

Abstract
Background:
Trunk stability is key in controlling body balance and movements. Trunk Stabilization Exercises (TSE) and Conventional Trunk Exercises (CTE) are performed to improve dynamic balance. The authors have previously reported that dynamic balance was improved by a 12-week and 6-week TSE program. However, there is a dearth of research on its immediate effect on dynamic balance in trained soccer players.
Objective:
To compare the immediate effect of TSE with that of CTE on dynamic balance in trained soccer players.
Methods:
Forty-eight male soccer players (24.60 ± 1.38 years) participated in this crossover study, wherein each participant took part in three exercise sessions: TSE, CTE, and No Exercise control (NE), each consisting of three steps: pre-test, intervention and post-test, with an interval of one week between each exercise condition. To assess dynamic balance, the Y Balance Test-Lower Quarter (YBT-LQ) score in the anterior, posteromedial, and posterolateral directions was measured before and 5 minutes after each intervention.
Results:
The YBT-LQ composite score was significantly improved after TSE (0.51) as compared to CTE (0.22) and NE (0.04) (p<0.05). Furthermore, in TSE and CTE conditions, YBT-LQ scores of the posterolateral and posteromedial directions significantly improved at the post-test (p<0.05).
Conclusion:
Both TSE and CTE are effective in immediately improving dynamic balance; however, TSE showed greater improvement as compared to the latter. Immediate improvements in the posteromedial and posterolateral directions of the YBT-LQ were demonstrated after performing the TSE and CTE.
Keywords: Core training, balance, trunk exercises, sit-ups
Introduction
The trunk acts at the center of the kinetic chain and essentially helps to maximize the athletic function.1,2 Function is produced primarily by sequenced and coordinated activation of body segments that station the distal segment in optimum position at the optimum velocity with the optimum timing in order to produce the desired athletic task.2 In sports such as soccer, besides its local functions of generating optimum force and providing stability, the trunk is also involved in most activities of the lower limbs such as kicking, running, throwing, and jumping.3
A common approach, for coaches or athletes, while designing a strength and conditioning regime, is to primarily focus on the body segment that is most seemingly required to succeed in the game.4 If the sport demands high impact activities such as jumping, sprinting, or kicking, like in soccer, training is conventionally focused on the lower segments, followed by the upper body. Trunk training is given least attention or is performed towards the end of the workout regime. However, Gambetta et al. claim that without adequate strength and stability of the trunk, the athlete shall not be able to apply sufficient extremity strength necessary for optimal strength development.5
A well strengthened core allows for improved force output, increased neuromuscular efficiency, and decreased incidence of overuse injuries which transfers to variety of sports related activities.6 Strengthening the core can enhance the ability to accurately utilize the musculature of upper and lower body segments leading to powerful and efficient movements.6 Conventional Trunk Exercises (CTE) such as sit-ups, abdominal crunches or back extensions are traditionally performed to strengthen the trunk muscles and include repeated flexion and extension movements of the trunk.7 Since the only resistance to core muscle activity is the body weight, these exercises do not provide sufficient levels of muscle activity to strengthen the trunk.8,9 Hence, substantial repetitions of these exercises may be required to achieve optimum performance.10
Alternatively, Trunk Stabilization Exercises (TSE) like side and back bridges are performed by adjusting the functional postures such as keeping the lumbar spine in a neutral position with little or no trunk movements. The chief goal of the TSE is to enhance and restore co-contraction and coordination of local and global muscles to improve the control of the pelvis and the lumbar spine.11,12 Besides, it also aims to restore the capacity of the trunk muscles to meet the demands of postural control.13,14 Previous studies have demonstrated significant improvement in trunk stability and athletic performance after training with TSE15,16 and have also proved its efficacy in rehabilitating patients with low back pain.17,18 Moreover, it has been reported that the warm-up programs including TSE reduced the incidence of anterior cruciate ligament injury.19
Previously, the effect of trunk exercises on static and dynamic balance was studied in healthy adults including college athletes. Kahle et al.20 reported that TSE improved the dynamic balance in healthy individuals. Although the training effects of trunk exercises have been reported, there are limited studies comparing the effect of the TSE and CTE. Previous investigations indicate that the TSE had a specific effect in immediately improving the static balance.21,22 Atsushi et al.23 and Kahle et al.20 reported that dynamic balance was improved by a 12-week and 6-week stabilization exercise program, respectively. On the other hand, Imai et al. illustrated that TSE brings about immediate improvements in the posteromedial and posterolateral directions of the star excursion balance test in adolescents.24 However, there is a lack of evidence to decisively prove the immediate effect of TSE and CTE on dynamic balance.
Therefore, this study aimed to compare the immediate effect of CTE on dynamic balance with that of TSE. The program that proves to bring about instantaneous trunk stability may further benefit players to prevent injuries and enhance performance.
Materials and Methods
In this prospective interventional study, a total of 83 male soccer players between ages 20–30 years were screened for the eligibility criteria. Zonal and University healthy soccer players, with three or more years of competitive experience, practicing regularly for minimum two hours/day for at least three days/week and not involved in any balance training program apart from their typical sports training were included in the study. The criteria for exclusion were recreational soccer players, those who reported vestibular problems, low back pain or lower limb injuries that required treatment or that may have impeded performance in the past year and those who had undergone lumbar spine or any lower extremity surgery in the past six months. Finally, 55 individuals (mean age 24.60 years and BMI ) were included between March 2018 to March 2019. A written informed consent was obtained from each participant. The study was approved by the ethics committee of A J Institute of Medical Sciences, Mangalore.
A crossover design was employed in this study in which every subject participated in three conditions i.e., TSE, CTE, and No Exercise (NE) control. Each participant was investigated during a course of three weeks with an interval of one week between three exercise conditions to preclude the impact of exercises performed previously. Every testing condition comprised of three stages: Pretest, intervention, and posttest. Performance on the Y Balance Test – Lower Quater was noted before and five minutes after each intervention. The TSE and CTE programs lasted five minutes each and were supervised and directed by a physical therapist. During the NE session, the subject rested for five minutes on a chair. Using the online randomization http://www.graphpad.com/quickcalcs/index.cfm, the physical therapist generated the randomized order of the three conditions to be performed by the participants, wherein they underwent TSE, CTE, and NE sessions in arbitrary order. Consequently, 19 subjects performed in the order of TSE, CTE, and NE; 18 subjects in the order of CTE, NE, and TSE; and 18 subjects in order of NE, TSE, and CTE. Seven participants could not complete all sessions due to personal reasons.
Interventions
The TSE and CTE exercise programs were adapted from a crossover design conducted by Imai et al. in adolescent soccer players.24 The TSE regime comprised of the back bridge, front plank and quadruped exercise (Fig. 1). The first exercise was performed in a back bridge position by raising the pelvis so that a neutral hip flexion angle was maintained and then raised on one leg with complete knee extension. This position was held for 5 s before raising the opposite leg followed by 10 s rest. In the front plank position, the participant was asked to simultaneously raise the left arm and right leg and hold it straight up for 5 s. This was immediately followed by raising the right arm and left leg simultaneously for 5 s after which he was asked to lower his body and rest for 10 s. In a similar manner, the last exercise was performed in a quadruped position. Each exercise was performed five times. Okubo et al.25 reported that the given TSE involve activity of trunk muscles higher than that of other conventional exercises of the trunk. The TSE was completed within an average of three minutes. The YBT-LQ was recorded immediately thereafter.
Fig. 1.
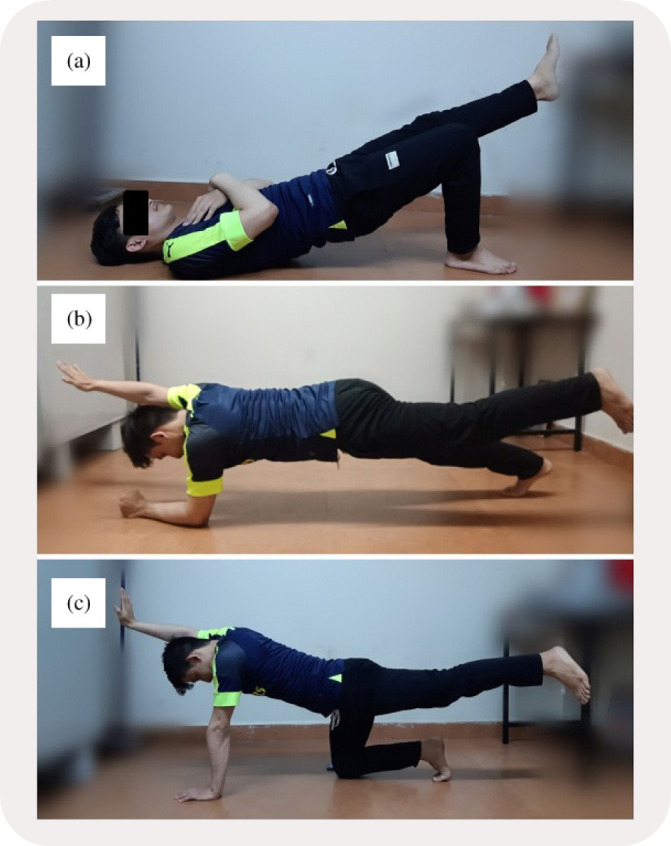
Trunk stabilization exercises. (a) Back Bridge; (b) Front Plank; (c) Quadruped Exercise.
For the CTE program, subjects performed back extensions, sit-ups, and sit-ups with trunk rotation (Fig. 2). Each exercise was repeated 30 times. The YBT-LQ was recorded immediately thereafter.
Fig. 2.
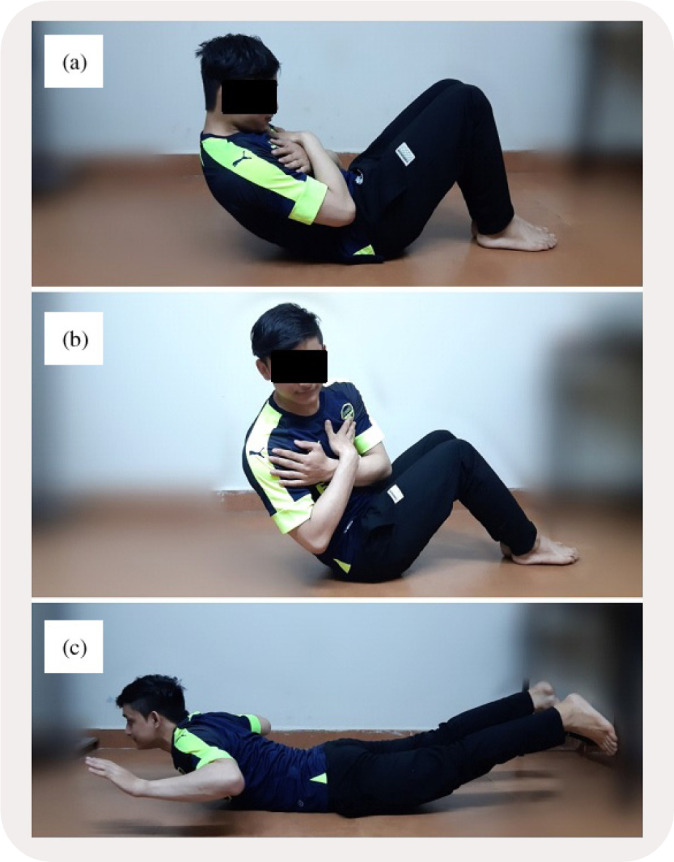
Conventional trunk exercises. (a) Sit-ups; (b) Sit-ups with trunk rotation; (c) Back Extensions.
Outcome measure
The Y Balance Test – Lower Quarter: The participants performed the YBT-LQ in the anterior, posterolateral, and posteromedial directions.26,27,28 Verbal instructions and visual demonstration of the test were given by the therapist before performing the test. During the test, both hands were held at the iliac crest. The leg used for kicking the ball during game was used as the stance limb, with the distal most part of the great toe set at the intersection of the three measuring tapes taped to on the floor (Fig. 3). While they maintained the single-leg stance, they were to use the opposite leg to reach on the line along the respective directions, touch the ground at the farthest point possible with the distal most part of the great toe and return to the starting position. In order to rule out the influence of shoes, the test was performed barefoot. After three practice trials, the subjects were asked to rest for 2 min and thereafter three test trials were performed in each direction. At each test trial, the order of the reaching directions was randomized. If a subject failed to maintain the stance leg or in returning the reaching foot to the starting position, the test was discarded and repeated over again. In each direction, the longest reach distance was used for further analysis. To exclude the influence of limb length, it was normalized with the reach distances of the subject.29,30 The limb length was measured from the anterior superior iliac spine to the center of the ipsilateral medial malleolus.30 The composite score was calculated using the following formula26:
Fig. 3.

Directions of the Y Balance Test - Lower Quarter. (a) Anterior; (b) Posterolateral; (c) Posteromedial.
Sample size and sampling
A sample size was estimated with 95% confidence level and 80% test power based on the parameters of Imai et al.24 where the mean difference () between pre and post intervention was 2.8. This showed that the ideal sample size for the study would be 46. The study subjects were recruited using convenience sampling on the basis of the inclusion and exclusion criteria.
Statistical analyses
Statistical package SPSS (IBM SPSS Statistics for Windows, ver. 21.0. Armonk, NY: IBM Corp.) was used to analyze the data. The Kolmogorov–Smirnov test and Levene test were used to test normality and equal variance assumptions, respectively. The baseline data of the YBT-LQ between groups were compared by using a one-way ANOVA. A two-way () repeated measures ANOVA was used to assess the changes over time and the between-group difference. Further, a Tukey’s HSD post hoc test was done when a statistically significant interaction effect was found. Statistical significance was inferred at . Effect size (ES) was calculated using Cohen’s to compare the results of the pre-test and the post-test. ESs were interpreted as large (), moderate (0.51–0.80), or small (0.21–0.50).
Results
There were no significant differences in the baseline data of the composite scores and each direction of the YBT-LQ between groups (). Significant condition-by-time interactions existed for the YBT-LQ composite score (; ). The composite score improved following both regimes however, the Tukey’s HSD post hoc test detected that the composite score was greater post TSE (, ) as compared to CTE (; ). Moderate to small ESs were associated with these relations. There was no significant change in the composite score after NE (; ) (Table 1).
Table 1.
Changes in normalized composite scores of the balance test — Lower quarter.
| Pre-test (Mean SD) | Post-test (Mean SD) | Tukey’s HSD ( value) | ES | % change | |
|---|---|---|---|---|---|
| Compositea | |||||
| TSE | 109.86 4.27 | 112.07 4.27* | 0.010 | 0.51 | 2.01 |
| CTE | 109.83 4.30 | 110.78 4.34* | 0.012 | 0.22 | 0.86 |
| NE | 109.78 4.28 | 109.98 4.33 | 0.131 | 0.04 | 0.18 |
Notes: aSignificant group-by-time interaction ().
Significant difference between the pre and post scores ().
CTE: Conventional Trunk Exercises; ES: Effect size; NE: No Exercise; TSE: Trunk Stabilization Exercises.
When scores of each direction were analyzed, there were significant condition-by-time interactions in the posteromedial direction (, ) and posterolateral direction (, ), with no effect in the anterior direction (, ). The Tukey’s HSD post hoc test revealed significantly greater scores in the posteromedial and posterolateral directions at the posttest than at the pretest in the TSE and CTE conditions. Moderate to small ESs were associated with these relations (Table 2).
Table 2.
Changes in normalized reach distance scores of the balance test — Lower quarter.
| Pre-test (Mean SD) | Post-test (Mean SD) | Tukey’s HSD ( value) | ES | % change | |
|---|---|---|---|---|---|
| Anterior | |||||
| TSE | 78.88 5.00 | 79.30 5.04 | — | 0.08 | 0.53 |
| CTE | 78.89 4.68 | 79.37 4.68 | — | 0.10 | 0.60 |
| NE | 78.87 4.80 | 79.30 4.79 | — | 0.06 | 0.54 |
| Posteromediala | |||||
| TSE | 108.43 4.82 | 113.04 4.71* | 0.000 | 0.96 | 4.25 |
| CTE | 108.64 4.62 | 110.17 4.45* | 0.012 | 0.33 | 1.40 |
| NE | 108.65 5.12 | 109.41 5.16 | 0.437 | 0.14 | 0.70 |
| Posterolaterala | |||||
| TSE | 106.90 4.95 | 108.78 5.85* | 0.000 | 0.34 | 1.75 |
| CTE | 106.84 4.72 | 107.35 4.73* | 0.009 | 0.12 | 0.48 |
| NE | 106.85 4.98 | 107.19 4.86 | 0.502 | 0.07 | 0.31 |
Notes: aSignificant group-by-time interaction ().
Significant difference between the pre and post scores ().
CTE: Conventional Trunk Exercises; ES: Effect size; NE: No Exercise; and TSE: Trunk Stabilization Exercises.
Discussion
This investigation aimed to compare the immediate effect of two different types of trunk exercise programs on dynamic balance in professional soccer players. It was observed that the YBT-LQ composite score significantly improved after TSE and CTE. However, the former had greater effect concerning immediate improvement in dynamic balance as compared to CTE. Imai et al. in a similar study in adolescent soccer players24 noted that the YBT-LQ composite score improved only after the TSE but not after CTE or NE. Although previous researchers have established that 6 weeks or 12 weeks of the SE improved dynamic balance,20,23 this study provides evidence that compares the acute effects of stabilization and conventional exercises on dynamic balance in young trained athletes.
Compared to the CTE and NE conditions, participants displayed improved reach distance scores of the YBT-LQ in the TSE condition as compared to CTE. The two exercise programs vary in terms of the stresses acting on specific body segments.24 To derive the optimal effects of physical training basic principles, such as the Specific Adaptation to Imposed Demands (SAID), must be followed, stating that the body adapts specifically in response to the demands and stresses placed on it.31 In CTE, stress to flexors and extensors of the lumbar spine is applied in a dynamic bilateral manner. SE program, to the contrary, maintain and control closed kinetic chain positions placing unilateral stresses on muscles involved in hip extension, in resemblance to stresses in the posterolateral and posteromedial directions of the YBT-LQ.24 Consequently, in terms of SAID, the SE may be more capable than the CTE as a training program in improving the dynamic balance.
Concerning the YBT-LQ maximum reach distance scores, the results demonstrated the improvements in the posterolateral and posteromedial reach distances with no change in the anterior reach direction. Imai et al. in their crossover study also demonstrated similar findings.24 The local and global trunk muscles are recruited and adjusted maintaining the trunk in position during the TSE program.25 The range of motion of hip flexion of the stance leg has a fundamental contribution while moving the contralateral limb in the posterior direction.32 Eccentric muscle contraction of the erector spinae, multifidus, and hamstrings is essential to maintain balance as the trunk leans forward in the YBT-LQ position.33,34 Consequently, participants may possibly have improved control over trunk position during the posterior directions of the YBT-LQ after the TSE due to the contribution of both local and global muscles, with trunk motion controlled by the latter.24 In addition, enhancing the control of the trunk rotation may have helped in control of the lower extremity during the posteromedial direction since the TSE involved both upper and lower limb excursions that has previously shown to involve increased external oblique activity.28
The anterior direction maximum reach scores, on the other hand, did not change post exercise in any of the exercise conditions. Previous studies that investigated both immediate and long term effects of training on dynamic balance, support these findings.24,26 It is probable that the anterior direction is sensitive to changes affected by distal segments than proximal as it is reported that dorsiflexion range influences the anterior direction to a greater extent than posterior directions.30
There are few limitations in this study, first being a limited sample size with all young male soccer players. Further, confirmation of these results must be carried out in larger and diverse populations, including female athletes and older individuals. The results apply only to the TSE and CTE programs used in this study. The existing literature consists of various trunk exercises and methods to enhance the strength of trunk muscles and trunk control. However, this investigation studied the effect on the YBT-LQ of the TSE and CTE programs comprising three exercises. This study also could not prove how long the immediate effect on the YBT-LQ lasts and will need to be investigated in the future to elucidate the efficacy of trunk exercises. Finally, this study could not prove if the exercises could play a role in terms of injury prevention in soccer players.
Conclusion
Posterolateral and posteromedial directions of the YBT-LQ improved immediately after the TSE as compared to the CTE. Since an immediate effect on YBT-LQ was demonstrated, a trunk exercise program may enhance the dynamic balance, vital for almost all athletic activities. Strength and conditioning professionals use various exercises as part of warm-up programs to improve the performance and the simple TSE program used in this study can be easily incorporated into a warm-up routine. Therefore, it is recommended that the coaches and trainers consider altering their warm-up sessions to include trunk strengthening exercises, with the hope of enhancing the athlete’s dynamic balance.
Acknowledgment
We would like to express our gratitude to the study participants and are thankful to the statistician, Mr. M. S. Kotian for his invaluable contribution to the study and also to the Principal and teaching staff of our institute for their support and guidance.
Conflict of Interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding/Support
The authors received no financial support for the research and/or authorship of this paper.
Author Contributions
Conception and design of study: C.J. D’souza, H. Santhakumar; Acquisition of data: C.J. D’souza, B. Bhandary, A. Rokaya; Analysis and/or interpretation of data: C.J. D’souza, H. Santhakumar, A. Rokaya. Drafting the manuscript: C.J. D’souza, A. Rokaya; Revising the manuscript critically for important intellectual content: H. Santhakumar, B. Bhandary. Approval of the version of the manuscript to be published: C.J. D’souza, H. Santhakumar, B. Bhandary, A. Rokaya.
References
- 1. Mills JD, Taunton JE, Mills WA. The effect of a 10-week training regimen on lumbo-pelvic stability and athletic performance in female athletes: A randomized controlled trial. Phys Ther Sport 2005;6:60–6. [Google Scholar]
- 2. Putnam CA. Sequential motions of body segments in striking and throwing skills: descriptions and explanations. J Biomech 1993;26:125–35. [DOI] [PubMed] [Google Scholar]
- 3. Kibler WB, Press J, Sciascia A. The role of core stability in athletic function. Sports Med 2006;36:189–98. [DOI] [PubMed] [Google Scholar]
- 4. Brittenham D, Brittenham G. Stronger Abs and Back. Champaign, IL: Human Kinetics, 1997. [Google Scholar]
- 5. Gambetta V, Clark M. Hard core training. Training Cond 1999;10:34–40. [Google Scholar]
- 6. Cook G, Fields K. Functional training for the torso. Strength Cond 1997;19:14–9. [Google Scholar]
- 7. Thomas TR, Ridder MB. Resistance exercise program effects on abdominal function and physique. J Sports Med Phys Fitness 1989;29:45–8. [PubMed] [Google Scholar]
- 8. Petrofsky JS, Morris AN, Jorritsma R, Bonacci J, Bonilla T. Aerobic training on a portable abdominal machine. J Appl Res Clin Exp Ther 2003;3:402–15. [Google Scholar]
- 9. Petrofsky JS, Bonacci J, Bonilla T, Jorritsma R, Morris AN, Almalty AM. Comparison between an abdominal curl with times curls on a portable abdominal machine. J Appl Res Clin Exp Ther 2003;3:394–401. [Google Scholar]
- 10. Petrofsky JS, Cuneo M, Dial R, Pawley AK, Hill J. Core strengthening in a geriatric population. J Appl Res Clin Exp Ther 2005;5:423–33. [Google Scholar]
- 11. Hodges PW. Core stability exercise in chronic low back pain. Orthop Clin North Am 2003;34(2): 245–54. [DOI] [PubMed] [Google Scholar]
- 12. Richardson CA, Jull GA, Hodges PW, Hides JA. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain: Scientific Basis and Clinical Approach. Edinburgh: Churchill Livingstone, 2003. [Google Scholar]
- 13. McGill S. Low Back Disorders: Evidence Based Prevention and Rehabilitation. Champaign, IL: Human Kinetics Publishers, Inc., 2002. [Google Scholar]
- 14. Saal JA, Saal JS. Non-operative treatment of herniated lumbar intervertebral disc with radiculopathy: An outcome study. Spine 1989;14:431–7. [DOI] [PubMed] [Google Scholar]
- 15. Butcher SJ, Craven BR, Chilibeck PD, Spink KS, Grona SL, Sprigings EJ. The effect of trunk stability training on vertical takeoff velocity. J Orthop Sports Phys Ther 2007; 37:223–31. [DOI] [PubMed] [Google Scholar]
- 16. Sato K, Mokha M. Does core strength training influence running kinetics, lower-extremity stability, and 5000-M performance in runners? J Strength Cond Res 2009; 23:133–40. [DOI] [PubMed] [Google Scholar]
- 17. Durall CJ, Udermann BE, Johansen DR, Gibson B, Reineke DM, Reuteman P. The effects of preseason trunk muscle training on low-back pain occurrence in women collegiate gymnasts. J Strength Cond Res 2009;23:86–92. [DOI] [PubMed] [Google Scholar]
- 18. Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilization exercises for first-episode low back pain. Spine 2001;26:243–8. [DOI] [PubMed] [Google Scholar]
- 19. Waldén M, Atroshi I, Magnusson H, Wagner P, Häggulund M. Prevention of acute knee injuries in adolescent female soccer players: cluster randomised controlled trial. BMJ 2012;344:3042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kahle NL, Gribble PA. Core stability training in dynamic balance testing among young, healthy adults. Athl Train Sports Health Care 2009;1:65–73. [Google Scholar]
- 21. Kaji A, Sasagawa S, Kubo T, Kanehisa H. Transient effect of core stability exercises on postural sway during quiet standing. J Strength Cond Res 2010;24:382–8. [DOI] [PubMed] [Google Scholar]
- 22. Imai A, Kaneoka K, Okubo Y. The immediate effects of different core exercises on static balance. Jpn Soc Clin Sports Med 2012;20:469–74. [Google Scholar]
- 23. Imai A, Kaneoka K, Okubo Y, Shiraki H. Effects of two types of trunk exercises on balance and athletic performance in youth soccer players. Int J Sports Phys Ther 2014;9:47–57. [PMC free article] [PubMed] [Google Scholar]
- 24. Imai A, Kaneoka K, Okubo Y, Shiraki H. Comparison of the immediate effect of different types of trunk exercise on the star excursion balance test in male adolescent soccer players. Int J Sports Phys Ther 2014;9:428–35. [PMC free article] [PubMed] [Google Scholar]
- 25. Okubo Y, Kaneoka K, Imai A, Shiina I, Tatsumara M, Izumi S et al. Electromyographic analysis of transversus abdominis and lumbar multifi dus using wire electrodes during lumbar stabilization exercises. J Orthop Sports Phys Ther 2010;40:743–50. [DOI] [PubMed] [Google Scholar]
- 26. Filipa A, Byrnes R, Paterno MV, Myer GD, Hewett TE. Neuromuscular training improves performance on the star excursion balance test in young female athletes. J Orthop Sports Phys Ther 2010;40:551–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Hoch MC, Staton GS, McKeon PO. Dorsiflexion range of motion significantly influences dynamic balance. J Sci Med Sport 2011;14:90–2. [DOI] [PubMed] [Google Scholar]
- 28. Gordon AT, Ambegaonkar JP, Caswell SV. Relationships between core strength, hip external rotator muscle strength, and star excursion balance test performance in female lacrosse players. Int J Sports Phys Ther 2013;8:97–104. [PMC free article] [PubMed] [Google Scholar]
- 29. Gribble PA, Hertel J, Plisky P. Using the Star Excursion Balance Test to assess dynamic postural control deficits and outcomes in lower extremity injury: A literature and systematic review. J Athl Train 2012;47:339–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Gribble PA, Hertel J. Considerations for normalizing measures of the star excursion balance test. Meas Phys Educ Exerc Sci 2003;7:89–100. [Google Scholar]
- 31. Pearson D, Faigenbaum A, Conley M, Kraemer WJ. The national strength and conditioning association’s basic guidelines for the resistance training of athletes. Strength Cond J 2000;22:14–27. [Google Scholar]
- 32. Robinson R, Gribble P. Kinematic predictors of performance on the star excursion balance test. J Sport Rehabil 2008;17:347–57. [DOI] [PubMed] [Google Scholar]
- 33. Earl JE, Hertel J. Lower-extremity muscle activation during the star excursion balance tests. J Sport Rehabil 2001;10(2):93–104. [Google Scholar]
- 34. Roy AL, Keller TS, Colloca CJ. Posture-dependant trunk extensor EMG activity during maximum isometrics exertions in normal male and female subjects. J Electromyogr Kinesiol 2003;13:469–76. [DOI] [PubMed] [Google Scholar]