

Abstract
Background
The aim of this study is to evaluate and compare the safety and efficacy of endoscopic mucosal resection with a cap (EMR-c) with those of endoscopic submucosal dissection (ESD) for rectal neuroendocrine tumors (R-NETs) ≤ 15 mm in diameter, and to analyze the risk factors of incomplete resection.
Methods
A total of 122 patients who underwent EMR-c or ESD for R-NETs at the Fourth Hospital of Hebei Medical University between February 2007 and December 2020 were invovled in this study. The clinical outcomes of two groups were compared and evaluated.
Results
A total of 122 patients with 128 R-NETs underwent endoscopic resection (EMR-c, 80; ESD, 48). In terms of duration of operation, EMR-c was significantly shorter than ESD (p < 0.001). Univariate analysis and multivariate analysis suggested that tumor diameter ≥ 8 mm was an independent risk factor for incomplete resection in patients with R-NETs in this study.
Conclusions
Both EMR-c and ESD were safe and effective treatments for R-NETs ≤ 15 mm in diameter. In addition, tumor diameter ≥ 8 mm was an independent risk factor for incomplete resection.
Keywords: Rectal neuroendocrine tumor, Endoscopic mucosal resection with a cap, Endoscopic submucosal dissection, Incomplete resection
Introduction
With the widespread use of screening colonoscopy, the incidence of rectal neuroendocrine tumors (R-NETs) has increased recently [1]. R-NETs account for up to 27% of gastroenteropancreatic NETs and 17.7% of all NETs in the SEERdatabase [1]. And R-NETs are reportedly more in Asian populations [2]. R-NETs can be found incidentally without symptoms and have good prognosis, but metastases can occur in some cases even with relatively small tumors [3, 4]. The prognosis for advanced R-NETs is similar to adenocarcinoma [3]. Hence, early detection and treatment are particularly important.
Endoscopic resection is recommended for small, non-lymph node metastatic R-NETs that invade the mucosa or submucosa. There are many methods of endoscopic resection, and different methods of endoscopic resection may be selected according to the habits of the surgeon and the limitations of equipment. Many literatures have described endoscopic mucosal resection with a cap (EMR-c) and endoscopic submucosal dissection (ESD) are two options of endoscopic resection for R-NETs [5–10]. However, the optimal strategy is poorly understood. Therefore, we compared the safety and efficacy of the two methods of endoscopic resection for R-NETs, and to analyze the risk factors of incomplete resection.
Methods
Patients
We collected the case characteristics and follow-up data of 122 patients with R-NETs who underwent resection in the Endoscopy Department of the Fourth Hospital of Hebei Medical University from February 2007 to December 2020. Inclusion criteria: patients underwent EMR-c or ESD; tumor size ≤ 15 mm. Exclusion criteria: (1) CT/MRI suggested lymphatic metastasis or distant metastasis; (2) complicated with other malignant tumors. We compared the duration of operation, complications, pathological types and clinical prognosis between the EMR-c group and the ESD group. The study was reviewed and approved by the Ethics Committee of the Fourth Hospital of Hebei Medical University (ID: 2021KS002).
EMR-c procedure and ESD procedure
It has been reported in the literatures, endoscopic ultrasonography (EUS) is useful for evaluating preoperatively the size and invasion depth of rectal NETs [11–13]. Therefore, EUS (20 MHz, Olympus, Japan) was used to assess the size and depth of the lesion before surgery to select an appropriate surgical approach. All lesions in this study did not invade muscularis propria and the size was less than 15 mm. As EUS was not available before 2010, 18 patients with18 lesions did not undergo preoperative ultrasound endoscopy. EMR-c procedure and ESD procedure, therapeutic endoscope with water supply function (GIF-H260J, Olympus, Japan) and high-frequency electric therapy instrument (Alerbo, Germany) were adopted. All surgeries were performed by four professional endoscopists who had worked for more than 7 years.
For EMR-c (Fig. 1), a wide (14.9 mm-diameter), transparent cap (D-201-11802, Olympus, Japan) was fitted to the tip of endoscope. The capped endoscope was placed over the lesion, followed by suction to engulf the lesion inside the cap, and a snare was then used to remove the lesion.
Fig. 1.
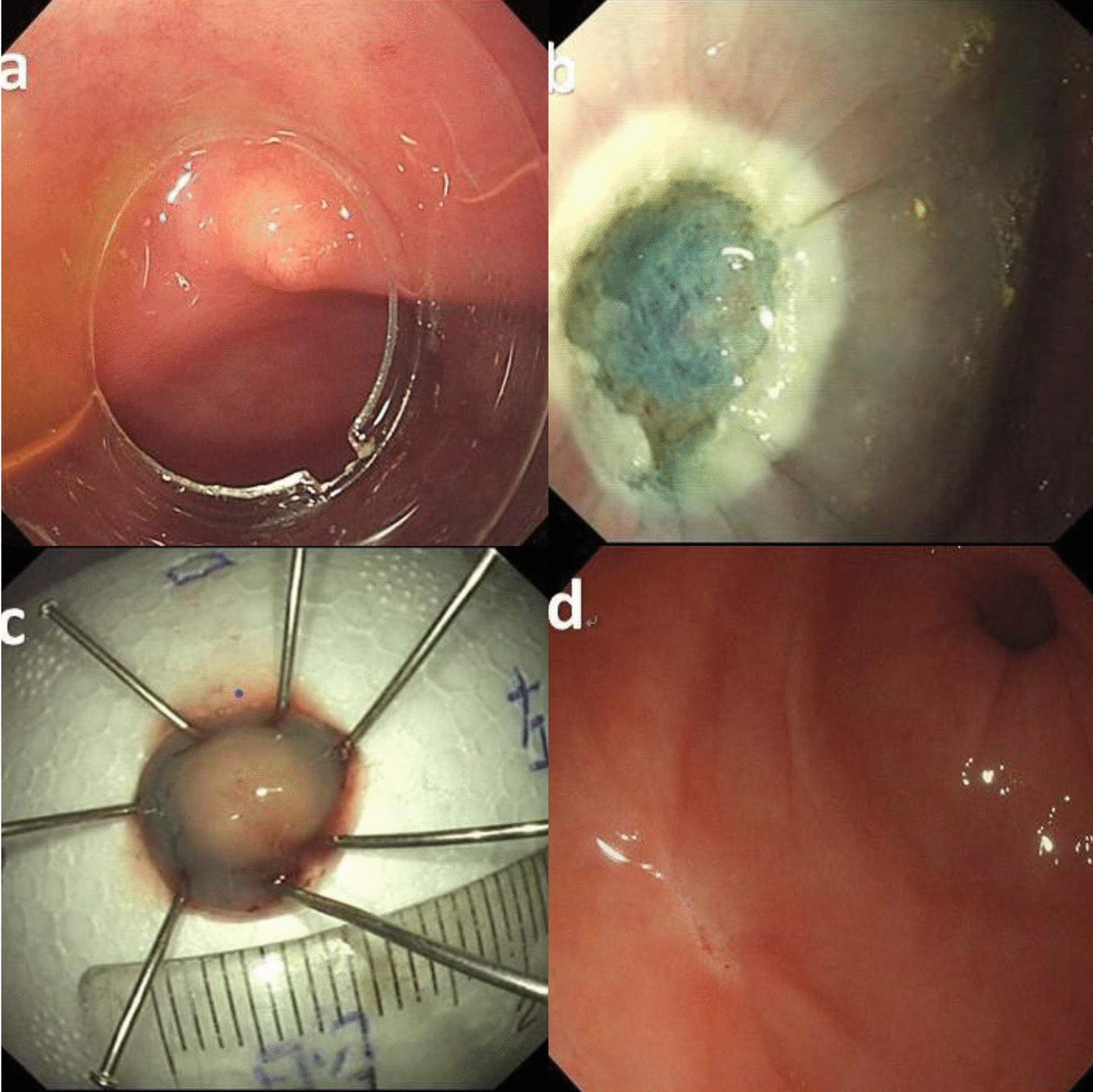
Endoscopic mucosal resection with a cap (EMR-c): a transparent cap is attached to the distal end of the scope; b a clear resection surface is observed; c the resection specimen is retrieved and measured; d scarring had formed after 6 months
For ESD (Fig. 2), a short transparent cap (D-201-11804, Olympus, Japan) was attached to the tip of endoscope. The lesion boundary was marked, the submucosal solution was injected, the circumferential mucosa of the lesion was incised using a dual knife (KD-650Q, Olympus, Japan), and the lesion was gradually exfoliated.
Fig. 2.
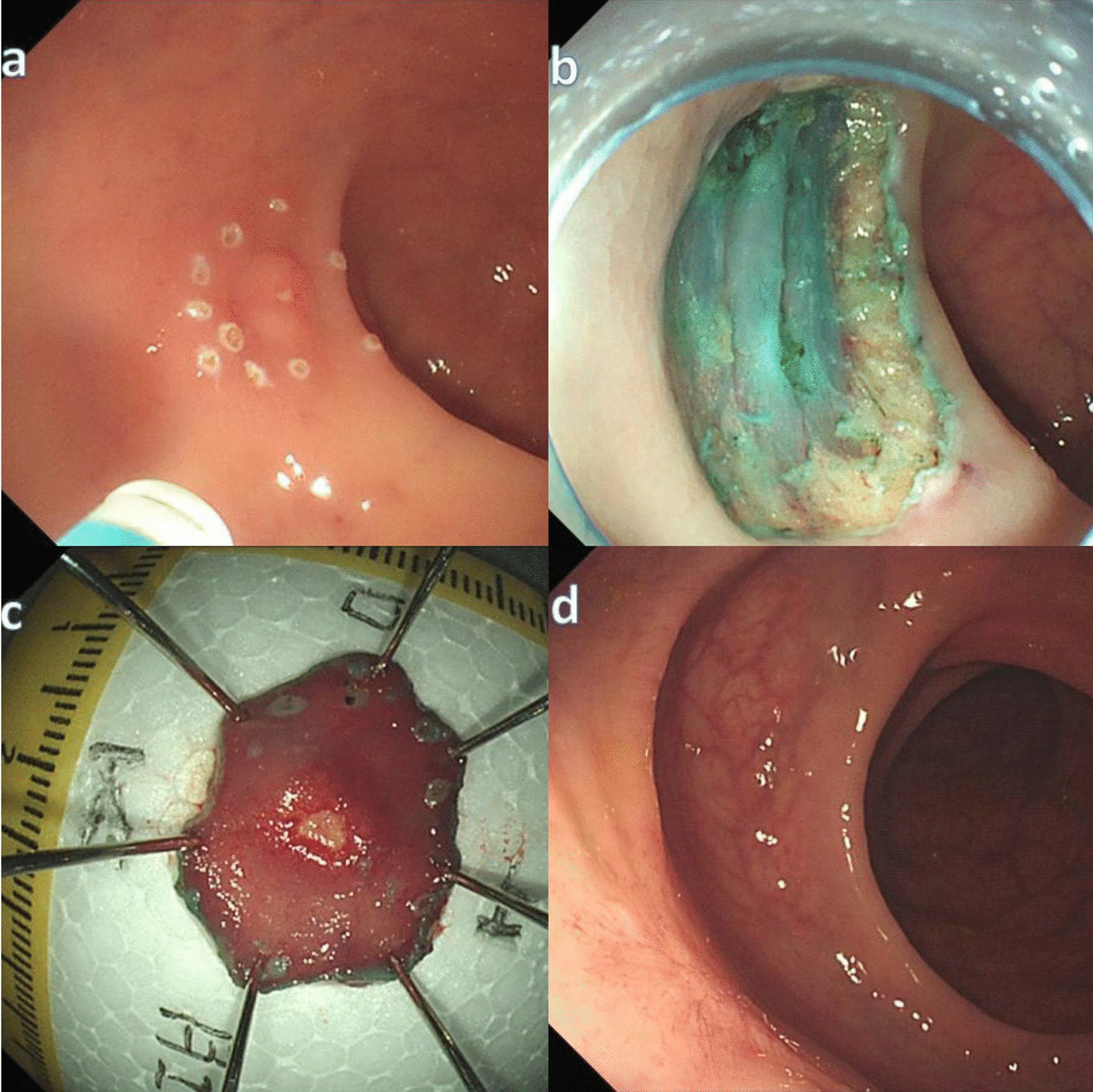
Endoscopic submucosal dissection (ESD): a labeled around the tumor; b a clear resection surface is observed; c the resection specimen is retrieved and measured; d scarring had formed after 6 months
Histological evaluation
Resected specimens were fixed to foam board with a ruler and then soaked in formalin solution. The histopathological evaluation included the histological type, lateral and vertical resection margins, and invasion layer, which was determined by hematoxylin & eosin and immunohistochemical staining in line with the 2019 World Health Organization classification of tumors of the digestive system. All sections were evaluated by experienced pathologists. En bloc resection was defined as the resection of the entire tumor in a single piece, as observed endoscopically. A pathologically complete resection (P-CR) was defined as an endoscopic resection with no lateral or vertical margins of the tumor. Incomplete resection was considered to have occurred when a resection failed to achieve tumor-free margins.
Complications
Postoperative bleeding and perforation are the two most common complications after endoscopic resection. Postoperative bleeding was determined when postoperative hematochezia occurs, requiring endoscopic hemostasis. Perforation was defined as a breakdown of the muscularis propria, postoperative abdominal pain, or the presence of gas in the abdominal cavity indicated by imaging examination.
Follow-up
Postoperative routine colonoscopy and CT were performed at 3 months, 6 months and 12 months to observe whether there was recurrence or metastasis. Colonoscopy and CT were recommended every 2 years thereafter. The deadline for our follow-up was September 2021.
Statistical analysis
Continuous variables are presented as the mean with standard deviation or the median with range and were evaluated by the t-test. Categorical data are expressed as numbers and percentages, and analysis was conducted through a chi-square test. Binary Logistic regression analysis was used for multivariate analysis for factors related to incomplete resection. Statistical analysis was performed using IBM SPSS Statistics v.25.0.0 (IBM Corp, New York), and p < 0.05 (two-tail) was considered statistically significant.
Results
In this study, we enrolled 122 patients with 128 lesions for analysis, including 76 patients receiving EMR-c and 46 patients receiving ESD for R-NETs resection. Preoperative evaluations were T1N0M0. Table 1 shows the patients’ baseline characteristics.
Table 1.
Baseline characteristics of patients and tumors
| EMR-c | ESD | p-value | |
|---|---|---|---|
| Patient characteristics | |||
| Patient number, n (%) | 76 | 46 | |
| Age, years | |||
| Mean ± SD | 52.39 ± 11.958 | 51.37 ± 10.186 | 0.629 |
| Gender, n (%) | |||
| Male | 47 (61.84) | 24 (52.17) | |
| Female | 29 (38.16) | 22 (47.83) | 0.345 |
| With single/multiple lesions, n (%) | |||
| Single | 72 (94.74) | 44 (95.65) | |
| Multiple | 4 (5.26) | 2 (4.35) | 1.000 |
| Lesion characteristics | |||
| Lesion number, n (%) | 80 | 48 | |
| Lesion size, mm | |||
| Mean ± SD | 6.988 ± 2.357 | 6.438 ± 1.988 | 0.179 |
| Lesion size group, n (%) | |||
| < 8 mm | 46 (57.50) | 29 (60.62) | |
| ≥ 8 mm | 34 (42.50) | 19 (39.58) | 0.853 |
| Location group, n (%) | |||
| Upper rectum | 4 (5.00) | 1 (2.08) | |
| Middle rectum | 50 (62.5) | 24 (50.00) | |
| Lower rectum | 26 (32.5) | 23 (47.82) | 0.223 |
| Histopathological grade, n (%) | |||
| G 1 | 62 (93.94) | 42 (89.36) | |
| G 2 | 4 (6.06) | 5 (10.64) | 0.486 |
EMR-c endoscopic mucosal resection with a cap, ESD endoscopic submucosal dissection
There were no statistically significant differences in age, gender, lesion size, lesion location and pathological grade between the EMR-c group and the ESD group. There were more males than females in the two groups (71/51). Among them, 58.59% of the lesions were smaller than 8 mm, 96.09% of the lesions were located in the middle and lower rectum, and the size of EMR-c group and ESD group were 6.988 ± 2.357 mm and 6.438 ± 1.988 mm, respectively. And 104 patients with 110 lesions were examined by EUS, and all lesions were located in the mucosal muscular layer and submucosal layer. Immunohistochemical examination of 113 lesions indicated that 104 lesions (92.04%) were G1.
Of the 128 lesions, 80 were excised by EMR-c and 48 by ESD (Table 2). In terms of duration of operation, EMR-c was significantly shorter than ESD (10.100 ± 2.096 min vs. 28.688 ± 4.172 min, p < 0.001). There was no significant difference in EMR-c and ESD between the two groups in terms of En bloc resection rate (97.5% vs. 100% respectively), P-CR rate (85% vs. 77.08%, respectively), and complication rate of 2.5% for both. Postoperative bleeding occurred in two lesions in EMR-c group, and titanium clips were used for hemostasis. Perforation occurred only in the ESD group, and only in 2 cases, and conservative treatment was effective after titanium clips were closed.
Table 2.
Clinical outcomes of EMR-c and ESD
| Factors | EMR-c | ESD | p-value |
|---|---|---|---|
| Number | 80 | 48 | |
| Duration of procedure, min | |||
| Mean ± SD | 10.100 ± 2.096 | 28.688 ± 4.172 | < 0.001 |
| En bloc resection, n (%) | 78 (97.50) | 48 (100.00) | 0.528 |
| P-CR rate, n (%) | 66 (84.62) | 37 (77.08) | 0.345 |
| Vertical positive | 10 | 11 | N/A |
| Lateral positive | 2 | 0 | |
| Complication | 2 (2.50) | 2 (4.17) | 0.276 |
| Postprocedural bleeding | 2 | 0 (0.00) | N/A |
| Perforation | 0 (0.00) | 2 | |
EMR-c endoscopic mucosal resection with a cap, ESD endoscopic submucosal dissection
Among them, 23 lesions were not completely resected, 2 lesions were positive for lateral resection margins, and 21 lesions were positive for vertical resection margins. Only one patient underwent additional surgery, and no residual tumor was found in surgical pathology.
During follow-up, 32 patients (32 lesions) were lost to follow-up. A total of 90 patients with 96 lesions were followed up in this study, including 52 patients in the EMR-c group and 38 patients in the ESD group. The median follow-up time was 36 months (range 9–120 months). There were no local recurrences or metastasis in any patients in either group during the follow-up period.
In the analysis of pathological features of the complete resection group and the incomplete resection group (Table 3), the difference in the lesion size between the two groups was statistically significant (p = 0.018). Multivariate analysis (Table 4) showed that tumor size ≥ 8 mm (OR: 3.419, 95% CI 1.295–9.026, p = 0.013) was independent risk factor for incomplete resection in patients with R-NETs in this study.
Table 3.
Clinicopathological features of complete and incomplete resection
| Factors | Complete resection (n = 105) | Incomplete resection (n = 23) | p-value |
|---|---|---|---|
| Lesion size group, n (%) | |||
| < 8 mm | 67 | 7 | |
| ≥ 8 mm | 38 | 16 | 0.018 |
| Location group, n (%) | |||
| Upper rectum | 4 | 1 | |
| Middle rectum | 59 | 15 | |
| Lower rectum | 42 | 7 | 0.592 |
| Histopathological grade, n (%) | |||
| G 1 | 83 | 21 | |
| G 2 | 7 | 2 | 1.000 |
| Operation, n (%) | |||
| EMR-c | 68 | 12 | |
| ESD | 37 | 11 | 0.342 |
EMR-c endoscopic mucosal resection with a cap, ESD endoscopic submucosal dissection
Table 4.
Multivariate analysis of risk factors for positive resection margin of R-NETs
| Factors | OR | 95% CI | p-value |
|---|---|---|---|
| Lesion size group, n (%) | |||
| < 8 mm | 1 | Reference | |
| ≥ 8 mm | 3.419 | 1.295–9.026 | 0.013 |
| Location group, n (%) | |||
| Upper rectum | 1 | Reference | |
| Middle rectum | 0.635 | 0.061–6.639 | 0.704 |
| Lower rectum | 0.410 | 0.036–4.700 | 0.474 |
| Operation, n (%) | |||
| EMR-c | 1 | Reference | |
| ESD | 2.010 | 0.759–5.323 | 0.160 |
OR odds ratio, 95% CI 95% confidence interval, EMR-c endoscopic mucosal resection with a cap, ESD endoscopic submucosal dissection
Discussion
R-NETs commonly appear as submucosal lesions with yellowish mucosa [14, 15]. There is still controversy on the treatment of R-NETs, and numerous treatment strategies have been reported [7, 16], including EMR, EMR-c, EMR-l, ESD, etc. In this study, we retrospectively analyzed the safety and effectiveness of EMR-c and ESD in R-NETs ≤ 15 mm, and predicted the risk factors of incomplete resection. The results showed that both EMR-c and ESD were safe and effective for R-NETs resection. The P-CR rate and complication rate were similar between the two groups, and the duration of operation was significantly shorter in EMR-c group than in ESD group. Furthermore, it was proposed that tumor larger than 8 mm was an independent risk factor for incomplete resection.
EMR-c has been widely used for small R-NETs due to its operability and short duration. However, its use has aroused great controversy in previous studies [6, 17–21]. The P-CR rate has been reported to range from 50 to 100%, probably because of the small sample size. In our study, 80 lesions were resected by EMR-c, and the P-CR rate was 85%, which was not significantly different from that (77.08%) in the ESD group. Wang [9] compared the therapeutic effect of EMR-c and ESD on R-NETs with a diameter less than 16 mm, and the P-CR rate of EMR-c group was 83.3%, which was consistent with our results. The higher P-CR rate of EMR-c may be due to the fact that CAP provides a sufficient vertical distance to excise the lesion. ESD is widely recommended because of its higher resection rate. Chen [22] conducted a retrospective study of 66 patients with R-NETs less than 15 mm in diameter, and the results showed that the P-CR rate was 96.43% for ESD. In this study, the duration of operation in the ESD group was relatively longer, with a P-CR rate of merely 77.08%. In addition, there were 2 cases of perforation, which might be attributed to two factors: the lesions that were located in the deep submucosal layer, and the different technical level of the operator. This indicates that ESD operation has a higher requirement for operators and a longer learning cycle. In order to prevent perforation, we can use titanium clip to seal the wound as an added precaution. This study showed that compared with ESD, EMR-c was simpler and the duration of operation was shorter, and this method is preferable for doctors in primary hospitals and less experienced/skilled doctors.
In this study, 23 lesions were not completely resected, among which 21 lesions were positive for vertical resection margins. We analyzed the relevant factors, which indicated that tumor size ≥ 8 mm was independent risk factor for incomplete resection. It suggests that lesions ≥ 8 mm may involve the submucosal depth, which require us to remove the lesions close to the muscular layer, or even remove part of the muscular layer. In previous studies, R-NETs could not be resected radically, and its influencing factors might include tumor size [23, 24], central depression [25], lesion morphology [26], pathological level [8], distance from anus [5], treatment methods [15], etc. However, incomplete resection does not necessarily indicate residual or recurrent tumors [6, 25]. In our study, only one of the 23 patients who did not receive complete resection was treated with additional surgery, and no tumor was found in the resected specimen, perhaps the electric cautery used in endoscopic resection could destroy the tumor margins [6]. The remaining 22 patients were followed up, and no recurrence or metastasis was reported to date.
In recent years, an underwater endoscopic mucosal resection (UEMR) has been used to remove small R-NETs [27, 28]. This method eliminates submucosal injection and may increase the buoyancy of submucosal tumors, which lift and float away from the muscularis propria [28]. In Sung Sil Park’s study [27], 36 patients were treated with UEMR and 79 with ESD. There was no difference in P-CR rate between the two groups, but the operative time of the UEMR group was significantly shorter than that of the ESD group. However, UEMR has its limitations [27]. Patients with inadequate intestinal preparation may not be able to identify lesions well. In future studies, we can try to evaluate the advantages and disadvantages of these methods comprehensively.
The study has several limitations. First, this study is a single-center retrospective study, which may cause selection bias. Second, the surgical procedure is not performed by the same physician, so differences between different people are inevitable. In our recent study [29], tumor size greater than 15 mm was considered to be an independent risk factor for lymph node metastasis in patients with colorectal neuroendocrine neoplasm, so 15 mm was used as the cut-off value to study the difference in endoscopic resection methods. We noticed that a recent report [30] suggested that tumor size greater than 11.5 mm was independent risk factor for lymph node metastases in patients with R-NETs. Maybe it's because of the different databases or the differences between the eastern and western populations. Therefore, a well-designed, multi-center, multi-site clinical study is needed to confirm these conclusions in the future.
Conclusions
Both EMR-c and ESD were safe and effective treatments for R-NETs ≤ 15 mm in diameter. The findings in this study suggested that tumor diameter ≥ 8 mm was an independent risk factor for incomplete resection in patients with R-NETs.
Acknowledgements
Informed consent was obtained from all participants in this study. We thank all the subjects of this study for their participation. Thanks to Ms. Liang Di for her help in statistical analysis of data.
Abbreviations
- R-NETs
Rectal neuroendocrine tumors
- EMR-c
Endoscopic mucosal resection with a cap
- ESD
Endoscopic submucosal dissection
- P-CR
Pathologically complete resection
- OR
Odds ratio
- 95% CI
95% Confidence interval
- UEMR
Underwater endoscopic mucosal resection
Author contributions
Study concept and design: XZ, MW, SL. Acquisition of data: XZ, LE. Analysis and interpretation of data: XZ, HS, KW, YC. Drafting of the manuscript: XZ. Critical revision of manuscript: XZ, MW, HS, LE, KW, YC, SL. All authors read and approved the final manuscript.
Funding
This project was supported by Bethune Charitable Foundation (BCF-NH-ZL-20201119-007). The funding had no role in study design, collection, analysis or interpretation of data, or manuscript preparation.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request without breaching participant confidentiality.
Declarations
Ethics approval and consent to participate
Our study was approved by the Ethics Committee of the Fourth Hospital of Hebei Medical University (ID: 2021KS002). All methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was obtained from all patients before performing any endoscopic procedures.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Folkert IW, Sinnamon AJ, Concors SJ, Bennett BJ, Fraker DL, Mahmoud NN, Metz DC, Stashek KM, Roses RE. Grade is a dominant risk factor for metastasis in patients with rectal neuroendocrine tumors. Ann Surg Oncol. 2020;27(3):855–863. doi: 10.1245/s10434-019-07848-0. [DOI] [PubMed] [Google Scholar]
- 2.Konishi T, Watanabe T, Muto T, Kotake K, Nagawa H, Japanese SFCO. Site distribution of gastrointestinal carcinoids differs between races. Gut. 2006;55(7):1051–1052. doi: 10.1136/gut.2006.093088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Konishi T, Watanabe T, Kishimoto J, Kotake K, Muto T, Nagawa H, On BOTJ, Japanese SFCO. Prognosis and risk factors of metastasis in colorectal carcinoids: results of a nationwide registry over 15 years. Gut. 2007;56(6):863–868. doi: 10.1136/gut.2006.109157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kang HS, Kwon MJ, Kim T, Han J, Ju Y. Lymphovascular invasion as a prognostic value in small rectal neuroendocrine tumor treated by local excision: a systematic review and meta-analysis. Pathol Res Pract. 2019;215(11):152642. doi: 10.1016/j.prp.2019.152642. [DOI] [PubMed] [Google Scholar]
- 5.Lee J. Comparison between cap-assisted and ligation-assisted endoscopic mucosal resection for rectal neuroendocrine tumors. Ann Gastroenterol. 2020;33(4):385–390. doi: 10.20524/aog.2020.0485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Park SB, Kim HW, Kang DH, Choi CW, Kim SJ, Nam HS. Advantage of endoscopic mucosal resection with a cap for rectal neuroendocrine tumors. World J Gastroenterol. 2015;21(31):9387–9393. doi: 10.3748/wjg.v21.i31.9387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ahmed Y, Othman M. EMR/ESD: techniques, complications, and evidence. Curr Gastroenterol Rep. 2020;22(8):1–12. doi: 10.1007/s11894-020-00777-z. [DOI] [PubMed] [Google Scholar]
- 8.Wang X, Chai N, Linghu E, Li H, Zhai Y, Feng X, Zhang W, Zou J, Li L, Xiang J. Efficacy and safety of hybrid endoscopic submucosal dissection compared with endoscopic submucosal dissection for rectal neuroendocrine tumors and risk factors associated with incomplete endoscopic resection. Ann Transl Med. 2020;8(6):368. doi: 10.21037/atm.2020.02.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang X, Xiang L, Li A, Han Z, Li Y, Wang Y, Guo Y, Zuang K, Yan Q, Zhong J, et al. Endoscopic submucosal dissection for the treatment of rectal carcinoid tumors 7–16 mm in diameter. Int J Colorectal Dis. 2015;30(3):375–380. doi: 10.1007/s00384-014-2117-2. [DOI] [PubMed] [Google Scholar]
- 10.Sivandzadeh GR, Ejtehadi F, Shoaee S, Aminlari L, Niknam R, Taghavi AR, Geramizadeh B, Hormati A, Safarpour AR, Bagheri Lankarani K. Endoscopic mucosal resection: still a reliable therapeutic option for gastrointestinal neuroendocrine tumors. BMC Gastroenterol. 2021;21(1):1–6. doi: 10.1186/s12876-021-01821-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gu Q, Lin Y, Cen L, Xu M, Li H, Lin X, Lu C. Endoscopic ultrasonography is useful in the diagnosis and treatment of rectal neuroendocrine neoplasms: a case series. J Zhejiang Univ Sci B. 2019;20(10):861–864. doi: 10.1631/jzus.B1900168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kobayashi K, Katsumata T, Yoshizawa S, Sada M, Igarashi M, Saigenji K, Otani Y. Indications of endoscopic polypectomy for rectal carcinoid tumors and clinical usefulness of endoscopic ultrasonography. Dis Colon Rectum. 2005;48(2):285–291. doi: 10.1007/s10350-004-0765-y. [DOI] [PubMed] [Google Scholar]
- 13.Hamada Y, Tanaka K, Hattori A, Umeda Y, Yukimoto H, Yamada R, Nakamura M, Miura H, Tsuboi J, Katsurahara M, et al. Clinical utility of endoscopic submucosal dissection using the pocket-creation method with a HookKnife and preoperative evaluation by endoscopic ultrasonography for the treatment of rectal neuroendocrine tumors. Surg Endosc. 2021;36(1):375–384. doi: 10.1007/s00464-021-08292-6. [DOI] [PubMed] [Google Scholar]
- 14.Jetmore AB, Ray JE, Gathright JJB, Mcmullen KM, Hicks TC, Timmcke AE. Rectal carcinoids: the most frequent carcinoid tumor. Dis Colon Rectum. 1992;35(8):717–725. doi: 10.1007/BF02050318. [DOI] [PubMed] [Google Scholar]
- 15.Modlin IM, Kidd M, Latich I, Zikusoka MN, Shapiro MD. Current status of gastrointestinal carcinoids. Gastroenterology. 2005;128(6):1717–1751. doi: 10.1053/j.gastro.2005.03.038. [DOI] [PubMed] [Google Scholar]
- 16.Park SJ. Tips and tricks for better endoscopic treatment of colorectal tumors: usefulness of cap and band in colorectal endoscopic mucosal resection. Clin Endosc. 2013;46(5):492–494. doi: 10.5946/ce.2013.46.5.492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Oshitani N, Hamasaki N, Sawa Y, Hara J, Nakamura S, Matsumoto T, Kitano A, Arakawa T. Endoscopic resection of small rectal carcinoid tumours using an aspiration method with a transparent overcap. J Int Med Res. 2000;28(5):241–246. doi: 10.1177/147323000002800507. [DOI] [PubMed] [Google Scholar]
- 18.Nagai T, Torishima R, Nakashima H, Ookawara H, Uchida A, Kai S, Sato R, Murakami K, Fujioka T. Saline-assisted endoscopic resection of rectal carcinoids: cap aspiration method versus simple snare resection. Endoscopy. 2004;36(3):202. doi: 10.1055/s-2004-814248. [DOI] [PubMed] [Google Scholar]
- 19.Yang DMP, Park YMP, Park SHM, Kim KMP, Ye BDMP, Byeon JMP, Myung SMP, Yang SMP. Cap-assisted EMR for rectal neuroendocrine tumors: comparisons with conventional EMR and endoscopic submucosal dissection (with videos) Gastrointest Endosc. 2016;83(5):1015–1022. doi: 10.1016/j.gie.2015.09.046. [DOI] [PubMed] [Google Scholar]
- 20.Son H, Son H, Sohn DK, Sohn DK, Hong CW, Hong CW, Han KS, Han KS, Kim BC, Kim BC, et al. Factors associated with complete local excision of small rectal carcinoid tumor. Int J Colorectal Dis. 2013;28(1):57–61. doi: 10.1007/s00384-012-1538-z. [DOI] [PubMed] [Google Scholar]
- 21.Imada-Shirakata Y, Sakai M, Kajiyama T, Kin G, Inoue K, Torii A, Kishimoto H, Ueda S, Okuma M. Endoscopic resection of rectal carcinoid tumors using aspiration lumpectomy. Endoscopy. 1997;29(1):34. doi: 10.1055/s-2007-1024058. [DOI] [PubMed] [Google Scholar]
- 22.Chen R, Liu X, Sun S, Wang S, Ge N, Wang G, Guo J. Comparison of endoscopic mucosal resection with circumferential incision and endoscopic submucosal dissection for rectal carcinoid tumor. Surg Laparosc Endosc Percutan Tech. 2016;26(3):e56–e61. doi: 10.1097/SLE.0000000000000266. [DOI] [PubMed] [Google Scholar]
- 23.Takita M, Sakai E, Nakao T, Kimoto Y, Ishii R, Konishi T, Ueno S, Kanda K, Negishi R, Muramoto T, et al. Clinical outcomes of patients with small rectal neuroendocrine tumors treated using endoscopic submucosal resection with a ligation device. Digestion. 2019;99(1):72–78. doi: 10.1159/000494416. [DOI] [PubMed] [Google Scholar]
- 24.Kim J, Kim JH, Lee JY, Chun J, Im JP, Kim JS. Clinical outcomes of endoscopic mucosal resection for rectal neuroendocrine tumor. BMC Gastroenterol. 2018;18(1):77. doi: 10.1186/s12876-018-0806-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Choi CW, Park SB, Kang DH, Kim HW, Kim SJ, Nam HS, Ryu DG. The clinical outcomes and risk factors associated with incomplete endoscopic resection of rectal carcinoid tumor. Surg Endosc. 2017;31(12):5006–5011. doi: 10.1007/s00464-017-5497-x. [DOI] [PubMed] [Google Scholar]
- 26.Wang X, Chai N, Linghu E, Qiu S, Li L, Zou J, Xiang J, Li X. The outcomes of modified endoscopic mucosal resection and endoscopic submucosal dissection for the treatment of rectal neuroendocrine tumors and the value of endoscopic morphology classification in endoscopic resection. BMC Gastroenterol. 2020;20(1):1–12. doi: 10.1186/s12876-019-1136-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Park SS, Han KS, Kim B, Chang Kim B, Hong CW, Sohn DK, Chang HJ. Comparison of underwater endoscopic mucosal resection and endoscopic submucosal dissection of rectal neuroendocrine tumors (with videos) Gastrointest Endosc. 2020;91(5):1164–1171. doi: 10.1016/j.gie.2019.12.039. [DOI] [PubMed] [Google Scholar]
- 28.Coutinho LMA, Lenz L, Kawaguti FS, Martins BC, Baba E, Gusmon C, Andrade G, Simas M, Safatle-Ribeiro A, Maluf-Filho F, et al. Underwater endoscopic mucosal resection for small rectal neuroendocrine tumors. Arq Gastroenterol. 2021;58(2):210–213. doi: 10.1590/s0004-2803.202100000-37. [DOI] [PubMed] [Google Scholar]
- 29.Zheng X, Wu M, Er L, Deng H, Wang G, Jin L, Li S. Risk factors for lymph node metastasis and prognosis in colorectal neuroendocrine tumours. Int J Colorectal Dis. 2022;37(2):421–428. doi: 10.1007/s00384-021-04082-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ricci AD, Pusceddu S, Panzuto F, Gelsomino F, Massironi S, De Angelis CG, Modica R, Ricco G, Torchio M, Rinzivillo M, et al. Assessment of the risk of nodal involvement in rectal neuroendocrine neoplasms: the NOVARA score, a multicentre retrospective study. J Clin Med. 2022;11(3):713. doi: 10.3390/jcm11030713. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request without breaching participant confidentiality.