

Abstract
Background
Acute myocardial infarctions are increasingly common among young adults. We investigated sex and racial differences in the evaluation of chest pain (CP) among young adults presenting to the emergency department.
Methods and Results
Emergency department visits for adults aged 18 to 55 years presenting with CP were identified in the National Hospital Ambulatory Medical Care Survey 2014 to 2018, which uses stratified sampling to produce national estimates. We evaluated associations between sex, race, and CP management before and after multivariable adjustment. We identified 4152 records representing 29 730 145 visits for CP among young adults. Women were less likely than men to be triaged as emergent (19.1% versus 23.3%, respectively, P<0.001), to undergo electrocardiography (74.2% versus 78.8%, respectively, P=0.024), or to be admitted to the hospital or observation unit (12.4% versus 17.9%, respectively, P<0.001), but ordering of cardiac biomarkers was similar. After multivariable adjustment, men were seen more quickly (hazard ratio [HR], 1.15 [95% CI, 1.05–1.26]) and were more likely to be admitted (adjusted odds ratio, 1.40 [95% CI, 1.08–1.81]; P=0.011). People of color waited longer for physician evaluation (HR, 0.82 [95% CI, 0.73–0.93]; P<0.001) than White adults after multivariable adjustment, but there were no racial differences in hospital admission, triage level, electrocardiography, or cardiac biomarker testing. Acute myocardial infarction was diagnosed in 1.4% of adults in the emergency department and 6.5% of admitted adults.
Conclusions
Women and people of color with CP waited longer to be seen by physicians, independent of clinical features. Women were independently less likely to be admitted when presenting with CP. These differences could impact downstream treatment and outcomes.
Keywords: chest pain, emergency department, myocardial infarction, race, sex, triage, young adult
Subject Categories: Cardiovascular Disease, Women, Health Services
Nonstandard Abbreviations and Acronyms
- NHAMCS
National Hospital Ambulatory Medical Care Survey
Clinical Perspective
What Is New?
In a large, nationally representative database of young people presenting to the emergency department with chest pain (aged ≤55 years), women and people of color waited longer to be evaluated by a physician, independent of other clinical features, compared with men and White adults, respectively.
Young women presenting to the emergency department with chest pain were less likely to be admitted to the hospital or to observation compared with young men.
Acute myocardial infarction was diagnosed in 1.4% of all young adults in the emergency department and 6.5% of admitted adults upon hospital discharge. There were too few observations to evaluate differences in acute myocardial infarction diagnosis by sex and race.
What Are the Clinical Implications?
Waiting longer to be evaluated for chest pain may reflect or contribute to downstream disparities seen in outcomes between young men and young women, as well as young adults of color versus young White adults.
Sex differences in admission rates should be evaluated further to elucidate whether this represents differences in ultimate diagnosis, which this study was underpowered to evaluate, or differences in decision making based on patient characteristics.
The number of acute myocardial infarctions (AMIs) occurring in young adults, particularly in young women (aged ≤55 years), is stagnating or even rising. 1 , 2 Young women with AMI present with greater comorbidity and have higher rates of in‐hospital mortality compared with young men. 3 Chest pain is the most common symptom of AMI in men and women, but in the VIRGO (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients) study, it was less likely to be recognized as related to heart disease among women. 4 On a population level, women have worse outcomes after AMI compared with men. 5 , 6 , 7 , 8 Women are less likely than men to undergo cardiac testing when presenting with chest pain, 9 , 10 , 11 and once diagnosed with AMI, are less likely to undergo revascularization 12 , 13 , 14 or to be prescribed guideline‐recommended medications. 8 , 13 Similar trends are seen by race. Black adults have poorer outcomes than White adults after AMI. 5 , 8 They are less likely to undergo electrocardiography or cardiac enzyme testing when presenting with chest pain, 9 , 15 , 16 and once diagnosed with AMI, they are less likely to undergo revascularization compared with White adults. 12
Using the National Institute of Minority Health and Health Disparities Research Framework, we sought to evaluate health care system factors that may influence the disparities in population health of young adults. 17 Our objective was to investigate sex and racial differences in the triage and management of nonspecific chest pain among young adults presenting to the emergency department (ED) in the United States.
Methods
Data Source
The Centers for Disease Control and Prevention’s National Hospital Ambulatory Medical Care Survey (NHAMCS)–Emergency Department from 2014 to 2018 was used for this analysis. 18 The NHAMCS is an annual, national probability sample of ambulatory visits made to nonfederal short‐stay hospitals in the United States. The NHAMCS–Emergency Department is a subset of the NHAMCS that only includes visits to EDs. The NHAMCS uses a 3‐stage probability design comprising (1) 112 geographically defined primary sampling units that are stratified by socioeconomic and demographic variables; (2) hospitals within primary sampling units; and (3) patient visits within all emergency service areas within sampled EDs. Therefore, the survey’s primary unit of analysis was ED visit.
From 2014 to 2015, NHAMCS used an automated mode of data collection. Beginning in 2016, all data were abstracted from medical records by Census Bureau field representatives for each sampled visit. Data are collected on patient demographics, reason for visit, vital signs, diagnoses, diagnostic tests, procedures, medications, and disposition. Medical coding of patients’ reason for visit and providers’ diagnoses was conducted by contracted medical coders. The unweighted survey response rate was 70.8% to 75.5% between 2014 and 2018. The NHAMCS is approved annually by the National Center for Health Statistics Ethics Review Board. Requirements for informed consent were waived. The data are publicly available at: https://www.cdc.gov/nchs/ahcd/datasets_documentation_related.htm#data.
Study Population
Patients aged 18 to 55 years presenting to the ED with chest pain between 2014 and 2018 were identified. Chest pain was defined using the Reason for Visit Classification for Ambulatory Care (National Center for Health Statistics–Centers for Disease Control and Prevention). Up to 5 reasons for the visit can be listed for each ED visit. Records were included for analysis if chest pain, chest pain and related symptoms, chest discomfort, pressure, tightness, burning sensation in the chest, or heart pain were any of the listed reasons for visit, which is a previously validated approach. 11 , 16 , 19 , 20 Race was defined as White or people of color, of which 89% were non‐Hispanic Black. Unfortunately, we could not analyze other racial or ethnic categories because of small numbers. Race was collected from the medical record. If >1 race was listed, the person was categorized as >1 race. When race was not available in the chart, it was imputed via a model‐based single, sequential regression method developed and validated by the NHAMCS.
Outcomes
The primary outcome was admission to the hospital or observation. Secondary outcomes included wait time, triage acuity, electrocardiography testing, cardiac biomarker testing, and administered medications. Triage level was defined by the NHAMCS on a 5‐level system, similar to the Agency for Healthcare Research and Quality’s Emergency Severity Index. Triage levels were defined by the recommended time frame for evaluation: immediate, emergent (1–14 minutes), urgent (15–60 minutes), semiurgent (1–2 hours), and nonurgent (>2 hours). Emergency rooms with a different numerical triage system (ie 3‐tier or 4‐tier system) were rescaled to a 5‐tier system using methodology determined by the Centers for Disease Control and Prevention in consultation with subject‐matter experts. An additional outcome was whether the patient was seen by a consulting physician in the ED; the survey does not provide information about the specialty of the consulting physician or consults outside of the ED. Medications were identified by therapeutic classification using the Cerner Multum’s Lexicon Plus Drug Database, consistent with previously published methods. 21 Therapeutic classification was defined by Cerner Multum’s 3‐level nested category system, in which each drug may have up to 3 therapeutic categories, with increasing specificity from level 1 to level 3. 22 The most specific category code and description for each medication category is listed in Table S1.
For each visit, up to 5 International Classification of Diseases, Ninth Revision (ICD‐9) or Tenth Revision (ICD‐10) codes were recorded during the ED encounter and, if admitted, on hospital discharge. Between 2014 and 2015, diagnostic codes were identified using ICD‐9, and from 2016 to 2018, codes were identified using ICD‐10. The Agency for Healthcare Research and Quality Clinical Classification software was used to estimate the frequency of diagnoses of interest by race and sex (Table S2). 22
Statistical Analysis
We compared patient and encounter characteristics by sex and by race within sex. Continuous variables were reported as mean with standard deviation and compared using the Wald test based upon the weighted survey design as recommended by Stata. 23 Categorical variables were reported as percentage with 95% CI adjusted for the survey sampling and compared using Pearson χ2 test. Missing data were either (1) reported as unknown for categorical variables or (2) excluded for calculation of means of continuous variables, and sample size was specified. Point estimates and corresponding χ2 P values were suppressed if they were based on <30 unweighted records, as specified by the NHAMCS, and are denoted by hyphens (‐) in the supplemental tables.
Multivariable logistic regression was used to estimate adjusted odds of the primary outcome, admission to hospital or observation unit, and specified secondary outcomes of interest (electrocardiography testing, cardiac enzyme testing, and immediate/emergent triage) for women versus men. We also conducted multivariable logistic regression to compare outcomes between people of color and White adults. Each model was adjusted for age; the model for sex comparison included race and vice versa. Variables selected for inclusion in the least absolute shrinkage and selection operator regression were selected a priori. Least absolute shrinkage and selection operator penalized regression analysis was then used to determine the inclusion of the select comorbid conditions and visit characteristics for each model. Variables considered in the least absolute shrinkage and selection operator analysis and ultimately included in the final regression model are listed in Table S3. We assessed for interaction between race and sex on outcomes in modeling. Cox regression was used to compare wait time by sex and race and was adjusted using the variables selected by least absolute shrinkage and selection operator analysis.
Survey data were analyzed using sampled visit weight, which are adjusted by the National Center for Health Statistics for nonresponse within time of year, geographic region, urban/rural, and hospital ownership. Sampling errors, as measured by linearized standard deviations and confidence intervals, were estimated using Stata version 15.1, which takes into account the clustered study design.
Results
Study Population
Between 2014 and 2018, we identified 101 372 ED visits, which represent an estimated 692 906 150 visits in the probability‐matched national population. Among these, 4152 ED visits were for adults aged 18 to 55 years with chest pain, which represent an estimated 29 730 145 visits. Women comprised 56.8% of the chest pain ED visits, and people of color comprised 34.9%.
The mean age of women was lower than that of men (37.6 years versus 38.8 years, respectively, P=0.016; Table 1). Asthma/chronic obstructive pulmonary disease (21.0% versus 15.3%, respectively, P<0.001), depression (16.5% versus 8.6%, respectively, P<0.001), and obesity (8.6% versus 6.3%, respectively, P=0.044) were more common in women, whereas hypertension (28.0% versus 33.2%, respectively, P=0.004) and substance abuse (7.3% versus 14.6%, respectively, P<0.001) were more common in men. Women had lower initial mean recorded blood pressure compared with men (136.7/81.8 mm Hg versus 140.2/85.1 mm Hg, respectively, P<0.001). There were no statistically significant differences between women and men in the likelihood of arrival by ambulance or of another ED visit in the prior 72 hours.
Table 1.
Characteristics of Young Patients Presenting to the Emergency Department With Chest Pain by Sex*
| Women | Men | P value | |
|---|---|---|---|
| Sample size | n=2319 | n=1833 | |
| National estimate | n=16 880 659 | n=12 849 486 | |
| Age, y, mean±SD | 37.6±10.6 | 38.8±10.7 | 0.016 |
| Person of color, % (95% CI) † | 37.3% (32.6%–42.3%) | 31.6% (28.1%–35.4%) | 0.026 |
| Expected source of payment, % (95% CI) | 0.014 | ||
| Private insurance | 37.3% (32.6%–42.3%) | 31.6% (28.1%–35.4%) | |
| Private insurance | 34.1% (31.4%–36.9%) | 34.2% (30.7%–38.0%) | |
| Medicare | 7.4% (6.1%–8.9%) | 8.8% (6.8%–11.2%) | |
| Medicaid or CHIP or state‐based program | 32.8% (29.3%–36.4%) | 25.9% (22.7%–29.3%) | |
| Self‐pay or no charge/charity, % (95% CI) | 11.6% (9.0%–14.7%) | 15.8% (13.3%–18.8%) | |
| Other | 3.2% (2.0%–4.9%) | 3.5% (2.5%–5.0%) | |
| Unknown | 11% (8.2%–14.7%) | 11.8% (8.4%–16.3%) | |
| Arrival by ambulance, % (95% CI) | 0.071 | ||
| Yes | 14.5% (12.2%–17.2%) | 18.4% (15.8%–21.3%) | |
| No | 82.5% (79.4%–85.2%) | 78.7% (75.7%–81.4%) | |
| Unknown | 3.0% (1.8%–5.0%) | 2.9% (1.9%–4.3%) | |
| Episode of care, % (95% CI) | 0.141 | ||
| Initial visit | 86.6% (82.3%–89.9%) | 89.0% (86.1%–91.4%) | |
| Follow‐up visit 72 hours | 3.1% (2.1%–4.7%) | 2.70% (1.9%–4.0%) | |
| Unknown | 10.3% (7.1%–14.8%) | 8.3% (6.0%–11.3%) | |
| Comorbidities, % (95% CI) | |||
| Asthma or COPD | 21.0% (18.7%–23.4%) | 15.3% (13.0%–17.9%) | <0.001 |
| Heart failure | 3.6% (2.6%–4.9%) | 4.5% (3.4%–6.0%) | 0.27 |
| Diabetes, type 1, type 2, unspecified, % (95% CI) | 11.9% (10.4%–13.7%) | 13.4% (11.7%–15.4%) | 0.227 |
| Hyperlipidemia | 9.0% (7.4%–10.8%) | 11.4% (9.3%–13.8%) | 0.055 |
| Hypertension | 28.0% (25.7%–30.4%) | 33.2% (30.2%–36.4%) | 0.004 |
| Obesity | 8.6% (6.9%–10.8%) | 6.3% (4.9%–8.2%) | 0.044 |
| Substance abuse | 7.3% (4.8%–8.0%) | 14.6% (9.3%–14.4%) | <0.001 |
| Depression | 16.5% (14.1%–19.2%) | 8.6% (7.1%–10.4%) | <0.001 |
| None of the listed comorbidities | 38.7% (35.8%–41.8%) | 37% (33.4%–40.7%) | 0.397 |
| Vitals before triage, mean±SD ‡ | |||
| Heart rate, beats per minute | 87.1±18.4 | 85.9±18.8 | 0.068 |
| Respiratory rate, breaths per minute | 18.6±5.5 | 18.2±3.4 | 0.023 |
| Systolic BP, mm Hg | 136.7±22.3 | 140.2±20.8 | <0.001 |
| Diastolic BP, mm Hg | 81.8±14 | 85.1±13.7 | <0.001 |
| Pulse oximetry | 98.0%±3.6% | 97.2%±4.4% | <0.001 |
BP indicates blood pressure; CHIP, Children’s Health Insurance Program; and COPD, chronic obstructive pulmonary disease.
Percentages are based on national estimates.
Eighty‐nine percent of the people‐of‐color patients reported race and ethnicity as non‐Hispanic Black.
Means calculated among those with values >0; estimated number of emergency department visits for which vital signs were available: heart rate (women: 16 037 871, men:12 178 818); respiratory rate (women: 16 050 610, men: 12 358 027); systolic BP (women: 16 357 118, men: 12 478 879); diastolic BP (women: 16 362 927, men:12 468 692); pulse oximetry (women: 16 059 599, men: 12 281 994).
Patient characteristics by race among sex are shown in Table S4 and S5. The mean age of women of color was lower than that of White women (36.6 years versus 38.2 years, respectively, P=0.003), but there was no significant age difference by race among men. Women of color were more likely to have history of hypertension (34.7% versus 24.0%, respectively, P<0.001) and obesity (11.0% versus 7.2%, respectively, P=0.014) than White women. Hyperlipidemia (7.0% versus 13.4%, respectively, P=0.002) and depression (4.9% versus 10.3%, respectively, P=0.003) were less common among men of color than White men. There was no statistically significant difference in initial mean recorded blood pressure between people of color and White adults presenting with chest pain. There were no significant differences by race in ambulance arrivals or recent prior ED visits.
Sex Differences in Evaluation and Treatment of Young Adults Presenting With Chest Pain
Women presenting to the ED with chest pain were less likely to be triaged as immediate/emergent compared with men (19.1% of chest pain encounters versus 23.3%, respectively, P=0.011), and waited longer to be seen by a provider (48.1 versus 37.2 minutes, respectively, P<0.001; Table 2). After multivariable adjustment, men were more likely to be seen than women at any given time (hazard ratio [HR] 1.15 [95% CI, 1.05–1.26], P=0.004). During the ED visit, electrocardiography testing (74.2% versus 78.8%, respectively, P=0.024) was less frequently ordered for women with chest pain than men, but D‐dimer testing (16.6% versus 11.9%, respectively, P=0.005) was more frequently ordered for women. After multivariable adjustment, there were no significant differences in electrocardiography (adjusted odds ratio [aOR], 1.08 [95% CI, 0.87–1.34]; P=0.493), cardiac enzyme testing (aOR, 1.03 [95% CI, 0.85–1.24]; P=0.790), or emergent triage (aOR, 1.23 [95% CI, 1.00–1.50]; P=0.050) by sex. Additionally, women were less likely to be seen by a consulting physician (8.5% versus 12.3%, respectively, P=0.001) while in the ED as compared with men. During the ED visit, women were less likely to be prescribed antiplatelet agents (17.1% versus 21.7%, respectively, P=0.004; Table 3) and antianginal medications (8.0% versus 11.2%, respectively, P=0.002) (Figure).
Table 2.
Triage and Assessment of Young Patients Presenting to the Emergency Department With Chest Pain by Sex*
|
Sample size National estimate |
Women n=2319 n=16 880 659 |
Men n=1833 n=12 849 486 |
P value |
|---|---|---|---|
| Triage level, % (95% CI) | <0.001 | ||
| Immediate/emergent | 19.1% (15.8%–22.8%) | 23.3% (19.3%–27.9%) | |
| Urgent | 38.0% (33.6%–42.8%) | 39.6% (34.9%–44.6%) | |
| Semiurgent/nonurgent | 12.8% (10.0%–16.3%) | 7.5% (5.5%–10.1%) | |
| No triage | 30.1% (23.4%–37.8%) | 29.5% (23.5%–36.3%) | |
| Diagnostic testing, % (95% CI) | |||
| BNP | 6.6% (5.2%–8.3%) | 8.7% (7.0%–10.8%) | 0.032 |
| Cardiac enzymes | 20.6% (16.8%–25.1%) | 22.9% (18.8%–27.5%) | 0.203 |
| D‐dimer | 16.6% (14.2%–19.4%) | 11.9% (9.8%–14.3%) | 0.005 |
| X‐ray | 71.4% (68.0%–74.6%) | 75.6% (72.8%–78.2%) | 0.041 |
| Electrocardiography | 74.2% (71.0%–77.2%) | 78.8% (76.1%–81.3%) | 0.024 |
| Cardiac monitor | 24.9% (21.7%–28.5%) | 30.0% (25.8%–34.5%) | 0.004 |
| CT chest | 8.9% (7.6%–10.5%) | 8.2% (6.8%–9.9%) | 0.447 |
| Toxicology screen | 3.9% (2.9%–5.2%) | 7.3% (5.9%–9.0%) | <0.001 |
| No testing | 24.6% (21.2%–29.0%) | 22.3% (18.9%–26.3%) | 0.058 |
| Seen by consulting physician | 8.5% (6.8%–10.5%) | 12.3% (9.8%–15.0%) | 0.001 |
| Wait time to see provider, min, mean±SD † | 48.1±82.1 | 37.2±61.8 | <0.001 |
BNP indicates B‐type natriuretic peptide; and CT, computed tomography.
Percentages based on national estimates.
Means calculated among those with values >0; estimated number of emergency department visits for wait times were available: women: 14 706 262; men: 11 181 998.
Table 3.
Medications Administered to Young Patients in ED Presenting With Chest Pain by Sex*
| Women, % (95% CI) | Men, % (95% CI) | P value | |
|---|---|---|---|
| Sample size | n=2319 | n=1833 | |
| National estimate | n=16 880 659 | n=12 849 486 | |
| Medications prescribed in ED or at discharge | 66.8% (63.7%–69.7%) | 69.3% (65.2%–73.0%) | 0.202 |
| Antiplatelets | 17.1% (14.4%–20.1%) | 21.7% (18.4%–25.6%) | 0.004 |
| Antianginal | 8.0% (6.3%–10.1%) | 11.2% (9.1%–13.7%) | 0.002 |
| Gastroenterological agents | 8.1% (6.7%–9.7%) | 9.1% (7.1%–11.6%) | 0.354 |
| Narcotic analgesics | 15.6% (13.1%–18.6%) | 15.2% (13.1%–17.5%) | 0.78 |
| Benzodiazepines | 9.1% (7.5%–11.0%) | 6.9% (5.3%–8.8%) | 0.052 |
| NSAIDs | 17.6% (15.6%–19.8%) | 16.6% (14.1%–19.5%) | 0.566 |
that anticoagulants could not be analyzed because of <30 unweighted records among women and men. ED indicates emergency department.
Percentages are based on national estimates.
Figure 1. Sex differences in evaluation and treatment of young adults presenting with chest pain in the National Hospital Ambulatory Medical Care Survey–Emergency Department, 2014 to 2018.
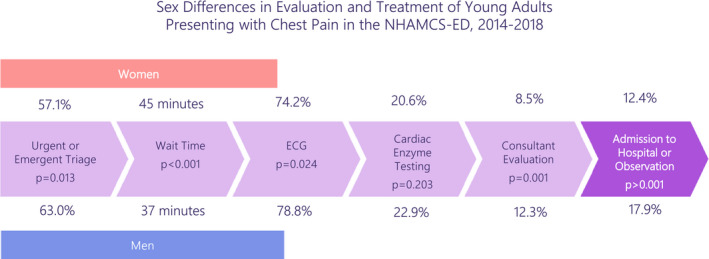
Unadjusted results are shown.
Chest pain encounters for young women were less likely to result in admission to the hospital or observation unit from the ED (12.4% versus 17.9% of encounters for men, P<0.001; Table 4). This association remained statistically significant after multivariable adjustment (aOR, 1.40 [95% CI, 1.08–1.81]; P=0.011).
Table 4.
Disposition of Young Patients Presenting to the Emergency Department With Chest Pain by Sex*
| Women, % (95% CI) | Men, % (95% CI) | P value | |
|---|---|---|---|
| Sample size | n=2319 | n=1833 | |
| National estimate | n=16 880 659 | n=12 849 486 | |
| No follow‐up | 5.6% (3.8%–8.1%) | 7.1% (5.2%–9.7%) | 0.223 |
| Return to care | 74.7% (70.9%–78.2%) | 66.7% (62.9%–70.3%) | <0.001 |
| Transfer to other hospital | 1.2% (0.7%–2.0%) | 2.3% (1.5%–3.4%) | 0.008 |
| Admit | 12.4% (10.1%, 15.1%) | 17.9% (15.3%–20.8%) | <0.001 |
| Admitted to observation | 3.9% (2.8%–5.5%) | 5.5% (3.9%–7.9%) | 0.026 |
| Admitted to hospital | 8.7% (6.7%–11.3%) | 13.4% (11.5%–15.7%) | <0.001 |
| Other disposition | 3.7% (1.5%–3.8%) | 5.5% (1.6%–4.0%) | 0.081 |
| Unknown | 1.2% (0.7%–1.8%) | 0.7% (0.3%–2.0%) | 0.35 |
| Left early | 3.5% (3.9%–8.1%) | 3.9% (4.6%–9.0%) | 0.694 |
Percentages are based on national estimates.
Racial Differences in the Evaluation and Treatment of Young Adults Presenting With Chest Pain
Women of color waited longer than White women for initial evaluation by a provider (57.8 versus 42.7 minutes, respectively, P=0.006). Men of color also waited longer than White men for initial evaluation by a provider (44.0 versus 34.0 minutes, respectively, P=0.006). On multivariable regression, people of color were less likely to be seen by a provider at any given time (HR, 0.82 [95% CI, 0.73–0.93]; P=0.001) compared with White adults. The P value for interaction between sex and race on wait time was 0.37.
There were no significant differences by race for either women or men in triage level, electrocardiography testing, or cardiac enzyme testing (Tables S6 and S7). There were no significant differences in the odds of electrocardiography testing (aOR, 0.81 [95% CI, 0.63–1.04]; P=0.095) or cardiac enzyme testing (aOR, 1.06 [95% CI, 0.78–1.44]; P=0.692), emergent triage (aOR, 0.80 [95% CI, 0.59–1.07]; P=0.133) for people of color versus White adults on multivariable analysis.
Women of color were less likely to be prescribed antiplatelet agents (10.6% of chest pain encounters versus 20.9%, respectively, P<0.001), narcotic analgesics (11.5% versus 18.1%, respectively, P=0.002), or benzodiazepines (10.8% versus 6.3%, respectively, P=0.019) compared with White women. Men of color were less likely to receive antianginal medications (5.8% versus 13.6%, respectively, P<0.001), narcotics (11.5% versus 16.9%, respectively, P=0.013) than White men, but were more likely to receive NSAIDs in the ED (20.8% versus 14.6%, respectively, P=0.038; Tables S8 and S9). There were no statistically significant racial differences in the proportion of encounters resulting in admission to the hospital or observation (Tables S10 and S11).
Sex and Racial Differences in Diagnoses of Young Adults Presenting With Chest Pain
Prespecified ED and discharge diagnoses of interest by race and sex are shown in Table S12. The most common of these diagnoses was the ED discharged diagnosis of other chest pain in 42.2% of ED visits. AMI was diagnosed in 1.4% of all adults in the ED. Women were less likely to be diagnosed with hypertensive diseases (10.1% versus 13.8%, respectively, P=0.011) or coronary atherosclerosis and other heart disease (1.9% versus 3.3%, respectively, P=0.044) in the ED. There were no observed differences by race.
Among those admitted, the most common of the prespecified hospital discharge diagnoses was other chest pain (57.3%, Table S13). AMI was diagnosed in 6.5% of admitted adults upon hospital discharge. There were too few observations to evaluate differences by race and sex in the diagnosis of AMI.
Discussion
In this national sample representing 29 million ED visits, we observed several differences related to sex and race in the evaluation and management of young adults aged 18 to 55 years presenting with chest pain. Young women with chest pain were less likely to be triaged as immediate/emergent, experienced longer wait times, and were less likely to undergo electrocardiography testing compared with young men. Young women were less likely to be admitted to the hospital or to observation compared with young men, and were prescribed medications used to treat acute coronary syndrome less frequently while in the ED. Sex differences in wait time and hospital admission persisted after multivariable adjustment. People of color waited longer for physician evaluation, but did not experience differences in triage, testing, consultant evaluation, or disposition. Diagnosis of AMI in the ED among young patients with chest pain was rare, occurring in 1.4% of visits, and the most common discharge diagnosis was other chest pain, reflecting the difficulty in making a specific diagnosis for chest pain complaints in young patients.
Obtaining an electrocardiography test within 10 minutes of arrival to the ED is a Class I recommendation for patients with chest pain, because electrocardiography testing can aid in the early diagnosis and treatment of AMI. 24 Delays in evaluation and electrocardiography testing can lead to delays in treatment, and increase the risk of morbidity and mortality. Although AMIs in young adults are rare, they are increasingly common, likely as a consequence of more prevalent multimorbidity. Moreover, a missed diagnosis of AMI means a missed opportunity at secondary prevention in a population of patients with a long lifespan and infrequent interaction with the medical system.
Sex Differences in ED Evaluation and Management of Chest Pain
Our study demonstrates differences between sexes in the evaluation of chest pain among young adults in the ED despite documentation of higher risk of mortality for women versus men with myocardial infarction in younger age groups. 1 These findings are particularly concerning given that cardiovascular mortality among young women has been stagnating, or even rising, in recent years. 1 , 25 , 26 , 27 , 28 However, ED visits for chest pain have increased in number between 2006 and 2016, whereas admissions for chest pain declined, and those admitted were increasingly older and men. 29 The reasons for these observed differences are likely multifactorial, including both true sex‐based clinical differences and underrecognition of heart disease in women.
Possible sex‐based clinical differences that could explain our study findings include the higher prevalence of AMI among young men versus young women, or more clinically severe presentations among men that led higher triage acuity, medication use, and rates of admission. The higher prevalence of traditional cardiovascular risk factors and disease in men may have informed testing, given that differences in electrocardiography testing were no longer significant after multivariable adjustment. 25
Although sex‐based clinical differences may have played a role in producing our study outcomes, we also know that historically, there has been an underrecognition of cardiovascular disease in women by physicians, and by women themselves. 30 , 31 , 32 Although studies have attributed sex differences in the evaluation of chest pain to atypical AMI symptoms among women, 33 , 34 these differences persist when controlling for symptom presentation, and the present analysis was restricted to patients with chest pain. 35 Limited studies show that AMI is more commonly missed among women, Black adults, and young adults, and a missed AMI is associated with higher mortality as compared with prompt myocardial infarction diagnosis. 36 , 37 Most young women with AMI experience chest pain, but women are more likely than men to present with myocardial infarction without chest pain, and there is a greater heterogeneity in associated symptoms among women. 34 , 38 This heterogeneity may introduce diagnostic uncertainty, translating into diagnostic delays or missed diagnoses, which is likely heightened among young adults, the age group at the lowest risk of AMI.
Racial Differences in ED Evaluation and Management of Chest Pain
We observed longer wait times for people of color as compared with White adults despite similar triage status, which persisted after multivariable adjustment. Prior studies in older adults with AMI have demonstrated longer wait times among Black adults compared with White adults. 39 This difference in wait time most likely reflects a disparity within the domain of the health care system at both the organizational and community level. For example, differences in wait time may be related to differences in medical decision by providers, given that standardized tools, such as the History EKG Age Risk‐Factors Troponin pathway, commonly underestimate the risk of people of color. 40 , 41 Additionally, there may be differences in the availability of resources among hospitals that serve a larger share of Black patients versus a large proportion of White patients, such as differences in availability of staff to assess patients in a timely manner. 42 , 43 We also found that women of color were less likely to receive AMI treatment with antiplatelet agents, and women of color were less likely to receive antianginals or narcotic pain medications in the ED. The finding that antiplatelet medications were prescribed less frequently during chest pain encounters by women of color is surprising, given that cardiovascular disease is common in women of color, and they have a higher risk of adverse outcomes. 44 These findings may reflect differences in overprescription of antiplatelets for noncardiovascular causes in White adults, as has been previously described, differences in final chest pain diagnosis (which we were underpowered to study), or undertreatment of ischemic heart disease in women of color. 45 Racial differences in the administration of narcotics in the ED have previously been reported, 46 , 47 although a recent study observed narcotic prescriptions are now equally common among White and Black adults, 48 which may be related to changing demographics of the opioid epidemic. Our findings may reflect differences in severity or quality of pain, false beliefs about biological race differences in the perception of pain, 49 or to historical differences in the opioid epidemic, which manifest as overprescription of narcotics to White adults.
Limitations
Data on testing or treatment performed by emergency medical services before hospital presentation or after hospital admission, such as electrocardiography or aspirin administration, were not available in this data set. Therefore, estimations of test use in the ED, such as electrocardiography, may underestimate the true prevalence of testing. The standardized NHAMCS survey form records only select comorbid conditions and diagnostic tests. Some cardiovascular risk factors particularly salient to young women, such as hypertensive diseases of pregnancy and autoimmune disorders, could not be analyzed. The survey also relies on documented medical history and therefore cannot ascertain comorbid conditions that have not been diagnosed, and comorbidity may be underestimated in adults who have less contact with the medical system or did not undergo testing in the ED. We did not have information on oral contraceptive use. We only analyzed visits associated with chest pain, but some patients with AMI present with symptoms other than chest pain. The number of diagnosed AMIs was small, and therefore it was not possible to assess sex or racial differences in triage, test use, or wait time within encounters ultimately resulting in diagnosis of AMI. Because of the low number of encounters in the NHAMCS among young patients with race other than White or Black, and the Centers for Disease Control and Prevention’s guidance not to analyze subgroups below a specified size in the NHAMCS, we were not able to analyze racial differences in detail or to analyze ethnicity. The NHAMCS does not link encounters over time by the same patient, so we cannot assess revisits after the chest pain ED visit, but there was no difference in the proportion of ED visits that were categorized as revisits within 72 hours across sex or racial groups. Given limitations in the data, we were unable to assess severity of illness upon presentation and were unable to include this in our multivariable model.
Conclusions
In this analysis of a large, nationally representative database, young women (aged <55 years) presenting to the ED with chest pain waited longer to be evaluated by a physician, and were less likely to be triaged as emergent, to undergo electrocardiography testing, be seen by a specialist, be given medications for AMI, or be admitted to the hospital or to observation than young men. Sex differences in wait time and hospital admission persisted after multivariable adjustment. Young adults of color experienced longer wait times despite similar triage status compared with White adults after multivariable adjustment. Differences by sex and race in the early evaluation and management of chest pain warrant further study to evaluate their association with clinical outcomes and to identify opportunities for improvement in clinical care.
Sources of Funding
The Centers for Disease Control and Prevention funds the NHAMCS‐Emergency Department registry.
Disclosures
Dr Reynolds received in‐kind donations to support unrelated studies from Abbott Vascular, Siemens, and BioTelemetry. The remaining authors have no disclosures to report.
Supporting information
Tables S1–S13
Supplemental Material for this article is available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.121.024199
For Sources of Funding and Disclosures, see page 9.
References
- 1. Gupta A, Wang Y, Spertus JA, Geda M, Lorenze N, Nkonde‐Price C, D'Onofrio G, Lichtman JH, Krumholz HM. Trends in acute myocardial infarction in young patients and differences by sex and race, 2001 to 2010. J Am Coll Cardiol. 2014;64:337–345. doi: 10.1016/j.jacc.2014.04.054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Arora S, Stouffer GA, Kucharska‐Newton AM, Qamar A, Vaduganathan M, Pandey A, Porterfield D, Blankstein R, Rosamond WD, Bhatt DL, et al. Twenty year trends and sex differences in young adults hospitalized with acute myocardial infarction. Circulation. 2019;139:1047–1056. doi: 10.1161/CIRCULATIONAHA.118.037137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bucholz EM, Strait KM, Dreyer RP, Lindau ST, D’Onofrio G, Geda M, Spatz ES, Beltrame JF, Lichtman JH, Lorenze NP, et al. Editor's choice‐sex differences in young patients with acute myocardial infarction: a VIRGO study analysis. Eur Heart J Acute Cardiovasc Care. 2017;6:610–622. doi: 10.1177/2048872616661847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lichtman JH, Leifheit EC, Safdar B, Bao H, Krumholz HM, Lorenze NP, Daneshvar M, Spertus JA, D'Onofrio G. Sex differences in the presentation and perception of symptoms among young patients with myocardial infarction: evidence from the VIRGO study (variation in recovery: role of gender on outcomes of young AMI patients). Circulation. 2018;137:781–790. doi: 10.1161/CIRCULATIONAHA.117.031650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Jneid H, Fonarow GC, Cannon CP, Hernandez AF, Palacios IF, Maree AO, Wells Q, Bozkurt B, LaBresh KA, Liang LI, et al. Sex differences in medical care and early death after acute myocardial infarction. Circulation. 2008;118:2803–2810. doi: 10.1161/CIRCULATIONAHA.108.789800 [DOI] [PubMed] [Google Scholar]
- 6. Vallabhajosyula S, Ya’Qoub L, Singh M, Bell MR, Gulati R, Cheungpasitporn W, Sundaragiri PR, Miller VM, Jaffe AS, Gersh BJ, et al. Sex disparities in the management and outcomes of cardiogenic shock complicating acute myocardial infarction in the young. Circ Heart Fail. 2020;13:e007154. doi: 10.1161/CIRCHEARTFAILURE.120.007154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Asleh R, Manemann SM, Weston SA, Bielinski SJ, Chamberlain AM, Jiang R, Gerber Y, Roger VL. Sex differences in outcomes after myocardial infarction in the community. Am J Med. 2021;134:114–121. doi: 10.1016/j.amjmed.2020.05.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Mehta LS, Beckie TM, DeVon HA, Grines CL, Krumholz HM, Johnson MN, Lindley KJ, Vaccarino V, Wang TY, Watson KE, et al. Acute myocardial infarction in women: a scientific statement from the American Heart Association. Circulation. 2016;133:916–947. doi: 10.1161/CIR.0000000000000351 [DOI] [PubMed] [Google Scholar]
- 9. Arnold AL, Milner KA, Vaccarino V. Sex and race differences in electrocardiogram use (the National Hospital Ambulatory Medical Care Survey). Am J Cardiol. 2001;88:1037–1040. doi: 10.1016/S0002-9149(01)01987-7 [DOI] [PubMed] [Google Scholar]
- 10. Mnatzaganian G, Hiller JE, Braitberg G, Kingsley M, Putland M, Bish M, Tori K, Huxley R. Sex disparities in the assessment and outcomes of chest pain presentations in emergency departments. Heart. 2020;106:111–118. doi: 10.1136/heartjnl-2019-315667 [DOI] [PubMed] [Google Scholar]
- 11. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997–2006. Acad Emerg Med. 2010;17:801–808. doi: 10.1111/j.1553-2712.2010.00823.x [DOI] [PubMed] [Google Scholar]
- 12. Vaccarino V, Rathore SS, Wenger NK, Frederick PD, Abramson JL, Barron HV, Manhapra A, Mallik S, Krumholz HM. Sex and racial differences in the management of acute myocardial infarction, 1994 through 2002. New Engl J Med. 2005;353:671–682. doi: 10.1056/NEJMsa032214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Humphries KH, Lee MK, Izadnegahdar M, Gao M, Holmes DT, Scheuermeyer FX, Mackay M, Mattman A, Grafstein E. Sex differences in diagnoses, treatment, and outcomes for emergency department patients with chest pain and elevated cardiac troponin. Acad Emerg Med. 2018;25:413–424. doi: 10.1111/acem.13371 [DOI] [PubMed] [Google Scholar]
- 14. Kaul P, Chang WC, Westerhout CM, Graham MM, Armstrong PW. Differences in admission rates and outcomes between men and women presenting to emergency departments with coronary syndromes. CMAJ. 2007;177:1193–1199. doi: 10.1503/cmaj.060711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997–2006. Acad Emerg Med. 2010;17:801–808. doi: 10.1111/j.1553-2712.2010.00823.x [DOI] [PubMed] [Google Scholar]
- 16. Mukhopadhyay A, D'Angelo R, Senser E, Whelan K, Wee CC, Mukamal KJ. Racial and insurance disparities among patients presenting with chest pain in the US: 2009–2015. Am J Emerg Med. 2020;38:1373–1376. doi: 10.1016/j.ajem.2019.11.018 [DOI] [PubMed] [Google Scholar]
- 17. Alvidrez J, Castille D, Laude‐Sharp M, Rosario A, Tabor D. The national institute on minority health and health disparities research framework. Am J Public Health. 2019;109:S16–S20. doi: 10.2105/AJPH.2018.304883 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. National Ambulatory Medical Care Survey (NAMCS) . 2021;2021:National Ambulatory Medical Care Survey (NAMCS).
- 19. Pezzin LE, Keyl PM, Green GB. Disparities in the emergency department evaluation of chest pain patients. Acad Emerg Med. 2007;14:149–156. doi: 10.1197/j.aem.2006.08.020 [DOI] [PubMed] [Google Scholar]
- 20. Makam AN, Nguyen OK. Use of cardiac biomarker testing in the emergency department. JAMA Intern Med. 2015;175:67–75. doi: 10.1001/jamainternmed.2014.5830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Center for Disease Control and Prevention . Cerner Multum Drug Database. 2021.
- 22. Agency for Healthcare Research and Quality . HCUP Clinical Classification Software. 2021.
- 23. UCLA Statistical Consulting Group . How Can I do a T‐Test with Survey Data? 2020;2020. [Google Scholar]
- 24. Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, et al. 2014 AHA/ACC guideline for the management of patients with non‐ST‐elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014;64:e139–e228. doi: 10.1016/j.jacc.2014.09.017. Epub 2014 Sep 23. Erratum in: J Am Coll Cardiol. 2014;64:2713‐4. Dosage error in article text. [DOI] [PubMed] [Google Scholar]
- 25. Mosca L, Barrett‐Connor E, Kass Wenger N. Sex/gender differences in cardiovascular disease prevention: what a difference a decade makes. Circulation. 2011;124:2145–2154. doi: 10.1161/CIRCULATIONAHA.110.968792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Ford ES, Capewell S. Coronary heart disease mortality among young adults in the U.S. from 1980 through 2002. J Am Coll Cardiol. 2007;50:2128–2132. doi: 10.1016/j.jacc.2007.05.056 [DOI] [PubMed] [Google Scholar]
- 27. Khan SU, Yedlapati SH, Lone AN, Khan MS, Wenger NK, Watson KE, Gulati M, Hays AG, Michos ED. A comparative analysis of premature heart disease‐ and cancer‐related mortality in women in the USA, 1999‐2018. Eur Heart J Qual Care Clin Outcomes. 2021;1999–2018. doi: 10.1093/ehjqcco/qcaa099 [DOI] [PubMed] [Google Scholar]
- 28. Champney KP, Frederick PD, Bueno H, Parashar S, Foody J, Merz CN, Canto JG, Lichtman JH, Vaccarino V. The joint contribution of sex, age and type of myocardial infarction on hospital mortality following acute myocardial infarction. Heart. 2009;95:895–899. doi: 10.1136/hrt.2008.155804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Aalam AA, Alsabban A, Pines JM. National trends in chest pain visits in US emergency departments (2006–2016). Emerg Med J. 2020;37:696–699. doi: 10.1136/emermed-2020-210306 [DOI] [PubMed] [Google Scholar]
- 30. Bairey Merz CN, Andersen H, Sprague E, Burns A, Keida M, Walsh MN, Greenberger P, Campbell S, Pollin I, McCullough C, et al. Knowledge, attitudes, and beliefs regarding cardiovascular disease in women: the women's heart alliance. J Am Coll Cardiol. 2017;70:123–132. doi: 10.1016/j.jacc.2017.05.024 [DOI] [PubMed] [Google Scholar]
- 31. Musey PI Jr, Kline JA. Do gender and race make a difference in acute coronary syndrome pretest probabilities in the emergency department? Acad Emerg Med. 2017;24:142–151. [DOI] [PubMed] [Google Scholar]
- 32. Cushman M, Shay CM, Howard VJ, Jiménez MC, Lewey J, McSweeney JC, Newby LK, Poudel R, Reynolds HR, Rexrode KM, et al. Ten‐year differences in women's awareness related to coronary heart disease: results of the 2019 American Heart Association National Survey: a special report from the American Heart Association. Circulation. 2021;143:e239–e248. doi: 10.1161/CIR.0000000000000907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Canto JG, Rogers WJ, Goldberg RJ, Peterson ED, Wenger NK, Vaccarino V, Kiefe CI, Frederick PD, Sopko G, Zheng Z‐J, et al. Association of age and sex with myocardial infarction symptom presentation and in‐hospital mortality. JAMA. 2012;307:813–822. doi: 10.1001/jama.2012.199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Brush JE Jr, Krumholz HM, Greene EJ, Dreyer RP. Sex differences in symptom phenotypes among patients with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2020;13:e005948. doi: 10.1161/CIRCOUTCOMES.119.005948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Humphries KH, Gao M, Lee MK, Izadnegahdar M, Holmes DT, Scheuermeyer FX, Mackay M, Mattman A, Grafstein E. Sex differences in cardiac troponin testing in patients presenting to the emergency department with chest pain. J Womens Health (Larchmt). 2018;27:1327–1334. doi: 10.1089/jwh.2017.6812 [DOI] [PubMed] [Google Scholar]
- 36. Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, Griffith JL, Selker HP. Missed diagnoses of acute cardiac ischemia in the emergency department. New Engl J Med. 2000;342:1163–1170. doi: 10.1056/NEJM200004203421603 [DOI] [PubMed] [Google Scholar]
- 37. Moy E, Barrett M, Coffey R, Hines AL, Newman‐Toker DE. Missed diagnoses of acute myocardial infarction in the emergency department: variation by patient and facility characteristics. Diagnosis. 2015;2:29–40. doi: 10.1515/dx-2014-0053 [DOI] [PubMed] [Google Scholar]
- 38. Canto JG, Canto EA, Goldberg RJ. Time to standardize and broaden the criteria of acute coronary syndrome symptom presentations in women. Can J Cardiol. 2014;30:721–728. doi: 10.1016/j.cjca.2013.10.015 [DOI] [PubMed] [Google Scholar]
- 39. Wilper AP, Woolhandler S, Lasser KE, McCormick D, Cutrona SL, Bor DH, Himmelstein DU. Waits to see an emergency department physician: U.S. trends and predictors, 1997–2004. Health affairs (Project Hope). 2008;27:w84–w95. [DOI] [PubMed] [Google Scholar]
- 40. Musey PI Jr, Kline JA. Do gender and race make a difference in acute coronary syndrome pretest probabilities in the emergency department? Acad Emerg Med. 2017;24:142–151. [DOI] [PubMed] [Google Scholar]
- 41. Snavely AC, Hendley N, Stopyra JP, Lenoir KM, Wells BJ, Herrington DM, Hiestand BC, Miller CD, Mahler SA. Sex and race differences in safety and effectiveness of the HEART pathway accelerated diagnostic protocol for acute chest pain. Am Heart J. 2021;232:125–136. doi: 10.1016/j.ahj.2020.11.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Bradley EH, Herrin J, Wang Y, McNamara RL, Webster TR, Magid DJ, Blaney M, Peterson ED, Canto JG, Pollack CV Jr, et al. Racial and ethnic differences in time to acute reperfusion therapy for patients hospitalized with myocardial infarction. JAMA. 2004;292:1563–1572. doi: 10.1001/jama.292.13.1563 [DOI] [PubMed] [Google Scholar]
- 43. Barnato AE, Lucas FL, Staiger D, Wennberg DE, Chandra A. Hospital‐level racial disparities in acute myocardial infarction treatment and outcomes. Med Care. 2005;43:308–319. doi: 10.1097/01.mlr.0000156848.62086.06 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Spertus JA, Jones PG, Masoudi FA, Rumsfeld JS, Krumholz HM. Factors associated with racial differences in myocardial infarction outcomes. Ann Intern Med. 2009;150:314–324. doi: 10.7326/0003-4819-150-5-200903030-00007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Takakuwa KM, Shofer FS, Hollander JE. Aspirin administration in ED patients who presented with undifferentiated chest pain: age, race, and sex effects. Am J Emerg Med. 2010;28:318–324. [DOI] [PubMed] [Google Scholar]
- 46. Tamayo‐Sarver JH, Hinze SW, Cydulka RK, Baker DW. Racial and ethnic disparities in emergency department analgesic prescription. Am J Public Health. 2003;93:2067–2073. doi: 10.2105/AJPH.93.12.2067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Chen I, Kurz J, Pasanen M, Faselis C, Panda M, Staton LJ, O’Rorke J, Menon M, Genao I, Wood J, et al. Racial differences in opioid use for chronic nonmalignant pain. J Gen Intern Med. 2005;20:593–598. doi: 10.1007/s11606-005-0105-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Harrison JM, Lagisetty P, Sites BD, Guo C, Davis MA. Trends in prescription pain medication use by race/ethnicity among US adults with noncancer pain, 2000–2015. Am J Public Health. 2018;108:788–790. doi: 10.2105/AJPH.2018.304349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci USA. 2016;113:4296–4301. doi: 10.1073/pnas.1516047113 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Tables S1–S13