

Abstract
Background:
How 5-alpha reductase inhibitor (5-ARI) use influences prostate cancer mortality is unclear. The objective of this study was to determine whether men taking 5-ARIs with regular healthcare access have increased prostate cancer mortality.
Methods:
We undertook two analyses in the Health Professionals Follow-up Study examining 5-ARI use, determined by biennial questionnaires, and prostate cancer. A cohort analysis followed 38,037 cancer-free men for prostate cancer incidence from 1996 through January 2017 and mortality through January 2019. A case-only analysis followed 4,383 men with localized/locally advanced prostate cancer for mortality over a similar period. Hazard ratios (HR) and 95% confidence intervals were calculated for prostate cancer incidence and mortality.
Results:
Men using 5-ARIs underwent more PSA testing, prostate exams and biopsies. Over 20 years of follow-up, 509 men developed lethal disease (metastases or prostate cancer death). Among men initially free from prostate cancer, 5-ARI use was not associated with developing lethal disease (HR 1.02, 0.71–1.46), but was associated with reduced rates of overall and localized disease (HR 0.71, 0.60–0.83). Among men diagnosed with prostate cancer, there was no association between 5-ARI use and cancer-specific (HR 0.78, 0.48–1.27) or overall survival (HR 0.88, 0.72–1.07).
Conclusions:
Men using 5-ARIs were less likely to be diagnosed with low-risk prostate cancer, without increasing long-term risk of lethal prostate cancer or cancer-specific death after diagnosis.
Impact:
Our results provide evidence that 5-ARI use is safe with respect to prostate cancer mortality in the context of regular healthcare access.
Keywords: prostate cancer, 5-alpha reductase inhibitors, finasteride, dutasteride, cancer incidence and mortality
Introduction
Prostate cancer is the leading cause of cancer incidence and second leading cause of cancer mortality in men in the United States, with a lifetime risk of 11.6% for prostate cancer diagnosis and 2.4% for prostate cancer death1. Chemoprevention has been proposed as a strategy to reduce morbidity and mortality from prostate cancer2. 5-alpha reductase inhibitors (5-ARIs) like finasteride have been suggested as such a chemopreventive agent. A common treatment for benign prostatic hyperplasia (BPH) due to their ability to reduce prostate size, 5-ARIs block the enzymatic conversion of testosterone to its biologically active form, dihydrotestosterone (DHT)3–7.
In 2003, the randomized Prostate Cancer Prevention Trial (PCPT) found finasteride reduced the risk of overall prostate cancer by almost 25%. However, the study also found a 27% increased risk of high-grade prostate cancer among men randomized to finasteride, raising concerns that a chemoprevention benefit would be offset by increased mortality8. As a result, there has been little use of 5-ARIs for cancer prevention due to the FDA’s Black Box label recommending against its use at a population level9.
Subsequent analyses explained these PCPT results could be due to detection bias. Men in the PCPT treated with finasteride had decreased prostate volumes, which improved detection of prostate cancer by increasing the sensitivity of the PSA test and digital rectal exam (DRE) and the accuracy of tumor grading on prostate biopsy10,11. Notably, 5-ARIs reduce serum prostate-specific antigen (PSA) concentrations by about 50%,12 highlighting the importance of regular PSA surveillance. While overall survival was similar between groups in the PCPT, concerns remained about the increased rate of high-grade tumors and the potential for increased prostate cancer mortality13–15.
Two 2019 publications addressed whether 5-ARIs increased prostate cancer mortality with differing results. An updated PCPT analysis with a median follow-up time of 18.4 years showed no excess risk of prostate cancer mortality with finasteride use16. In contrast, an observational study of men with prostate cancer treated at Veterans Affairs (VA) hospitals demonstrated that 5-ARI use was associated with later stage at presentation and a 39% higher risk of prostate cancer death17.
To address these conflicting results, we performed a prospective cohort study among 38,037 U.S. men with regular access to health care and PSA screening, and a case-only analysis of 4,383 men with prostate cancer.
Methods
Study Population
The study population was nested within the Health Professionals Follow-up Study (HPFS), a prospective cohort of 51,529 U.S. male health professionals who were 40–75 years old at baseline in 1986 and completed a mailed baseline questionnaire. Information on age, height and weight, ancestry, medications, disease history, physical activity, lifestyle factors, and diet were gathered, with follow-up questionnaires sent biennially to update information and record health outcomes. Questionnaires began asking about prostate-specific antigen (PSA) testing in 1994 and 5-ARI use in 1996. Men diagnosed with prostate cancer were sent prostate cancer-specific questionnaires to assess treatments, disease progression, and metastases biennially starting in 2010, and these data have been used to answer questions regarding prostate cancer epidemiology and outcomes18–22. The research was approved by institutional review boards at the Harvard T.H. Chan School of Public Health, Mass General Brigham and those of participating registries as required.
The study population was restricted to men in HPFS who did not already have a cancer diagnosis (except non-melanoma skin cancer) and completed a study questionnaire in 1996. Similarly to the PCPT, we followed these 38,037 men prospectively for cancer incidence. We also undertook a case-only study, like the VA, by following 4,383 men with localized/locally advanced prostate cancer for cancer-specific and overall mortality.
5-ARI exposure
The primary exposure, 5-ARI use during the study period, was determined on biennial questionnaires starting in 1996 with a question about regular use of Proscar (finasteride). From 2000–2010, questionnaires additionally asked about Proscar and Propecia (finasteride) use (2000–2004, 2008, 2010), and also about Avodart (dutasteride) use (2012–2016). Since the medications were grouped together in questions regarding use, we could not distinguish between 5-ARI types. However, it is likely that the predominant medication during the study period was Proscar (5 mg) because of its earlier FDA approval (1992) than Propecia (1 mg; approved in 1997) or Avodart (0.5 mg; approved in 2002)23. Exposure duration was the sum of two-year periods of use, as indicated by reporting regular use on the biennial questionnaires.
Outcomes
In the cohort analysis, the primary outcome was lethal prostate cancer, defined as development of metastatic disease or prostate cancer death. The secondary outcomes were stage and Gleason score at presentation. In the case-only analysis, the primary endpoints were progression to lethal prostate cancer and total mortality.
Grade was categorized as either Gleason 3+4 and lower, or Gleason 4+3 and higher based on surgical or biopsy reports. Analyses for Gleason score 8–10, score ≤6, score 7 (3+4), and score 7 (4+3) were also performed. Advanced cancers were TNM stage T3b/T4, N1, or M1; non-advanced cancers were TNM stage T1/T2/T3a, and N0/NX, M0/MX at diagnosis. Cases with missing stage or grade information were included in the analysis for total prostate cancer but excluded from analyses for stage or grade. Deaths were obtained from next-of-kin, the postal system, and the National Death Index, with a previously reported sensitivity of >98%24. Cause of death was assigned by an Endpoints Committee of physicians by reviewing medical history, medical records, registry information, and death certificates.
Statistical Analysis
For cohort analyses, study participants contributed person-time from the return date of the 1996 questionnaire until prostate cancer diagnosis, death, or end of follow-up (January 2017). Use of 5-ARIs (ever/never use) was the time-dependent exposure in all analyses, and was updated with each questionnaire. To avoid immortal time bias, men only contributed exposed person-time after they reported 5-ARI use on a questionnaire. For case-only survival analyses, follow-up started at time of cancer diagnosis and ended at death, development of metastases or end of follow-up (January 2019).
In cohort analyses, Cox proportional hazards models were used to estimate hazard ratios (HR) and 95% confidence intervals (95% CIs) for development of all incident prostate cancer and lethal, advanced, localized, high-grade and low-grade disease. Multivariable models included race (white, African-American, Asian-American, other); family history of prostate cancer in brother or father (yes/no); smoking history (never, former quit >10 years ago, former quit ≤10 years ago, current); BMI (four categories); height (continuous); vigorous physical activity (quintiles); diabetes mellitus (yes/no); use of multivitamins, statins, alpha-blockers, digoxin (all yes/no); PSA screening (lagged by one period, yes/no); PSA screening intensity (indicator for having PSA test in 50% or more questionnaire cycles); physical exam, prostate biopsy or rectal ultrasound (all in prior two years, yes/no); and vasectomy (yes/no).
In case-only analyses, Cox proportional hazards models were used to estimate HRs and 95% CIs for lethal prostate cancer and all-cause mortality. Multivariable models adjusted for stage, Gleason grade, current smoking status, race, family history of prostate cancer, physical activity quintiles, BMI and PSA at diagnosis.
All models used the questionnaire period as the timescale, were age-adjusted, and all covariates except race and height were updated with each questionnaire. Missing indicator variables were used for missing covariate information. Outcome comparisons were made between the exposure groups defined by use of 5-ARIs, ever versus never, and by cumulative duration of use, <4 years and ≥4 years. Four years was used as the cutoff as it represents use of 5-ARIs over two questionnaire periods.
As a sensitivity analysis, a Fine-Gray competing risk model estimated subdistribution hazard ratios for prostate cancer survival. Diagnostic bias associated with PSA testing was examined by restricting the cohort to 22,424 men in who reported PSA testing between 1994–1996. Given the increased prostate cancer risk among men with a family history of prostate cancer, we examined the effect of 5-ARI use on prostate cancer diagnoses in this population using real-world data. Additionally, the cohort analysis was repeated with alpha-blockers, another treatment for BPH, as the exposure to account for the effect of medical attention for BPH symptoms. Alpha-blocker models were adjusted for 5-ARI use.
The proportional hazards assumption was tested by comparing models with and without interaction terms between 5-ARI use and calendar time using log-likelihood tests; non-proportional hazards were not detected (p >0.05). Analyses were performed using SAS version 9.4 (SAS Institute, Inc.; Cary, NC).
Data Availability Statement
The data generated in this study are available upon request from the corresponding author.
Results
Full Cohort Study
Out of 38,037 men, 5,099 (13.4%) men reported ever use of 5-ARIs between 1996–2016 (Table 1), with a median duration of use of four years. Ever users were older on average than never users (63.4 vs. 62.8 years). In addition, men who had ever used 5-ARIs were more likely to have had recent PSA screening (prevalence difference 16%, 95% CI 15–18%) and were more likely to have had a prostate biopsy or rectal ultrasound prior to 1996 (prevalence difference 11%, 95% CI 10–13%).
Table 1.
Age-standardized characteristics of the Health Professionals Follow-up Study population in 1996 by end-of-study 5-ARI status (n=38,037)1
| Never Use (n=32,938) | Ever Use (n=5,099) | |
|---|---|---|
|
| ||
| Age in years 2 | 62.8 (9.3) | 63.4 (8.6) |
| Body Mass Index kg/m2 | 26.1 (3.6) | 26.2 (3.6) |
| Height in centimeters | 178.3 (7.0) | 178.2 (6.6) |
| Race | ||
| White | 91% | 92% |
| African American | 1% | 1% |
| Asian American | 2% | 1% |
| Other race | 2% | 2% |
| Unknown | 5% | 5% |
| Smoking Status | ||
| Never smoker | 49% | 52% |
| Past smoker (quit >10 years ago) | 32% | 34% |
| Past smoker (quit ≤10 years ago) | 12% | 10% |
| Current smoker | 7% | 4% |
| Family history of prostate cancer | 12% | 14% |
| Had a PSA test in the last two years | 57% | 72% |
| History of prostate exam | 69% | 78% |
| History of prostate biopsy | 9% | 19% |
| Vasectomy | 26% | 27% |
| Diabetes mellitus type 2 | 6% | 5% |
| Medications | ||
| Ever used alpha-blockers | 3% | 8% |
| Current statin use | 8% | 12% |
| Current digoxin use | 3% | 3% |
| Current aspirin use | 42% | 48% |
| Current acetaminophen use | 6% | 6% |
| NSAID use | 4% | 5% |
| Current multivitamin user | 38% | 43% |
| Physical activity in MET-hours/week | 32.1 (31.9) | 32.9 (31.6) |
Values are means (SD) for continuous variables; percentages for categorical variables and are standardized to the age distribution of the study population
Age value is not age-adjusted
Participants contributed 628,257 person-years over the study period, during which 4,575 men developed prostate cancer and 509 developed lethal disease (Table 2). Among men diagnosed with prostate cancer, 83.7% presented with localized disease, and 71.8% presented with a Gleason score of 3+4 or lower. In both age-adjusted and fully-adjusted models, we found no association between ever use of 5-ARIs and lethal (mHR 1.02, 0.71–1.46), advanced (mHR 1.02, 0.73–1.41) or high-grade prostate cancer (mHR 1.06, 0.84–1.33). In fully-adjusted models, there was a 21% reduced risk of overall prostate cancer (95% CI, 0.70–0.90), a 29% lower risk of localized disease (95% CI, 0.60–0.83), and a 38% reduced risk of low-grade disease (95% CI, 0.51–0.74). We found similar results examining duration of use (<4 and ≥4 years).
Table 2.
Association between 5-ARI use (ever use and duration of use) and prostate cancer outcomes in 38,037 men who were initially cancer-free in HPFS (628,257 person-years), 1996–2017
| Ever Use of 5-ARIs |
< 4 Years of 5-ARI Use |
≥ 4 Years of 5-ARI Use |
||||||
|---|---|---|---|---|---|---|---|---|
| Total Events | Number of Events | Age-adjusted HR (95%CI) | Adjusted HR1 (95% CI) | Number of Events | Adjusted HR1 (95% CI) | Number of Events | Adjusted HR1 (95% CI) | |
|
| ||||||||
| All Incident prostate cancer | 4575 | 253 | 1.03 (0.90, 1.17) | 0.79 (0.70, 0.90) | 154 | 0.76 (0.65, 0.90) | 99 | 0.85 (0.69, 1.04) |
| Lethal prostate cancer2 | 509 | 34 | 1.08 (0.76, 1.54) | 1.02 (0.71, 1.46) | 22 | 1.03 (0.66, 1.59) | 12 | 1.01 (0.56, 1.81) |
|
| ||||||||
| Stage at diagnosis | ||||||||
| Advanced3 | 648 | 42 | 1.12 (0.81, 1.53) | 1.02 (0.73, 1.41) | 25 | 0.94 (0.62, 1.42) | 17 | 1.17 (0.71, 1.91) |
| Localized4 | 3324 | 170 | 0.96 (0.82, 1.13) | 0.71 (0.60, 0.83) | 104 | 0.69 (0.56, 0.84) | 66 | 0.74 (0.58, 0.95) |
|
| ||||||||
| Gleason score | ||||||||
| High-grade (4+3 and above) | 1126 | 84 | 1.24 (0.99, 1.56) | 1.06 (0.84, 1.33) | 45 | 0.92 (0.67, 1.24) | 39 | 1.30 (0.93, 1.80) |
| Score 8–10 | 657 | 53 | 1.27 (0.95, 1.69) | 1.11 (0.82, 1.49) | 29 | 0.98 (0.67, 1.43) | 24 | 1.32 (0.86, 2.01) |
| Score 7 (4+3) | 469 | 31 | 1.20 (0.82, 1.73) | 0.99 (0.68, 1.45) | 16 | 0.83 (0.50, 1.37) | 15 | 1.27 (0.75, 2.16) |
| Low-grade (3+4 and below) | 2865 | 122 | 0.86 (0.72, 1.03) | 0.62 (0.51, 0.74) | 80 | 0.63 (0.51, 0.79) | 42 | 0.59 (0.43, 0.80) |
| Score 7 (3+4) | 1057 | 33 | 0.57 (0.40, 0.81) | 0.45 (0.31, 0.63) | 20 | 0.43 (0.28, 0.68) | 13 | 0.47 (0.27, 0.81) |
| Score ≤6 | 1808 | 89 | 1.06 (0.85, 1.31) | 0.73 (0.58, 0.90) | 60 | 0.75 (0.58, 0.98) | 29 | 0.68 (0.46, 0.98) |
HR (95% CI) = Hazard ratio and 95% confidence interval
adjusted for age, smoking status, race, family history of prostate cancer, vigorous activity levels, BMI, height, diabetes, PSA testing intensity, multivitamin use, statin use, current alpha-blocker use, digoxin use, vasectomy, prostate exam and biopsy, aspirin and NSAID use.
defined as death from prostate cancer or metastases over follow-up
defined as T3b or T4, N1, or M1
defined as T1, T2 or T3a, N0/NX and M0/MX
Case-Only Study
In the case-only group of 4,383 men with localized/locally-advanced prostate cancer, 235 (5.4%) men ever used 5-ARIs (Supplementary Table 1). Ever users were on average older than never users (75.1 vs. 70.3 years) and had shorter follow-up (10.4 vs. 11.8 years). Diagnostic PSA levels were approximately equal between ever and never users of 5-ARIs (8.9 vs. 8.8 ng/mL never users). Ever users also had a slightly higher percent of stage T1 cancer (77% vs. 69% never users) and a slightly higher percent of Gleason ≤6 cancer (53% vs. 47% never users).
At the end of follow-up, 320 men in the case-only cohort developed lethal prostate cancer (Table 3). In the fully-adjusted multivariable model, there was no association between ever using 5-ARIs and total mortality (mHR 0.88, 0.72–1.07) or lethal prostate cancer (mHR 0.78, 0.48–1.27). Findings were similar stratifying by duration of use.
Table 3.
Association between 5-ARI use and lethal prostate cancer and total mortality in men with localized or locally advanced prostate cancer at diagnosis (n=4,383), 1996–2019
| Number of Events | Age-adjusted HR (95% CI) | Model 1 adjusted HR (95% CI)1 | Model 2 adjusted HR (95% CI)2 | |
|---|---|---|---|---|
|
| ||||
| Lethal prostate cancer3 | 320 | |||
| Ever use of 5-ARIs | 19 | 1.03 (0.65, 1.65) | 0.73 (0.45, 1.18) | 0.78 (0.48, 1.27) |
| < 4 years of use | 13 | 1.30 (0.74, 2.26) | 1.05 (0.60, 1.85) | 1.11 (0.63, 1.96) |
| ≥ 4 years of use | 6 | 0.71 (0.32, 1.61) | 0.44 (0.19, 0.99) | 0.46 (0.20, 1.06) |
|
| ||||
| Total mortality (including lethal prostate cancer)4 | 1899 | |||
| Ever use of 5-ARIs | 107 | 0.96 (0.79, 1.17) | 0.87 (0.71, 1.06) | 0.88 (0.72, 1.07) |
| < 4 years of use | 57 | 0.91 (0.70, 1.18) | 0.85 (0.65, 1.11) | 0.85 (0.65, 1.11) |
| ≥ 4 years of use | 50 | 1.03 (0.78, 1.37) | 0.89 (0.67, 1.19) | 0.91 (0.69, 1.22) |
adjusted for stage at diagnosis, Gleason grade, and age at diagnosis
adjusted for everything in model 1 and BMI, family history of prostate cancer, PSA at diagnosis, activity level, smoking status at diagnosis, and race
defined as prostate cancer death or distant metastases over follow-up
defined as death from any cause or distant prostate cancer metastases
Sensitivity Analyses
In the 22,424 men with PSA screening in 1996, we found that results were similar to the primary analyses (Figure 1A; Supplementary Table 2). There was a reduced risk of overall, localized and low-grade prostate cancer among ever-users of 5-ARI in multivariable models, and no significant association between 5-ARI use and lethal, advanced or high-grade disease.
Figure 1.
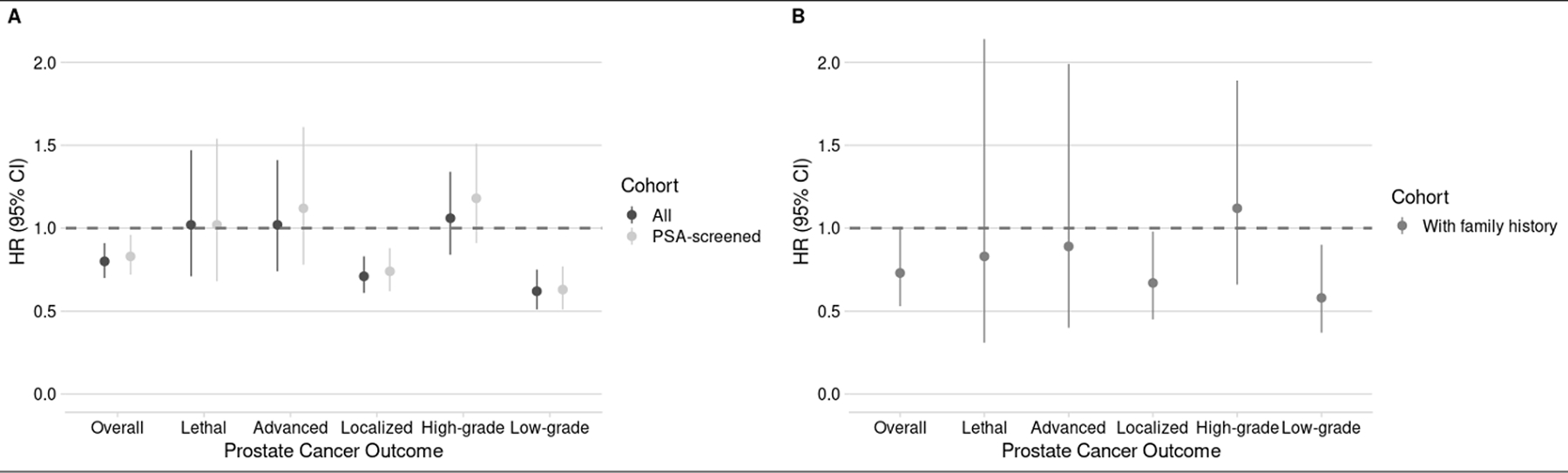
Hazard ratios (HR) and 95% confidence intervals (CI) for the association between ever use of 5-ARIs and prostate cancer outcomes. (A) HRs and 95% CIs for all 38,037 men in the study population and the subset of 22,424 men who had PSA screening at baseline. (B) HRs and 95% CIs for 4,824 men who have a family history fo prostate cancer in their father or brother. (Note: High-grade is Gleason score 4+3 and higher; low-grade is Gleason score 3+4 and lower.)
In 4,824 men with a family history of prostate cancer, we found 5-ARI use reduced risk of all prostate cancer by 27%, localized disease by 33% and low-grade disease by 42% without increasing risk of lethal disease (Figure 1B; Supplementary Table 2).
The alpha-blocker cohort analysis showed that the 5-ARI results were likely not influenced by diagnostic intensity, as alpha-blocker use was not appreciably associated with a decreased risk of overall, localized, or low-grade prostate cancer (Supplementary Table 3). Furthermore, there was an inverse association between alpha-blocker use and developing high-grade prostate cancer.
In the case-only cohort, a Fine-Gray competing risk model, which models a world free from death from other causes (Supplementary Table 4), showed no association between ever using 5-ARIs and developing lethal prostate cancer (sHR 0.81, 0.49–1.33).
Discussion
We found no increased risk of lethal prostate cancer among cancer-free men using 5-ARIs nor an increased risk of death or progression to lethal disease in 5-ARI users with localized/locally advanced cancer at diagnosis. Our findings align with the PCPT cohort analysis, which found no excess risk of prostate cancer death. Additionally, we found 5-ARI users had a lower risk of low-grade and localized prostate cancer. We found no significant association between use of 5-ARIs and risk of high-grade or advanced disease. Men on 5-ARIs had greater screening and interactions with the healthcare system, as evidenced by higher prevalence of PSA screening (prevalence difference 16%, 95% CI 15–18%), prostate exams (10%, 8–11), and prostate biopsies (11%, 10–13), which could have influenced our results.
To understand the relationship between 5-ARIs and prostate cancer mortality, findings from the PCPT and VA studies must be considered in the context of their strengths and limitations. The PCPT was a randomized study design, which reduces bias due to confounding; however, all PCPT participants received a planned prostate biopsy by the end of follow-up. This is a major difference from observational data and could lead to earlier detection regardless of 5-ARI use. The VA study found men on 5-ARIs had delayed diagnostic biopsy, were more likely to present with high-grade disease, had higher PSA values and higher prostate cancer mortality. It is possible that, in the observational VA study, 5-ARI-related PSA suppression was not properly accounted for in screening, and so men presented with higher risk disease. In HPFS, 5-ARI users had similar unadjusted PSA levels at diagnosis to 5-ARI never users (8.9 vs. 8.8 ng/mL) and also had more interactions with healthcare providers including screening and biopsy. Therefore, it is possible their diagnoses were not delayed, leading to no difference in stage or grade at presentation, and ultimately no difference in mortality.
Our findings for a reduction of overall and low grade cancers are like those from both PCPT and REDUCE25 (Reduction by Dutasteride of Prostate Cancer Events), a randomized, double-blind trial comparing dutasteride with placebo in prostate cancer incidence. The reduction in less aggressive tumors without an increase in high-grade cancers has several implications. Early diagnosis due to PSA screening has led to over-detection of cancers, particularly low-grade disease. Patients with cancer that is not clinically significant could have an improved quality of life by saving money on healthcare costs and avoiding side effects that accompany unnecessary treatment and testing.
An observational study in Sweden examined 5-ARIs and prostate cancer among 89,000 participants, specifically examining prostate cancer mortality differences between users and nonusers in the same Gleason Grade Groups 26. Similar to our findings, there was no evidence of increased mortality associated with 5-ARIs in men with high or low Gleason scores. In contrast to our study, the Swedish study found a higher proportion of high-grade cases among 5-ARI users compared to non-users, but this could be due to differences in clinical presentation and follow-up of our study populations, or the length of follow-up.
Despite evidence in favor of 5-ARIs for chemoprevention, it is important to consider potential side effects of 5-ARIs. Some prior studies have shown increased risks of depression27,28; however, a study on psychological adverse events in patients treated with finasteride suggested the association between depression and suicidality and finasteride was likely due to reporting bias29. Sexual dysfunction and other symptoms have been noted with mixed evidence30,31. Still, the reduction in overall and low-risk prostate cancer may be useful in select populations32–35.
Strengths of this study include its prospective nature, large sample size and number of events, and long-term and complete follow-up for two decades. Biennial questionnaires captured time-varying exposure and covariate data and had >90% participant response. Information on PSA screening and healthcare interactions allowed us to assess the potential for diagnostic bias and to interpret findings in the context of regular access to healthcare. Furthermore, this study avoids the issue of prevalent use because FDA approval for Proscar occurred shortly before the start of the study. The results of this study should be interpreted in the context of its limitations. Although survey findings were self-reported, they remain high quality due to the study participants being health professionals and high participation rates across the study. The generalizability may be limited by the fact that the cohort consists predominantly of non-Hispanic white men, and it would be important to address this hypothesis in a multiracial/ethnic setting.
Taken together, our results and the 2019 PCPT and VA studies emphasize the importance of real-world data in framing the benefits and risks associated with 5-ARIs. Our results contribute evidence that 5-ARI use is safe with respect to prostate cancer mortality, in concert with proper healthcare follow-up. Physicians must be aware that adjustment of PSA level is required for patients on 5-ARIs and that persistent increase in PSA levels of these patients should prompt close follow-up9. This should alleviate concerns in settings of 5-ARI use for BPH and alopecia and encourage further discussion on 5-ARIs for chemoprevention. The benefit of 5-ARIs reducing the risk of low-risk cancers, particularly among populations at high-risk for prostate cancer, should be weighed against its potential side effects.
Supplementary Material
Acknowledgments
We thank the participants and staff of the HPFS and the PHS for their valuable contributions. In particular, we would like to recognize the contributions of Liza Gazeeva, Siobhan Saint-Surin, Ruifeng Li, Robert Sheahan, Betsy Frost-Hawes, and Eleni Konstantis. We would like to thank the following state cancer registries for their help: AL, AZ, AR, CA, CO, CT, DE, FL, GA, ID, IL, IN, IA, KY, LA, ME, MD, MA, MI, NE, NH, NJ, NY, NC, ND, OH, OK, OR, PA, RI, SC, TN, TX, VA, WA, and WY. The authors assume full responsibility for analyses and interpretation of these data.
Funding
The Health Professionals Follow-up Study is supported by a grant from the National Cancer Institute (U01 167552). KHS and CHP were supported by the Department of Defense (Early-Investigator Research Award W81XWH-18-1-0330 and W81XWH-19-1-0412). KMW, KHS, MAP, and LAM were supported by the Prostate Cancer Foundation Young Investigator Award. MAP was supported by the American Urologic Association Research Scholars Program. AP was supported by the Swedish Society for Medical Research. AFO was supported by NIH R01DK124502. EMR was supported by the Program for Training in Cancer Epidemiology (T32CA009001).
Footnotes
Author disclosures
LA Mucci has been a paid consultant for Bayer Pharmaceutical and has given Expert testimony on behalf of Bayer. She receives research funding support from Astra Zeneca and Janssen. She is co-PI of a research study funded by Sanofi, Bayer, Astra Zeneca, and Janssen. The authors declare no potential conflicts of interest in this study.
References
- 1.American Cancer Society. American Cancer Society: Cancer Facts & Statistics. https://cancerstatisticscenter.cancer.org/. Published 2020. Accessed.
- 2.Fitzpatrick JM, Schulman C, Zlotta AR, Schroder FH. Prostate cancer: a serious disease suitable for prevention. BJU Int. 2009;103(7):864–870. [DOI] [PubMed] [Google Scholar]
- 3.Thomas LN, Douglas RC, Lazier CB, Too CK, Rittmaster RS, Tindall DJ. Type 1 and type 2 5alpha-reductase expression in the development and progression of prostate cancer. Eur Urol. 2008;53(2):244–252. [DOI] [PubMed] [Google Scholar]
- 4.McConnell JD, Bruskewitz R, Walsh P, et al. The effect of finasteride on the risk of acute urinary retention and the need for surgical treatment among men with benign prostatic hyperplasia. Finasteride Long-Term Efficacy and Safety Study Group. N Engl J Med. 1998;338(9):557–563. [DOI] [PubMed] [Google Scholar]
- 5.McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349(25):2387–2398. [DOI] [PubMed] [Google Scholar]
- 6.Niu Y, Ge R, Hu L, et al. Reduced levels of 5-alpha reductase 2 in adult prostate tissue and implications for BPH therapy. Prostate. 2011;71(12):1317–1324. [DOI] [PubMed] [Google Scholar]
- 7.McConnell JD, Wilson JD, George FW, Geller J, Pappas F, Stoner E. Finasteride, an inhibitor of 5 alpha-reductase, suppresses prostatic dihydrotestosterone in men with benign prostatic hyperplasia. J Clin Endocrinol Metab. 1992;74(3):505–508. [DOI] [PubMed] [Google Scholar]
- 8.Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349(3):215–224. [DOI] [PubMed] [Google Scholar]
- 9.Theoret MR, Ning YM, Zhang JJ, Justice R, Keegan P, Pazdur R. The risks and benefits of 5alpha-reductase inhibitors for prostate-cancer prevention. N Engl J Med. 2011;365(2):97–99. [DOI] [PubMed] [Google Scholar]
- 10.Thompson IM, Tangen CM, Goodman PJ, et al. Finasteride improves the sensitivity of digital rectal examination for prostate cancer detection. J Urol. 2007;177(5):1749–1752. [DOI] [PubMed] [Google Scholar]
- 11.Lucia MS, Darke AK, Goodman PJ, et al. Pathologic characteristics of cancers detected in The Prostate Cancer Prevention Trial: implications for prostate cancer detection and chemoprevention. Cancer Prev Res (Phila) 2008;1(3):167–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Andriole GL, Guess HA, Epstein JI, et al. Treatment with finasteride preserves usefulness of prostate-specific antigen in the detection of prostate cancer: results of a randomized, double-blind, placebo-controlled clinical trial. PLESS Study Group. Proscar Long-term Efficacy and Safety Study. Urology. 1998;52(2):195–201; discussion 201–192. [DOI] [PubMed] [Google Scholar]
- 13.Pinsky PF, Black A, Grubb R, et al. Projecting prostate cancer mortality in the PCPT and REDUCE chemoprevention trials. Cancer. 2013;119(3):593–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Robinson D, Garmo H, Bill-Axelson A, Mucci L, Holmberg L, Stattin P. Use of 5alpha-reductase inhibitors for lower urinary tract symptoms and risk of prostate cancer in Swedish men: nationwide, population based case-control study. BMJ. 2013;346:f3406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Thompson IM Jr., Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med. 2013;369(7):603–610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Goodman PJ, Tangen CM, Darke AK, et al. Long-Term Effects of Finasteride on Prostate Cancer Mortality. N Engl J Med. 2019;380(4):393–394. [DOI] [PubMed] [Google Scholar]
- 17.Sarkar RR, Parsons JK, Bryant AK, et al. Association of Treatment With 5alpha-Reductase Inhibitors With Time to Diagnosis and Mortality in Prostate Cancer. JAMA Intern Med. 2019;179(6):812–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kasper JS, Liu Y, Giovannucci E. Diabetes mellitus and risk of prostate cancer in the health professionals follow-up study. Int J Cancer. 2009;124(6):1398–1403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kenfield SA, Stampfer MJ, Chan JM, Giovannucci E. Smoking and prostate cancer survival and recurrence. JAMA. 2011;305(24):2548–2555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wilson KM, Kasperzyk JL, Rider JR, et al. Coffee consumption and prostate cancer risk and progression in the Health Professionals Follow-up Study. J Natl Cancer Inst. 2011;103(11):876–884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Platz EA, Leitzmann MF, Visvanathan K, et al. Statin drugs and risk of advanced prostate cancer. J Natl Cancer Inst. 2006;98(24):1819–1825. [DOI] [PubMed] [Google Scholar]
- 22.Platz EA, Yegnasubramanian S, Liu JO, et al. A novel two-stage, transdisciplinary study identifies digoxin as a possible drug for prostate cancer treatment. Cancer Discov. 2011;1(1):68–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hamilton RJ, Kahwati LC, Kinsinger LS. Knowledge and use of finasteride for the prevention of prostate cancer. Cancer Epidemiol Biomarkers Prev. 2010;19(9):2164–2171. [DOI] [PubMed] [Google Scholar]
- 24.Stampfer MJ, Willett WC, Speizer FE, et al. Test of the National Death Index. Am J Epidemiol. 1984;119(5):837–839. [DOI] [PubMed] [Google Scholar]
- 25.Andriole GL, Bostwick DG, Brawley OW, et al. Effect of dutasteride on the risk of prostate cancer. N Engl J Med. 2010;362(13):1192–1202. [DOI] [PubMed] [Google Scholar]
- 26.Bonde Miranda T, Garmo H, Stattin P, Robinson D. 5alpha-Reductase Inhibitors and Risk of Prostate Cancer Death. J Urol. 2020;204(4):714–719. [DOI] [PubMed] [Google Scholar]
- 27.Unger JM, Till C, Thompson IM Jr., et al. Long-term Consequences of Finasteride vs Placebo in the Prostate Cancer Prevention Trial. J Natl Cancer Inst. 2016;108(12). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rahimi-Ardabili B, Pourandarjani R, Habibollahi P, Mualeki A. Finasteride induced depression: a prospective study. BMC Clin Pharmacol. 2006;6:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nguyen DD, Marchese M, Cone EB, et al. Investigation of Suicidality and Psychological Adverse Events in Patients Treated With Finasteride. JAMA Dermatol. 2021;157(1):35–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Baas WR, Butcher MJ, Lwin A, et al. A Review of the FAERS Data on 5-Alpha Reductase Inhibitors: Implications for Postfinasteride Syndrome. Urology. 2018;120:143–149. [DOI] [PubMed] [Google Scholar]
- 31.Hagberg KW, Divan HA, Persson R, Nickel JC, Jick SS. Risk of erectile dysfunction associated with use of 5-alpha reductase inhibitors for benign prostatic hyperplasia or alopecia: population based studies using the Clinical Practice Research Datalink. BMJ. 2016;354:i4823. [DOI] [PubMed] [Google Scholar]
- 32.Margel D, Fleshner N. The role of 5-alpha-reductase inhibitors in active surveillance. Curr Opin Urol. 2012;22(3):243–246. [DOI] [PubMed] [Google Scholar]
- 33.Wong LM, Fleshner N, Finelli A. Impact of 5-alpha reductase inhibitors on men followed by active surveillance for prostate cancer: a time-dependent covariate reanalysis. Eur Urol. 2013;64(2):343. [DOI] [PubMed] [Google Scholar]
- 34.Ross AE, Feng Z, Pierorazio PM, et al. Effect of treatment with 5-alpha reductase inhibitors on progression in monitored men with favourable-risk prostate cancer. BJU Int. 2012;110(5):651–657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fleshner NE, Lucia MS, Egerdie B, et al. Dutasteride in localised prostate cancer management: the REDEEM randomised, double-blind, placebo-controlled trial. Lancet. 2012;379(9821):1103–1111. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data generated in this study are available upon request from the corresponding author.