

ABSTRACT
Introduction:
Family planning is one of the essential health care services to promote and ensure reproductive health. Nearly 40.2 percent of men think it as a woman’s responsibility as per the National Family Health Survey 4. Not much attention has been given to the male partners in the usage of contraceptives. So, this study was conducted to assess the male participation in family planning among married males in a rural area of Chhattisgarh.
Methodology:
A sample of 365 married males were interviewed through a semi-structured questionnaire at a primary health care center.
Results:
Only 48 (13.1%) participants were using condoms or male sterilization as a method of contraception at the time of the study. Good involvement of males in family planning was found to be (10.9%) in our study. Those who were above the poverty line and educated (graduation and above) had good involvement in family planning. The chief reason cited for not opting for male sterilization by participants was fear of physical weakness followed by family opposition.
Conclusion:
The socio-cultural barrier in itself demotivates men from getting involved in the family planning program. This study recommends increasing health literacy regarding family planning among men by including it in the school curriculum and through awareness activities and counseling that influences them positively and motivates them to accept contraceptive services and shared decision making. Sterilization facilities should be made accessible to them to further encourage them.
Keywords: Contraception, family planning, male involvement
Introduction
Ensuring universal access to family planning has been identified as a key priority for realizing the Sustainable Development Goals (SDGs) and as one of the most cost-effective SDG targets. Although contraceptive methods and services are mostly focused on women, men are often the primary decision-makers on family planning. India has continued its efforts to expand the range and reach of contraceptive options by rolling out newer contraceptives and delivering a full range of family planning services at all levels of health care.
Family planning is one of the essential health care services that can promote and ensure reproductive health. Studies reported that male intention to discuss family planning is affected by their attitudes, norms, and self-efficacy.[1,2] Family planning is also affected by males’ perception that family planning is the duty of women.
As per the National Family Health Survey (NFHS-4) data, the two methods of contraception available to men – vasectomy and condoms – cumulatively account for only 12 percent of the overall modern contraceptive prevalence rate. This suggests that women are the driving force behind the family planning drive and surprisingly, 40.2 percent of the men think it is a woman’s responsibility to avoid getting pregnant.[3] Most family planning programs focus on women as primary contraceptive users, whereas men are viewed as supportive partners despite evidence indicating the interest of male users in existing programs.[4,5] Family planning was always thought to be a woman’s prerogative, especially in a male-dominant society like India, and most of the studies on family planning in developing countries have long focused on women as the subject of interest. It is now increasingly recognized that the actions required to achieve improvements in family planning statistics should also encourage the active participation of men, hence exploring the role of husband’s contraceptive practices is particularly important. Male involvement also encompasses encouragement and support of their partner and peers to use family planning, and influence the policy environment to be more conducive for developing male-centered programs.[6,7,8]
The male involvement includes not only male contraception but also all the other national program activities which work towards increasing the awareness, acceptability, and prevalence of family planning methods among males. The primary aim of family planning is to enable women and men to plan their families and space their children through the use of modern contraceptives.[9,10,11]
Numerous factors influence contraceptive use such as interpersonal relationships, family, community members, religious leaders, health care providers, and intimate partners.[12] The most significant interpersonal relationship affecting family planning use is the intimate male partner relationship and the role of gender dynamics.[13] Male dominance is reinforced through political and economic mechanisms that limit women’s access to financial independence and therefore their ability to access and use family planning methods and services. Patriarchal views on gendered roles are socially constructed and reinforced within various cultural settings and result in women lacking autonomy to make their own decisions about using family planning methods. These patriarchal cultural views more often give men the power to decide how many children a couple should have.
Most family planning studies are conducted from the female perspective and focus on women who are clinic attendees to understand the family planning experience. Therefore, the female view is predominantly captured in family planning studies, which results in the male voice being silenced. There is also an overbearing assumption that men are always barriers, uninterested, or by-standers in family planning use, and that their influence results in discontinuation of family planning use.[14]
Few studies have been conducted on male involvement in family planning from India. However, not much attention has been given to the male partners while assessing the usage of contraceptives, specifically in empowered action group states like Chhattisgarh. Hence, this study was undertaken to assess male involvement in family planning among married males in a rural area. We hope the findings of the study will reinforce the frontline health workers and primary care providers, who are the driving force in reducing the unmet needs in contraception, to renew focus on males as a major stakeholder in the usage of contraception, and stabilizing the population growth.
Materials and Methods
This cross-sectional study was done at Community Health Centre (CHC) in Abhanpur, Chhattisgarh. This area caters to about 2,42,069 population including 105 villages. The study included those married males who came to the health center for their own health issues or to accompany patients. Married males aged 18–60 years who were permanent residents of that area for at least the past 6 months were included. The sample size was found out to be 347 as the prevalence of practices of family planning method was taken from Rekha et al.[8] study as 71.2% and with a nonresponse rate of 10%. The interview was conducted at the Primary health center, Khorpa, through a convenient sampling till an adequate sample size was achieved. A total of 365 eligible men were interviewed.
Data collection
A semi-structured questionnaire was prepared and pretested on 10% of the sample size among the eligible persons of a different rural area of Chhattisgarh. Informed consent was taken before the interview from each study participant. The confidentiality was maintained. Those participants who wished to withdraw from the study during the interview were excluded and replaced by other participants till the completion of the sample size. The data were entered directly on the google form application while interviewing.
Data analysis
The data were entered into MS Excel and then transferred to statistical package for social siences (SPSS) 22.0 for analysis. Appropriate tests were applied. A P value of less than 0.05 was taken as significant.
Ethical clearance
Ethical clearance (AIIMSRPR/IEC/2020/568) was taken from the Institutional Ethical Committee of All India Institute of Medical Sciences (AIIMS), Raipur (Chhattisgarh). Consent was taken from the participants after giving information and explaining to them the purpose of the study. They were assured that their information would be used only for academic research purposes. Confidentiality was maintained.
Results
The mean age of the participants was 35.56 ± 7.82 years. Out of them, 40.8% of the participants had three or more children. Almost one-fifth of the participants were illiterate [Table 1]. Only 4.9% of respondents belonged to the upper (general) caste. Most of the participants (80.8%) thought that one boy and one girl child was ideal for a family. The majority of participants (98.9%) had heard about family planning. Most (98.1%) of the respondents were of the opinion that family planning is the responsibility of both husband and wife. However, only 48 (13.1%) participants were active users of family planning methods at the time of the study. Among them, only 7 (1.9%) were using vasectomy, and the rest 41 (11.23%) were using condoms [Table 1]. Out of those who had adopted male sterilization, all had undergone no-scalpel vasectomy at a government hospital and received cash benefits for the same. Among those who were not using any terminal method of contraception with their spouses, only 63 had a future intention to opt for male sterilization. The score for male involvement in family planning included predictors like intention to use in the future, to know about male involvement, and current use (condoms/vasectomy). If there was an intention to involve by the male respondent in the future, the score given was 1, to know about male involvement was given a score of 2, and the current use of contraception was given a score of 3. The total lowest score was “0,” and the total highest score was “6.” If the sum of the score of the individual on the basis above three predictors was 3 or more, it was considered as good involvement, and if less than 3, was considered as poor involvement of males in family planning. The lower educational status of the wife seems to be a hindrance for understanding the role of the male in family planning as it is conceived by them it is sole the responsibility of the female. There was a significant association between the above poverty line and good involvement in family planning by the male [Table 2]. Fear of physical weakness (85.6%) and family opposition (62.6%) were commonly cited reasons by the participants for their poor involvement [Table 3]. Health care workers followed by television were the most common sources for male involvement in family planning [Figure 1].
Table 1.
Sociodemographic details of participants (n=365)
| Socio-demographic details | Frequency (%) |
|---|---|
| Age group | |
| 21-25 | 27 (7.4) |
| 26-30 | 97 (26.6) |
| 31-35 | 84 (23.0) |
| 36-45 | 108 (29.6) |
| >45 | 49 (13.4) |
| Type of Family | |
| Nuclear | 184 (50.4) |
| Joint | 181 (49.6) |
| Education | |
| Graduation and above | 26 (7.1) |
| Higher Secondary | 53 (14.5) |
| High School | 56 (15.3) |
| Middle | 92 (25.2) |
| Primary | 67 (18.4) |
| Illiterate | 71 (19.5) |
| Caste | |
| General | 18 (4.9) |
| Other Backward Caste (OBC) | 282 (77.3) |
| Scheduled Caste | 50 (13.7) |
| Scheduled Tribe | 15 (4.1) |
| The ideal number of children according to the participants | |
| 1 boy and 1 Girl | 295 (80.8) |
| 1 Boy and 2 girls | 35 (9.6) |
| 1 Boy or 1 Girl | 28 (7.7) |
| 1 Girl | 1 (0.3) |
| 1 Girl and 2 Boys | 3 (0.8) |
| 2 Boys and 2 Girls | 3 (0.8) |
| Ever used contraceptive | |
| Yes | 277 (75.9) |
| No | 88 (24.1) |
| Ever heard about family planning | |
| Yes | 361 (98.9) |
| No | 4 (1.1) |
| Family planning is the responsibility of | |
| Husband | 3 (0.8) |
| Wife | 4 (1.1) |
| Both | 358 (98.1) |
| Free provision of contraceptive at government facility | |
| Yes | 356 (97.5) |
| No | 9 (2.5) |
| Currently used contraceptive method by them | |
| Condom | 41 (11.2) |
| Oral Contraceptive Pill (OCP) | 12 (3.3) |
| Intra-Uterine Devices (IUD) | 8 (2.2) |
| Injectable Contraceptive | 1 (0.3) |
| Female sterilization | 203 (55.6) |
| Male sterilization | 7 (1.9) |
| None | 93 (25.5) |
Table 2.
Association between the score of male involvement in family planning and socio-demographic variables (n=365)
| Socio-demographic Variables | Poor involvement of male in family planning | Good involvement of male in family planning | Total | P |
|---|---|---|---|---|
| Age | ||||
| 18-25 | 24 | 03 | 27 | 0.012 |
| 26-35 | 152 | 29 | 181 | |
| 36-45 | 101 | 07 | 108 | |
| >45 | 48 | 01 | 49 | |
| Age at marriage | ||||
| <21 | 97 | 10 | 107 | 0.525 |
| ≥21 | 228 | 30 | 258 | |
| Economic status | ||||
| Below poverty line | 305 | 34 | 339 | 0.040 |
| Above poverty line | 20 | 06 | 26 | |
| Living child | ||||
| ≤2 | 186 | 29 | 215 | 0.064 |
| >2 | 139 | 11 | 150 | |
| Education | ||||
| Illiterate | 34 | 01 | 35 | 0.084 |
| Primary | 58 | 06 | 64 | |
| Middle | 100 | 09 | 109 | |
| High School | 62 | 07 | 69 | |
| Higher secondary | 32 | 08 | 40 | |
| Graduation and above | 39 | 09 | 48 | |
| Wife education | ||||
| Illiterate | 70 | 01 | 71 | 0.006 |
| Primary | 62 | 05 | 67 | |
| Middle | 83 | 09 | 92 | |
| High school | 47 | 09 | 56 | |
| Higher secondary | 43 | 10 | 53 | |
| Graduation and above | 20 | 04 | 24 | |
| Unplanned pregnancy | ||||
| Yes | 307 | 35 | 342 | 0.087 |
| No | 18 | 05 | 23 |
Table 3.
Reasons cited for not opting for male sterilization in future* (n=99)
| Reasons cited for not opting for male sterilization in future | Frequency (%) |
|---|---|
| Fear of Physical weakness | 85 (85.8) |
| Family Opposition | 62 (62.6) |
| Against social values | 9 (9.09) |
| Fear of impotence | 4 (4.04) |
| Fear of surgical complications | 1 (1.01) |
*Multiple responses
Figure 1.
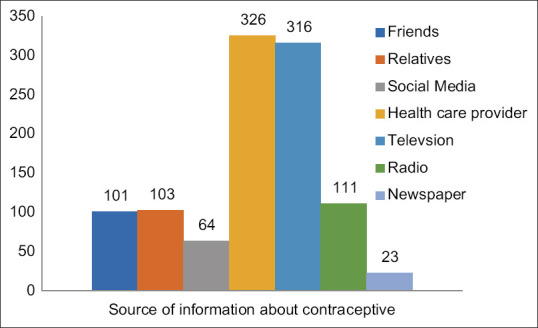
Sources of information about Contraceptive methods* (N = 365) (*multiple responses)
Discussion
Worldwide, few studies have been conducted to explore male participation in family planning, and inconsistent results have been found. Most studies on family planning have been exclusively conducted on women subjects. This study aimed to assess the involvement of husbands in family planning use and its associated factors among married men of a rural area of Chhattisgarh. The present study was conducted among men who were visiting the primary health center. The mean age of the study population was 35.56 ± 7.83 years, the mean age at marriage was 22.7 years, and the average income was around Rs 8,842 per month. This was similar to a study conducted in Haryana[2] where participants were 25–39 years and also similar to a study done in Pakistan[15] where the mean age of marriage was 23 years. Studies conducted in Mangalore[3] and Pondicherry[8] found that the mean age of participants was around 29 years, which is dissimilar to our study in which the study participants were comparatively younger.
In this study, 80.8% of the participants preferred two children (one boy and one girl) to complete the family. Most of the participants (98.9%) had heard about family planning. They heard mostly from health care providers (89.3%) followed by friends (86.7%) which are in concordance with other studies done by Rekha et al.[8] and Basu et al.[16] where the most common sources of information are health care providers and friends. This might be due to larger awareness campaigns through government and other nongovernmental Organizations (NGOs).[3] Only 48 (13.1%) participants were using either a condom or had undergone male sterilization at the time of the study which is in concordance with a study done in Uttar Pradesh by Khan and Patel et al.[17] but lower than that reported by Rekha et al.[8] Only seven participants had undergone male sterilization after getting counseled by health care providers. Findings are similar to a study done in Gadchiroli[18] where vasectomy was encouraged by health care workers. But these seven participants could not motivate other males to undergo male sterilization after sharing their own experiences. The reasons cited for not opting for male sterilization by participants were fear of physical weakness followed by family opposition and the perception that it is against social values. Our study suggested that socio-cultural factors such as stereotyping, and the feminization of family planning hinder male involvement which is also found in the study done in by Lusambili AM et al.[19] in Kenya. Our study revealed that active community involvement of health care workers will help to engage more males in family planning methods which will help further decrease maternal morbidity and mortality.
According to the scoring, good involvement of males in family planning was found in only 10.9% of the men in our study. Those who belonged to the above poverty line, educated (graduation and above), and elderly male participants had good involvement in family planning which is similar to studies done by Rekha et al. in Mangalore,[8] Onasoga et al.[20] in Nigeria, and Wondim et al.[21] in Ethiopia. In this study, more females (86.8%) were involved in the family planning method use as compared to males. This finding is in discordance with a study done in New York by James et al.[22] where more males were involved than females in family planning. Low socioeconomic status came out as a hindrance for male involvement in family planning in a study conducted by Walia et al.[23] in Haryana similar to our study. This finding shows that there is a need to promote the acceptance of vasectomy by disseminating information about its ease of use and negligible side effects and hence motivate the males in the rural area to increase their involvement in family planning. As frontline health workers and primary care and family physicians are usually first contacts for any health-related information, they are instrumental in convincing the male partners to adopt and be a part of the change to decrease the gaps in unmet needs of contraception.
Conclusion
Socio-cultural barriers demotivate men from getting involved in the family planning programme. Community sensitization programs aimed at improving male involvement in family planning should be conducted by the government and non-governmental agencies. Also, there is a need to engage community leaders to advocate for the involvement of males in family planning. The ongoing female-oriented family planning programs should be modified to accommodate men as active stakeholders. Furthermore, this study recommends increasing health literacy regarding family planning among men either by including it in the school curriculum or through awareness activities that will address their apprehensions and motivate them to use contraceptive services. This will bring gender equity in society and attainment of positive health. Sterilization facilities should be made available in the vicinity of their community so that they can easily avail the services. Providing men with information and involving them in counseling sessions can help them to be more supportive of shared decision-making. The educational system, knowledge and attitude of males towards family planning, number of living children and most important shared decision making, and spousal communication shall improve male involvement in family planning and other maternal and child health services.
Key messages
Shared responsibilities should be promoted for family planning instead of only females at the primary health care level. Effective communication tools for men to understand male involvement in family planning should be made in a such way that leads to change in demand-side behavior from the couple.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Balaiah D, Ghule M, Naik DD, Parida RC, Hazari KT. Fertility attitudes and family planning practices of men in rural community of Maharashtra. J Fam Welf. 2001;47:56–67. [Google Scholar]
- 2.Yadav K, Singh B, Goswami K. Unmet family planning need: Differences and levels of agreement between husband-wife, Haryana, India. Indian J Community Med. 2009;34:188–91. doi: 10.4103/0970-0218.55281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mumbai: IIPS; 2015-2016. International Institute for Population Sciences. National Family Health Survey-4 India Factsheet. [Google Scholar]
- 4.Reddy R, Premarajan KC, Narayan KA, Mishra AK. Rapid appraisal of knowledge, attitude and practices related to family planning methods among men within 5 years of married life. Indian J Prev Soc Med. 2003;34:62–7. [Google Scholar]
- 5.Verma GR, Rohini A. Attitude of spouse towards family planning: A study among married men and women of a rural community in West Godavari District, Andhra-Pradesh. Anthropologist. 2008;10:71–5. [Google Scholar]
- 6.Levtov RG, Barker G, Contreras-Urbina M, Heilman B, Verma R. Pathways to gender-equitable men: Findings from the international men and gender equality survey in eight countries. Men Masc. 2014;17:467–501. [Google Scholar]
- 7.Hardee K, Croce-Galis M, Gay J. Are men well served by family planning programs? Reprod Health. 2017;14:14. doi: 10.1186/s12978-017-0278-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rekha T, Unnikrishnan B, Mithra PP, Kumar N, Holla R, Raina V, et al. Married Men's involvement in family planning – A study from coastal Southern India. J Clin Diagn Res. 2015;9:LC04–7. doi: 10.7860/JCDR/2015/12101.5837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chankapa YD, Pal R, Tsering D. Male behavior toward reproductive responsibilities in Sikkim. Indian J Community Med. 2010;35:40–5. doi: 10.4103/0970-0218.62552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chaudhary BK, Wantamutte AS, Angolkar M, Sah JK. Knowledge, attitude and practice of condom use among married men in an Urban Slum Area of Ramnagar, Karnataka. Int Organisation Scientific Research- J Humanit Soc Sci. 2015;20:106–9. [Google Scholar]
- 11.Shekhar R, Bhar D, Singh C. Awareness, knowledge and practices of contraceptive methods among married males of slums of Phulwarisharif block of Patna District, Bihar. Indian J Community Health. 2019;31:236–43. [Google Scholar]
- 12.Cleland J, Harbison S, Shah IH. Unmet need for contraception: Issues and challenges. Stud Fam Plan. 2014;45:105–22. doi: 10.1111/j.1728-4465.2014.00380.x. [DOI] [PubMed] [Google Scholar]
- 13.Dudgeon MR, Inhorn MC. Men's influences on women's reproductive health: Medical anthropological perspectives. Soc Sci Med. 2004;59:1379–95. doi: 10.1016/j.socscimed.2003.11.035. [DOI] [PubMed] [Google Scholar]
- 14.Varga CA. The forgotten fifty percent: A review of sexual and reproductive health research and programs focused on boys and young men in sub-Saharan Africa. Afr J Reprod Health. 2001;5:175–95. [PubMed] [Google Scholar]
- 15.Abdul Nasir J, Tahir MH, Zaidi AA. Contraceptive attitude and behaviour among university men: A study from Punjab, Pakistan. J Ayub Med Coll Abbottabad. 2010;22:125–8. [PubMed] [Google Scholar]
- 16.Basu S, Kapoor AK, Basu SK. Knowledge, attitude and practice of family planning among tribals. J Fam Welf. 2004;50:24–30. [Google Scholar]
- 17.Khan ME, Patel BC. Male involvement in family planning-A KABP study of Agra district- Final report. Population Council of New Delhi. 1997 [Google Scholar]
- 18.Jungari S, Paswan B. Male perception and participation in family planning among tribal communities of Maharashtra, India: A mixed-method study. Int Q Community Health Educ. 2020;40:163–9. doi: 10.1177/0272684X19875017. [DOI] [PubMed] [Google Scholar]
- 19.Lusambili AM, Muriuki P, Wisofschi S, Shumba CS, Mantel M, Obure J, et al. Male involvement in reproductive and maternal and new child health: An evaluative qualitative study on facilitators and barriers from Rural Kenya. Front Public Health. 2021;9:644293. doi: 10.3389/fpubh.2021.644293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Onasoga OA, Edoni EER, Ekanem J. Knowledge and attitude of men towards vasectomy as a family planning method in Edo state, Nigeria. J Res Nurs Midwifery. 2013;2:12–21. [Google Scholar]
- 21.Wondim G, Degu G, Teka Y, Diress G. Male involvement in family planning utilization and associated factors in Womberma District, Northern Ethiopia: Community-based cross-sectional study. Open Access J Contracept. 2020;11:197–207. doi: 10.2147/OAJC.S287159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.James M, Hoff T. A new national survey on men's role in preventing pregnancy: Women and men think men need to be more involved in contraceptive choice and use. [Last accessed on 2021 Dec 07]. Available from: http://kaiserfamilyfoundation.files.wordpress.com/1997/02/1252-nr-another-gender-gap.pdf .
- 23.Walia M, Mittal A, Kumar D. Male participation in reproductive health care of women and factors associated with interpersonal relationship: A cross-sectional study in a rural community of Ambala District in Haryana. Indian J Public Health. 2021;65:178–8. doi: 10.4103/ijph.IJPH_262_20. [DOI] [PubMed] [Google Scholar]