

Abstract
Purpose.
Despite life-saving potential, many women struggle to adhere to adjuvant endocrine therapy (AET) for their breast cancer (BCa). Prior research has demonstrated that emotional distress is a barrier to AET adherence. We followed women from a trial to test the long-term effects of two 5-week post-surgical group-based stress management interventions, cognitive behavioral therapy (CBT) and relaxation training, versus an attention-matched health education control, on AET adherence.
Methods.
We conducted a long-term follow-up (median=8 years) of women randomized to CBT, relaxation training, or health education after surgery for stage 0–3 BCa. We measured adherence with the Endocrine Therapy Medication Usage Questionnaire (ETMUQ). First, we established factors on the ETMUQ via confirmatory factor analysis. We then used Bayesian structural equation modeling to regress these factors on study arm, controlling for age and treatments received.
Results.
Of those who completed long-term follow-up (N=59, 44.7%); over half (n=33; 55.9%) reported problems with adherence generally. Women receiving relaxation training (n=15) had better adherence than those receiving health education (n=24) on the Forgetfulness/Inconsistency (B(SE)=.25(.14), p=.049) and Intentional Nonadherence (B(SE)=.31(.14), p=.018) factors of the ETMUQ. Similar results were observed for those receiving relaxation training compared to CBT (N=20): Forgetfulness/Inconsistency (B(SE)=-.47(.25), p=.031); Intentional Nonadherence (B(SE)=-.31(.15), p=.027).
Conclusion.
Women receiving relaxation training were less likely to 1) forget to take their AET and 2) intentionally miss doses of AET in the long-term compared to women receiving health education or CBT. This is evidence for the need of randomized trials that aim to improve adherence by incorporating theoretically based behavioral change techniques.
Keywords: Endocrine therapy, adherence, behavior change, psycho-oncology, breast cancer
Introduction
Breast cancer remains a significant and deadly disease in the U.S., and despite advancements in treatment, 1 in 39 women still die from the disease[1]. Adjuvant endocrine therapy (AET) is an effective treatment for the 80% of women with early-stage disease who have hormone receptors for estrogen or progesterone expressed in their tumor[2]. Importantly, non-adherence has been associated with early mortality[3]. Despite life-saving potential, approximately half of women with hormone-receptor positive, early-stage breast cancer do not complete the recommended 10-year course of AET[4, 5].
Adherence can be defined as the level of conformity to prescribed treatment relating to frequency, dosage, and timing[6]. Prior research has elucidated several barriers to AET adherence, including side effects[7, 8], provider relationships[9], perceptions of recurrence risk[10], anxiety[8], depression[11, 12], poor social support[13], and psychological distress[10, 14]. The psychosocial barriers to adherence are persistent and may be related to distress post-diagnosis[15], AET as a daily reminder of cancer[16], ongoing fears of cancer recurrence[16, 17] and distress related to symptoms and side effects[7, 8, 16]. The value of mitigating distress to improve AET adherence has not yet been fully explored.
Psychosocial distress is a primary target of Cognitive-Behavioral Stress Management (CBSM), a group-based intervention for women with newly diagnosed breast cancer and encompasses relaxation training and cognitive-behavioral therapy (CBT). Ten-week CBSM has show to decrease distress (depressive symptoms, negative affect) in women with breast cancer[18, 19] during treatment and over the long-term (5-year and 11-year median follow-up)[20, 21]. We developed a briefer 5-week group-based version of CBT and relaxation training, based on the original CBSM protocol, and compared them to a 5-week group-based health education control[22]. The initial trial results testing these brief interventions showed improvements in depressive affect, emotional well-being, and stress management skills[22], as well as improvements in inflammatory markers[23, 24], in the two intervention conditions compared to the health education control.
Given that psychological distress is related to poorer AET adherence, and previous evidence that brief CBT and relaxation training effectively target distress, the present study examined whether these brief stress management interventions influenced AET adherence behaviors in the long-term. We examined AET adherence at 8-year follow-up of the women in this trial who were hormone receptor positive and receiving AET in a post-hoc analysis. We hypothesized that women randomized to CBT or relaxation training would show greater adherence versus those assigned to health education while controlling for age and adjuvant treatments received (chemotherapy/radiation).
Methods
Participants
The cohort for the current study consisted of women who participated in a randomized controlled trial of stress management at the University of Miami from 2006–2014. The parent trial was approved by the Institutional Review Board and is registered as National Institutes of Health Clinical Trial NCT02103387. All women participating in the study completed informed consent procedures.
We recruited women ages 21–75 with stages 0–3 cancer who were 2–10 weeks post-surgery from cancer clinics in South Florida. Exclusion criteria were metastatic disease, severe mental illness, a previous diagnosis of cancer, having already started adjuvant treatment, and lack of fluency in English. For this analysis, we examined only women who were prescribed AET.
Procedures from Parent Study
Participants completed psychosocial questionnaires at baseline prior to randomization (T1), post-intervention (T2), 6-months post-baseline (T3), 12-months post-baseline (T4). At baseline, demographic and medical information was collected by self-report, and was verified through chart review. For the purposes of this study, we followed-up with participants at 8-years post-baseline (T5) for an additional psychosocial questionnaire.
Study Conditions from Parent Study
We conducted all three study interventions in groups of 3–7 participants that met for 1.5 hours weekly for 5 weeks. Group facilitators were pre-doctoral students in the Clinical Psychology Ph.D. program at the University of Miami who were trained on the intervention protocols. We video-recorded all intervention sessions and conducted weekly supervision sessions with a licensed psychologist to maintain fidelity. Intervention session attendance was high across all 3 groups, with median attendance of 4 out of 5 sessions and no significant differences across the different interventions (F(2, 98)=1.87, p=.25).
CBT:
The CBT intervention comprised the cognitive-behavioral components of CBSM[25]. The intervention aimed to use CBT techniques to teach adaptive coping skills and improve social support, with an emphasis on cancer-related stressors. Throughout the five weeks, women receiving CBT were taught stress awareness, cognitive restructuring, coping effectiveness training, and interpersonal skills for utilizing social support such as anger management, and assertiveness training. At-home assignments were given for additional practice of CBT skills.
Relaxation Training:
We modeled the relaxation training intervention after the relaxation component of CBSM. The intervention aimed to reduce anxiety by teaching relaxation techniques through weekly in-session exercises including abdominal breathing, progressive muscle relaxation, guided imagery, and meditation. In addition, we provided rationale and psychoeducation on the relaxation response, the benefits of relaxation, and justification for each technique taught. Audio recordings of the exercises were given to participants to practice at home.
Health Education:
The health education intervention served as the time and attention-matched control. The intervention consisted of educational information related to a diagnosis of breast cancer, including symptom management, available treatment, resources, and healthy lifestyle choices. The health education groups received no information on stress management, relaxation, or medication adherence.
Procedures for the Follow-up Study
We recontacted women who participated in the parent study 8 years after their initial baseline assessment. Participants completed a psychosocial battery similar to the one they completed at baseline with the addition of adherence measures. Study staff administering the psychosocial batteries were blind to original treatment assignment of the participants.
Measures
AET Adherence.
We collected AET adherence data from women with hormone-receptor positive breast cancer by self-report. As there is currently no gold standard measure of AET adherence, our team created the Endocrine Therapy Medication Usage Questionnaire (ETMUQ) (Appendix). The ETMUQ was partially adapted from the AIDS Clinical Trials Group questionnaire[26], a well-validated measure of adherence to antiretroviral therapy. The ETMUQ measures either current or past long-term adherence with 7 questions related to frequency experienced (i.e., “How often do you/did you forget to take your endocrine therapy?”). After completion of data collection, we ran a Bayesian confirmatory factor analysis (CFA) of 7 frequency questions in the ETMUQ to determine whether the measure adequately captured both intentional nonadherence and forgetfulness as related but distinct constructs. We then tested the composite reliability of the valid subscales that emerged, per factor analysis convention[27], and these latent variables were used as adherence outcome scores.
Covariates:
Covariates for behavioral outcomes included age and adjuvant treatments received (chemotherapy and/or radiation). These variables were collected in the initial psychosocial questionnaire (at enrollment) and verified with medical chart review. Covariates were selected based on previous literature suggesting a role in medication-taking behaviors[5, 28, 29] and because of their theoretical implications for both intentional nonadherence (i.e., burden of side effects, perception of risk)[5, 29] and forgetfulness/inconsistency (i.e., cognitive deficits)[30], the two factors of interest for the current study. In addition to these covariates, household income, race/ethnicity, and stage at diagnosis were assessed as predictors of long-term follow-up response.
Analytic Plan
We initially screened data for outliers, normality, and homoscedasticity, and no influential outliers were observed. One item (#11) on the ETMUQ had high skewness (>3), and another had 0 variability (#12) and were subsequently excluded from all analyses. All other variables were within acceptable ranges of skewness (<3) and kurtosis (<8) [31].
We used Bayesian structural equation modeling (BSEM) to estimate all models. BSEM combines structural equation modeling (SEM) and Bayesian estimation such that issues associated with low sample size use in SEM, including bias and low power, are addressed[32]. Model fit was evaluated based on the posterior predictive p-value (PPP), such that a PPP of approximately .50 and a 95% confidence interval symmetric around 0 indicates perfect fit. A PPP < .10 or > .90, or a positive lower posterior 95% confidence limit indicated poor model fit [33]. In the case of poor model fit, modification indices guided model re-specification (e.g., inclusion of a residual covariance).
We conducted a Bayesian CFA to determine the validity of the ETMUQ as well as the factor loadings, and then tested composite reliability (CR) (i.e., internal consistency) per factor analysis convention[27]. Finally, we added dummy-coded vectors of group predicting all emerging ETMUQ factors such that each comparison between interventions was tested (i.e., CBT versus health education, relaxation training versus health education, and CBT versus relaxation training) controlling for age, chemotherapy, and radiation.
Results
Overall, 739 women were assessed for eligibility, 194 women were eligible and interested and signed informed consent, and 184 women completed baseline prior to randomization. Of these, 135 (73.8%) were prescribed AET. At the 8-year follow-up, 59 completed the psychosocial battery with 20 of those in the CBT arm, 15 in relaxation training, and 24 in health education. See Figure 1 for the CONSORT flow diagram.
Fig. 1.
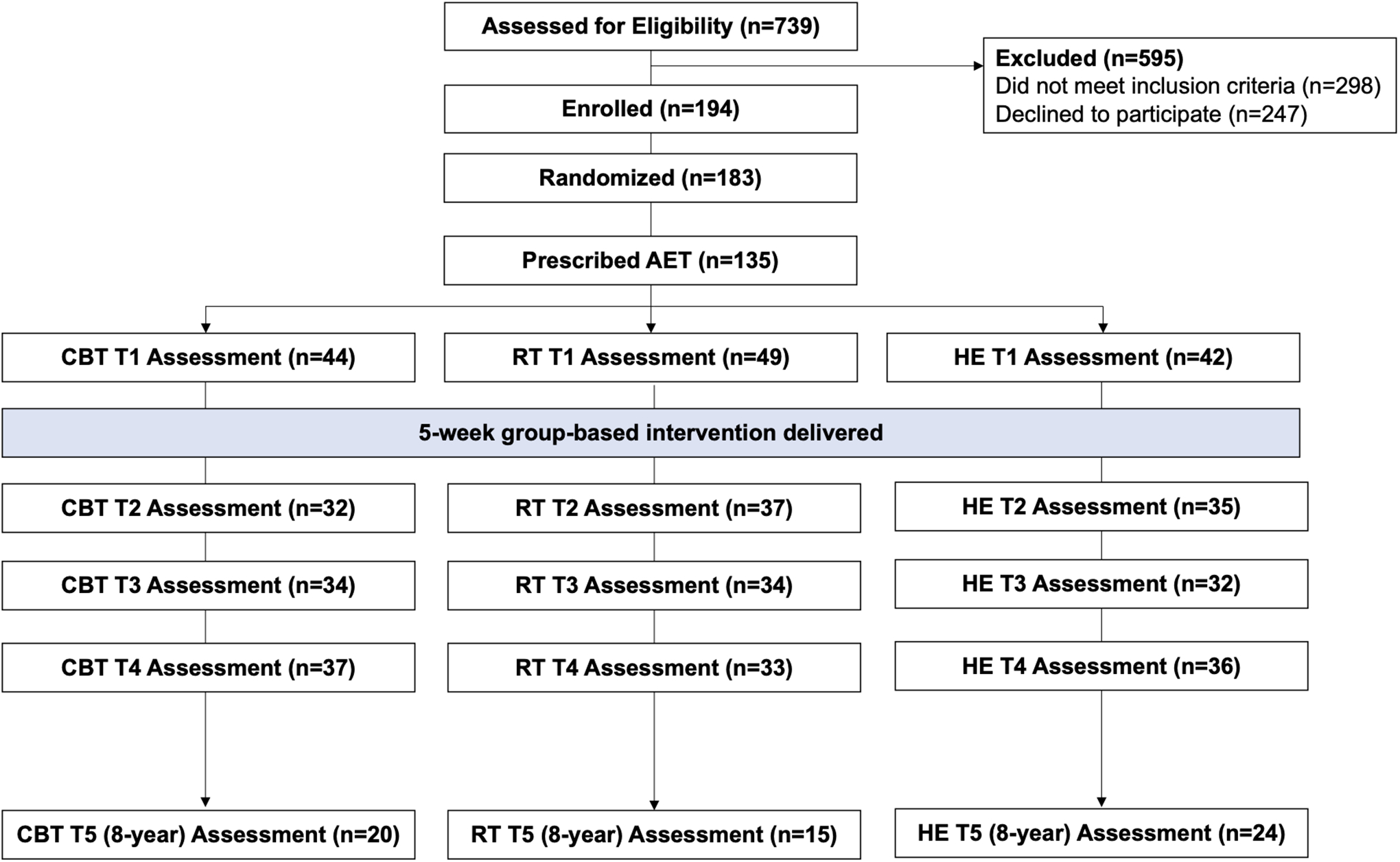
CONSORT Flow Diagram
Descriptive Statistics
The sample was predominately middle-aged (M=54.81 years, SD=10.19), Hispanic (42.2%) and White (41.5%), partnered (62.2%) with stage 1 (57.0%) or stage 2 (25.9%) disease. Complete demographic and prognostic descriptive statistics by study condition can be found in Table 1. There was an effect of income (F(1, 115)=8.15, p=.01) and condition (χ2(2) = 6.55, p = .040) on the likelihood of completing long-term follow-up (Table 2).
Table 1.
Baseline Medical and Demographic Variables by Group Condition (n=135)
| Variable | CBT (n=44) | Relaxation Training (n=49) | Health Education (n=42) | Test Statistic | P |
|---|---|---|---|---|---|
| Age at diagnosis (years) | 54.84 (9.00) | 54.08(12.12) | 55.64(9.00) | F(2,132) = 0.26 | 0.77 |
| Years Education | 16.09 (2.71) | 14.98 (3.30) | 15.46 (3.20) | F(2,128) = 1.47 | 0.23 |
| Household Income (thousands) | 99.58 (70.36) | 82.85 (62.94) | 137.30(166.96) | F(2,114) = 2.50 | 0.09t |
| Race/Ethnicity | χ2(6) = 7.25 | 0.30 | |||
| Non-Hispanic White | 21 (48.8%) | 16 (34.0%) | 19 (45.2%) | ||
| Hispanic | 16 (37.2%) | 25 (53.2%) | 16 (38.1%) | ||
| African-American | 3 (7.0%) | 2 (4.3%) | 6 (14.3%) | ||
| Other | 3 (7.0%) | 4 (8.5%) | 1 (2.4%) | ||
| Partnered at Diagnosis | 31 (72.1%) | 28 (59.6%) | 25 (59.5%) | χ2(2) = 1.97 | 0.37 |
| Stage at Diagnosis | χ2(6) = 1.64 | 0.95 | |||
| Stage 0 | 6 (13.6%) | 4 (8.2%) | 5 (11.9%) | ||
| Stage 1 | 26 (59.1%) | 27 (55.1%) | 24 (57.1%) | ||
| Stage 2 | 10 (22.7%) | 15 (30.6%) | 10 (23.8%) | ||
| Stage 3 | 2 (4.5%) | 3 (6.1%) | 3 (7.1%) | ||
| Positive Nodes | 6 (14.3%) | 14 (29.8%) | 13 (31.7%) | χ2(2) = 4.08 | 0.13 |
| Surgery | χ2(2) = 0.20 | 0.91 | |||
| Lumpectomy | 21 (47.7%) | 24 (49.0%) | 22 (52.4%) | ||
| Mastectomy | 23 (52.3%) | 25 (51.0%) | 20 (47.6%) | ||
| Hormonal Status | |||||
| ER positive | 40 (93.0%) | 45 (97.8%) | 360(94.7%) | χ2(2) = 1.17 | 0.56 |
| PR positive | 34 (82.9%) | 39 (84.8%) | 32 (88.9%) | χ2(2) = 0.57 | 0.75 |
| Days f/ Surgery to T1 | 34.05 (21.14) | 38.45 (24.75) | 37.43 (20.72) | F(2,132) = 0.48 | 0.62 |
| Received Radiation | 23 (52.3%) | 21 (45.7%) | 24 (58.5%) | χ2(2) = 1.45 | 0.49 |
| Received Chemo | 15 (34.1%) | 20 (41.7%) | 13 (31.7%) | χ2(2) = 1.07 | 0.59 |
note. CBT = Cognitive Behavioral Therapy; ER = Estrogen Receptor; PR = Progesterone Receptor.
p < 1.0,
p < .05,
p < .01,
p < .001
Table 2.
Group Assignment and Demographic Differences between Patients Who Completed versus Did Not Complete Long-Term (T5) Follow-up
| Variable | Completed (N=59) | Did Not Complete (N=76) | Test Statistic | p |
|---|---|---|---|---|
| Group Assignment | χ2(2) = 6.55 | .04* | ||
| CBT | 20 (33.9%) | 24 (31.6%) | ||
| Relaxation Training | 15 (25.4%) | 34 (44.7%) | ||
| Health Education | 24 (40.7%) | 18 (23.7%) | ||
| Stage at Diagnosis | χ2(3) = 1.88 | .60 | ||
| Stage 0 | 5 (8.5%) | 10 (13.2%) | ||
| Stage 1 | 33 (55.9%) | 44 (57.9%) | ||
| Stage 2 | 16 (27.1%) | 19 (25.0%) | ||
| Stage 3 | 5 (8.5%) | 3 (3.9%) | ||
| Race/Ethnicity | χ2(3) = 0.89 | .84 | ||
| Non-Hispanic White | 27 (46.6%) | 29 (39.2%) | ||
| Hispanic | 23 (39.7%) | 34 (45.9%) | ||
| African-American | 5 (8.6%) | 6 (8.1%) | ||
| Other | 3 (5.2%) | 5 (6.8%) | ||
| Income (thousands) | 137.37 (142.13) | 80.52 (66.94) | F(1, 115) = 8.15 | .01* |
| Age (years) | 54.17 (9.21) | 55.32 (10.92) | F(1, 133) = 0.42 | .52 |
note. CBT = Cognitive Behavioral Therapy.
p < 1.0,
p < .05,
p < .01,
p < .001
Of the 59 women reached for long-term follow-up, less than half (n=28, 47.5%) reported still taking their medication at 8-year follow-up. Of the 28 still taking the medication, the average number of doses missed in the past 30 days was 1.07 (SD=1.76, range=0–6). In addition, 33 of the 59 (55.9%) reported having at least some specific problems with adherence while taking the medication. In preliminary chi-square tests, we found a significant difference between groups in endorsing forgetfulness (χ2(2) = 6.53, p = .038) and in reporting any problems with adherence (χ2(2) = 6.36, p = .042), but no significant differences between groups in endorsing intentional nonadherence (χ2(2) = 2.10, p = .350) (Table 3). Reported reasons for nonadherence are depicted in Figure 2.
Table 3.
Rates of Adherence Problems in Long-Term per ETMUQ by Group Condition (n=59)
| Factor | CBT (n=20) | Relaxation Training (n=15) | Health Education (n=24) | Test Statistic | p |
|---|---|---|---|---|---|
| Forgetfulness/Inconsistency | χ2(2) = 6.53 | 0.04* | |||
| Not Endorsed | 8 (40.0%) | 12 (80.0%) | 11 (45.8%) | ||
| Endorsed | 12 (60.0%) | 3 (20.0%) | 13 (54.2%) | ||
| Intentional Nonadherence | χ2(2) = 2.10 | 0.35 | |||
| Not Endorsed | 13 (65.0%) | 13 (86.7%) | 18 (75.0%) | ||
| Endorsed | 7 (35.0%) | 2 (13.3%) | 6 (25.0%) | ||
| Any Adherence Problems | χ2(2) = 6.36 | 0.04* | |||
| Not Endorsed | 6 (30.0%) | 11 (73.3%) | 9 (37.5%) | ||
| Endorsed | 14 (70.0%) | 4 (26.7%) | 15 (62.5%) |
note. ETMUQ= Endocrine Therapy Medication Usage Questionnaire; CBT = Cognitive Behavioral Therapy.
p < 1.0,
p < .05,
p < .01,
p < .001
Fig. 2.
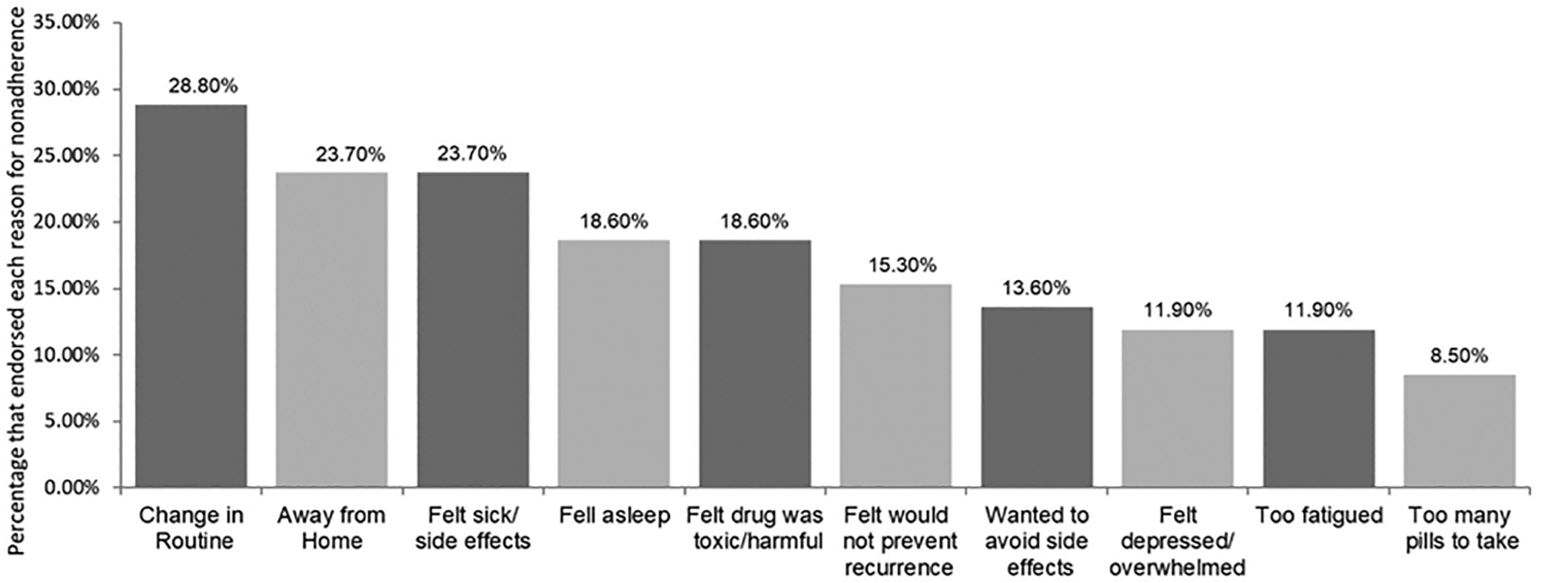
Distributions of self-reported reasons for non-adherence at 8-year follow-up
ETMUQ Validity and Reliability
A single factor CFA had poor fit to the data (PPP 95% CI [-4.72, 29.85], p =.056). A specified two-factor model fit the data well (PPP 95% CI [-15.26, 16.60], p =.452), with Factor 1 capturing “Forgetfulness/Inconsistency” and Factor 2 capturing “Intentional Nonadherence”. Both factors met acceptable values of composite reliability (Forgetfulness/Inconsistency CR=.70, Intentional Nonadherence CR=.81). See Supplemental Figure 1 for the factor loadings of the final CFA.
Intervention Effects on AET Adherence
First, two models were run such that effects of CBT versus health education on both adherence factors were tested controlling for covariates. The models assessing effects on Forgetfulness/Inconsistency (PPP 95% CI [−13.09, 36.89], p =.146) and Intentional Nonadherence (PPP 95% CI [−19.87, 26.11], p =.341) each had adequate fit to the data. There was no significant effect of group in predicting AET Forgetfulness/Inconsistency (B(SE) = −.20(.30), p =.346) nor AET Intentional Nonadherence (B(SE) = −.06(.14), p =.201). Among the covariates, there was a significant effect of radiation receipt (B(SE) = −.47(.13), p=.005) and of age (B(SE) = −.29(.09), p =.006) on Intentional Nonadherence, and of radiation receipt on Forgetfulness/Inconsistency (B(SE) = −.40(.25), p =.046), such that those who did not receive radiation were more likely to report greater Intentional Nonadherence and Forgetfulness/Inconsistency, and younger women were more likely to report greater Intentional Nonadherence.
Second, two models were run such that effects of relaxation training versus health education on both adherence factors were tested controlling for covariates. The models assessing effects on Forgetfulness/Inconsistency (PPP 95% CI [−18.99, 29.52], p=.349) and Intentional Nonadherence (PPP 95% CI [−11.43, 53.98], p=.122) each had adequate fit to the data. There was a significant effect of group in predicting AET Forgetfulness/Inconsistency (B(SE) = .25(.14), p =.049) and AET Intentional Nonadherence (B(SE) = .31(.14), p =.018), such that those who received relaxation training reported significantly better adherence on both factors than did those who received health education. Among the covariates, there was a significant effect of radiation receipt on Intentional Nonadherence (B(SE) = −.41(.14), p=.006), and of age on Forgetfulness/Inconsistency (B(SE) = .15(.16), p =.001), such that those who did not receive radiation were more likely to report greater Intentional Nonadherence, and younger women were more likely to report greater Forgetfulness/Inconsistency.
Finally, two models were run such that effects of CBT versus relaxation training on both adherence factors were tested controlling for covariates. The models assessing effects on Forgetfulness/Inconsistency (PPP 95% CI [−23.43, 26.67], p=.448) and Intentional Nonadherence (PPP 95% CI [−25.79, 32.90], p=.444) each had good fit to the data. There was a significant effect of group in predicting AET Forgetfulness/Inconsistency (B(SE) = −.47(.25), p =.031) and AET Intentional Nonadherence (B(SE) = −.31(.15), p =.027), such that those who received relaxation training reported significantly better adherence on both factors than did those who received CBT. Among the covariates, there was a significant effect of radiation receipt on Intentional Nonadherence (B(SE) = −.37(.14), p=.014), and Forgetfulness/Inconsistency (B(SE) = −.50(.23), p=.031), such that those who received radiation were more likely to report better adherence on both factors. See Table 4 for a summary of model fit and parameter estimates of all BSEM intervention effect models.
Table 4.
Model Fit and Parameter Estimates of Intervention Effects using Bayesian SEM
| Model Fit Statistics | Estimates of Intervention Effects | |||||
|---|---|---|---|---|---|---|
| No. of Free Parameters | 95%CI for difference of Chi-square values | PPP | B | Posterior SD | p-value | |
| CBT v. Health Education | ||||||
| Intentional Nonadherence | 19 | [−19.87, 26.12] | .341 | −.06 | .14 | .33 |
| Forgetfulness/Inconsistency | 19 | [−13.08, 36.89] | .146 | −.20 | .30 | .20 |
| Relaxation Training v. Health Education | ||||||
| Intentional Nonadherence | 19 | [−11.43, 53.94] | .122 | .31 | .14 | .02* |
| Forgetfulness/Inconsistency | 19 | [−18.99, 29.52] | .349 | .25 | .14 | .05* |
| CBT v. Relaxation Training | ||||||
| Intentional Nonadherence | 19 | [−25.80, 32.90] | .444 | −.31 | .15 | .03* |
| Forgetfulness/Inconsistency | 19 | [−23.43, 26.67] | .448 | −.47 | .25 | .03* |
note. CBT = Cognitive Behavioral Therapy; PPP= Posterior p-value.
p < 1.0,
p < .05,
p < .01,
p < .001
Discussion
The present study examined whether brief stress management interventions delivered in the post-surgical period influenced AET medication adherence behaviors in the long-term. Less than half of women in the current trial persisted with their AET medication at 8-year follow-up. Moreover, over half of the women reported at least some specific problems with adhering to their medication. This is consistent with prior literature suggesting that adherence declines over time[4, 5].
This trial demonstrated that participation in relaxation training was associated with better long-term adherence. This is evidence for the need of future interventions that aim to improve AET adherence by incorporating theoretically based behavioral change techniques[34, 35]. To date, the majority of interventions studied have consisted of written educational materials and reminder systems in the form of telephone calls and/or mailed letters; and no such interventions have proved efficacious[36–40]. This is consistent with our finding that health education did not improve adherence as compared to relaxation training. Although women in the health education condition received direct information regarding symptom management, the evidence of previous trials suggests that one-way communication is not sufficient for behavior change in AET adherence[36–40].
Future work should investigate the mechanisms by which relaxation training may improve adherence. It is plausible that relaxation training, which involves training in physical and psychological relaxation, is an effective coping mechanism for AET-related side effects. Given that 90% of women on AET experience somatic side effects[41], learning skills to relax the body, such as progressive muscle relaxation and diaphragmatic breathing, may improve physical well-being and decrease rates of non-persistence and non-adherence by decreasing some of these side effects or improving self-efficacy for symptom management. This is especially true given that the burden of physical side effects is consistently linked to worse AET adherence[8, 14, 28, 42–46]. In addition, it is possible that mindfulness-based skills, another focus of our relaxation training condition, improve attention and awareness[47], thereby decreasing forgetfulness and inconsistency with AET adherence.
In assessing the intervention effects on self-reported adherence, effects emerged among covariates of age and radiation. Specifically, younger women and those who received radiation were more likely to report greater levels of nonadherence. This is consistent with previous research that demonstrated women at the age extremes demonstrate the worst adherence [5, 28]. Less research has investigated the role of adjuvant treatment type (i.e., chemotherapy and/or radiation) in predicting adherence to AET, although there is some evidence that receiving either chemotherapy or radiation is related to better adherence [29]. It is plausible that there is an underlying construct that promotes a patient to both adhere to their AET medication and decide to undergo radiation treatment for their breast cancer. Specifically, it could be the case that an optimal level of anxiety relating to recurrence risk motivates women to decide to receive radiation and be adherent to AET, with too low anxiety leading to a lack of motivation and too high anxiety causing women to decline or be nonadherent to treatment. This may be an explanation for inconsistent results in the literature linking anxiety to adherence [8, 29, 48].
There are several limitations of the current analysis to consider when interpreting findings. First, there may have been a degree of selection bias to participate in the voluntary clinical trial, such that the sample may not be clinically generalizable. In addition, the study is limited in the use of a self-report, non-validated measure of AET adherence. Self-report measures are at risk of response and recall bias, which is especially true for this analysis given that the ETMUQ assessed both current and past adherence, and many women were reporting on adherence from years prior. However, prior work has demonstrated that most women show concordance on self-reported and objective (electronic pill bottle) AET adherence measures[49]. Also, factor analysis was utilized to establish the validity of the two factors emerging from the ETMUQ, and construct reliability was adequate on both factors. We also note that there was a significant difference across groups in long-term response rates, with those receiving relaxation training responding less than those receiving CBT and health education. It is therefore plausible that those patients in the relaxation training group who did respond differed in adherence from those who did not, impacting our results. However, there was a stronger effect of income on response rates, and at baseline patients in relaxation training also had significantly lower income than other groups, which may explain the lower response rates within this group.
The study is also limited in that there was a significant drop-off in assessment completion between T4 and T5 (8-year follow-up), such that only 59 of the 135 women completed the T5 assessment. This retention was expected due to a combination of morbidity/mortality and loss-to-follow-up, and was similar to retention rates observed in previous long-term follow-up studies[21]. However, factors influencing response rates may further bias the findings. We did not adjust for multiple comparisons given that these were planned and complementary comparisons; however, we recommend caution in interpreting these findings given our small sample size and encourage further testing of these hypotheses in a larger, well-powered cohort.
This analysis adds to the literature by demonstrating that relaxation training may have some impact on AET self-reported adherence in the long-term. Only a small number of trials to improve AET adherence have been conducted[36–40] and most neglect to incorporate theoretically based intervention components for behavior change. Current trials are underway that are attempting to bridge this gap and incorporate evidence-based techniques[34, 35]. For example, one is testing the ability of a psychosocial intervention that incorporates relaxation training and other evidence-based psychological treatments with adherence counseling on AET adherence[34, 35]. Interventions that integrate psychological treatment to lower the volume of distress and provide specific adherence counseling have demonstrated efficacy in improving adherence and depression in other disease groups, including HIV[50] and type 2 diabetes[51]. Given the results of the current analyses, such trials for AET adherence are important to determine whether psychological intervention with adherence counseling is more effective than psychological treatment alone, as has been demonstrated within the HIV literature[52, 53]. A future large-scale, prospective randomized trial testing the impact on AET adherence of integrated relaxation training plus adherence counseling would give further insight into the efficacy of this intervention.
Over half of women with early stage, hormone-receptor positive breast cancer had difficulties adhering and persisting to AET in the long-term. There was a significant effect of stress management on self-reported adherence, such that women receiving brief relaxation training had significantly lower levels of Forgetfulness/Inconsistency and Intentional Nonadherence as opposed to women who received time-matched brief cognitive-behavioral therapy or health education. Future research should investigate whether relaxation training improves a patients’ self-efficacy to cope with the somatic symptoms related to AET adherence or improves focused attention. These findings illustrate the potential value of psychosocial interventions to improve AET adherence in the long-term.
Supplementary Material
Acknowledgments and Funding Information
The parent study (2R01-CA-064710) and current project (F31CA254148-01) were funded by National Cancer Institute of the National Institutes of Health grant. Dr. Safren was supported by grant 9K24DA040489.
Funding:
The parent study was funded by National Cancer Institute of the National Institutes of Health grant 2R01-CA-064710, and the current project was funded by F31CA254148-01 for analyses. Dr. Safren was supported by grant 9K24DA040489.
Footnotes
Trial Registration and Dates: Trial 2R01-CA-064710 was registered March 26, 2006.
Conflicts of Interest/Competing Interests:
Dr. Michael Antoni is an inventor of the intellectual property used in the study. Dr. Antoni is also a compensated consultant for Blue Note Therapeutics and Atlantis Healthcare.
Ethics approval:
The parent trial was approved by the Institutional Review Board at the University of Miami and is registered as National Institutes of Health Clinical Trial NCT02103387. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate:
All women participating in the study completed informed consent procedures.
Availability of Data and Material:
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- 1.DeSantis CE, Ma J, Gaudet MM, et al. (2019) Breast cancer statistics, 2019. CA Cancer J Clin 69:. 10.3322/caac.21583 [DOI] [PubMed] [Google Scholar]
- 2.Konecny G, Pauletti G, Pegram M, et al. (2003) Quantitative association between HER-2/neu and steroid hormone receptors in hormone receptor-positive primary breast cancer. J Natl Cancer Inst 95:. 10.1093/jnci/95.2.142 [DOI] [PubMed] [Google Scholar]
- 3.Hershman DL, Shao T, Kushi LH, et al. (2011) Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res Treat 126:. 10.1007/s10549-010-1132-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chlebowski RT, Kim J, Haque R (2014) Adherence to endocrine therapy in breast cancer adjuvant and prevention settings. Cancer Prev. Res 7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Partridge AH, Wang PS, Winer EP, Avorn J (2003) Nonadherence to adjuvant tamoxifen therapy in women with primary breast cancer. J Clin Oncol 21:. 10.1200/JCO.2003.07.071 [DOI] [PubMed] [Google Scholar]
- 6.Wassermann J, Rosenberg SM (2017) Treatment Decisions and Adherence to Adjuvant Endocrine Therapy in Breast Cancer. Curr. Breast Cancer Rep 9 [Google Scholar]
- 7.Burstein HJ, Temin S, Anderson H, et al. (2014) Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American Society of Clinical Oncology clinical practice guideline focused update. J. Clin. Oncol 32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bender CM, Gentry AL, Brufsky AM, et al. (2014) Influence of patient and treatment factors on adherence to adjuvant endocrine therapy in breast cancer. Oncol Nurs Forum 41:. 10.1188/14.ONF.274-285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Given BA, Spoelstra SL, Grant M (2011) The Challenges of Oral Agents as Antineoplastic Treatments. Semin Oncol Nurs 27:. 10.1016/j.soncn.2011.02.003 [DOI] [PubMed] [Google Scholar]
- 10.Stanton AL, Petrie KJ, Partridge AH (2014) Contributors to nonadherence and nonpersistence with endocrine therapy in breast cancer survivors recruited from an online research registry. Breast Cancer Res Treat 145: 10.1007/s10549-014-2961-3 [DOI] [PubMed] [Google Scholar]
- 11.Lebovits AH, Strain JJ, Messe MR, et al. (1990) Patient noncompliance with self-administered chemotherapy. Cancer 65:. [DOI] [PubMed] [Google Scholar]
- 12.Mausbach BT, Schwab RB, Irwin SA (2015) Depression as a predictor of adherence to adjuvant endocrine therapy (AET) in women with breast cancer: a systematic review and meta-analysis. Breast Cancer Res. Treat 152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kroenke CH, Hershman DL, Gomez SL, et al. (2018) Personal and clinical social support and adherence to adjuvant endocrine therapy among hormone receptor-positive breast cancer patients in an integrated health care system. Breast Cancer Res Treat 170:. 10.1007/s10549-018-4774-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Demissie S, Silliman RA, Lash TL (2001) Adjuvant tamoxifen: Predictors of use side effects, and discontinuation in older women. J Clin Oncol 19:. 10.1200/JCO.2001.19.2.322 [DOI] [PubMed] [Google Scholar]
- 15.Burgess C, Cornelius V, Love S, et al. (2005) Depression and anxiety in women with early breast cancer: Five year observational cohort study. Br Med J 330:. 10.1136/bmj.38343.670868.D3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jacobs JM, Walsh EA, Park ER, et al. (2020) The Patient’s Voice: Adherence, Symptoms, and Distress Related to Adjuvant Endocrine Therapy After Breast Cancer. Int J Behav Med 27:. 10.1007/s12529-020-09908-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Clancy C, Lynch J, OConnor P, Dowling M (2020) Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: A qualitative evidence synthesis. Eur J Oncol Nurs 44:. 10.1016/j.ejon.2019.101706 [DOI] [PubMed] [Google Scholar]
- 18.Antoni MH, Wimberly SR, Lechner SC, et al. (2006) Reduction of cancer-specific thought intrusions and anxiety symptoms with a stress management intervention among women undergoing treatment for breast cancer. Am J Psychiatry 163:. 10.1176/ajp.2006.163.10.1791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Antoni MH, Lutgendorf SK, Blomberg B, et al. (2012) Cognitive-behavioral stress management reverses anxiety-related leukocyte transcriptional dynamics. Biol Psychiatry 71:. 10.1016/j.biopsych.2011.10.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stagl JM, Antoni MH, Lechner SC, et al. (2015) Randomized controlled trial of cognitive behavioral stress management in breast cancer: A brief report of effects on 5-year depressive. Heal Psychol 34:. 10.1037/hea0000125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stagl JM, Lechner SC, Carver CS, et al. (2015) A randomized controlled trial of cognitive-behavioral stress management in breast cancer: survival and recurrence at 11-year follow-up. Breast Cancer Res Treat 154:. 10.1007/s10549-015-3626-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gudenkauf LM, Antoni MH, Stagl JM, et al. (2015) Brief cognitive-behavioral and relaxation training interventions for breast cancer: A randomized controlled trial. J Consult Clin Psychol 83:. 10.1037/ccp0000020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Taub CJ, Lippman ME, Hudson BI, et al. (2019) The effects of a randomized trial of brief forms of stress management on RAGE-associated S100A8/A9 in patients with breast cancer undergoing primary treatment. Cancer 125:. 10.1002/cncr.31965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Diaz A, Taub CJ, Lippman ME, et al. (2021) Effects of Brief Stress Management Interventions on Distress and Leukocyte Nuclear Factor Kappa B Expression During Primary Treatment for Breast Cancer: a Randomized Trial. Psychoneuroendocrinology. 10.1016/j.psyneuen.2021.105163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Antoni MH (2004) Stress management intervention for women with breast cancer.
- 26.Chesney MA, Ickovics JR, Chambers DB, et al. (2000) Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: The AACTG Adherence Instruments. In: AIDS Care - Psychological and Socio-Medical Aspects of AIDS/HIV [DOI] [PubMed] [Google Scholar]
- 27.Hair JF, Black WC, Babin BJ, Anderson RE (2010) Multivariate Data Analysis. Vectors [Google Scholar]
- 28.Kahn KL, Schneider EC, Malin JL, et al. (2007) Patient centered experiences in breast cancer: Predicting long-term adherence to tamoxifen use. Med Care 45:. 10.1097/01.mlr.0000257193.10760.7f [DOI] [PubMed] [Google Scholar]
- 29.Llarena NC, Estevez SL, Tucker SL, Jeruss JS (2015) Impact of Fertility Concerns on Tamoxifen Initiation and Persistence. J Natl Cancer Inst 107:. 10.1093/jnci/djv202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kovalchuk A, Kolb B (2017) Chemo brain: From discerning mechanisms to lifting the brain fog—An aging connection. Cell Cycle 16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Klein RB (2016) Principles and Practice of Structural Equation Modeling, Fourth Edition. Guilford Press; 8: [Google Scholar]
- 32.Kaplan D, Depaolo S (2012) No Title. In: Hoyle RH (ed) Handbook of Structural Equation Modeling. Guilford Press [Google Scholar]
- 33.Garnier-Villarreal M, Jorgensen TD (2019) Adapting Fit Indices for Bayesian Structural Equation Modeling: Comparison to Maximum Likelihood. Psychol Methods. 10.1037/met0000224 [DOI] [PubMed] [Google Scholar]
- 34.Jacobs JM, Walsh EA, Rapoport CS, et al. (2020) Development and Refinement of a Telehealth Intervention for Symptom Management, Distress, and Adherence to Adjuvant Endocrine Therapy after Breast Cancer. J Clin Psychol Med Settings. 10.1007/s10880-020-09750-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Jacobs JM, Rapoport CS, Horenstein A, et al. (2021) Study protocol for a randomised controlled feasibility trial of a virtual intervention (STRIDE) for symptom management, distress and adherence to adjuvant endocrine therapy after breast cancer. BMJ Open 11:. 10.1136/bmjopen-2020-041626 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ziller V, Kyvernitakis I, Knöll D, et al. (2013) Influence of a patient information program on adherence and persistence with an aromatase inhibitor in breast cancer treatment - the COMPAS study. BMC Cancer 13:. 10.1186/1471-2407-13-407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yu K Da, Zhou Y, Liu GY, et al. (2012) A prospective, multicenter, controlled, observational study to evaluate the efficacy of a patient support program in improving patients’ persistence to adjuvant aromatase inhibitor medication for postmenopausal, early stage breast cancer. Breast Cancer Res Treat 134:. 10.1007/s10549-012-2059-8 [DOI] [PubMed] [Google Scholar]
- 38.Hadji P, Blettner M, Harbeck N, et al. (2013) The patient’s anastrozole compliance to therapy (PACT) program: A randomized, in-practice study on the impact of a standardized information program on persistence and compliance to adjuvant endocrine therapy in postmenopausal women with early breast cancer. Ann Oncol 24:. 10.1093/annonc/mds653 [DOI] [PubMed] [Google Scholar]
- 39.Neven P, Markopoulos C, Tanner M, et al. (2014) The impact of educational materials on compliance and persistence rates with adjuvant aromatase inhibitor treatment: First-year results from the Compliance of ARomatase Inhibitors AssessmenT In Daily practice through Educational approach (CARIATIDE) study. Breast 23:. 10.1016/j.breast.2014.02.009 [DOI] [PubMed] [Google Scholar]
- 40.Ell K, Vourlekis B, Xie B, et al. (2009) Cancer treatment adherence among low-income women with breast or gynecologic cancer: A randomized controlled trial of patient navigation. Cancer 115:. 10.1002/cncr.24500 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Gupta P, Sturdee DW, Palin SL, et al. (2006) Menopausal symptoms in women treated for breast cancer: The prevalence and severity of symptoms and their perceived effects on quality of life. Climacteric 9:. 10.1080/13697130500487224 [DOI] [PubMed] [Google Scholar]
- 42.Friese CR, Pini TM, Li Y, et al. (2013) Adjuvant endocrine therapy initiation and persistence in a diverse sample of patients with breast cancer. Breast Cancer Res Treat 138:. 10.1007/s10549-013-2499-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kirk MC, Hudis CA (2008) Insight into barriers against optimal adherence to oral hormonal therapy in women with breast cancer. Clin Breast Cancer 8:. 10.3816/CBC.2008.n.016 [DOI] [PubMed] [Google Scholar]
- 44.Lash TL, Fox MP, Westrup JL, et al. (2006) Adherence to tamoxifen over the five-year course. Breast Cancer Res Treat 99:. 10.1007/s10549-006-9193-0 [DOI] [PubMed] [Google Scholar]
- 45.Liu Y, Malin JL, Diamant AL, et al. (2013) Adherence to adjuvant hormone therapy in low-income women with breast cancer: The role of provider-patient communication. Breast Cancer Res Treat 137:. 10.1007/s10549-012-2387-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Van Londen GJ, Donovan HS, Beckjord EB, et al. (2014) Perspectives of postmenopausal breast cancer survivors on adjuvant endocrine therapy-related symptoms. Oncol Nurs Forum 41:. 10.1188/14.ONF.660-668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Farb NAS, Anderson AK, Segal ZV. (2012) The mindful brain and emotion regulation in mood disorders. Can. J. Psychiatry 57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kyvernitakis I, Ziller V, Hars O, et al. (2014) Prevalence of menopausal symptoms and their influence on adherence in women with breast cancer. Climacteric 17:. 10.3109/13697137.2013.819327 [DOI] [PubMed] [Google Scholar]
- 49.Bright EE, Stanton AL (2019) Correspondence between objective and self-reported endocrine therapy adherence among women with breast cancer. Ann Behav Med 53:. 10.1093/abm/kay094 [DOI] [PubMed] [Google Scholar]
- 50.Safren SA, Bedoya CA, O’Cleirigh C, et al. (2016) Cognitive behavioural therapy for adherence and depression in patients with HIV: a three-arm randomised controlled trial. Lancet HIV 3:. 10.1016/S2352-3018(16)30053-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Safren SA, Gonzalez JS, Wexler DJ, et al. (2016) Erratum: A randomized controlled trial of cognitive behavioral therapy for adherence and depression (CBT-AD) in patients with uncontrolled type 2 diabetes (Diabetes Care (2014) 37 (625–633)). Diabetes Care 39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Pence BW, Gaynes BN, Adams JL, et al. (2015) The effect of antidepressant treatment on HIV and depression outcomes: Results from a randomized trial. AIDS 29:. 10.1097/QAD.0000000000000797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Tsai AC, Karasic DH, Hammer GP, et al. (2013) Directly observed antidepressant medication treatment and HIV outcomes among homeless and marginally housed HIV-positive adults: A randomized controlled trial. Am J Public Health 103:. 10.2105/AJPH.2011.300422 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.