

Summary
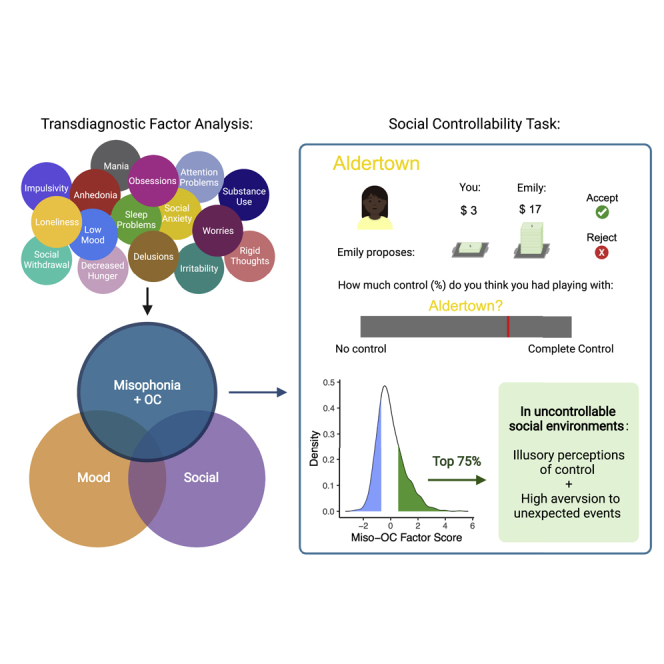
Misophonia is a disorder in which certain sounds produced by other people lead to intense negative reactions. It remains unknown how misophonia relates to other psychiatric conditions or impairments. To identify latent constructs underlying symptoms, we conducted a factor analysis consisting of items from questionnaires assessing symptoms of misophonia and other psychiatric conditions. One thousand forty-two participants completed the questionnaires and a social exchange task in which they either could (“controllable”) or could not (“uncontrollable”) influence future monetary offers from other people. Misophonia and obsessive-compulsive (OC) symptoms loaded onto the same factor. Compared with individuals with low Miso-OC factor scores, individuals with high scores reported higher perceived controllability of their social interactions during the uncontrollable condition and stronger aversion to social norm violations in the uncontrollable compared with the controllable condition. Together, these results suggest misophonia, and OC symptoms share a latent psychiatric dimension characterized by aberrant computations of social controllability.
Subject areas: Biological sciences, Neuroscience, Behavioral neuroscience, Clinical neuroscience, Sensory neuroscience
Graphical abstract
Highlights
-
•
Factor analysis of psychiatric survey items in over 1,000 subjects reveals three factors
-
•
Misophonia and obsessive-compulsive (OC) symptoms load onto the same factor
-
•
Those with high miso-OC factor scores display illusory perceptions of social control
-
•
The same individuals also show increased aversion to unexpected social events
Biological sciences; Neuroscience; Behavioral neuroscience; Clinical neuroscience; Sensory neuroscience
Introduction
Misophonia is a disorder in which sounds generated by other people—such as slurping, chewing, or clicking a pen—lead to intense, negative physical, and/or emotional responses, including disgust, irritation, rage, or anxiety in the individual (Brout et al., 2018; Wu et al., 2014). It is estimated that as much as 20% of the population may experience some form of misophonia, with a smaller subset experiencing a more severe form (Brout et al., 2018; Wu et al., 2014). The heightened physiological responsivity and emotional reactivity experienced by misophonia patients in response to trigger sounds often correspond with high levels of distress and debilitating impairments in daily functioning, including strained relationships and isolation due to social avoidance (Brout et al., 2018; Jager et al., 2021).
The social nature of triggers in misophonia suggests that social impairments might play an important role in the aversive response (Rouw and Erfanian, 2018; Schröder et al., 2013). Initial evidence suggests that negative reactions are associated with the perceived source of the sound rather than its particular acoustic properties (Edelstein et al., 2013). For example, individuals with misophonia have reported that feelings of anger and distress often dissipate upon realization that a trigger sound is coming from a source other than another human, such as an animal, a machine, or themselves (Edelstein et al., 2013; Natalini et al., 2020). The specificity of misophonic reactions to social sounds may be related to the idea of agency, which refers to voluntary control over one’s actions. Sounds produced by other people are uniquely intentional (Tomasello and Rakoczy, 2003) and can be misattributed to the self, especially in psychiatric populations (de Bézenac et al., 2015; Kashihara et al., 2017). Misophonia may therefore involve impairments in agency discrimination and associated disruptions in perceived controllability.
Despite growing interest of researchers seeking to understand misophonia and a recent consensus definition (Swedo et al., 2022), we still have little understanding of its exact causes, mechanisms, or comorbidities, posing major challenges for patients seeking treatment (Brout et al., 2018). In particular, it is unknown to what extent misophonia exists on a spectrum, how it relates to more established psychiatric diagnoses, or how social and control-related cognition may play a role in the disorder. To fill these gaps in the knowledge, the current study used large-scale online assessment to characterize misophonia by (1) identifying the relationship between misophonia and existing psychiatric symptom dimensions and (2) examining the role of perceived social controllability in individuals with reported misophonia symptoms.
Misophonia shows high rates of co-occurrence with anxiety (Quek et al., 2018), posttraumatic stress disorder (PTSD; Erfanian et al., 2019; Rouw and Erfanian, 2018), eating disorders (Kluckow et al., 2014), and obsessive-compulsive disorder (OCD) (Erfanian et al., 2019; Jager et al., 2020). Such disorders share a common feature of dysregulations in perceived controllability, which represents the amount of influence individuals believe they have over their environment or their own internal states (Wadsworth and Hayes-Skelton, 2020). This observation raises the possibility that misophonia represents a transdiagnostic symptom common to disorders with disrupted perceptions of controllability. Although perceived controllability has yet to be directly explored in misophonia, much work has shown that anxiety, PTSD, eating disorders, and OCD symptoms are associated with low levels of perceived controllability (Berman, 2006; Gallagher et al., 2014a; Wadsworth and Hayes-Skelton, 2020). In contrast, some work suggests that OCD symptoms are actually associated with a high illusory sense of control (Reuven-Magril et al., 2008). It may be the case that levels of perceived controllability in such disorders vary depending on the situation. For instance, individuals with misophonia may present with high baseline levels of perceived controllability that become low in response to trigger sounds, as control passes into the hands of another. As such, deficits in the perception of controllability may represent an underlying component of these disorders.
Given the high rates of comorbidity between misophonia and disorders related to control, our primary hypothesis explored whether items from the misophonia questionnaire loaded onto a factor with items from the OC, anxiety, and eating disorder questionnaires. However, given the social nature of common trigger sounds, we considered the alternative hypothesis that items from the misophonia questionnaire would load onto a factor with items from questionnaires assessing disorders characterized by social impairment, such as autism spectrum disorder (ASD). Furthermore, given the relevance of control and social context to the phenomenology of the disorder, we hypothesized that individuals with high levels of self-reported misophonia symptoms would perceive inaccurate levels of control within a social environment and show more aversive reactions to events that occur outside of their control. To test these hypotheses, participants completed questionnaires assessing symptoms of misophonia and 13 other psychiatric conditions. A factor analysis including each individual item from the surveys was used to identify the latent constructs underlying these symptoms. In addition, an interactive social controllability task probed the role of control within social environments in misophonia.
Results
Misophonia characterization
Recruited online through Prolific, 1,175 participants completed 14 questionnaires assessing symptoms of misophonia and various other psychiatric conditions (see STAR Methods). Misophonia scores, as measured by the Amsterdam Misophonia Scale (A-MISO-S) ranged from 0 (indicating no symptoms) to 19 (indicating severe symptoms). The mean score on the A-MISO-S was 5.47 with an SD of 3.71. 54.9% of participants had clinically significant symptoms (n = 645, total score: 5–24), although only 15.5% of participants had at least moderate symptoms (n = 182, total score: 10–24). Such results are consistent with prior prevalence studies using this measure (Figure 1; Naylor et al., 2020).
Figure 1.

Characterization of misophonia within our sample
The histogram shows the spread of total scores from the A-MISO-S (Amsterdam Misophonia Scale; n = 1,175). Bins are color coded by severity range (subclinical, mild, moderate, and severe). In total, 530 participants reported subclinical symptoms (45.1%), 463 participants reported mild symptoms (39.4%), 168 participants reported moderate symptoms (14.3%), 14 reported severe symptoms (1.2%), and 0 reported extreme symptoms (0%).
Factor analysis
In order to identify potential latent transdiagnostic constructs in the data and to identify the natural psychiatric and misophonic symptom clusters among participants, a factor analysis was performed using all individual items from the psychiatric surveys rather than total scores (see STAR Methods). Prior work has shown this to be an effective method for identifying psychiatric symptom dimensions (Gillan et al., 2016). The Cattell-Nelson-Gorsuch (CNG) test determined three factors to be appropriate for our data. Given this, we extracted three dissociable factors, which we labeled “mood,” “social,” and “Miso-OC,” based on the individual items that loaded most highly. Specifically, the mood factor consisted of items that came primarily from the happiness (negatively, mean loading = −0.72, SD = 0.11), anxiety (mean loading = 0.65, SD = 0.11), stress (mean loading = 0.64, SD = 0.04), loneliness (mean loading = 0.56, SD = 0.15), depression (mean loading = 0.49, SD = 0.20), and apathy (mean loading = 0.33, SD = 0.15) questionnaires. Items that loaded most highly onto the social factor were primarily from the avoidant personality disorder (mean loading = 0.52, SD = 0.17), social anxiety (mean loading = 0.54, SD = 0.13), and ASD (mean loading = 0.43, SD = 0.20) questionnaires. Items that loaded most highly onto the Miso-OC factor were primarily from the misophonia (mean loading = 0.30, SD = 0.05) and OC (mean loading = 0.48, SD = 0.05) questionnaires (Figure 2 and Table 1).
Figure 2.

Visualization of factor analysis loadings
The plot shows the loading of each item, represented by individual bars, onto each of the three factors: mood (F1), social (F2), and Miso-OC (F3). Items are color coded by the psychiatric questionnaire to which they belong. Black boxes indicate the highest loading items for each factor. ASD: autism spectrum disorder; AvPD: avoidant personality disorder; BPD: borderline personality disorder; OC: obsessive compulsive.
Table 1.
Factor analysis loadings
| Factor 1: Mood Mean (SD) | Factor 2: Social Mean (SD) | Factor 3: Miso-OCD Mean (SD) | |
|---|---|---|---|
| Apathy | 0.33 (0.15) | 0.23 (0.15) | −0.06 (0.13) |
| Stress | 0.64 (0.04) | −0.05 (0.06) | 0.11 (0.15) |
| Happiness | −0.72 (0.11) | −0.09 (0.01) | 0.12 (0.11) |
| Depression | 0.49 (0.20) | 0.005 (0.06) | 0.10 (0.16) |
| Trait Anxiety | 0.65 (0.11) | 0.01 (0.04) | 0.10 (0.18) |
| Loneliness | 0.56 (0.15) | 0.06 (0.22) | 0.02 (0.11) |
| BPD | 0.06 (0.08) | 0.11 (0.07) | 0.15 (0.05) |
| Social Anxiety | −0.04 (0.04) | 0.54 (0.13) | 0.18 (0.08) |
| AvPD | 0.19 (0.10) | 0.52 (0.17) | 0.03 (0.09) |
| ASD | 0.07 (0.12) | 0.43 (0.20) | 0.05 (0.19) |
| Eating Disorders | 0.03 (0.09) | 0.05 (0.06) | 0.22 (0.09) |
| Alcohol Use | 0.06 (0.05) | −0.09 (0.05) | 0.24 (0.08) |
| OC | 0.13 (0.16) | 0.05 (0.05) | 0.48 (0.05) |
| Misophonia | 0.09 (0.05) | 0.18 (0.04) | 0.30 (0.05) |
The mean and SD for loadings of items belonging to each psychiatric questionnaire onto each factor are shown. Bold entries represent higher loading (≥ 0.30); underlined entries represent medium loading (≥ 0.2).
ASD, autism spectrum disorder; AvPD, avoidant personality disorder; BPD, borderline personality disorder; OC, obsessive compulsive.
To gain a more in-depth conceptual understanding of the factor on which misophonia symptoms loaded most highly, we also identified the items that loaded most highly from other questionnaires. Such items included, from the anxiety questionnaire: “Some unimportant thoughts run through my mind and bother me,” “I have disturbing thoughts,” and “I get in a state of tension or turmoil as I think over my recent concerns and interests; ” from the depression questionnaire: “I am restless and can't keep still; ” from the ASD questionnaire: “I have been told that I talk too much about certain topics; ” from the eating disorders questionnaire: “[I] Feel uncomfortable after eating sweets;” and from the alcohol use questionnaire: “How often during the last year have you had a feeling of guilt or remorse after drinking?” Although these items represent a diverse set of symptoms, they generally reflect a pattern of disrupted control (i.e., intrusive thoughts and impulse control).
Social controllability
In order to investigate the role of social control in misophonia, we employed a task previously developed by our lab (Na et al., 2021) that explores how individuals exploit controllability in their social environments (Figure 3). The task is a take on the classic ultimatum game (Güth et al., 1982), with the addition of a novel social controllability component. For the task, 1,041 participants decided whether to accept or reject a split of $20 proposed by other people. Participants played with two teams representing two conditions in which they unknowingly could (“controllable”) or could not (“uncontrollable”) influence future monetary offers from other team members. At the end of the task, participants rated how much control they felt they had over each team (see STAR Methods).
Figure 3.

Task paradigm
(A) Panels show the screens that were presented to participants during the task. Participants played the game with two different teams sequentially, the order of which was counterbalanced. For each team, participants viewed a set of character avatars and the team’s name and then played 30 rounds of the game with various team members, represented by avatars and names. Team membership was denoted by the color of the avatars’ shirts. After the partner was presented, an offer amount was shown with corresponding stacks of money. Participants could then choose to accept or reject the proposal. Choices were followed by outcome presentation. At the end of the task, participants were asked to rate how much influence they thought they had on the offers from each team.
(B) In the controllable condition, the next offer increased (or decreased) by $0, 1, or 2 with a uniform probability (⅓ each) if participants rejected (or accepted).
Group formation
To assess relationships between social controllability and the latent construct underlying misophonia symptoms, we divided the subset of 1,041 participants who completed the questionnaires and the task into groups based on the highest and lowest quartile of scores on the Miso-OC Factor (n = 260 participants per group; see Table 2 for group characteristics).
Table 2.
Group characteristics
| High Miso-OCD Group (n = 260) mean/count (SD/%) | Low Miso-OCD Group (n = 260) mean/count (SD/%) | Group Comparison t/F (p value) | |
|---|---|---|---|
| Age (years) | 31.6 (11.17) | 39.3 (14.17) | 6.9 (p < 0.001)∗∗∗ |
| Sex (female) | 143 (55.0%) | 114 (43.8%) | 6.2 (p = 0.012)∗ |
| Gender (female) | 135 (51.9%) | 115 (44.2%) | 8.6 (p = 0.003)∗∗ |
| ICAR Total | 5.80 (3.31) | 6.99 (3.45) | 4.0 (p < 0.001)∗∗∗ |
| Education Level (13–15 years, some college) | 106 (40.8%) | 84 (32.3%) | 2.4 (p = 0.12) |
| Income ($100,000 to $149,999) | 32 (12.3%) | 43 (16.5%) | 0.63 (p = 0.43) |
| A-MISO-S Score | 7.90 (3.77) | 3.63 (2.82) | −14.6 (p < 0.001)∗∗∗ |
Demographic information is shown for the high (n = 260) and low (n = 260) Miso-OC groups. Welch t tests examined differences between continuous variables; one-way ANOVA examined differences between factor variables. For education, gender, and income levels, counts and percentages for the most common category are shown.
A-MISO-S, Amsterdam Misophonia Scale; ICAR, International Cognitive Ability Resource.
Significance levels for Welch t tests and ANOVAs: ∗∗∗p < 0.001, ∗∗p < 0.01, ∗p < 0.05.
Model-agnostic task behavior
To explore task validity, we examined descriptive task behavior in both low and high Miso-OC groups. Both groups successfully raised the offers over time under the controllable condition compared with the uncontrollable condition, in which offers were random (Figures 4A and 4B). The mean offer over all trials was also comparable between the two groups for the controllable condition (mean offer low Miso-OC group = 6.03, mean high Miso-OC group = 5.96, t(517.87) = 0.425, p = 0.67).
Figure 4.

Model agnostic task results
(A–D) The offer trajectories were comparable between the low and high Miso-OC groups under the (A) controllable and (B) uncontrollable conditions. The rejection patterns by offer size were also comparable between groups under the (C) controllable and (D) uncontrollable conditions.
(E) Bar plot shows a significant interaction effect of Miso-OC group by condition on perceived controllability.
(F) Estimation plot of the same data emphasizing the effect size of interest: the difference between Miso-OC group means. Here, relative to individuals in the low Miso-OC group, those in the high group report higher perceived controllability in the uncontrollable condition.
Error bars and shading represent SE. In the mean difference estimation plot, dots represent each included individual. Larger circles with lines represent the 95% confidence intervals. Distributions of expected sampling error for the difference between the means are shown in gray.
See also Tables S1–S4. Significance levels for post-hoc Welch t tests: ∗∗∗p < 0.001, ∗∗p < 0.01, ∗p < 0.05.
The groups also showed similar rejection patterns in both the controllable [low offers: mean high Miso-OC group = 68.3%, mean low Miso-OC group = 67.7%, t(183) = 0.14, p = 0.89; medium offers: mean high Miso-OC group = 66.3%, mean low Miso-OC group = 66.6%, t(516.07) = −0.11, p = 0.91; high offers: mean high Miso-OC group = 47.9%, mean low Miso-OC group = 45.3%, t(358.57) = 0.93, p = 0.36; Figure 4C] and the uncontrollable condition [low offers: mean high Miso-OC group = 85.2%, mean low Miso-OC group = 85.1%, t(517.28) = 0.08, p = 0.93; medium offers: mean high Miso-OC group = 60.8%, mean low Miso-OC group = 58.8%, t(516.62) = 0.66, p = 0.51; high offers: mean high Miso-OC group = 16.1%, mean low Miso-OC group = 14.1%, t(511.77) = 0.99, p = 0.32; Figure 4D]. These results suggest that both high and low Miso-OC groups were able to distinguish between the controllable and uncontrollable environments.
To test our central hypothesis, we examined whether participants in the high and low Miso-OC groups differed in self-reported perceived controllability between the controllable and uncontrollable tasks conditions. Using two-way ANOVA, we detected a significant interaction effect of group by condition on perceived controllability (F(1034) = 7.73, p = 0.006; Figures 4E and 4F). Parsing these effects, follow-up tests revealed that, compared with the low Miso-OC group, individuals in the high Miso-OC group reported a higher level of perceived controllability (t(499.07) = −4.37, p < 0.001) during the uncontrollable condition. There were no group differences in perceived controllability (t(516.28) = 0.03, p = 0.978) during the controllable condition.
Model-based task behavior
To quantify the strategies used in the social controllability task, we applied a 2-step forward thinking model to participants’ task behavior, as in prior work (Na et al., 2021). The forward thinking model outlines how participants mentally simulate future offers by calculating the downstream effects of their current decision. The number of steps (i.e., “2-step”) represents the number of future offers that participants simulate when considering each choice. From this model, we can extract participants’ sensitivity to norm violation, which reflects aversion to offer amounts that were very different than the expected offers, and expected influence, which reflects the amount by which participants simulated the offers changing based on their choices. We then investigated group by condition interaction effects on model-derived task parameters (see STAR Methods for further statistical and modeling details).
We detected a significant interaction effect of group by condition on the discrepancy between perceived controllability and expected influence (F(1033) = 4.67, p = 0.031, Figures 5B and 5C), such that, relative to individuals in the low Miso-OC group, those in the high Miso-OC group displayed a higher discrepancy during the uncontrollable condition (t(515.82) = −2.17, p = 0.030), indicating a higher level of perceived relative to actual control. Unlike individuals in the low Miso-OC group, those in the high Miso-OC group also displayed a higher discrepancy during the uncontrollable relative to the controllable condition (t(486.99) = 2.521, p = 0.012). There were no group differences in discrepancy (t(515.73) = 0.75, p = 0.453) during the controllable condition.
Figure 5.

Model-based task results
(A) The forward-thinking model we employed assumed that individuals simulated their future actions and consequential future offers based on the “expected influence (δ)” and value functions. The thick and solid lines show an example of a simulated path.
(B) Bar plot shows a significant interaction effect of Miso-OC group by condition on the discrepancy between perceived and actual control.
(C) Estimation plot of the same data emphasizing the effect size of interest: the difference between the Miso-OC group means. Here, relative to individuals in the low Miso-OC group, those in the high group show higher levels of reported perceived controllability relative to actual control in the uncontrollable condition.
(D) Bar plot shows a significant interaction effect of Miso-OC group by condition on sensitivity to norm violation.
(E) Estimation plot of the same data emphasizing the effect size of interest: differences in the mean value for each condition. Here, unlike those in the low Miso-OC group, those in the high group show heightened sensitivity to norm violation in the uncontrollable relative to the controllable condition.
Error bars represent SE. In the mean difference estimation plots, dots represent each included individual. Larger circles with lines represent the 95% confidence intervals. Distributions of expected sampling error for the difference between the means are shown in gray.
See also Tables S1–S4. Significance levels for post-hoc Welch t tests: ∗∗∗p < 0.001, ∗∗p < 0.01, ∗p < 0.05.
Results also show a significant Miso-OC group by condition effect on sensitivity to norm violations (F(1033) = 4.10, p = 0.043, Figures 5E and 5F), such that, unlike individuals in the low Miso-OC group (t(514.94) = 0.51, p = 0.614), those in the high Miso-OC group displayed increased sensitivity to norm violations in the uncontrollable versus controllable conditions (t(482.21) = −3.251, p = 0.001). There was no significant group by condition effect on expected influence (F(1033) = 1.24, p = 0.265). We did not detect any significant interactions for the “mood” (F(1033)’s < 1.50, p’s > 0.1) or “social” (F(1036)’s < 1.50, p’s > 0.1) transdiagnostic factors.
Discussion
Our findings suggest that misophonia falls within a psychiatric dimension characterized by maladaptive perceptions of control. Questions from the misophonia and OC questionnaires loaded highly onto a common factor. These disorders share a common pathology of illusory perceptions of controllability (Natalini et al., 2020; Reuven-Magril et al., 2008; Schröder et al., 2013). Consistent with this observation, in the social controllability task, relative to individuals with scores in the lowest quartile for the Miso-OC factor, those in the highest quartile reported heightened levels of perceived controllability as well as a higher perceived relative to actual control (reflecting a belief-behavior disconnect) during the uncontrollable condition. In addition, unlike individuals in the low Miso-OC group, those in the high Miso-OC group showed heightened sensitivity to norm violation in the uncontrollable compared with the controllable condition. These results suggest that individuals with stronger reported misophonia and OC symptoms have a heightened sense of control even when none is actually afforded to them, as well as aversive reactions when offers do not match expectations.
The most commonly reported triggers in misophonia, including eating, breathing, and repetitive tapping sounds, are socially generated (Rouw and Erfanian, 2018; Schröder et al., 2013). The social context of these sounds appears to be crucial to the misophonic response, as similar sounds produced by nonsocial sources, including the individuals with misophonia themselves, do not elicit strong reactions (Bruxner, 2016; Natalini et al., 2020). As a result, individuals with misophonia often actively avoid social situations that are likely to provoke symptoms (Bruxner, 2016; Schröder et al., 2013). Knowing this, we may have expected to see items from the misophonia questionnaire load more highly onto the “social” factor alongside questions probing symptoms of ASD and social anxiety. Instead, the items from misophonia questionnaire loaded most heavily onto a separate factor, along with items from the OC questionnaire. Such results are consistent with prior reports of high rates of comorbidities between misophonia and OCD. However, although the factor analysis results suggest that symptoms of misophonia are separable from symptoms of social impairment, the results from the social controllability task suggest that both social and control components are at play. Indeed, it appears that misophonia may be linked to the interaction between disruptions in perceived controllability and unpredictable social agents in the environment.
Consistent with our results, some work suggests that OCD is associated with heightened illusory perceptions of controllability in uncontrollable situations (Reuven-Magril et al., 2008). Although other studies report decreased perception of controllability among individuals diagnosed with OCD (Brown and Naragon-Gainey, 2013; Gallagher et al., 2014b; Moulding et al., 2009; Moulding and Kyrios, 2007), this discrepancy is likely reflective of differences in the definition and measurement of perceived controllability, as these results are based on questionnaires assessing control in the context of anxiety and obsessive-compulsive symptoms. Thus, although individuals with OCD perceive a lack of control over their specific symptoms, they appear to perceive a heightened sense of control over their environments in general; this may be due to a compensatory desire for control, wherein individuals with OCD have an intense need to regain the control that they feel they lack over their symptoms, leading to illusory overestimations of their levels of control over the environment (Moulding et al., 2009; Moulding and Kyrios, 2007; Reuven-Magril et al., 2008). Such a phenomenon could explain the intense reactions that characterize misophonia. If an individual desires control and therefore perceives a high level of influence over their environments, the occurrence of a disturbing sound that they cannot control could disrupt their wishful prediction and cause a negative reaction that seems out of proportion. As the individual experiences symptoms that they are unable to control, they may react with withdrawal, agitation, or anxiety.
Several standalone items from the anxiety, depression, ASD, eating disorder, and alcohol use questionnaires loaded onto the same factor as the items from the misophonia and OC questionnaires. Investigation of these items revealed that they reflect symptoms of disrupted impulse control and subsequent negative emotions, including intrusive thoughts, hyperactivity (restlessness and talkativeness), and guilt, after overindulgence. The co-loading of items from a diverse set of questionnaires thus appears to have captured a transdiagnostic construct of control-related symptoms, including those seen in misophonia and OCD.
Limitations of the study
Study limitations include a current lack of a consensus gold-standard measure of misophonia. We believe the A-MISO-S to be a robust measure of misophonia, as it has been widely used in research and shows preliminary validity (Naylor et al., 2020; Schröder et al., 2013). However, future work should reinvestigate the results of this study once a psychometrically validated scale for misophonia is established. In addition, although allowing for large-scale data collection, the online nature of the study meant reliance on self-report data for measures of psychiatric symptoms. Such data must be interpreted with caution, as the accuracy of self-reports varies as a function of participants’ self-awareness and introspection. Furthermore, the situational context presented in the task differs from the real-life contexts that would typically trigger individuals with misophonia. Although we purposely sought to explore the isolated effects of manipulating social controllability in the absence of misophonia triggers in order to investigate alterations in a baseline state, future work should directly explore the relevance of these perceived controllability differences to trigger response. Finally, as participants were not selected on the basis of any particular diagnoses, the symptoms reported in this study should be interpreted as trait-level features rather than aspects of clinically confirmed psychiatric disorders.
In sum, this study used digital phenotyping to investigate the relationship between misophonia and other psychiatric diagnoses and characterize the role of social control in the pathophysiology of the disorder. Future work should further explore the role of control in misophonia, including investigation into the neural underpinnings of disrupted control, and whether treatments known to be effective for treating other disorders of control may similarly provide promise for misophonia.
STAR★Methods
Key resources table
| REAGENT or RESOURCE | SOURCE | IDENTIFIER |
|---|---|---|
| Deposited data | ||
| Subject’s characteristics and psychiatric questionnaire responses | This manuscript | https://osf.io/ad7np/ |
| Social controllability task data | This manuscript | https://github.com/smbneuro5/social_controllability_miso_oc/ |
| Software and algorithms | ||
| Matlab | Mathworks | www.mathworks.com/products/matlab.html |
| R | R Foundation for Statistical Computing | https://www.r-project.org/ |
Resource availability
Lead contact
Requests for additional information should be directed to the lead contacts, Daniela Schiller (daniela.schiller@mssm.edu) and Xiaosi Gu (xiaosi.gu@mssm.edu).
Material availability
This study did not generate new unique reagents.
Experimental model and subject details
Participants were enrolled in the study as part of a larger online project examining social cognition and mental health. Participants were recruited from Prolific (www.prolific.co), an online research participant recruitment site, with the eligibility criteria of (1) age between 18 and 64, (2) currently living in the United States, (3) >90% approval rating in Prolific. Potential participants opted to take part in the study based on a brief description informing them that they would be completing surveys assessing mood, personality, and sensitivity to certain sounds, as well as compensation amount ($8 in total for an estimated rate of $10.66 per hour). In total, 1,269 individuals attempted the study, 38 were excluded for non-completion, 9 were excluded for exceeding the time limit, and 47 were excluded due to missed attention checks or ID errors. This resulted in a total of 1,175 participants to be included in the factor analysis. Of these participants, 1,041 individuals completed the social controllability task. The study was approved by the Institutional Review Board at the Icahn School of Medicine at Mount Sinai and all participants provided informed consent online prior to participation. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Method details
Misophonic and other psychiatric measures
To assess levels of misophonic traits in the sample, participants completed the Amsterdam Misophonia Scale (A-MISO-S), a 7-item self-report measure assessing the severity of misophonia symptoms including preoccupation with trigger sounds, negative emotional responses to trigger sounds, lack of thought control, and interference with daily life (Schröder et al., 2013). The first 6 questions are scored on a 5-point Likert scale (0–4), whereas the last question allows for free-response. The A-MISO-S was adapted from the Yale-Brown Obsessive-Compulsive Scale (Goodman et al., 1989). Total scores range from 0 to 24, with score categories of 0–4 (subclinical), 5–9 (mild), 10–14 (moderate), 15–19 (severe), and 20–24 (extreme; Schröder et al., 2013). There is currently no validated assessment for the diagnosis of misophonia; However, the A-MISO-S has been widely used in research (Eijsker et al., 2021; Jager et al., 2020; Naylor et al., 2020; Quek et al., 2018; Rouw and Erfanian, 2018).
In order to compare misophonia to other psychiatric conditions, participants also completed the Broad Autism Spectrum Questionnaire (BAPQ; Hurley et al., 2007), Obsessive-Compulsive Inventory - Revised (OCI-R; Foa et al., 2002), The State-Trait Anxiety Inventory (STAI Trait questions; Spielberger, 1983), Liebowitz Social Anxiety Scale (LSAS Avoidance questions; Liebowitz, 1987), Zung Self Rating Depression Scale (SDS; Zung, 1986), Eating Attitudes Test (EAT; Garner and Garfinkel, 1979), Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993), Avoidant Personality Disorder Impairment Scale (AvPD-IS; Liggett et al., 2017), Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD; Zanarini et al., 2003), Apathy Evaluation Scale (AES; Marin et al., 1991), Subjective Happiness Scale (SHH; Lyubomirsky and Lepper, 1999), UCLA Loneliness Scale (UCLA-LS; Russell, 1996). To measure conigitve ability, participants also completed the International Cognitive Ability Resource – Sample Test (ICAR; Condon and Revelle, 2014).
Factor analysis
The factor analysis was performed in R (RStudio Version 1.3.959). First, we generated a correlation matrix consisting of the 212 questionnaire items. Because the responses to the ZAN-BPD questionnaire were dichotomous, we used the ‘hetcor’ function in R to generate a heterogeneous correlation matrix. To determine the appropriate number of factors for the correlation matrix, we then used the Cattell-Nelson-Gorsuch (CNG) test, which computes the slopes of all possible sets of three adjacent eigenvalues and determines the point at which there is the greatest differences in slope (Gorsuch and Nelson, 1981). Finally, we performed the factor analysis with the ‘fa’ package in R using Maximum Likelihood Estimation (MLE) and oblique rotation (oblimin). Factor scores for each participant were calculated using the ‘factor.scores’ function in R with the ‘tenBerge’ method due to the oblique rotation.
Social controllability task
In the social controllability game, participants are paired one by one with virtual partners from two 30-person teams, representing 2 conditions consisting of 30 trials each. To create a social context without explicit deception, participants were instructed that they were playing with “partners,” with no specification about whether they were real people or computers. Teams are denoted by a name (“Aldertown” and “Banyan Bay”) as well as a common color for the background and team members’ t-shirts. In each trial, the virtual partner proposes a split of $20, and the participant must decide whether to accept or reject the offer. If the participant chooses to accept, both parties receive the proposed portion of the money. If they choose to reject the proposal, neither party receives any money. Each team that the participant plays against represents a different condition: controllable and uncontrollable, though participants are not explicitly told about this manipulation.
In the controllable condition, but not in the uncontrollable condition, participants can either increase the value of the next offer by rejecting the current offer or decrease the value of the next offer by accepting the current offer. The amount of the offer change is determined in a probabilistic manner: ⅓ chance of changing the offer by $2, ⅓ chance of changing the offer by $1, and ⅓ chance of no change (Figure 3B). In contrast, in the uncontrollable condition, offer amounts are sampled from a predetermined distribution (mean = $5.0, SD = $2.3) and the order is randomized for each participant. In both conditions, the initial offer is $5 and the offers are constrained to be an integer between $1 and $9 (inclusive). The order of the conditions and the offers in the uncontrollable condition were randomized across participants. At the end of the task, participants were asked to rate how much control they perceived they had over the proposers on each team on a scale of 0–100%.
Quantification and statistical analysis
Computational modeling
All computational modeling was performed in MATLAB (MATLAB R2020a). In order to understand the computational mechanisms subserving social controllability, we applied a 2-step forward thinking model to task behavior, as our prior work has shown that this model best explains behavior on this task (Na et al., 2021). The forward thinking model outlines how individuals mentally simulate future outcomes by computing the downstream effects of their current action in order to guide these decisions. The number of steps (i.e., “2-step”) represents the number of future trials participants take into consideration when making their choices. In this model, the action taken at the ith trial, which can be either acceptance or rejection of the offer, is denoted by . The immediate reward (or actual offer size) is denoted by , and the internal norm (or expected offer size) is denoted by .
We assumed that the internal norm (expected offer) was updated each trial based on observations of partners’ offers (), using Rescorla-Wagner learning (Sutton and Barto, 2018) with learning rate () that could vary between participants depending on how quickly they learned what offers to expect. The initial norm (expected offer at the start of the task) was set as a free parameter that was assumed to vary between participants (; Gu et al., 2015):
To model how people decide whether to accept or reject on a given trial, we can calculate the utility of each choice, which represents the expected immediate reward for that choice. Given a certain expected offer (e.g., $8), the utility of the immediate reward is computed as the actual offer amount subtracted by the prediction error (i.e., the difference between the actual and expected reward, times ), where () represents how sensitive someone is to unexpected offers (sensitivity to norm violation; Sutton and Barto, 2018):
For models considering future trials, or “steps”, the value of the current action on a given trial was calculated by taking the sum of 1) the utility of the expected immediate reward (see above), and 2) the utility of the mentally simulated outcomes in future trials. The utility of simulated future outcomes was defined as sum of the discounted utilities of the future rewards based on hypothetical future actions (). The utilities of these future rewards are "discounted” because people tend to place less value on rewards that they have to wait for. The future discounting factor (), which described how much weight one puts on future rewards, was fixed at 0.8 following a previous study (Na et al., 2021). The hypothetical trial-by-trial change in offer size (+/− $0, $1, or $2) was contingent on one’s hypothetical choices (accept or reject) and represented by the expected influence variable (; ). was applied in a symmetric manner, such that the offer changed by if the prior choice was rejected and if the prior choice was accepted. The hypothetical offers were constrained to have a positive value, assuming that participants were aware that the offers would always be greater than $0. In summary, the action value was computed as follows:
The difference in utility between accepting and rejecting was entered into a softmax function to compute the trial-by-trial probability of choice. In other words, was the participant more likely to accept or reject? The first 3 trials were excluded to account for an initial learning period, and the last 3 trials were excluded based on the assumption that strategic behavior would differ toward the end of the task (e.g., less incentive to reject). The model was thus fit at the individual-level for the middle 24 trials in order to focus on the exploitation of controllability. Parameter estimates from the 2-step model were extracted for analysis for each participant. Specifically, we extracted the sensitivity to norm violation (reflecting aversion to offer amounts that were very different than the expected offers) and expected influence (how much they believed they could change the offer based on their choices).
Statistical analysis
All statistical analyses were performed in R (RStudio Version 1.3.959). In order to test for differences in task behavior between individuals with and without high rates of reported misophonia symptoms, we divided participants into two groups based on the highest and lowest quartile of scores for the factor on which misophonia loaded mostly highly (see Table 2 for group characteristics). To examine the relationship between symptoms and social controllability, we then assessed task outcomes in these groups. First, we examined offer sizes and rejection rates in each group to explore the general task performance. Welch t-tests explored behavioral differences between groups. We then used ANOVA to test for effects of group-by-condition interactions on several parameters. Given our hypothesis that misophonia may be associated with a disrupted illusion of control, our primary parameter of interest was perceived control, which is self-reported at the end of each condition in the task.
To explore whether any differences in perceived controllability corresponded to differences in actual exertion of control, we also tested group-by-condition interactions on the model-derived expected influence , as well as the discrepancy between perceived and expected influence (self-reported perceived controllability minus model-derived ). This discrepancy is a measurement of belief-behavior disconnect; higher values reflect higher perception of control relative to mentally simulated control. Finally, to test whether any differences in perceived or actual control were associated with aversion to unexpected outcomes, we tested group-by-condition interactions on sensitivity to norm violation , representing unwillingness to accept an offer below the expected value.
Each model controlled for sex, age, and ICAR scores. Significant interaction effects were followed up by Welch t-tests to parse the direction of the effect. To test for specificity, we conducted exploratory analyses to see if any significant group-by-condition interaction effects were present for the mood and social factors.
To further explore the unique contributions of misophonia and OC symptoms to task performance, we performed three additional variations of same group-by-condition interaction analyses with newly defined groups: 1) those in the lowest vs. the highest quartiles based on misophonia symptoms alone, 2) those in the lowest quartile based on misophonia symptoms alone vs. those in highest quartile for both misophonia and OC-symptoms, and 3) those in the lowest quartile based on misophonia symptoms alone vs. those in highest quartile for misophonia but lowest quartile for OC-symptoms (i.e., misophonia without comorbid OC symptoms). Additionally, to utilize the power afforded by the full sample, we performed the group-by-condition interaction analyses comparing those in the top and bottom 50% percentile on the Miso-OC factor. Results for these additional analyses are presented in supplemental information.
All statistical details can be found in the Results section. For Welch t-tests and ANOVAs in all figures, three asterisks (∗∗∗) represent p values of less than 0.001; two asterisks (∗∗) represent p values of less than 0.01; one asterisk (∗) represents p values of less than 0.05.
Acknowledgments
This work was supported by funding from the Ream Foundation—Misophonia Research Fund and internal institutional funding from the Icahn School of Medicine at Mount Sinai. S.M.B. is supported by the National Institute of Mental Health (Grant No. R01MH122611) and the Beatrice and Samuel A. Seaver Foundation (Fellowship). H.W.K. is supported by the National Institute of Mental Health (Grant Nos R01MH109730, R01MH123069, and R61MH125130) and the Veterans Affairs Medical Center. J.F.-F. is supported by the National Institute of Mental Health (Grant Nos R01MH122611 and R01MH119172), the National Institute of Neurological Disorders and Stroke (Grant No. R01NS105845), the Simons Foundation Autism Research Initiative, and the Seaver Foundation Rare Disease Program. X.G. is supported by the National Institute of Mental Health (Grant Nos R01MH122611, R01MH123069, and R21MH120789), and the Simons Foundation Autism Research Initiative. D.S. is supported by the National Institute of Mental Health (Grant Nos R01MH122611, R01MH123069, and R21MH120789), the Simons Foundation Autism Research Initiative, and the Ream Foundation.
Author contributions
Conceptualization, D.S., X.G., J.F.-F., and H.W.K.; Methodology, S.M.B., D.S., X.G., and J.F.-F.; Investigation, S.M.B., S.N., and J.B.; Writing—Original Draft, S.M.B.; Writing—Review & Editing, S.M.B., S.N., J.B., D.S., X.G., J.F.-F.; Funding Acquisition, D.S. and X.G.; Resources, S.N; Supervision, D.S., X.G., J.F.-F, and H.W.K.
Declaration of interest
The authors declare no competing interests in relation to this work.
Inclusion and diversity
We worked to ensure gender balance in the recruitment of human subjects. We worked to ensure ethnic or other types of diversity in the recruitment of human subjects. We worked to ensure that the study questionnaires were prepared in an inclusive way. One or more of the authors of this paper self-identifies as an underrepresented ethnic minority in science. One or more of the authors of this paper received support from a program designed to increase minority representation in science.
Published: July 15, 2022
Footnotes
Supplemental information can be found online at https://doi.org/10.1016/j.isci.2022.104617.
Contributor Information
Xiaosi Gu, Email: xiaosi.gu@mssm.edu.
Daniela Schiller, Email: daniela.schiller@mssm.edu.
Supplemental information
Data and code availability
-
•
De-identified data have been deposited on GitHub and OSF and are publicly available as of the date of publication. They can be freely accessed and downloaded via https://osf.io/ad7np/ and https://github.com/smbneuro5/social_controllability_miso_oc.
-
•
All code associated with this paper can be freely accessed and downloaded via https://github.com/smbneuro5/social_controllability_miso_oc.
-
•
Any additional information required to reanalyze the data reported in this paper is available from the lead contact upon request.
The institutional review board at the Icahn School of Medicine at Mount Sinai approved the study. All research was performed in accordance with the relevant guidelines and regulations.
References
- Berman E.S. The relationship between eating self-efficacy and eating disorder symptoms in a non-clinical sample. Eat. Behav. 2006;7:79–90. doi: 10.1016/j.eatbeh.2005.07.004. [DOI] [PubMed] [Google Scholar]
- Brout J.J., Edelstein M., Erfanian M., Mannino M., Miller L.J., Rouw R., Kumar S., Rosenthal M.Z. Investigating misophonia: a review of the empirical literature, clinical implications, and a research agenda. Front. Neurosci. 2018;12:36. doi: 10.3389/fnins.2018.00036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown T.A., Naragon-Gainey K. Evaluation of the unique and specific contributions of dimensions of the triple vulnerability model to the prediction of DSM-IV anxiety and mood disorder constructs. Behav. Ther. 2013;44:277–292. doi: 10.1016/j.beth.2012.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruxner G. ‘Mastication rage’: a review of misophonia – an under-recognised symptom of psychiatric relevance? Australas Psychiatry. 2016;24:195–197. doi: 10.1177/1039856215613010. [DOI] [PubMed] [Google Scholar]
- Condon D.M., Revelle W. The international cognitive ability resource: development and initial validation of a public-domain measure. Intelligence. 2014;43:52–64. doi: 10.1016/j.intell.2014.01.004. [DOI] [Google Scholar]
- de Bézenac C.E., Sluming V., O’Sullivan N., Corcoran R. Ambiguity between self and other: individual differences in action attribution. Conscious. Cognit. 2015;35:1–15. doi: 10.1016/j.concog.2015.04.010. [DOI] [PubMed] [Google Scholar]
- Edelstein M., Brang D., Rouw R., Ramachandran V.S. Misophonia: physiological investigations and case descriptions. Front. Hum. Neurosci. 2013;7:296. doi: 10.3389/fnhum.2013.00296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eijsker N., Schröder A., Smit D.J.A., van Wingen G., Denys D. Structural and functional brain abnormalities in misophonia. Eur. Neuropsychopharmacol. 2021;52:62–71. doi: 10.1016/j.euroneuro.2021.05.013. [DOI] [PubMed] [Google Scholar]
- Erfanian M., Kartsonaki C., Keshavarz A. Misophonia and comorbid psychiatric symptoms: a preliminary study of clinical findings. Nord J Psychiatry. 2019;73:219–228. doi: 10.1080/08039488.2019.1609086. [DOI] [PubMed] [Google Scholar]
- Foa E.B., Huppert J.D., Leiberg S., Langner R., Kichic R., Hajcak G., Salkovskis P.M. The Obsessive-Compulsive Inventory: development and validation of a short version. Psychol. Assess. 2002;14:485–496. doi: 10.1037/1040-3590.14.4.485. [DOI] [PubMed] [Google Scholar]
- Gallagher M.W., Bentley K.H., Barlow D.H. Perceived control and vulnerability to anxiety disorders: a meta-analytic review. Cogn. Ther. Res. 2014;38:571–584. doi: 10.1007/s10608-014-9624-x. [DOI] [Google Scholar]
- Gallagher M.W., Naragon-Gainey K., Brown T.A. Perceived control is a transdiagnostic predictor of cognitive-behavior therapy outcome for anxiety disorders. Cognit. Ther. Res. 2014;38:10–22. doi: 10.1007/s10608-013-9587-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garner D.M., Garfinkel P.E. The Eating Attitudes Test: an index of the symptoms of anorexia nervosa. Psychol. Med. 1979;9:273–279. doi: 10.1017/S0033291700030762. [DOI] [PubMed] [Google Scholar]
- Gillan C.M., Kosinski M., Whelan R., Phelps E.A., Daw N.D. Characterizing a psychiatric symptom dimension related to deficits in goal-directed control. eLife. 2016;5:e11305. doi: 10.7554/eLife.11305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman W.K., Price L.H., Rasmussen S.A., Mazure C., Fleischmann R.L., Hill C.L., Heninger G.R., Charney D.S. The Yale-Brown obsessive compulsive scale: I. Development, use, and reliability. Arch. Gen. Psychiatr. 1989;46:1006. doi: 10.1001/archpsyc.1989.01810110048007. [DOI] [PubMed] [Google Scholar]
- Gorsuch R., Nelson J. 1981. Cng Scree Test: An Objective Procedure for Determining the Number of Factors. [Google Scholar]
- Gu X., Wang X., Hula A., Wang S., Xu S., Lohrenz T.M., Knight R.T., Gao Z., Dayan P., Montague P.R. Necessary, yet dissociable contributions of the insular and ventromedial prefrontal cortices to norm adaptation: computational and lesion evidence in humans. J. Neurosci. 2015;35:467–473. doi: 10.1523/jneurosci.2906-14.2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Güth W., Schmittberger R., Schwarze B. An experimental analysis of ultimatum bargaining. J. Econ. Behav. Organ. 1982;3:367–388. doi: 10.1016/0167-2681(82)90011-7. [DOI] [Google Scholar]
- Hurley R.S.E., Losh M., Parlier M., Reznick J.S., Piven J. The Broad autism phenotype questionnaire. J. Autism Dev. Disord. 2007;37:1679–1690. doi: 10.1007/s10803-006-0299-3. [DOI] [PubMed] [Google Scholar]
- Jager I., de Koning P., Bost T., Denys D., Vulink N. Misophonia: phenomenology, comorbidity and demographics in a large sample. PLoS One. 2020;15:e0231390. doi: 10.1371/journal.pone.0231390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jager I.J., Vulink N.C.C., Bergfeld I.O., van Loon A.J.J.M., Denys D.A.J.P. Cognitive behavioral therapy for misophonia: a randomized clinical trial. Depress. Anxiety. 2020;38:da.23127. doi: 10.1002/da.23127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kashihara S., Kanayama N., Miyatani M., Nakao T. Attentive observation is essential for the misattribution of agency to self-performance. Front. Psychol. 2017;8:890. doi: 10.3389/fpsyg.2017.00890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kluckow H., Telfer J., Abraham S. Should we screen for misophonia in patients with eating disorders? A report of three cases. Int. J. Eat. Disord. 2014;47:558–561. doi: 10.1002/eat.22245. [DOI] [PubMed] [Google Scholar]
- Liebowitz M.R. Social phobia. Mod. Probl. Pharmacopsychiatr. 1987;22:141–173. doi: 10.1159/000414022. [DOI] [PubMed] [Google Scholar]
- Liggett J., Carmichael K.L.C., Smith A., Sellbom M. Validation of self-report impairment measures for section III obsessive–compulsive and avoidant personality disorders. J. Pers. Assess. 2017;99:1–14. doi: 10.1080/00223891.2016.1185613. [DOI] [PubMed] [Google Scholar]
- Lyubomirsky S., Lepper H.S. A measure of subjective happiness: preliminary reliability and construct validation. Soc. Indicat. Res. 1999;46:137–155. doi: 10.1023/A:1006824100041. [DOI] [Google Scholar]
- Marin R.S., Biedrzycki R.C., Firinciogullari S. Reliability and validity of the apathy evaluation scale. Psychiatr. Res. 1991;38:143–162. doi: 10.1016/0165-1781(91)90040-V. [DOI] [PubMed] [Google Scholar]
- Moulding R., Kyrios M. Desire for control, sense of control and obsessive-compulsive symptoms. Cogn. Ther. Res. 2007;31:759–772. doi: 10.1007/s10608-006-9086-x. [DOI] [Google Scholar]
- Moulding R., Kyrios M., Doron G., Nedeljkovic M. Mediated and direct effects of general control beliefs on obsessive compulsive symptoms. Can. J. Behav. Sci. 2009;41:84–92. doi: 10.1037/a0014840. [DOI] [Google Scholar]
- Na S., Chung D., Hula A., Perl O., Jung J., Heflin M., Blackmore S., Fiore V.G., Dayan P., Gu X. Humans use forward thinking to exploit social controllability. Elife. 2021;10:e64983. doi: 10.7554/eLife.64983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Natalini E., Dimaggio G., Varakliotis T., Fioretti A., Eibenstein A. Misophonia, maladaptive schemas and personality disorders: a report of three cases. J. Contemp. Psychother. 2020;50:29–35. doi: 10.1007/s10879-019-09438-3. [DOI] [Google Scholar]
- Naylor J., Caimino C., Scutt P., Hoare D.J., Baguley D.M. The prevalence and severity of Misophonia in a UK undergraduate medical student population and validation of the amsterdam misophonia scale. Psychiatr Q. 2020 doi: 10.1007/s11126-020-09825-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quek T.C., Ho C.S., Choo C.C., Nguyen L.H., Tran B.X., Ho R.C. Misophonia in Singaporean psychiatric patients: a cross-sectional study. Int J. Environ. Res. Public Health. 2018;15:E1410. doi: 10.3390/ijerph15071410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reuven-Magril O., Dar R., Liberman N. Illusion of control and behavioral control attempts in obsessive-compulsive disorder. J. Abnorm. Psychol. 2008;117:334–341. doi: 10.1037/0021-843X.117.2.334. [DOI] [PubMed] [Google Scholar]
- Rouw R., Erfanian M. A large-scale study of misophonia. J. Clin. Psychol. 2018;74:453–479. doi: 10.1002/jclp.22500. [DOI] [PubMed] [Google Scholar]
- Russell D.W. UCLA loneliness scale (version 3): reliability, validity, and factor structure. J. Pers. Assess. 1996;66:20–40. doi: 10.1207/s15327752jpa6601_2. [DOI] [PubMed] [Google Scholar]
- Saunders J.B., Aasland O.G., Babor T.F., De La Fuente J.R., Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction. 1993;88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- Schröder A., Vulink N., Denys D. Misophonia: diagnostic criteria for a new psychiatric disorder. PLoS One. 2013;8:e54706. doi: 10.1371/journal.pone.0054706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spielberger C.D. State-trait anxiety inventory for adults. 1983. [DOI]
- Sutton R.S., Barto A.G. MIT Press; 2018. Reinforcement Learning: An Introduction. [Google Scholar]
- Swedo S.E., Baguley D.M., Denys D., Dixon L.J., Erfanian M., Fioretti A., Jastreboff P.J., Kumar S., Rosenthal M.Z., Rouw R., et al. Consensus definition of misophonia: a delphi study. Front. Neurosci. 2022;16:841816. doi: 10.3389/fnins.2022.841816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomasello M., Rakoczy H. What makes human cognition unique? From individual to shared to collective intentionality. Mind Lang. 2003;18:121–147. doi: 10.1111/1468-0017.00217. [DOI] [Google Scholar]
- Wadsworth L.P., Hayes-Skelton S.A. Exploring perceived control, a low-control task, and a brief acceptance intervention in a low and high transdiagnostic anxiety sample. Neurol. Psychiatr. Brain Res. 2020;35:1–9. doi: 10.1016/j.npbr.2019.11.001. [DOI] [Google Scholar]
- Wu M.S., Lewin A.B., Murphy T.K., Storch E.A. Misophonia: incidence, phenomenology, and clinical correlates in an undergraduate student sample. J. Clin. Psychol. 2014;70:994–1007. doi: 10.1002/jclp.22098. [DOI] [PubMed] [Google Scholar]
- Zanarini M.C., Vujanovic A.A., Parachini E.A., Boulanger J.L., Frankenburg F.R., Hennen J. Zanarini rating scale for borderline personality disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J. Pers. Disord. 2003;17:233–242. doi: 10.1521/pedi.17.3.233.22147. [DOI] [PubMed] [Google Scholar]
- Zung W.W.K. In: Assessment of Depression. Sartorius N., Ban T.A., editors. Springer; 1986. Zung self-rating depression scale and depression status inventory; pp. 221–231. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
-
•
De-identified data have been deposited on GitHub and OSF and are publicly available as of the date of publication. They can be freely accessed and downloaded via https://osf.io/ad7np/ and https://github.com/smbneuro5/social_controllability_miso_oc.
-
•
All code associated with this paper can be freely accessed and downloaded via https://github.com/smbneuro5/social_controllability_miso_oc.
-
•
Any additional information required to reanalyze the data reported in this paper is available from the lead contact upon request.
The institutional review board at the Icahn School of Medicine at Mount Sinai approved the study. All research was performed in accordance with the relevant guidelines and regulations.