

Abstract
Objective
Despite evidence of disparate uptake of breast density (BD) information, little is known about diverse women’s preferences for and experiences learning about BD.
Methods
Telephone survey among 2,306 racially/ethnically and literacy diverse women; qualitative interviews with 61 survey respondents. Responses by participant race/ethnicity and literacy were examined using bivariate, then multivariable analyses. Interviews were content-analyzed for themes.
Results
Most women (80%) preferred learning of personal BD from providers, with higher rates among Non-Hispanic Black (85%) than Non-Hispanic White women (80%); and among Non-Hispanic White than Asian women (72%, all ps<.05). Women with low literacy less often preferred receiving BD information from providers (76% v. 81%), more often preferring written notification (21% vs. 10%); women with high literacy more often preferred learning through an online portal (9% vs 3%). Most women (93%) received BD information from providers (no between group differences). Qualitative findings detailed women’s desires for obtaining BD information from providers, written information, and visual depictions of BD.
Conclusions
When educating women about BD, one size does not fit all.
Practice Implications
Additional educational methods are needed beyond written BD notifications to sufficiently address the varying informational needs and preferences of all USA women.
1. Introduction
Breast density notifications aim to educate women about the risks of high breast density, defined as having more fibroglandular tissue than fatty tissue, as visualized on a mammogram. Risks of higher density include reduced sensitivity of mammography by masking of breast cancers, and a 1.6 to 2.0 fold increased risk for breast cancer (1, 2). Prompted by activists whose own breast density had obscured breast cancers on their mammograms (3), 38 U.S. states and Washington, DC have enacted legislation requiring written notification of a patient’s breast density (DBN) after a mammogram,(4) and language for a federal notification is forthcoming from the U.S.A. Food and Drug Administration (FDA). Yet, these notifications were developed with limited input and without extensive testing among women in the general population, and many are written at a high literacy level, often discordant with population literacy levels (5, 6). Prior studies of women’s knowledge from and reactions to DBNs demonstrated racial/ethnic disparities (7). Low awareness of breast density, especially among racial/ethnic minority and socioeconomically disadvantaged women (8, 9), supports the need for input from varied population groups.
A key activity in the successful development of health education materials is the solicitation of feedback from a diverse sample of target populations about preferences for receiving information about health concerns, ensuring understandability for the general population (10–13). Indeed, communications designed to be inclusive of populations with limited literacy or limited English proficiency are preferred by individuals of all literacy levels (14). As the FDA prepares federal DBN text (15), we sought feedback about women’s experiences of and preferences for receiving such information among a racially/ethnically and literacy-level diverse national sample.
2. Methods
We employed a sequential mixed-methods study design, assessing preferences and experiences regarding receipt of breast density information with a telephone survey, followed by qualitative interviews with a subset of survey respondents to gain an in-depth perspective of experiences with notification. We based the survey and qualitative interview guides on existing literature, prior studies (16–18), and the Health Belief Model, a framework to explain health-related behaviors and describe factors influencing health-related decisions (19, 20). The survey research was approved by the university Institutional Review Board; qualitative interviews were determined to meet criteria for exemption.
Telephone Survey
Participant Sampling and Recruitment.
We conducted a cross-sectional, national, random digit dial telephone survey. The sampling approach was detailed previously (21). Briefly, structured telephone surveys by professional interviewers from the survey firm SSRS used questions within SSRS’ Omnibus survey (7/2019–4/2020), a national, weekly, dual-frame bilingual random digit dial telephone survey using landlines and cell phones, conducted in English and Spanish, to identify a representative sample of USA women 40 to 76 years old meeting the following eligibility criteria: (1) had a mammogram within the prior 2 years; (2) no personal history of breast cancer; and (3) had heard the term “dense breasts” or “breast density”. Eligible participants were also invited to participate using a prescreened, callback sample from prior Omnibus waves to increase participation of Hispanic, Black and Asian women, women with less than a high school education, and those living in less populous non-DBN states. A third group of eligible participants were invited to participate using a sample specifically modeled by SSRS to reach Asian-American women. Figure 1 delineates the yield and cooperation rates from each sampling approach.
Figure 1.
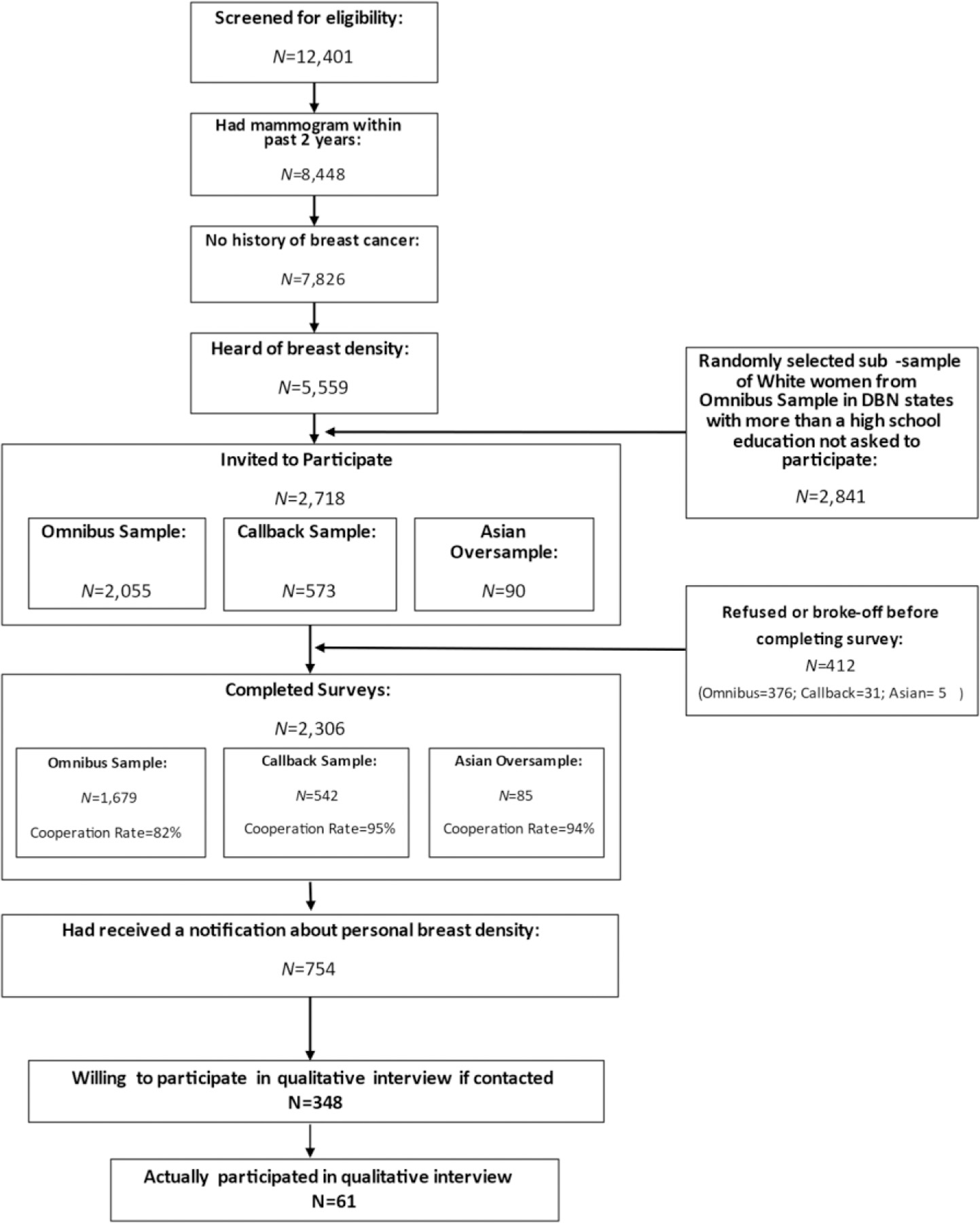
Cohort Derivation
Measures.
Dependent Variables.
The study team, consisting of clinicians and researchers, (all consumers), and assisted by feedback from a Patient Advisory Council, assessed women’s preferences for and experiences with learning about personal breast density with questions from prior surveys (Table 2) (7, 18). We asked respondents whether they would most like to receive such information through: a) a letter or notice in the mail; b) a secure website or online portal where one accesses personal health information; or c) being told by a healthcare provider. For those indicating they knew their personal breast density, we asked how they actually received this information, using the same response categories, though they could select all response options that applied.
Table 2.
Bivariate results
| Overall | Race/Ethnicity | Literacy | ||||||
|---|---|---|---|---|---|---|---|---|
| Variable | NH White | NH Black | Hisp. | Asian | Other | High | Low | |
| Among full sample, N=2,306ƚ | ||||||||
| In thinking about your personal breast density, how would you most like to receive information about your personal breast density? Would you prefer to get this information… | ||||||||
| χ2(8)=49.42, p<.001 | χ2(2)=55.98, p<.001 | |||||||
| -in a letter or notice in the mail (%yes) | 12% | 14% a | 9% b | 16 a | 10% a,b | 11% a,b | 10% a | 21% b |
| -from a website or online portal such as My Chart where you access your personal health information? (%yes) | 7% | 6% a | 7% a | 6% a | 18% b | 8% a | 9% a | 3% b |
| -by being told by a healthcare provider (%yes) | 80% | 80% a | 85% b | 78% a,c | 72% c | 82% a,b,c | 81% a | 76% b |
| Among women who had received information about their personal breast density (N=1,322) ƚ | ||||||||
| How did you learn about your personal breast density (select all that apply)? | ||||||||
| χ2(4)=16.42, p=.003 | χ2(1)=0,01, p=.915 | |||||||
| -in a letter or notice (%yes) | 53% | 50% a,b | 56% b | 47% a | 70% c | 57% a,b,c | 53% | 53% |
| χ2(4)=14.45, p=.006 | χ2(1)=16.68, p<.001 | |||||||
| -from a website or online portal such as My Chart where you access your personal health information? (%yes) | 20% | 17% a | 23% b | 22% a,b | 31% b | 18% a,b | 18% a | 30% b |
| χ2(4)=2.94, p=.592 | χ2(1)=3.42, p=.064 | |||||||
| by being told by a healthcare provider (%yes) | 93% | 92% | 94% | 91% | 91% | 96% | 93% | 90% |
Note: Within a given row, cells that contain different superscripted letters differ significantly from one another after Bonferroni correction for multiple comparisons; cells that contain the same superscripted letter do not differ significantly.
Missing n=30 (1%);
Weighted N=1,303,, Missing n=19 (1%); NH=non-Hispanic
Sociodemographic Characteristics.
We assessed respondents’ race and ethnicity (Non-Hispanic White, Non-Hispanic Black, Hispanic or Latino, Asian, other) and literacy. Low literacy was defined as either having less than a high school education or reporting sometimes/often/always needing assistance to complete medical forms using the validated Single Item Literacy Screener(22). Those responding as never or rarely needing assistance to complete medical forms or having more than a high school education were classified as having high literacy. Race, ethnicity, and literacy were assessed among all participants of the quantitative survey and this information was shared with the study team by SSRS to facilitate purposive sampling during qualitative data collection.
Covariates.
We assessed residence in a state with mandated DBNs (DBN state), age (40–49, 50–64, 65+ years), and income (<$50K, $50–99.9K, $100K+). To control for breast cancer risk factors as covariates, we assessed self-reported family history of breast cancer or prior biopsy.
Statistical Analysis
First, we assessed whether responses to each survey item were associated with participant race/ethnicity and literacy separately, using bivariate, chi-square analyses. Post-hoc comparisons across pairs of levels for each categorical variable were conducted as Z-tests with Bonferroni corrected p-values. Then, we assessed these associations using multivariable binary logistic regressions predicting responses to each survey item from both race/ethnicity and literacy simultaneously, while controlling for DBN state residence, age, income, family history of breast cancer, and prior biopsy. For multivariable analyses, response options (letter/notice, online portal, provider) were coded (0=did not select; 1=selected) and 6 separate regression models were built, one for each of the 3 response options for preferences for receiving information about personal breast density and one for each of the 3 response options for experiences receiving such information. All analyses utilized data weights provided by SSRS to account for sampling probability and systematic nonresponse along known population parameters.
Qualitative Interviews
Participant Sampling and Recruitment.
We sought to enroll a subset of 64 survey study participants who consented to re-contact.
Of the 754 survey participants indicating they had received a DBN, 348 agreed to participate in a qualitative interview. Among these, we employed purposive sampling, enrolling up to 8 participants/group into one of 8 groups based on race and ethnicity (White, Black, Hispanic, and Other, which included women identifying as Asian, mixed race, or another race or ethnicity) and literacy (high (HL), low (LL)).
Interview Guide Development.
We developed an open-ended, semi-structured interview guide to examine women’s experiences with learning about personal breast density, and preferences for receiving such information. The guide (see Appendix), which also covered additional topics not reported here, was pilot tested with a patient advisory group before implementation (n=5).
Data Collection.
From February – May 2020, interviewers trained in qualitative research methods conducted 30–45 minute telephone interviews; participants received $25 debit cards. Interviews were audio recorded and professionally transcribed verbatim.
Analysis.
We reviewed audio files against transcripts to ensure accuracy and remove any identifiable data unintentionally disclosed. De-identified transcripts were imported into NVivo qualitative coding software 12.1 for analysis. Content analysis methods guided coding and theme development (23). We drafted an initial codebook based on domains from the interview guide and the conceptual model. Multiple research team members independently coded five interviews representing different literacy and racial/ethnic categories to test and refine the codebook, including the addition of inductive codes. The remaining transcripts were coded by one of two coders, with questions reviewed and reconciled via consensus with four research team members. For this analysis, we analyzed codes regarding women’s preferences for and experiences with receiving breast density information.
3. Results
Characteristics of the samples
Quantitative Sample.
Overall, 5,559 women were eligible for survey participation, 2,718 of these women were invited to participate, and 412 participants declined to participate or withdrew before completing the full survey, leaving a sample of 2,306 (85% overall cooperation rate; Figure 1). Quantitative sample characteristics are provided in Table 1.
Table 1.
Quantitative Sample Characteristics
| Overall (unweight) N (%) | Overall (weighted) % | |
|---|---|---|
| Sample Size | N=2,306 | N=2,306 |
| Age Group | ||
| 40–49 | 449 (19.5) | 24.5% |
| 50–64 | 1107(48.0) | 51.0% |
| 65+ | 750 (32.5) | 24.5% |
| Income (missing n=153) | ||
| < $50k | 962 (41.7) | 43.7% |
| $50–99.9K | 693 (30.1) | 29.0% |
| ≥ $100K | 503 (21.8) | 20.7% |
| Education (missing n=4) | ||
| ≤HS | 498 (21.6) | 29.3% |
| Some college | 674 (29.2) | 32.2% |
| College or more | 1128 (48.9%) | 38.2% |
| Race/Ethnicity | ||
| NH White | 1058(45.9) | 48.0% |
| NH Black | 581 (25.2) | 24.0% |
| Hispanic | 338 (14.7) | 14.7% |
| Asian | 168 (7.3%) | 8.7% |
| Other | 160 (6.9%) | 4.6% |
| Literacy a | ||
| Low | 388 (16.8%) | 20.7% |
| High | 1918 (83.2%) | 79.3% |
| Individual Breast Cancer Risk Factor | ||
| Family History of Breast (missing n=20) | 410 (17.8%) | 16.8% |
| Prior Breast Biopsy (missing n=22) | 559 (24.2%) | 21.9% |
Low literacy was defined as either having less than a high school education or reporting sometimes/often/always needing assistance to complete medical forms using the validated Single Item Literacy Screener(22).
Qualitative Sample.
Sixty-one women completed a qualitative interview, with at least 6 participants in each group defined by both literacy and race/ethnicity. To preserve anonymity, qualitative interview respondents were not linked to survey data, limiting linking to additional demographic information. Quotes are labeled using race/ethnicity and literacy group.
Women’s Preferences for Receiving Personal Breast Density Information
Survey results showed that the majority of women indicated that they would most like to receive information about their personal breast density from their provider (80%), followed by a letter/notice in the mail (12%), or through an online portal (7%; Table 2). Preferences for how to receive such information varied significantly by race/ethnicity. Paired comparisons revealed that preferences for receiving this information from a provider were significantly higher among Non-Hispanic Black women (85%) than Non-Hispanic White women (80%), and significantly higher among both Non-Hispanic White women and Non-Hispanic Black women compared to Asian women (72%; these and all following reported differences had significant Bonferroni-corrected p-values at ps<.05). Preference for receiving personal breast density information from a letter/notice in the mail was significantly higher among Non-Hispanic White women (14%) and Hispanic women (16%) compared to Non-Hispanic Black women (9%). Preference for receiving personal breast density information from an online portal was significantly higher among Asian women (18%) compared to all other racial/ethnic groups (Non-Hispanic White women=6%; Non-Hispanic Black women=7%; Hispanic women=6%; women from other racial/ethnic categories=8%). These differences persisted in multivariable analyses, except the difference in preference to receive information from a provider between Non-Hispanic White and Non-Hispanic Black women was no longer significant (see Table 3).
Table 3.
Multivariable results
| Preferences: How would you most like to receive your personal breast density? (N=2,306) | Experiences: How did you learn about your personal breast density (select all that apply)? (N=1,322; Weighted N=1,303) | |||||
|---|---|---|---|---|---|---|
| Letter/Notice1 | Online Portal1 | Provider1 | Letter/Notice2 | Online Portal3 | Provider3 | |
| Omnibus χ 2 | 61.33 | 63.34 | 27.18 | 25.63 | 36.65 | 17.72 |
| Omnibus p | <.001* | <.001* | .007* | .012* | <.001* | .125 |
| −2LL | 1521.99 | 1035.51 | 2064.76 | 1625.84 | 1196.90 | 565.63 |
| Constant | .11 | .15 | 3.63 | .92 | .18 | 33.66 |
| Race | ||||||
| Non-Hispanic White | -- | -- | -- | -- | -- | -- |
| Non-Hispanic Black | .62* [.43, .90] | 1.16 [.73, 1.85] | 1.29 [.96, 1.74] | 1.45* [1.07, 1.97] | 1.55* [1.06, 2.26] | 1.38 [.73, 2.61] |
| Hispanic | 1.14 [.78, 1.67] | .91 [.50, 1.66] | .93 [.67, 1.30] | .94 [.66, 1.35] | 1.35 [.87, 2.11] | .76 [.39, 1.46] |
| Asian | .77 [.44, 1.35] | 2.77* [1.64, 4.67] | .66* [.45, .98] | 2.74 * [1.62, 4.61] | 2.67* [1.54, 4.61] | .92 [.38, 2.22] |
| Other | .80 [.40, 1.57] | 1.39 [.63, 3.10] | 1.02 [.59, .94] | 1.48 [.86, 2.56] | 1.10 [.55, 2.23] | 2.23 [.51, 9.78] |
| Literacy | ||||||
| Low | 2.05* [1.52, 2.77] | .40* [.21, .74] | .72* [.55, .94] | 1.02 [.75, 1.40] | 2.15* [1.51, 3.05] | .77 [.43, 1.39] |
| High | -- | -- | -- | -- | -- | -- |
| CONTROL VARIABLES | ||||||
| DBN State | 1.13 [.78, 1.64] | .82 [.51, 1.33] | .98 [.72, 1.33] | .94 [.67, 1.31] | .90 [.59, 1.40] | .49 [.22, 1.08] |
| Age | ||||||
| Less than 50 | -- | -- | -- | -- | -- | -- |
| 50–64 | .96 [.68, 1.36] | .93 [.63, 1.36] | 1.06 [.81, 1.38] | 1.16 [.88, 1.54] | 1.04 [.74, 1.47] | .67 [.36, 1.24] |
| 65+ | 1.46 [.99, 2.14] | .49* [.28, .88] | .95 [.69, 1.32] | .97 [.68, 1.38] | .86 [.56, 1.34] | .38* [.18, .77] |
| Income | ||||||
| <$50K | 1.19 [.81, 1.75] | .58* [.37, .89] | 1.16 [.86, 1.56] | .99 [.71, 1.36] | 1.26 [.84, 1.88] | 1.36 [.71, 2.61] |
| $50–99.9K | .78 [.52, 1.19] | .64* [.42, .99] | 1.48* [1.09, 2.03] | .91 [.67, 1.24] | .96 [.65, 1.43] | 1.07 [.58, 1.99] |
| $100K+ | -- | -- | -- | -- | -- | -- |
| Family History of Breast Cancer | .87 [.61, 1.24] | 1.32 [.85, 2.07] | .99 [.74, 1.33] | 1.18 [.86, 1.61] | 1.11 [.76, 1.62] | .93 [.51, 1.70] |
| Prior Biopsy | 1.15[.84, 1.57] | 84[.54, 1.30] | 97[.74, 1.26] | 1.05[.80, 1.37] | 1.02[.73, 1.41] | 1.54[.86, 2.76] |
Note: Each column represents a separate multivariable binary logistic regression. Cells list odds ratios for each model coefficient, with 95% Confidence Intervals in square brackets. Significant effects (at p<.05) are indicated with an asterisk (*).
Missing n=162 (7.1%);
Missing n=95 (7.3%);
Missing n=85 (6.5%)
Literacy significantly influenced preferences for receiving personal breast density information. Compared to women with high literacy, women with low literacy were significantly less likely to prefer to receive breast density information from their provider (76% v. 81%) or through an online portal (3% v. 9%), and significantly more likely to prefer to receive breast density information from a letter/notice (21% v. 10%) (see Table 2); these significant differences persisted in multivariable analyses (Table 3).
Women’s Experiences Receiving Personal Breast Density Information
Among the sub-sample of women (N=1,322; Weighted N=1,303) who reported receiving information about personal breast density, 93% indicated they had learned this information from a provider, with no differences by race/ethnicity or literacy (Tables 2 and 3). Fifty-three percent had learned in a letter/notice, and bivariate analyses revealed this differed significantly based on participants’ race/ethnicity. Paired comparisons revealed that Asian women were significantly more likely (70%) to report receiving a letter/notice than Non-Hispanic White (50%), Non-Hispanic Black (56%), or Hispanic (47%) women. In multivariable analyses, Asian and Non-Hispanic Black women remained significantly more likely than Non-Hispanic White women to have received breast density information this way (Table 3). There were no differences in the likelihood of having received a letter or notice by literacy in bivariate or multivariable analyses (Tables 2 and 3). Twenty percent of women reported receiving personal breast density information from an online portal, and bivariate analyses revealed this differed significantly by participant race/ethnicity. Paired comparisons revealed that Non-Hispanic White women were significantly less likely to have received information via an online portal (17%) than were Non-Hispanic Black women (23%) and Asian women (31%) in bivariate and multivariable analyses (Tables 2 and 3). Women with low literacy (30%) were more likely to receive information from an online portal than women with high literacy (18%) in bivariate and multivariable analyses (Tables 2 and 3).
Qualitative Results
Qualitative results illustrated details of women’s reasons for their preferences for modes of receiving breast density information and their experiences receiving such information, as well as their suggestions for improving information delivery approaches. Four themes emerged regarding preferences around written notification. First, a number of women found a letter to be ‘cold’ and impersonal, and valued the opportunity to discuss the results, ask questions, assess the level of concern based on body language of the provider, and elicit next steps. As one woman said,
“I think in person is good. I think that that needs to be discussed with the patient. I mean, it’s great doing it that way I feel because it’s more personable. Because if you were given, you know, just a written report and just said, “Well, you have dense breasts.” It’s like, “Okay, yeah. So and what? What next?” You can’t ask any other questions really.” (Black woman, High literacy).
“But the way they let you know, it’s kind of cold. I don’t know. It’s weird. You open up a letter and it says, “You have breast density.” … You’re doing something to my body and this is how you’re going to let me know that there’s some type of issue… how do I know that that’s not saying that this might be the start of breast cancer for me? I think the letter comes from the doctor that reads the x-ray and it just seems like stock, like they pulled this letter up from the file and they put my name on it and the date and it already has his signature on it and they send it out. It’s as if I were number 1011. Number 1011 has a breast density, send the letter … And not like, “Oh, it’s [INTERVIEWEE] who has the thing. Let me talk to her and if she has any questions she can call me.” I think you should be able to have a conversation with the person that reads the X rays. He’s the doctor…..”Why can’t I call you and talk to you about it? You’re the one who did the x-ray. Can I ask you what it means?” But they don’t even want you to call them. Right away they’re pushing you off to your PCP who’s probably overworked, overwhelmed. You know what I mean? Be the doctor, that’s what they chose to do.” (Black woman, Low literacy)
“The most difficult part? That instead of a phone call or something from the nurse or doctors, that it was a letter in the mail, a two sentence letter in the mail. It just seemed kind of… I don’t know, very detached and cold…. Well, I wished that someone would explain to me more about what it means to have dense breasts or what I needed to be aware of with my specific tissue that I have… Well, I would prefer to have more information.” (White woman, High literacy)
“So I want someone to look me in the eyes so that I can, you know, read their expressions. Do I need to worry about this or don’t I? And it answers those questions instead of just sitting there wondering and then you’ve got to make a phone call. “Oh, I got this letter” and they’re like, “Oh please. Oh, no, don’t worry about it.” Okay, well why’d you send me the letter if I don’t need to worry about it?” (Hispanic woman, Low literacy)
Second, some women indicated that they appreciated that a letter could provide factual information to read at one’s leisure, or in advance of a discussion with a provider. Several women attributed these preferences to their cultural background or personal characteristics.
“Yeah, through the mail or a letter would be nice. Something I could sit down and read.” (Woman of Other race, High literacy)
“But for me, getting a letter saying, “This is the deal and here’s what we can do about it” is exactly the right way to handle it. But I understand that might not be true for everyone… I mean, we joke in this part of the country about being of Norwegian heritage and part of what that means is that we don’t come across as very emotional. And so, I guess that’s what I’m feeling in this is that, “Oh. It was factual information. I’m glad to have it.” (White woman, High literacy)
“It would be nice to get a letter with some kind of photographs showing how dense tissues can develop later on or something more than just remaining as the same. And then what happens with that? So, if there are pictures of something that kind of would give me more idea and make me more aware of what I should be doing and how often I should be checking and things like that.” (Woman of Other race, Low literacy)
“I think the letter is the best way for me because my reading is better than my talking in English. So if people call me or talk to me about the breast density, I might meet some medical terms I don’t understand. But if I receive the letter, when I read it, if I find any words is new, I can pick it up in the dictionary to find the meaning. I can take my time to read it slowly and understand it.” (Woman of Other race, Low literacy)
A third theme illustrated women’s desires for receiving information both in writing and from a provider, or being given the option to talk with someone if they preferred.
“Well, I liked it all, both to tell you the truth. I liked that I had a conversation in person, but that I also liked getting it in writing because sometimes you don’t pay attention or you’re distracted or if you think it’s bad news, you don’t listen well. You know what I mean? So it was nice to have a follow-up in writing.” (Woman of Other race, High literacy)
“Well, I preferred it, how can I say it? Them calling me and then following up with the letter…That confirmed what they said over the phone. It’s a confirmation that everything is okay.” (Hispanic woman, Low literacy)
Women describing this multi-modality form of communication (letter plus conversation) emphasized the importance of being able to ask questions in a timely manner, as exemplified by this woman:
“I think it’d be nice if simply at the end of the thing, you have breast density, “If you have any questions about what it is, you can give us a call at this number.” That would be nice. Because the nurse that answers the phone, or the clerical or whoever, can probably tell you what it means, but you’re not even giving me the option to talk to you about it… Or, “Talk to nurse X, Y, and Z.” Something like that. Then that puts a different color on the letter.” (Black woman, Low literacy)
Finally, many women recognized that ‘one size does not fit all’ and suggested that approaches should cater to different learning styles, including visual depictions of breast density, to aid in understanding the concept.
“Anything that’s going to get it across to the person that helps them learn, you know. Some people need a video, some people need it written down. It just depends.” (Hispanic woman, High literacy)
“Or, maybe some graphics. I mean, I know it’s kind of graphic for some people, but maybe a lot of people are visual learners. That maybe some pictures would be helpful to show this is what a normal breast looks like, this is what a dense breast looks like. And kind of try to educate more so people aren’t as fearful about it.” (White woman, High literacy)
“I think for me, personally, I think the letter itself was pretty sufficient, but now as we were talking, now I was trying to struggle with my answers to answer those questions, I thought in the letter, if we use charts instead of writing, that may be helpful, just kind of showing if you have a higher density, meaning higher risk. Maybe use visual.” (Woman of Other race, Low literacy)
“Ultimately, it would be great to receive color information with photographs so that I understood…” (White woman, Low literacy)
4. Discussion and Conclusion
4.1. Discussion
We conducted a national survey of a large, diverse and nationally representative sample of US women, followed by in-depth qualitative interviews to understand women’s preferences for receiving personal breast density information. Our results reinforce and provide further validation of prior findings, some from a small sample from a single geographic area, (24), providing additional detail about how groups would most prefer to learn such information from their provider. Results from our large sample with a significant proportion of Asian women and those from other racial/ethnic groups allowed us to see that this preference was somewhat lower for Asian women given their greater preference for receiving this information via an online portal compared to all other groups, and slightly higher for Non-Hispanic Black women given their slightly lower preference for receiving a letter/notice in the mail than other groups. Women with low literacy more often preferred a written notification, while those with high literacy more often preferred learning through an online portal. We found, as have others (25, 26), that most women received breast density information from their providers, without sociodemographic differences.
Qualitative findings provided additional depth, elucidating that while some women were satisfied with a written letter/notice, women with low literacy and non-native English speakers had less confidence in their ability to process information provided verbally without a written backup, or provided in writing without the opportunity to discuss with a provider; this may explain the new and somewhat counter-intuitive survey findings of low literacy women’s preferences for written notifications. Though we could not locate other literature documenting a general sentiment among people with low literacy to prefer written health information, the explanations women provided helped clarify that written information gives them an opportunity to look up the definitions of words they do not understand, to re-read the information, and to take time to process it, different from what a single verbal encounter would provide. This new insight about the value of a written communication for women with low literacy provides further support for multi-modal breast density educational materials. Furthermore, consistent with the only other study we could locate regarding women’s preferences for receipt of breast density information (24), women in our study requested visual depictions of breast density, to illustrate the concept.
Our study was limited by its reliance on respondents’ self-report and potential recall bias, especially for those who received a breast density notification long before this survey. However, self-report methods are widely used and the only way to learn women’s preferences and experiences, even as they are subject to some biases. We had only race/ethnicity and literacy data on participants in the qualitative interview sample, limiting our ability to link responses to other sociodemographic characteristics. Finally, questions referring to health care providers did not specify type of provider, so we are unable to determine the exact source of information.
4.2. Conclusion
Together, these findings suggest that ‘one size does not fit all’, with regard to breast density education. Women had varying preferences for learning about personal breast density, only partly associated with literacy level or race/ethnicity. This suggests that a multi-modal notification (e.g., a letter accompanied by an educational brochure or links to online information including visuals), and provision of opportunities to speak with a clinician to ask questions and receive personalized information and guidance, would meet more women’s needs than the single-mode DBN letters currently in use.
4.3. Practice Implications
As the FDA prepares a federal DBN, and health educators and providers consider further breast density educational strategies, these results suggest that the current sole focus on written breast density notifications will not fully address the varying needs and preferences of the diverse population of US women, and that additional methods of education should be considered. For women preferring to learn of their breast density from a provider, it seems important to make a telephone consultation available at a minimum, but some women may prefer to have a clinic visit to discuss the results and decide upon future screening in consultation with their provider. Another option would be for radiologists to read mammograms in real time and provide breast density and mammography results to women in-person, as has been implemented in some settings (27). Wider implementation of this approach might address women’s desire for personal communication of results and assuage anxiety as well.
Supplementary Material
Highlights.
To explore women’s preferences and experiences for receiving breast density information, we conducted a national telephone survey of a large, diverse sample of American women and qualitative interviews with a subset of these women.
This study is among the first to examine women’s preferences and experiences in receiving breast density information, an important step when preparing health education materials that are accessible to a broad audience.
We found significant differences in preferences for receiving breast density information by race/ethnicity and literacy levels. We learned details of women’s preferences and obtained suggestions for future breast density health education materials.
The findings suggest that a written letter alone is insufficient, that ‘one size does not fit all’ for breast density education, and the use of multi-modal educational materials is recommended.
Acknowledgments:
We appreciate the assistance of Ariel Maschke and Magda Pankowska in the conduct of this research.
This work was supported by the American Cancer Society (133017-RSG-19–085-01-CPHPS) and the National Cancer Institute (1K07CA221899). The funding sources had no role in study design, data collection, analysis or interpretation, or in the writing of the report.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
CRediT authorship contribution statement
NR Kressin Conceptualization, Methodology, Investigation, Resources, Writing - Original Draft, Supervision, Project Administration, Funding acquisition
JB Wormwood Formal analysis, visualization, Writing - Review & Editing, Funding acquisition
TA Battaglia Conceptualization, Methodology, Writing - Review & Editing, Funding acquisition
PJ Slanetz Writing - Review & Editing
CM Gunn Conceptualization, Methodology, Writing - Review & Editing, Funding acquisition
References
- 1.Nelson HD, Zakher B, Cantor A, Fu R, Griffin J, O’Meara ES, et al. Risk factors for breast cancer for women aged 40 to 49 years: a systematic review and meta-analysis. Ann Intern Med 2012. May 1;156(9):635–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kerlikowske K, Hubbard RA, Miglioretti DL, Geller BM, Yankaskas BC, Lehman CD, et al. Comparative effectiveness of digital versus film-screen mammography in community practice in the United States: a cohort study. Ann Intern Med 2011. Oct 18;155(8):493–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cappello NM. Decade of ‘normal’ mammography reports--the happygram. J Am Coll Radiol: JACR 2013. Dec;10(12):903–8. [DOI] [PubMed] [Google Scholar]
- 4.DenseBreast-Info.org. DenseBreast-Info.org. 2021. [cited 2021 June 22]; Available from: https://densebreast-info.org/.
- 5.Kressin NR, Gunn CM, Battaglia TA. Content, Readability, and Understandability of Dense Breast Notifications by State. J Amer Med Assoc 2016. Apr 26;315(16):1786–8. [DOI] [PubMed] [Google Scholar]
- 6.Dooling BCE. The FDA’s Opaque Approach To Breast Density Communications. HEALTH AFFAIRS BLOG Washington, DC: Health Affairs; 2019. [Google Scholar]
- 7.Rhodes DJ, Breitkopf CR, Ziegenfuss JY, Jenkins SM, Vachon CM. Awareness of Breast Density and Its Impact on Breast Cancer Detection and Risk. J Clin Oncol 2015;33(10):1143–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nickel B, Copp T, Brennan M, Farber R, McCaffery K, Houssami N. The Impact of Breast Density Information or Notification on Women’s Cognitive, Psychological, and Behavioral Outcomes: A Systematic Review. J Natl Cancer Inst 2021. Feb 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Manning M, Purrington K, Penner L, Duric N, Albrecht TL. Between-race differences in the effects of breast density information and information about new imaging technology on breast-health decision-making. Patient Educ Couns 2016. Jun;99(6):1002–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dopp AR, Parisi KE, Munson SA, Lyon AR. A glossary of user-centered design strategies for implementation experts. Transl Behav Med 2019. Nov 25;9(6):1057–64. [DOI] [PubMed] [Google Scholar]
- 11.Lyon AR, Koerner K. User-Centered Design for Psychosocial Intervention Development and Implementation. Clin Psychol 2016. Jun;23(2):180–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Farrell-Miller P, Gentry P. How effective are your patient education materials? Guidelines for developing and evaluating written educational materials. Diabetes Educ 1989. Sep-Oct;15(5):418–22. [DOI] [PubMed] [Google Scholar]
- 13.Doak LG, Doak CC, Meade CD. Strategies to improve cancer education materials. Oncol Nurs Forum 1996. Sep;23(8):1305–12. [PubMed] [Google Scholar]
- 14.Davis TC, Crouch MA, Wills G, Miller S, Abdehou DM. The gap between patient reading comprehension and the readability of patient education materials. J Fam Pract 1990. Nov;31(5):533–8. [PubMed] [Google Scholar]
- 15.U.S. Food and Drug Administration. Mammography Quality Standards Act 2019. [July 27, 2020]; Available from: https://www.federalregister.gov/documents/2019/03/28/2019-05803/mammography-quality-standards-act.
- 16.Gunn CM, Battaglia TA, Paasche-Orlow MK, West AK, Kressin NR. Women’s perceptions of dense breast notifications in a Massachusetts safety net hospital: “So what is that supposed to mean?”. Patient Educ Couns 2018. Jun;101(6):1123–9. [DOI] [PubMed] [Google Scholar]
- 17.Gunn CM, Fitzpatrick A, Waugh S, Carrera M, Kressin NR, Paasche-Orlow MK, et al. A Qualitative Study of Spanish-Speakers’ Experience with Dense Breast Notifications in a Massachusetts Safety-Net Hospital. J Gen Intern Med 2019. Feb;34(2):198–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kressin NR, Wormwood JB, Battaglia TA, Gunn CM. Differences in Breast Density Awareness, Knowledge, and Plans Based on State Legislation Status and Sociodemographic Characteristics. J Gen Intern Med 2020. Jun;35(6):1923–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Becker M The health belief model and personal health behavior Thorofare, NJ: CB Slack; 1974. [Google Scholar]
- 20.Rosenstock IM. Why People Use Health Services. The Milbank M Fund Q 1966;44(3):94–127. [PubMed] [Google Scholar]
- 21.Kressin NR, Battaglia TA, Wormwood JB, Slanetz PJ, Gunn CM. Dense Breast Notification Laws’ Association With Outcomes in the US Population: A Cross-Sectional Study. J Am Coll Radiol 2021. May;18(5):685–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Morris NS, MacLean CD, Chew LD, Littenberg B. The Single Item Literacy Screener: evaluation of a brief instrument to identify limited reading ability. BMC Fam Pract 2006. Mar 24;7:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Burla L, Knierim B, Barth J, Liewald K, Duetz M, Abel T. From Text to Codings: Intercoder Reliability Assessment in Qualitative Content Analysis. Nurs Res 2008;57(2):113–7. [DOI] [PubMed] [Google Scholar]
- 24.Marcus EN, Yepes M, Dietz N. Perception of Breast Density Information Among Women in Miami, FL: a Qualitative Study. J Cancer Educ 2020. Jun 6. [DOI] [PubMed] [Google Scholar]
- 25.Cappello NM, Richetelli D, Lee CI. The Impact of Breast Density Reporting Laws on Women’s Awareness of Density-Associated Risks and Conversations Regarding Supplemental Screening With Providers. J Am Coll Radiol 2019. Feb;16(2):139–46. [DOI] [PubMed] [Google Scholar]
- 26.Rhodes DJ, Jenkins SM, Hruska CB, Vachon CM, Breitkopf CR. Breast Density Awareness, Knowledge, and Attitudes Among US Women: National Survey Results Across 5 Years. J Am Coll Radiol 2020. Mar;17(3):391–404. [DOI] [PubMed] [Google Scholar]
- 27.Dontchos BN, Achibiri J, Mercaldo SF, Wang GX, Lamb LR, Miles RC, et al. Disparities in Same-Day Diagnostic Imaging in Breast Cancer Screening: Impact of an Immediate-Read Screening Mammography Program Implemented During the COVID-19 Pandemic. AJR Am J Roentgenol 2022. Feb;218(2):270–8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.