

Abstract
Aims
To investigate the correlations between meeting the muscle‐strengthening activities guideline, body fat %, and mortality for individuals living with obesity and to explore if these correlations are moderated by sex.
Methods
Data from 3915 adults (51.9% women; 48.1% men) living with obesity (body fat % ≥25 for men and ≥35 for women) from two cycles of the National Health and Nutrition Examination Survey (NHANES 2003‐04/2005‐06) were analyzed. Muscle‐strengthening activities were self‐reported via a questionnaire, body fat % was measured via Dual Energy X‐ray, and mortality was obtained via administrative data for an average of 10 years.
Results
18.7% of men and 15.2% of women living with obesity met the muscle‐strengthening activities guideline (p = 0.021). Sex was correlated with body fat %; (β (SE)= 11.34 (0.18); p ≤ 0.001) and risk of mortality (hazard ratio (95% confidence interval) = 0.36 (0.24–0.54); p ≤ 0.001), once adjusted for confounders (weekly aerobic activities, ethnicity, education, household income, smoking, and the sum of chronic conditions). The interaction between sex and meeting the muscle‐strengthening activities guideline was not significantly correlated with the studied outcomes.
Conclusion
Performing muscle‐strengthening activities a minimum of two times per week does not impact body fat % or risk of mortality (over 10 years) differently in men or women living with obesity.
Keywords: gender, obese, resistance training, strength training
1. INTRODUCTION
Obesity is a complex and costly disease. 1 Regardless of an individual's obesity status, physical activity is an essential component of health and weight management. 2 International physical activity guidelines state that adults should accumulate a minimum of 150 min of aerobic activities at moderate intensity and two sessions of muscle‐strengthening activities per week, 3 because of the multiple health benefits correlated with this practice. 4 Despite decades of promotion and evidence of the benefits of regular physical activity, the proportion of adults meeting both components of the guidelines (using self‐reported measures) is low. For example, in the United States, only 23% meet both components 5 with 30.2% of individuals meeting muscle‐strengthening activities recommendation 6 versus 52.6% meeting aerobic activities recommendation. 7 The proportion for meeting both guideline components is even lower (9%) in individuals living with obesity. 7
Individuals living with obesity may prefer muscle‐strengthening activities over aerobic exercise to reap the benefits of exercise. Individuals living with obesity are often stronger than their leaner counterparts, perhaps because of greater absolute muscle mass. 8 Additionally, individuals living with obesity tend to report a lower rate of perceived exertion 9 and display greater self‐efficacy 10 when performing muscle‐strengthening activities compared to aerobic exercises at the same intensity.
While muscle‐strengthening activities are recommended for both men and women, evidence suggests that women are less likely to engage in muscle‐strengthening exercises than men throughout their lifetime. 11 , 12 Muscle‐strengthening activities improve body composition in adults, 13 , 14 , 15 but the difference between men and women living with obesity is unknown. In two meta‐analyses on sex differences in muscular adaptations following strength training, 31 studies 16 and 17 studies 17 were analyzed. Their results showed that lower body and upper body strength gained following muscle‐strengthening interventions are different in men and women, explaining sex‐dependent adaptations. As suggested, sex and gender need to be explored as a moderator and not only as a confounder. 18
This study aims to investigate the correlations between meeting the muscle‐strengthening activities guideline, body fat % and mortality in people living with obesity and further explore if these correlations are moderated by sex.
2. MATERIALS AND METHODS
2.1. Study overview
This study used data collected from the National Health and Nutritional Examination Surveys (NHANES). NHANES is conducted bi‐yearly by the US Center for Disease Control and Prevention (CDC) to assess the US population's health, dietary practices, and nutritional status. It includes questionnaires, medical examinations, and laboratory biomonitoring methods to determine the prevalence of diseases and environmental exposures in a sample of the noninstitutionalized general US population. Participants receive a health examination at mobile examination centers and are interviewed in their homes. Each cycle, the CDC collects data on a new group of participants.
Although NHANES is cross‐sectional, the mortality status of participants is also tracked via administrative data. The 2003–2005 and 2005–2006 continuous NHANES cycles were combined and used in this study. These cycles were chosen because they contain data on body fat %, muscle‐strengthening activity participation, and time spent in moderate to vigorous physical activity (MVPA) calculated using accelerometers.
2.2. Study sample
An initial sample of 20,470 participants was available from the 2003–2004 and 2005–2006 NHANES databases. The inclusion criteria were: age 19 or above and had data on muscle‐strengthening activity participation, DXA calculated body fat %, and accelerometer measured MVPA levels. A total of 3915 participants were included in the current analysis once, removing people with no data on muscle‐strengthening activities (N = 6080); age 18 years old or younger (N = 3813); missing body fat % (N = 2062); not meeting the criteria for obesity (N = 1862); not having a minimum of 4 days data of accelerometer wear time (N = 2451); and missing data for smoking, household income, education and mortality (N = 287). No difference was observed between the age of the selected sample between men and women (51.6 years men vs. 52.0 years women p = 0.373), but a difference was observed for sex with slightly more women (51.9% women vs. 48.1% men; p = 0.016).
2.3. Exposure variables
2.3.1. Muscle‐strengthening activities
Participants self‐reported their muscle‐strengthening activities by answering the following questions: (1) Over the past 30 days, did you do any physical activities specifically designed to strengthen your muscles, such as lifting weight, push‐ups, or sit‐ups? If a participant answered yes, then they were asked the second question, (2) Over the past 30 days, how many times did you do these activities designed to strengthen your muscles, such as lifting weights, push‐ups, or sit‐ups? According to the most recent international physical activity guidelines, 3 it is recommended to perform muscle‐strengthening activities a minimum of two times/week. As a result, the sample was divided into two groups: meeting the muscle‐strengthening activities recommendation (≥8 times/30 days) or (<8 times/30 days).
2.3.2. Obesity
Body composition was captured via Dual‐energy X‐ray absorptiometry (DXA) (Hologic), and body fat % was estimated. Details of the DXA protocol are available on the NHANES website. 19 Based on the WHO definition, men having ≥ 25% and women having ≥35% body fat were classified as living with obesity. 20 Body mass index (BMI) was calculated following standardized procedures; weight (kg) divided by height (m) squared. 21
2.3.3. Mortality rate
Mortality data were obtained via the National Death Index, which is linked with the NHANES database. 22 The time to death was recorded in years based on the day of a participant's examination to the time of death or up to the end of follow‐up. The average follow‐up time for the sample for 10.2 ± 2.3 years.
2.4. Potential confounders
The following variables were selected as potential confounders based on relevance and availabilities. Demographic characteristics included age, ethnicity (Mexican American and other Hispanic; non‐Hispanic White; non‐Hispanic Black; Others), education (below diploma grade 12; high school and some college degree; college graduate and above), smoking behavior (current smoker or nonsmoker), and household income (under $20,000; between $20,000 and $74,999; $75,000 and above). The sum of chronic conditions was computed using five conditions that could influence the ability to perform muscle‐strengthening activities: arthritis, cardiovascular diseases, diabetes, lung diseases, and cancer. These conditions were self‐reported using the question “Did a doctor ever say you had_________?”; the possible answers being yes, or no. One score was given for each yes, and a sum out of five (either ≥ 2 or < 2) was used in the analysis. The aerobic activities were also considered confounders, collected using the ActiGraph 7164 accelerometer (ActiGraph). Participants were asked to wear an accelerometer for seven consecutive days. A minimum of 4 days of data and 10 h per day of wear time was required to be included in study. 23 Moderate intensity cut‐point for physical activity was defined as ≥5998 counts/min. 24 Weekly time (minutes) of aerobic activities spent at moderate to vigorous intensity was calculated. Menopause was quantified using two available variables. The first variable came from a question asking whether the individual had a period in the past 12 months. The second variable asked the individual who responded no to the above question whether this was due to pregnancy, breastfeeding, menopause/hysterectomy, medical condition/treatment or other. Those who answered that their lack of a period in the last 12 months was due to menopause/hysterectomy were defined as being menopaused.
2.5. Statistical analysis
Descriptive data are reported as unweighted average ± standard deviation or N (%) by sex. Potential differences among groups were tested using the Chi‐square test or t tests. Weighted linear regression models were used to test if practicing muscle‐strengthening activities (≥ two sessions/week) affects the body fat % of men and women living with obesity differently after adjusting for potential confounders. Model 1 was unadjusted. Model 2 was adjusted for age, and aerobic activity (minutes of MVPA per week). Model 3 was further adjusted for ethnicity, education, and household income. The fully adjusted model was further adjusted for smoking and the sum of chronic conditions. Kaplan–Meier and Proportional hazard Cox regression were used to describing and determine if meeting the muscle‐strengthening activities guideline (≥ two sessions/week) was correlated with mortality at a different rate for men and women, once weighted and adjusted for covariates. Statistical analyses were performed using R 4.1.1.1 and SPSS 21.0.
3. RESULTS
Descriptive data for the study sample are presented in Table 1. The average age, BMI, and body fat % of participants was 51.8 ± 16.4 years, 30.1 ± 5.8, and 37.0 ± 7.3%, respectively. Participants spent an average of 138.6 ± 146.4 min of MVPA in a week. The majority of the sample was non‐Hispanic White (51.7%) and completed high school (54.2%). Among women who had data for menopausal status (n = 1183), 58.2% of women were categorized as menopausal. Only 28.8% of participants were categorized as having low household income (less than $20,000), and 18.8% reported current smokers. About a fifth of the sample (12.2%) self‐reported having a minimum of two of the five chronic conditions evaluated. A proportion of 18.7% of men and 15.2% of women (p = 0.021) met the muscle‐strengthening activities recommendation.
Table 1.
Descriptive characteristics of the study sample
| Men | Women | ||
|---|---|---|---|
| N = 3915 | N = 1882 | N = 2033 | |
| Age (years) | 51.8 ± 16.4 | 51.6 ± 16.5 | 52.0 ± 16.2 |
| BMI (kg/m2) | 30.1 ± 5.8 | 29.8 ± 4.9 | 30.4 ± 6.5* |
| Body fat percentage (%) | 37.0 ± 7.3 | 30.9 ± 4.0 | 42.7 ± 4.5* |
| Weekly minutes spent at moderate to vigorous intensity (min) | 138.6 ± 146.4 | 178.0 ± 170.5 | 102.6 ± 108.3* |
| Ethnicity (non‐Hispanic White) | 2126 (51.7) | 1018 (54.0) | 1008 (49.6)* |
| Education (high school or more) | 2122 (54.2) | 971 (51.5) | 1151 (56.6)* |
| Household income (less than $20,000) | 1129 (28.8) | 483 (25.6) | 646 (31.8)* |
| Current smoker (yes) | 736 (18.8) | 416 (22.1) | 320 (15.7)* |
| Reporting ≥ 2 chronic conditions | 450 (12.2) | 362 (12.5) | 812 (11.9) |
| Menopausal status | – | – | 1183 (58.2) |
| Years of follow‐up for mortality outcome | 10.3 ± 2.3 | 10.0 ± 2.6 | 10.5 ± 2.0* |
Note: N (%) or average ± SD.
Abbreviations: BMI, body mass index; SD, standard deviation.
Significant difference between men and women.
The results of the regression model fully adjusted for potential confounders (MVPA, ethnicity, education, household income, smoking, sum of chronic conditions) showed that sex (being women) (β = 11.35; p ≤ 0.001) and meeting the muscle‐strengthening activities guideline (β = −0.77; p = 0.004) were significantly correlated with lower body fat %. However, the interaction between sex and meeting muscle‐strengthening activities guideline was not statistically significant (β = −0.14; p = 0.681) (Table 2). The regression model results did not change with the absence of MVPA as a confounder.
Table 2.
Muscle‐strengthening activities 2+/week and body fat %
| Model 1 | Model 2 | Model 3 | Full model | |
|---|---|---|---|---|
| Sex (women) | 11.73 (0.15) | 11.43 (0.18)* | 11.41 (0.18)* | 11.36 (0.18)* |
| Muscle‐strengthening activities 2+/week | −1.03 (0.25) | −0.79 (0.25) | −0.70 (0.25)* | −0.78 (0.25)* |
| Muscle‐strengthening activities 2+/week* sex | −0.13 (0.36) | −0.11 (0.35) | −0.16 (0.35) | −0.14 (0.35) |
Note: Data presented as β‐value (SE). Model 1 is unadjusted, Model 2 adjusted for age, aerobic activity (minutes of MVPA per week), and Model 3, further adjusting for ethnicity, education, household income, the fully adjusted model is further adjusted for smoking, sum of chronic conditions.
Abbreviations: MVPA, moderate to vigorous physical activity; SE, standard error.
Represents a p value below 0.01.
The average follow‐up for survival analysis was 10 years ± 2.3, during which 644 deaths were recorded: 19.0% men versus women 12.0% (p ≤ 0.001). The proportion of death was nonsignificantly lower for men meeting the muscle‐strengthening activities guideline compared with men not meeting the guideline (15.0% vs.19.8%). Similar results were seen in women meeting the muscle‐strengthening activities guideline compared to women not meeting the guideline (9.7% vs. 12.1%) (Figure 1).
Figure 1.
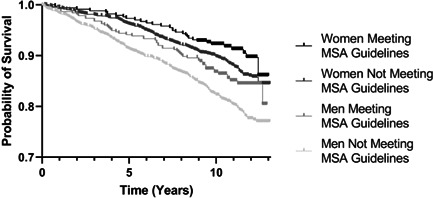
Probability of survival of men and women meeting the muscle strength activities guideline. *MSA guidelines = muscle‐strengthening activities two times or more per week.
Being a woman protected against death (hazard ratio [HR] (95% confidendence interval [CI]) = 0.36 (0.24–0.54); p ≤ 0.001). However, meeting the muscle‐strengthening activities guideline was not significantly correlated with mortality (p = 0.44) when fully adjusted for potential confounders (MVPA, ethnicity, education, household income, smoking, and sum of chronic conditions). The interaction between sex and meeting muscle‐strengthening activities guideline was not statistically significant (p = 0.36) (Figure 2).
Figure 2.
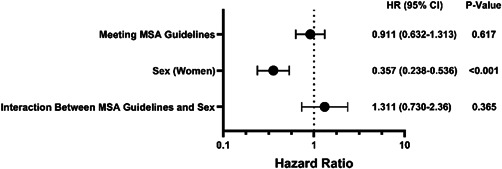
The association between selected variables and risk of death. Meeting MSA Guidelines = Two or more sessions/week. MSA, muscle‐strengthening activities
4. DISCUSSION
The main objective of the current study was to investigate the correlations between meeting the muscle‐strengthening activities guideline, body fat %, and mortality in people living with obesity and further explore if these correlations are moderated by sex. The results show that more men than women living with obesity meet the muscle‐strengthening activities guideline. Meeting the muscle‐strengthening activities guideline was correlated with a lower body fat % in both men and women. There was no interaction between sex and meeting the muscle‐strengthening activities guideline; meaning that practicing muscle‐strengthening activities equally influences men and women living with obesity in terms of body fat % and mortality.
Although it is known that sex and gender influences body fat %, mortality, and the preference for muscle‐strengthening activities, this study is among the first attempts to understand the potential sex interaction for adults living with obesity reaching muscle‐strengthening activities guidelines or not. As observed before, women are less likely to engage in muscle‐strengthening activities than men, 11 , 12 and the same applies to adults living with obesity. Given the strength advantages that both men and women living with obesity have over lean people, tailored suggestions to both men and women living with obesity about the specific benefits of muscle‐strengthening activities to them might be a useful addition to public health interventions.
Although systematic reviews with meta‐analysis design 16 , 17 included 40 studies have stated that men and women may gain relative lower body (95% CI 0.33–0.10, p = 0.0003) and upper body (E.S. = 0.60 ± 0.16; p = 0.002) strength differently when performing muscle‐strengthening activities, these studies almost exclusively focus on muscle strength and muscle size, but not on body fat % or mortality rate. However, using BMI cut‐offs to classify obesity in two different cross‐sectional studies found that meeting muscle‐strengthening activities guidelines was correlated with a lower rate of obesity in 400,000 US adults 6 and 1.7 million US adults. 25 In a prospective cohort study, meeting the muscle‐strengthening activities guideline was correlated with a reduced risk of developing obesity. 26 Our findings could address the gap in the literature as sex does not appear to significantly moderate body fat % in individuals living with obesity who are meeting muscle‐strengthening activities guidelines.
Most studies on muscle‐strengthening activities and mortality have focused on the correlation between muscle strength and mortality rather than participation in muscle‐strengthening activities and mortality. 27 , 28 , 29 , 30 Many beneficial outcomes can be obtained when performing muscle‐strengthening activities besides muscle strength. For example, in a study, 31 the authors reported a reduced risk of cardiovascular disease by 17% (HR: 0.83, 95% CI: 0.72–0.96) and type 2 diabetes by 30% (HR: 0.70, 95% CI: 0.61–0.80) in women who had any muscle‐strengthening activities experiences in their life. Other outcomes such as metabolic risk factors and anthropometrics have been also studied where an improvement was shown in cardiovascular (endothelium) function and waist circumference as a result of performing muscle‐strengthening activities by 3% (95% CI: 1.5–4.5) and 1.4% (95% CI:− 2.7 to −0.8) respectively. 32 Nonetheless, a meta‐analysis of 11 prospective studies (370,256 participants; mean follow‐up = 8.85 years) 33 reported that performing muscle‐strengthening activities was independently correlated with 21% lower risk of all‐cause mortality (HR; 95% CI, 0.79; 0.69–0.91). Our results do not confirm the correlation between muscle‐strengthening activities and mortality rate, and this can potentially be explained by the limitations in the current study, such as the studied population and mortality timeline as the differences may become more pronounced over time (Figure 1).
4.1. Strengths and limitations
The current study is strengthened by using NHANES database, which is nationally representative and is an appropriately weighted sample. Using the DXA to measure body fat % reduced measurement errors and social desirability bias of reporting weight and height and avoided many of the issues BMI measurements present. As for limitation, the weighted analysis aimed to be used for the original sample. Therefore, the final sample may not represent individuals living with obesity in the US participation in muscle‐strengthening activities was self‐reported and therefore potentially biased. Also, meeting muscle strength activities guidelines was considered in 4 weeks (28 days), while the NHANES database is based on a month (30 days).
5. CONCLUSION
This study shows that meeting muscle‐strengthening activities is correlated with lower body fat %, but no interaction was observed between sex and the two outcomes studied. Therefore, based on our results, performing muscle‐strengthening activities a minimum of 2 days per week does not impact body fat % or risk of mortality over 10 years in men and women living with obesity differently. The biggest addition to the literature of this study is that no significant interaction between sex and muscle‐strengthening activities was observed for the studied outcomes. Therefore, regular participation in muscle‐strengthening activities benefits both men and women living with obesity similarly.
6. PERSPECTIVE
Performing muscle‐strengthening activities reduces the risks correlated with many chronic conditions such as obesity. Men and women experience different barriers and facilitators when participating in exercise. Little research examined if the benefits of doing muscle‐strengthening activities for individuals living with obesity are moderated by sex. The results of the current study suggest that performing muscle‐strengthening activities a minimum of two times per week does not impact body fat % or risk of mortality (over 10 years) differently in men or women living with obesity. As a result, muscle‐strengthening activities should be promoted equally for both sexes.
AUTHOR CONTRIBUTIONS
M. Keshavarz: Conceptualization; formal analysis; investigation; methodology; project administration; writing—original draft. M. Sénéchal: Conceptualization; data curation; formal analysis; supervision; writing—review & editing. S. U. Dombrowski: Conceptualization; methodology; supervision; writing—review & editing. D. Meister: Data curation; software; writing—review & editing. D. R. Bouchard: Conceptualization; formal analysis; methodology; project administration; supervision; writing—review & editing.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
TRANSPARENCY STATEMENT
The corresponding author confirms that the manuscript is an honest, accurate, and transparent account of the study being reported, no important aspects of the study have been omitted, and any discrepancies from the study as planned have been explained.
Keshavarz M, Sénéchal M, Dombrowski SU, Meister D, Bouchard DR. Examining the role of sex on the benefits of muscle‐strengthening activities for people living with obesity: a cross‐sectional study. Health Sci Rep. 2022;5:e720. 10.1002/hsr2.720
DATA AVAILABILITY STATEMENT
All the relevant data are in the manuscript. The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab. 2004;89:2583‐2589. [DOI] [PubMed] [Google Scholar]
- 2. Jakicic JM, Otto AD. Treatment and prevention of obesity: what is the role of exercise? Nutr Res. 2006;64:57‐61. [DOI] [PubMed] [Google Scholar]
- 3. WHO . 2020. Physical activity. https://www.who.int/news-room/fact-sheets/detail/physical-activity
- 4. Bennie JA, Shakespear‐Druery J, De Cocker K. Muscle‐strengthening exercise epidemiology: a new frontier in chronic disease prevention. Sports Med‐Open. 2020;6:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bennie JA, De Cocker K, Teychenne MJ, Brown WJ, Biddle SJH. The epidemiology of aerobic physical activity and muscle‐strengthening activity guideline adherence among 383,928 US adults. Int J Behav Nutr Phys Act. 2019;16:1‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bennie JA, Lee D‐c, Khan A, et al. Muscle‐strengthening exercise among 397,423 US adults: prevalence, correlates, and associations with health conditions. Am J Prev Med. 2018;55:864‐874. [DOI] [PubMed] [Google Scholar]
- 7. Bennie JA, Pedisic Z, van Uffelen JGZ, et al. The descriptive epidemiology of total physical activity, muscle‐strengthening exercises and sedentary behaviour among Australian adults–results from the National nutrition and Physical Activity Survey. BMC Public Health. 2015;16:1‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Gill A, Kok G, Peters G‐JY, et al. The psychological effects of strength exercises in people who are overweight or obese: a systematic review. Sports Med. 2017;47:2069‐2081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ten Hoor GA, Plasqui G, Ruiter RA, et al. A new direction in psychology and health: resistance exercise training for obese children and adolescents. 31. Taylor & Francis; 2016:214‐219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Gill A, Plasqui G, Schols AM, Kok G. Combating adolescent obesity: an integrated physiological and psychological perspective. Curr Opin Clin Nutr Metab Care. 2014;17:521‐527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Control CfD, Prevention . Data 2010: The healthy people 2010 database. National Center for Health Statistics; 2011. [Google Scholar]
- 12. Strain T, Fitzsimons C, Kelly P, Mutrie N. The forgotten guidelines: cross‐sectional analysis of participation in muscle strengthening and balance & co‐ordination activities by adults and older adults in Scotland. BMC Public Health. 2016;16:1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ho SS, Dhaliwal SS, Hills AP, Pal S. The effect of 12 weeks of aerobic, resistance or combination exercise training on cardiovascular risk factors in the overweight and obese in a randomized trial. BMC Public Health. 2012;12:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lynch HM, Buman MP, Dickinson JM, Ransdell LB, Johnston CS, Wharton CM. No significant differences in muscle growth and strength development when consuming soy and whey protein supplements matched for leucine following a 12 week resistance training program in men and women: a randomized trial. Int J Environ Res Public Health. 2020;17:3871‐3875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Willis LH, Slentz CA, Bateman LA, et al. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J Appl Physiol. 2012;97:188‐193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Jones MD, Wewege MA, Hackett DA, Keogh J, Hagstrom AD. Sex differences in adaptations in muscle strength and size following resistance training in older adults: a systematic review and meta‐analysis. Sports Med. 2021;51:503‐517. [DOI] [PubMed] [Google Scholar]
- 17. Roberts BM, Nuckols G, Krieger JW. Sex differences in resistance training: a systematic review and meta‐analysis. J Strength Conditioning Res. 2020;34:1448‐1460. [DOI] [PubMed] [Google Scholar]
- 18. Regitz‐Zagrosek V. Sex and gender differences in health: science & society series on sex and science. EMBO Rep. 2012;13:596‐603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. NHANES . 2003‐2004 data documentation, codebook, and frequencies. Dual Energy X‐ray Absorptiometry ‐ Android/Gynoid. 2013. https://wwwn.cdc.gov/Nchs/Nhanes/2003-2004/DXXAG_C.htm
- 20. WHO . Physical status: the use of and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organization; 1995. [PubMed] [Google Scholar]
- 21. Navalta JW, Stone WJ, Lyons TS. Ethical issues relating to scientific discovery in exercise science. Int J Exer Sci. 2019;12:1‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. NHIS . Public‐use linked mortality file. 2020. https://www.cdc.gov/nchs/data/datalinkage/public-use-2015-linked-mortality-file-description.pdf
- 23. Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181‐188. [DOI] [PubMed] [Google Scholar]
- 24. Metzger JS, Catellier DJ, Evenson KR, Treuth MS, Rosamond WD, Siega‐Riz AM. Patterns of objectively measured physical activity in the United States. Med Sci Sports Exerc. 2008;40:630‐638. [DOI] [PubMed] [Google Scholar]
- 25. Bennie JA, De Cocker K, Pavey T, Stamatakis E, Biddle S, Ding D. Muscle strengthening, aerobic exercise, and obesity: a pooled analysis of 1.7 million US adults. Obesity. 2020;28:371‐378. [DOI] [PubMed] [Google Scholar]
- 26. Brellenthin AG, Lee D‐C, Bennie JA, Sui X, Blair SN. Resistance exercise, alone and in combination with aerobic exercise, and obesity in Dallas, Texas, US: a prospective cohort study. PLoS Med. 2021;18:1003‐1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Nakamura T, Kamiya K, Hamazaki N, et al. Quadriceps strength and mortality in older patients with heart failure. Can J Cardiol. 2021;37:476‐483. [DOI] [PubMed] [Google Scholar]
- 28. Malhotra R, Tareque MI, Tan NC, Ma S. Association of baseline hand grip strength and annual change in hand grip strength with mortality among older people. Arch Gerontol Geriat. 2020;86:103‐109. [DOI] [PubMed] [Google Scholar]
- 29. Jochem C, Leitzmann M, Volaklis K, Aune D, Strasser B. Association between muscular strength and mortality in clinical populations: a systematic review and meta‐analysis. J Am Med Dir Assoc. 2019;20:1213‐1223. [DOI] [PubMed] [Google Scholar]
- 30. Ruiz JR, Sui X, Lobelo F, et al. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008;61:337‐345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Shiroma EJ, Cook NR, Manson JE, et al. Strength training and the risk of type 2 diabetes and cardiovascular disease. Med Sci Sports Exerc. 2017;49:40‐48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Stensvold D, Tjønna AE, Skaug E‐A, et al. Strength training versus aerobic interval training to modify risk factors of metabolic syndrome. J Appl Physiol. 2010;108:804‐810. [DOI] [PubMed] [Google Scholar]
- 33. Saeidifard F, Medina‐Inojosa JR, West CP, et al. The association of resistance training with mortality: a systematic review and meta‐analysis. Eur J Prev Cardiol. 2019;26:1647‐1665. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All the relevant data are in the manuscript. The data that support the findings of this study are available from the corresponding author upon reasonable request.