

Abstract
Mindfulness interventions have been shown to improve several subcomponents of attention; however, the psychological mechanisms driving these improvements are unknown. Mindfulness interventions train individuals to monitor present moment experiences; while adopting an attitude of acceptance towards these experiences. We conducted a theoretically-driven randomized controlled trial to test the putative mechanisms of mindfulness training that drive improvements in attentional control. Participants were randomly assigned to one of three conditions: (i) Monitor & Accept (MA) training, a standard 8-week MBSR intervention that included cultivation of both monitoring and acceptance skills; (ii) Monitor Only (MO) training, a well-matched modified 8-week MBSR-adapted intervention that focused on monitoring skills only; or (iii) No Treatment (NT) control. Momentary attentional control was measured via ecological momentary assessment for three days at baseline and post-intervention. Trait attentional control was assessed at baseline and post-intervention using traditional self-report. Participants also completed a dichotic listening task to assess sustained attention at baseline and post-intervention. We found that MA and MO participants improved in momentary and trait attentional control (but not attention task performance) relative to NT participants. Analysis of indirect effects were consistent with the possibility that increased momentary attentional control partially accounts for MA/MO intervention-related increases in trait attentional control. This randomized controlled trial provides one of the first experimental tests of the mechanisms of mindfulness interventions that drive improvements in attention outcomes. These findings support the notion that present-focused monitoring skills training drives mindfulness intervention-related improvements in momentary attentional control, which in turn fosters greater trait attentional control.
Keywords: mindfulness, randomized controlled trial, ecological momentary assessment (EMA), attentional control, attention
During the past two decades, there has been considerable public and scientific interest in mindfulness meditation practices (Creswell, 2017). Most definitions of mindfulness used in contemporary research contexts (e.g., Bishop et al., 2004; Kabat-Zinn, 2009) include two primary components: (i) intentionally paying attention to monitor present moment experiences; and (ii) adopting an attitude of acceptance and nonjudgment towards these experiences. One domain thought to be improved by mindfulness meditation is attention, as mindfulness practices fundamentally involve maintaining focus on the present moment and shifting attention back to the present when it wanders (Bishop et al., 2004). Consistent with this possibility, earlier evidence suggests that mindfulness interventions are associated with improvements in several subcomponents of attention (e.g., Farb, Segal, & Anderson, 2012; Jha, Krompinger, & Baime, 2007; review by Chiesa, Calati, & Serretti, 2011).
The attention system consists of multiple networks that are thought to underlie different functions (Petersen & Posner, 2012; Posner & Petersen, 1990). One attentional network that may be improved by mindfulness meditation is attentional control – the capacity to voluntarily direct and shift the focus of attention (Derryberry & Reed, 2002). Attentional control facilitates the effective deployment of attention by allowing individuals to selectively attend to goal-relevant information and ignore potential distractions (Hopfinger et al., 2000). Impairments in attentional control have been implicated in clinical models as one potential mechanism linking anxiety with poorer cognitive performance (e.g., Attentional Control Theory; Eysenck & Derakshan, 2011). Similarly, other studies have found that greater attentional control is associated with better performance on task-based measures of cognitive control (Hallion et al., 2019).
Cross-sectional evidence suggests that greater trait mindfulness is associated with greater trait attentional control (Walsh, Balint, Smolira, Fredericksen, & Madsen, 2009). Similarly, there is also evidence that mindfulness interventions may improve trait attentional control relative to active comparator interventions such as cognitive behavioral therapy (Garland et al., 2017) and cognitive training (Walsh, Saab, & Farb, 2019). However, these earlier intervention studies have examined relatively small non-generalizable samples (e.g., undergraduates, Walsh et al., 2019; individuals with social anxiety disorder, Garland et al., 2017). No previous studies have examined whether mindfulness interventions can also improve attentional control among healthy community adults. Moreover, the active psychological mechanisms of mindfulness training interventions that drive improvements in attentional control also remain unknown.
Monitor and Acceptance Theory (MAT) is one recent mechanistic account which posits that the training of monitoring and acceptance skills are the primary psychological components of mindfulness interventions that play both distinct and synergistic roles in driving intervention-related improvements (Lindsay & Creswell, 2017). Within the context of MAT, monitoring is defined as maintaining ongoing awareness of present-moment sensory and perceptual experiences, while acceptance is defined as maintaining an attitude of non-judgment towards momentary internal and external experiences. Much of the experimental research to date testing MAT predictions has focused on the benefits of acceptance skills training for emotion regulation, stress reduction, and health outcomes (Chin et al., 2019; Lindsay, Chin, et al., 2018; Lindsay, Young, Smyth, Brown, & Creswell, 2018). No research to date has tested the MAT prediction that learning monitoring skills drives improvements in attentional outcomes, including attentional control. However, cross-sectional evidence suggests that self-reported monitoring skills are associated with better performance on task-based measures of attentional control (Moore & Malinowski, 2009). It is therefore possible that monitoring skills training may be a critical mechanism of mindfulness interventions that drives improvements in attentional control.
Another question unaddressed by previous research is whether changes in trait measures of attentional control are also mirrored by changes in momentary measures of attentional control in daily life. To this end, the use of Ecological Momentary Assessment (EMA) to measure momentary attentional control in real-world settings and contexts may be particularly informative. EMA is well-suited to assess dynamic processes (such as attentional control) because these measures employ a significantly shorter recall period than traditional self-report measures, thereby helping to minimize recall biases (Shiffman et al., 2008; Smyth & Stone, 2003; Solhan et al., 2009). During shorter recall periods, individuals may provide more accurate reports of their experiences because they are less likely to rely on heuristics about their typical states (Solhan et al., 2009). Previous studies have found only modest correlations between momentary and trait measures of the same psychosocial construct (e.g., Anestis et al., 2010; Solhan et al., 2009), supporting the notion that momentary and trait measures may provide unique insight into an underlying construct (Lindsay, Young, Brown, Smyth, & Creswell, 2019; Moore, Depp, Wetherell, & Lenze, 2016).
Finally, we also wanted to assess whether changes in momentary and trait attentional control were accompanied by improved performance on a task-based measure of sustained attention. MAT predicts that the training of monitoring skills is sufficient for improving performance on task-based measures of cognition (Lindsay & Creswell, 2017). Consistent with this possibility, earlier studies have reported improved performance on task-based measures of attention following three months of intensive meditation training (e.g., Lutz et al., 2009). Thus, we also tested the possibility that mindfulness training would be associated with improved performance on a dichotic listening task, an auditory task-based measure of selective sustained attention (Hillyard et al., 1973).
Here we report the results of a randomized controlled trial that aimed to elucidate the active psychological mechanism of mindfulness training that drives improvements in attentional control. To address this aim, we randomly assigned participants to either: (i) Monitor and Accept (MA) training, a standard 8-week Mindfulness-Based Stress Reduction (MBSR) training program that included both monitoring and acceptance skills; (ii) Monitor Only (MO) training, a modified but structurally equivalent intervention that focused on monitoring skills only; or (iii) a no treatment (NT) assessment-only control condition. Attentional control was assessed at baseline and post-intervention using both momentary and trait measures. Participants also completed a dichotic listening task to assess sustained attention at the baseline and post-intervention laboratory sessions. Following MAT’s predictions (Lindsay & Creswell, 2017), we hypothesized that MA and MO participants would improve in momentary attentional control, trait attentional control, and sustained attention task performance from baseline to post-intervention relative to NT participants. Additionally, this study aimed to explore the possibility that changes in momentary attentional control during daily life may precede and potentially drive improvements in trait attentional control. We therefore tested the secondary hypothesis that improvements in momentary attentional control would partially account for intervention-related improvements in trait measures of attentional control.
Methods
Participants
Participants were 137 stressed community adults between the ages of 18–67 (M=37 years1, SD=13.4). The sample was 67.2% female, 66.4% Caucasian, 15.3% African-American, 10.2% Asian, and 8.0% other ethnicities. Recruitment was conducted via participant registries, community advertisements, and mass emails to local organizations for a study testing 8-week training programs for stress reduction and well-being. Eligible participants for the parent study were fluent English-speaking smartphone owners (Android or iPhone) between the age of 18–70 years in good mental and physical health, who scored >5 on the 4-item Perceived Stress Scale (Cohen & Williamson, 1988; Cohen, Kamarck, & Mermelstein, 1983)2. Participant exclusion criteria included: chronic mental or physical disease (listed in online supplement); hospitalization in the past 3 months; medication use that interferes with HPA axis or immune system functioning; current oral contraceptive use; current pregnancy; current antibiotic, antiviral, or antimicrobial treatment; recreational drug use or excessive alcohol or tobacco use; and travel to countries on the CDC travel alert list in the past 6 months. Finally, individuals reporting significant experience with or daily practice of mindfulness meditation or related mind-body practices (defined as >2 times per week or >90 minutes of weekly practice) were also excluded. All participants provided written informed consent and all study procedures were approved by the Carnegie Mellon University IRB. Study data were collected at Carnegie Mellon University in Pittsburgh, Pennsylvania between August 2015 and November 2016. Recruitment was halted once the target sample size had been reached.
G*Power was used to calculate an a priori target sample size needed to test primary trial aims. These calculations were based upon previous 8-week mindfulness intervention studies typically demonstrating medium-large effect sizes (~η2=.06-.18) for both daily stress and stress-reactivity outcomes relative to no treatment (e.g., Creswell, Pacilio, Lindsay, & Brown, 2014). Using a two-tailed Type I error rate of .05, a desired power of .90, an estimated ICC for time of .6, and a design of 3 groups measured at 2 time points, the required calculated sample size for an omnibus test of primary study aims was 120.
We also used G*Power to calculate a post-hoc test of observed power. These calculations were based upon previous 8-week mindfulness intervention studies that have demonstrated small-medium effect sizes (Cohen’s f=.15-.20) for within-group changes in attentional control (e.g., de Bruin, van der Zwan, & Bögels, 2016). Using a two-tailed Type I error rate of .05, an estimated ICC for time of .6, a sample size of 137, and a design of 3 groups at 2 time points, the observed power for this study was greater than .90.
Interventions
Participants were randomly assigned to one of three study conditions: (i) 8-week Monitor & Acceptance (MA) MBSR training program; (ii) 8-week Monitor Only (MO) adapted-MBSR training program; or (iii) No Treatment control condition (NT). Briefly, MBSR is a standardized group-based program consisting of 8 weekly 2.5–3-hour sessions, 1 day-long retreat during the sixth week, and approximately 45 minutes of daily home practice of meditation and informal mindfulness in daily life (Kabat-Zinn, 1990). Home practice audio recordings were hosted on a commercial web platform which tracked the duration of time that participants spent listening to the recordings each day. These timestamps were used to assess participant compliance with home practice during the intervention period. Participants were not provided with additional compensation for home practice compliance.
The MA program adhered to the standard MBSR curriculum although the length of the sessions was shortened to 2 hours. The MO program, which also included 2-hour weekly sessions, was adapted from MBSR by emphasizing the concentration/observing aspects of MBSR and removing acceptance/non-judgment language and practices. The MA and MO programs were taught in counterbalanced order across study cohorts by a certified MBSR instructor and a qualified MBSR instructor (i.e., instructors alternated between interventions for each cohort), both of whom had completed teacher trainings through the University of Massachusetts Center for Mindfulness; one of the MBSR instructors was a co-investigator in this research who remained blind to study hypotheses and did not participate in data collection. The MO program was adapted from the standard MBSR curriculum by co-authors in consultation with a former senior teacher at the University of Massachusetts Center for Mindfulness (see Author Contributions and Acknowledgements) along with supporting mindfulness training sources (e.g., Foust, 2014; Goenka, 1994; Trungpa, 2003). The NT control group received minimal contact from study personnel during the intervention period, and completed all other study activities and assessments. Consistent with recent recommendation (Kechter et al., 2019), we provide additional information about treatment fidelity in the online supplementary material.
Monitor & Accept (MA; Standard MBSR program).
During each group session, an MBSR instructor leads guided mindfulness meditations intended to foster the ability to come into direct contact with, and monitor one’s current body sensations, mental images, emotions, and thoughts with an accepting, allowing attitude. As the sessions proceed, participants are invited to acknowledge their habitual reactions to stressful situations, eventually discovering that mindful awareness allows for additional choices in response to stress. Acceptance, or a non-judgmental, matter-of-fact attitude, is encouraged in the MA condition only. All class sessions and home practice audios include instructions for focusing on a perceptual object (e.g., sensations of breathing) and returning attention to it when the mind wanders, using language that encourages a gentle and accepting attitude towards psychological experiences, including mind-wandering. This attitudinal quality is also reinforced during instructor-led class discussions.
Monitoring, or focusing and returning attention, is included in the MA training program because developing this skill is an important building block for learning to regulate attention. During class activities, MA participants are encouraged to “invite in” experiences with curiosity and interest, and to adopt a non-judgmental and accepting attitude towards their monitored experiences regardless of whether they are positive, negative, or neutral. Participants attend a seven-hour retreat during the sixth week of MBSR that is focused on integrating and elaborating upon the mindfulness skills learned throughout the course. Finally, participants are asked to complete approximately 40–45-minutes of daily home practice six days per week during the eight-week course (4.0–4.5 hours of practice per week). Daily home practice consists of recordings from the classroom instructor guiding participants through meditations such as body scanning, mindful movement, and sitting meditation, as well as informal mindfulness practice during daily life.
Monitor Only (MO; Adapted from MBSR).
Monitoring, or training to sense into and observe one’s experience, is included in standard MBSR and in the MO condition of this project. Participants are taught to focus their attention on an aspect of their present moment experience, such as sensations of breathing or other body sensations. They are asked to notice when their attention wanders and return it to the direct perception of the focal sensory object, and to monitor their present moment experiences during guided activities. The MO adaptations of the MBSR program primarily consisted of 1) changes in language, and 2) emphasizing concentration practices, specifically regarding body awareness. Changes in language included avoiding use of the words: accept, acceptance, allow, being with, letting go of judgment, non-judgment, and instead referring to: direct perception, observe, monitor, return to the anchor (e.g., of breath sensation). Thus, acceptance language was not included in the MO class instruction or home practice audios, and was also avoided by the instructor as much as possible during group discussions. The MO program emphasized concentration and attention monitoring. One such practice consisted of anchoring attention to breath or other body sensation or sound in order to train attention to present moment experience. The MO program did not include some meditative practices that are typically included in standard MBSR, such as open awareness meditation without a focal object. Like MA, MO participants completed a retreat day and the same amount of guided home practice. As a conservative test of study hypotheses, it is important to note that although the language and practices associated with acceptance were excised as much as possible from MO, the teachers still embodied the acceptance and inclusion that are considered essential to cultivating a safe and effective learning environment for participants in the MBSR program. Moreover, focusing and returning attention can result in a greater sense of clarity and reduced distraction and distress, so it is also possible that some participants developed a more accepting attitude over time on their own as they continued to practice MO meditation.
No Treatment (NT).
Following randomization, NT participants were asked to return to their normal day-to-day routines until the end of the intervention period. NT control group received minimal contact from study personnel during the intervention period, and completed all other study activities and assessments. After the study had concluded, NT participants were provided with a list of community and online resources to support meditation practice.
Procedures
This study was a three-arm randomized controlled trial preregistered with Clinical Trials identifier NCT02502227. This manuscript reports pre-registered secondary (momentary attentional control, dichotic listening task performance) and other (trait attentional control, treatment expectancies) outcome measures from this trial. All outcome measures reported here remained unanalyzed until data collection was complete. This trial pre-registered the study design, outcomes, and measures. The primary hypothesis tested in this paper was stated explicitly in our MAT theory paper, written before this trial data was analyzed (Lindsay & Creswell, 2017). Minor discrepancies between the pre-registration and reported methods are reported in the online supplementary material.
Interested participants were screened for eligibility both via telephone and at an in-person baseline appointment by trained research assistants and staff. During this baseline appointment, eligible participants provided a dried blood spot sample, completed a questionnaire and task battery, and were oriented to the study’s schedule and activities. Participants then completed three consecutive days of pre-intervention EMA and daily diary assessments. Next, participants were randomized into one of three study conditions using a random number generator in a 3-3-2 randomization sequence generated by a study statistician who was not involved with participant enrollment (for every 8 participants randomized, 3 were assigned to Monitor & Accept, 3 to Monitor Only, 2 to No Treatment). To maintain allocation concealment, only essential study personnel (e.g., the MBSR instructors) had knowledge of participant allocation. All outcome assessors were blind to condition assignment. Following the 8-week intervention period, participants completed three consecutive days of post-intervention EMA and diary assessments before returning to the laboratory for a post-intervention appointment. At this appointment, condition-blind research staff directed participants as they provided a dried blood spot sample and completed a questionnaire and task battery. Finally, all participants were debriefed, informed of the study’s primary aims, and compensated for their participation.
To provide helpful context for interpreting these results, we briefly summarize other outcome measures from this dataset that have been reported in other publications: (i) MA training reduced momentary stress ratings compared to both MO training and NT control (Chin et al., 2019); (ii) MA training increased daily life positive affect relative to MO training and NT control; MA and MO training decreased daily life negative affect relative to NT control (Lindsay, Chin, et al., 2018); and (iii) MA or MO training did not reduce circulating levels of the inflammatory biomarker C-Reactive Protein (Villalba et al., 2019).
Measures.
Momentary attentional control was assessed prior to the baseline and post-intervention laboratory sessions using signal-prompted ecological momentary assessments five times daily for three days at baseline and three days at post-intervention. Momentary attentional control was assessed using two items (“Since the last survey, I’ve been having trouble focusing my attention” and “Since the last survey, I’ve been distracted by thoughts or events around me”). Responses were provided on a 1 (never) to 6 (almost always) scale, reverse-scored such that higher values indicate greater attentional control, and averaged to form a composite representing momentary attentional control (α=.863).
Trait attentional control was assessed via self-report at the baseline and post-intervention laboratory sessions using the 20-item Attentional Control Scale (ACS; Derryberry & Reed, 2002). The ACS asks participants to rate the frequency with which they have difficulty focusing their attention (e.g., “It’s very hard for me to concentrate on a difficult task when there are noises around.”) on a four-point scale ranging from 1 (almost never) to 4 (always). Responses are coded such that higher scores indicate greater attentional control and averaged to create an index of total trait attentional control (baseline α=.82, post-intervention α=.84). In addition, the ACS yields two subscale scores that represent different aspects of trait attentional control – focusing and shifting (Judah et al., 2014). The focusing subscale consists of seven items that are averaged to create a score for attentional focus (e.g., “When trying to focus my attention on something, I have difficulty blocking out distracting thoughts”) (baseline α=.81, post α=.79). The shifting subscale consists of five items that are also averaged (e.g., “I can become interested in a new topic very quickly when I need to”) (baseline α=.67, post α=.79).
Participants completed a dichotic listening sustained attention task at the baseline and post-intervention laboratory sessions (Tiitinen et al., 1993). During this task, participants were instructed to attend to tones presented in one ear (i.e., right ear for right-handed participants) and press a button each time that they detected a deviant tone. Importantly, participants were asked to ignore tones that were presented in the opposite ear. Participants completed four 5-minute blocks of 350 auditory stimuli (80 dB, 60 ms in duration). Each block contained 300 standard stimuli (dominant ear, 1000 Hz; non-dominant ear, 500 Hz) and 50 deviant stimuli (dominant ear, 1050 Hz; non-dominant ear, 475 Hz). The low and high tones were presented randomly for each ear. Task performance was assessed using a sensitivity measure (d’) that reflects the ability to correctly identify deviant stimuli (Swets et al., 1978). At the end of the task, participants were asked to indicate how distracted they felt during the dichotic listening task using a visual analog scale. Participants placed a slash mark on a bipolar, 140 mm line to indicate how distracted they felt during the task from 0 (Not at all) to 140 (Highly). We used the distance of the slash marks to create numerical values ranging from 0–100, such that higher values indicated greater self-reported distraction during the dichotic listening task.
Participants assigned to either the MA or MO MBSR conditions (n=107) completed the 6-item Credibility/Expectancy Questionnaire (CEQ; Devilly & Borkovec, 2000), which asked participants to rate the degree to which they believed the classes would be beneficial. This measure was included to ensure that any differences in how MA and MO training affected stress and non-judgmental perceptions were not due to differences in positive treatment expectancies (i.e., placebo effects). Responses across all six items were averaged to create a single value (α=.912). Treatment expectancy (CEQ) scores were not collected from the NT group because participants assigned to this condition did not receive any treatment.
To assess perceptions of non-judgment, participants were asked to indicate the degree to which they agreed that they had been judging as good or bad each of four domains since the previous assessment: (i) themselves; (ii) their thoughts and feelings; (iii) situations they were in or events that occurred; and (iv) other people they interacted with or thought about, on a six-point scale from 1 (strongly disagree) to 6 (strongly agree). Items assessing perceptions of non-judgment were adapted from existing trait mindfulness and acceptance scales (e.g., Baer, Smith, & Allen, 2004; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) and extended to include more general perceptions of non-judgment. Responses to all four items were reverse scored such that higher values indicated greater non-judgment and were averaged to create a single value representing overall non-judgment (α=.88).
Ecological momentary assessment.
EMA surveys were administered via participants’ personal smartphones using web-based Qualtrics software delivered through SurveySignal and MetricWire text links. Participants were prompted to complete five EMA surveys daily at quasi-random times each day (30 surveys total across the baseline and post-intervention periods). Text links were sent during each of five 2-hour blocks distributed between 9:00 am and 7:00 pm, with links expiring after 45 minutes. Although not reported here, participants were also prompted to complete daily diary assessments at 8:30 pm each day (6 daily diary assessments total across the baseline and post-intervention periods); links were sent at exactly 8:30 pm and remained active until 11:30 pm. Participants were trained to complete EMA assessments during the baseline study appointment. To encourage adherence, participants received $60 base compensation plus an additional maximum of $40 for compliance with the EMA protocols. At both baseline and post-intervention, EMA assessments began on a Wednesday and concluded on a Friday.
Data analysis
To assess changes in momentary attentional control, we used 3-level multilevel models nesting EMA observations (Level-1) within days (Level-2) within individuals (Level-3) to test for time (baseline, post-intervention) × condition (MA, MO, NT) differences using Stata’s mixed command. Multilevel models were fit using REML estimation with an identity covariance matrix. Time, condition, and the time × condition interaction were modeled as fixed effects. In addition, we also modeled observation number within day as a fixed effect to control for potential autocorrelation between consecutive measurements and to account for time of day. Random intercepts were included in the model for both participant and day of assessment.
To assess changes in trait attentional control, dichotic listening task performance, and self-reported distraction during the dichotic listening task, we used 2-level multilevel models nesting observations (Level-1) within individuals (Level-2) to test for a time (baseline, post-intervention) × condition (MA, MO, NT) interaction using Stata’s mixed command (Version 15.1, StataCorp, College Station, Texas). These models were fit using REML estimation with an identity covariance matrix. Time, condition, and the time × condition interaction were modeled as fixed effects, and a random intercept was included in the models for participant.
Finally, we used procedures recommended by Shrout and Bolger (2002) to test the hypothesis that intervention-related increases in momentary attentional control would account for intervention-related improvements in trait attentional control. First, average values for momentary attentional control were calculated separately for baseline and post-intervention momentary assessments. Next, the PROCESS macro for SPSS (Version 2.16.3; Hayes, 2017) was used to test the strength and significance of the hypothesized indirect effect using bias-corrected bootstrapped with 50,000 resamples. We tested for an indirect effect of intervention condition (dummy coded: NT=0, MA/MO=1) on post-intervention trait attentional control through momentary attentional control at post-intervention. These analyses controlled for baseline levels of momentary and trait attentional control in modeling both the dependent and mediator variables.
Results
Preliminary analyses
The preliminary analyses reported here (i.e., tests for randomization failure and condition differences in treatment expectancies) have been previously published (Chin et al., 2019; Lindsay, Chin, et al., 2018). Of the 137 randomized participants, 125 completed the post-intervention assessment, and 125 completed at least one post-intervention EMA survey (see CONSORT flow chart; Figure 1). Of the 107 individuals assigned to one of the 8-week MBSR classes, 98 completed the intervention (91.6%). Success of randomization on major demographic characteristics in the full randomized sample (N=137) was evaluated. There were no baseline differences across conditions in age, sex, race, or education (see Table 1). Baseline PSS scores also did not differ between groups, F(2,134)=.493, p=.612. There were also no condition differences in compliance with EMA protocols at baseline. Among the 125 participants who completed post-intervention EMA, there were also no condition differences in adherence to the EMA protocol at post-intervention. Overall, participants completed 69.2% of all possible EMA surveys across baseline and post-intervention.
Figure 1.
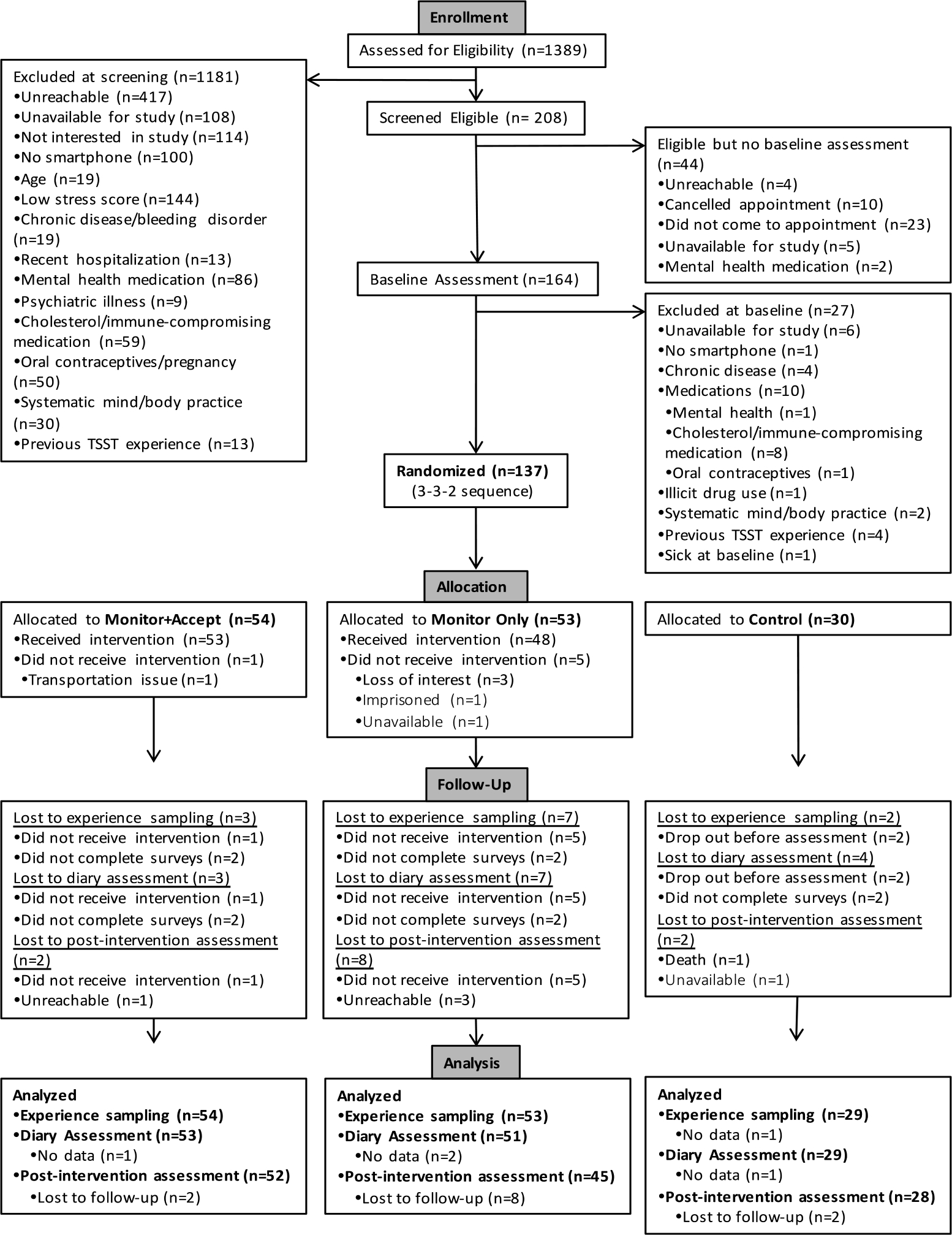
CONSORT flow chart of participant progress through phases of randomized controlled trial
Note. TSST = Trier Social Stress Test.
Table 1.
Baseline characteristics of participants (N=137) by study condition
| Characteristic | Full Sample (N=137)a | Monitor + Accept (N=54) | Monitor Only (N=53) | No Treatment (N=30) | Condition Difference |
|---|---|---|---|---|---|
|
| |||||
| Age in yearsb | 37.68 (13.43) | 36.02 (14.40) | 37.58 (12.60) | 40.83 (13.00) | F(2,133)=1.25 |
| Sex | χ2(2)=0.96 | ||||
| Female | 92 (67.15%) | 34 (62.96%) | 36 (67.92%) | 22 (73.33%) | |
| Male | 45 (32.85%) | 20 (37.04%) | 17 (32.08%) | 8 (26.67%) | |
| Race | χ2(8)=7.56 | ||||
| American Indian/Alaska Native | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (00.0%) | |
| Asian | 14 (10.22%) | 7 (12.96%) | 6 (11.32%) | 1 (3.33%) | |
| Black/African American | 21 (15.33%) | 10 (18.52%) | 7 (13.21%) | 4 (13.33%) | |
| White/Caucasian | 91 (66.42%) | 33 (61.11%) | 36 (67.92%) | 22 (73.33%) | |
| Bi- or Multi-Racial | 6 (4.38%) | 2 (3.70%) | 1 (1.89%) | 3 (10.00%) | |
| Other | 5 (3.65%) | 2 (3.70%) | 3 (5.66%) | 0 (0.00%) | |
| Ethnicity c | χ2(2)=1.70 | ||||
| Not Hispanic or Latino | 130 (95.59%) | 51 (94.44%) | 50 (94.34%) | 29 (96.67%) | |
| Hispanic or Latino | 6 (4.41%) | 3 (5.56%) | 3 (5.66%) | 0 (0.00%) | |
| Education Level | χ2(16)=11.18 | ||||
| No High School Diploma | 1 (0.73%) | 0 (0.00%) | 1 (1.89%) | 0 (0.00%) | |
| GED | 2 (1.46%) | 1 (1.85%) | 1 (1.89%) | 0 (0.00%) | |
| High School Diploma | 10 (7.30%) | 4 (7.41%) | 3 (5.66%) | 3 (10.00%) | |
| Technical Training | 2 (1.46%) | 0 (0.00%) | 1 (1.89%) | 1 (3.33%) | |
| Some College, no degree | 18 (13.14%) | 9 (16.67%) | 4 (7.55%) | 5 (16.67%) | |
| Associate Degree | 10 (7.30%) | 3 (5.56%) | 5 (9.43%) | 2 (6.67%) | |
| Bachelor’s Degree | 41 (29.93%) | 19 (35.19%) | 17 (32.08%) | 5 (16.67%) | |
| Master’s Degree | 40 (29.20%) | 12 (22.22%) | 17 (32.08%) | 11 (36.67%) | |
| MD, PhD, JD, PharmD | 13 (9.49%) | 6 (11.11%) | 4 (7.55%) | 3 (10.00%) | |
Note: Data are reported as means (SD) or percentages (%).
Of the 137 participants randomized, 12 did not complete the post-intervention assessment (8.8%). Those who dropped out did not differ in age (F(1,134)=0.20, p=.652), sex (χ2(1)=0.46, p=.496), race (χ2(4)=5.62, p=.229), or ethnicity (χ2(1)=0.48, p=.488). However, dropouts were more likely to have lower educational attainment (χ2(8)=21.25, p=.007).
Age missing from one participant in the Monitor Only condition (N=136).
Ethnicity missing from one participant in the No Treatment condition (N=136).
p<.05
Next, condition differences in treatment expectancies at Week 1, Week 4, and Week 8 of the intervention were tested using all available data from individuals assigned to one of the two study interventions (n=107). There was a main effect of time on treatment expectancies, F(2,174)=14.802, p<.001, such that all participants increased in treatment expectancies during the intervention (Week 1: M=6.50, SE=.17; Week 4: M=6.74, SE=.15; Week 8: M=7.50, SE=.14). However, there was no evidence for a Time × Condition (MA vs MO) interaction, F(2,174)=.003, p=.997, indicating that MA and MO participants did not differ in change over time. There were also no differences between the two training conditions in positive treatment expectancies at any time point (all ps>.53).
Condition differences in treatment adherence were also tested among the 98 individuals who completed their assigned intervention. There were no differences between the two training conditions in the number of classes attended. There was also no difference between the two training conditions in number of minutes of home practice4 (F(1,96)=2.97, p=.088) or number of home practice sessions (F(1,96)=1.72, p=.193). On average, MA participants completed 13.57 hours of home practice (SD=7.97; range: 0–29.94) across 27.1 sessions (SD=10.9, range: 0–42) whereas MO participants completed 10.72 hours of practice (SD=8.41; range: 0.02–26.31 hours) across 24.2 sessions (SD=10.5, range: 2–41) during the eight-week intervention.
As previously reported by Chin et al. (2019), condition differences in change in non-judgment over time were examined as a manipulation check for the experimental dismantling approach used in this study. It was hypothesized that MA training would increase non-judgment relative to both MO training and NT control. To test this hypothesis, 3-level MLMs were used to evaluate the hypothesized time by condition interaction. There was no main effect of condition (χ2(2)=4.90, p=.0865) but there was a main effect of time (χ2(1)=255.50, p<.0001). Consistent with predictions, this was qualified by an interaction between time and condition (χ2(2)=30.82, p<.0001). Participants across all conditions showed an increase in daily life non-judgmental perceptions from baseline to post-intervention (MA: 3.83(.12) to 4.58(.12), d=.88; MO: 3.64(.12) to 4.25(.12), d=.73; NT: 3.65(.17) to 3.92(.16), d=.31); however as predicted, this increase was significantly greater for MA participants compared to both MO (χ2(1)=4.40, p=.0360, d=.16) and NT participants (χ2(1)=30.82, p<.0001, d=.56). This increase was also significantly greater for MO participants compared to NT participants (χ2(1)=14.25, p=.0002, d=.39).
Momentary attentional control
Analysis of momentary attentional control showed a main effect of time across conditions (χ2(1)=112.49, p<.001), a main effect of condition across time (χ2(2)=10.86, p=.004), and a significant time × condition interaction (χ2(2)=7.99, p=.018) (see Figure 3). All participants increased in momentary attentional control from baseline to post-intervention (MA mean change=.46, p<.001, d=.57; MO mean change=.44, p<.001, d=.57; NT mean change=.21, p=.004, d=.27). Consistent with our primary hypothesis, both MA participants (χ2(1)=7.38, p=.007, d=.31) and MO participants (χ2(1)=5.87, p=.015, d=.29) had greater increases in momentary attentional control relative to NT participants, whereas MA and MO participants did not differ in the magnitude of this increase (χ2(1)=0.09, p=.767, d=.01) (see Table 2 for condition means).
Figure 3.
Changes in momentary attentional control from baseline to post-intervention by study condition
Note. *** = p<.001. ** = p<.01. Time × condition interaction: χ2(2)=9.69, p=.008. Momentary attentional control was assessed at baseline and post-intervention using signal-prompted ecological momentary assessment.
Table 2.
Momentary attentional control, trait attentional control, and dichotic listening task measures at baseline and post-intervention by study condition
| Outcome | Monitor + Accept (Pre and Post N=51) |
Monitor Only (Pre N=51; Post N=46) |
No Treatment Control (Pre N=26;Post N=28) |
Time x Condition Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | d | Pre | Post | d | Pre | Post | d | ||
|
| ||||||||||
| Trait AC | 2.43 (.06) | 2.79 (.06) | .84 | 2.42 (.06) | 2.69 (.06) | .64 | 2.40 (.08) | 2.46 (.08) | .14 | χ2(2)=9.69, p=.008 |
| Momentary ACa | 4.41 (.11) | 4.86 (.11) | .57 | 4.09 (.11) | 4.53 (.11) | .57 | 3.97 (.15) | 4.18 (.15) | .27 | χ2(2)=7.99, p=.018 |
| Task Performance | 2.80 (.20) | 2.94 (.20) | .10 | 2.85 (.20) | 3.11 (.21) | .18 | 2.28 (.26) | 2.58 (.27) | .22 | χ2(2)=0.48, p=.787 |
| Task Distraction | 36.24 (3.52) | 26.72 (3.64) | .37 | 37.97 (3.56) | 25.04 (3.88) | .50 | 34.38 (4.73) | 39.78 (5.10) | .21 | χ2(2)=7.53, p=.023 |
Note: Data are reported as means (SE) adjusted for observation number within day (coded 0–4). AC = attentional control. d = Cohen’s d effect size estimate.
There were not significant between-group differences in trait attentional control, task performance, or task distraction at baseline.
There were small between-group differences in momentary attentional control at baseline (χ2(2)=7.63, p=.022).
Trait attentional control
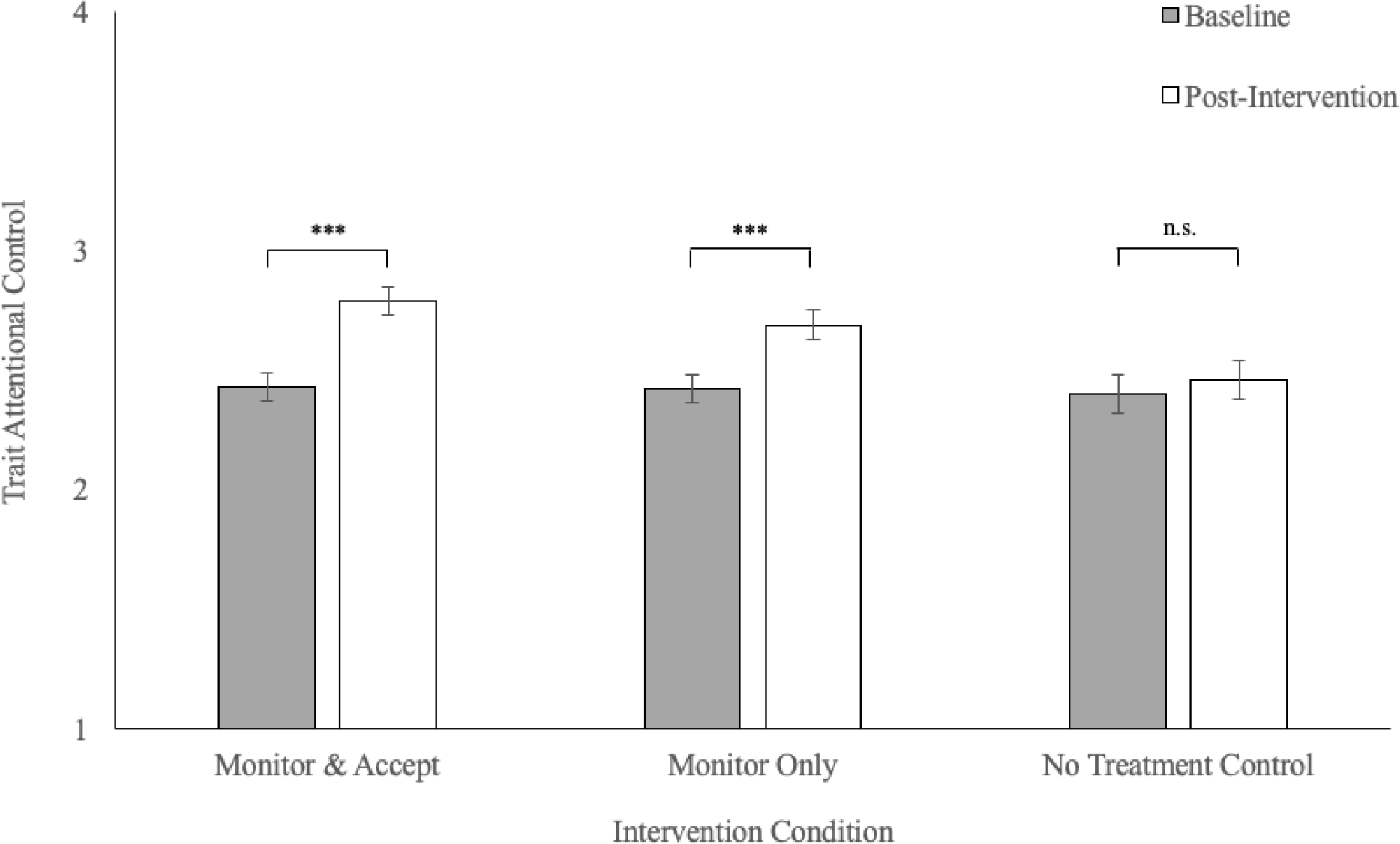
Analysis of trait attentional control scores showed a main effect of time across conditions (χ2(1)=38.57, p<.001), no effect of condition across time (χ2(2)=5.03, p=.081), and a significant time × condition interaction (χ2(2)=9.69, p=.008) (see Figure 2). Participants assigned to either mindfulness intervention increased in trait attentional control from baseline to post-intervention (MA mean change=.35, p<.001, d=.84; MO mean change=.27, p<.001, d=.64), whereas no treatment (control) participants did not change over time (NT mean change=.06, p=.410, d=.14). Consistent with our pre-registered primary hypothesis, both MA (χ2(1)=9.67, p=.002, d=.71) and MO participants (χ2(1)=4.54, p=.033, d=.49) increased in trait attentional control relative to NT participants, whereas MA and MO participants did not differ in magnitude of change over time (χ2(1)=1.19, p=.275, d=.21). (See Table 2 for condition means).
Figure 2.
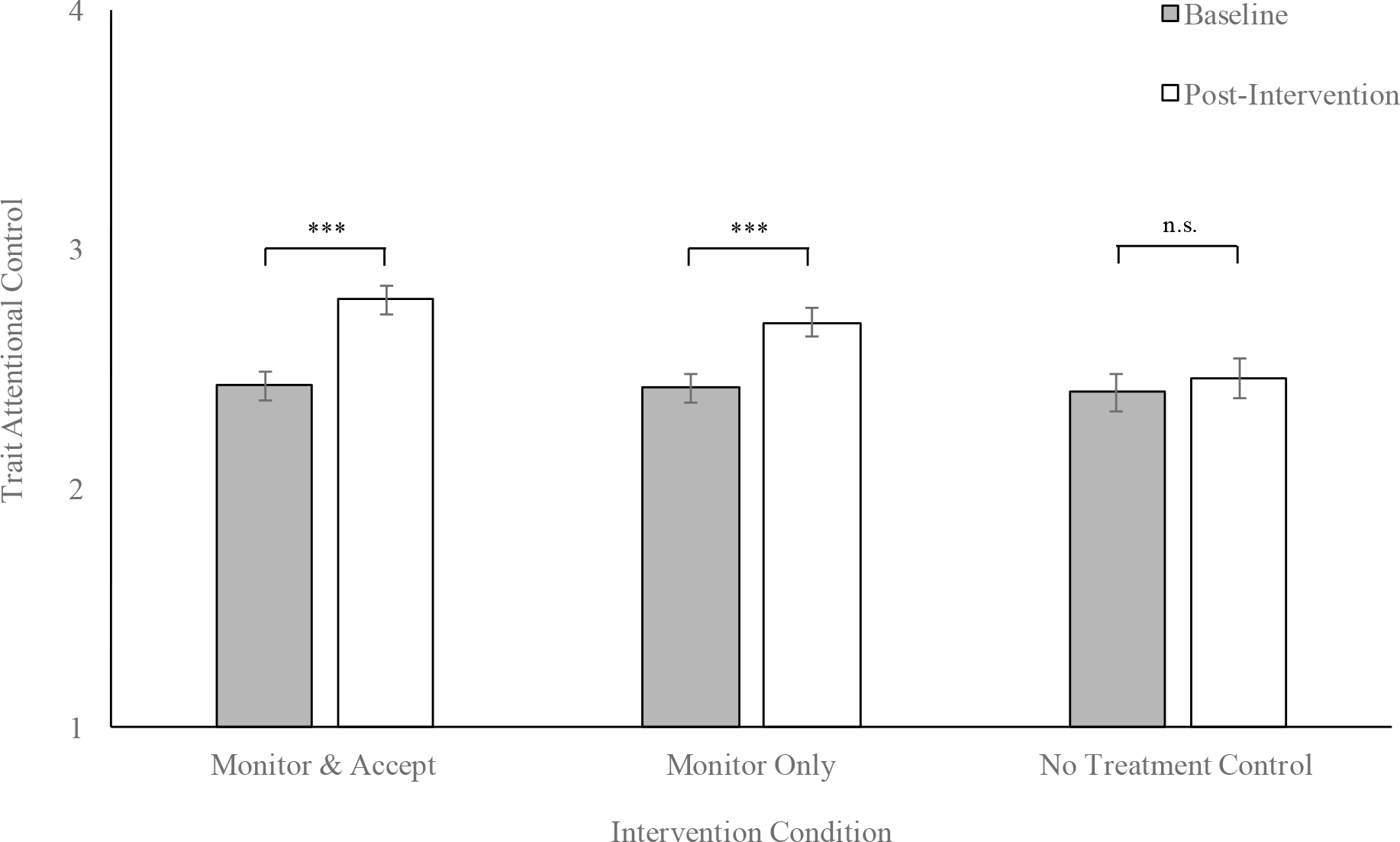
Changes in trait attentional control from baseline to post-intervention by study condition
Note. *** = p<.001. n.s. = not statistically significant. Time × condition interaction: χ2(2)=7.99, p=.018. Trait attentional control was assessed at baseline and post-intervention using the Attentional Control Scale (Derryberry & Reed, 2002).
These mindfulness training effects on trait attentional control were more robust for attentional focus compared to attention shifting. For the attention focusing subscale, there was a main effect of time across conditions (χ2(1)=25.60, p<.001), no main effect of condition across time (χ2(2)=1.76, p=.416), and a significant time × condition interaction (χ2(2)=10.03, p=.007). Participants assigned to either intervention condition increased in attentional focus from baseline to post-intervention (MA mean change=.43, p<.001, d=.77; MO mean change=.36, p<.001, d=.65), whereas no treatment (control) participants did not change significantly over time (NT mean change=.01, p=.905, d=.02). We found that both MA (χ2(1)=9.62, p=.002, d=.76) and MO participants (χ2(1)=6.26, p=.012, d=.62) increased in attentional focus relative to NT participants, whereas MA and MO participants did not differ in magnitude of change over time (χ2(1)=0.41, p=.524, d=.14).
For the attention shifting subscale, there was a main effect of time across conditions (χ2(1)=22.52, p<.001) and a main effect of condition across time (χ2(2)=7.04, p=.030), but no time × condition interaction (χ2(2)=4.58, p=.102).
Sensitivity analyses
In sensitivity analyses, there was still a significant Time × Condition interaction for momentary attentional control in models including additional covariates for average positive treatment expectancies (χ2(2)=8.03, p=.018), hours of home practice (χ2(2)=8.18, p=.017), or change in treatment expectancies from Week 1 to Week 8 (χ2(2)=7.92, p=.019). We found no association between momentary attentional control and average positive treatment expectancies (b=.014, SE=.054, p=.794), hours of home practice (b=−.0003, SE=.0001, p=.080), or change in treatment expectancies from Week 1 to Week 8 (b=.059, SE=.057, p=.300).
We also conducted analyses testing the alternative hypothesis that intervention effects on momentary attentional control were attributable to reductions in psychological stress or negative affect. However, there was no evidence for a three-way interaction of Time × Condition × Negative Affect (assessed continuously using EMA; see Lindsay et al., 2018) in predicting momentary attentional control (MA vs AO: b<.001, SE=.062, p=.997; MO vs AO: b=.008, SE=.064, p=.902). Similarly, there was no evidence for a three-way interaction of Time × Condition × Stress (assessed continuously using EMA; see Chin et al., 2019) in predicting momentary attentional control (MA vs AO: b=−.016, SE=.054, p=.767; MO vs AO: b=.010, SE=.054, p=.854). In addition, there was still a significant Time × Condition interaction for momentary attentional control in analyses that included additional covariates for negative affect (χ2(2)=8.30, p=.016) and psychological stress (χ2(2)=6.93, p=.031) at each assessment.
Testing indirect pathways
There was a significant correlation between momentary attentional control (averaged across all assessments at baseline and post-intervention separately) and trait attentional control (baseline: r=.55, p<.001; post-intervention: r=.49, p<.001). We used the PROCESS macro for SPSS (Version 2.16.3; Hayes, 2017) to test if the data were consistent with the hypothesis that increased momentary attentional control accounted for MA/MO intervention-related increases in trait attentional control (see Figure 4). Controlling for momentary and trait attentional control at baseline, there was a significant indirect effect of the MA/MO training conditions on trait attentional control through increased momentary attentional control (b=.103, SE=.042, 95% CI = [.038, .207]). The direct effect of the MA/MO training conditions on trait attentional control was no longer significant when accounting for increases in momentary attentional control (b=.146, SE=.080, 95% CI = [−.012, .304]). The indirect effect explained 41.35% of the total effect of the MA/MO training interventions for increasing trait attentional control.
Figure 4.
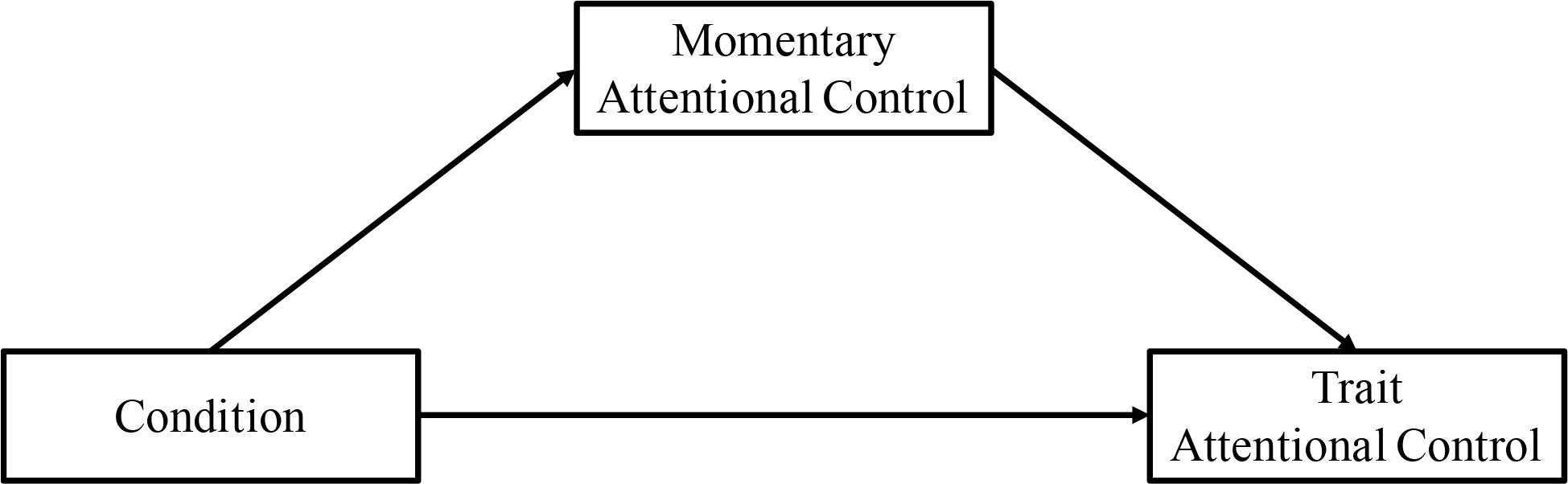
Theoretical model of intervention-related changes in momentary and trait attentional control tested in analysis of indirect pathway
Dichotic listening attention task
Dichotic listening attention task data was available from 135 of 137 participants (98.5%). Analysis of task performance (d’) showed a main effect of time across conditions (χ2(1)=5.24, p=.022), such that all participants improved in task performance from baseline (M=2.71, SE=.126) to post-intervention (M=2.92, SE=.129). However, there was no main effect of condition across time (χ2(2)=3.31, p=.191), and no significant time × condition interaction (χ2(2)=0.48, p=.787). (See Table 2). Analysis of self-reported distraction during the dichotic listening task showed a main effect of time across conditions (χ2(1)=4.65, p=.031), no main effect of condition across time (χ2(2)=1.46, p=.482), and a significant time × condition interaction (χ2(2)=7.53, p=.023). Participants assigned to the mindfulness interventions reported being less distracted during the dichotic listening task at post-intervention relative to baseline (MA mean change=−9.517, p=.015, d=.37; MO mean change=−12.932, p=.002, d=.50), whereas no treatment participants did not change significantly over time (NT mean change=5.394, p=.324, d=.21). Both MA (χ2(1)=4.91, p=.027, d=.60) and MO participants (χ2(1)=7.11, p=.008, d=.73) decreased in self-reported distraction during the dichotic listening task relative to NT participants. Like the attentional control outcomes reported above, MA and MO participants did not differ in magnitude of change over time (χ2(1)=0.36, p=.550, d=.13). (See Table 2).
Discussion
This pre-registered randomized controlled trial provides the first experimental test of the active psychological mechanisms linking mindfulness training interventions with improved attentional control. Following the MAT account of mindfulness training interventions (Lindsay & Creswell, 2017), we predicted that mindfulness interventions teaching attention monitoring skills would improve both momentary and trait attentional control. Consistent with our primary hypothesis, MA and MO participants increased in both momentary and trait attentional control from baseline to post-intervention relative to NT participants (there was not a statistically significant difference between MA and MO participants for either outcome). Contrary to initial predictions, MA and MO participants did not improve in dichotic listening attention task performance relative to NT participants. However, MA and MO participants decreased in self-reported distraction during the dichotic listening task relative to NT participants (there was not a statistically significant difference between MA and MO participants). This study provides the first evidence that an 8-week mindfulness training intervention can improve momentary measures of attentional control assessed during daily life. Moreover, these findings extend earlier research suggesting that mindfulness interventions improve trait attentional control (e.g., Garland et al., 2017; Walsh et al., 2019) by providing the first evidence that these benefits may be driven by the training of present-focused monitoring skills.
Monitor and Acceptance Theory (MAT) is one mechanistic account of mindfulness positing that monitoring and acceptance skills training have both distinct and synergistic roles in driving intervention-related improvements in various outcomes (Lindsay & Creswell, 2017). Although previous experimental work has tested MAT predictions regarding the benefits of acceptance skills training (e.g., Chin et al., 2019; Lindsay et al., 2018), this is the first study to test the MAT prediction that monitoring skills training alone (i.e., independent of acceptance skills training) drives intervention-related improvements in attention outcomes (Lindsay & Creswell, 2017). MAT posits that the capacity to monitor present moment experiences is reliant upon executive functioning skills, such as attentional control – the capacity to voluntarily focus attention and ignore distractions (Derryberry & Reed, 2002; Hopfinger et al., 2000). Interventions training monitoring skills may improve attentional control because the monitoring practices (e.g., focused attention meditation, body scan, open monitoring) involved in these interventions repeatedly engage attentional control networks and allow individuals to practice deploying their attention more effectively (Tang & Posner, 2009).
Consistent with MAT predictions, we found that the MA and MO training programs similarly improved both momentary and trait measures of attentional control, relative to a no-treatment control condition. This study builds upon earlier research suggesting that self-reported monitoring skills are associated with better performance on task-based measures of attentional control (Moore & Malinowski, 2009) by providing initial evidence that monitoring skills training improves trait and momentary measures of attentional control. We also tested the alternative mechanistic hypothesis that intervention effects on momentary attentional control were attributable to reductions in negative psychological states. However, we did not find evidence that intervention effects were moderated (or confounded) by psychological stress or negative affect.
We had initially hypothesized that intervention-related improvements in self-report measures of attentional control would also translate into improved performance on a dichotic listening task used to assess sustained attention. Consistent with this possibility, previous research suggests that greater trait attentional control is associated with better performance on task-based measures of attention (e.g., Hallion, Tolin, Billingsley, Kusmierski, & Diefenbach, 2019). We did not find evidence for intervention-related improvements in dichotic listening attention task performance; however, we did find that the MA and MO training programs reduced distractibility during the dichotic listening task relative to a no treatment control condition. One possible reason that we observed improvements in momentary and trait attentional control, but not dichotic listening attention task performance, is that larger doses of mindfulness training may be required to significantly improve task-based measures of sustained attention. This possibility is consistent with previous work showing that a three month intensive meditation retreat modestly improved dichotic listening task performance (Lutz et al., 2009). Another possible explanation is that intervention-related benefits may be specific to self-reported perceptions of attentional control and distractibility, and do not translate to task-based measures of attention. However, other studies have found that greater trait attentional control is associated with better attention task performance (e.g., Hallion et al., 2019). Additional research is necessary to test whether intervention-related improvements in momentary and trait attentional control also translate into improvements on other measures of cognitive performance. Future studies are also necessary to determine how monitoring and acceptance skills training affects other attentional networks (i.e., alerting and orienting networks; Petersen & Posner, 2012).
Another potentially surprising result was that NT participants also showed small improvements in momentary attentional control from baseline to post-intervention. A possible explanation that should be tested in future research is that repeatedly assessing attentional control in daily life may have led NT participants to become more aware of their attentional processes and led to subsequent improvement (i.e., Hawthorne effects; McCambridge, Witton, & Elbourne, 2014).
Trait and momentary measures provide unique insight into attentional control. Our measure of trait attentional control (Attentional Control Scale; Derryberry & Reed, 2002) asked individuals to make a general estimation of how frequently they have difficulty with focusing their attention. When making this assessment, individuals must recall their experiences across a wide range of situations and contexts. This measure may therefore reflect an individual’s general belief about their own typical attentional states (Gorin & Stone, 2001; Solhan, Trull, Jahng, & Wood, 2009). In contrast, our measure of momentary attentional control (assessed using EMA) asked individuals to report how frequently they have had difficulty focusing their attention during the previous two hours (i.e., since the previous assessment). These repeated assessments were used to derive a measure of momentary attentional control that was based on an individual’s experienced attentional control across different real-world contexts. Though still susceptible to recall biases inherent in the use of self-report, EMA measures minimize these influences by asking individuals to report on their experiences during a substantially shorter recall period (Solhan et al., 2009).
We tested the secondary hypothesis that improvements in momentary attentional control would drive intervention-related increases in trait attentional control. Consistent with our hypothesis, we found that MA and MO intervention-related increases in momentary attentional control statistically accounted for intervention-related improvements in trait attentional control. These results support the possibility that intervention-related changes in momentary experiences may precede and drive (i.e., mediate) subsequent changes in individuals’ general beliefs about their own typical states. This is consistent with earlier research suggesting that EMA measures may be more sensitive than trait measures for detecting intervention-related changes in psychological processes (Lindsay, Young, Brown, Smyth, & Creswell, 2019; Moore, Depp, Wetherell, & Lenze, 2016). One potential implication of these findings is that changes in momentary attentional control may occur earlier following intervention-onset relative to changes in trait attentional control. However, a limitation of these analyses was that our measures of momentary and trait attentional control were moderately correlated. While the magnitude of this association (baseline: r=.55; post-intervention: r=.49) suggests that these measures may capture distinct psychological processes, additional research is needed to establish their discriminant validity. This could be tested rigorously in future studies by including measures of both momentary and trait attentional control in daily life assessments.
There are several limitations to this study. One limitation was that the MA and MO training programs were compared to an NT assessment-only comparison condition. Although the comparison of two well-matched interventions was a significant strength of this study, the use of an NT comparison condition meant that we were unable to make inferences regarding the benefits of monitoring skills training for attentional control beyond the effects attributable to non-specific features of the intervention such as contact with classmates and instructors. Nonetheless, we found evidence for intervention-related improvements in momentary and trait attentional control even when statistically controlling for positive treatment expectancies, change in treatment expectancies, or amount of home practice. Although participants in both intervention conditions increased in treatment expectancies during the intervention period, we did not find evidence for a Time × Condition interaction, indicating that MA and MO participants did not differ in change over time. Sensitivity analyses also suggested that intervention effects on momentary attentional control could not be accounted for by treatment expectancies. However, we acknowledge that these analyses were suboptimal because treatment expectancy data was not collected from NT participants (because these participants did not receive any treatment).
A second limitation of this study is that the learning of monitoring and acceptance skills was not directly measured. An important direction for future research is to develop new measures which assess the learning of these skills. A third limitation of this study is that it was not possible to know whether participants were implementing the monitoring skills that they learned during the intervention. Future studies could consider including additional EMA items that explicitly ask participants to indicate whether they have been using the (monitoring) skills they learned during their intervention since the previous assessment. Additionally, the EMA items used to assess momentary attentional control have not been extensively tested or validated. Future studies are also needed both to further develop the psychometric properties of the measures used in this study and to replicate these findings. A fourth limitation is that this study examined a sample that was predominantly white, female, and highly educated. Future research is necessary to test the degree to which these results are generalizable to other populations. Another potential limitation of this study was that our exclusion criteria for previous meditation experience (>2 times per week or >90 minutes of weekly practice) may not have been a stringent enough cutoff given earlier evidence that even low doses of meditation practice may have beneficial effects (e.g., Schumer et al., 2018). Future studies could test previous exposure to low doses of meditation as a potential moderator or boundary condition of the effects observed in this study. A final limitation is that this study relied on self-report measures of attentional processes. Future studies are needed to test whether these improvements in momentary and trait attentional control also translate into improved performance on task-based measures of attentional control.
This theoretically-driven randomized controlled dismantling trial aimed to test the active mechanisms of mindfulness training interventions that drive improvements in attentional control. Consistent with our primary hypothesis, MA and MO participants improved in both momentary and trait attentional control compared to NT participants. In addition, we also found evidence that increased momentary attentional control statistically accounted for MA and MO intervention-related improvements in trait attentional control. Notable strengths of this study include the assessment of attentional control during daily life, as well as the use of a rigorous randomized controlled trial design. These findings provide some of the first evidence that mindfulness interventions improve attentional control through the training of present-focused monitoring skills. Further, this study contributes to a new wave of mechanistically-focused mindfulness research that allows researchers to evaluate the relative contributions of specific intervention components (Britton et al., 2017; Chin et al., 2019; Lindsay et al., 2018).
Context of the research.
Our laboratory has spent the last decade and a half focusing on how mindfulness interventions become biologically embedded – how they can change the brain and body to impact health. During the previous few years, we have stepped back to ask what psychological skills individuals learn in mindfulness training interventions that drive these biological cascades. We have developed the MAT account (Lindsay & Creswell, 2017) to provide an architecture for thinking about these psychological mechanisms of mindfulness interventions. In the current manuscript, we were interested in testing the MAT prediction that the training of attention monitoring skills would drive intervention-related improvements in daily life attention processes. Other work from our laboratory has focused on understanding how mindfulness interventions can promote stress resilience and improve physical health through the training of non-judgmental acceptance and equanimity skills (e.g., Chin et al., 2019). We plan to continue building out the MAT account of mindfulness training interventions by testing these predictions among stress sensitive individuals and patient populations. We are also enthusiastic about extending our research to examine how the training of monitoring and acceptance skills in mindfulness interventions can affect long-term mental and physical health outcomes.
Supplementary Material
Acknowledgements.
The authors gratefully acknowledge Melissa Myozen Blacker, MA, Roshi, former senior teacher at University of Massachusetts Center for Mindfulness for her contributions to the development and design of the intervention programs; Deanna Burkett for contributions to the development, design, and teaching of the intervention programs; and Jeffrey DeBoer, Hayley Rahl, and Lauren Simicich for help with study management.
Funding Sources.
Research reported in this publication was supported by grants from the National Center For Complementary & Integrative Health (NCCIH) of the National Institutes of Health (NIH) (R21AT008493; R01AT008685) awarded to JDC. Recruitment for this study was supported by the NIH (UL1TR000005). Contributions to this manuscript made by EL were supported by a grant from the NIH (F32AT009508). The funding sources had no involvement in study design; manuscript preparation; data collection, analysis, or interpretation; or the decision to submit this article for publication. The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Footnotes
Trial registration: clinicaltrials.gov; Identifier: NCT02502227
Age was missing from one participant; age based on n=136 participants.
The four-item PSS is a validated measure and this short form was used to minimize participant burden during the phone screening. Cutoff score (>5) was selected based on previously reported population means for this scale (M=4.49, SD=2.96 by Cohen & Williamson, 1988).
Cronbach’s α-values were calculated by averaging reliability values computed at each time point.
Although home practice audios were 40–45 minutes in duration, participants would occasionally receive credit for additional practice time due to issues with the software platform. To correct these outliers, any home practice session greater than 45 minutes in duration were recoded to 45 minutes.
Prior Dissemination. Outcomes reported in this manuscript have not been previously disseminated.
References
- Anestis MD, Selby EA, Crosby RD, Wonderlich SA, Engel SG, & Joiner TE (2010). A comparison of retrospective self-report versus ecological momentary assessment measures of affective lability in the examination of its relationship with bulimic symptomatology. Behaviour Research and Therapy, 48(7), 607–613. 10.1016/j.brat.2010.03.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baer RA, Smith GT, & Allen KB (2004). Assessment of mindfulness by self-report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11(3), 191–206. [DOI] [PubMed] [Google Scholar]
- Baer RA, Smith GT, Hopkins J, Krietemeyer J, & Toney L (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45. [DOI] [PubMed] [Google Scholar]
- Bishop SR, Lau M, Shapiro S, Carlson L, Anderson ND, Carmody J, Segal ZV, Abbey S, Speca M, Velting D, & Devins G (2004). Mindfulness: A Proposed Operational Definition. Clinical Psychology: Science and Practice, 11(3), 230–241. 10.1093/clipsy.bph077 [DOI] [Google Scholar]
- Britton WB, Davis JH, Loucks EB, Peterson B, Cullen BH, Reuter L, Rando A, Rahrig H, Lipsky J, & Lindahl JR (2017). Dismantling Mindfulness-Based Cognitive Therapy: Creation and validation of 8-week focused attention and open monitoring interventions within a 3-armed randomized controlled trial. Behaviour Research and Therapy. 10.1016/j.brat.2017.09.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiesa A, Calati R, & Serretti A (2011). Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clinical Psychology Review, 31(3), 449–464. 10.1016/j.cpr.2010.11.003 [DOI] [PubMed] [Google Scholar]
- Chin Brian, Lindsay EK, Greco CM, Brown KW, Smyth JM, Wright AGC, & Creswell JD (2019). Psychological mechanisms driving stress resilience in mindfulness training: A randomized controlled trial. Health Psychology, 38(8), 759–768. 10.1037/hea0000763 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Kamarck T, & Mermelstein R (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 385–396. [PubMed] [Google Scholar]
- Cohen S, & Williamson G (1988). Perceived stress in a probability sample of the US In Spacapam S & Oskamp S (Eds.), The social psychology of health: Claremont symposium on applied social psychology (pp. 31–67). Newbury Park, CA: Sage. [Google Scholar]
- Creswell JD (2017). Mindfulness Interventions. Annual Review of Psychology, 68(1), 491–516. 10.1146/annurev-psych-042716-051139 [DOI] [PubMed] [Google Scholar]
- Creswell JD, Pacilio LE, Lindsay EK, & Brown KW (2014). Brief mindfulness meditation training alters psychological and neuroendocrine responses to social evaluative stress. Psychoneuroendocrinology, 44(2014), 1–12. [DOI] [PubMed] [Google Scholar]
- de Bruin EI, van der Zwan JE, & Bögels SM (2016). A RCT comparing daily mindfulness meditations, biofeedback exercises, and daily physical exercise on attention control, executive functioning, mindful awareness, self-compassion, and worrying in stressed young adults. Mindfulness, 7(5), 1182–1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Derryberry D, & Reed MA (2002). Anxiety-related attentional biases and their regulation by attentional control. Journal of Abnormal Psychology, 111(2), 225–236. 10.1037/0021-843X.111.2.225 [DOI] [PubMed] [Google Scholar]
- Devilly GJ, & Borkovec TD (2000). Psychometric properties of the credibility/expectancy questionnaire. Journal of Behavior Therapy and Experimental Psychiatry, 31(2), 73–86. [DOI] [PubMed] [Google Scholar]
- Eysenck MW, & Derakshan N (2011). New perspectives in attentional control theory. Personality and Individual Differences, 50(7), 955–960. 10.1016/j.paid.2010.08.019 [DOI] [Google Scholar]
- Farb NA, Segal ZV, & Anderson AK (2012). Mindfulness meditation training alters cortical representations of interoceptive attention. Social Cognitive and Affective Neuroscience, 8(1), 15–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foust J (2014). Body-Centered Inquiry: Meditation Training to Awaken Your Inner Guidance, Vitality, and Loving Heart. Sounds True. [Google Scholar]
- Garland EL, Hanley AW, Goldin PR, & Gross JJ (2017). Testing the mindfulness-to-meaning theory: Evidence for mindful positive emotion regulation from a reanalysis of longitudinal data. PloS One, 12(12), e0187727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goenka SN (1994). Discourse Summaries: Evening Discourses by S.N. Goenka from a Ten-Day Course of Vipassana. Pariyatti Publishing. [Google Scholar]
- Hallion LS, Tolin DF, Billingsley AL, Kusmierski SN, & Diefenbach GJ (2019). “Cold” Cognitive Control and Attentional Symptoms in Anxiety: Perceptions Versus Performance. Behavior Therapy, 50(6), 1150–1163. 10.1016/j.beth.2019.04.002 [DOI] [PubMed] [Google Scholar]
- Hayes AF (2017). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Publications. [Google Scholar]
- Hillyard SA, Hink RF, Schwent VL, & Picton TW (1973). Electrical Signs of Selective Attention in the Human Brain. Science, 182(4108), 177–180. 10.1126/science.182.4108.177 [DOI] [PubMed] [Google Scholar]
- Hopfinger JB, Buonocore MH, & Mangun GR (2000). The neural mechanisms of top-down attentional control. Nature Neuroscience, 3(3), 284. [DOI] [PubMed] [Google Scholar]
- Jha AP, Krompinger J, & Baime MJ (2007). Mindfulness training modifies subsystems of attention. Cognitive, Affective, & Behavioral Neuroscience, 7(2), 109–119. 10.3758/CABN.7.2.109 [DOI] [PubMed] [Google Scholar]
- Judah MR, Grant DM, Mills AC, & Lechner WV (2014). Factor structure and validation of the attentional control scale. Cognition & Emotion, 28(3), 433–451. [DOI] [PubMed] [Google Scholar]
- Kabat-Zinn J (1990). Full catastrophe living: The program of the stress reduction clinic at the University of Massachusetts Medical Center. New York: Delta. [Google Scholar]
- Kabat-Zinn J (2009). Wherever you go, there you are: Mindfulness meditation in everyday life. Hachette UK. [Google Scholar]
- Kechter A, Amaro H, & Black DS (2019). Reporting of Treatment Fidelity in Mindfulness-Based Intervention Trials: A Review and New Tool Using NIH Behavior Change Consortium Guidelines. Mindfulness, 10(2), 215–233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsay EK, Chin B, Greco CM, Young S, Brown KW, Wright AG, Smyth JM, Burkett D, & Creswell JD (2018). How mindfulness training promotes positive emotions: Dismantling acceptance skills training in two randomized controlled trials. Journal of Personality and Social Psychology, 115(6), 944–973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsay EK, & Creswell JD (2017). Mechanisms of mindfulness training: Monitor and Acceptance Theory (MAT). Clinical Psychology Review, 51, 48–59. 10.1016/j.cpr.2016.10.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsay EK, Young S, Brown KW, Smyth JM, & Creswell JD (2019). Mindfulness training reduces loneliness and increases social contact in a randomized controlled trial. Proceedings of the National Academy of Sciences, 116(9), 3488–3493. 10.1073/pnas.1813588116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsay EK, Young S, Smyth JM, Brown KW, & Creswell JD (2018). Acceptance lowers stress reactivity: Dismantling mindfulness training in a randomized controlled trial. Psychoneuroendocrinology, 87, 63–73. [DOI] [PubMed] [Google Scholar]
- Lutz A, Slagter HA, Rawlings NB, Francis AD, Greischar LL, & Davidson RJ (2009). Mental Training Enhances Attentional Stability: Neural and Behavioral Evidence. The Journal of Neuroscience, 29(42), 13418–13427. 10.1523/JNEUROSCI.1614-09.2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCambridge J, Witton J, & Elbourne DR (2014). Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. Journal of Clinical Epidemiology, 67(3), 267–277. 10.1016/j.jclinepi.2013.08.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore A, & Malinowski P (2009). Meditation, mindfulness and cognitive flexibility. Consciousness and Cognition, 18(2009), 176–186. [DOI] [PubMed] [Google Scholar]
- Moore RC, Depp CA, Wetherell JL, & Lenze EJ (2016). Ecological momentary assessment versus standard assessment instruments for measuring mindfulness, depressed mood, and anxiety among older adults. Journal of Psychiatric Research, 75, 116–123. 10.1016/j.jpsychires.2016.01.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petersen SE, & Posner MI (2012). The Attention System of the Human Brain: 20 Years After. Annual Review of Neuroscience, 35(1), 73–89. 10.1146/annurev-neuro-062111-150525 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Posner MI, & Petersen SE (1990). The Attention System of the Human Brain. Annual Review of Neuroscience, 13(1), 25–42. 10.1146/annurev.ne.13.030190.000325 [DOI] [PubMed] [Google Scholar]
- Schumer MC, Lindsay EK, & Creswell JD (2018). Brief mindfulness training for negative affectivity: A systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 86(7), 569–583. 10.1037/ccp0000324 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S, Stone AA, & Hufford MR (2008). Ecological Momentary Assessment. Annual Review of Clinical Psychology, 4(1), 1–32. 10.1146/annurev.clinpsy.3.022806.091415 [DOI] [PubMed] [Google Scholar]
- Shrout PE, & Bolger N (2002). Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods, 7(4), 422–445. 10.1037//1082-989X.7.4.422 [DOI] [PubMed] [Google Scholar]
- Smyth JM, & Stone AA (2003). Ecological Momentary Assessment Research in Behavioral medicine. Journal of Happiness Studies, 4(1), 35–52. 10.1023/A:1023657221954 [DOI] [Google Scholar]
- Solhan MB, Trull TJ, Jahng S, & Wood PK (2009). Clinical assessment of affective instability: Comparing EMA indices, questionnaire reports, and retrospective recall. Psychological Assessment, 21(3), 425–436. 10.1037/a0016869 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swets JA, Green DM, Getty DJ, & Swets JB (1978). Signal detection and identification at successive stages of observation. Perception & Psychophysics, 23(4), 275–289. 10.3758/BF03199711 [DOI] [PubMed] [Google Scholar]
- Tang Y-Y, & Posner MI (2009). Attention training and attention state training. Trends in Cognitive Sciences, 13(5), 222–227. 10.1016/j.tics.2009.01.009 [DOI] [PubMed] [Google Scholar]
- Tiitinen HT, Sinkkonen J, Reinikainen K, Alho K, Lavikainen J, & Näätänen R (1993). Selective attention enhances the auditory 40-Hz transient response in humans. Nature, 364(6432), 59–60. 10.1038/364059a0 [DOI] [PubMed] [Google Scholar]
- Trungpa C (2003). Training the Mind and Cultivating Loving-Kindness. Shambhala Publications. [Google Scholar]
- Villalba DK, Lindsay EK, Marsland AL, Greco CM, Young S, Brown KW, Smyth JM, Walsh CP, Gray K, Chin B, & Creswell JD (2019). Mindfulness training and systemic low-grade inflammation in stressed community adults: Evidence from two randomized controlled trials. PLOS ONE, 14(7), e0219120. 10.1371/journal.pone.0219120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsh JJ, Balint MG, Smolira SJ DR, Fredericksen LK, & Madsen S (2009). Predicting individual differences in mindfulness: The role of trait anxiety, attachment anxiety and attentional control. Personality and Individual Differences, 46(2), 94–99. 10.1016/j.paid.2008.09.008 [DOI] [Google Scholar]
- Walsh KM, Saab BJ, & Farb NA (2019). Effects of a Mindfulness Meditation App on Subjective Well-Being: Active Randomized Controlled Trial and Experience Sampling Study. JMIR Mental Health, 6(1), e10844. 10.2196/10844 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.