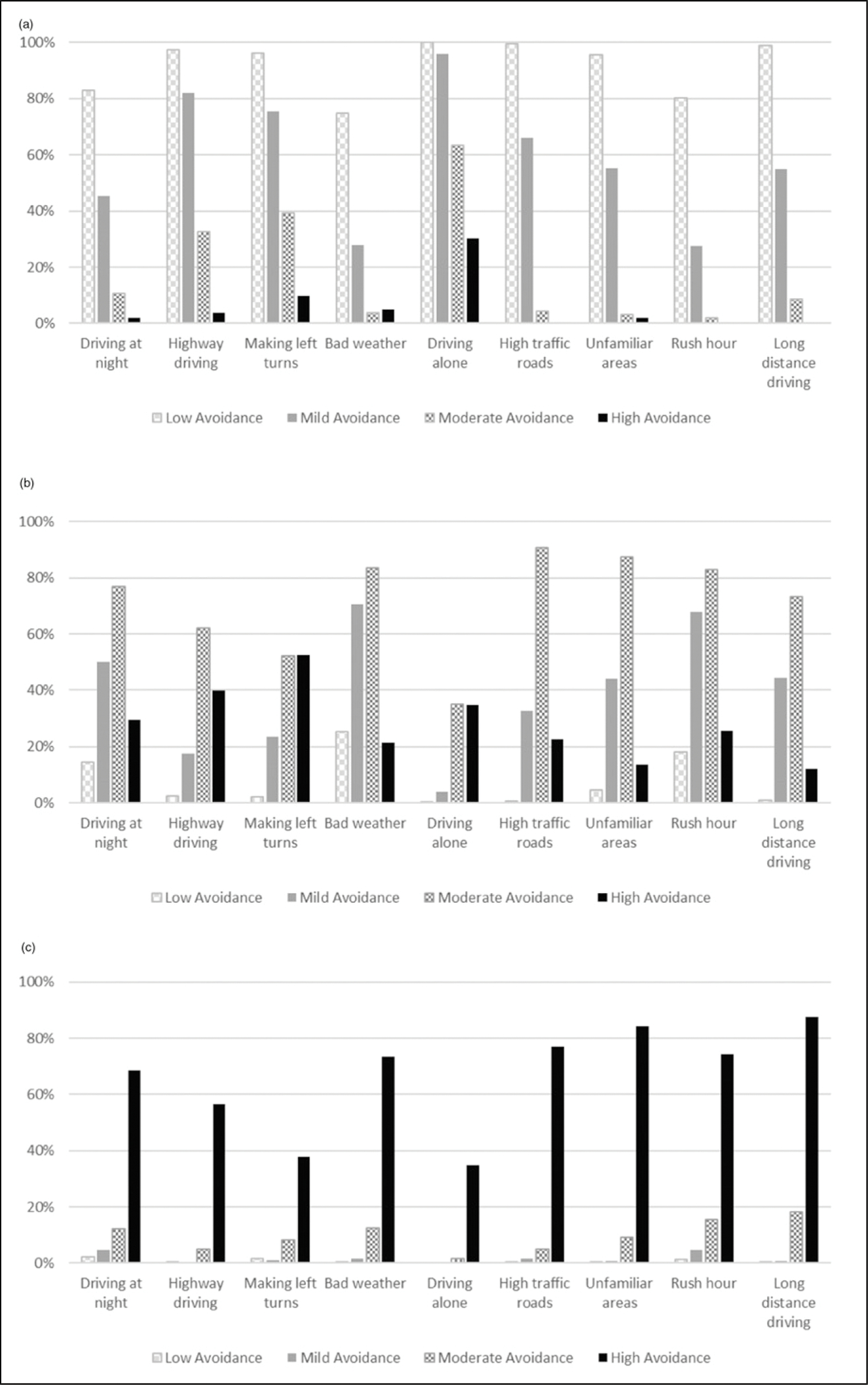
Weighted Prevalence of (a) Never, (b) Sometimes, or (c) Always Avoiding Driving Conditions by Driving Avoidance Class Among Current Drivers Age 60+ Years, ConsumerStyles 2015, United States, Sample N = 1198.
Differences were observed by avoidance class for frequency of passing up opportunities to go out because of driving concerns. Among low-avoidance drivers, 94.4% (95% CI = 91.6%, 97.2%) reported “never” passing up opportunities to go out, while 86.0% (95% CI = 82.0%, 90.0%), 55.6% (95% CI = 49.4%, 61.9%), and 20.4% (95% CI = 9.6%, 31.3%) of mild-, medium-, and high-avoidance drivers, respectively, reported “never” doing so (data not shown).
Education level and income were statistically significant in bivariate analyses and therefore included in the final model along with gender, age group, and race/ethnicity. Table 3 presents adjusted odds ratios separately for drivers in high, moderate, and mild (versus low) avoidance classes. AORs can be interpreted as the odds of one group (e.g., females) being in a particular class (e.g., high avoidance) over low avoidance relative to the odds of the referent group (e.g., males). Compared with males, females were more likely to be in high- (AOR = 6.9, 95% CI = 2.9, 16.4) and moderate-avoidance classes (AOR = 2.7; 95% CI = 1.7, 4.3) than the low-avoidance class. Drivers aged 75+ were more likely to be in the high-avoidance class (AOR = 5.7; 95% CI = 2.8, 11.9) than the low-avoidance class compared with drivers aged 60–74. Compared with White, non-Hispanic drivers, drivers in all other race/ethnicity categories were more likely to be in the high-avoidance class than the low-avoidance class. Compared with those with high school education or less, drivers with at least a bachelor’s degree were less likely to be in the high-avoidance class (AOR = 0.2, 95% CI = 0.1, 0.6) than the low-avoidance class. Drivers with annual household income <$25,000 were more likely to be in the high- (AOR = 4.0, 95% CI = 1.7, 9.1) and moderate-avoidance classes (AOR = 3.7, 95% CI = 1.9, 7.0) than the low-avoidance class compared with drivers with income ≥$25,000.
TABLE 3.
Multivariate Regression Predicting Membership in Driving Avoidance Latent Classes Among Current Drivers Age 60+ Years, ConsumerStyles 2015, United States, Sample N = 1198.a
| Variable | aORb (95% CI) for High Vs. Low Avoidance | aOR (95% CI) for Moderate Vs. Low Avoidance | aOR (95% CI) for Mild Vs. Low Avoidance |
|---|---|---|---|
|
| |||
| Gender (ref: Male): Female | 6.9 (2.9–16.4) | 2.7 (1.7–4.3) | 1.4 (0.8–2.4) |
| Age Group (ref: 60–74 years): 75+ years | 5.7 (2.8–11.9) | 1.4 (0.8–2.5) | 1.3 (0.8–2.4) |
| Race/Ethnicity (ref: White, non-Hispanic) | |||
| Black, non-Hispanic | 12.7 (3.3–48.9) | 4.8 (1.8–13.2) | 2.5 (0.7–9.3) |
| Hispanic | 3.3 (1.3–8.5) | 1.7 (0.8–3.8) | 0.7 (0.3–1.9) |
| Other or multiple races, non-Hispanic | 5.6 (1.4–22.0) | 1.5 (0.5–4.7) | 1.2 (0.4–3.5) |
| Education (ref: High school or less) | |||
| Some college | 1.1 (0.5–2.2) | 1.2 (0.7–2.0) | 1.2 (0.7–2.2) |
| Bachelor’s degree or higher | 0.2 (0.1–0.6) | 1.1 (0.6–1.9) | 1.1 (0.6–2.0) |
| Annual household income (ref: $25,000 or more): Less than $25,000 | 4.0 (1.7–9.1) | 3.7 (1.9–7.0) | 1.8 (0.8–4.0) |
Note. a OR = adjusted odds ratio. CI = confidence interval.
Data weighted on gender, age, household income, race/ethnicity, household size, education, census region, metropolitan status, and household internet access prior to panel participation.
Odds ratios adjusted for all other variables in table.
Discussion
Our study identified four classes of driving avoidance (low, mild, moderate, and high) among older drivers. High-avoidance drivers were more likely than those in other avoidance classes to always avoid measured behaviors, with more than half of high-avoidance drivers reporting “always” avoiding seven of the nine measured behaviors. In contrast, more than 95% of the low-avoidance drivers reported “never” avoiding six of the nine behaviors. High-avoidance drivers were more likely than low-avoidance drivers to be female, aged 75+, and not White/non-Hispanic. They were also more likely to have lower income and less likely to have a college education. While our study did not measure motivations for avoiding driving situations, the associations found between driving avoidance and sociodemographic characteristics are consistent with research on driving avoidance (Bergen et al., 2017), strategic self-regulation (Davis et al., 2016), and the broader concept of self-regulation (Ang et al., 2019; Barrett & Gumber, 2019). In a systematic review of studies on driving self-regulation among older people, Ang et al. (2019) found that females and those with advanced age were more likely to self-regulate. Barrett and Gumber (2019) reported that people with less education and who were non-Hispanic Black race/ethnicity were more likely to self-regulate.
While increasing age is associated with greater likelihood of driving self-regulation, driving avoidance, and cessation, it is not a singular predictor of when someone should stop driving. Rather, visual, physical, and cognitive functions are more important determinants of driving safety (Fraade-Blanar et al., 2018; Huisingh et al., 2017; Pomidor, 2019). Some medical conditions whose prevalence increases with age (e.g., diabetes, glaucoma, and obstructive sleep apnea) can affect driving ability and increase crash risk (Lococo et al., 2018; Marshall, 2008). Treatment for these and other conditions may include medications (e.g., insulin and oral diabetes medications and benzodiazepines) that increase crash risk (Hetland & Carr, 2014; Ivers & White, 2016; Lococo et al., 2018). Less is known about medical conditions, medication use, and driving behaviors, including driving avoidance, among older people. Our study did not find an association between number of self-reported medical conditions and driving avoidance, although we lacked data on medication use, how well medical conditions were managed, and onset and severity of disease.
Previous research has shown that former drivers are at risk not only for adverse health outcomes (Chihuri et al., 2016; Edwards et al., 2009; Fonda et al., 2001) but also for social isolation, as indicated by a lack of contacts or connections with family, friends, or neighbors (Chihuri et al., 2016; Edwards et al., 2009; Fonda et al., 2001; Qin et al., 2020). While gradual declines in social engagement occur with aging, these declines happen at a more rapid rate once driving cessation occurs (Curl et al., 2014). Some older drivers in our study may have been already experiencing some effects of reduced mobility with about one-fourth reporting sometimes or always passing up opportunities to go places because of concerns about driving. The frequency of sometimes or always passing up these opportunities was highest for high-avoidance drivers (80% versus 6% for low-avoidance drivers).
Given that driving cessation is associated with adverse health and quality of life outcomes (Chihuri et al., 2016; Edwards et al., 2009; Fonda et al., 2001), it could be beneficial to screen older drivers for their risk of driving cessation. The transition to driving cessation is often a gradual process, suggesting the possibility for intervention during stages of this process. Many people do not anticipate they will stop driving in the future and are unprepared when the time comes (Goins et al., 2015; King et al., 2011; Oxley & Charlton, 2009). Vivoda et al. (2021) found that driving cessation planning was relatively low among older drivers but identified important factors associated with planning, including lack of driving confidence and having a positive view of alternative transportation options. One way to increase awareness and encourage planning is the Centers for Disease Control and Prevention’s (n.d.) MyMobility Plan, which was designed to help people plan for how to stay safe, mobile, and independent as they age and has been shown to increase people’s thinking about and planning for future mobility changes (West et al., 2021). Harmon et al. (2018) found that older people believe they will have better future mobility if they plan for changes that come with age. Oxley and Charlton (2009) showed higher satisfaction with mobility among older people who chose when to stop driving compared to those for whom the decision was made without their input. Interventions could include promoting awareness of transportation options to help preserve mobility when people stop driving. In recent years, ride-hailing (or ride-sharing) has become more common in the U.S. and may become a viable option both for those who are limiting driving and for former drivers if their preferences and concerns regarding ride-hailing can be addressed (Bayne et al., 2021; Chaiyachati et al., 2018). Older people in rural areas are of special concern. Transportation options such as public transportation and ride-hailing services are not widely available in rural communities, which may explain at least in part, why older drivers in rural areas view driving as more important than drivers in suburban or urban areas (Strogatz et al., 2020).
Limitations
There are several limitations to consider. First, data were collected in 2015 as the use of ride-hailing (e.g., Uber, Lyft) was becoming more widespread in the U.S. While ride-hailing is less common among older than younger adults (4% of adults aged 65+ and 36% of adults aged 18–29 had used ride-hailing services during our study period [Clewlow & Mishra, 2017]), it is unknown how the increasing availability of ride-hailing services might influence older people’s driving patterns in the future. Second, data were self-reported and social desirability bias may have influenced respondents’ answers to questions they considered sensitive. Third, while randomly sampled to be nationally representative, participants were part of a survey panel and it is unknown how people who choose to be in a panel may differ from the general public. Fourth, we could not determine respondents’ motivations for avoiding certain driving behaviors, which is important for the concept of self-regulation (Molnar et al., 2015). Previous research has noted that some drivers avoid certain driving situations (e.g., bad weather) for reasons of personal preference and that these situations may be avoided by drivers of any age, although older people have a higher prevalence of avoidance (Naumann et al., 2011). It is unknown how much of the driving avoidance behavior measured in our study reflects personal preference versus self-regulation undertaken to compensate for functional limitations. Finally, we could not determine from the cross-sectional data whether the avoidance classes represent progressive stages over time. Longitudinal studies could help to overcome this limitation.
Strengths
Some strengths of the present study are worth noting. First, we used a nationally representative sample of older people to identify drivers. The sample’s distribution by age group and sex (78% aged 60–74; 54% female) was similar to, though slightly younger than, that of the U.S. population of people aged 60+ (70% and 55%, respectively). Exclusion of non-drivers from the study may explain the age difference between our sample and the U.S. population. Second, this study expands upon exploratory research conducted with members of a ride service program, who were much older (68% aged 80+) and more likely female (76%) than our sample and the U.S. population (Bergen et al., 2017). While Bergen et al. (2017) identified three classes of driving avoidance, our study identified four. Specifically, while our high and moderate classes resembled the high and medium classes from Bergen et al. (2017), we identified two distinct classes (low and mild) among people who reported lesser amounts of avoidance behavior compared to Bergen et al.’s (2017) one. Interestingly, while no sociodemographic differences were observed between these two classes, they were notably different in driving avoidance behaviors. For example, 15% and 50% of low- and mild-avoidance drivers, respectively, reported sometimes avoiding driving at night. As a result of these strengths, we believe the four classes are a better representation of driving avoidance than the three identified in Bergen et al.’s (2017) exploratory study.
Conclusions
The connections between driving and mobility, health, and quality of life point to the importance of preserving driving when it is safe to do so. Our study on driving avoidance behaviors identified four avoidance classes ranging from “low” to “high”. These four classes add to previous research to suggest an older adult driving continuum of six groups of drivers—those with no limitations, low-avoidance drivers, mild-avoidance drivers, moderate-avoidance drivers, high-avoidance drivers, and former drivers. Longitudinal studies are needed to evaluate whether the classes identified in our study represent stages through which an individual progresses on the route from unrestricted driving to driving cessation. Additionally, future studies of older drivers should explore motivations for driving avoidance—which could be due to lack of comfort or awareness of a need to address functional limitations—to better determine how these classes can further our understanding of strategic driving self-regulation.
Interventions tailored to individual drivers can improve driving performance (Fausto et al., 2021; Sangrar et al., 2019), suggesting that an approach focused on meeting the needs of older drivers in different classes may be important. High-avoidance drivers may have a more pressing need than others for information about transportation options (such as ride-hailing or ride-sharing) to meet mobility needs when they are not able or choose not to drive. The classification of driving avoidance behavior allows for the characterization of older drivers who may be approaching driving retirement who could benefit from resources to prepare for this transition and minimize negative outcomes associated with driving cessation.
Supplementary Material
What This Paper Adds.
The four classes of driving avoidance identified among older people, adding to previous research, suggest an older adult driving continuum of six groups of drivers—those with no limitations, low-avoidance drivers, mild-avoidance drivers, moderate-avoidance drivers, high-avoidance drivers, and former drivers.
Compared with low-avoidance drivers, high-avoidance drivers were less likely to drive as their primary mode of transportation and more likely to report concerns about driving that caused them to miss opportunities to go out.
Applications of Study Findings.
Driving avoidance class may be useful for identifying those who are close to driving cessation and most in need of non-driving transportation options.
Utilization of latent class analysis methods that identified distinct classes of driving avoidance could be beneficial for future research on self-regulation of driving among older people.
Acknowledgments
The authors wish to acknowledge Krishnaveni Subbiah, MPH, for her assistance with preliminary data analysis during her internship through the Emory University’s Rollins Earn and Learn program.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Supplemental Material
Supplemental material for this article is available online.
References
- Administration for Community Living. (2021). 2020 profile of older Americans. U.S. Department of Health and Human Services. https://acl.gov/sites/default/files/Aging%20and%20Disability%20in%20America/2020ProfileOlderAmericans.Final_.pdf [Google Scholar]
- Ang BH, Oxley JA, Chen WS, Yap KK, Song KP, & Lee S (2019). To reduce or to cease: A systematic review and metaanalysis of quantitative studies on self-regulation of driving. Journal of Safety Research, 70, 243–251. 10.1016/j.jsr.2019.07.004 [DOI] [PubMed] [Google Scholar]
- Barrett AE, & Gumber C (2019). Feeling older and driving less: The effect of age identity on older adults’ transition from driving. Innovation in Aging, 3(1), igz004. 10.1093/geroni/igz004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bayne A, Siegfried A, Beck LF, & Freund K (2021). Barriers and facilitators of older adults’ use of ride share services. Journal of Transport & Health, 21, 101055. 10.1016/j.jth.2021.101055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bergen G, West BA, Luo F, Bird DC, Freund K, Fortinsky RH, & Staplin L (2017). How do older adult drivers self-regulate? Characteristics of self-regulation classes defined by latent class analysis. Journal of Safety Research, 61, 205–210. 10.1016/j.jsr.2017.01.002 [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (n.d.) My Mobility Plan. Retrieved February 9, 2021, from https://www.cdc.gov/transportationsafety/older_adult_drivers/mymobility/index.html
- Chaiyachati KH, Hubbard RA, Yeager A, Mugo B, Lopez S, Asch E, Shi C, Shea JA, Rosin R, & Grande D (2018). Association of rideshare-based transportation services and missed primary care appointments: A clinical trial. JAMA Internal Medicine, 178(3), 383–389. 10.1001/jamainternmed.2017.8336 [DOI] [PubMed] [Google Scholar]
- Chihuri S, Mielenz TJ, DiMaggio CJ, Betz ME, DiGuiseppi C, Jones VC, & Li G (2016). Driving cessation and health outcomes in older adults. Journal of the American Geriatrics Society, 64(2), 332–341. 10.1111/jgs.13931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi M, Adams KB, & Mezuk B (2012). Examining the aging process through the stress-coping framework: application to driving cessation in later life. Aging & Mental Health, 16(1), 75–83. 10.1080/13607863.2011.583633 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clewlow RR, & Mishra GS (2017). Disruptive transportation: The adoption, utilization, and impacts of ride-hailing in the United States. Institute of Transportation Studies, University of California, https://escholarship.org/uc/item/82w2z91j [Google Scholar]
- Curl AL, Stowe JD, Cooney TM, & Proulx CM (2014). Giving up the keys: How driving cessation affects engagement in later life. The Gerontologist, 54(3), 423–433. 10.1093/geront/gnt037 [DOI] [PubMed] [Google Scholar]
- Davis J, Conlon E, Ownsworth T, & Morrissey S (2016). Measuring situational avoidance in older drivers: an application of Rasch analysis. Accident Analysis & Prevention, 87, 68–77. 10.1016/j.aap.2015.11.018 [DOI] [PubMed] [Google Scholar]
- Dickerson AE, Molnar LJ, Eby DW, Adler G, Bédard M, Berg-Weger M, Classen S, Foley D, Horowitz A, Kerschner H, Page O, Silverstein NM, Staplin L, & Trujillo L (2007). Transportation and aging: A research agenda for advancing safe mobility. The Gerontologist, 47(5), 578–590. 10.1093/geront/47.5.578 [DOI] [PubMed] [Google Scholar]
- Edwards JD, Lunsman M, Perkins M, Rebok GW, & Roth DL (2009). Driving cessation and health trajectories in older adults. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 64(12), 1290–1295. 10.1093/gerona/glp114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fabbri E, Zoli M, Gonzalez-Freire M, Salive ME, Studenski SA, & Ferrucci L (2015). Aging and multimorbidity: New tasks, priorities, and frontiers for integrated gerontological and clinical research. Journal of the American Medical Directors Association, 16(8), 640–647. 10.1016/j.jamda.2015.03.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fausto BA, Adorno Maldonado PF, Ross LA, Lavallière M, & Edwards JD (2021). A systematic review and metaanalysis of older driver interventions. Accident Analysis and Prevention, 149(11), 105852. 10.1016/j.aap.2020.105852 [DOI] [PubMed] [Google Scholar]
- Fonda SJ, Wallace RB, & Herzog AR (2001). Changes in driving patterns and worsening depressive symptoms among older adults. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 56(6), S343–S351. 10.1093/geronb/56.6.s343 [DOI] [PubMed] [Google Scholar]
- Fraade-Blanar LA, Ebel BE, Larson EB, Sears JM, Thompson HJ, Chan K, & Crane PK (2018). Cognitive decline and older driver crash risk. Journal of the American Geriatrics Society, 66(6), 1075–1081. 10.1111/jgs.15378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goins RT, Jones J, Schure M, Rosenberg DE, Phelan EA, Dodson S, & Jones DL (2015). Older adults’ perceptions of mobility: A metasynthesis of qualitative studies. The Gerontologist, 55(6), 929–942. 10.1093/geront/gnu014 [DOI] [PubMed] [Google Scholar]
- Gwyther H, & Holland C (2012). The effect of age, gender and attitudes on self-regulation in driving. Accident Analysis & Prevention, 45, 19–28. 10.1016/j.aap.2011.11.022 [DOI] [PubMed] [Google Scholar]
- Harmon A, Babulal G, Vivoda J, Zikmund-Fisher B, & Carr D (2018). Planning for a nondriving future: Behaviors and beliefs among middle-aged and older drivers. Geriatrics (Basel, Switzerland), 3(2), 19. 10.3390/geriatrics3020019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hetland A, & Carr DB (2014). Medications and impaired driving. The Annals of Pharmacotherapy, 48(4), 494–506. 10.1177/1060028014520882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huisingh C, Levitan EB, Irvin MR, MacLennan P, Wadley V, & Owsley C (2017). Visual sensory and visual-cognitive function and rate of crash and near-crash involvement among older drivers using naturalistic driving data. Investigative Ophthalmology & Visual Science, 58(7), 2959–2967. 10.1167/iovs.17-21482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ivers T, & White ND (2016). Potentially Driver-Impairing Medications. American Journal of Lifestyle Medicine, 10(1), 17–20. 10.1177/1559827615609050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- King MD, Meuser TM, Berg-Weger M, Chibnall JT, Harmon AC, & Yakimo R (2011). Decoding the Miss Daisy syndrome: An examination of subjective responses to mobility change. Journal of Gerontological Social Work, 54(1), 29–52. 10.1080/01634372.2010.522231 [DOI] [PubMed] [Google Scholar]
- Lanza ST, Collins LM, Lemmon DR, & Schafer JL (2007). PROC LCA: A SAS procedure for latent class analysis. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 671–694. 10.1080/10705510701575602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanza ST, Dziak JJ, Huang L, Wagner A, & Collins LM (2015). PROC LCA user’s guide, version 1.3.2. The Methodology Center, The Pennsylvania State University. https://www.methodology.psu.edu/files/2019/03/proc_lca_lta_1-3-2-1_users_guide-2ggq4d3.pdf [Google Scholar]
- Lanza ST, Flaherty BP, & Collins LM (2003). Latent class and latent transition analysis. In Schinka JA & Velicer WF (Eds.), Handbook of psychology: Research methods in psychology (Vol. 2, pp. 663–685). John Wiley & Sons, Inc. 10.1002/0471264385.wei0226 [DOI] [Google Scholar]
- Lococo KH, Staplin L, & Schultz MW (2018). The effects of medical conditions on driving performance: A literature review and synthesis. National Highway Traffic Safety Administration. https://www.nhtsa.gov/sites/nhtsa.gov/files/documents/13394-mediconlitreview-073018-v3-tag.pdf [Google Scholar]
- Marfeo E, Grinnell M, Coffey A, & Ward N (2021). Driver rehabilitation utilization and need among community-dwelling older adults. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association, 75(2), 7502205040p1–7502205040p7. 10.5014/ajot.2020.040501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marottoli RA, de Leon CFM, Glass TA, Williams CS, Cooney LM Jr, & Berkman LF (2000). Consequences of driving cessation: decreased out-of-home activity levels. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 55(6), S334–S340. 10.1093/geronb/55.6.s334 [DOI] [PubMed] [Google Scholar]
- Marshall SC (2008). The role of reduced fitness to drive due to medical impairments in explaining crashes involving older drivers. Traffic Injury Prevention, 9(4), 291–298. 10.1080/15389580801895244 [DOI] [PubMed] [Google Scholar]
- Molnar LJ, Eby DW, Zhang L, Zanier N, St Louis RM, & Kostyniuk LP (2015). Self-regulation of driving by older adults: A LongROAD study (Technical Report). AAA Foundation for TrafficSafety. https://aaafoundation.org/self-regulationdriving-older-adults/ [Google Scholar]
- Naumann RB, Dellinger AM, & Kresnow MJ (2011). Driving self-restriction in high-risk conditions: How do older drivers compare to others? Journal of Safety Research, 42(1), 67–71. 10.1016/j.jsr.2010.12.001 [DOI] [PubMed] [Google Scholar]
- Oxley J, & Charlton J (2009). Attitudes to and mobility impacts of driving cessation: Differences between current and former drivers. Topics in Geriatric Rehabilitation, 25(1), 43–54. 10.1097/TGR.0b013e3181914aeb [DOI] [Google Scholar]
- Pomidor A (Ed.). (2019). Clinician’s guide to assessing and counseling older drivers(4th ed.). The American Geriatrics Society. [Google Scholar]
- Porter Novelli. (n.d.). Porter Novelli styles: ConsumerStyles & Youth Styles. Retrieved February 9, 2021, from Porter Novelli. http://styles.porternovelli.com/consumer-youthstyles/ [Google Scholar]
- Qin W, Xiang X, & Taylor H (2020). Driving cessation and social isolation in older Adults. Journal of Aging and Health, 32(9), 962–971. 10.1177/0898264319870400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sangrar R, Mun J, Cammarata M, Griffith LE, Letts L, & Vrkljan B (2019). Older driver training programs: A systematic review of evidence aimed at improving behind-the-wheel performance. Journal of Safety Research, 71, 295–313. 10.1016/j.jsr.2019.09.022. [DOI] [PubMed] [Google Scholar]
- Shen S,Koech W,Feng J,Rice TM,&Zhu M(2017).Across-sectional study of travel patterns of older adults in the USA during 2015: Implications for mobility and traffic safety. BMJ open, 7(8), e015780. 10.1136/bmjopen-2016-015780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strogatz D, Mielenz TJ, Johnson AK, Baker IR, Robinson M, Mebust SP, Andrews HF, Betz ME, Eby DW, Johnson RM, Jones VC, Leu CS, Molnar LJ, Rebok GW, & Li G (2020). Importance of driving and potential impact of driving cessation for rural and urban older adults. The Journal of Rural Health, 36(1), 88–93. 10.1111/jrh.12369 [DOI] [PubMed] [Google Scholar]
- United Nations Department of Economic and Social Affairs, Population Division. (2020). World population ageing 2020 highlights: Living arrangements of older persons (ST/ESA/SER.A/451). https://www.un.org/development/desa/pd/sites/ www.un.org.development.desa.pd/files/undesa_pd-2020_world_population_ageing_highlights.pdf
- United States Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. (2020). Bridged-race population estimates, United States July 1st resident population by state, county, age, sex, bridged-race, and Hispanic origin. Compiled from bridged-race vintage 2019 (2010–2019) postcensal population estimates. Retrieved January 28, 2021, from http://wonder.cdc.gov/bridged-race-v2019.html
- Vivoda JM, Cao J, Koumoutzis A, Harmon AC, & Babulal GM (2021). Planning for driving retirement: the effect of driving perceptions, driving events, and assessment of driving alternatives. Transportation Research Part F, Traffic Psychology and Behaviour, 76, 193–201. 10.1016/j.trf.2020.11.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- West BA, Bergen G, & Moreland B (2021). Older adults’ attitudes about future mobility changes and the usefulness of mobility assessment materials. Journal of Applied Gerontology, 40(10), 1356–1365. 10.1177/0733464820947927 [DOI] [PubMed] [Google Scholar]
- Wong IY, Smith SS, Sullivan KA, & Allan AC (2016). Toward the multilevel older person’s transportation and road safety model: A new perspective on the role of demographic, functional, and psychosocial factors. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 71(1), 71–86. 10.1093/geronb/gbu099 [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2015). World report on ageing and health. WHO. https://apps.who.int/iris/handle/10665/186463 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.