

Abstract
Aims
Women’s participation is steadily growing in medical schools, but they are still not sufficiently represented in cardiology, particularly in cardiology leadership positions. We present the contemporary distribution of women leaders in cardiology departments in the World Health Organization European region.
Methods and results
Between August and December 2020, we applied purposive sampling to collect data and analyse gender distribution of heads of cardiology department in university/third level hospitals in 23 countries: Austria, Azerbaijan, Belgium, Bosnia-Herzegovina, Croatia, France, Germany, Greece, Italy, North Macedonia, Morocco, Poland, Portugal, Russia, Serbia, Slovakia, Slovenia, Spain, Switzerland, Tunisia, Turkey, Ukraine, and the UK. Age, cardiology subspecialty, and number of scientific publications were recorded for a subgroup of cardiology leaders for whom data were available. A total of 849 cardiology departments were analysed. Women leaders were only 30% (254/849) and were younger than their men counterpart (♀ 52.2 ± 7.7 years old vs. ♂ 58.1 ± 7.6 years old, P = 0.00001). Most women leaders were non-interventional experts (♀ 82% vs. ♂ 46%, P < 0.00001) and had significantly fewer scientific publications than men {♀ 16 [interquartile range (IQR) 2–41] publications vs. ♂ 44 (IQR 9–175) publications, P < 0.00001}.
Conclusion
Across the World Health Organization European region, there is a significant gender disparity in cardiology leadership positions. Fostering a diverse and inclusive workplace is a priority to achieve the full potential and leverage the full talents of both women and men.
Keywords: Gender gap, Women in cardiology, Cardiology leadership
Graphical Abstract
Graphical Abstract.

Introduction
Women are entering the medical and scientific community in growing numbers and reaching and even surpassing their male counterparts in medical schools. However, despite these recent changes, international cardiology community remains in a static imbalance of women and men.1–3 In the USA, women represent <15% of the cardiology workforce,1 while in Europe, women account for only one-third of cardiologists4 (Table 1). This disparity is also reflected in leadership positions in cardiology departments.
Table 1.
Number of women and men members of the European Society of Cardiology in the 23 countries studied
| Country | Women |
Men |
Total | ||
|---|---|---|---|---|---|
| % | No. | % | No. | ||
| Germany | 23 | 577 | 77 | 1929 | 2506 |
| France | 26.8 | 187 | 73.2 | 512 | 699 |
| Greece | 27.3 | 237 | 72.7 | 632 | 869 |
| Austria | 30.5 | 129 | 69.5 | 294 | 423 |
| Turkey | 31.1 | 151 | 68.9 | 334 | 485 |
| Switzerland | 31.4 | 228 | 68.6 | 497 | 725 |
| Belgium | 32.1 | 203 | 67.9 | 429 | 632 |
| Poland | 34.1 | 278 | 65.9 | 537 | 815 |
| Italy | 34.5 | 835 | 65.5 | 1585 | 2420 |
| Spain | 37.3 | 539 | 62.7 | 907 | 1446 |
| Bosnia-Herzegovina | 38.5 | 20 | 61.5 | 32 | 52 |
| UK | 38.8 | 1160 | 61.2 | 1826 | 2986 |
| Slovakia | 40.9 | 52 | 59.1 | 75 | 127 |
| Croatia | 42.2 | 95 | 57.8 | 130 | 225 |
| Tunisia | 42.4 | 36 | 57.6 | 49 | 85 |
| Serbia | 43.5 | 84 | 56.5 | 109 | 193 |
| Morocco | 46.4 | 32 | 53.6 | 37 | 69 |
| Slovenia | 47.2 | 59 | 52.8 | 66 | 125 |
| Portugal | 47.8 | 313 | 52.2 | 342 | 655 |
| North Macedonia | 48.5 | 32 | 51.5 | 34 | 66 |
| Azerbaijan | 57.8 | 26 | 42.2 | 19 | 45 |
| Russia | 58.3 | 427 | 41.7 | 306 | 733 |
| Ukraine | 59.5 | 260 | 40.5 | 177 | 437 |
| Grand total | 35.4 | 5960 | 64.6 | 10 858 | 16 818 |
In this analysis, we aimed to gain further inside and explore the current proportion of women and men in cardiology leadership positions in countries of World Health Organization (WHO) European region.
Methods and results
In this study, the Pink International Young Academy of Cardiology (IYAC) group looked at clinical heads of cardiology departments in university hospitals with the tertiary level of care.
The pink IYAC is an independent group of like-minded women cardiologists with the common goal of promoting and supporting women’s personal and professional growth in both the clinical and academic settings. It is a growing community, now counting representatives from over 20 countries around the world.5
Among members of the Pink IYAC, national representatives were selected to purposively screen the following countries: Austria, Azerbaijan, Belgium, Bosnia-Herzegovina, Croatia, France, Germany, Greece, Italy, North Macedonia, Morocco, Poland, Portugal, Russia, Serbia, Slovakia, Slovenia, Spain, Switzerland, Tunisia, Turkey, Ukraine, and the UK. Most of these countries belong to the WHO European region; two countries, Morocco and Tunisia, belong to WHO Eastern Mediterranean region.
National representatives identified all their respective countries’ university hospitals with tertiary cardiac care facilities and their cardiology department heads via university websites and, when required, using additional national systems. Tertiary institutions were defined as centres with specialized staff, equipment, and clinical services, performing 24/7 cardiac intervention services.6 The hospitals were identified and screened between August and December 2020. For a subgroup of cardiology departments’ leaders, whose curricula vitae were publicly available, we conducted a subgroup analysis investigating age, cardiology subspecialty, and number of total, first, and last author publications. We obtained these data from the University website, Hospital’s website, ClinicalTrials.gov, and PubMed database. In the subgroup analysis, we excluded leaders with very common surnames to avoid homonymy errors; we excluded, then, countries with over 50% data missing to have a good representation of the entire nation. We analysed 7 countries for leaders’ age, 10 countries for cardiology subspecialties, and 15 countries for scientific publications.
We used only publicly available data; thus, no ethical committee approval was required.
We presented continuous variables as mean (standard deviation) or median (interquartile range) as appropriate. Categorical variables were reported as counts and percentages. Comparisons between subgroups were tested using T-test, Mann–Whitney U-test, or Chi-square (χ2) test. Correlations between continuous variables were assessed by Pearson test. A P-value of <0.05 was considered statistically significant. Statistical analysis was performed with SPSS version 23.0 (SPSS, Chicago, IL, USA).
Out of the 23 countries analysed, we identified 849 university cardiology departments with tertiary level facilities. Out of the 849 cardiology departments, 254 (30%) had women heads (Figure 1A and B). There were only two countries with more women than men leading cardiology departments: Russia (168 women vs. 102 men, 62%) and Morocco (4 women vs. 3 men, 57%). Apart from Russian data, the total women leaders were 15% (86/579 cardiologists) among the other 22 countries. There were no women leading cardiology departments in eight nations: Azerbaijan, Germany, Greece, North Macedonia, Portugal, Serbia, Slovenia, and Switzerland.
Figure 1.

Cardiology leadership in European and neighbouring countries compared by gender. (A) Countries map with the percentage of women leaders. (B) Bar plot charts displaying the number of women and men cardiology leaders by nations. (C) Bar plot chart displaying cardiology subspecialty by gender in Belgium, Germany, Italy, North Macedonia, Portugal, Spain, Tunisia, Turkey, Ukraine, and the UK. Non-interventional: clinical cardiologists and imaging experts. Interventionalists: hemodynamic interventionalists and electrophysiologists. (D) Bar plot chart displaying number of total publication and first/last author publication by gender in Austria, Belgium, Croatia, France, Germany, Italy, Morocco, North Macedonia, Serbia, Slovenia, Spain, Tunisia, Turkey, Ukraine, and the UK.
The percentage of women leaders per country was correlated to the Gender Inequality Index (GII, United Nations Development Programme).7 This index measures gender inequalities in three specific aspects of human development, empowerment, economic status, and reproductive health. It is calculated using the proportions of men and women achieving higher education, the proportion of women in parliament, female and male workforce participation rate, teen birth rate, and maternal mortality rate. GII ranges from 0 to 1, with 0 showing perfect gender equality and 1 showing perfect gender inequality in favour of men.
Interestingly, there was a trend (R = 0.62) for countries with a higher percentage of women leaders to have a higher GII, i.e. lower gender parity (Figure 2).
Figure 2.
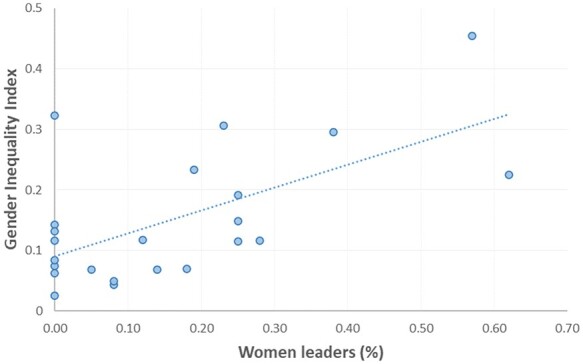
Scatter plots demonstrating correlation between the percentage of women leaders in each country and the Gender Inequality Index. Gender Inequality Index by country available at http://hdr.undp.org/en/content/gender-inequality-index-gii.
Among 7 countries where the age of those in leading positions was available (Germany, Italy, Portugal, Spain, Tunisia, Turkey, and Ukraine), women leaders were significantly younger than their male counterparts (52.2 ± 7.7 years old vs. 58.1 ± 7.6 years old, P = 0.00001).
Analysing the cardiology subspecialization in Belgium, Germany, Italy, North Macedonia, Portugal, Spain, Tunisia, Turkey, Ukraine, and the UK, we found the majority of women heads were non-interventional experts, namely clinical cardiologist or cardiovascular imaging expert (women 82% vs. men 46%, P < 0.00001) (Figure 1C).
On further analysis of women’s representation in published research in Austria, Belgium, Croatia, France, Germany, Italy, Morocco, North Macedonia, Serbia, Slovenia, Spain, Tunisia, Turkey, Ukraine, and the UK, we observed a significant gender disparity in the number of total publications {women 16 [interquartile range (IQR) 2–41] publications vs. men 44 (IQR 9–175) publications, P < 0.00001} and a trend of underrepresentation of women as first and last authors [4 (IQR 0–10) publications vs. 12 (IQR 1–41) publications, P < 0.001] (Figure 1D).
Discussion
To our knowledge, this article is the first to study the contemporary proportion of women in cardiology leadership in the WHO European region. This analysis shows a vast prevalence of men in senior positions in university cardiology departments.
Several reasons may explain the limited number of women leading cardiology departments. In our study, we found only 18% of women were interventionists. Traditionally, interventional specialties have been marred with misconceptions around radiation safety in pregnancy, which might partially explain the fewer number of women in such procedural subspecialties.2,8 Women are far more likely to face discrimination because of their sex or parental duty. Child care and other domestic responsibilities potentially lead to reduce work hours and pursue less than full-time training, and this hardly fits with the demanding interventional career and its such little flexible schedule.
As shown in our study, women cardiology leaders may have less opportunity to publish and this may hinder career advancement. Furthermore, because of the imbalance in senior-level roles, it can be difficult to encounter women role models and mentors, which can perpetuate their deficiency in cardiology and in leadership positions.
In our observation, Russia and Morocco present an encouraging good representation of women in leadership positions; however, this might partially reflect the social and economic challenges these two countries encountered in the last decades, leading the public healthcare system to be less attractive to men.9
Interestingly, countries with a higher GII (i.e. lower gender equality in society) had a higher percentage of women leaders. Gender balance in cardiology leadership positions would not reflect the gender equality development in the society but rather may depend on the overall percentage of women cardiologists in the country.
It is encouraging that we did observe younger women in leadership positions; this potentially shows the progressive feminization of the medical profession,2,3 as well as the active intervention by professional societies in increasing the visibility of women in recent years.
Dedicated activities and projects are emerging to promote women’s self-realization, personal and professional growth, and community recognition. The Women Transforming Leadership Programme, along with the many activities during annual European Society of Cardiology’s meetings, is just some of the notable efforts made by the society in recent years to strengthen gender balance in cardiology.4 The European Heart Rhythm Association’s Women in Electrophysiology initiatives foster the recognition of the gender-specific aspects of female arrhythmias and women professionals.10 Recently, the European Association of Cardiovascular Imaging Task Force on Women is launching several initiatives entirely dedicated to women, particularly those from developing countries, to promote their professionals. The Escalator Award and CLIMB training in procedural subspecialties, offered by the women as one organization, are initiatives to expand women’s opportunities in cardiology leadership and procedural competency. Finally, the Pink IYAC group supports female colleagues with various ongoing projects; as a part of our commitment, we endorse valuable young women researchers in developing their high-potential ideas and thriving in the scientific arena.5
This study has some limitations. Data were collected purposively, in countries in which Pink IYAC members were present and had access to such data; as such, the analysis is not comprehensive but a reasonable preliminary attempt to quantify the problem of gender disparities in cardiology leadership of the European region. Also, some representatives from WHO Eastern Mediterranean countries were involved in the effort of balancing the observation. We focused only on university hospitals with tertiary level of care; therefore, many hospitals, even with tertiary level of care, were missing from the analysis. We did use only publicly available data and not tools, such as questionnaires and surveys; thus, some further gender differences may have been missed. Clinical heads of cardiology departments in university hospitals represent only a part of the entire community of cardiologists, yet the gender dis-balance among them allows us to show, on a small scale, a much wider issue.
In conclusion, across European region, a significant gender gap exists in cardiology and in cardiology leadership positions. There is a pressing need to identify and overcome specific barriers to women’s career opportunities, to build a sustainable work environment that fosters inclusion and diversity and promotes the full potential of all its members, regardless of gender.
Author contributions

Nunzia Borrelli graduated from University of Campania “L.Vanvitelli”. She received the board certification in cardiovascular diseases in 2019 and was a research fellow at the Royal Brompton Hospital Paediatric Echo-Lab—Imperial College of London, from 2018 to 2019. She is currently working at the tertiary centre for Adult Congenital Heart Disease, AORN Dei Colli—Monaldi Hospital, Naples. She is an expert in non-invasive cardiovascular imaging of paediatric and adult heart diseases. Her areas of research include congenital heart disease in paediatric and adult age and non-invasive cardiovascular imaging. She was a recipient of the European Association of Cardiovascular Imaging training grant 2019.
Conflict of interest: none declared.
Data Availability
The datasets were derived from sources in the public domain: https://pubmed.ncbi.nlm.nih.gov/; ClinicalTrials.gov; Universities' and hospitals' websites.
Acknowledgment: We would like to thank the European Society of Cardiology Membership Committee for kindly providing data on the number of European Society of Cardiology members.
References
- [1]. Burgess S, Shaw E, Zaman S.. Women in cardiology. Circulation 2019;139:1001–1002. [DOI] [PubMed] [Google Scholar]
- [2]. Sinclair HC, Joshi A, Allen C, Joseph J, Sohaib SMA, Calver A, Smith R.. Women in cardiology: The British Junior Cardiologists' Association identifies challenges. Eur Heart J 2019;40:227–231. Jan 14 [DOI] [PubMed] [Google Scholar]
- [3]. Andreotti F, Crea F.. Women in cardiology: a European perspective. Heart 2005;91:275–276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4]. European Society of Cardiology. Sophia Antipolis Cedex, France. Women in ESC. https://www.escardio.org/The-ESC/What-we-do/Initiatives/Women-in-ESC#:∼:text=On%20average%20only%2034%25%20of,economic%20growth%2C%20sustainability%20and%20competitiveness (20 January 2021).
- [5]. Moscatelli S, Kotlar I, Babazade N, Sabatino J, Öz TK.. Women empowerment in cardiology: the pink international young academy of cardiology. JACC Case Rep 2020;2:2037–2039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6]. Søholm H, Kjaergaard J, Bro-Jeppesen J, Hartvig-Thomsen J, Lippert F, Køber L, Nielsen N, Engsig M, Steensen M, Wanscher M, Karlsen FM, Hassager C.. Prognostic implications of level-of-care at tertiary heart centers compared with other hospitals after resuscitation from out-of-hospital cardiac arrest. Circ Cardiovasc Qual Outcomes 2015;8:268–276. [DOI] [PubMed] [Google Scholar]
- [7]. United Nation Development Programme. Human development reports. Gender inequality index. http://hdr.undp.org/en/content/gender-inequality-index-gii (23 May 2021).
- [8]. Burgess S, Shaw E, Ellenberger K, Thomas L, Grines C, Zaman S.. Women in medicine: addressing the gender gap in interventional cardiology. J Am Coll Cardiol 2018;72:2663–2667. [DOI] [PubMed] [Google Scholar]
- [9]. Stepantchikova N, Lakunina L, Tchetvernina T. Socio-Economic Status of Health Care Workers in the Russian Federation. Paper presented at the Workshop on Health Care Privatization: Workers Insecurities in Eastern Europe. Geneva: International Labour Office 2001.
- [10]. European Society of Cardiology. Sophia Antipolis Cedex, France. Women in electrophysiology. https://www.escardio.org/Sub-specialty-communities/European-Heart-Rhythm-Association-(EHRA)/Advocacy/Women-in-Electrophysiology (09 May 2021).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets were derived from sources in the public domain: https://pubmed.ncbi.nlm.nih.gov/; ClinicalTrials.gov; Universities' and hospitals' websites.
Acknowledgment: We would like to thank the European Society of Cardiology Membership Committee for kindly providing data on the number of European Society of Cardiology members.