

Abstract
Background:
Theories of suicide suggest that suicidal ideation (SI) results in part from difficulty imagining the future, which itself relies on the ability to remember the past. The present study examines multiple components of episodic future thinking and memory including event richness, which is commonly measured within the cognitive literature but has not previously been assessed with suicidal individuals.
Method:
Here, we tested the associations between SI and episodic future thinking and episodic memory across two studies (n = 25. n = 141): the first with a healthy comparison group and the second with a psychiatric comparison group.
Results:
Future event richness yielded large but statistically non-significant deficits in the SI group relative to healthy controls in Study 1 after controlling the False Discovery Rate. The most robust effects for future thinking deficits emerged in the case of perceived duration of future events, such that the SI group (vs. psychiatric comparison) imagined future events as longer-lasting in Study 2. Across both studies episodic memory was unrelated to SI, and neither episodic future thinking nor memory predicted future SI.
Conclusions:
Episodic future thinking may better distinguish individuals with SI history from psychiatric controls when compared with episodic memory, but that this effect is limited to select components of future thinking.
Keywords: Episodic future thinking, episodic memory, cognition, suicidal ideation, suicide, veterans
Suicidal ideation (SI) is prevalent, distressing, and debilitating. Nearly one in ten people have experienced SI in their lifetime (Nock et al., 2008), and suicidal individuals are vulnerable to a wide range of adverse psychosocial outcomes, including lower socioeconomic status, higher likelihood of psychopathology, and greater risk for suicide attempt later in life (Reinherz et al., 2006). Yet, despite our increased awareness of SI as a public health problem, we are remarkably limited in our understanding of who is at greatest risk of killing themselves (Franklin et al., 2017).
Both theory and empirical research suggest that cognition – everyday thought processes that ultimately affect our decisions, desires, and behaviors – is a domain of particular importance for understanding suicidal thoughts and behaviors (Cha et al., 2019). Cognitive risk factors1 for SI may include thought patterns that directly pertain to SI (e.g., implicit biases about death and life; Cha et al., 2018; Glenn et al., 2017) as well as more basic cognitive deficits (e.g., executive functioning; Miranda et al., 2013). Although prospective studies investigating suicide-related thought patterns have revealed some robust effects, more general cognitive deficits have received less attention and the work that has been conducted has revealed mixed findings (Cha et al., 2019). To help address this knowledge gap, here we focus on two particular aspects of cognition: episodic future thinking and episodic memory.
Episodic future thinking, or imagining a specific personal event occurring in the future (Schacter et al., 2017), may play an especially critical role in explaining SI. Prior theories have proposed that poor episodic future thinking may leave a person with few solutions to their current situation, impair one’s ability to ‘rescue’ themselves from such a scenario, and may ultimately facilitate the transition from a sense of entrapment2 to suicidal thoughts and behaviors (O’Connor, 2011; Williams, 2001). This idea has been supported by numerous studies detecting episodic future thinking deficits among suicidal individuals (MacLeod et al., 1998; O’Connor et al., 2008; O’Connor et al., 2007).
A closely related but distinct cognitive domain is episodic memory. Episodic memory refers to the recollection of a specific personal event that occurred in the past and is distinct from semantic memory (i.e., the remembering of facts and occurrences that were not personally experienced; Tulving, 1983). Suicide theories have suggested that an overly vague sense of the past marks limited access to discrete event details from which they can learn and draw from, thereby inhibiting judgments and decisions and exacerbating a perceived lack of opportunity to escape (Wenzel & Beck, 2008; Williams et al., 2006). These episodic memory deficits have also been detected among suicidal individuals, and those deficits have been reported to be greater than deficits in other forms of memory (e.g., semantic memory; Petterson et al., 2010; Richard-Devantoy et al., 2014, 2015) and have been found to be associated with problem-solving deficits among suicidal individuals (Pollock & Williams, 2001; Sidley et al., 1997). Like episodic future thinking, episodic memory has multiple components (Tulving, 2002). Within the suicide literature, perhaps the most commonly studied aspect of episodic memory is specificity: the ability to recall a past event that occurred at a specific time (less than 1 day) and a specific place (e.g., Williams & Broadbent, 1986).
Despite the empirical support and conceptual appeal of these cognitive processes, there remains much to be understood about episodic future thinking, episodic memory deficits, and their association with SI. Whereas cognitive psychologists have emphasized the multifaceted nature of episodic future thinking and episodic memory (see Schacter et al., 2017; Szpunar et al., 2014; Tulving, 1983, 2002), the extant SI literature has not tested exactly which of these many features relate to SI. One possible obstacle to understanding these individual components is the use of composite scores to assess future thinking in the clinical literature. For example, one common measure of future thinking in the SI literature is a composite measure that integrates event fluency (i.e., the ease with which an individual can imagine multiple future events) with other subjectively perceived event characteristics (e.g., the likelihood of the event occurring in the future and emotional valence of the event; Hunter & O’Connor, 2003; MacLeod et al., 1998; MacLeod et al., 2004, 2005). These composite measures are theoretically grounded and not inherently problematic, but they risk obscuring discrete underlying deficits. Indeed, research in related areas (e.g., depression) has shown that event fluency is more strongly associated with depressive symptoms than event characteristics (e.g., self-reported likelihood; Kosnes et al., 2013). A higher-resolution and more multi-faceted assessment of episodic future thinking has never been applied to the SI literature3 but offers considerable promise. Indeed, developers of composite measures themselves have argued that future thinking is not a uniform construct, and that its associations with clinical outcomes will depend on the features assessed (MacLeod & Cropley, 1995).
Another obstacle to better understanding future thinking and its association with suicidal thoughts is the predominant use of measures developed within the clinical literature rather than those drawn from cognitive science. Indeed, there are other features of episodic future thinking and episodic memory that have been studied by cognitive psychologists that have never been explored with suicidal individuals. Of particular relevance is the quality of single-event imagination or recall—hereafter referred to as event richness. In the cognitive psychology literature, this feature is typically captured using the Autobiographical Interview (Levine et al., 2002), which offers a performance-based index of one’s ability to fill a single recalled or imagined event with episodic details (i.e., internal details; for a review, see Miloyan et al., 2019). A unique feature of this measure is that it captures the quality of each event, which is different from prior measures in the SI literature that emphasize the quantity of events (i.e., event fluency). Moreover, the performance-based nature of this measure helps to capture demonstrated ability rather than perceived ability (i.e., event characteristics). Drawing from event richness data, cognitive psychologists have found that episodic future thinking plays an integral role in many aspects of everyday functioning, including problem-solving (Madore & Schacter, 2014) and prosocial intentions (Gaesser & Schacter, 2014; for a review, see Schacter et al., 2017). Further, there is evidence to suggest that increasing event richness can improve problem-solving, reduce negative affect, and increase positive affect (Jing et al., 2016). Despite its potential clinical relevance, event richness has never been used to assess future thinking among suicidal individuals. Doing so may not only help bridge the SI literature with a broader knowledge base around episodic future thinking, but it may also connect suicidal adults with the promising aforementioned manipulations designed to improve episodic future thinking (Jing et al., 2016; Madore et al., 2014; Madore & Schacter, 2016).
In this study, we aimed to address these gaps in the prior literature by investigating episodic future thinking and episodic memory among suicidal and nonsuicidal adults using assessments drawn from both the clinical and cognitive psychology literatures. We assessed multiple features of these cognitive processes: event fluency (i.e., number of total events listed), event richness (i.e., internal details), and event characteristics (i.e., self-report ratings of vividness of recollection, event duration, likelihood of event occurrence, similarity to other events, emotional valence, and arousal). First, we examined whether any features of episodic future thinking and episodic memory were concurrently associated with SI. Second, we examined whether any features of episodic future thinking and episodic memory prospectively predicted SI. Given the prior literature, we expected to observe less fluent, specific, and detailed past and future thinking among those with suicidal thoughts relative to those without. A priori hypotheses pertaining to the relative strength of associations were not specified as this was the first time administering this full assessment battery to suicidal adults.
We pursued our aims across two studies. In Study 1, we compared suicidal adults with healthy non-psychiatric controls. This initial study allowed us to gauge the feasibility of this novel battery and was adequately powered to detect very large deficits in episodic memory or future thinking in those with SI relative to healthy controls, which have been commonly reported in the prior literature (Williams et al., 2007). In Study 2, we compared suicidal military veterans seeking psychiatric care with psychiatric controls also seeking care at the time of the assessment. Study 2 allowed us to investigate whether specific episodic future thinking and episodic memory deficits were present among those with SI relative to those with other psychiatric diagnoses.
STUDY 1
Method
Sample
Participants were 26 adults (M = 33.4 years, SD = 13.6) recruited through online advertisements and flyers posted throughout the community and local hospitals. This sample size, with a planned equal number of SI and nonsuicidal control participants (n = 13 each), was determined a priori based on: (a) an efficient study timeline to yield a quick and preliminary gauge of feasibility, (b) a sample sufficient to have adequate power for detecting very large effects,4 as have been commonly reported in the literature when comparing clinical and non-clinical samples (achieved power = 78% to detect d = 1.12, with two-tailed α = .05 as reported in comparison of clinical vs. non-clinical samples in Williams et al., 2007), and (c) the limited amount of study funds available to support the project. Participants were mostly female (60%), White (68%; 12% Black, 4% Hispanic, 4% Asian, 12% other), and never married (68%; 16% married, 8% divorced, 8% other), with at least some college education (88%). The sample featured 13 adults with SI in the past year (i.e., SI group) and 13 adults who had never experienced SI or suicide attempt in their lifetime (i.e., control group). One enrolled participant from the SI group was unable to comprehend and complete key measures during their lab visit and so was excluded from analyses a priori, yielding a final sample of 25 adults. Although inclusion criteria required suicidal ideation to have been experienced within the past year, it is worth noting that 50.0% (n = 6) of the SI group had most recently experienced suicidal ideation in the past week. Moreover, 58.3% (n = 7) reported having ever attempted suicide. There were no significant differences between SI and control groups across age, gender, race/ethnicity, marital status, or education level (ps = .13−.69). The SI group, however, was more likely to identify as non-heterosexual (Φ = .52, p = .01) and endorsed more depressive symptoms (d = 3.51, p < .001). See Table 1 for additional details.
Table 1.
Sample Characteristics
| Study 1 | Study 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy Control1 (n=13) | SI (n=12) | df | ES | Psychiatric Control2 (n=67) | SI (n=74) | df | ES | ||
|
Age
M (SD) |
38.4 (32.0) | 29.0 (11.4) | 23 | d=−0.66 | 45.2 (14.2) | 39.2 (12.3) | 139 | r=−.21* | |
|
Gender
% Female |
53.8 | 66.7 | 1 | Φ=.13 | 16.4 | 40.5 | 1 | Φ=.27** | |
| Race/Ethnicity (%) | 3 | Φ=.33 | 3 | Φ=.17 | |||||
| White | 69.2 | 66.7 | 80.6 | 78.3 | |||||
| Black | 15.4 | 8.3 | 17.9 | 13.5 | |||||
| Hispanic | 0.0 | 8.3 | 0.0 | 4.1 | |||||
| Other | 15.4 | 16.7 | 1.5 | 4.1 | |||||
|
Sexual Orientation % Non-Heterosexual |
0.0 | 41.7 | 1 | Φ=.52* | -- | -- | -- | -- | |
| Education (%) | 3 | Φ=.22 | 4 | Φ=.13 | |||||
| High School or earlier | 15.4 | 8.3 | 28.4 | 25.7 | |||||
| Technical School | 0.0 | 0.0 | 6.0 | 10.8 | |||||
| Some College | 30.8 | 50.0 | 38.8 | 44.6 | |||||
| College graduate | 38.4 | 25.0 | 16.4 | 12.2 | |||||
| Post-grad | 15.4 | 16.7 | 10.4 | 6.7 | |||||
| Marital Status (%) | 3 | Φ=.28 | 3 | Φ=.10 | |||||
| Never Married | 61.5 | 75.0 | 40.3 | 39.2 | |||||
| Married | 15.4 | 16.7 | 16.4 | 10.8 | |||||
| Divorced/Separated | 15.4 | 0.0 | 40.3 | 44.6 | |||||
| Other | 7.7 | 8.3 | 3.0 | 5.4 | |||||
|
Depression
M (SD) |
1.2 (1.2) | 10.6 (3.8) | 23 | d=3.51*** | 13.3 (6.4) | 20.2 (6.0) | 138 | r=.43*** | |
| Verbal Fluency | 24.2 (5.6) | 22.4 (4.6) | 20 | d=0.20 | -- | -- | -- | -- | |
Note. SI=Suicidal ideation (past year history); Healthy Control
=Nonpsychiatric comparison group featuring no lifetime history of SI and attempt. Psychiatric Control
=Psychiatric comparison group featuring no past year history of SI and attempt. Depression was assessed via QIDS in Study 1 and via PHQ-9 in Study 2.
p < .05.
p < .01.
p < .001.
Procedure
Participants completed a series of measures assessing episodic future thinking and episodic memory, followed by all other assessments, including an interview to obtain a history of self-injurious thoughts and behaviors. Participants then returned to the lab one week later for a follow-up visit, from which data on past-week SI were procured. They were offered $50 compensation for the initial visit, $50 for the second visit, and an additional $20 for completing both visits. All participants who completed lab-based assessments (n = 25) at baseline returned to the lab one week later, and among them, 16.0% (n = 4) experienced suicidal ideation during this brief follow-up period. These procedures and measures were approved by the Institutional Review Board of Harvard University.
Measures
Episodic Future Thinking.
Episodic future thinking was assessed in three parts: fluency count to capture event fluency, self-report ratings to capture event characteristics, and internal details to capture event richness. Example participant responses to each part of this assessment battery are provided in Table 2.
Table 2.
Measures of future event fluency, characteristics, and richness
| Event Fluency Think of as many [neg/pos] events as you can | Event Characteristics Rate each [previously listed] event | Event Richness Tell me as much detail as you can about [select event] | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Vivid | Duration | Likely | Similar | Valence | Arousal | ||||
| Negative | 1 | I will wait for the bus in the cold tonight | 5 | 1 | 4 | 4 | 2 | 4 | It’ll feel like it’s below freezing [PE] / at the bus station [PL] / waiting for the 66 to arrive. [E] / It usually takes me 15 minutes to walk to the bus stop from work / so this should be around 5:30 or so. [T] / Sometimes I forget my gloves / when I leave the house in the morning. / And I’ll be wondering how, yet again, I could forget gloves on such a cold day. [ET] / I’ll stick my hands in my pockets [E] / but still feel the cold wind hit my bare wrists. [PE] / |
| 2 | I will be late for work | 3 | 2 | 3 | 2 | 3 | 2 | ||
| 3 | I will be sick | 2 | 4 | 2 | 3 | 1 | 2 | ||
| Positive | 1 | I will play board games with friends | 4 | 2 | 5 | 2 | 4 | 3 | We’ll drive up [E] / to the steakhouse [PL] / around 7:00. [T] / It’s an expensive restaurant / but we go since we hear that the food is worth it. / We’ll sit down [E] / and order some beers [E] / and hear a game on TV in the background. [PE] / Maybe the Red Sox are playing the Yankees. [E] / And I look at the menu [E] / and am tempted by all of the starters. [ET] / The waitress will then walk up. [E] / I order a boneless rib-eye [E] / cooked medium-well [E] / with sauce on the side. [E] / |
| 2 | I will try a new restaurant this weekend | 5 | 2 | 4 | 4 | 4 | 4 | ||
| 3 | I will do well at work | 2 | 4 | 3 | 4 | 5 | 3 | ||
| 4 | I will buy flowers | 3 | 1 | 2 | 2 | 3 | 2 | ||
Note. Example responses are provided for fluency, characteristics, and richness of future (next week) events. Event fluency was assessed based on the ability to list as many events as possible in 1 minute. This process was implemented through four conditions determined by the combination of emotional valence (positive vs. negative) and temporal distance (next week vs. next 5–10 years). Event characteristics were assessed based on self-report ratings provided for each aforementioned future event. Event richness was assessed using internal details (IDs) coded from a bolded, single-event assessment, determined based on self-report ratings indicating sufficient temporal specificity and high vividness (i.e., highest vividness rating among those events with duration ratings equal to or less than 3). Bracketed annotations refer to internal detail subtypes assigned by coders: [E]=event, [T]=time, [PL]=place, [PE]=perceptual, [ET]=emotion/thought. Slashes separate individual detail segments, bolded text mark internal details, and italicized text grey highlights mark external details.
Part 1: Fluency count.
Fluency was assessed using an adapted version of the Future Thinking Task (MacLeod et al., 1998). Participants were asked to say out loud as many future events as possible within 1 minute. Participants listed events for four distinct categories characterized by emotional valence and temporal distance: negative events within the next week, positive events within the next week, negative events within the next 5–10 years, and positive events within the next 5–10 years. They were instructed to imagine events that could realistically happen within those time frames and that were fixed in a specific place and time. Across all participants, proximal time frames (next week) were assessed before distal time frames (5–10 years). Ordering of positive and negative event cues within each time frame was counterbalanced across participants.
Part 2: Self-report ratings.
After listing as many events as possible, participants then rated six characteristics of each future event they had listed during Part 1. These characteristics included: vividness (i.e., 1 = No image at all; 5 = Perfectly Clear/As Vivid as Normal Vision), duration (i.e., 1 = Minutes; 5 = 1 Week or More), likelihood (i.e., 1 = Not at all; 5 = Extremely), similarity to past events (i.e., 1 = Not at all; 5 = Extremely), valence (i.e., 1 = Very Negative; 5 = Very Positive), and arousal (i.e., 1 = Not at all; 5 = Extremely). In addition, a composite score of future thinking, originally developed by MacLeod et al. (1998) and commonly used within the suicide literature, was calculated by multiplying the total number of events (i.e., fluency) by the mean likelihood ratings and valence ratings. Composite scores are traditionally examined by valence, and are included in valence-specific analyses below.
Part 3: Internal details (IDs).
One event from each category listed in Part 1 (i.e., negative next week, positive next week, negative next 5–10 years, and positive next 5–10 years) was selected for Part 3. Events were selected based on self-report ratings indicating sufficient specificity (i.e., perceived as lasting less than 24 hours) and high vividness (i.e., perceived as the most vivid among the events listed within its respective category). If multiple events were rated as equally vivid within a single category, the first event listed by the participant was selected. For each Part 3 event, participants were shown an event-related phrase on a computer screen and asked to describe the event aloud in as much detail as possible. The phrase was taken from Part 1 of the Episodic Future Thinking measure. Following a procedure adapted from the Autobiographical Interview (Levine et al., 2002), participants were instructed to provide as many details as possible when describing the event, including spatiotemporal details, perceptual details, and thoughts and feelings they may experience during the imagined event. Participants completed this procedure for each of the four categories, describing the events aloud into a microphone for 3 minutes per event. The ordering of event cues was identical to each participant’s assigned category ordering during Part 1.
Trained coders who were blind to group membership later segmented and categorized the transcribed event descriptions according to the Autobiographical Interview coding procedure (Levine et al., 2002). Segments of event details were first coded as either being internal (i.e., episodic detail directly pertaining to the central event in the description) or external (i.e., semantic information, commentary, off-topic information, or episodic detail pertaining to an event different from the central event in the description). This coding yielded total internal detail (ID; i.e., the number of all episodic details generated within a single imagined future event) and total external detail (ED), averaged across event categories. IDs were further classified into subtypes capturing details specific to imagined event-related actions (ID-Event), places (ID-Place), time (ID-Time), perception (ID-Perceptual), and emotions/thoughts (ID-Emotion/Thought). Coders demonstrated good to excellent reliability across Total ID and ID-Time (average ICCs = .72−.75 [95% CIs = .40, .96]) and fair reliability across ID-Event and ID-Emotion/Thought (average ICCs = .51−.54 [95% CIs = .17, .92]). ID-Place and ID-Perceptual were excluded as their ICCs fell under .50. Coders demonstrated good reliability when coding external details (average ICC = .74 [95% CI = .43, .96]).5
Episodic Memory.
Following the assessment of episodic future thinking, participants underwent the same procedure but instead responded to past event prompts. Four past event categories were used (i.e., negative past week, positive past week, negative past 5–10 years, and positive past 5–10 years), with each participant following the same valence order as episodic future thinking measures.
Suicidal Thoughts and Behaviors.
SI was assessed through a portion of the Self-Injurious Thoughts and Behaviors Interview (SITBI; Nock et al., 2007). The SITBI is an interview assessing characteristics (e.g., recency, frequency) of SI, plan, gesture, attempt, and nonsuicidal self-injury. SI group membership was characterized by SITBI responses endorsing engagement in SI (i.e., thoughts of killing yourself) at least once in the past year. This was determined using responses to two SITBI questions: one screening for lifetime history of suicidal ideation and another assessing frequency of suicidal thoughts in the past year. Control group membership was characterized by SITBI responses denying past year or lifetime suicidal ideation or suicide attempt.
Depressive Symptoms.
The 16-item Quick Inventory of Depressive Symptoms (QIDS; Rush et al., 2003) was used to assess the frequency of major depressive disorder symptoms from the past two weeks. QIDS total scores range from 0 to 27, with higher scores indicating greater severity of depression symptoms. All items were used to calculate the total score except for item 12, as it pertained to SI.
Verbal Fluency.
Verbal fluency was captured using the Verbal Fluency Task (VFT), where individuals listed as many animals as they could within a single minute. VFT scores represent the total number of unique animals named.
Data Analysis Plan
To address Aim 1, we conducted independent samples t tests to examine measures of episodic future thinking and episodic memory between participants who have experienced SI in the past year versus nonsuicidal control participants. When needed, we applied square root transformations for measure scores to meet assumptions of normality. Ultimately, skewness and kurtosis of past and future thinking scores were acceptable (Zs < 2.58), except self-reported vividness ratings of past events (Zs = 2.91–3.37) for which nonparametric analyses were applied. Relatedly, we conducted Mixed ANOVAs to check for potential valence effects, where positively- and negatively-valenced measures of episodic future thinking and episodic memory were compared between SI and control groups. To address Aim 2, we conducted logistic regressions with baseline measures of episodic future thinking and episodic memory predicting presence (vs. absence) of SI one week later.
We applied the Benjamini-Hochberg procedure (Benjamini & Hochberg, 1995) throughout all analyses to control the false discovery rate (FDR) set at .05. All 25 participants included in the final sample completed key measures of past and future thinking. Select cases of missing data for other variables were handled via pairwise deletion. Little’s (1988) test yielded non-significant results, suggesting that these data were missing completely at random. Effect sizes were interpreted as small (d = 0.3, r = .1, ORs = 1.46–1.68)6, medium (d = 0.5, r = .3, ORs = 2.50–3.48), or large (d = 0.8, r =.5, ORs = 4.13–6.71) (Chen et al., 2010; Cohen, 1988). All analyses were run in SPSS version 27 (IBM Corporation, Armonk, NY, USA).
Results
Cross-sectional association with SI
No measure of episodic future thinking significantly differentiated the SI group from the control group after controlling the FDR (ps > .05; Table 3). However, ID and ID subtypes yielded medium to large effect sizes, with the SI group generating fewer Total IDs (d = −1.03) and fewer ID subtypes (ds = −0.86−−0.57) within each future event description relative to the control group. Total ID and ID-Event yielded the largest group differences, which were initially significant but then were no longer significant after controlling the FDR. Of note, non-episodic EDs yielded some of the smallest group differences. The contrasting pattern across episodic IDs and non-episodic EDs was notable (Figure 1a), though this interaction was not significant (F = 3.12, p = .09, ηp2 = .12).
Table 3.
Baseline Comparisons in Episodic Future Thinking
| Study 1 | Study 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy Control | Past Year SI | Psychiatric Control | Past Year SI | ||||||
| M (SD) | M (SD) | df | d | M (SD) | M (SD) | df | r | ||
| Fluency count | 6.52 (1.91) | 5.98 (1.57) | 23 | −0.32 | 6.61 (1.41) | 5.89 (1.62) | 137 | −.25a | |
| Self-report ratings | |||||||||
| Vivid | 3.31 (0.71) | 3.44 (0.46) | 23 | 0.24 | 3.60 (0.31) | 3.61 (0.37) | 136 | .05 | |
| Duration | 3.07 (0.74) | 3.41 (0.82) | 23 | 0.44 | 2.74 (0.49) | 3.03 (0.74) | 135 | .26 a | |
| Likely | 3.36 (0.50) | 3.36 (0.36) | 23 | −0.01 | 3.31 (0.41) | 3.31 (0.36) | 135 | .03 | |
| Similar | 3.12 (0.43) | 2.99 (0.36) | 23 | −0.32 | 3.32 (0.39) | 3.33 (0.51) | 135 | .01 | |
| Valence | 4.17 (0.25) | 4.24 (0.35) | 23 | 0.24 | 4.17 (0.25) | 4.24 (0.35) | 135 | .08 | |
| Arousal | 3.40 (0.52) | 3.72 (0.64) | 23 | 0.57 | -- | -- | -- | -- | |
| Internal details (IDs) | |||||||||
| Total ID | 35.67 (11.49) | 24.08 (11.94) | 23 | −1.03a | 26.18 (12.88) | 24.64 (12.27) | 136 | −.06 | |
| ID-Event | 17.98 (7.26) | 12.75 (5.22) | 23 | −0.86a | 14.71 (8.46) | 14.08 (8.14) | 136 | −.03 | |
| ID-Place | -- | -- | -- | -- | 1.95 (1.26) | 1.58 (1.09) | 136 | −.16 | |
| ID-Time | 2.02 (0.84) | 1.33 (0.96) | 23 | −0.79 | 1.14 (1.05) | 0.81 (0.53) | 136 | −.19 | |
| ID-Percept | -- | -- | -- | -- | 3.12 (2.79) | 3.45 (3.43) | 136 | .02 | |
| ID-Em/Tho | 5.08 (2.09) | 3.67 (3.00) | 23 | −0.57 | 5.34 (4.12) | 4.69 (3.00) | 136 | −.06 | |
| External details | 19.92 (8.86) | 20.06 (11.15) | 23 | 0.01 | 15.70 (9.22) | 14.00 (8.78) | 136 | −.08 | |
Note. ID=Internal details (coded episodic detail count from imagining/recalling events for 3 minutes); ID-Percept=Perceptual internal detail subtype; ID-Em/Tho=Emotion or thought-related internal details. External details represent non-episodic details. Fluency represents the total number of events imagined/recalled within 1 minute. All values represent an average across positive and negative event prompts. SR-Likely ratings were not assessed for past events. Bolded comparisons represent those that remain significant after controlling the False Discovery Rate via the Benjamini-Hochberg procedure.
p < .05 before controlling the FDR
Figure 1.
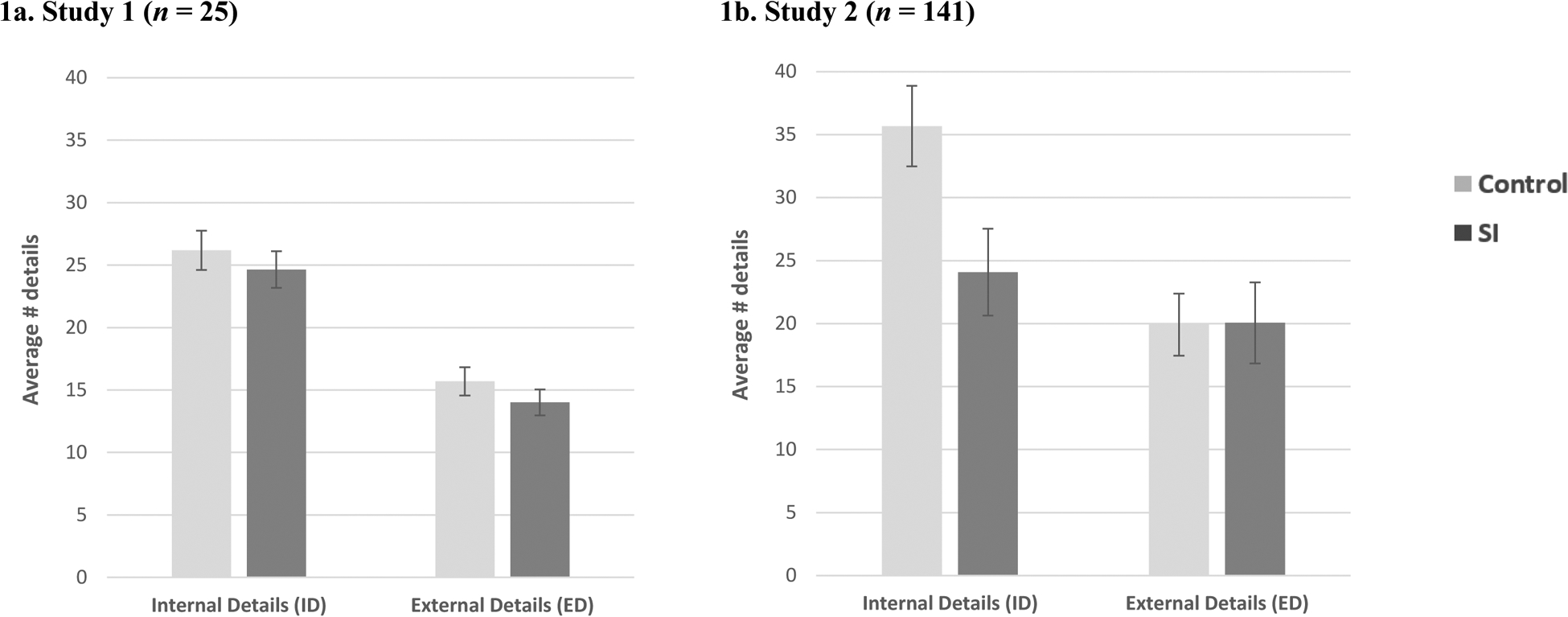
Comparison of Episodic and Non-Episodic Future Thinking
Note. Event richness is represented via Total ID (internal details), with higher values representing greater episodic future thinking. Higher values on external detail counts represent greater non-episodic thinking. None of these Group by Time interactions were significant (Fs = 0.00–3.12, ps = .09−.96). Error bars represent standard error.
Fluency yielded a relatively small effect size (d = −0.32), with the SI group listing fewer future events relative to the control group. Additionally, effect sizes of self-reported event characteristics ranged from small to medium,│ds│= 0.24–0.57, with the largest effects observed for event arousal (d = 0.57) and duration (d = 0.44). SI and control groups rated future events as equally likely to occur on average (d = −0.01). The aforementioned patterns did not significantly differ across positive and negative future events (i.e., Fs = 0.06–6.39, ps > .05; Supplemental Table 1).
Individual measures of future thinking were infrequently associated with one another (rs = −.43−.36, ps > .05; Supplemental Table 2). These relatively weak associations may help explain the differential findings across future thinking measures with suicidal thoughts and suggest that the assessment battery administered here is assessing distinct types of future-related thinking.
No measure of episodic memory significantly differentiated the SI group from the control group after controlling the FDR (Table 4), and nearly all effects ranged from small to medium. The largest effect sizes were observed for IDs, specifically Total ID (d = −0.66).
Table 4.
Baseline Comparisons in Episodic Memory
| Study 1 | Study 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy Control | Past Year SI | Psychiatric Control | Past Year SI | ||||||
| M (SD) | M (SD) | df | d | M (SD) | M (SD) | df | r | ||
| Fluency count | 6.19 (1.90) | 5.73 (1.64) | 23 | −.27 | 6.33 (1.65) | 5.97 (2.04) | 137 | −.14 | |
| Self-report ratings | |||||||||
| Vivid | 3.94 (0.85) | 4.04 (0.56) | 23 | .02b | 4.35 (0.30) | 4.43 (0.44) | 134 | .18a | |
| Duration | 3.13 (0.54) | 3.01 (0.80) | 23 | −.18 | 3.28 (0.61) | 3.39 (0.62) | 134 | .12 | |
| Similar | 3.27 (0.53) | 3.04 (0.48) | 23 | −.46 | -- | -- | -- | -- | |
| Valence | 3.79 (0.38) | 4.03 (0.48) | 23 | .59 | 2.97 (0.17) | 3.06 (0.54) | 134 | .03 | |
| Arousal | 3.14 (0.61) | 3.71 (0.51) | 23 | .47 | -- | -- | -- | -- | |
| Internal details (IDs) | |||||||||
| Total ID | 35.15 (12.19) | 27.73 (11.15) | 23 | −.66 | 35.71 (12.00) | 31.65 (11.06) | 98 | −.21a | |
| ID-Event | 17.27 (8.65) | 13.60 (5.65) | 23 | −.52 | 19.09 (6.39) | 17.38 (6.56) | 98 | −.15 | |
| ID-Place | -- | -- | -- | -- | 3.04 (1.66) | 2.56 (1.84) | 98 | −.19 | |
| ID-Time | 2.73 (1.05) | 2.23 (1.39) | 23 | −.43 | 2.72 (1.89) | 2.10 (1.33) | 98 | −.15 | |
| ID-Percept | -- | -- | -- | -- | 5.41 (4.33) | 4.70 (4.23) | 98 | .09 | |
| ID-Em/Tho | 4.83 (1.99) | 4.40 (1.87) | 23 | −.23 | 5.48 (4.40) | 5.09 (3.04) | 98 | −.01 | |
| External details | 25.85 (9.93) | 24.52 (15.14) | 23 | −.11 | 18.34 (10.74) | 16.26 (10.09) | 98 | −.09 | |
Note. ID=Internal details (coded episodic detail count from imagining/recalling events for 3 minutes); ID-Percept=Perceptual internal detail subtype; ID-Em/Tho=Emotion or thought-related internal details. External details represent non-episodic details. Fluency represents the total number of events imagined/recalled within 1 minute. No significant differences in autobiographical memory were detected across suicidal and nonsuicidal adults. No group comparisons remained significant after controlling the False Discovery Rate via the Benjamini-Hochberg procedure.
p < .05 before controlling the FDR
represents r value from non-parametric group comparisons.
Aforementioned patterns of episodic future thinking and memory did not significantly differ across positive and negative past events (Fs = 0.20–2.51, ps > .05). There were select Group by Measure interactions involving self-reported vividness, self-reported frequency, and the composite score, but none were significant after applying the Benjamini-Hochberg procedure. External details did not differ across groups (d = −0.11, p > .05).
Prospective prediction of SI
No measures of episodic future thinking significantly predicted SI one week later. The largest effect size emerged for ID-Time, which was initially predictive of future SI but no longer significant after controlling the FDR. The overall directionality of effects was as expected in the case of IDs, with lower counts predicting later SI (ORs = 0.17–0.91 [95% CIs = 0.03, 1.28], ps > .05). Neither fluency nor self-report ratings predicted future SI (ORs = 0.51–1.46 [95% CIs = 0.04, 56.92], ps > .05). Similarly, no measure of episodic memory significantly predicted future SI (ORs = 0.16–0.98 [95% CIs = 0.02, 7.45], ps > .05), and all effect sizes were small. See Supplemental Table 3 for additional details.
Discussion
Study 1 investigated multiple features of episodic future thinking and episodic memory in participants with and without a history of suicidal thoughts during the past year. This initial study demonstrated that an assessment battery of this scale could feasibly be administered to suicidal and nonsuicidal adults and identified areas in which the assessment could be improved (see the Method section of Study 2 for further detail). Apart from one participant who was excluded due to reasons unrelated to the episodic future thinking and memory measures, all participants provided complete sets of scores across event fluency, event characteristics, and event richness. Notably, we found that the individual components of future thinking (e.g., fluency, event duration, and event richness) exhibited weak correlations with one another, suggesting that this assessment may capture distinct aspects of future thinking and underscoring the value of having a single assessment that covers multiple components of future-related thought.
Study 1 findings concerning the association between these cognitive processes and suicidal ideation were more equivocal. For several of our measures of future thinking, we found moderate to large effect sizes in comparisons between suicidal and nonsuicidal adults. The largest differences were observed for event richness, a construct drawn from the cognitive psychology literature which had not previously been assessed in relation to suicidal thoughts. This pattern, however, was not significant after controlling the FDR. Moderate, nonsignificant effects were observed for measures of future thinking similar to those previously identified as being impaired in those with suicidal thoughts (i.e., event fluency, event duration). Similarly, though there were medium to large effects produced for event richness in our measures of episodic memory, there were again no statistically significant differences between groups for any component of episodic memory after controlling the FDR. Moreover, neither episodic memory nor episodic future thinking prospectively predicted SI one week later.
Both the effect size estimates and the significance tests from this initial study must be considered in the context of its small sample size, which limits our ability to obtain statistically significant findings for anything but very large effects, especially when adjusting for the many statistical tests that were run. Accordingly, although the effect size estimates suggest the possibility of a sizeable difference between groups, the small sample suggests that these estimates should be interpreted with caution. Further, the statistically non-significant findings signal that this study alone cannot be taken as evidence that either episodic memory or future thinking is poorer among those with suicidal thoughts. Nonetheless, the magnitude of these effects in the context of the prior literature suggests further research is warranted.
STUDY 2
Study 2 differed from Study 1 in several important ways. First, Study 2 featured a substantially larger sample, thereby overcoming a major limitation of Study 1 by providing greater power to detect differences between groups. Second, Study 2 made use of a psychiatric control group. In Study 1, there was a significant and very large difference between groups in the severity of depression, making it unclear whether the observed findings were specific to suicidal thoughts or attributable to the high rate of depression in the sample. Recruiting a large sample and psychiatric control group in Study 2 allowed us to evaluate whether any episodic future thinking and episodic memory deficits were specifically associated with SI relative to other psychiatric diagnoses in the absence of SI. Third, in Study 2 we tested longer-term prospective models. Whereas in Study 1 we were limited to evaluating suicidal ideation 1 week later, in Study 2 we assessed SI both 1 and 3 months later. Within the context of these changes, the same aims as Study 1 were pursued with the same expectation of less fluent, specific, and detailed past and future thinking in those with suicidal thoughts relative to those without.
Method
Sample
Participants for Study 2 were 158 veterans presenting for psychiatric care at either a Department of Veterans Affairs (VA) hospital psychiatric inpatient unit or VA outpatient treatment clinic who agreed to participate in a broader study of cognitive factors related to suicide (see Millner et al., 2018). This sample size was achieved through maximizing resources available within a three-year funding period. Veterans were at least 18 years of age (M = 42.1 years, SD = 13.5) and fluent in English. Any veteran who was deemed severely cognitively impaired or actively psychotic was not eligible for the study. From the overall sample of 158 participants, 17 were excluded from the current study for the following reasons: withdrawal from the study (n = 3), no future thinking data available (n = 5), and administration issues affecting quality of baseline assessment (e.g., clinical care-related interruptions during timed responses, computer error; n = 9). This yielded a final sample of 141 veterans for the current study. The sample was mostly male (70.1%), White (79.4%; 15.6% Black, 2.1% Hispanic, 2.9% other), never married (39.7%; 36.2% divorced, 13.5% married, 10.6% other), with at least some college education (64.5%). Veterans on average had multiple concurrent psychiatric diagnoses (M = 2.3, SD = 0.9), predominantly posttraumatic stress disorder (PTSD; 74.6%), substance use (74.6%), and depression (53.1%). There were no significant differences between those included and excluded across baseline characteristics (ps = .11−.98), with the exception of current PTSD diagnosis which was less common among those excluded from the study (p = .01). Within the final sample of 141 veterans, 52.5% (n = 74) had a past year history of SI, leaving sufficient power (1 - β = .84, α = .05, two-tailed) to detect medium-sized group differences (d = 0.5). Although inclusion criteria required suicidal ideation experienced at any point in the past year, it is worth noting that 93.2% (n = 69) of the SI group had most recently experienced suicidal ideation in the past week. Moreover, 68.9% (n = 51) reported having ever attempted suicide. The psychiatric control group (47.5%, n = 67) had no past year history of suicidal ideation or attempt, though some (n = 25) had experienced suicidal ideation prior to the past year. The SI group tended to be younger, had a higher proportion of females, and endorsed more severe depressive symptoms (ps = .00−.01). SI and control groups did not differ across other aforementioned baseline characteristics (ps = .30−.87). See Table 1 for details.
Procedure
Participants first completed self-report measures and interviews, including an assessment of demographic factors and history of suicidal thoughts and behaviors. Participants then completed key measures pertaining to episodic future thinking and episodic memory. Follow-up measures were administered by phone 1 and 3 months later by the research staff. Participants were compensated $15/hour in cash for the baseline assessments, and then mailed a $15 gift card for each follow-up call. Among the baseline sample, 63.8% (n = 90) completed the 1-month assessment and 46.1% (n = 65) completed the 3-month assessment. Those who did (vs. did not) complete the two follow-up time points were similar across baseline characteristics (ps = .14−.99). Exceptions included age, such that those who did complete both 1- and 3-month follow-up assessments tended to be older (ps = .01), and current diagnosis of depression which was more common among those who completed the 1-month follow-up assessment (p < .05). Among those who completed follow-up assessments, 22.2% (n = 20) and 20.0% (n = 13) reported suicidal ideation 1 and 3 months later, respectively. These procedures and measures were approved by the Institutional Review Boards of the VA Boston Healthcare System and Harvard University and by the Human Research Protection Office of the United States Army Medical Research and Materiel Command.
Measures
Episodic Future Thinking.
Study 2 used the same measures of episodic future thinking (fluency, self-report ratings, and IDs) used in Study 1, but with three exceptions. First, the ordering of both valence and temporal distance (vs. valence only) was counterbalanced across participants. Second, the research team offered additional guidance to participants during the Autobiographical Interview. Specifically, participants completed two practice events prior to critical event description trials and were prompted during event descriptions if they did not stay on task (e.g., described an event that lasted more than 24 hours, described multiple events). Finally, Study 2 featured stronger inter-rater reliability relative to Study 1. Study 2 coders underwent similar training as described under Study 1 and demonstrated good to excellent reliability when coding Total ID, ID-Event, ID-Time, ID-Perceptual, and ID-Emotion/Thought (average ICCs = .64−.87 [95% CIs = .48, .94]). They demonstrated fair reliability when coding ID-Place (average ICC = .54 [95% CI = .36, .73]) and good reliability when coding external details (average ICC = .62 [95% CI = .45, .79]).
Episodic Memory.
Measures of episodic memory used in Study 2 were identical to Study 1, with two exceptions made to reduce participant burden for the overall study. First, self-reported ratings of only vividness, duration, and valence of past events were collected. Second, event richness was assessed for only one time-frame: the past 5–10 years. Both positively- and negatively-valenced past event prompts were provided for audio recordings, with emotional valence counterbalanced across participants.
Self-Injurious Thoughts and Behavior.
The SITBI was administered at both baseline and follow-up time points. Those who endorsed past year history of SI were included in the SI group. Consistent with prior investigations from this dataset (Millner et al., 2018) and Study 1, the SITBI was used to determine SI group membership.
Depressive Symptoms.
The 9-item Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) was used to assess the frequency of major depressive disorder symptoms from the past two weeks. PHQ-9 total scores range from 0 to 27, with higher scores indicating greater severity of depressive symptoms. All items were used to calculate the total score except for item 9, as it pertained to SI.
Other Psychiatric Diagnoses.
Current diagnoses of the most common psychiatric diagnoses, PTSD and substance use disorder, were extracted from medical records.
Data Analysis Plan
Data analyses to test Aim 1 in Study 2 were similar to Study 1, but with several exceptions. First, non-normal distributions of episodic future thinking variables could not be resolved via transformations, and most past and future thinking variables displayed unacceptable levels of skewness and kurtosis (Zs > 2.58). We therefore used Mann-Whitney tests to make group comparisons. Second, the larger sample size featured in Study 2 provided more statistical power to test the robustness of prediction models via multivariate models testing baseline differences controlled for demographic and clinical correlates of SI history (i.e., age, gender, depressive symptoms, PTSD, substance use). Finally, we conducted logistic regressions with episodic future thinking and episodic memory measures predicting SI at baseline and two follow-up time points (1 and 3 months later). This analysis was carried out with the intention of conducting bivariate models first, then multivariate models controlling for the aforementioned covariates. Missing data were handled via pairwise deletion. Few (1–2%) participants were missing any measures of episodic future thinking at baseline, and more (1–29%) were missing measures of episodic memory. Little’s (1988) test indicated non-significant results, suggesting that these data were missing completely at random.
Results
Cross-sectional association with SI
Only select episodic future thinking measures revealed group differences. The SI group demonstrated modest deficits in future event fluency and self-reported duration relative to the psychiatric control group, which remained significant after controlling the FDR. In the case of fluency (r = −.25, p < .05), suicidal veterans tended to generate fewer future events compared with nonsuicidal veterans. Regarding duration (r = .26, p < .05), suicidal veterans reported that the future events they generated lasted longer relative to nonsuicidal veterans. When controlling for relevant demographic and clinical covariates (i.e., age, gender, PTSD, substance use, depressive symptoms), self-reported duration remained significantly associated with SI (OR = 2.25 [95% CI = 1.03, 4.91], p = .04) but fluency did not (OR = 0.89 [95% CI = 0.67, 1.17], p = .41). None of the other future thinking measures revealed significant group differences, including Total ID7 and ID subtypes (rs = −.19−.02, ps > .05) and the remaining self-report ratings (i.e., vividness, likelihood, uniqueness, valence; rs = .01−.08, ps > .05). Groups did not significantly differ in Total ID relative to external details (Figure 1b; F = 0.00, p = .96, ηp2 = .00). Similar to Study 1, these measures were infrequently associated with one another (Supplemental Table 5).
Suicidal veterans did not display episodic memory deficits relative to nonsuicidal veterans. Effects were uniformly modest, ranging from negligible group differences emerging in valence ratings (r = .03, p > .05) to a small difference in Total ID (r = −.21, p < .05) that was not significant after controlling the FDR. Self-reported vividness was similarly initially statistically significant but did not remain so after applying the Benjamini-Hochberg procedure. Unlike Total ID, the group differences for self-reported vividness were in the opposite direction of our expectation. See Table 3 for additional details.
Prospective prediction of SI
Bivariate models revealed that no measure of episodic future thinking nor non-episodic thinking prospectively predicted SI. This was the case predicting SI 1 month later (ORs = 0.37–1.36 [95% CIs = 0.04, 4.95], ps > .05) and 3 months later (ORs = 0.60–4.05 [95% CIs = 0.05, 22.84], ps > .05). Similarly, no measure of episodic memory prospectively predicted SI (ORs = 0.47–1.49 [95% CIs = 0.10, 22.81], ps > .05). Of note, ID-Time for both future and past events initially predicted SI 1 month later, but this was no longer significant after controlling the FDR. See Supplemental Table 3 for additional details. Multivariate models were not run in light of these nonsignificant findings.
Discussion
Study 2 investigated episodic future thinking and episodic memory in those with a recent history of suicidal ideation relative to other psychiatric diagnoses. There was some evidence of future thinking difficulties in the case of event fluency and self-reported event duration, such that suicidal veterans tended to generate fewer future events and imagine events that occurred over longer periods of time relative to nonsuicidal veterans. Self-reported duration of future events yielded particularly robust findings, with this deficit characterizing suicidal veterans even after controlling for age, gender, depressive symptoms, PTSD, and substance use. Notably, these indices are those most closely linked to prior literature on future thinking deficits in those with suicidal thoughts (i.e., future fluency and event specificity). In contrast, there was negligible difference between those in the SI and psychiatric control groups in event richness (i.e., IDs).
Counter to our expectations, we found no consistent pattern of evidence suggesting that suicidal and nonsuicidal veterans differ in episodic memory processes. There was a small difference between groups in event richness (i.e., Total ID) in the expected direction, but this finding did not remain significant after controlling the FDR. Further, the only other finding to reach statistical significance before applying FDR-controlling procedures—vividness of the recollection—is conceptually similar to event richness but the difference was in the opposite direction of what was predicted.
Finally, neither episodic future thinking nor episodic memory was strongly predictive of future SI. This result is similar to Study 1, but applies to a longer-term time frame since Study 2 tested prediction of SI occurring 1 month and 3 months later.
General Discussion
To our knowledge, this investigation is the most comprehensive examination of episodic future thinking and episodic memory deficits among suicidal individuals to date. Testing multiple features of these cognitive processes makes possible the potential cross-validation of findings as well as the detection of differential patterns to inform future assessment and treatment efforts. We draw the following conclusions pertaining to each cognitive process.
Future thinking deficits
The strongest evidence we found for an association between future thinking and suicidal ideation was for self-reported duration of events. Despite being instructed to imagine specific events lasting less than 1 day, individuals with SI tended to imagine events lasting greater than 1 day in both Study 1 and Study 2. In Study 1, there was a moderate difference between suicidal adults and healthy controls, though this finding was non-significant. In Study 2, there was a similarly moderate difference between suicidal veterans and nonsuicidal psychiatric controls. This finding remained significant after controlling for relevant demographic and clinical characteristics previously linked to future thinking (e.g., age, depression, PTSD; Addis et al., 2016; Addis et al., 2008; Brown et al., 2013; Hallford et al., 2018). This finding is consistent with past work identifying suicidal patients’ tendency to imagine less specific events relative to nonsuicidal patients (Williams et al., 1996) and points to an individual component of specificity that may be associated with suicidal thinking: temporal specificity. In contrast to this finding, there was no evidence that self-reported vividness, likelihood, similarity, and valence of future events differentiated the SI group from the control group in either study.
Other measures of future thinking revealed notable yet tentative patterns. In both studies, suicidal adults displayed moderately lower fluency of future events relative to nonsuicidal adults. In Study 1, this effect was small but not significant. In Study 2, this finding remained significant after controlling the FDR, but was no longer significant after adjusting for covariates. On the one hand, these event fluency trends show some alignment with the past SI literature, which includes event fluency as one of three components used to create a common, composite measure of episodic future thinking (Hunter & O’Connor, 2003; MacLeod et al., 1998; MacLeod et al., 2004, 2005). On the other hand, the effects in the present study for event fluency alone were modest and not related to SI above and beyond depressive symptoms.
Regarding measures from the cognitive literature, we found no evidence that individuals with suicidal thoughts differ from other psychiatric patients in event richness. The implications of our findings for those with suicidal thoughts relative to healthy controls are less straightforward. In Study 1, we observed a large difference between these groups, but that finding did not remain statistically significant after controlling the FDR. Notably, event richness in both the SI and psychiatric control groups from Study 2 was comparable to the SI group but lower than the healthy control group from Study 1. Diminishment in future event richness may therefore characterize psychiatric history broadly. Consistent with this possibility, future thinking deficits have been reported in other clinical groups, including individuals displaying depressive symptoms and PTSD (Addis et al., 2016; Addis et al., 2008; Brown et al., 2013; Gamble et al., 2019; Hallford et al., 2018). It remains important for future research to more thoroughly investigate whether those with suicidal thoughts are indeed similarly characterized by low event richness.
Of note, the notion that future thinking difficulties are not unique to suicidal thinking does not negate its potential clinical relevance in understanding suicide. Difficulty imagining details related to future events, for instance, may impact one’s ability to engage in psychotherapeutic skills that may in turn minimize suicide risk (e.g., safety planning, problem-solving, mental imagery, mental contrasting with implementation intentions; D’Zurilla & Nezu, 2010; Fritzsche et al., 2016; Holmes et al., 2016; Lang et al., 2012; Oettingen, 2012; Stanley & Brown, 2012). Indeed, future efforts to clarify the relationship of future event richness with respect to SI may look to brief experimental manipulations (i.e., episodic specificity induction; Madore & Schacter, 2014, 2016) that have been used by cognitive psychologists to temporarily improve future thinking and observe whether this reduces SI or addresses other clinically-relevant processes (i.e., improved problem-solving, reduced negative affect, and increased positive affect; Jing et al., 2016).
Memory deficits
Episodic memory deficits were not observed among those who have experienced SI. This pattern was consistent across Studies 1 and 2 and across all measure types. Further, effect size estimates across measures were modest, except for ID counts in Study 1 which ranged from small to large and revealed the expected pattern of fewer IDs among suicidal adults compared with nonsuicidal adults. Besides this exception, the overall pattern of findings remains surprising given prior evidence for overgeneralized memory in suicidal individuals (Richard-Devantoy et al., 2015; Williams & Broadbent, 1986; Williams et al., 1996). One potential reason for this may be participants’ fatigue, as measures of episodic memory always followed an already-extensive assessment battery of episodic future thinking.
Another possible reason for this unexpected finding lies in the suicide-related outcome assessed. Nearly all studies within the suicide literature detecting episodic memory deficits have focused on suicide attempt (Richard-Devantoy et al., 2015). These studies presumably included cases of SI, but those cases were also characterized by suicide attempt and thereby were more clinically severe. This characteristic does not appear to be driven solely by clinical severity of samples, as group differences between suicide attempters and non-attempters have been shown with comparison groups ranging from healthy controls to psychiatric patients (e.g., Arie et al., 2008; Kaviani et al., 2005). Indeed, the one prior study to our knowledge that has looked specifically at SI among adults found no significant group differences in ‘overgeneralized memory’ (Williams et al., 2005). Of note, this issue remains difficult to resolve in light of the more extensive depression literature, which presumably overlaps with SI, that has also detected episodic memory deficits (King et al., 2009; Söderlund et al., 2014). Future research is needed to clarify this association by directly comparing adults who have experienced SI only, adults who have attempted suicide, and depressed adults without history of suicidal ideation or attempt.
Finally, the stronger presence of future thinking deficits relative to memory deficits suggests that the former may be more implicated in the development of suicidal thinking. Indeed, future thinking deficits have been shown to account for memory deficits among depression-prone individuals (e.g., Addis et al., 2016). This may be explained by the fact that episodic future thinking is more cognitively demanding than episodic memory. Indeed, prior work has shown that the ability for episodic future thinking relies on the ability to flexibly recombine information from memory (Schacter & Addis, 2007, 2020).
Limitations
The present findings should be interpreted in light of several limitations. First, Study 1 featured a small sample size, and Study 2 featured low retention rates. This increases the possibility of Type II error, especially when applying prospective analyses to small samples. Second, we did not account for other non-episodic processes such as narrative style (i.e., the general manner in which people talk about their experiences in the present, past, or future), which may partially account for deficits in episodic future thinking and episodic memory (Gaesser et al., 2011). Although episodic future thinking and episodic memory have been found to be dissociable from narrative style (Madore et al., 2014; Schacter et al., 2017), future research is encouraged to test the dissociable effects within clinical populations with the use of a control task (e.g., Picture Description Task; Gaesser et al., 2011). Third, the potential confounding role of depression could not be ruled out entirely, as the SI group reported substantially more depressive symptoms compared with the nonsuicidal control group in both samples. Although Study 2 was able to address this to some extent through multivariate analyses, having a separate depressed nonsuicidal group would have more fully addressed this concern. Fourth, cross-sectional findings were based on past year history of suicidal ideation. Despite the fact that the SI group in both studies featured many adults who recently experienced suicidal ideation (i.e., past week), recency of suicidal ideation varied (i.e., up to 1 year ago) and the present conclusions cannot definitively be linked to current states of active suicidal ideation. The use of ambulatory assessments in future work (e.g., daily diary studies, ecological momentary assessments) may help address this limitation. Fifth, despite the wide variety of measures included in the present study, there remain some features of past and future thinking that were not accounted for. In addition to the earlier referenced Autobiographical Memory Task (Williams & Broadbent, 1986), we did not examine thematic content of imagined future events (i.e., whether event content pertains to oneself, others, or specific emotions; O’Connor et al., 2015). More specific thought content (e.g., themed, emotionally-valenced) has generally been shown to yield more robust prediction of suicidal thoughts and behaviors (Cha et al., 2019), and may warrant further exploration as it applies to imagining the future.
These limitations aside, the present study offers a unique lens with which we examine cognitive deficits among suicidal individuals. Findings shed light on the novel domain of episodic future thinking, contextualize it within episodic memory, and emphasize its unique subcomponents. Future work is encouraged to continue considering the multifaceted nature of these cognitive processes and their clinical implications.
Supplementary Material
Acknowledgements
The authors are grateful to Dr. Brendan Gaesser for his consultation regarding the administration and coding of the Autobiographical Interview. The authors also thank Julianne Chu, Britta Ekdahl, Brittany Iles, Julia Harris, Brittany Iles, Kathryn Linthicum, Samantha Reber, Eliza Ryan, Hiba Salem, Emily Shoov, Rachel Snow, and Linh Tranh-Phuong for their assistance with data collection, transcription, and coding of materials; as well as Kelly Wilson, Kerri-Anne Bell, Rachel Nam, and Angelique Simeone for their assistance with data analysis and manuscript preparation. Funding: This research was funded by the Military Suicide Research Consortium (MSRC), an effort supported by the Office of the Assistant Security of Defense for Health Affairs (Award W81XWH-10-2-0181; Christine B. Cha, Donald J. Robinaugh, Brian P. Marx, Terence M. Keane, Matthew K. Nock). Opinions, interpretations, conclusions, and recommendations are those of the authors and not necessarily endorsed by MSRC or the Department of Defense. Dr Robinaugh’s work on this paper was also supported by the Charles A. King Trust Postdoctoral Research Fellowship Program, Bank of America, N.A., Co-Trustees and the National Institute of Mental Health Career Development Award (K23MH113805). Dr. Cha’s work on this paper was also supported by the Talley Fund of Harvard University.
Footnotes
We acknowledge that SI itself could be considered a clinically significant cognitive state. Consistent with prior work (e.g., Rudd, 2006; Wenzel & Beck, 2008), we assume that SI can be distinguished from other maladaptive cognitive processes that may lead to SI and maintain it over time. Even the most phenomenologically similar cognitive risk factors (e.g., identification with death) are distinct from SI in that they do not involve a conscious desire or decision to kill oneself.
Appraisals of defeat or humiliation from which there is no sense of escape (O’Connor & Kirtley, 2018)
The most promising example of feature-specific effects within the SI literature pertains to emotional valence, such that suicidal individuals have been shown to display future thinking deficits when imagining positive (vs. negative) events (MacLeod et al., 1998; O’Connor et al., 2008; O’Connor et al., 2007). This literature draws from the use of composite scores. Although we do conduct valence-specific analyses, the primary scope of this paper is not to explore the moderating role of emotional valence, but instead to investigate main effects across multiple measures.
This sample size determination was made a priori and did not account for efforts to control the false discovery rate (FDR), which authors decided to apply post-hoc.
These reliability values capture all coders except one, whose reliability data could not be retrieved. All coders underwent the same process of training and feedback with an experienced coder.
Interpretations of odds ratios vary depending on prevalence rates (e.g., 1–10%), but display fairly discrete ranges capturing small (1.46–1.68), medium (2.50–3.48), and large (4.13–6.71) effect sizes regardless (Chen et al., 2010).
When comparing SI and control groups based on lifetime (vs. past year) SI history, the directionality of effects across IDs reversed, such that the SI group expressed better future thinking compared with nonsuicidal veterans (Supplemental Table 4). We report this here to maintain transparency of results but do not elaborate on these findings since ‘past year’ was the timeframe selected for assessment a priori. Moreover, the effect sizes for these comparisons were small, not statistically significant, and not observed for past event IDs.
References
- Addis DR, Hach S, & Tippett LJ (2016). Do strategic processes contribute to the specificity of future simulation in depression? British Journal of Clinical Psychology, 55(2), 167–186. 10.1111/bjc.12103 [DOI] [PubMed] [Google Scholar]
- Addis DR, Wong AT, & Schacter DL (2008). Age-related changes in the episodic simulation of future events. Psychological Science, 19(1), 33–41. 10.1111/j.1467-9280.2008.02043.x [DOI] [PubMed] [Google Scholar]
- Arie M, Apter A, Orbach I, Yefet Y, & Zalsman G (2008). Autobiographical memory, interpersonal problem-solving, and suicidal behavior in adolescent inpatients. Comprehensive Psychiatry, 49(1), 22–29. 10.1016/j.comppsych.2007.07.004 [DOI] [PubMed] [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B, 57(1), 289–300. Retrieved August 3, 2020, from www.jstor.org/stable/2346101 [Google Scholar]
- Brown AD, Root JC, Romano TA, Chang LJ, Bryant RA, & Hirst W (2013). Overgeneralized autobiographical memory and future thinking in combat veterans with posttraumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry, 44(1), 129–134. 10.1016/j.jbtep.2011.11.004 [DOI] [PubMed] [Google Scholar]
- Cha CB, O’Connor RC, Kirtley O, Cleare S, Wetherall K, Eschle S, Tezanos KM, & Nock MK (2018). Testing mood-activated psychological markers for suicidal ideation. Journal of Abnormal Psychology, 127(5), 448–457. 10.1037/abn0000358 [DOI] [PubMed] [Google Scholar]
- Cha CB, Wilson KM, Tezanos KM, DiVasto KA, & Tolchin GK (2019). Cognition and self-injurious thoughts and behaviors: A systematic review of longitudinal studies. Clinical Psychology Review, 69, 97–111. 10.1016/j.cpr.2018.07.002 [DOI] [PubMed] [Google Scholar]
- Chen H, Cohen P, & Chen S (2010). How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Communications in Statistics—Simulation and Computation, 39(4), 860–864. 10.1080/03610911003650383 [DOI] [Google Scholar]
- Cohen J (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- D’Zurilla TJ & Nezu AM (2010). Problem-solving therapy. In Dobson KS (Ed.) Handbook of cognitive-behavioral therapies (3rd ed., pp. 197–225). New York: The Guildford Press. [Google Scholar]
- Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, Musacchio KM, Jaroszewski AC, Chang BP, & Nock MK (2017). Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin, 143(2), 187–232. 10.1037/bul0000084 [DOI] [PubMed] [Google Scholar]
- Fritzsche A, Schlier B, Oettingen G, & Lincoln TM (2016). Mental contrasting with implementation intentions increases goal-attainment in individuals with mild to moderate depression. Cognitive Therapy and Research, 40(4), 557–564. 10.1007/s10608-015-9749-6 [DOI] [Google Scholar]
- Gaesser B, Sacchetti DC, Addis DR, & Schacter DL (2011). Characterizing age-related changes in remembering the past and imagining the future. Psychology and Aging, 26(1), 80–84. 10.1037/a0021054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaesser B, & Schacter DL (2014). Episodic simulation and episodic memory can increase intentions to help others. Proceedings of the National Academy of Sciences of the United States of America, 111(12), 4415–4420. 10.1073/pnas.1402461111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gamble B, Moreau D, Tippett LJ, & Addis DR (2019). Specificity of future thinking in depression: A meta-analysis. Perspectives on Psychological Science, 14(5), 816–834. https://doi-org.ezproxy.cul.columbia.edu/10.1177/1745691619851784 [DOI] [PubMed] [Google Scholar]
- Glenn CR, Kleiman EM, Coppersmith DDL, Santee AC, Esposito EC, Cha CB, Nock MK, & Auerbach RP (2017). Implicit identification with death predicts change in suicidal ideation during psychiatric treatment in adolescents. Journal of Child Psychology and Psychiatry, 58(12), 1319–1329. 10.1111/jcpp.12769 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallford DJ, Austin DW, Takano K, & Raes F (2018). Psychopathology and episodic future thinking: A systematic review and meta-analysis of specificity and episodic detail. Behaviour Research and Therapy, 102, 42–51. 10.1016/j.brat.2018.01.003 [DOI] [PubMed] [Google Scholar]
- Holmes EA, Blackwell SE, Heyes SB, Renner F, & Raes F (2016). Mental imagery in depression: Phenomenology, potential mechanisms, and treatment implications. Annual Review of Clinical Psychology, 12, 249–280. 10.1146/annurev-clinpsy-021815-092925 [DOI] [PubMed] [Google Scholar]
- Hunter EC, & O’Connor RC (2003). Hopelessness and future thinking in parasuicide: The role of perfectionism. British Journal of Clinical Psychology, 42(4), 355–365. 10.1348/014466503322528900 [DOI] [PubMed] [Google Scholar]
- Jing HG, Madore KP, & Schacter DL (2016). Worrying about the future: An episodic specificity induction impacts problem solving, reappraisal, and well-being. Journal of Experimental Psychology: General, 145(4), 402–418. 10.1037/xge0000142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaviani H, Rahimi-Darabad P, & Naghavi HR (2005). Autobiographical memory retrieval and problem-solving deficits of Iranian depressed patients attempting suicide. Journal of Psychopathology and Behavioral Assessment, 27(1), 39–44. 10.1007/s10862-005-3264-0 [DOI] [Google Scholar]
- King MJ, MacDougall AG, Ferris SM, Levine B, MacQueen GM, & McKinnon MC (2009). A review of factors that moderate autobiographical memory performance in patients with major depressive disorder. Journal of Clinical and Experimental Neuropsychology, 32, 1122–1144. 10.1080/13803391003781874 [DOI] [PubMed] [Google Scholar]
- Kosnes L, Whelan R, O’Donovan A, & McHugh LA (2013). Implicit measurement of positive and negative future thinking as a predictor of depressive symptoms and hopelessness. Consciousness and Cognition, 22(3), 898–912. 10.1016/j.concog.2013.06.001 [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, & Williams JBW (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lang TJ, Blackwell SE, Harmer CJ, Davison P, & Holmes EA (2012). Cognitive bias modification using mental imagery for depression: Developing a novel computerized intervention to change negative thinking styles. European Journal of Personality, 26(2), 145–157. 10.1002/per.855 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levine B, Svoboda E, Hay JF, Winocur G, & Moscovitch M (2002). Aging and autobiographical memory: Dissociating episodic from semantic retrieval. Psychology and Aging, 17(4), 677–689. 10.1037/0882-7974.17.4.677 [DOI] [PubMed] [Google Scholar]
- Little RJA (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. 10.1080/01621459.1988.10478722 [DOI] [Google Scholar]
- MacLeod AK, & Cropley ML (1995). Depressive future-thinking: The role of valence and specificity. Cognitive Therapy and Research, 19(1), 35–50. 10.1007/BF02229675 [DOI] [Google Scholar]
- MacLeod AK, Tata P, Evans K, Tyrer P, Schmidt U, Davidson K, Thornton S, & Catalan J (1998). Recovery of positive future thinking within a high-risk parasuicide group: Results form a pilot randomized controlled trial. British Journal of Clinical Psychology, 37(4), 371–379. 10.1111/j.2044-8260.1998.tb01394.x [DOI] [PubMed] [Google Scholar]
- MacLeod AK, Tata P, Tyrer P, Schmidt U, Davidson K, & Thompson S (2004). Personality disorder and future-directed thinking in parasuicide. Journal of Personality Disorders, 18(5), 459–466. 10.1521/pedi.18.5.459.51329 [DOI] [PubMed] [Google Scholar]
- MacLeod AK, Tata P, Tyrer P, Schmidt U, Davidson K, & Thompson S (2005). Hopelessness and positive and negative future thinking in parasuicide. British Journal of Clinical Psychology, 44(4), 495–504. 10.1348/014466505X35704 [DOI] [PubMed] [Google Scholar]
- Madore KP, Gaesser B, & Schacter DL (2014). Constructive episodic simulation: Dissociable effects of a specificity induction on remembering, imagining, and describing in young and older adults. Journal of Experimental Psychology: Learning, Memory, and Cognition, 40(3), 609–622. 10.1037/a0034885 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madore KP, & Schacter DL (2014). An episodic specificity induction enhances means-end problem solving in young and older adults. Psychology and Aging, 29(4), 913–924. 10.1037/a0038209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madore KP, & Schacter DL (2016). Remembering the past and imagining the future: Selective effects of an episodic specificity induction on detail generation. Quarterly Journal of Experimental Psychology, 69(2), 285–298. 10.1080/17470218.2014.999097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Millner AJ, Ursano RJ, Hwang I, King AJ, Naifeh JA, Sampson NA, Zaslavsky AM, Stein MB, Kessler RC, & Nock MK (2018). Lifetime suicidal behaviors and career characteristics among U.S. Army soldiers: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). Suicide and Life-Threatening Behavior, 48(2), 230–250. 10.1111/sltb.12363 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miloyan B, McFarlane K, & Vásquez-Echeverría A (2019). The adapted Autobiographical Interview: A systematic review and proposal for conduct and reporting. Behavioural Brain Research, 370, 111881. 10.1016/j.bbr.2019.03.050 [DOI] [PubMed] [Google Scholar]
- Miranda R, Valderrama J, Tsypes A, Gadol E, & Gallagher M (2013). Cognitive inflexibility and suicidal ideation: Mediating role of brooding and hopelessness. Psychiatry Research, 210(1), 174–181. 10.1016/j.psychres.2013.02.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, Beautrais A,…Williams D (2008). Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. British Journal of Psychiatry, 192(2), 98–105. 10.1192/bjp.bp.107.040113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK, Holmberg EB, Photos VI, & Michel BD (2007). Self-Injurious Thoughts and Behaviors Interview: Development, reliability, and validity in an adolescent sample. Psychological Assessment, 19(3), 309–317. 10.1037/1040-3590.19.3.309 [DOI] [PubMed] [Google Scholar]
- O’Connor RC (2011). The integrated motivational-volitional model of suicidal behavior. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 32(6), 295–298. 10.1027/0227-5910/a000120 [DOI] [PubMed] [Google Scholar]
- O’Connor RC, Fraser L, Whyte M, MacHale S, & Masterton G (2008). A comparison of specific positive future expectancies and global hopelessness as predictors of suicidal ideation in a prospective study of repeat self-harmers. Journal of Affective Disorders, 110(3), 207–214. 10.1016/j.jad.2008.01.008 [DOI] [PubMed] [Google Scholar]
- O’Connor RC, & Kirtley OJ (2018). The integrated motivational-volitional model of suicidal behavior. Philosophical Transactions of the Royal Society, 373, 20170268. 10.1098/rstb.2017.0268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Connor RC, Smyth R, & Williams JMG (2015). Intrapersonal positive future thinking predicts repeat suicide attempts in hospital-treated suicide attempters. Journal of Consulting and Clinical Psychology, 83(1), 169–176. 10.1037/a0037846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Connor RC, Whyte M, Fraser L, Masterton G, Miles J, & MacHale S (2007). Predicting short-term outcome in well-being following suicidal behavior: The conjoint effects of social perfectionism and positive future thinking. Behaviour Research and Therapy, 45(7), 1543–1555. 10.1016/j.brat.2006.11.006 [DOI] [PubMed] [Google Scholar]
- Oettingen G (2012). Future thought and behaviour change. European Review of Social Psychology, 23(1), 1–63. 10.1080/10463283.2011.643698 [DOI] [Google Scholar]
- Petterson K, Rydningen NN, Christensen TB, & Walby FA (2011). Autobiographical memory and suicide attempts in schizophrenia. Suicide and Life-Threatening Behavior, 40, 369–375. 10.1521/suli.2010.40.4.369 [DOI] [PubMed] [Google Scholar]
- Pollock LR, & Williams JMG (2001). Effective problem solving in suicide attempters depends on specific autobiographical recall. Suicide and Life-Threatening Behavior, 31(4), 386–396. 10.1521/suli.31.4.386.22041 [DOI] [PubMed] [Google Scholar]
- Reinherz HZ, Tanner JL, Berger SR, Beardslee WR, & Fitzmaurice GM (2006). Adolescent suicidal ideation as predictive of psychopathology, suicidal behavior, and compromised function at age 30. American Journal of Psychiatry, 163(7), 1226–1232. 10.1176/appi.ajp.163.7.1226 [DOI] [PubMed] [Google Scholar]
- Richard-Devantoy S, Berlim MT, & Jollant F (2014). A meta-analysis of neuropsychological markers of vulnerability to suicidal behavior in mood disorders. Psychological Medicine, 44(8), 1663–1673. 10.1017/S0033291713002304 [DOI] [PubMed] [Google Scholar]
- Richard-Devantoy S, Berlim MT, & Jollant F (2015). Suicidal behavior and memory: A systematic review and meta-analysis. The World Journal of Biological Psychiatry, 16(8), 544–566. 10.3109/15622975.2014.925584 [DOI] [PubMed] [Google Scholar]
- Rudd D (2006). Fluid Vulnerability Theory: A cognitive approach to understanding the process of acute and chronic suicide risk. In Ellis TE (Ed.), Cognition and suicide: Theory, research, and therapy (pp. 355–368). American Psychological Association. 10.1037/11377-016 [DOI] [Google Scholar]
- Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, Markowitz JC, Ninan PT, Kornstein S, Manber R, Thase ME, Kocsis JH, & Keller MB (2003). The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): A psychometric evaluation in patients with chronic major depression. Biological Psychiatry, 54(5), 573–583. 10.1016/s0006-3223(02)01866-8 [DOI] [PubMed] [Google Scholar]
- Schacter DL, & Addis DR (2007). The cognitive neuroscience of constructive memory: Remembering the past and imagining the future. Philosophical Transactions of the Royal Society B: Biological Sciences, 362(1481), 773–786. 10.1098/rstb.2007.2087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schacter DL, & Addis DR (2020). Memory and imagination: Perspectives on constructive episodic simulation. In Abraham A (Ed.), The Cambridge handbook of the imagination (pp. 111–131). Cambridge: Cambridge University Press. [Google Scholar]
- Schacter DL, Benoit RG, & Szpunar KK (2017). Episodic future thinking: Mechanisms and functions. Current Opinion in Behavioral Sciences, 17, 41–50. 10.1016/j.cobeha.2017.06.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sidley GL, Whitaker K, Calam RM, & Wells A (1997). The relationship between problem-solving and autobiographical memory in parasuicide patients. Behavioural and Cognitive Psychotherapy, 25(2), 195–202. 10.1017/S1352465800018397 [DOI] [Google Scholar]
- Söderlund H, Moscovitch M, Kumar N, Daskalakis ZJ, Flint A, Herrmann N, & Levine B (2014). Autobiographical episodic memory in major depressive disorder. Journal of Abnormal Psychology, 123(1), 51–60. 10.1037/a0035610 [DOI] [PubMed] [Google Scholar]
- Stanley B, & Brown GK (2012). Safety planning intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioral Practice, 19(2), 256–264. 10.1016/j.cbpra.2011.01.001 [DOI] [Google Scholar]
- Szpunar KK, Spreng RN, & Schacter DL (2014). A taxonomy of prospection: Introducing an organizational framework for future-oriented cognition. Proceedings of the National Academy of Sciences, 111(52), 18414–18421. 10.1073/pnas.1417144111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tulving E (1983). Elements of episodic memory. New York: Oxford University Press. [Google Scholar]
- Tulving E (2002). Episodic memory: From mind to brain. Annual Review of Psychology, 53(1), 1–25. 10.1146/annurev.psych.53.100901.135114 [DOI] [PubMed] [Google Scholar]
- Wenzel A, & Beck AT (2008). A cognitive model of suicidal behavior: Theory and treatment. Applied and Preventive Psychology, 12(4), 189–201. 10.1016/j.appsy.2008.05.001 [DOI] [Google Scholar]
- Williams JMG (2001). Suicide and attempted suicide: Understanding the cry of pain. London: Penguin. [Google Scholar]
- Williams JMG, Barnhofer T, Beck AT, & Crane C (2005). Problem solving deteriorates following mood challenge in formerly depressed patients with a history of suicidal ideation. Journal of Abnormal Psychology, 114(3), 421–431. 10.1037/0021-843X.114.3.421 [DOI] [PubMed] [Google Scholar]
- Williams JMG, Barnhofer T, Crane C, Hermans D, Raes F, Watkins E, & Dalgleish T (2007). Autobiographical memory specificity and emotional disorder. Psychological Bulletin, 133, 122–148. 10.1037/0033-2909.133.1.122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams JMG, & Broadbent K (1986). Autobiographical memory in suicide attempters. Journal of Abnormal Psychology, 95(2), 144–149. 10.1037/0021-843X.95.2.144 [DOI] [PubMed] [Google Scholar]
- Williams JMG, Duggan DS, Crane C, & Fennell MJV (2006). Mindfulness-based cognitive therapy for prevention of recurrence of suicidal behavior. Journal of Clinical Psychology, 62(2), 201–210. 10.1002/jclp.20223 [DOI] [PubMed] [Google Scholar]
- Williams JMG, Ellis NC, Tyers C, Healy H, Rose G, & MacLeod AK (1996). The specificity of autobiographical memory and imageability of the future. Memory and Cognition, 24(1), 116–125. 10.3758/BF03197278 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.