

Abstract
Fostamatinib is the first approved spleen tyrosine kinase inhibitor for chronic immune thrombocytopenia. This review summarizes the clinical development, pharmacokinetics, pharmacodynamics, drug–drug interactions, adverse events, and comprehensive analyses of fostamatinib. While integrating these findings, we discuss the fostering and improvement of fostamatinib for further clinical applications. Fostamatinib is designed as a prodrug and cleavage of its active moiety R406 in the intestine. As R406 is the major product in the blood, this review mainly discusses the pharmacokinetics and pharmacodynamics of R406. It is metabolized by cytochrome 3A4 and UGT1A9 in the liver and is dominantly excreted in feces after anaerobic modification by the gut microbiota. As fostamatinib and R406 strongly inhibit the breast cancer resistance protein, the interaction with those substrates, particularly statins, should be carefully monitored. In patients with immune thrombocytopenia, fostamatinib administration started at 100 mg twice daily, and most patients increased to 150 mg twice daily in the clinical trial. Although responders showed a higher R406 concentration than non-responders, the correlation between R406 exposure and achievement of the platelet count as a pharmacodynamic marker was uncertain in the pharmacokinetic/pharmacodynamic analysis. Additionally, R406 concentration was almost halved in patients with a heavy body weight; hence, the exposure-efficacy study for suitable dosing should be continued with post-marketing data. In contrast, the pharmacokinetic/pharmacodynamic analysis for exposure safety revealed that R406 exposure significantly correlated with the incidence of hypertension. Even though the influence of elevated exposure on other toxicities, including diarrhea and neutropenia, is still unclear, careful management is required with dose escalation to avoid toxicity-related discontinuation.
Key Points
| Fostamatinib is a prodrug rapidly cleaved by alkaline phosphatase in the intestine to its active moiety R406. R406 has a high protein binding ratio and is mainly metabolized by cytochrome P450 3A4 and UGT1A9 in the liver and excreted into feces. |
| R406 is a substrate of P-glycoprotein, whereas fostamatinib and R406 inhibit breast cancer resistance protein with high intestinal concentration/IC50 values. Great attention should be paid to the drug–drug interactions with the substrates of these transporters, especially statins. |
| Fostamatinib dosage can be increased during treatment. Whereas a R406 exposure-dependent increase in efficacy was not clear; a significant correlation between systemic exposure and adverse events such as hypertension has been reported. During the dose escalation, careful management is required to avoid toxicity-related treatment discontinuation. |
Introduction
In April 2018, the US Food and Drug Administration (FDA) approved fostamatinib disodium (Tavalisse®), which is the first known agent to target spleen tyrosine kinase (Syk), for the treatment of chronic immune thrombocytopenia (ITP) [1, 2]. Spleen tyrosine kinase is a cytoplasmic non-receptor protein tyrosine kinase that was first discovered in the early 1990s [3, 4]. The human SYK gene is located on chromosome 9q22, and its coding sequence is 1908 bp long and encodes a 635 amino acid polypeptide with an estimated molecular weight of 72 kDa [4, 5]. Spleen tyrosine kinase is widely expressed in hematopoietic lineage cells, and its function in the adaptive immune system as a mediator of antigen-associated signals has been extensively studied [6, 7]. Spleen tyrosine kinase is considered a possible therapeutic target for treating antibody-mediated and immune-complex-mediated diseases, including allergic and autoimmune conditions.
Fostamatinib is an orally available, small-molecule Syk inhibitor drug that is prescribed as a new treatment option to patients with ITP who have had an insufficient response to a previous treatment [8]. Immune thrombocytopenia is an acquired autoimmune bleeding disorder characterized by a low platelet count resulting from increased platelet destruction and impaired platelet production [9]. The incidence rates of ITP appear to have a bimodal distribution, with peaks among children and adults [10, 11]. In adults newly diagnosed with ITP, clinical guidelines recommend corticosteroid treatment as first-line therapy. For the patients who are corticosteroid dependent or show no response to corticosteroids, the guidelines recommend the thrombopoietin receptor agonist, rituximab, and splenectomy as second-line therapy [9]. Although the most important treatment goal for patients with ITP is to maintain their platelet count and avoid major bleeding events, a certain proportion of patients, particularly those with persistent or chronic ITP, remain refractory to treatment. Additional therapeutic approaches using agents with different mechanisms of action, such as the novel Syk inhibitor fostamatinib, have essential clinical roles [12]. Although fostamatinib showed a 44% overall response rate in patients with refractory ITP in phase III trials [13], non-responders were also present. In addition, adverse events (AEs) have been reported in approximately 90% of the patients in clinical trials [13]. Further studies are needed to elucidate more information on such drugs from the perspective of pharmacokinetics and pharmacodynamics.
This review provides an overview of the clinical pharmacokinetics and pharmacodynamics of fostamatinib and its active moiety R406. As fostamatinib was developed as a prodrug, R406 plays an essential role in its pharmacokinetics and pharmacodynamics. Fostamatinib was initially developed for rheumatoid arthritis (RA); therefore, this review includes the trial results in patients with RA and those in patients with ITP. In considering the clinical development, pharmacodynamics, pharmacokinetics, safety profile, and integrated investigations of fostamatinib such as population pharmacokinetic (PK) and PK/pharmacodynamic (PD) analyses, we discuss the fostering and improvement of fostamatinib for clinical applications.
Clinical Development of Fostamatinib
Initially, fostamatinib was developed as a new treatment option for RA, as there was ample evidence to support the role of Syk in amplifying inflammation in the synovium. Furthermore, R406 significantly suppressed clinical arthritis and synovitis in rats [14]. Two placebo-controlled phase II trials were designed for patients with RA, wherein they were administered fostamatinib with a combination of methotrexate (MTX) daily (NCT00326339: fostamatinib 50 mg, 100 mg, and 150 mg twice daily [BID], and NCT00665925: fostamatinib 150 mg once daily [QD] and 100 mg BID) [15, 16]. Fostamatinib with MTX significantly improved the American College of Rheumatology 20% response criteria (ACR20) at week 12 compared with those in the MTX group, and the response rate of ACR20 increased in a dose-dependent manner (NCT00326339: 65% with the 100-mg BID group and 72% with the 150-mg BID group at 3 months; NCT00326339: 57% with the 150-mg QD group and 67% with the 100-mg BID group at 6 months) [15–17]. Based on these trials, one phase IIb and three phase III studies, named OSKIRA, were designed. In OSKIRA-1 and OSKIRA-2, fostamatinib improved ACR20 at week 24 in combination with MTX (NCT01197521) and disease-modifying antirheumatic drugs (NCT01197534) (Fig. 1a) [18, 19]. In addition, fostamatinib increased ACR20 in patients inadequately responding to MTX and tumor necrosis factor-α antagonists in the OSKIRA-3 trial (NCT01197755) [20]. In addition, the efficacy and safety of fostamatinib monotherapy were compared with those of adalimumab, an anti-tumor necrosis factor-α antibody, in the OSKIRA-4 study (NCT01264770). In this trial, fostamatinib was found to be inferior to adalimumab with regard to the efficacy score at week 24, and also showed a higher incidence of treatment discontinuation because of AEs (fostamatinib, 12.5–16.7%, adalimumab, none) [21]. Based on these results, regulatory filings for fostamatinib were withheld in RA [21].
Fig. 1.
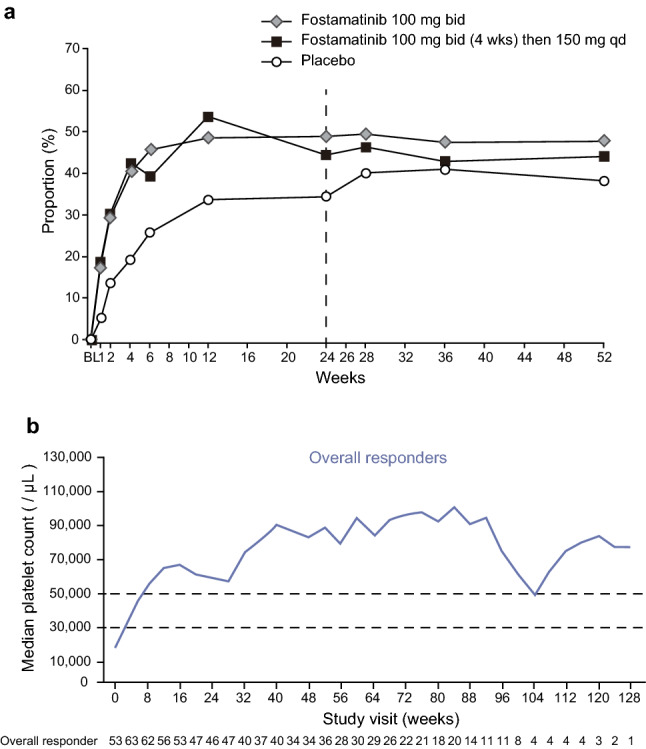
Changes in pharmacodynamic markers over time during fostamatinib treatment. a American College of Rheumatology 20% improvement response rates over time in a phase III randomized clinical trial in patients with rheumatoid arthritis. Republished with permission of John Wiley & Sons [18]; permission conveyed through
Copyright Clearance Center, Inc. b Median platelet levels over time in a phase III clinical trial for immune thrombocytopenia patients. Republished with permission of John Wiley & Sons [13]; permission conveyed through Copyright Clearance Center, Inc. bid twice daily, qd once daily
Concurrently, Podolanczuk et al. showed that Syk inhibition by fostamatinib inhibited platelet phagocytosis by macrophages, and this proof of concept was initially realized in clinical practice in 2009 [22]. They conducted a single-arm, dose-escalation phase II trial to assess the efficacy and safety of fostamatinib in adult refractory ITP (NCT00706342). The trial was initiated at 75 mg BID, and the dosage increased to 175 mg BID unless toxicity occurred, or a persistent response was observed. Twelve out of 16 patients responded to fostamatinib, and the efficacy was sustained in eight patients [22]. Following this success, two parallel phase III, randomized, double-blind, placebo-controlled studies named FIT1 (NCT02076399) and FIT2 (NCT02076412) were conducted [8]. Patients with persistent or chronic ITP were randomized in the ratio of 2:1 to receive either fostamatinib (n = 101) or placebo (n = 49) for 24 weeks. Fostamatinib was initially administered at 100 mg BID and could be increased to 150 mg BID after 4 weeks or later, depending on the therapeutic response. The primary endpoint was a stable response, defined by a platelet count of ≥ 50,000/μL by week 24. The overall response was fostamatinib 43% versus placebo 14% in FIT1 and FIT2 pooled subjects; thus, fostamatinib significantly ameliorated the platelet count and met the primary endpoint [8]. A total of 123 patients were enrolled in FIT3 (NCT02077192), which is a long-term follow-up, open-label extension study, and the results showed durability of stable and overall platelet responses, with the median ongoing at over 28 months (Fig. 1b) [13]. Consequently, fostamatinib was approved by the FDA in 2018 and the European Medicines Agency in 2020 as a promising treatment for patients with chronic or persistent ITP with a new therapeutic scheme.
In addition, clinical trials such as the OSKIRA-ASIA-1 (NCT01569074) and OSKIRA-ASIA-1X study (NCT01640054) were conducted in 2021 for Asian patients with RA [23]. In addition to RA and ITP, fostamatinib has been considered efficacious for the treatment of warm antibody autoimmune hemolytic anemia [24, 25], hematologic malignancies [26, 27], immunoglobulin A nephropathy [28–31], and coronavirus disease 2019 [32–34]. For further clinical development of fostamatinib and more effective and safer treatment of patients with ITP, we need to reconsider the PK and PD data obtained in RA and ITP and discuss their correlation with efficacy and safety.
Fostamatinib Pharmacology and Pharmacodynamics
The active metabolite of fostamatinib, R406 [N4-(2,2-dimethyl-3-oxo-4H-pyrid [1, 4] oxazin-6-yl)-5-fluoro-N2-(3,4,5-trimethoxyphenyl)-2,4-pyrimidinediamine], was initially identified during the drug screening of immunoglobulin E and immunoglobulin G-mediated activation of the receptor for the Fc region of immunoglobulin E (Fcε-receptor I) and receptor for the Fc region of immunoglobulin G (Fcγ-receptor, FcγR) signaling in cultured human mast cells. A further in vitro assessment revealed that R406 blocked Syk activation, resulting in the inhibition of immunoglobulin receptor signaling [35].
Physiologically, Syk plays an essential role in signal transduction via both immunoglobulin receptors and the B-cell receptor (BCR) [6]. Activation of Syk-mediated signaling primarily leads to interaction between the immunoreceptor tyrosine-based activation motifs of BCR or FcγR and Lyn, a tyrosine kinase of the Src family. Activated Lyn then phosphorylates another ITAM region and interacts with activated Syk, which is also phosphorylated by Lyn. Sequentially, Syk phosphorylates the adaptor molecule linker for activation of T cells (LAT), which results in cellular processes such as chemokine release, actin cytoskeletal rearrangement, proliferation or differentiation, and cell survival [6, 36].
R406 inhibits the phosphorylation of LAT (Y191), but not that of Syk (Y352) and Lyn-dependent phosphorylation of ITAM. This strongly suggests that R406 is a potent inhibitor of Syk kinase activity [35]. Moreover, an enzyme kinetic assay and crystallography of R406-bound Syk protein revealed that R406 competitively inhibits ATP binding, with a Ki of 30 nM [35, 37]. Additionally, R406 inhibits immunoglobulin G and FcγR-mediated cytokine release in macrophages (EC50 = 111 nM) and oxidative burst in neutrophils (EC50 = 33 nM) [35]. To confirm the R406 effect on immune complex-mediated inflammation in vivo, a reverse passive Arthus reaction, a classical experimental model of type III allergic reaction, was performed in mice. A 1-hour pre-treatment of R406 at 1 and 5 mg/kg before the immune complex challenge inhibited the cutaneous Arthus reaction by approximately 72% and 86%, respectively [35]. As FcγR signaling in synovial macrophages is an important pathophysiological mechanism of RA, R406 (5 and 10 mg/kg) was administered in mouse models. R406 significantly reduced inflammation and swelling, and the progression of arthritis was slower in the treatment groups than in the vehicle group [35]. To further understand the suitability of R406 in human studies, the basophil activation test was conducted in healthy volunteers. After administering a single dose of R406 (80, 250, 400, 500, and 600 mg), heparinized blood was collected at several timepoints and stimulated ex vivo with anti-immunoglobulin E to assess the cluster of differentiation 63 upregulation on the cell surface of basophils as proof of activation of Fcε-receptor I signaling. R406 significantly suppressed cluster of differentiation 63 expression in a dose-dependent manner (Fig. 2). This pharmacological effect was also correlated with the plasma concentration of R406, and a 50% reduction in basophil activation was observed at 496 ± 42 ng/mL, which is equivalent to an EC50 of 1.06 µM [35]. The disparity in EC50 values between the in vitro (33–111 nM) and in vivo (1.06 µM) assays may attribute to a high protein binding ratio of R406 (> 98%). Braselmann et al. reported that a comparable shift of EC50 was observed when human serum was added to an in vitro assay system [35]. In addition, the in vivo EC50 496 ng/mL (1.06 µM) is calculated to approximately 12,000 ng·h/mL as the daily area under the plasma concentration–time curve in steady state (DAUCss). In the phase IIb studies in patients with RA, DAUCss of R406 was 12,000–13,000 ng·h/mL following 100 mg BID [38]. These results suggest that an initial dose of fostamatinib could generate an effective R406 concentration to inhibit Syk signaling from the PD view.
Fig. 2.
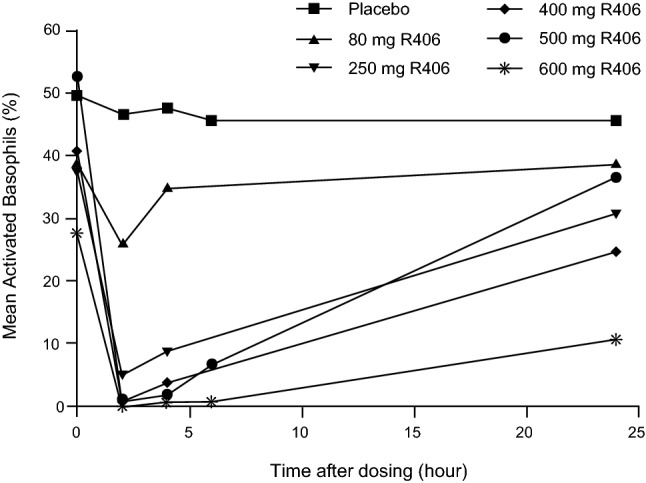
Changes in basophil activation in the dose-dependent manner. Dose-dependent inhibition of basophil activation was observed after single dosing of R406 in healthy human volunteers. Heparinized blood was stimulated ex vivo with α immunoglobulin E, and changes in cell surface expression of CD63 were measured by flow cytometry. Republished with permission of American Society for Pharmacology and Experimental Therapeutics [35]; permission conveyed through
Copyright Clearance Center, Inc.
As Syk kinase is also known to play a role in platelet coagulation via the ITAM-containing collagen receptor (glycoprotein VI) and some specific integrins (αIIbβ3) [39], the effect of R406 on hemostasis has been assessed in previous studies. In the tail-tip amputation assay in mice, high systemic exposure of R406 did not negatively affect bleeding times compared to that with aspirin as a positive control. In a clinical trial, collagen-induced and ADP-induced platelet aggregation was assessed using platelet-rich plasma prepared from R406-administered healthy volunteers; however, even at the highest dose of R406, platelet aggregation was not inhibited [35].
Pharmacological profiling, including the off-target inhibition of other proteins, may contribute to the identification of the mechanism underlying beneficial and adverse effects. R406 acts as a potent antagonist of the adenosine A3 receptor in the range relevant to clinical effects (IC50 = 18 nM) [40]. Four adenosine receptor subtypes (A1, A2a, A2b, and A3) are expressed in the lungs and are targets for drug development against human asthma [41, 42]. In addition, Matsubara et al. reported that Syk inhibition by R406 in dendritic cells and mast cells prevents allergen-induced airway hyperresponsiveness and airway inflammation in an experimental mouse model [43, 44]. Based on these two separate mechanisms of action, fostamatinib and R406 may represent a promising therapeutic option for the treatment of allergic asthma; however, further studies are needed.
R406 has a low selectivity for binding to the kinase domain, and it can bind a variety of protein kinases at therapeutically relevant concentrations [40]. Previous studies reported that R406 has inhibitory effects on vascular endothelial growth factor receptor (VEGFR)-1, VEGFR-2, proto-oncogene tyrosine-protein kinase SRC, and tyrosine-protein kinase KIT [40]. These inhibitory effects may cause an increase in blood pressure (BP) as well as the use of other tyrosine kinase inhibitors [45]. In fact, treatment with R406 inhibits VEGF-induced tube formation in vascular endothelial cells in vitro [40]. In vivo experiments in rodents showed that mean arterial BP was significantly increased when fostamatinib was administered at 10, 30, and 100 mg/kg [46]. Hypertension was one of the major AEs associated with fostamatinib use in clinical trials [8]. Even though these off-target AEs could be controlled by withdrawal or a dose reduction of fostamatinib, or the addition of antihypertensive drugs [8, 13, 47], the dose-dependent elevation of BP was observed in rodents [46]; its relevance to the pharmacokinetics should be further evaluated for the safety management of fostamatinib.
Fostamatinib Pharmacokinetics
Absorption
Considering the low aqueous solubility of R406, fostamatinib was synthesized and tested in preclinical and clinical studies [48]. Fostamatinib was designed as a methylene-phosphate prodrug that is cleaved by alkaline phosphatase at the apical brush-border membranes of intestinal enterocytes to its active moiety R406, as shown in Fig. 3 [48]. After oral administration, fostamatinib was rapidly and completely hydrolyzed to R406 and absorbed within 1–2 h, and negligible concentrations of fostamatinib were found in the plasma. The absolute bioavailability of R406 is determined to be 55% after a single oral dose of 150 mg of fostamatinib and a 100-µg intravenous dose of R406 in healthy subjects [49–51]. Several studies investigated whether R406 and fostamatinib were a substrate of absorption-related transporters. An in vitro assay using a polarized Caco-2 cell monolayer showed that R406 is a substrate of P-glycoprotein (P-gp) from the basolateral to the apical compartment in a concentration-dependent manner [52]. In contrast, another in vitro assay showed that breast cancer resistance protein (BCRP) did not transport R406 and fostamatinib [49].
Fig. 3.

Graphical scheme of fostamatinib pharmacokinetics. Fostamatinib was designed as a prodrug cleaved to R406 by alkaline phosphatase in the intestine. R406 was mainly metabolized by cytochrome P450 (CYP) 3A4 and UGT1A9 in the liver. In human plasma, R406 and other three metabolites (M647, M633, and M537) were detected; however, these three accounted for less than 3%. In the human mass balance study, almost 80% of the radioactivity was recovered in feces, which consisted of two primary metabolites: one was R406 and the other was M413; the 3,5-benzene diol metabolite of R406. The other 20% of metabolites were eliminated into urine as an N-glucuronide R406 (M647)
A phase I study in healthy adults examined the effect of diet (high-fat or high-calorie breakfast) on the absorption of fostamatinib tablets [53]. Even though there was a decline in the rate of absorption, as shown by a delayed time to maximum concentration [tmax] (fasting: 1.39 h, fed: 3.22 h) and lower maximum concentration [Cmax] (fasting: 605 ng/mL, fed: 363 ng/mL), the area under the the plasma concentration–time curve from dosing to infinity (AUC0→∞) of R406 was similar (fasting: 6490 ng·h/mL, fed: 7140 ng·h/mL), and the 90% confidence interval for the ratio of the geometric means in both conditions was within the acceptable equivalency range (Table 1) [53].
Table 1.
Pharmacokinetic parameters of R406
| (i) Single dose in healthy subjects | Dosage (mg) | Analyte | Tmax (h) | Cmax (ng/mL) | AUC0→∞ (ng·h/mL) | t1/2 (h) | CL/F (L/min) | Vz/F (L) | References |
|---|---|---|---|---|---|---|---|---|---|
| R406 besylate in a TPGS/PG (40:60) solution | 80 (n = 5) | R406 | 1.30 ± 0.27 | 501 ± 128 | 4410 ± 997 | 14.5 ± 3.9 | 0.32 ± 0.07 | 409 ± 175 | [53] |
| 250 (n = 5) | R406 | 1.20 ± 0.27 | 2030 ± 489 | 18,100 ± 2930 | 14.9 ± 3.6 | 0.24 ± 0.04 | 306 ± 94.8 | ||
| 400 (n = 6) | R406 | 1.50 ± 0.27 | 3410 ± 745 | 34,900 ± 14,600 | 17.8 ± 10.6 | 0.22 ± 0.09 | 340 ± 276 | ||
| 500 (n = 5) | R406 | 1.10 ± 0.27 | 3660 ± 713 | 29,600 ± 6270 | 20.9 ± 5.8 | 0.29 ± 0.06 | 546 ± 249 | ||
| 600 (n = 6) | R406 | 1.25 ± 0.27 | 3920 ± 888 | 36,600 ± 7760 | 12.9 ± 5.9 | 0.29 ± 0.09 | 316 ± 146 | ||
| Fostamatinib in an aqueous suspension | 80 (n = 5) | R406 | 1.10 ± 0.22 | 306 ± 46.1 | 3150 ± 982 | 14.8 ± 4.7 | 0.45 ± 0.13 | 557 ± 166 | [53] |
| 250 (n = 5) | R406 | 1.60 ± 0.42 | 1140 ± 122 | 13,700 ± 3140 | 16.0 ± 2.8 | 0.32 ± 0.07 | 431 ± 82.0 | ||
| 400 (n = 5) | R406 | 1.60 ± 0.42 | 1220 ± 317 | 13,400 ± 4360 | 12.1 ± 2.0 | 0.54 ± 0.15 | 545 ± 109 | ||
| Fostamatinib in an aqueous suspension (fasted) | 100 (n = 6) | R406 | 1.17 ± 0.24 | 682 ± 187 | 7510 ± 1560 | 19.0 ± 4.3 | – | – | [53] |
| Fostamatinib in tablet (fasted) | 75 (n = 6) | R406 | 1.39 ± 0.74 | 605 ± 221 | 6490 ± 1750 | 17.9 ± 4.0 | – | – | |
| Fostamatinib in tablet (fed) | 75 (n = 6) | R406 | 3.22 ± 1.62 | 363 ± 94 | 7140 ± 1760 | 18.4 ± 5.0 | – | – |
| (ii) Single dose in special populations | Dosage (mg) | Analyte | Tmax (h) | Cmax (ng/mL) | AUC(0,∞) (ng·h/mL) | t1/2 (h) | CL/F (L/min) | Vz/F (L) | References |
|---|---|---|---|---|---|---|---|---|---|
| Fostamatinib for normal renal function | 150 (n = 8) | R406 | 2.50 | 690 | 6750 | 20.5 | – | – | [57] |
| Fostamatinib for moderate renal function | 150 (n = 8) | R406 | 2.50 | 425 | 6110 | 23.8 | – | – | |
| Fostamatinib for ESKD, post-dialysis dosing | 150 (n = 8) | R406 | 2.25 | 407 | 4950 | 19.6 | – | – | |
| Fostamatinib for ESKD, pre-dialysis dosing | 150 (n = 8) | R406 | 3.00 | 529 | 6280 | 22.1 | – | – | |
| Fostamatinib for normal hepatic function | 150 (n = 8) | R406 | 1.5 | 692 | 8970 | 19.4 | – | – | [57] |
| Fostamatinib for mild (Child-Pugh class A) | 150 (n = 8) | R406 | 2.5 | 615 | 6390 | 16.7 | – | – | |
| Fostamatinib for moderate (Child-Pugh class B) | 150 (n = 8) | R406 | 1.75 | 602 | 6860 | 16.1 | – | – | |
| Fostamatinib for severe (Child-Pugh class C) | 150 (n = 8) | R406 | 1.5 | 582 | 9490 | 19.2 | – | – |
| (iii) Single and multiple dosing in healthy subjects | Dosage (mg) | Analyte | Tmax (h) | Cmax (ng/mL) | AUC(0,∞) (ng·h/mL) | t1/2 (h) | CL/F (L/min) | Vz/F (L) | References |
|---|---|---|---|---|---|---|---|---|---|
| Fostamatinib in an aqueous suspension: day 1 | 160 BID (n = 6) | R406 | 1.25 ± 0.42 | 747 ± 286 | 8250 ± 3970 | 19.9 ± 9.2 | – | – | [53] |
| Fostamatinib in an aqueous suspension: day 7 | 160 BID (n = 6) | R406 | 1.08 ± 0.20 | 1530 ± 534 | 19,900 ± 8750 | – | – | – |
| (iv) Single and multiple dosing in patients with RA | Dosage (mg) | Analyte | Tmax (h) | Cmax (ng/mL) | AUC(0,∞) (ng·h/mL) | t1/2 (h) | CL/F (L/min) | Vz/F (L) | References |
|---|---|---|---|---|---|---|---|---|---|
| Fostamatinib in an aqueous suspension: day 1 | 100 BID (n = 12) | R406 | 1.00 ± 0.37 | 397 ± 177 | 3260 ± 990 | 14.5 ± 4.32 | – | – | [60] |
| Fostamatinib in an aqueous suspension: day 7 | 100 BID (n = 12) | R406 | 1.29 ± 0.40 | 761 ± 234 | NA | 20.4 ± 8.90 | – | – |
AUC0→∞ area under the plasma concentration–time curve from dosing to infinity, BID twice daily, CL/F apparent oral clearance, Cmax maximum concentration, ESKD end-stage kidney disease, Ref. reference, t1/2 terminal elimination half-life, Tmax time to Cmax, TPGS/PG d-alpha-tocopheryl-polyethylene-glycol-1000 succinate/propylene glycol, Vz/F apparent oral volume of distribution, NA not applicable
Distribution
R406 is distributed to extravascular sites and the volume of distribution at a steady state is found to be 256 ± 92 L, based on the results of the radiotracer study [50, 51]. An in vivo study showed that R406 is widely distributed in all tissues, with the exception of the central nervous system [54]. This could be explained by R406 being a substrate of P-gp, which acts as an efflux pump at the blood–brain barrier [52]. R406 distributes reversibly into the blood cell, and the red blood cell-to-plasma concentration ratio is approximately 2.6 [54, 55].
In vitro studies showed that R406 had a mean binding of 96.3% to purified human serum albumin (HSA) and that to purified alpha-1 acid glycoprotein was 75.5%; hence R406 is highly bound to plasma proteins [50, 51, 54]. Although HSA is known to have several drug-binding sites [56], the information on the binding sites of HSA and R406 is not available. When R406 was administered in combination with drugs that bind more tightly to the same site, an increase in the concentration of unbound R406 should be concerned. Moreover, low albumin levels associated with malnutrition or cirrhosis may also affect the increase in unbound R406 concentration. Martin et al. showed that the patients with cirrhosis had a higher unbound R406 ratio compared with healthy patients [57]. Further study is needed to explore the R406 binding site to HSA and the correlation between an elevated unbound R406 concentration and the frequency and severity of adverse events.
Metabolism
For evaluating the major metabolic pathways of R406, several in vitro studies and a human mass balance study in healthy subjects were performed [48]. A summary of the metabolic pathways after fostamatinib administration is shown in Fig. 3. After incubation of R406 with human hepatic microsomes in vitro, R406 levels gradually decreased, and the para-O-demethylated metabolite of R406 (R529) was identified. When the effects of the chemical inhibitors of cytochrome P450 [CYP] (ketoconazole, 3A4; furafylline, CYP1A2; quinidine, CYP2D6; sulfaphenazole, CYP2C9; and 3-N-benzylnirvanol, CYP2C19) on R406 metabolism were assessed, only ketoconazole could inhibit R529 production [48, 58]. Thus, R406 was predominantly metabolized by CYP3A4. Additionally, direct N-glucuronide conjugates of R406 (M647) were observed after incubation in hepatic microsomes with UDP-glucuronic acid, and further studies revealed that UGT1A9 was involved in this reaction [48, 54]. Consistent with in vitro findings, after C14-labeled fostamatinib was administered in a mass balance study, three minor peaks—M647, O-glucuronide conjugate R529 (M633), and sulfate conjugate of R529 (M537)—were identified [48]. However, these metabolites (M647, M633, and M537) accounted for less than 3% of the total radioisotopes in human plasma [48]. In summary, R406 is mainly metabolized by CYP3A4 and UGT1A9 in the liver. Although there is no information on which metabolic pathway predominantly metabolizes R406, a drug–drug interaction with CYP3A4 inhibitors and inducers should be considered in clinical practice.
Elimination
In the human mass balance study, 80% of the radioactivity was recovered in feces within 96 hours, and 19.3% was recovered in urine within 72 h. Therefore, hepatic clearance was a major clearance pathway of R406 [48]. In cynomolgus monkeys, 68.9% of the administered radioactivity was transported into the bile. Biliary metabolites consisted of M647, M633, and M537 [59]. In pooled feces, two major radioactive peaks were observed via liquid chromatography-tandem mass spectrometry; one was R406 (m/z 471), and the other was M413; the 3,5-benzene diol metabolite of R406. Although fostamatinib, R406, M647, and conjugates of R529 (M633 and M537) may all be present in the intestinal tract, production of M413 was observed only from R529 in the incubation of human feces under in vitro anaerobic conditions [48, 59]. These results indicate that the biliary metabolite (M647, M633, and M537) once hydrolyzed to R406 and R529, then R529 was O-demethylated and dehydroxylated by anaerobic gut bacteria. In urine, the major metabolite was M647, and a negligible level of R406 was detected (Fig. 3).
Among six healthy male subjects (aged 19–35 years) who participated in the mass balance study, the ratio of R406 to M413 in feces varied among the individuals (R406:M413; 1:0.18–11.6) [48]. This may be due to individual differences in the metabolic activity of CYP3A4, which metabolizes R406 to R529, or that of gut microbiota, which metabolizes R529 conjugates to M413. Given that R529 and its conjugates were not detected in feces, the occurrence of the former was more likely [48]. In addition, diarrhea is a common AE associated with fostamatinib therapy. Although the mechanism of this AE has not been elucidated, it cannot be denied that metabolites excreted and retained in the intestinal tract might cause intestinal toxicity. The relationship between diarrhea and the individual differences in fecal metabolites should be investigated.
PK Profiles in Healthy Volunteers and Patients
Baluom et al. reported three clinical studies to evaluate the human PK properties of R406 in healthy subjects [53]. The PK parameters are summarized in Table 1. The first was a single ascending dose (80, 250, 400, 500, 600 mg) study of orally administered R406 besylate formulated in a d-alpha-tocopheryl-polyethylene-glycol-1000 succinate/propylene glycol (40:60) solution. The concentration-time curve of R406 revealed a rapid absorption phase (tmax: 1.1–1.5 h) and a bi-phase decline in plasma concentrations (terminal elimination half-life [t1/2]: 12.9–20.9 h) [53]. The systemic exposure (Cmax and AUC0→∞) linearly increased when the dose ranged from 80 to 400 mg, although the exposure was essentially unchanged from 400-mg to 600-mg doses [53]. Second, they conducted a single oral dose study (80, 250, and 400 mg) and multiple repeated-dose studies (160 mg twice daily) of fostamatinib suspension. After administration, the R406 concentration reached a peak within 1–2 h, which was consistent with the results of R406 oral administration, indicating that fostamatinib was rapidly hydrolyzed and absorbed into the blood (Fig. 4) [53]. The linearity of R406 systemic exposure was observed only in the range of 80–250 mg of the fostamatinib dosage but not in 400 mg [53]. These results indicated that there was saturation of R406 absorption into the systemic circulation. Therefore, the initial dose of fostamatinib is set at between 100 and 250 mg in a clinical trial. Given that the active moiety, R406, and its N-glucuronide have existed in the intestinal tract, the possibility of entero-hepatic cycling and its effect on systemic circulation should be considered. Contrary to this expectation, the apparent secondary peak was not observed in the PK profile after fostamatinib oral administration in any phase I PK study (Fig. 4).
Fig. 4.
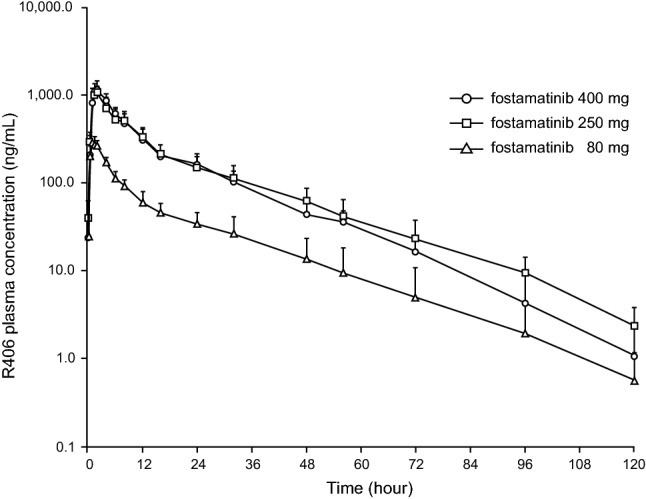
Plasma R406 concentration after a single oral administration of fostamatinib. Plasma R406 concentrations (ng/mL) in healthy human volunteers after an oral administration of a single dose of 80 mg, 250 mg, and 400 mg of fostamatinib in phase I clinical trial. Blood samples were collected at pre-dose, 0.25, 0.5, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 16, 24, 32, 48, 56, 72, 96, and 120 h after dosing.
Republished with permission of John Wiley & Sons [53]; permission conveyed through Copyright Clearance Center, Inc.
Absolute bioavailability was estimated at 55% according to the results of oral administration of fostamatinib 150 mg and intravenous administration of R406 100 µg. In this micro-dose intravenous study, t1/2 and clearance were 15.3 h and 15.7 L/h, respectively. These parameters were consistent with those in the dose-ascending trial and might suggest that saturation has not occurred in the metabolism and excretion in clinical doses of fostamatinib.
After repeated administration of fostamatinib 160 mg BID in healthy volunteers, an approximately 2-fold to 2.5-fold increase of R406 exposure was observed at day 7 as shown in Table 1, and fostamatinib achieved steady state following 3–4 days of administration BID [53]. As fostamatinib has been investigated for the treatment of RA, PK parameters of R406 were confirmed in patients who had stable disease with a weekly MTX regimen [60]. The PK parameters are shown in Table 1 and the data obtained from the patients were comparable to those from healthy volunteers [60].
PK Profiles in Special Populations
A phase I open-label clinical trial was performed to investigate the effect of renal or hepatic impairment on the R406 PK parameters [57]. Specifically, the criterion for renal function was determined by a creatinine clearance (mL/min) scale and dialysis requirements. The enrolled patients were divided into three groups (normal; 80 ≤ creatinine clearance, moderate; 30 ≤ creatinine clearance < 50, end-stage kidney disease; requiring hemodialysis). The results of the R406 PK parameters after a single oral dose of fostamatinib 150 mg are shown in Table 1. Each parameter indicated that fostamatinib could be administered regardless of the extent of renal impairment and the timing of hemodialysis in patients with end-stage kidney disease [57].
In addition, the criterion for hepatic impairment was determined based on the Child-Pugh score system, and the patients were divided into four groups (no hepatic impairment, mild; class A, moderate; class B, severe; class C). As hepatic metabolism by CYP3A4 and UGT1A9 is involved in the R406 pharmacokinetics [48], hepatic impairment could have a significant effect on its blood concentration; however, the PK parameters of R406 were consistent regardless of hepatic function, as shown in Table 1. Moreover, hypoalbuminemia due to hepatic impairment could influence the protein-binding rate, and unbound R406 concentration was also evaluated at 1, 6, and 24 h after fostamatinib administration. At all sampling times, the geometric mean of the unbound R406 ratio was the highest (60%) in the group with severe hepatic impairment compared with healthy patients [57]. Increased unbound drug concentrations could lead to individual differences in therapeutic efficacy and the incidence of AEs. Further analysis based on accumulated experience in clinical use to special populations is needed.
Drug–Drug Interactions
Several studies have examined the influence of drug–drug interactions of fostamatinib, and the results are summarized in Tables 2 and 3. As R406 is metabolized by CYP3A4 [48], CYP3A4 inhibitors or inducers may affect the R406 PK parameters. Martin et al. performed clinical studies of drug–drug interactions between fostamatinib and the CYP3A4 modulator ketoconazole (a potent inhibitor), verapamil (a moderate inhibitor), and rifampicin (an inducer) [58]. The co-administration of ketoconazole increased the R406 plasma concentration (Cmax and area under the plasma concentration–time curve [AUC]) and prolonged tmax and t1/2 [58]. Verapamil also increased AUC and t1/2, whereas there was no consistent effect on Cmax and tmax [58]. The co-administration of rifampicin was associated with a reduction of approximately 75% in AUC and 60% in Cmax of R406 [58]. CYP3A4 is also involved in the metabolism of oral contraceptives, especially ethinylestradiol. Concomitant dosage of fostamatinib and oral contraceptives significantly increased the Cmax and AUC of ethinylestradiol by 34.7% and 28.2%, respectively [61]. In addition, PK and PD interactions between fostamatinib and warfarin, an anticoagulant, were also reported in healthy volunteers [61]. Warfarin is a racemic mixture comprising equal proportions of S-warfarin and R-warfarin. CYP2C9 is responsible for the metabolism of S-warfarin, while R-warfarin is metabolized to inactive hydroxylated compounds by CYP1A2, CYP2C19, and CYP3A4 [62, 63]. Fostamatinib increased the systemic exposure to R-warfarin by 17.8%, whereas there was no difference in Cmax. These small fluctuations in warfarin pharmacokinetics did not translate into changes in the prothrombin time-international normalized ratio as a PD marker until 168 h post-dose [61].
Table 2.
Drug–drug interactions affected by R406 exposure
| Co-administered drugs | Dosage of co-administered drugs (daily) | Dosage of fostamatinib (daily) | Analyte | Geometric mean ratio (90% CI) | References | |
|---|---|---|---|---|---|---|
| AUC | Cmax | |||||
| Ketoconazole | 200 mg twice | 80 mg once | R406 | 2.02 (1.77–2.30) | 1.37 (1.23–1.53) | [54, 58] |
| Verapamil | 80 mg three times | 150 mg once | R406 | 1.39 (1.08–1.80) | 1.06 (0.78–1.44) | [54, 58] |
| Rifampicin | 600 mg once | 150 mg once | R406 | 0.25 (0.19–0.32) | 0.41 (0.30–0.56) | [54, 58] |
| Rosuvastatin | 20 mg once | 100 mg twice | R406 | 1.10 (1.04–1.16) | 1.13 (1.02–1.25) | [54, 61, 66] |
| Simvastatin | 40 mg once | 100 mg twice | R406 | 1.11 (1.01–1.22) | 1.12 (0.98–1.27) | [54, 61] |
| Ranitidine | 150 mg once | 150 mg once | R406 | 0.97 (0.80–1.18) | 0.98 (0.71–1.34) | [49, 54] |
AUC area under the plasma concentration–time curve, CI confidence interval, Cmax maximum concentration, Ref. references
Table 3.
Effect of fostamatinib drug–drug interactions on co-administered drugs
| Co-administered drugs | Dosage of co-administered drugs (daily) | Dosage of fostamatinib (daily) | Analyte | Geometric mean ratio (90% CI) | References | |
|---|---|---|---|---|---|---|
| AUC | Cmax | |||||
| Microgynon (OC) | Ethinyl estradiol 30 µg once | 100 mg twice | Ethinyl estradiol | 1.28 (1.22–1.36) | 1.34 (1.26–1.43) | [54, 61] |
| Microgynon (OC) | Levonorgestrel 150 µg once | 100 mg twice | Levonorgestrel | 1.05 (0.98–1.13) | 0.91 (0.90–1.04) | [54, 61] |
| Pioglitazone | 30 mg | 100 mg twice | Pioglitazone | 1.18 (1.08–1.28) | 0.83 (0.64–1.07) | [54, 64] |
| Digoxin | 0.25 mg once | 100 mg twice | Digoxin | 1.37 (1.30–1.46) | 1.70 (1.46–1.98) | [52, 54] |
| Warfarin | 25 mg once | 100 mg twice | R-warfarin | 1.18 (1.13–1.23) | 1.02 (0.97–1.08) | [54, 61] |
| Warfarin | 25 mg once | 100 mg twice | S-warfarin | 1.13 (1.07–1.19) | 0.99 (0.93–1.06) | [54, 61] |
| Rosuvastatin | 20 mg once | 100 mg twice | Rosuvastatin | 1.95 (1.77–2.15) | 1.88 (1.69–2.09) | [54, 61] |
| Simvastatin | 40 mg once | 100 mg twice | Simvastatin | 1.64 (1.33–2.02) | 2.12 (1.64–2.74) | [54, 61] |
AUC area under the plasma concentration–time curve, CI confidence interval, Cmax maximum concentration, OC oral contraceptive, Ref. references
For evaluating R406 as a CYP inducer, an in vitro assay was performed using human hepatocytes [64]. R406 (3 µM and 10 µM) induced CYP2C8 to 52.8% and 74.7%, respectively, of the level achieved by rifampicin as a positive control, whereas R406 had minor effects on other CYP subtypes such as CYP1A2, CYP2B6, CYP2C9, CYP2C19, CYP3A4, and CYP3A5. Therefore, a clinical trial was carried out to evaluate the influence of fostamatinib on the pharmacokinetics of pioglitazone, which is a potent CYP2C8 substrate [64]. Consequently, there were relatively small differences in the AUC of pioglitazone and its metabolite hydroxy pioglitazone, regardless of the co-administration of fostamatinib. These results suggest that fostamatinib is unlikely to have a clinically significant effect on pioglitazone, and the result could potentially be extrapolated to other CYP2C8 substrates [64].
As pH changes in the gastrointestinal tract could affect bioavailability, the effect of ranitidine, an H2 blocker, on the pharmacokinetics of fostamatinib was evaluated [49]. Ranitidine decreased R406 AUC and Cmax by less than 5% and had modest effects on R406 exposure [49].
Several studies reported drug–drug interactions via transporters related to fostamatinib and R406. An in vitro assay showed that fostamatinib was determined to be an inhibitor of digoxin, a P-gp substrate drug (IC50 = 3.2 μM), whereas R406 did not show inhibitory activity even at the highest soluble concentration [52]. As fostamatinib did not appear in blood plasma, inhibiting intestinal P-gp by fostamatinib could cause a drug–drug interaction. The ratio of the theoretical intestinal concentration (I2) and IC50 can be used to estimate whether there could be a drug–drug interaction related to transporter inhibition in the intestine [65]. Intestinal concentration/IC50 of P-gp after fostamatinib 100 mg was approximately 216 (I2 = 691 μM, fostamatinib molecular weight = 578.52) [52, 66]. Drug interaction guidance from the FDA suggested that there exists a potential for a drug–drug interaction if [I2]/IC50 is >10; thus, considerable attention should be paid when fostamatinib is co-administered with P-gp substrates [65]. When digoxin, a substrate of P-gp, was co-administered with fostamatinib, the digoxin geometric mean AUC and Cmax increased by 36.6% and 65.2%, respectively, although there were no serious AEs due to elevated exposure [52].
R406 also inhibited OATP1B1-mediated probe substrate ([3H] estradiol glucuronide) uptake, but the IC50 was greater than 10 μM. It had no effect on the probe substrate ([3H] methotrexate) uptake via OAT3 [66] and did not inhibit MRP2, OAT1, or OCT2 [54].
Moreover, both fostamatinib and R406 strongly inhibited the BCRP-mediated transport of estrone 3-sulfate, with IC50 values of 0.050 and 0.031 μM, respectively [66]. Compared with those of other drugs known to have BCRP inhibition, the IC50 values of fostamatinib and R406 against estrone 3-sulfate were equivalent or much stronger than those of eltrombopag (0.04 µM), imatinib (0.4 µM), sulfasalazine (0.56 µM), and cyclosporine (6.7 µM) [66–68]. Intestinal concentration/IC50 of BCRP in orally administered fostamatinib 100 mg was 13,820 [52, 66]. As this value was considerably higher than that of eltrombopag (75-mg dose, 323), clopidogrel (75-mg dose, 15; 300-mg dose, 59), and ezetimibe (10-mg dose, 34), significant attention should be paid when fostamatinib is co-administered with known BCRP substrates, such as ciprofloxacin, acyclovir, cimetidine, and especially statins [65, 66]. Martin et al. investigated the effects of fostamatinib on the pharmacokinetics of rosuvastatin and simvastatin in healthy subjects. The results showed that fostamatinib increased the AUC and Cmax of rosuvastatin by 95.6% and 88.4%, respectively, and those of simvastatin by 64.1% and 112.5%, respectively [61, 66]. Keskitalo et al. reported that BCRP in the intestine restricted the rosuvastatin absorbance and bioavailability by 50% [69]. Therefore, this drug–drug interaction resulting in doubled AUC was thought to be caused by the inhibition of intestinal BCRP by fostamatinib and R406. In addition, the incidence of statin-induced rhabdomyolysis or myopathy was dose dependent [70], and thus, careful monitoring of laboratory values should be recommended upon co-administration of statins and fostamatinib.
Population Pharmacokinetics of Fostamatinib
A few published studies and a regulatory filing assessed fostamatinib population pharmacokinetics [54, 71, 72]. Boström et al. reported the population PK model using data from three phase I studies in healthy volunteers, one phase II study, and three phase III studies in RA. These datasets included 5056 observations from 1441 subjects [72]. R406 concentration–time data were described by a two-compartment model with first-order, delayed absorption, and first-order elimination. For an individual with a 70-kg body weight and a daily dose of 200 mg, Css,ave, apparent oral clearance, and apparent oral volume of distribution at steady state was estimated to 446 ng/mL, 18.7 L/h, and 410 L, respectively. The estimate absorption rate of constant was 1.55 h-1, and the lag time was 0.44 h [72]. The estimated DAUCss in patients with RA was 10,716 ± 5028 ng·h/mL, while the mean daily dose was 194 ± 28.1 mg [38]. The predicted average DAUCss in patients with ITP was 10,232 ng·h/mL for fostamatinib 100 mg BID and 15,101 ng·h/mL for fostamatinib 150 mg BID, and no difference was observed by disease etiology [54]. In addition, the average DAUCss obtained in 12 patients with ITP was approximately 11,000 ng·h/mL, which is consistent with the results of population pharmacokinetics [38].
In addition, a population PK analysis revealed that body weight was an important covariate for both volume of distribution and clearance, but not age, sex, or race [38, 54]. R406 exposure decreases with an increase in body weight; in detail, the DAUCss were 7232, 5183, and 3936 ng·h/mL for subjects with body weight < 50 kg, 50–90 kg, and > 90 kg, respectively [38]. This result suggests that weight-based dosing may be desirable for fostamatinib from the PK view. However, there was no difference in body weight in the ITP clinical trial between subjects who continuously received 100 mg BID and those who received a dose escalation to 150 mg BID. As the dose escalation was performed because of the platelet response of each patient, if there is a correlation between therapeutic response and systemic exposure, there should be a difference in body weight in both groups. Accounting for these results, the effect of systemic exposure fluctuated by weight seemed not to be as large as other backgrounds such as the baseline platelet count. Therefore, an initial dose of fostamatinib was decided to be 100 mg BID regardless of weight [38]. In contrast, patients with a low body weight may have an unexpected increase in exposure. We need to extrapolate this important suggestion from the population PK analysis into the understanding of systemic exposure with treatment-related adverse effects.
Safety and AEs of Fostamatinib
The incidence of AEs in the clinical trials is summarized in Table 4. In FIT1 and FIT2, 83% and 75% of patients experienced any AE in the fostamatinib and placebo groups, respectively. Hypertension, diarrhea, elevation of hepatic enzymes, and neutropenia were significantly associated with fostamatinib treatment. Overall infections were slightly increased in the fostamatinib group compared with the placebo group (30% vs 21%). Most AEs were classified as either mild or moderate (81% in the fostamatinib and placebo groups). Patients receiving fostamatinib treatment had a higher rate of dose reductions (9% taking fostamatinib and 2% taking the placebo) or temporary dose interruptions (18% taking fostamatinib and 10% taking the placebo), and the common AEs leading to dose reductions were diarrhea and hypertension [8, 55].
Table 4.
Summary of AEs in clinical trials of fostamatinib
| Disease | RA | RA | RA | RA | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Phase | Phase II | Phase II | Phase II | Phase III | |||||||
| Trial number | NCT00326339 | NCT00665925 | NCT01569074 | NCT01197521 | |||||||
| Trial name | TASKI-1 | TASKI-2 | OSKIRA-ASIA-1 | OSKIRA-1 | |||||||
| Dosage | 50 mg BID | 100 mg BID | 150 mg BID | 150 mg QD | 100 mg BID | 50 mg BID | 75 mg BID | 100 mg BID 150 mg QD |
100 mg BID | 100 mg BID 150 mg QD |
100 mg BID |
| Patients (%) | 46 | 49 | 47 | 152 | 152 | 33 | 33 | 33 | 31 | 304 | 310 |
| Any AE | 80.0 | 40.8 | 48.0 | 72.7 | 63.6 | 69.7 | 74.2 | 71.1 | 66.8 | ||
| Severe AE | 3.5 | 3.3 | 0.7 | 9.1 | 0.0 | 3.0 | 3.2 | 4.9 | 2.9 | ||
| Hypertension | 0.0 | 6.1 | 4.3 | 11.8 | 13.8 | 9.1 | 18.2 | 18.2 | 29.0 | 15.1 | 15.8 |
| Neutropenia | 2.2 | 10.2 | 29.8 | 15.2 | 12.1 | 6.1 | 12.9 | ||||
| ALT increase | 4.3 | 6.1 | 8.5 | 4.6 | 5.3 | 0.0 | 0.0 | 0.0 | 0.0 | 3.9 | 3.5 |
| URTI | 6.5 | 0.0 | 0.0 | 2.0 | 6.6 | 0.0 | 3.0 | 6.1 | 9.7 | 5.3 | 3.5 |
| Diarrhea | 10.9 | 16.3 | 44.7 | 11.8 | 19.1 | 3.0 | 6.1 | 18.2 | 16.1 | 15.1 | 13.9 |
| Nausea | 4.3 | 14.3 | 14.9 | 5.9 | 4.6 | 0.0 | 0.0 | 0.0 | 3.2 | 8.9 | 6.9 |
| Gastritis | 2.2 | 4.1 | 14.9 | 3.0 | 0.0 | 3.0 | 9.7 | ||||
| Dyspepsia | 2.2 | 10.2 | 6.4 | 1.6 | 3.2 | ||||||
| Abdominal pain | 0.0 | 4.1 | 6.4 | 5.3 | 3.9 | ||||||
| Headache | 13.0 | 2.0 | 6.4 | 6.6 | 5.9 | 0.0 | 3.0 | 6.1 | 3.2 | 6.3 | 3.2 |
| Dizziness | 4.3 | 8.2 | 10.6 | 3.0 | 3.0 | 0.0 | 3.2 | ||||
| Fatigue | 6.5 | 6.1 | 0.0 | ||||||||
| Edema | 2.2 | 2.0 | 8.5 | ||||||||
| Rash | 6.5 | 8.2 | 4.3 | 1.3 | 2.0 | ||||||
| Disease | RA | RA | RA | ITP | ITP | DLBCL | B-cell NHL | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Phase | Phase III | Phase III | Phase IIb | Phase III | Phase III | Phase II | Phase II | |||||
| Trial number | NCT01197534 | NCT01197534 | NCT01264770 |
NCT02076399 NCT02076412 |
NCT02077192 | NCT01499303 | NCT00446095 | |||||
| Trial name | OSKIRA-2 | OSKIRA-3 | OSKIRA-4 | FIT1, FIT2 | FIT3 | – | – | |||||
| Dosage | 100 mg BID 150 mg QD |
100 mg BID | 100 mg BID 150 mg QD |
100 mg BID | 100 mg BID 100 mg QD |
100 mg BID 150 mg QD |
100 mg BID | 100 mg BID 150 mg BID |
100 mg BID 150 mg BID |
100 mg BID | 200 mg BID | 200 mg BID |
| Patients (%) | 298 | 308 | 108 | 105 | 48 | 48 | 54 | 102 | 146 | 21 | 47 | 68 |
| Any AE | 51.0 | 55.2 | 45.4 | 48.6 | 59.6 | 60.4 | 72.2 | 83.0 | 86.0 | 62.0 | 72.0 | |
| Severe AE | 8.4 | 9.7 | 6.5 | 6.7 | 7.0 | 2.1 | 9.3 | 16.0 | 23.3 | 48.0 | 53.0 | |
| Hypertension | 18.5 | 22.1 | 13.9 | 13.3 | 8.8 | 6.3 | 13.0 | 28.0 | 21.0 | 4.8 | 10.6 | 24.0 |
| Neutropenia | 0.0 | 0.0 | 5.6 | 6.0 | 6.0 | 19.0 | 8.5 | 31.0 | ||||
| ALT increase | 4.7 | 6.8 | 3.5 | 2.1 | 5.6 | 11.0 | 10.0 | 10.0 | ||||
| URTI | 9.7 | 12.0 | 1.9 | 5.7 | 1.8 | 4.2 | 1.9 | 11.0 | 10.0 | |||
| Diarrhea | 15.8 | 14.3 | 26.9 | 20.0 | 21.1 | 27.1 | 16.7 | 31.0 | 35.0 | 0.0 | 29.8 | 41.0 |
| Nausea | 4.2 | 6.5 | 6.5 | 3.8 | 4.2 | 3.7 | 19.0 | 19.0 | 14.3 | 21.3 | 21.0 | |
| Gastritis | 1.9 | 5.7 | ||||||||||
| Dyspepsia | 1.8 | 0.0 | 0.0 | |||||||||
| Abdominal pain | 4.0 | 6.2 | 6.0 | 6.0 | 7.0 | |||||||
| Headache | 8.3 | 7.6 | 13.0 | 16.0 | ||||||||
| Dizziness | 5.6 | 6.7 | 11.0 | 11.0 | 10.0 | |||||||
| Fatigue | 0.0 | 0.0 | 6.0 | 9.0 | 14.3 | 19.1 | 41.0 | |||||
| Edema | ||||||||||||
| Rash | 9.0 | 6.0 | ||||||||||
AE adverse events, ALT alanine aminotransferase, BID twice daily, DLBCL diffuse large B-cell lymphoma, ITP immune thrombocytopenia, NHL non-Hodgkin lymphoma, QD once daily, RA rheumatoid arthritis, URTI upper respiratory tract infection
In the OSKIRA-4 study, fostamatinib monotherapy was administered at three different doses: arm A (100 mg BID), arm B (100 mg BID for 4 weeks, followed by 150 mg QD as a maintenance dose), and arm C (100 mg BID for 4 weeks, followed by 100 mg QD as a maintenance dose) [21]. By the end of the observation period (week 24), dose-dependent increases in AEs were reported (72.2%, 60.4%, and 59.6% in arm A, B, and C). Serious AEs occurred in 9.3%, 2.1%, and 7.0%, respectively. Discontinuation because of AEs was 16.7%, 12.5%, and 14.0% in arms A, B, and C. A dose-dependent increase in diarrhea incidence was not observed. In considering the mechanism of diarrhea, previous research showed that R406 regulates mucin production in epithelial cells [73]. As mucin plays an important role as a biological mucosal barrier for limiting the direct contact of the epithelium with microorganisms, mucin reduction accompanied by barrier disruption might result in the development of diarrhea [74]. As individual differences were observed in the excretion of R406 to the intestinal tract and feces [48], further analysis is expected regarding the relationship between the intestinal metabolite concentration and the incidence of diarrhea.
An increase in BP was the off-target effect of fostamatinib, as R406 has inhibitory effects on VEGFR-1 and VEGFR-2 [40]. According to the results of ambulatory BP monitoring after 4 weeks of fostamatinib 100 mg BID, 24-hour mean systolic BP and diastolic BP were significantly increased by 2.9 mmHg and 3.5 mmHg, respectively. This elevated BP returned to baseline 1 week after fostamatinib discontinuation [75]. In the OSKIRA-4 study, hypertension was prominent in patients receiving a high fostamatinib dose (13.0%, 6.3%, and 8.8% in arms A, B, and C) [21]. According to the meta-analysis for the cardiovascular risk of fostamatinib in 5618 patients with RA, fostamatinib 100 mg BID significantly increased the relative risk of hypertension compared with the placebo group (relative risk: 3.82, 95% confidence interval 2.88–5.05) and the 100-mg QD group (relative risk: 1.98, 95% confidence interval 1.26–3.11), but not with the 150-mg QD group (relative risk: 0.94, 95% confidence interval 0.80–1.10) [76].
In a phase II trial for non-Hodgkin lymphoma and chronic lymphocytic leukemia, 200 mg BID, a higher dose compared with the ITP and RA study, was selected. Common AEs such as diarrhea (41%) and hypertension (21%) were almost consistent with the results of FIT1 and FIT2. In contrast, neutropenia occurred in 31% of patients (6.0% of patients in FIT1 and FIT2), and febrile neutropenia occurred in 7% of patients in this study [26]. An increase in neutropenia was observed in a dose-dependent manner in the TASKI-1 trial. As there is little information on the R406 exposure and neutropenia, further analysis is expected for the safe use of fostamatinib in clinical settings.
According to animal reproduction studies, fostamatinib administration to pregnant rats or rabbits during organogenesis caused embryo-fetal mortality in a dose-dependent manner [50, 51, 77]. This was mainly because R406 was an inhibitor of RET kinase, resulting in urogenital and major vessel defects during development [54]. R406 was detected in maternal milk of rodents at concentrations five-fold to ten-fold higher than in maternal plasma [50]. Based on this evidence, fostamatinib has a potential risk to the fetus, and women of reproductive potential need contraception during treatment, and lactation should also be avoided for a month after the last dose [50, 51].
PK/PD Assessment
Exposure-Efficacy Analysis
Maringwa et al. reported the PK/PD analysis of the efficacy of fostamatinib in patients with RA [71]. This study included 641 patients from two phase II studies (TASKI-1 and TASKI-2), and efficacy was described using ACR20 for 26 weeks. Consequently, the ACR20 response was linearly related to the average R406 plasma concentration. Furthermore, elevated fostamatinib dosage from 100 mg BID to 150 mg BID resulted in an increased dropout from treatment and a subsequent loss of efficacy. This integrated analysis to assess the correlation between exposure and response supported the dosage decision that fostamatinib 100 mg BID could have provided the optimal ACR20 efficacy in the next phase III trial [71].
A population PK/PD analysis was conducted using data from two phase III studies in patients with ITP. Blood platelet count was used as an efficacy marker. Of the 101 patients taking fostamatinib, 89 (88%) increased their dose from 100 mg BID to 150 mg BID at or after week 4 [8]. During the 24-week follow-up, a higher R406 concentration on average was evident in responders compared with non-responders only for week 12, but not in other observational times [54]. In addition, body weight was not a significant covariate in the exposure-response population model, although it affected R406 exposure, suggesting that body weight has little effect on the efficacy of fostamatinib [38, 54]. Thus, the response to fostamatinib treatment in patients with ITP is not only attributed to individual variability of R406 exposure. As the population PK/PD analysis of ITP was performed on a smaller population compared with RA, continuous analysis with post-marketing data is required. As well as the achievement of a platelet count goal at several timepoints, the platelet count as a continuous variable as a PD marker should be proposed for further exposure-efficacy analysis.
Exposure-Safety Analysis
A population PK/PD analysis was also performed to explore the relationship between R406 exposure and the incidence of AEs, such as hypertension, decreased neutrophil count, and increased liver enzyme and bilirubin levels. An increase in R406 exposure had little effect on liver enzymes and bilirubin levels. Although the neutrophil count tended to decrease with a higher exposure to R406, the maximum effect was relatively small and likely had no effect on clinical outcomes [54]. In addition, Boström et al. reported an exposure-dependent increase in BP using data from 1378 patients with RA in the OSKIRA trial [72]. In detail, a direct effect model adequately described the PK/PD relationship between systemic exposure and BP. The estimated Emax and EC50 were 10.2 mmHg and 16,300 ng·h/mL for systolic blood pressure and 9.2 mmHg and 17,000 ng·h/mL for diastolic blood pressure, respectively [38, 72]. According to a population PK analysis, patients with a low body weight (< 50 kg) had an almost doubled R406 exposure compared with patients with a large body weight (> 90 kg) [38]. Together with these results, when considering the dose escalation especially in patients with a low body weight, healthcare providers need to be alert and carefully monitor the BP fluctuation for an early detection of hypertension.
Conclusions and Future Perspectives
Fostamatinib is the first and only Syk inhibitor for treating adult patients with ITP who showed an insufficient response to a previous treatment. The PK parameters of R406 in patients with ITP were consistent with those in healthy patients. Even though severe hepatic function or end-stage kidney disease, including dialysis, showed little effect on its PK parameters, an increase of unbound R406 should be considered owing to hypoalbuminemia because R406 has a high protein binding ratio. R406 is dominantly metabolized by CYP3A4 and UGT1A9 in the liver, and eliminated mainly in feces. In addition, R406 is a substrate of P-gp and fostamatinib is an inhibitor of P-gp. Both fostamatinib and R406 inhibit the BCRP transporter function. Thus, CYP3A4, P-gp, and BCRP are mainly related to the drug–drug interactions of fostamatinib. In particular, the potential of a drug interaction via intestinal BCRP is important ([I2]/IC50 of fostamatinib 100 mg was 13,820), and this prediction is in line with the trial results showing the AUC of rosuvastatin is almost doubled when co-administered with fostamatinib. Considerable attention should be paid to the elevated risk of statin-induced rhabdomyolysis.
According to the population PK analysis, body weight was a significant covariate affecting the systemic exposure of R406. In detail, the DAUCss was almost halved in patients weighing > 90 kg compared with that in patients weighing < 50 kg. These results suggested that weight-based initial dosing is preferable for constant R406 exposure among patients. However, in the PK/PD analysis evaluating the exposure efficacy of fostamatinib, responders showed higher R406 concentrations than those of non-responders but the threshold as a target concentration remains unknown. Moreover, the correlation between R406 exposure and the achievement of a platelet count goal as a PD marker was not evident. While integrating these results, fostamatinib was finally approved as a fixed dose at the start of treatment. If the platelet counts of patients could be maintained and major bleeding events could be regulated with 100 mg BID as an initial dose, increasing the dosage might not be necessary.
In contrast, the PK/PD analysis for exposure-safety indicated that R406 exposure significantly correlated with the incidence of hypertension. Specifically, when considering the dose increase in patients with a low body weight, we should be alert and carefully monitor the BP fluctuation for the early detection of hypertension. Even though the relationship between the exposure and the other major toxicities including diarrhea and neutropenia remains unclear, careful management is required with the dose escalation to avoid toxicity-related discontinuation.
In conclusion, we focused on the pharmacodynamics, pharmacokinetics, and safety profile of fostamatinib throughout its clinical development. For effective clinical development of fostamatinib to other diseases, and for fostering and improving fostamatinib therapy in patients with ITP, continuous clinical studies are essential in terms of pharmacokinetics and pharmacodynamics.
Declarations
Funding
No funding was received for the preparation of this article.
Conflicts of interest/Competing interests
The authors have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Not applicable.
Code availability
Not applicable.
Authors’ contributions
Not applicable.
Contributor Information
Ryosuke Matsukane, Email: matsukane.ryosuke.096@m.kyushu-u.ac.jp.
Kimitaka Suetsugu, Email: suetsugu.kimitaka.345@m.kyushu-u.ac.jp.
Takeshi Hirota, Email: hirota.takeshi.612@m.kyushu-u.ac.jp.
Ichiro Ieiri, Email: ieiri@phar.kyushu-u.ac.jp.
References
- 1.Newland A, Lee E-J, McDonald V, Bussel JB. Fostamatinib for persistent/chronic adult immune thrombocytopenia. Immunotherapy. 2018;10:9–25. doi: 10.2217/imt-2017-0097. [DOI] [PubMed] [Google Scholar]
- 2.Kapur R. Fine-tuning the treatment toolbox of immune thrombocytopenia: fostamatinib as a second-line therapy. Br J Haematol. 2020;190:817–818. doi: 10.1111/bjh.16958. [DOI] [PubMed] [Google Scholar]
- 3.Sakai K, Nakamura S, Sada K, Kobayashi T, Uno H, Yamamura H. Characterization of partially purified cytosolic protein-tyrosine kinase from porcine spleen. Biochem Biophys Res Commun. 1988;152:1123–1130. doi: 10.1016/S0006-291X(88)80401-7. [DOI] [PubMed] [Google Scholar]
- 4.Taniguchi T, Kobayashi T, Kondo J, Takahashi K, Nakamura H, Suzuki J, et al. Molecular cloning of a porcine gene syk that encodes a 72-kDa protein-tyrosine kinase showing high susceptibility to proteolysis. J Biol Chem. 1991;266:15790–15796. doi: 10.1016/S0021-9258(18)98478-4. [DOI] [PubMed] [Google Scholar]
- 5.Ku G, Malissen B, Mattei MG. Chromosomal location of the Syk and ZAP-70 tyrosine kinase genes in mice and humans. Immunogenetics. 1994;40:300–302. doi: 10.1007/BF00189976. [DOI] [PubMed] [Google Scholar]
- 6.Mócsai A, Ruland J, Tybulewicz VLJ. The SYK tyrosine kinase: a crucial player in diverse biological functions. Nat Rev Immunol. 2010;10:387–402. doi: 10.1038/nri2765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Geahlen RL. Getting Syk: spleen tyrosine kinase as a therapeutic target. Trends Pharmacol Sci. 2014;35:414–422. doi: 10.1016/j.tips.2014.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bussel J, Arnold DM, Grossbard E, Mayer J, Treliński J, Homenda W, et al. Fostamatinib for the treatment of adult persistent and chronic immune thrombocytopenia: results of two phase 3, randomized, placebo-controlled trials. Am J Hematol. 2018;93:921–930. doi: 10.1002/ajh.25125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Neunert C, Terrell DR, Arnold DM, Buchanan G, Cines DB, Cooper N, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3:3829–3866. doi: 10.1182/bloodadvances.2019000966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Terrell DR, Beebe LA, Vesely SK, Neas BR, Segal JB, George JN. The incidence of immune thrombocytopenic purpura in children and adults: a critical review of published reports. Am J Hematol. 2010;85:174–180. doi: 10.1002/ajh.21833. [DOI] [PubMed] [Google Scholar]
- 11.Lee JY, Lee JH, Lee J-O, Bang S-M. Epidemiology and management of immune thrombocytopenia: a nationwide population-based study in Korea. Blood. 2016;128:4934. doi: 10.1182/blood.V128.22.4934.4934. [DOI] [PubMed] [Google Scholar]
- 12.McKeage K, Lyseng-Williamson KA. Fostamatinib in chronic immune thrombocytopenia: a profile of its use in the USA. Drugs Ther Perspect. 2018;34:451–456. doi: 10.1007/s40267-018-0551-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bussel JB, Arnold DM, Boxer MA, Cooper N, Mayer J, Zayed H, et al. Long-term fostamatinib treatment of adults with immune thrombocytopenia during the phase 3 clinical trial program. Am J Hematol. 2019;94:546–553. doi: 10.1002/ajh.25444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pine PR, Chang B, Schoettler N, Banquerigo ML, Wang S, Lau A, et al. Inflammation and bone erosion are suppressed in models of rheumatoid arthritis following treatment with a novel Syk inhibitor. Clin Immunol. 2007;124:244–257. doi: 10.1016/j.clim.2007.03.543. [DOI] [PubMed] [Google Scholar]
- 15.Weinblatt ME, Kavanaugh A, Burgos-Vargas R, Dikranian AH, Medrano-Ramirez G, Morales-Torres JL, et al. Treatment of rheumatoid arthritis with a Syk kinase inhibitor: a twelve-week, randomized, placebo-controlled trial. Arthritis Rheum. 2008;58:3309–3318. doi: 10.1002/art.23992. [DOI] [PubMed] [Google Scholar]
- 16.Weinblatt ME, Kavanaugh A, Genovese MC, Musser TK, Grossbard EB, Magilavy DB. An oral spleen tyrosine kinase (Syk) inhibitor for rheumatoid arthritis. N Engl J Med. 2010;363:1303–1312. doi: 10.1056/NEJMoa1000500. [DOI] [PubMed] [Google Scholar]
- 17.Weinblatt ME, Kavanaugh A, Genovese MC, Jones DA, Musser TK, Grossbard EB, et al. Effects of fostamatinib (R788), an oral spleen tyrosine kinase inhibitor, on health-related quality of life in patients with active rheumatoid arthritis: analyses of patient-reported outcomes from a randomized, double-blind, placebo-controlled trial. J Rheumatol. 2013;40:369–378. doi: 10.3899/jrheum.120923. [DOI] [PubMed] [Google Scholar]
- 18.Weinblatt ME, Genovese MC, Ho M, Hollis S, Rosiak-Jedrychowicz K, Kavanaugh A, et al. Effects of fostamatinib, an oral spleen tyrosine kinase inhibitor, in rheumatoid arthritis patients with an inadequate response to methotrexate: results from a phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheumatol. 2014;66:3255–3264. doi: 10.1002/art.38851. [DOI] [PubMed] [Google Scholar]
- 19.Dawes P, Dimic A, Genovese MC, van der Heijde D, Jenkins M, O’Brien C, et al. OSKIRA-2: a phase III, multicenter, randomized, double-blind, placebo-controlled parallel-group study of 2 dosing regimens of fostamatinib in rheumatoid arthritis patients with an inadequate response to disease-modifying antirheumatic drugs. Arthritis Rheum. 2013;65:S198–S199. [Google Scholar]
- 20.Genovese MC, van der Heijde DM, Keystone EC, Spindler AJ, Benhamou C, Kavanaugh A, et al. A phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study of 2 dosing regimens of fostamatinib in patients with rheumatoid arthritis with an inadequate response to a tumor necrosis factor-α antagonist. J Rheumatol. 2014;41:2120–2128. doi: 10.3899/jrheum.140238. [DOI] [PubMed] [Google Scholar]
- 21.Taylor PC, Genovese MC, Greenwood M, Ho M, Nasonov E, Oemar B, et al. OSKIRA-4: a phase IIb randomised, placebo-controlled study of the efficacy and safety of fostamatinib monotherapy. Ann Rheum Dis. 2015;74:2123–2129. doi: 10.1136/annrheumdis-2014-205361. [DOI] [PubMed] [Google Scholar]
- 22.Podolanczuk A, Lazarus AH, Crow AR, Grossbard E, Bussel JB. Of mice and men: an open-label pilot study for treatment of immune thrombocytopenic purpura by an inhibitor of Syk. Blood. 2009;113:3154–3160. doi: 10.1182/blood-2008-07-166439. [DOI] [PubMed] [Google Scholar]
- 23.Tanaka Y, Millson D, Iwata S, Nakayamada S. Safety and efficacy of fostamatinib in rheumatoid arthritis patients with an inadequate response to methotrexate in phase II OSKIRA-ASIA-1 and OSKIRA-ASIA-1X study. Rheumatology. 2021;60:2884–2895. doi: 10.1093/rheumatology/keaa732. [DOI] [PubMed] [Google Scholar]
- 24.Rogers KA, Boxer MA, Choi MY, Agajanian R, Arnold DM, Broome CM, et al. Fostamatinib, a spleen tyrosine kinase (SYK) inhibitor, for the treatment of warm antibody autoimmune hemolytic anemia (wAIHA): final results of the phase 2, multicenter, open-label study. Blood. 2019;134:3518. doi: 10.1182/blood-2019-126509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Barcellini W, Zaninoni A, Giannotta JA, Fattizzo B. New insights in autoimmune hemolytic anemia: from pathogenesis to therapy stage 1. J Clin Med. 2020;9:3859. doi: 10.3390/jcm9123859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Friedberg JW, Sharman J, Sweetenham J, Johnston PB, Vose JM, Lacasce A, et al. Inhibition of Syk with fostamatinib disodium has significant clinical activity in non-Hodgkin lymphoma and chronic lymphocytic leukemia. Blood. 2010;115:2578–2585. doi: 10.1182/blood-2009-08-236471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Flinn IW, Bartlett NL, Blum KA, Ardeshna KM, LaCasce AS, Flowers CR, et al. A phase II trial to evaluate the efficacy of fostamatinib in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) Eur J Cancer. 2016;54:11–17. doi: 10.1016/j.ejca.2015.10.005. [DOI] [PubMed] [Google Scholar]
- 28.Ma TK-W, McAdoo SP, Tam FW-K. Spleen tyrosine kinase: a crucial player and potential therapeutic target in renal disease. Nephron. 2016;133:261–269. doi: 10.1159/000446879. [DOI] [PubMed] [Google Scholar]
- 29.McAdoo S, Tam FWK. Role of the spleen tyrosine kinase pathway in driving inflammation in IgA nephropathy. Semin Nephrol. 2018;38:496–503. doi: 10.1016/j.semnephrol.2018.05.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tam WKF, Tumlin J, Barratt J, Rovin HB, Roberts SDI, Roufosse C, et al. SUN-036 Spleen tyrosine kinase (SYK) inhibition in IgA nephropathy: a global, phase II, randomized placebo-controlled trial of fostamatinib. Kidney Int Rep. 2019;4:S168. doi: 10.1016/j.ekir.2019.05.431. [DOI] [Google Scholar]
- 31.McAdoo SP, Prendecki M, Tanna A, Bhatt T, Bhangal G, McDaid J, et al. Spleen tyrosine kinase inhibition is an effective treatment for established vasculitis in a pre-clinical model. Kidney Int. 2020;97:1196–1207. doi: 10.1016/j.kint.2019.12.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tabassum N, Zhang H, Stebbing J. Repurposing fostamatinib to combat SARS-CoV-2-induced acute lung injury. Cell Rep Med. 2020;1:100145. doi: 10.1016/j.xcrm.2020.100145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Strich JR, Ramos-Benitez MJ, Randazzo D, Stein SR, Babyak A, Davey RT, et al. Fostamatinib inhibits neutrophils extracellular traps induced by COVID-19 patient plasma: a potential therapeutic. J Infect Dis. 2021;223:981–984. doi: 10.1093/infdis/jiaa789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Strich JR, Tian X, Samour M, King CS, Shlobin O, Reger R, et al. Fostamatinib for the treatment of hospitalized adults with Coronavirus Disease 2019: a randomized trial. Clin Infect Dis. 2021; p. ciab732. [DOI] [PMC free article] [PubMed]
- 35.Braselmann S, Taylor V, Zhao H, Wang S, Sylvain C, Baluom M, et al. R406, an orally available spleen tyrosine kinase inhibitor blocks fc receptor signaling and reduces immune complex-mediated inflammation. J Pharmacol Exp Ther. 2006;319:998–1008. doi: 10.1124/jpet.106.109058. [DOI] [PubMed] [Google Scholar]
- 36.Aksentijevich I. The sickening consequences of too much SYK signaling. Nat Genet. 2021;53:432–434. doi: 10.1038/s41588-021-00837-8. [DOI] [PubMed] [Google Scholar]
- 37.Villaseñor AG, Kondru R, Ho H, Wang S, Papp E, Shaw D, et al. Structural insights for design of potent spleen tyrosine kinase inhibitors from crystallographic analysis of three inhibitor complexes. Chem Biol Drug Des. 2009;73:466–470. doi: 10.1111/j.1747-0285.2009.00785.x. [DOI] [PubMed] [Google Scholar]
- 38.US Food and Drug Administration. Tavalisse (fostamatinib disodium hexahydrate) [multi-disciplinary review]. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/209299Orig1s000MultidisciplineR.pdf. Accessed 22 Mar 2022.
- 39.Obergfell A, Eto K, Mocsai A, Buensuceso C, Moores SL, Brugge JS, et al. Coordinate interactions of Csk, Src, and Syk kinases with [alpha]IIb[beta]3 initiate integrin signaling to the cytoskeleton. J Cell Biol. 2002;157:265–275. doi: 10.1083/jcb.200112113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rolf MG, Curwen JO, Veldman-Jones M, Eberlein C, Wang J, Harmer A, et al. In vitro pharmacological profiling of R406 identifies molecular targets underlying the clinical effects of fostamatinib. Pharmacol Res Perspect. 2015;3:e00175. doi: 10.1002/prp2.175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wilson CN. Adenosine receptors and asthma in humans. Br J Pharmacol. 2008;155:475–486. doi: 10.1038/bjp.2008.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Brown RA, Spina D, Page CP. Adenosine receptors and asthma. Br J Pharmacol. 2008;153(Suppl. 1):S446–S456. doi: 10.1038/bjp.2008.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Matsubara S, Koya T, Takeda K, Joetham A, Miyahara N, Pine P, et al. Syk activation in dendritic cells is essential for airway hyperresponsiveness and inflammation. Am J Respir Cell Mol Biol. 2006;34:426–433. doi: 10.1165/rcmb.2005-0298OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Matsubara S, Li G, Takeda K, Loader JE, Pine P, Masuda ES, et al. Inhibition of spleen tyrosine kinase prevents mast cell activation and airway hyperresponsiveness. Am J Respir Crit Care Med. 2006;173:56–63. doi: 10.1164/rccm.200503-361OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Versmissen J, Mirabito Colafella KM, Koolen SLW, Danser AHJ. Vascular cardio-oncology: vascular endothelial growth factor inhibitors and hypertension. Cardiovasc Res. 2019;115:904–914. doi: 10.1093/cvr/cvz022. [DOI] [PubMed] [Google Scholar]
- 46.Skinner M, Philp K, Lengel D, Coverley L, Lamm Bergström E, Glaves P, et al. The contribution of VEGF signalling to fostamatinib-induced blood pressure elevation. Br J Pharmacol. 2014;171:2308–2320. doi: 10.1111/bph.12559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lengel D, Lamm Bergström E, Barthlow H, Oldman K, Musgrove H, Harmer A, et al. Prevention of fostamatinib-induced blood pressure elevation by antihypertensive agents. Pharmacol Res Perspect. 2015;3:e00176. doi: 10.1002/prp2.176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Sweeny DJ, Li W, Clough J, Bhamidipati S, Singh R, Park G, et al. Metabolism of fostamatinib, the oral methylene phosphate prodrug of the spleen tyrosine kinase inhibitor R406 in humans: contribution of hepatic and gut bacterial processes to the overall biotransformation. Drug Metab Dispos. 2010;38:1166–1176. doi: 10.1124/dmd.110.032151. [DOI] [PubMed] [Google Scholar]
- 49.Flanagan T, Martin P, Gillen M, Mathews D, Lisbon E, Kruusmägi M. Effects of ranitidine (antacid), food, and formulation on the pharmacokinetics of fostamatinib: results from five phase I clinical studies. Eur J Clin Pharmacol. 2017;73:185–195. doi: 10.1007/s00228-016-2156-4. [DOI] [PubMed] [Google Scholar]
- 50.US Food and Drug Administration. Tavalisse (fostamatinib disodium hexahydrate) [package insert]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/209299lbl.pdf. Accessed 22 Mar 2022.
- 51.European Medicines Agency. Tavlesse (fostamatinib disodium hexahydrate) [product information]. https://www.ema.europa.eu/en/documents/product-information/tavlesse-epar-product-information_en.pdf. Accessed 22 Mar 2022.
- 52.Martin P, Gillen M, Millson D, Oliver S, Brealey C, Elsby R, et al. Effects of fostamatinib on the pharmacokinetics of digoxin (a P-glycoprotein substrate): results from in vitro and phase I clinical studies. Clin Ther. 2015;37:2811–2822. doi: 10.1016/j.clinthera.2015.09.018. [DOI] [PubMed] [Google Scholar]
- 53.Baluom M, Grossbard EB, Mant T, Lau DTW. Pharmacokinetics of fostamatinib, a spleen tyrosine kinase (SYK) inhibitor, in healthy human subjects following single and multiple oral dosing in three phase I studies. Br J Clin Pharmacol. 2013;76:78–88. doi: 10.1111/bcp.12048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.European Medicines Agency. Tavlesse (fostamatinib disodium hexahydrate) [assessment report]. https://www.ema.europa.eu/en/documents/assessment-report/tavlesse-epar-public-assessment-report_en.pdf. Accessed 22 Mar 2022.
- 55.Newland A, McDonald V. Fostamatinib: a review of its clinical efficacy and safety in the management of chronic adult immune thrombocytopenia. Immunotherapy. 2020;12:1325–1340. doi: 10.2217/imt-2020-0215. [DOI] [PubMed] [Google Scholar]
- 56.Ghuman J, Zunszain PA, Petitpas I, Bhattacharya AA, Otagiri M, Curry S. Structural basis of the drug-binding specificity of human serum albumin. J Mol Biol. 2005;353:38–52. doi: 10.1016/j.jmb.2005.07.075. [DOI] [PubMed] [Google Scholar]
- 57.Martin P, Oliver S, Gillen M, Marbury T, Millson D. Pharmacokinetic properties of fostamatinib in patients with renal or hepatic impairment: results from 2 phase I clinical studies. Clin Ther. 2015;37:2823–2836. doi: 10.1016/j.clinthera.2015.09.016. [DOI] [PubMed] [Google Scholar]
- 58.Martin P, Gillen M, Millson D, Oliver S, Brealey C, Grossbard EB, et al. Effects of CYP3A4 inhibitors ketoconazole and verapamil and the CYP3A4 inducer rifampicin on the pharmacokinetic parameters of fostamatinib: results from in vitro and phase I clinical studies. Drugs R D. 2016;16:81–92. doi: 10.1007/s40268-015-0118-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Sweeny DJ, Li W, Grossbard E, Lau DTW. Contribution of gut bacteria to the metabolism of the spleen tyrosine kinase (Syk) inhibitor R406 in cynomolgus monkey. Xenobiotica. 2010;40:415–423. doi: 10.3109/00498251003734244. [DOI] [PubMed] [Google Scholar]
- 60.Baluom M, Samara E, Grossbard EB, Lau DT-W. Fostamatinib, a Syk-kinase inhibitor, does not affect methotrexate pharmacokinetics in patients with rheumatoid arthritis. J Clin Pharmacol. 2011;51:1310–1318. doi: 10.1177/0091270010381496. [DOI] [PubMed] [Google Scholar]
- 61.Martin P, Gillen M, Ritter J, Mathews D, Brealey C, Surry D, et al. Effects of fostamatinib on the pharmacokinetics of oral contraceptive, warfarin, and the statins rosuvastatin and simvastatin: results from phase I clinical studies. Drugs R D. 2016;16:93–107. doi: 10.1007/s40268-015-0120-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Kaminsky LS, Zhang ZY. Human P450 metabolism of warfarin. Pharmacol Ther. 1997;73:67–74. doi: 10.1016/S0163-7258(96)00140-4. [DOI] [PubMed] [Google Scholar]
- 63.Lane S, Al-Zubiedi S, Hatch E, Matthews I, Jorgensen AL, Deloukas P, et al. The population pharmacokinetics of R- and S-warfarin: effect of genetic and clinical factors. Br J Clin Pharmacol. 2012;73:66–76. doi: 10.1111/j.1365-2125.2011.04051.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Martin P, Gillen M, Millson D, Oliver S, Brealey C, Surry D, et al. Effects of fostamatinib on the pharmacokinetics of the CYP2C8 substrate pioglitazone: results from in vitro and phase 1 clinical studies. Clin Pharmacol Drug Dev. 2016;5:170–179. doi: 10.1002/cpdd.243. [DOI] [PubMed] [Google Scholar]
- 65.U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). In vitro drug interaction studies: cytochrome P450 enzyme- and transporter-mediated drug interactions guidance for industry. https://www.fda.gov/media/134582/download. Accessed 22 Mar 2022.
- 66.Elsby R, Martin P, Surry D, Sharma P, Fenner K. Solitary inhibition of the breast cancer resistance protein efflux transporter results in a clinically significant drug-drug interaction with rosuvastatin by causing up to a 2-fold increase in statin exposure. Drug Metab Dispos. 2016;44:398–408. doi: 10.1124/dmd.115.066795. [DOI] [PubMed] [Google Scholar]
- 67.Xia CQ, Liu N, Miwa GT, Gan L-S. Interactions of cyclosporin a with breast cancer resistance protein. Drug Metab Dispos. 2007;35:576–582. doi: 10.1124/dmd.106.011866. [DOI] [PubMed] [Google Scholar]
- 68.Sáfár Z, Kecskeméti G, Molnár J, Kurunczi A, Szabó Z, Janáky T, et al. Inhibition of ABCG2/BCRP-mediated transport-correlation analysis of various expression systems and probe substrates. Eur J Pharm Sci. 2021;156:105593. doi: 10.1016/j.ejps.2020.105593. [DOI] [PubMed] [Google Scholar]
- 69.Keskitalo JE, Zolk O, Fromm MF, Kurkinen KJ, Neuvonen PJ, Niemi M. ABCG2 polymorphism markedly affects the pharmacokinetics of atorvastatin and rosuvastatin. Clin Pharmacol Ther. 2009;86:197–203. doi: 10.1038/clpt.2009.79. [DOI] [PubMed] [Google Scholar]
- 70.Alla VM, Agrawal V, DeNazareth A, Mohiuddin S, Ravilla S, Rendell M. A reappraisal of the risks and benefits of treating to target with cholesterol lowering drugs. Drugs. 2013;73:1025–1054. doi: 10.1007/s40265-013-0072-9. [DOI] [PubMed] [Google Scholar]
- 71.Maringwa J, Kågedal M, Hamrén UW, Martin P, Cox E, Hamrén B. Pharmacokinetic-pharmacodynamic modeling of fostamatinib efficacy on ACR20 to support dose selection in patients with rheumatoid arthritis (RA) J Clin Pharmacol. 2015;55:328–335. doi: 10.1002/jcph.406. [DOI] [PubMed] [Google Scholar]
- 72.Boström E, Öhrn F, Hanze E, Sandström M, Martin P, Wählby-Hamrén U. Exposure vs. response of blood pressure in patients with rheumatoid arthritis following treatment with fostamatinib. J Clin Pharmacol. 2014;54:1337–1346. doi: 10.1002/jcph.341. [DOI] [PubMed] [Google Scholar]
- 73.Kost-Alimova M, Sidhom E-H, Satyam A, Chamberlain BT, Dvela-Levitt M, Melanson M, et al. A high-content screen for mucin-1-reducing compounds identifies fostamatinib as a candidate for rapid repurposing for acute lung injury. Cell Rep Med. 2020;1:100137. doi: 10.1016/j.xcrm.2020.100137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Shen L, Su L, Turner JR. Mechanisms and functional implications of intestinal barrier defects. Dig Dis. 2009;27:443–449. doi: 10.1159/000233282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kitas GD, Abreu G, Jedrychowicz-Rosiak K, Miller JL, Nakov R, Panfilov S, et al. The effects of the spleen tyrosine kinase inhibitor fostamatinib on ambulatory blood pressure in patients with active rheumatoid arthritis: results of the OSKIRA-ABPM (ambulatory blood pressure monitoring) randomized trial. J Am Soc Hypertens. 2014;8:780–790. doi: 10.1016/j.jash.2014.08.013. [DOI] [PubMed] [Google Scholar]
- 76.Chen Y, Liu H, Huang Y, Lin S, Yin G, Xie Q. The cardiovascular risks of fostamatinib in patients with rheumatoid arthritis: a systematic review and meta-analysis. Front Pharmacol. 2021;12:632551. doi: 10.3389/fphar.2021.632551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Clemens GR, Schroeder RE, Magness SH, Weaver EV, Lech JW, Taylor VC, et al. Developmental toxicity associated with receptor tyrosine kinase Ret inhibition in reproductive toxicity testing. Birth Defects Res A Clin Mol Teratol. 2009;85:130–136. doi: 10.1002/bdra.20505. [DOI] [PubMed] [Google Scholar]