

Abstract
Background:
Migraine, one of the most common headaches in children, has a significant impact on children and their family's quality of life (QoL). There are two approaches for controlling migraine headaches preventative and controlling acute attacks. Several drugs have been used for this purpose, and tricyclic antidepressants were at the top. Amitriptyline has shown not only a desirable effect on controlling the headaches but also some adverse side effects. Recently, finding effective drugs with fewer side effects, become more critical. Among them, nutraceuticals were one of the promising ones.
Materials and Methods:
In this randomized clinical trial on 72 patients aged 5–15 years old with diagnosis of migraine based on the International Headache Society criteria, we compare the effectiveness of coenzyme Qten on frequency, duration, and severity of childhood migraine. For comparing the QoL, we used the International PedMIDAS questionnaire.
Results:
Coenzyme Qten showed good therapeutic effects in children, especially in long-term use; however, amitriptyline showed more rapid response. After 3 months of treatment, clinical outcomes in the two groups did not significantly differ from each other. Similarly, Children's QoL increased in the same way. There are more reported side effects in children using amitriptyline compared to coenzyme Qten.
Conclusions:
According to results, Co-enzyme Q10, with fewer side effects and comparable therapeutic effects, especially in the long term, could be a good drug for prophylactic treatment of migraine headaches.
Keywords: Child, clinical trial, co-enzyme Q10, migraine disorders, therapy amitriptyline
Introduction
Migraine is the most common type of headache diagnosed in children and the most common recurrent headache that draws the attention of parents and primary care providers. Ten percent of 5-15 years old children have migraines, and 75% of children referred for neurological consultation due to headaches are diagnosed with migraines. Migraine is an inherited disorder. When both parents are evaluated, at least 90% of them would have a history of migraines.[1,2,3,4,5,6,7,8,9]
Migraine causes school absenteeism, restrictions on home activities, restrictions on social activities, and has a significant impact on patient lives. As headaches recur, their adverse effects increase and cause more complications, such as anxiety about avoiding school and a more expensive treatment plan. Common triggers of migraines include stress, exercise, decreased estrogen levels in the premenstrual cycle, and changes in barometric pressure.[3,5,6]
There are three groups of migraine in children: Migraine with aura, migraine without aura, and migraine-equivalent syndromes. Migraine without aura is more common than other types. In addition to headaches in specific periods of life, migraine can manifest in the form of recurrent symptoms such as periodic vomiting, recurrent abdominal pain, benign seizure vertigo, basilar migraine, seizure torticollis, and hemiplegic migraine. These are considered migraine-equivalent syndromes, which sometimes are associated with headaches or transform to migraine headaches at some stages in later life.[3,5,6]
Migraine is diagnosed based on clinical symptoms, therefore physicians cannot make a diagnosis based on brain imaging. Two treatment approaches for migraines include acute attack treatment and preventive treatment, if necessary.[3,5,6]
For preventing migraine and its variants, in addition to improving the quality of life (QoL), sleep, and avoiding foods such as caffeine-containing substances, medication can also be administered in cases where there are multiple attacks and severe daily disabilities. Known treatments for migraine headaches include amitriptyline, beta-blockers, biofeedback, coenzyme Q10, behavioral-cognitive therapies, riboflavin, and Topiramate.[10]
Numerous studies have suggested using tricyclic antidepressants, especially amitriptyline.[3,5,6] However, drug use is limited due to side effects such as drowsiness, cardiac arrhythmias, age restriction, and its form, which is only available in tablet form. Recently, other drugs are becoming more popular, including nutraceuticals such as Vitamin D, riboflavin, coenzyme Q10, magnesium, butterbur, and polyunsaturated fatty acid. These supplements have been widely accepted due to fewer side effects.[3,5,6,11,12]
Coenzyme Q10 is available in capsules, coated tablets, and gels, with no age limit, and minimal side effects compared to other drugs used. Due to low side effects and better tolerance, if effective, it can replace previous drugs, such as amitriptyline. We found that there is no study on the efficacy of this drug in children in Iran so, in our study, we determined to study the effect of this drug on duration, frequency, the severity of headaches, and QoL in children with migraines in comparison with previously approved one, amitriptyline.
Materials and Methods
This study is a randomized parallel clinical trial with control group, involving children with migraines, diagnosed based on ICHD-III (The International Classification of Headache Disorders) criteria[13] by pediatric neurologists. Seventy-two children aged 5–15 years with migraine with or without aura, who diagnosed based on (International Headache Society [IHS]) criteria that have migraine attacks at least twice a week or four times a month, forcing them to consume painkiller or disrupt their daily activities were recruited. Children not willing to enter the study, showing severe and uncontrolled side effects of Q10 or Amitriptyline, diagnosed other than migraine during the study, having complicated epilepsy or migraine, having a history of drug allergy, taking migraine prophylaxis (except for Q10 and amitriptyline) were excluded from the study. Also, children having migraines with severe psychiatric problems such as depression and attention deficit hyperactivity disorder, using painkillers more than four times a week to control migraine attacks, were excluded from the study. Furthermore, in case of lacking ability to obtain data or inaccessibility to patients, they were discontinued from the study.
Medications: Coenzyme Q10 is available in the form of 100 mg laminated tablets, 30 and 100 mg capsules and 100 mg soft gel. In this study, the Q10 dosage used for children <30 kg was 30 mg and for children over 30 kg was 60 mg. Q10 tablets were bought from Euro-vital Pharmaceutical Company. Amitriptyline is in the form of 25 mg tablets and was used in the dosage of 1–2 mg/kg for all children, and if the dose is higher than 1 mg/kg, the entire dosage was divided into two doses to be taken at noon and before bedtime.[8] In addition to prescribing medication to all patients, advice on the factors that may exacerbate the headaches was made, such as nutritional, physical, and psychological factors.[3,5,6]
Randomization: In this clinical trial, starting in winter 2018, 72 patients were randomly selected from children referred to the neurology clinic of Imam Hossein Hospital, who have met the inclusion criteria. They were then randomly assigned to the two study groups (Coenzyme Q10 or amitriptyline) by binary blocks. Adequate explanations were given to parents and informed consent was obtained. In this study, only statistical analysis is blind for treatment groups; however, physicians and patients are aware of groups.
Preenrollment investigations: During a 4-weeks phase, all study candidates underwent systemic and neurological examinations before enrollment. If necessary, electroencephalography and Neuro-imaging tests will be performed based on the neurologist's diagnosis, and a laboratory examination including CBC, liver function test, and creatinine was done. All patients were given the necessary training to accurately record the number, severity, and duration of headaches.
Outcome Measures: In addition to demographic information, data on headache severity, frequency of headaches, duration of headaches in each attack, presence or absence of associated symptoms, as well as drug side effects were collected using a well-designed checklist. For headaches severity, we use Wong-baker faces pain rating scale ranging from zero to ten, which could be used easily for children.[14] Evaluated drug side effects include drowsiness, restlessness, and constipation, which were reported in previous studies.[15,16,17,18] Patients’ QoL was assessed before and after treatment using the standard PedMIDAS Grading Scale used in previous studies.[14,19] Except for appropriate treatment, no other prophylactic medication was prescribed to patients in the two groups. Only, painkillers such as acetaminophen or NSAIDs were allowed in case of acute headache attacks. The number of days in need of acetaminophen and ibuprofen painkillers during the month was also recorded.
Duration of study
For all patients who are potential candidates for enrollment, the 1st month was devoted to initial screening and parents training to be able to accurately describe their child's headaches in terms of severity, duration, and severity. Then, the patient or parents were required to record the frequency, duration, and severity of the headache daily, weekly, and monthly in the provided checklist. Furthermore, parents and patients were required to have a migraine diary, so we got an accurate estimate of the headaches each week during the study. After entering the study, patients were followed for 3 months, during which patients were visited every month. The QoL checklist (PedMIDAS) was completed before and after the study.
Statistical analysis
Patients’ data were divided into quantitative and qualitative variables. Statistical indices appropriate to the nature of the variable were used to describe the variables, including mean, standard deviation (SD), frequency, and relative frequency. Kolmogorov–Smirnov test was used to evaluate the normality of the data, and Levene and Mauchly's tests were used to assess the homogeneity of variances. We used the parametric tests when assuming the normality of the data distribution and homogeneity of variances. We use the independent t-test and repeated measures analysis of variances tests to determine and compare the effectiveness of the drugs in the frequency, duration, and severity of the headaches in two groups during the consecutive months of study. Nonparametric Mann–Whitney U and Friedman tests were used when data is not normally distributed. Chi-square and independent t-tests were used to compare the variables in the two groups. Data were analyzed using SPSS software version 24 (IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.)
Ethical considerations
After determining potential candidates, all aspects of the study were explained to them and a written consent form was obtained from them or their parents. All patient information, including name and address, was strictly confidential. Previous studies had already shown the efficacy of each drug used in the study; therefore, the opportunity for appropriate treatment was available to all patients, and treatment of them was not postponed due to participation in the study. This study was registered in the Iranian registry of clinical trials (IRCT code: IRCT20190208042654N2). This study was approved by the ethical committee of the Isfahan University of Medical Science (Project number: IR.MUI.MED.REC.1398.239).
Results
In this study, we recruited 72 children with headaches aged 5–15 years old referring to the pediatric neurology clinic. After the migraine was diagnosed according to IHS criteria, they entered the study and followed up in terms of frequency, duration, and severity of headaches in each of the amitriptyline and coenzyme Q10 groups.
Demographic characteristics
The mean age of recruited children was 9.07 ± 2.81 (Mean ± SD) and the mean number of years which they already suffered headaches was 1.58 ± 1.25 years. There are 25 and 21 boys in amitriptyline and coenzyme Q10 groups, respectively. There is no significant difference in age, gender, and history of headaches between the two groups [Table 1].
Table 1.
Characteristics of children with diagnose of migraine headaches participating in the study (n=72)
| Variable | Amitriptyline (control) (n=36) | Co-enzyme Q10 (case) (n=36) | P |
|---|---|---|---|
| Age (years) | 9.56±2.76 | 8.58±2.82 | 0.144 |
| Years with a history of headaches (years) | 1.67±1.6 | 1.5±0.77 | 0.356* |
| Gender, n (%) | |||
| Boys | 25 (34) | 21 (29) | 0.326 |
| Girls | 11 (15) | 15 (21) |
*Mann-Whitney U test was used
Headaches frequency
Assessing the frequency of headaches showed that there is a significant reduction in the frequency of headaches in two groups (Freidman test, P < 0.001). Although the frequency of headaches before treatment was not significantly different from each other in the two groups, 1 month after treatment, there was a significant difference with lower amounts in the control group (P < 0.001) [Table 2]. However, the two groups were not significantly different in the following months (P = 0.101 and 0.288), and therefore, two drugs showed equal efficacy in 3 months in terms of headaches frequency. Figure 1 shows the changes in the frequency of headaches in two groups assessed on monthly visits [Figure 1].
Table 2.
Changes in frequency, duration, severity and pediatric migraine disability assessment score in two groups in time and comparison between two groups
| Variable | mean±SD | P | |
|---|---|---|---|
|
| |||
| Amitriptyline (control) | Co-enzyme Q10 (case) | ||
| Headaches frequency (headaches/month) | |||
| Before treatment | 15.53±11.390 | 8.75±4.795 | 0.104**** |
| 1 month after treatment | 2.53±1.748 | 8±15.975 | <0.001**** |
| 2 months after treatment | 2.94±3.144 | 3.28±2.337 | 0.101**** |
| 3 months after treatment | 2.28±3.309 | 2.47±2.311 | 0.288**** |
| P* | <0.001 | <0.001 | |
| Headaches duration (total hours/affected day) | |||
| Before treatment | 6.806±8.116 | 4.889±3.284 | 0.193*** |
| 1 month after treatment | 1.208±1.921 | 3.667±2.097 | <0.001*** |
| 2 months after treatment | 2.647±11.897 | 2.611±2.046 | 0.986*** |
| 3 months after treatment | 1.847±7.927 | 2.139±1.944 | 0.831*** |
| P* | <0.001 | <0.001 | |
| Headaches severity (Scale from 0 to 10) | |||
| Before treatment | 8.11±1.737 | 6.61±1.573 | <0.001**** |
| 1 month after treatment | 4.58±1.697 | 5.36±1.222 | 0.025**** |
| 2 months after treatment | 4.08±1.5 | 4.11±1.968 | 0.567**** |
| 3 months after treatment | 2.78±2.126 | 3.31±2.4 | 0.244**** |
| P* | <0.001 | <0.001 | |
| PedMIDAS score | |||
| Before treatment | 51.03±28.464 | 20±8.915 | <0.001**** |
| 3 months after treatment | 12.78±22.391 | 7.14±5.394 | 0.153**** |
| P** | <0.001 | <0.001 | |
*Friedman test was used, **Dependent t-test was used, ***Independent t-test was used, ****Man-Whitney U test was used, *****Data are shown in mean±SD format. SD: Standard deviation, PedMIDAS; Pediatric migraine disability assessment
Figure 1.
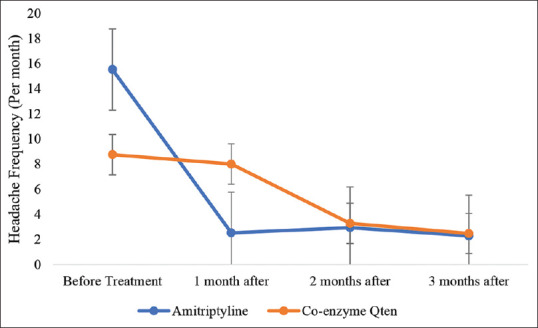
Changes in the frequency of headaches in two groups assessed on monthly visits
Headaches duration
Evaluation of headaches duration showed that two drugs effectively lowered the duration of headaches. Duration of headaches was similar between the two groups before treatment (P = 0.193). Although the trend of changes in time was similar to changes for headache frequency. Patients in the amitriptyline group showed less duration than the other group at 1 month after starting treatment (P < 0.001). However, in the following month, there was not any significant difference between the two groups (P = 0.986 and 0.931), suggesting the equal efficacy of two drugs in lowering the duration of headaches in 3 months. Figure 2 shows the changes in the duration of headaches in two groups assessed on monthly visits [Figure 2].
Figure 2.
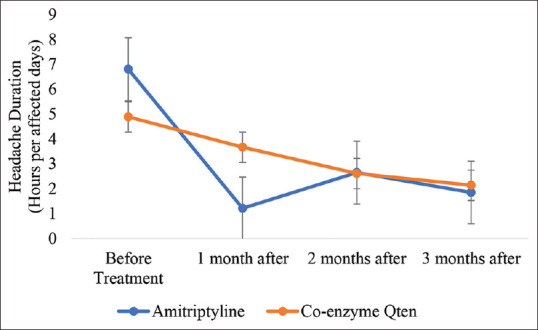
Changes in the duration of headaches in two groups assessed on monthly visits
Headaches severity
Assessing the severity of headaches in the progression of time showed that two drugs made a significant reduction in the severity of headaches. Two groups were significantly different before starting treatment with less severe headaches in the Co-enzyme Q10 group (P < 0.001). However, this comparison became vice versa in 1 month after treatment, with significantly more severe headaches in the Co-enzyme Q10 group (P = 0.025). Although, in the following months, there was no significant difference between the two groups (P = 0.567 and 0.244). Figure 3 shows the changes in the severity of headaches in two groups assessed on monthly visits [Figure 3].
Figure 3.
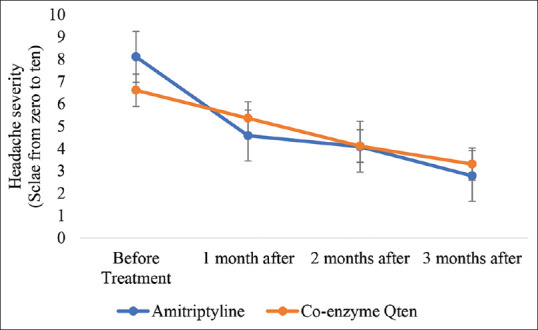
Changes in the severity of headaches in two groups assessed on monthly visits
PedMIDAS disability scoring
Assessing the patients’ QoL before treatment and 3 months after starting treatment showed that in either group, QoL was significantly improved. Children in the amitriptyline group have a lower QoL before starting the treatment (higher PedMIDAS disability grade: severe in amitriptyline group versus mild in coenzyme Q10 group) (P < 0.001). However, comparing two groups showed that there was no significant difference between the two groups 3 months after treatment (P = 0.153) [Figure 4].
Figure 4.
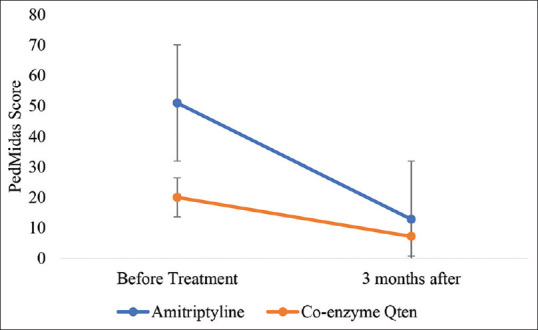
Changes in quality of life (PedMIDAS score) in two groups assessed before and after treatment (Higher score means lower quality of life)
Monitoring drug side effects in two groups showed four children showed drowsiness in the amitriptyline group, and one child showed belly pain in the Co-enzyme Q10 group.
Discussion
This Randomized clinical trial showed that Co-enzyme Q10 might be effective in lowering the frequency, duration, severity of migraine attacks, and ultimately improve patients’ QoL. Other studies supported the effectiveness of this substance on the frequency and severity of children and adults with migraine headaches. In 2019, Hajihashemi et al.[20] assessed the effect of coenzyme Q10 and L-carnitine supplementation on different aspects of migraine headaches in 20–40 years old patients with migraine. They demonstrated a significant reduction in severity, duration, frequency of migraine headaches. Another recent study on the effect of Q10 supplementation on 45 nonmenopausal women aged 18–50 years with migraine showed favorable reduction in frequency, severity, and duration of migraine attacks compared to placebo.[21] In 2015, Dalla Volta et al., studying 40 adults with migraines aged between 18 and 65 years, showed that administering Co-enzyme Q10 results in a decrease in frequency and severity of almost half of the patients’ headaches for more than 50%.[18] In another study, using coenzyme Q10 supplementation, even in patients with normal levels of it, significantly lower the frequency of migraine attacks.[16,22] Studying coenzyme Q10 in children is much more limited. Hershey et al. showed that coenzyme Q10 supplementation for 3 months, in coenzyme Q10 deficient children, would result in much lower migraine headaches frequency.[23] Another randomized clinical trial reported similar results and demonstrated that if coenzyme Q10 supplementation discontinues, migraine headaches may exacerbate again.
In line with other studies, in this study, we found significant effects of amitriptyline lowering the frequency, duration, and severity of migraine headaches. Amitriptyline has been studied for many years and is one of the most suggested drugs for the prevention and treatment of migraine headaches. It has shown that even low-dose amitriptyline would work for almost everyone in controlling migraine attacks.[8] A randomized clinical trial study in 2018 in Iran evaluating the efficacy of amitriptyline on the pediatric population, showed that this drug significantly prevents migraine headaches. However, it has more side effects in comparison with other drugs such as melatonin.[24] Reported side effects for amitriptyline include mouth dryness, constipation, increased appetites, drowsiness, and prolonged QT interval.
Recently, studies for finding other drugs with minimal side effects and at the same time, reasonable therapeutic effects became more interesting. Hershey et al. studied the therapeutic effects of gradually increasing doses of amitriptyline against its side effects, while in another study, compared it with Topiramate, another drug with potentially good results in childhood migraines. In this study, we found comparable effects of coenzyme Q10 with amitriptyline. We should note that amitriptyline has a greater effect than coenzyme Q10 in the short term, especially in terms of duration and frequency of migraine headaches. However, when it comes to a more prolonged effect (e.g., 3 months here), their effects were almost similar.
Similarly, the effect of coenzyme Q10 on improving QoL was acceptable in comparison with amitriptyline. Although the two groups have different quality of life before the treatment, the ultimate quality of life was statistically similar to each other. It seems that coenzyme Q10 could be an adequate substitute for amitriptyline in controlling migraine attacks.
In this study, in the dosage of 1–2 mg/kg, four children showed drowsiness in the control group, which in comparison to one individual with stomachache occurred for coenzyme Q10 in the dosage of 30–60 mg (approximately 1–2 mg/kg), showed more unwanted effects. Furthermore, in general, reported side effects for coenzyme Q10 are minimal, including nausea and diarrhea.[10]
Conclusions
According to results, Co-enzyme Q10, with fewer side effects and comparable therapeutic effects, especially in the long term, could be a good drug for prophylactic treatment of migraine headaches and a potential one for substituting amitriptyline, a widely accepted drug. However, future prospective studies with larger samples would be needed to strengthen this evidence.
Authors contributions
OY, NH, and VM contributed in the study concept, statistical analysis, drafting, and editing the manuscript. OY, MMS, JN and NH contributed in the study design, data collection, and editing the manuscript. NH and TM contributed in conducting the study, and editing the manuscript.
Financial support and sponsorship
This work was supported by Isfahan University of Medical Sciences (grant number: 398286).
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We should thank the pediatric neurology department for their support and every patient and their family for their patience. This clinical trial has been submitted in the Iranian Registry of Clinical Trials (IRCT code: IRCT20190208042654N2).
References
- 1.Ashrafi MR, Salehi S, Malamiri RA, Heidari M, Hosseini SA, Samiei M, et al. Efficacy and safety of cinnarizine in the prophylaxis of migraine in children: A double-blind placebo-controlled randomized trial. Pediatr Neurol. 2014;51:503–8. doi: 10.1016/j.pediatrneurol.2014.05.031. [DOI] [PubMed] [Google Scholar]
- 2.Green A, Kabbouche M, Kacperski J, Hershey A, O’Brien H. Managing migraine headaches in children and adolescents. Expert Rev Clin Pharmacol. 2016;9:477–82. doi: 10.1586/17512433.2016.1135050. [DOI] [PubMed] [Google Scholar]
- 3.Kabbouche MA, Kacperski J, O’Brien HL, Powers SW, Hershey AD. Headache in Children and Adolescents. In: Swaiman KF, Ashwal S, Ferriero DM, Schor NF, Finkel RS, Gropman AL, et al., editors. Swaiman’s Pediatric Neurology. Edinburgh: Elsevier Saunders: Elsevier; 2017. pp. 647–55. [Google Scholar]
- 4.Kacperski J, Kabbouche MA, O’Brien HL, Weberding JL. The optimal management of headaches in children and adolescents. Ther Adv Neurol Disord. 2016;9:53–68. doi: 10.1177/1756285615616586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kliegman RM, Stanton B, Geme JW, Schor NF, Behrman RE. Philadelphia, PA: Elsevier; 2016. Nelson Textbook of Pediatrics. [Google Scholar]
- 6.Piña-Garza JE, Fenichel GM. Philadelphia, PA: Elsevier.: Elsevier Saunders; 2013. Fenichel’s Clinical Pediatric Neurology: A Signs and Symptoms Approach. [Google Scholar]
- 7.Sabri MR, Dehghan B, Yaghini O, Nasiri J, Mansourian M, Khalifehsoltani S. Endothelial dysfunction state in migraine headache and neutrally mediated syncope in children and young adults. J Res Med Sci. 2015;20:771–6. doi: 10.4103/1735-1995.168384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Teleanu RI, Vladacenco O, Teleanu DM, Epure DA. Treatment of pediatric migraine: A review. Maedica (Bucur) 2016;11:136–43. [PMC free article] [PubMed] [Google Scholar]
- 9.Yaghini O, Shahkarami SM, Mahmoudian T, Hashemi EH. Comprehensive assessment of the relative frequency of sleep disorders in migraine and non migraine in 6 to 14-year-old children. Iran J Child Neurol. 2011;4:33–6. [Google Scholar]
- 10.Schwedt TJ. Preventive Therapy of Migraine. Continuum (Minneap Minn) 2018;24:1052–65. doi: 10.1212/CON.0000000000000635. (4, Headache) [DOI] [PubMed] [Google Scholar]
- 11.Orr SL, Venkateswaran S. Nutraceuticals in the prophylaxis of pediatric migraine: Evidence-based review and recommendations. Cephalalgia. 2014;34:568–83. doi: 10.1177/0333102413519512. [DOI] [PubMed] [Google Scholar]
- 12.Orr SL. The evidence for the role of nutraceuticals in the management of pediatric migraine: A review. Curr Pain Headache Rep. 2018;22:37. doi: 10.1007/s11916-018-0692-6. [DOI] [PubMed] [Google Scholar]
- 13.Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders. Cephalalgia. (3rd edition) 2018;38:1–211. doi: 10.1177/0333102417738202. [DOI] [PubMed] [Google Scholar]
- 14.Topcu Y, Hiz Kurul S, Bayram E, Sozmen K, Yis U. The paediatric migraine disability assessment score is a useful tool for evaluating prophylactic migraine treatment. Acta Paediatr. 2014;103:e484–9. doi: 10.1111/apa.12752. [DOI] [PubMed] [Google Scholar]
- 15.Sadeghian H, Motiei-Langroudi R. Comparison of levetiracetam and sodium valproate in migraine prophylaxis: A randomized placebo-controlled study. Ann Indian Acad Neurol. 2015;18:45–8. doi: 10.4103/0972-2327.144290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sándor PS, Di Clemente L, Coppola G, Saenger U, Fumal A, Magis D, et al. Efficacy of coenzyme Q10 in migraine prophylaxis: A randomized controlled trial. Neurology. 2005;64:713–5. doi: 10.1212/01.WNL.0000151975.03598.ED. [DOI] [PubMed] [Google Scholar]
- 17.Slater SK, Nelson TD, Kabbouche MA, LeCates SL, Horn P, Segers A, et al. A randomized, double-blinded, placebo-controlled, crossover, add-on study of CoEnzyme Q10 in the prevention of pediatric and adolescent migraine. Cephalalgia. 2011;31:897–905. doi: 10.1177/0333102411406755. [DOI] [PubMed] [Google Scholar]
- 18.Dalla Volta G, Carli D, Zavarise P, Ngonga G, Vollaro S. P026.Pilot study on the use of coenzyme Q10 in a group of patients with episodic migraine without aura. J Headache Pain. 2015;16:A186. doi: 10.1186/1129-2377-16-S1-A186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tonekaboni SH, Ghazavi A, Fayyazi A, Khajeh A, Taghdiri MM, Abdollah Gorji F, et al. Prophylaxis of childhood migraine: Topiramate versus propranolol. Iran J Child Neurol. 2013;7:9–14. [PMC free article] [PubMed] [Google Scholar]
- 20.Hajihashemi P, Askari G, Khorvash F, Reza Maracy M, Nourian M. The effects of concurrent Coenzyme Q10, L-carnitine supplementation in migraine prophylaxis: A randomized, placebo-controlled, double-blind trial. Cephalalgia. 2019;39:648–54. doi: 10.1177/0333102418821661. [DOI] [PubMed] [Google Scholar]
- 21.Dahri M, Tarighat-Esfanjani A, Asghari-Jafarabadi M, Hashemilar M. Oral coenzyme Q10 supplementation in patients with migraine: Effects on clinical features and inflammatory markers. Nutr Neurosci. 2019;22:607–15. doi: 10.1080/1028415X.2017.1421039. [DOI] [PubMed] [Google Scholar]
- 22.Guilbot A, Bangratz M, Ait Abdellah S, Lucas C. A combination of coenzyme Q10, feverfew and magnesium for migraine prophylaxis: A prospective observational study. BMC Complement Altern Med. 2017;17:433. doi: 10.1186/s12906-017-1933-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hershey AD, Powers SW, Vockell AL, Lecates SL, Ellinor PL, Segers A, et al. Coenzyme Q10 deficiency and response to supplementation in pediatric and adolescent migraine. Headache. 2007;47:73–80. doi: 10.1111/j.1526-4610.2007.00652.x. [DOI] [PubMed] [Google Scholar]
- 24.Fallah R, Fazelishoroki F, Sekhavat L. A randomized clinical trial comparing the efficacy of melatonin and amitriptyline in migraine prophylaxis of children. Iran J Child Neurol. 2018;12:47–54. [PMC free article] [PubMed] [Google Scholar]