

To the Editor
Prone positioning may recruit gas exchange-efficient regions for typical acute respiratory distress syndrome (ARDS) and improve oxygenation. It is also a mainstay of treatment in COVID-19-related ARDS (C-ARDS) and reduces the need for intubation without any signal of harm [1]. In the early phase of COVID-19, hypoxemia may be caused by impaired regulation of pulmonary perfusion [2]. Whether awake prone positioning can improve ventilation/perfusion (V/Q) matching through redistribution of pulmonary perfusion has not been demonstrated. In this study, we assessed the effect of prone position on V/Q matching using electrical impedance tomography (EIT) in non-intubated COVID-19 patients.
Inclusion criteria were: age > 18 and ≤ 75 years, admitted to ICU with confirmed COVID-19-related pneumonia, receiving supplemental oxygen (standard oxygen therapy or high-flow nasal cannula (HFNC)) for < 24 h. Exclusion criteria are given in Additional file 1.
Demographic, anthropometric and baseline data (arterial blood gases and ventilation parameters) were collected while the patient was supine (time-point SP1). EIT measurement was performed with PulmoVista 500 (Dräger Medical GmbH, Lübeck, Germany). The patients received instructions as to how to perform an end expiratory occlusion lasting at least 10 s. About one second after the start of the occlusion, a bolus of 10 mL 10% NaCl solution was injected via the central venous catheter manually. Subsequently, each patient was helped to change position from supine to prone; this took several minutes. After approximately 1 h, data were collected during an end expiratory occlusion and NaCl injection (time-point PP). The patient was then encouraged to maintain the prone position for > 3 h (ranged from 3 to 5.8 h without interruption) before being returned to the supine position. Clinical data collection, end expiratory occlusion and injection were repeated 1 h after resupination (time-point SP2).
From offline analyses of EIT data obtained 5 min before and during saline bolus injection, we calculated V/Q matching as described previously [3]. V/Q matching was quantified as percentage of pixels classified as ventilated divided by the number of pixels classified as perfused. Pixels were denoted as dead space if they were identified as ventilated but not perfused. Pixels were denoted as shunt if they were identified as perfused but not ventilated. To quantify the relative contribution of the dead space versus shunt fraction to V/Q mismatch, we calculated the dead space-to--shunt ratio.
Fourteen patients with bilateral pneumonia were enrolled (Additional file 1: Table S1).
V/Q matching, dead space fraction and oxygenation improved at PP, but were not maintained 1 h after resupination (Fig. 1). Prone positioning improved V/Q matching and PaO2/FiO2 in all the patients. Eight out of 14 patients had increased PaO2/FiO2 from SP1 to SP2. The dead space-to-shunt ratio was 1.9 ± 2.3, 1.4 ± 1.4 and 2.6 ± 2.5 at SP1, PP and SP2 (P = 0.392). Prone positioning decreased dead space fraction in 12 patients, decreased shunt fraction in 11 and decreased both shunt and dead space in 9. Dorsal ventilation and dorsal perfusion increased slightly during prone, and the respiratory rate was comparable (Additional file 1: Table S2).
Fig. 1.
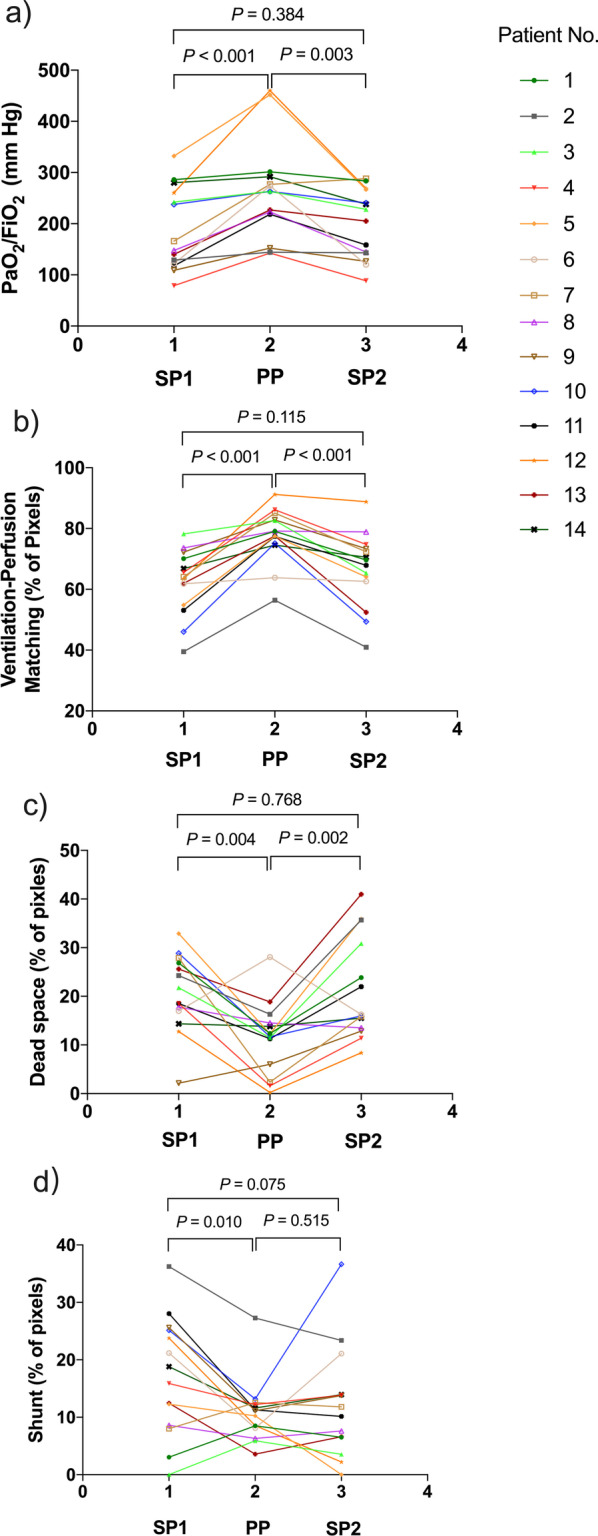
Per-patient trajectory of PaO2/FiO2 (a), ventilation–perfusion matching (b), dead space (c) and shunt (d) at the three study time points, SP1, PP and SP2. Each line is the trajectory of one patient. PaO2, partial pressure of oxygen; FiO2, fractional concentration of oxygen in inspired air; SP1, baseline supine position; PP, 1 h after prone positioning; SP2, 1 h after resuming supine position
These spontaneously breathing patients with COVID-19 pneumonia were characterized by reduced V/Q matching and a higher percentage of dead space lung units compared to shunt lung units. Prone positioning substantially improved overall V/Q matching mainly through decreased dead space, although this effect was lost after reverting to the supine position.
Hypoxemia in COVID-19 patients is primarily due to derangements in gas exchange caused by regional mismatch between ventilation and perfusion. Our data provide further evidence of V/Q mismatching, mainly due to nonperfused but ventilated units. The underlying biological mechanism might be microthrombi formation reflected by elevated d-dimers and loss of regulation of perfusion possibly by loss of hypoxic vasoconstriction, which may represent a key pathophysiological trait of C-ARDS.
The improvement in V/Q matching in the prone position was not surprising. Gravity is one of the variables responsible for V/Q matching, in concert with lung structure and fractal geometry, gas distribution and regulation of lung vascular tone [4]. The decrease in percentage of dead space lung units and slightly declining percentage of shunt lung units in our study during prone positioning might be related to several mechanisms including more uniform distribution of perfusion and ventilation in the prone position. Greater vascular conductance and greater nitric oxide expression in dorsal than in ventral lung vasculature might contribute to perfusion redistribution from supine to prone position [5]. There are other mechanisms impacting gas exchange in the prone position: pulmonary compression by the heart is decreased, changes in diaphragmatic function, and more uniform distribution of ventilation due to changes in elastance of the lung and chest wall.
This study has strengths in that it is the first to address the mechanisms leading to changes in gas exchange in the supine versus prone in spontaneously breathing patients not receiving CPAP. However, the major weakness is the small sample size and lack of a non-C-ARDS comparator group.
Supplementary Information
Additional file 1. Supplemental data including exclusion criteria, EIT measurement, statistical analyses, main characteristics of the study population, as well as Respiratory physiology, blood gas and ventilation homogeneity parameters.
Acknowledgements
Not applicable.
Abbreviations
- ARDS
Acute respiratory distress syndrome
- C-ARDS
COVID-19-related ARDS
- V/Q
Ventilation/perfusion matching
- EIT
Electrical impedance tomography
- HFNC
High-flow nasal cannula
- SP1
Baseline supine position
- PP
1 H after prone positioning
- SP2
1 H after resuming supine position
Author contributions
LL, YY, JX, MZ and HQ contributed to the conception and design. CW, YZ and XY contributed to data acquisition. ZZ, LL and AS contributed to data analysis and interpretation. LL, ZZ and AS contributed to drafting manuscript for important intellectual content. All authors revised the report. All authors read and approved the final manuscript.
Funding
This work was supported, in part, by Key Research and Development Plan of Jiangsu Province (BE2020786 and BE2019749) and research grants from the Ministry of Science and Technology of the People’s Republic of China (2020YFC0843700).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The study was approved by the Zhongda Hospital ethics committee (2020ZDSYLL057-P01). Written informed consent was obtained from all patients. Registered on clinicaltrials.gov (NCT04754113).
Consent for publication
Yes.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Ling Liu, Jianfeng Xie and Changsong Wang contributed equally and are co-first authors
References
- 1.Ehrmann S, Li J, Ibarra-Estrada M, Perez Y, Pavlov I, McNicholas B, et al. Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial. Lancet Respir Med. 2021;9:1387–1395. doi: 10.1016/S2213-2600(21)00356-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gattinoni L, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, et al. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med. 2020;46:1099–1102. doi: 10.1007/s00134-020-06033-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.He H, Chi Y, Long Y, Yuan S, Zhang R, Frerichs I, et al. Bedside evaluation of pulmonary embolism by saline contrast electrical impedance tomography method: a prospective observational study. Am J Respir Crit Care Med. 2020;202:1464–1468. doi: 10.1164/rccm.202005-1780LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lindahl SGE. Using the prone position could help to combat the development of fast hypoxia in some patients with COVID-19. Acta Paediatr. 2020;109:1539–1544. doi: 10.1111/apa.15382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nyrén S, Radell P, Lindahl SGE, Mure M, Petersson J, Larsson SA, et al. Lung ventilation and perfusion in prone and supine postures with reference to anesthetized and mechanically ventilated healthy volunteers. Anesthesiology. 2010;112:682–687. doi: 10.1097/ALN.0b013e3181cf40c8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Supplemental data including exclusion criteria, EIT measurement, statistical analyses, main characteristics of the study population, as well as Respiratory physiology, blood gas and ventilation homogeneity parameters.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.