

Abstract
Eagle’s syndrome is one of the commonly overlooked cause of foreign body sensation in throat with referred otalgia. Incidence of symptomatic cases was rare. Elongated Styloid process may present with myriad symptoms. The diagnosis needs a cautious approach and the management is mainly aimed at reduction of the length of elongated section. Prospective study in the Department of ENT Stanley Medical College, Chennai. Study period-January 2018 to September 2018. Clinical examination followed by radiological investigations done to confirm the diagnosis. Stylo-tonsillectomy was done in the selected 20 subjects and post-operative outcomes were compared with pre-operative questionnaires. The progression of symptoms were evaluated for resolution and studied. Pharyngeal symptoms are more common. The length of styloid is associated with symptom complex presentation. The incidence was 0.17% in general population coming to ENT OPD and more common among women with mean age of 43 years. Bilateral presentation was more common and the longest length recorded in the study was 78 mm. Single investigation is not enough to confirm the diagnosis. A minimum of two investigations are needed for planning surgical management. Intra-oral approach with stylo-tonsillectomy was done with no major complications in post-operative period. Pre-operative symptoms were recoreded by use of McGill’s pain questionnaire and compared with post-operative scores. Dysphagia was the major post-operative early symptom which took a week minimum to subside. Clinical findings and atleast 2 imaging studies needed for diagnosis of the disorder. OPG though economical can be aided to great extent by use of Conebeam CT or 3D CT to study the elongated styloid process. Stylo-tonsillectomy is a safer approach with minimum complications and earlier relief of pre-operative symptoms. Surgical management with reduction of length of elongated styloid followed by adequate analgesia remains mainstay in treatment.
Keywords: Eagle’s syndrome, CBCT styloid, 3D styloid imaging, OPG styloid, Eagle’s syndrome, Stylalgia, Otalgia, Foreign body sensation of throat, Cervicofacial pain, 3D reconstruction CT of neck
Introduction
The styloid is a slender bone meaning pillar in greek. It is a part of temporal bone derived from tympanohyale and stylohyale part of stylohyoid chain. The length and angulation of the styloid process is of importance as the close relation of glossopharyngeal and carotid complex to its tip can lead to Eagle’s syndrome. The syndrome is named after Watt W. Eagle who first described it in his cases report. Elongated styloid process causes a variety of symptoms only on its impingement with the adjacent neural and vascular structures. An attempt has been made through various studies to see for post-operative relief of symptoms. This study aims to study the symptomatology with regards to presentation, gender relation and relief found post-operatively.
Anatomy
Often called the ‘Riolan’s bouquet’—the styloid process is attached with three muscles—stylohyoid, stylopharyngeus and styloglossus; and two ligaments—stylohyoid and stylomandibular. The muscles each have separate innervation. The normal length is less than 2.5 cm. Any longer is considered elongated by Eagle. Scott–Brown considers elongated as more than 4 cm. The angulation of styloid with the base is more important than its length in cases of neuralgia.
The styloid apparatus lies lateral to carotid sheath. The external carotid artery passes between the muscles of stylohyoid apparatus. It runs deep to digastric and stylohyoid but superficial to stylopharyngeus to enter parotid gland. The retromandibular vein on the other hand passes down from parotid gland superficial to stylohyoid and digastric.
The glossopharyngeal nerve emerges from brainstem in line with vagus and accessory nerves and exits from skull via jugular foramen. It descends between jugular vein and carotid artery, picking up sympathetic fibres from carotid plexus as it loops forwards medially to reach the soft tissues of the oropharynx, posterior tongue and palate. In its course it gives off lesser petrosal nerve conveying the secretomotor fibres for the parotid gland to the otic ganglion [1].
Eagle’s Syndrome
A wide variety of symptoms have been attributed to elongated styloid process.
Cervicofacial pain
Otalgia
Foreign body sensation of throat
Pain on changing head position
Cervical pain
Pain on swallowing
Eagle described two forms based on symptom. First group consisted of patients suffering from pharyngeal pain localized to tonsillar fossa that sometimes radiate to hyoid bone due to scarring around styloid tip following tonsillectomy. Second group where people who were having pain and foreign body sensation and who have previously not undergone tonsillectomy [2].
Various theories have been proposed by Steinmann to explain the calcification of stylohyoid ligament: reactive hyperplasia, reactive metaplasia and anatomic variance. Among them most accepted cause for calcification is being reactive hyperplasia due to chronic ‘micro trauma’ [3].
Several mechanisms for symptomatology in elongated styloid process have been proposed. These include.
Compression of neural elements in particularly the glossopharyngeal nerve
Granulation following fracture of ossified stylohyoid ligament leading to pain
Impingement on the carotid sheath
Insertion tendinosis
Irritation of the pharyngeal mucosa
Stretching and fibrosis of tonsillar bed following tonsillectomy, involving the trigeminal, facial, glossopharyngeal and vagus nerves.
‘Stylalgia’ is pain in elongated styloid process due to formation of stiff bony clasp which hampers the elastic movement of stylohyoid ligament during contraction of pharyngeal muscles, the pain being secondary to irritation of sympathetic plexus around carotid arteries or sinus branch of glossopharyngeal nerve. Thus cause for the neuralgia is believed to be due to compression of neural elements by styloid itself and or due to reparative granuloma surrounding the styloid process.
The length of styloid process is normally 20–30 mm. Symptoms start with elongation of 25 mm due to varied angulation of styloid process. By definition 40 mm and above is considered elongated styloid process.
The cause of onset of pain in subjects previously free of symptoms is unknown but several mechanisms have been studied upon including rheumatic styloiditis causing pharyngeal infection, trauma, tonsillectomy and involutional changes associated with ageing (degenerative cervical discopathy) may shorten the cervical spine and alter the direction of styloid process.
There can be several variations in the styloid chain as in
Length of the styloid
Thickness of segments
Angle and direction of tip of styloid
Degree of calcification
The commonest clinical features are foreign body sensation in throat, otalgia, odynophagia, pain on change in head position and cervical pain. Craniofacial pain may also be a feature.
Evaluation of Styloid
The evaluation of symptomatic Eagle’s syndrome is combination of clinical and radiographic features.
Clinical examination must include clinical palpation of styloid and testing with lignocaine for pain relief.
- Palpation
- The tip of styloid should be palpablevvv
- Point to note where the tip is palpable- superior, middle or inferior part of tonsillar region
- Lignocaine pain relief test
- 4% lignocaine soaked cotton ball placed over point of palpable styloid for 10 s.
- To assess the pain relief as positive for Stylalgia—if there is no pain after the cotton ball removed.
Radiographic examination must include atleast any 2 of the following
Orthopantomogram
Cone beam Computer tomogram
3D reconstruction of styloid process in Computer Tomography of Neck and Skull base
Orthopantomogram
It is a panoromic radiography for detection of elongation and ossification of styloid process and the temperomandibular joint. The limitations are trismus and motion artifacts. Rotational OPGs are obtained by rotating slender X-ray beam in a horizontal axis that is positioned extra orally. To eliminate scatter and artefact X-ray beam is angled beneath occipital condyle of skull approximately 4° to 7°. The patient remains stationary as X-ray tube and film cassette holder rotate around patient’s face during exposure [4] (Fig. 1).
Fig. 1.
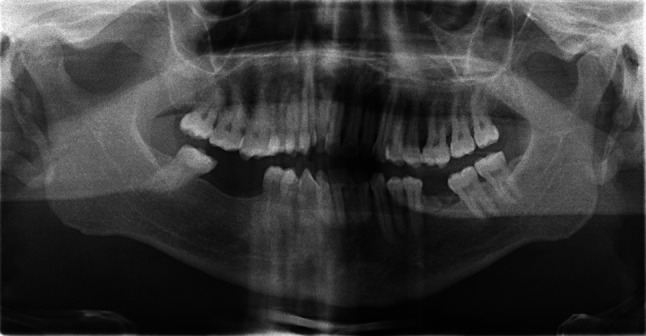
OPG elongated Styloid process
Cone Beam CT of Styloid
CBCT technique consists of the use of a round or rectangular cone shaped X-ray beam with a single 360° scan where the X-ray source and a reciprocating array of detector simultaneously move around the patient’s head, which is stabilized with a head holder. Single projection images, known as “basis” images, are acquired at certain degree intervals, which are similar to lateral cephalometric radiographic images, each slightly offset from one another. The series of such basis projection images is referred to as the projection data, on which software programs incorporating sophisticated algorithms are applied to generate a 3D volumetric data set, which can be used to provide primary reconstruction images in all three orthogonal planes (axial, sagittal, and coronal) [5] (Fig. 2).
Fig. 2.
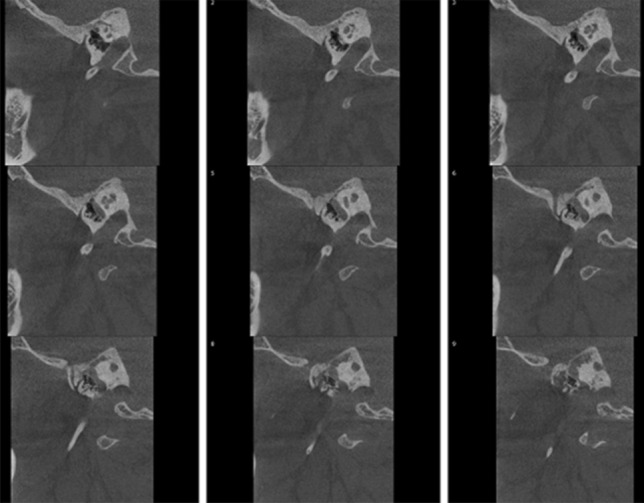
Conebeam CT( left) showing elongated styloid process
3D Reconstruction of Styloid in Computer Tomography
The 3D reconstruction CT of styloid gives an accurate assessment of length actual styloid process and ossified parts of stylohyoid ligament. The true character of bilateral asymmetrical malformations may be evaluated with this imaging technique as overlap of structures is not encountered. The alternative is HRCT of temporal bone for measuring the number of cuts the styloid is visible along with the ossified ligament and multiplying with the slice thickness to get the length of styloid elongation. This does not differentiate styloid from calcified ligament [6] (Fig. 3).
Fig. 3.
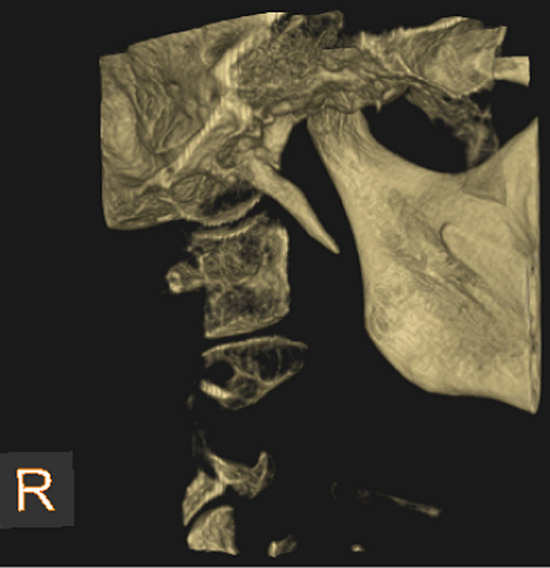
3D reconstruction image showing Styloid process
Other methods of imaging studies are:
Lateral view of neck X-ray
Reverse Towne’s view X-ray of Skull
High resolution CT of temporal bone-count the number of films showing the styloid to assess the length of styloid,
The former two roentgenograms mentioned show the elongation but have many a bony superimposition of other structures, hence diagnosis can be easily missed.
Methods
A prospective study was done in academic tertiary care centre of patients who had elongated styloid process with symptoms of foreign body sensation in throat, odynophagia and otalgia from January 2018 to September 2018.
All patients were evaluated for the commonly presenting symptoms related to elongated styloid process with a questionnaire and clinical tests to identify the styloid tip projection and relief of symptom with 4% lignocaine.
Inclusion criteria:
Age: 18 years of age and above—65 years of age and below
Clinically and/ or radiologically significant elongation of styloid process
Calcified stylohyoid ligament
Exclusion criteria:
Age: 17 years and below and
More than 66 years of age
Systemic co-morbities—coronary vascular and cerebrovascular diseases
Malignancies
Dental malocclusion
The patients were all subjected to Orthopantomogram (OPG) for confirmation of elongated styloid. The length of the elongated styloid was studied both with OPG and CT. Cone beam CT and 3D reconstruction CT was done randomly. The length and nature of elongated styloid was assessed.
All the subjects were admininstered McGill’s pain questionnaire to assess degree of preoperative symptoms and post-operative resolution of same. Chosen method of excision by intraoral approach of stylo-tonsillectomy under GA and had a course of intravenous antibiotics for a week and oral antibiotics for a fortnight. Analgesia was required in post-operative period for pharyngodynia and dysphagia for 1 week. Of the 20 patients only 2 required a 3 month Gabapentin and Amitryptilline. Post-operative symtoms were recorded for dysphagia using IOWA Clinical bedside swallowing assessment scale. Besides the 20 patients 3 patients were managed conservatively since they had ankylosing spondylosis and paget’s disease and their data was not included in the study.
Results
Incidence was found to be 20 cases among average 11,175 OPD cases over a period of 9 months. Making it 0.20%, in tune with reported incidence worldwide.
The gender most commonly affected was female. There were only 3 cases of male when compared to 17 cases of female patients. The mean age of presentation was 43 years (Fig. 4).
Fig. 4.

Gender distribution
Bilateral elongation of styloid was more common when compared to unilateral presentation with respect to symptomatic side. Of the 20 cases, 2 had symptoms only on the left, 4 only on the right and remaining 14 both sides (Fig. 5).
Fig. 5.

Side of symptoms
There was no specific predilection of side when compared to gender. Both sexes where equally affected with respect to side affected the most- being bilateral.
Symptomatic presentation was most common in throat—with foreign body sensation in throat, odynophagia, ear related symptoms of ear pain and tinnitus and lastly cervical pain. Of the 20 subjects studied: 9 had ear related symptoms, 18 had foreign body sensation of throat, 6 had cervical pain and all 20 had odynophagia. Thus the most common presentation is throat related. Tinnitus was present only in 1 subject. Only 1 patient had sole symptom of odynophagia. The remaining 19 had a complex of symptoms very assuming of diagnosis (Fig. 6).
Fig. 6.

Presenting symptoms
The length and nature of styloid process which were symptomatic were studied by using OPG and ConebeamCT and the results are tabulated as follows. The maximum length in current study was measured to be 78 mm and the minimum length which was symptomatic to be 25 mm. Our study had only one styloid as of segmented nature. No correlation could be done regarding nature of styloid process and post tonsillectomy status as only one patient had a history of tonsillectomy done but even that patient had only unsegmented elongation (Tables 1, 2).
Table 1.
Length of styloid
| Side of Styloid | Number patients | Minimum length in mm | Maximum length in mm | Mean | SD |
|---|---|---|---|---|---|
| Right | 20 | 25 | 51 | 34.65 | 6.491 |
| Left | 20 | 28 | 78 | 34.05 | 13.288 |
Table 2.
Nature of styloid
| Side | No. Unsegmented elongation | No.Segmented Elongation |
|---|---|---|
| Right | 17 | 1 |
| Left | 16 | 0 |
The position of styloid tip palpable was studied clinically in initial examination and confirmed on surgical intervention as follows (Table 3).
Table 3.
Position of styloid tip palpable in relation to Tonsillar fossa
| Gender | Superior pole | Middle of Fossa | Inferior Pole /Could not be palpable |
|---|---|---|---|
| Right | 4 | 11 | 3 |
| Left | 4 | 9 | 3 |
There was no correlation on the gender and site of palpable styloid tip (Table 4).
Table 4.
Post-operative evaluation of symptoms
| Symptom | Pre-operative | Post-operative | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Number | SD | Std Error of Mean | Mean | Number | SD | Std Error of Mean | |
| Ear | 5.89 | 9 | 1.054 | 0.351 | 1.67 | 9 | 0.707 | 0.236 |
| Odynophagia | 7.00 | 20 | 1.170 | 0.262 | 1.80 | 20 | 0.616 | 0.138 |
| Cervical pain | 4.00 | 7 | 1.915 | 0.724 | 1.00 | 7 | 0.577 | 0.218 |
| Foreign body sensation | 7.39 | 18 | 0.979 | 0.231 | 2.00 | 18 | 0.686 | 0.162 |
Based on the above analysis it has been found that considerable reduction in 4 main symptoms which have been used as parameters of the study. The mean score for ear related symptoms is 5.89 in pre op period which reduced to 1.67 in post op period. With the mean score for preop odynophagia is 7.00 which only 1.80 in post op period. The study also shows a pre op cervical pain mean of 4 and post op cervical pain score of 1. With regards to foreign body sensation in throat pre op score is mean of 7.39 which reduce to 2.00 in post op analysis. This shows a considerable reduction in each of the symptom parameter studied with p value of < 0.01, which is considered highly significant.
Of the 20 subjects 16 cases had moderate dysphagia and 4 cases had severe dysphagia in the 30 days following procedure. The progression of dysphagia had a crescendo-decrescendo pattern in appearance and disappearance. The dysphagia in post-operative period was assessed by bedside swallowing test which showed cough and voice change were common and that they were due to inadequate swallowing due to pain thus leading to saliva pooling in the vallecula and pyriform fossa (Figs. 7, 8).
Fig. 7.
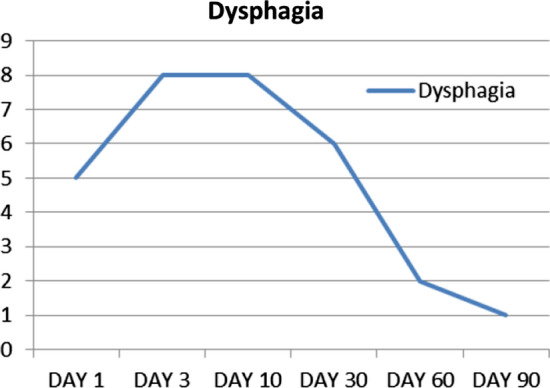
Progression of dysphagia in post-operative period
Fig. 8.
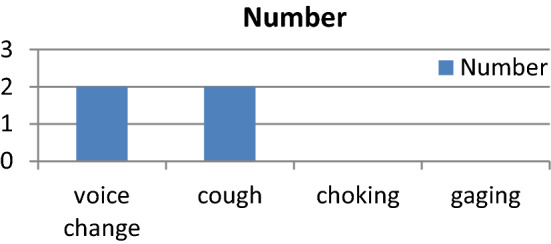
Post-operative bedside assessment of swallowing
The collected data were analysed with IBM.SPSS statistics software 23.0 Version.
To describe about the data descriptive statistics frequency analysis, percentage analysis were used for categorical variables and the mean & S.D were used for continuous variables. To find the significant difference between the bivariate samples in Paired groups the Paired sample t test was used. In the above statistical tool the probability value 0.05 is considered as significant level.
Discussion
Sandev et al., studied the differential diagnosis and concluded that Eagles’ syndrome was not such a rare entity and occurs in 30% men and women. Incidence is 4% in general population of which only 4% present with symptoms [7].
Prasad et al. studied the various presentations in South Indian population retrospectively over 10 year period in 58 subjects with only OPG and lateral radiographs- aided by Goldstein and Scoop et al. studies. They concluded that though bilateral elongated SP may present with unilateral symptoms it is advised to do bilateral excision. Further intra oral approach was used in all subjects and minimum complications were encountered [8].
Donmez et al. studied that cone beam computer tomogram was more effective tool in diagnosing accurately the length of styloid elongated [9].
In Raja et al. study, the incidence of stylgia, classical Eagles syndrome, was found to be 0.44 per 1000 ENT OPD visiting people. The mean age at presentation was found to be 40.70 years. The Females cases were more than twice as common as males. The average duration of symptoms was 22 months at presentation, and bilateral symptoms were found in 9 out of 10 patients, with left and right predominant in 5 cases each. The patients had varied symptomatology with oropharyngeal pain as most common. The average styloid process size was found to be 3.99 cm on right and 4.29 cm on left. All patients were operated by intraoral tonsilostyloidectomy method, and 0.8 to 2.5 cm bone size removed. Three of the patients were off all drugs within 3 week time, while 9 more patients were weaned off in 6 week time and 5 more in two months. Complete resolution was achieved in 17/19 patients, (89.4%). And concluded that a high index of suspicion and an active look out for enlarged styloid processes in cases of chronic pharyngeal pain is highly recommended. Patients diagnosed with stylgia should be actively counselled for surgical intervention. The surgical approach, i.e. intraoral tonsilostyloidectomy, is a safe and highly effective procedure [10].
Salam et al. studied and gave the conclusion that Eagle’s syndrome is a relatively common disorder that is frequently misdiagnosed. Patients with vague cervico facial pain, throat pain, foreign body sensation throat, referred otalgia, etc., should be palpated for elongated styloid process and investigated for the same. This condition has a female preponderance, and the most commonly affected age group is 30–39 years. CT scan styloid remains a radiological investigation to diagnose elongated styloid process with or without calcified stylohyoid ligament. Medical treatment will not give a long-standing symptomatic relief in elongated styloid process [11].
Nayak et al. study showed that elongated styloid process is a relatively common cause of facial and neck pain, but it is often misdiagnosed due to its varied clinical presentation. Since an elongated styloid process is often confirmed by radiological means, it would be helpful to find a more accurate mode of depicting the styloid process. In their prospective study, 39 cases were evaluated. A three-dimensional computed tomography (3D CT) reconstruction of the styloid process was performed in 18 cases. In these patients, they compared the length and medial angulation of the symptomatic styloid process as viewed on an orthopantomogram and a 3D CT reconstruction. It was noted that a 3D CT reconstruction was more accurate in depicting the styloid process. Thus the investigation can be considered as the 'gold standard' in the radiological diagnosis of an elongated styloid process [12].
Conclusion
This observational study was conducted in the department of ENT and Head and Neck Surgery of Government Stanley Medical College and Hospital from January 2018 to September 2018. A total of 20 patients were identified and the presenting symptoms were studied along with assessment of severity of pain by McGill’s pain questionnaire.
Our study showed average of 34.65 cm on the right and 34.05 cm on the left as mean length in elongation in styloid process. The 3 major theories for elongation of styloid process were discussed. Of them the theory of anatomic variance holds good to support the study subjects in our study Irrespective of presentation of varied complex of symptoms odynophagia remains the more common presentation followed by foreign body sensation in throat. Referred Otalgia and tinnitus and the cervical pain were low-with 9 patients presenting with ear complaints, 20 with odynophagia, 7 with cervical pain and 18 with foreign body sensation in throat. The common cause for the symptom of foreign body sensation- in elongated styloid process remains the irritation of pharyngeal mucosa as shortening of styloid process by excision has relieved the same in majority of the subjects. The maximum length measured in the study was 78 mm and unsegmented form is more common. The presentation of palpable tip of styloid was more in the middle of tonsillar fossa.
The use of OPG as sole determining factor of Eagle’s syndrome though economically valid can be supported with either cone beam Computer tomogram or 3D reconstruction images to study the nature of styloid process and its relation to surrounding structures.
The effect of styloidectomy on swallowing was additionally assessed by bed side assessment using IOWA swallowing protocol. Dysphagia in post-operative period is detected by means of the presence of coughing, choking and voice change on the act of swallowing. The presence of wet speech after swallowing signified the inadequate bolus clearance which was due to dysphagia. Further aspiration symptoms pointed to dysphagia.
Of the 20 patients all 20 had dysphagia due to post-operative oedema in the 1 month following surgery. They were given adequate analgesics and anti-inflammatory drugs to tide over the pain. The severity of dysphagia was assessed and its progression was analysed- a crescendo-decrescendo pattern in appearance and disappearance of dysphagia was seen. 16 patients had moderate dysphagia and 4 patients had severe dysphagia. Of the 4 patients with severe dysphagia, 2 had voice change due to wet nature of voice signifying inadequate clearing and 2 had cough on swallowing. All 16 patients were relieved of symptoms by day 90 post-operatively.
The styloidectomy induced difficulty in articulation of jaw movements to swallowing, though expected, was not that prominent as symptom. The absence of latter was most probably because of compensatory action of the other muscles of mastication and deglutition.
Instability in temperomandibular joint, an expected complication was not seen in any of the cases. Hence change in facial symmetry an effect of the latter was not seen.
Intra oral approach for excision of the elongated process is better in terms of prevention of cranial nerve injuries. With adequate antibiotics in early pre-operative period the risk of infections can be negligible.
Acknowledgements
The corresponding author wishes to acknowledge the ever supportive teaching faculty of the institution where the study was conducted; Dr. K. Athiyaman, Dr. P. Chozhan and Dr. V. Saravanaselvan without whom surgical treatment of the population studied would not have been accomplished and the faculty of Government Dental College and Hospital, Chennai and the radiologists of Government Stanley Medical College, Chennai without whom the radiological studies could not have be done.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
Obtained from Institutional Ethical Committee. Informed written consent was obtained from all participants of the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Philip DY, Otalgia (2018) In: Watkinson JC et al. Scott-Brown’s otorhinolaryngology head and neck surgery, volume 3 8th edn, p 1145
- 2.Eagle WW. Elongated styloid process: report of two cases. Arch Otolaryngol. 1937;25:584–586. doi: 10.1001/archotol.1937.00650010656008. [DOI] [PubMed] [Google Scholar]
- 3.Steinmann EP. Styloid syndrome in absence of an elongated process. Acta Otolaryngol. 1968;66:347–356. doi: 10.3109/00016486809126301. [DOI] [PubMed] [Google Scholar]
- 4.Divyadharshini, Jayanth Kumar V (2016) Assessment of styloid process length in orthopantomogram—a radiographic study. Int J Pharm Bio Sci 7(4): 503–506
- 5.Kumar M, Shanavas M, Sidappa A, Kiran M. Cone beam computed tomography—know its secrets. J Int Oral Health. 2015;7(2):64–68. [PMC free article] [PubMed] [Google Scholar]
- 6.Huang C-C, Tsai Y-H, Liao Y-S, Weng H-H, Yang B-Y. Three-dimensional reconstruction CT in diagnosis of Eagle’s syndrome: a retrospective study. Chin J Radiol. 2006;31:221–225. [Google Scholar]
- 7.Sebastijan S, Klara S. Styloid process syndrome. Actastomatolcroat. 2000;34(4):451–456. [Google Scholar]
- 8.Prasad KC, et al. Elongated styloid process (Eagle's syndrome): A clinical study. J Oral Maxillofac Surg. 2002;60(2):171–175. doi: 10.1053/joms.2002.29814. [DOI] [PubMed] [Google Scholar]
- 9.Donmez M, Okumus O, Pekiner FN. Cone beam computed tomographic evaluation of styloid process: a retrospective study of 1000 patients. Eur J Dent. 2017;11:210–215. doi: 10.4103/ejd.ejd_56_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Raja SK, et al. Active surgical management of pharyngodynia in cases attributable to styloid complex. Int J Appl Res. 2018;4(3):319–323. [Google Scholar]
- 11.Salam RTA. A clinical analysis of Eagle’s syndrome by its clinical features and therapeutic response to surgical treatment. Int J Sci Stud. 2017;5(10):97–104. [Google Scholar]
- 12.Nayak DR, Pujary K, Aggarwal M, Punnoose SE, Vachaly (2007) Role of three-dimensional computed tomography reconstruction in the management of elongated styloid process: a preliminary study. J Laryngol Otol 121:349–353. [DOI] [PubMed]