

Abstract
Objective
Brain arteriovenous malformations (AVM) are commonly treated with endovascular embolization. Due to the rapid evolution of endovascular technology and lack of consistent practice guidelines regarding AVM embolization, further study of AVM embolization outcomes is warranted.
Methods
We conducted a retrospective review of AVMs embolized at a single center from 2002-2019. Patient demographics, AVM characteristics, intention of embolization, and angiographic and clinical outcome after embolization were recorded. We compared the embolization results of those treated with n-butyl cyanoacrylate (n-BCA) and Onyx.
Results
Over an 18-year period at our institution, 30 (33%) of 92 AVMs were treated with embolization. n-BCA was used in 12 cases and Onyx in 18 cases. Eighty-seven pedicles were embolized over 47 embolization sessions. Fifty percent of AVMs treated with n-BCA underwent more than one embolization session compared to 22% when Onyx was used. The median total percent volume reduction in the n-BCA AVMs was 52% compared to 51% in Onyx AVMs. There were 2 periprocedural complications in the n-BCA cohort and none in the Onyx cohort.
Conclusions
In this small retrospective series, Onyx and n-BCA achieved similar occlusion results, although n-BCA required more sessions and pedicles embolized to do so.
Keywords: Arteriovenous malformation, Embolization, n-butyl cyanacrylate (n-BCA), Ethylene vinyl alcohol copolymer, Onyx
INTRODUCTION
Brain arteriovenous malformations (AVM) are connections between cerebral arteries and veins by way of an interposing nidus. AVMs may become symptomatic by hemorrhage, seizure, headache, or cause focal neurological deficits without evidence of hemorrhage. Treatment modalities for AVMs are aimed at their angiographic eradication. This is accomplished by sole implementation or a combination of microsurgery, radiation therapy, and embolization [24].
Embolization involves endovascular administration of materials into feeding arteries, the nidus, and/or draining veins. The embolic material of choice has evolved from polyvinyl alcohol particles to cyanoacrylate liquid embolic agents including n-butyl cyanoacrylate (n-BCA), (Trufill, Johnson and Johnson, New Brunswick, NJ, USA) to ethylene vinyl alcohol copolymer liquid embolic (Onyx, Medtronic, Minneapolis, MN, USA) [16,18]. The goal of embolization can be categorized as curative, adjuvant (pre-surgical, pre-radiosurgery), targeted (e.g. occluding a ruptured perinidal aneurysm), or palliative (e.g. reducing flow in patients with cerebral ischemia due to vascular steal).
Metrics for successful embolization vary based on the initial goal of embolization [22]. For curative treatment, the metric is permanent angiographic eradication of the lesion. For adjuvant and palliative treatment, the most accepted metric is a percentage reduction of AVM volume [25]. Contrarily, a successful targeted embolization may only occlude a perinidal aneurysm or ruptured portion of the nidus with less focus on reducing the volume of the nidus [2].
Due to the rarity of AVMs, heterogeneity in endovascular technique, and rapid evolution of endovascular technology, consistent practices regarding AVM embolization have been hard to define [4,6,11,13,22,25,26]. Retrospective analysis of AVM embolization results remains invaluable to our development of safe and effective embolization practices. In this study, we retrospectively evaluate the AVM embolization experience at a single center over 18 years with specific focus on the goals of intervention, embolic agent used (n-BCA vs Onyx), and AVM volume reduction.
METHODS
The Loyola Health electronic health records were accessed to obtain adult patients who were diagnosed with brain AVMs from the date imaging was still available within our electronic medical records (2002-2019). Loyola University Medical Center electronic medical record was queried for ICD-9 (747.81) and ICD-10 (Q28.2 and Q28.3) codes corresponding to vascular malformations and CPT codes for AVM treatment (61680, 61682, 61684, 61686, 61690, and 61692). Individual patient charts were then reviewed to confirm an AVM diagnosis by angiographic or pathologic criteria. Patients with insufficient information in their medical record regarding their AVM diagnosis were excluded. Only patients who received an embolization treatment with reviewable angiograms were selected. Interventions were provided by 1 interventional neurologists, 3 interventional neuroradiologists, and 4 endovascular neurosurgeons over this time period. Over the 18-year period from 2002-2019, 92 AVMs were treated by surgery, radiosurgery, embolization, or a combination of these modalities at our institution. In this cohort, 30 AVM patients were treated with embolization as either a primary or adjunctive method and were included in the study.
Variables extracted from the medical record included patient demographics of age at diagnosis, sex, and race. Presentations were recorded as hemorrhage, headache, seizure, incidental, and other (including focal neurological deficit without hemorrhage). AVM characteristics included nidus appearance (diffuse versus compact), eloquence, deep venous drainage, size, location (cerebellar, deep cerebral, frontal, temporal, and parieto-occipital), nidal volume, AVM rupture status, eloquence, and Spetzler-Martin grade. Embolization variables including embolic agent, number of sessions, numbers of arterial pedicles treated, relative volume of AVM embolized ([pre-embolization AVM volume – post-embolization AVM volume]/[pre-embolization AVM volume]), embolization 30-day complication outcomes, and status of cure were collected through a comprehensive chart review [3]. The volume of the AVM was calculated with (A+B+C)/2 methodology. The height and width of the AVM was taken from the anteroposterior (AP) angiogram and the depth was measured from the orthogonal lateral angiogram on the baseline and post-treatment studies [8,15,19,21]. Successful embolization was defined as ≥50% devascularization after the final embolization [16]. Complications were categorized into three groups of minor (transient or non-disabling fixed deficit), major (disabling non-fatal), and death. AVMs embolized for cure were only defined as cured if a delayed (>6 months) angiogram confirmed angiographic eradication [14].
The intention of treatment was categorized based on retrospective review on the interventionalists’ clinical and procedural notes into 5 categories: curative, palliative, pre-radiotherapy, pre-surgical, or targeted. The latter 4 categories were then combined to make a non-curative embolization cohort. Embolization outcomes based on intention of treatment was evaluated.
Statistical analysis
Patient and AVM characteristics for normally distributed continuous variables are presented as means with standard deviations. Continuous variables that are not normally distributed are presented as medians and interquartile ranges. Categorical variables are presented as counts and proportions. Spearman rank correlation statistics were used to estimate the relationship between continuous variables of interest. Student t-tests were used to test the associations of continuous variables. Chi-square test or Fisher’s exact test were used to test the associations of categorical variables. All analyses were performed with SAS 9.4 (Cary, NC, USA) and two-sided p-value <0.05 were deemed statistically significant.
RESULTS
Over an 18-year period, 30 AVMs were embolized at our institution. Patient and AVM characteristics are listed in Table 1. The average age at diagnosis was 36±16 years, and 17 patients (57%) were male. Fifteen (50%) of the AVMs were Spetzler Martin (SM) Grade 1-2, 9 (30%) were SM Grade 3, and 6 (20%) were SM Grade 4-5. The AVM locations was cerebellar (10%), frontal (43%), temporal (10%), and parieto-occipital (30%). AVMs presented with hemorrhage, seizure, headache, neurological deficit without hemorrhage, and other in 6 (20%), 6 (20%), 12 (40%), 2 (6.7%), and 4 (17%) cases, respectively.
Table 1.
Patient, AVM, and treatment demographics
| All patients, n (%): N=30 | ||
|---|---|---|
| n-BCA group | Onyx group | |
| n=12 | n=18 | |
| Patient characteristics | ||
| Age, yr | ||
| Mean±SD | 35±17 | 37±17 |
| Sex | ||
| Male | 8 (67) | 9 (50) |
| Race/ethnicity | ||
| White | 7 (58) | 7 (39) |
| Presenting symptom | ||
| Hemorrhage | 2 (17) | 4 (22) |
| Seizure | 1 (9) | 5 (28) |
| Headache | 7 (58) | 5 (28) |
| Neurological deficit | 1 (9) | 1 (6) |
| Other/Incidental | 1 (9) | 3 (17) |
| AVM characteristics | ||
| Diffuse nidus | ||
| Yes | 1 (9) | 1 (6) |
| Eloquent area | ||
| Yes | 10 (83) | 8 (44) |
| Deep venous drainage | ||
| Yes | 7 (58) | 4 (22) |
| Nidal aneurysm | ||
| Yes | 3 (27) | 3 (17) |
| Ruptured | ||
| Yes | 4 (67) | 8 (44) |
| Size | ||
| <3 | 6 (50) | 8 (44) |
| 3–6 | 6 (50) | 8 (44) |
| >6 | 0 (0) | 2 (11) |
| Location | ||
| Cerebellar | 1 (10) | 2 (11) |
| Frontal | 5 (50) | 8 (44) |
| Temporal | 1 (10) | 2 (11) |
| Parieto-occipital | 3 (30) | 6 (33) |
| Spetzler-Martin grade | ||
| Grade 1 | 0 (0) | 6 (33) |
| Grade 2 | 4 (33) | 5 (28) |
| Grade 3 | 5 (42) | 4 (22) |
| Grade 4 | 3 (25) | 1 (6) |
| Grade 5 | 0 (0) | 2 (11) |
| Number of arterial feeders | ||
| Median | 2 | 2 |
| Treatment characteristics | ||
| Modality of treatment | ||
| Embolization alone | 4 (33) | 4 (22) |
| Embolization+surgery | 4 (33) | 8 (44) |
| Embolization+SRS | 4 (33) | 5 (28) |
| Embolization+surgery+SRS | 0 (0) | 1 (5.6) |
| Objective of embolization | ||
| Curative | 4 (33) | 2 (11) |
| Non-curative: palliative | 1 (8.3) | 0 (0) |
| Non-curative: targeted | 2 (17) | 3 (17) |
| Non-curative: pre-surgery | 3 (25) | 9 (50) |
| Non-curative: pre-SRS | 2 (17) | 4 (22) |
Note: Summary of the treatment modalities, AVM characteristics, and patient demographics of all 30 patients included in this study.
AVM, arteriovenous malformations; n-BCA, n-butyl cyanoacrylate; SRS, stereotactic radiosurgery
These 30 patients underwent 47 embolization sessions (median 1, interquartile range (IQR) 1-2 sessions per patient) and had 87 pedicles embolized (median 2 IQR 1-2.3 pedicles per session and median 2 IQR 2-3 pedicles embolized per patient). The embolic agent used was n-BCA in 12 (40%) patients and 42 (48%) of the pedicles treated and Onyx in 18 (60%) patients and 45 (52%) of the pedicles treated. There were no complications associated with AVMs embolized with Onyx, and one minor complication (quadrantanopia) and one major complication (anterior choroidal artery stroke) were associated with the AVMs embolized with n-BCA. The overall complications rate was 6.7% per AVM, 4.3% per session, and 2.3% pedicle. Ultimately, 8 patients (27%) only had embolization, 12 patients (40%) had surgery in addition to embolization, 9 patients (30%) had radiosurgery in addition to embolization, and 1 patient (3%) had all three modalities of treatment (Table 1). Clinical follow-up for these patients was 39 months±42 months. Angiographic follow-up for these patients was 19 months±26 months.
The median size of the AVMs treated with n-BCA was 3.5 mL (IQR 1.1-9.9 mL) compared to 4.4 mL (IQR 1.9-11 mL) in those that were embolized with Onyx. The median total percent volume reduction (percent devascularization) in the AVMs that were embolized with n-BCA was 52% (IQR 31-67%) compared to 51% (IQR 27-86%) in those that were embolized with Onyx (Table 2). Successful embolization (≥50% devascularization) occurred in 58% of n-BCA embolized versus 56% of Onyx embolized AVMs (Fig. 1). After the initial embolization, n-BCA AVMs had a median percent devascularization of 30% (IQR 0-52) compared to 43% (IQR 15-86) in the Onyx AVMs. The total number of pedicles embolized in the first embolization was 1.8 per patient in n-BCA AVMs compared to 2.2 per patient in the Onyx AVMs. Six (50%) of n-BCA embolized AVMs underwent more than one embolization session compared to 4 (22%) of the Onyx AVMs (Table 2).
Table 2.
Angiographic outcomes and embolization complications
| All patients, n (%): N=30 | ||
|---|---|---|
| Angiographic outcomes | n-BCA group | Onyx group |
| n=12 | n=18 | |
| Initial volume, mL | ||
| Median (Q1, Q3) | 3.5 (1.1, 9.9) | 4.3 (1.9, 11) |
| Total % devascularization | ||
| Median (Q1, Q3) | 52 (31, 67) | 51 (27, 86) |
| <25%, n (%) | 2 (17) | 3 (17) |
| 25-49% | 3 (25) | 5 (28) |
| 50-75% | 5 (42) | 4 (22) |
| 75-99% | 1 (8) | 5 (28) |
| >99% | 1 (8) | 1 (5) |
| Need for >1 embolization | ||
| Yes, n (%) | 6 (50) | 4 (22) |
| Total number of sessions | ||
| n | 22 | 25 |
| Number of sessions per person | ||
| Mean±SD | 1.8±1.0 | 1.4±0.8 |
| Total number of pedicles | ||
| n | 42 | 45 |
| Number of pedicles per person | ||
| Mean±SD | 3.5±1.9 | 2.6±2.0 |
| Number of pedicles per session | ||
| Mean±SD | 2.1±0.9 | 1.9±1.1 |
| % devascularization per pedicle | ||
| Mean±SD | 16±14 | 34±29 |
| % devascularization by objective | Both groups:Mean±S``D | n=30 |
| Curative (n=6) | 61±34 | |
| Non-Curative: Palliative (n=1) | 79±N/A | |
| Non-Curative: Targeted (n=5) | 48±19 | |
| Non-Curative: Pre-surgery (n=12) | 47±29 | |
| Non-Curative: Pre-SRS (n=6) | 54±36 | |
| Complications, n (%) | n-BCA group | Onyx group |
| n=12 | n=18 | |
| Minor | 1 (8.3) | 0 (0) |
| Major | 1 (8.3) | 0 (0) |
| Mortality | 0 (0) | 0 (0) |
| Total | 2 (17) | 0 (0) |
Note: Summary of the embolization objectives, angiographic changes, and complication rates associated with embolization treatments.
n-BCA, n-butyl cyanoacrylate; SRS, stereotactic radiosurgery
Fig. 1.
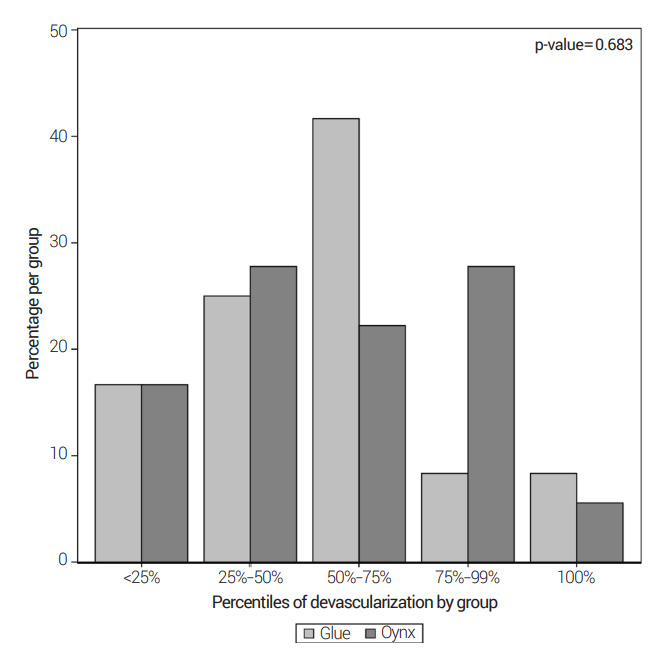
Bar plot demonstrating the distribution of embolization sessions based on percent devascularization, in 25% increment bins, for n-BCA and Onyx groups. n-BCA, n-butyl cyanoacrylate
The total number of sessions per person was 1.8±1.0 in n-BCA and 1.4±0.8 in Onyx. The total number of pedicles per session was 2.1±0.9 in n-BCA and 1.9±1.1 in Onyx. The percent devascularization per pedicle was 16% ±14 in n-BCA and 34% ±29 in Onyx with a p-value of 0.032 (Fig. 2). Additionally, the correlation of percent devascularization with initial AVM volume and number of pedicles are presented in Fig. 3 and 4 respectively. Lastly, the percent devascularization based on the objective of embolization was 61% ±34 in cure attempt, 79% in palliative, 54% ±36 in targeted, 47% ±29 in pre-surgery, and 48% ±19 in pre-radiosurgery (Table 2). This further summarizes into 61% ±34 in the cure attempt group versus 50% ±28 in the non-curative group.
Fig. 2.
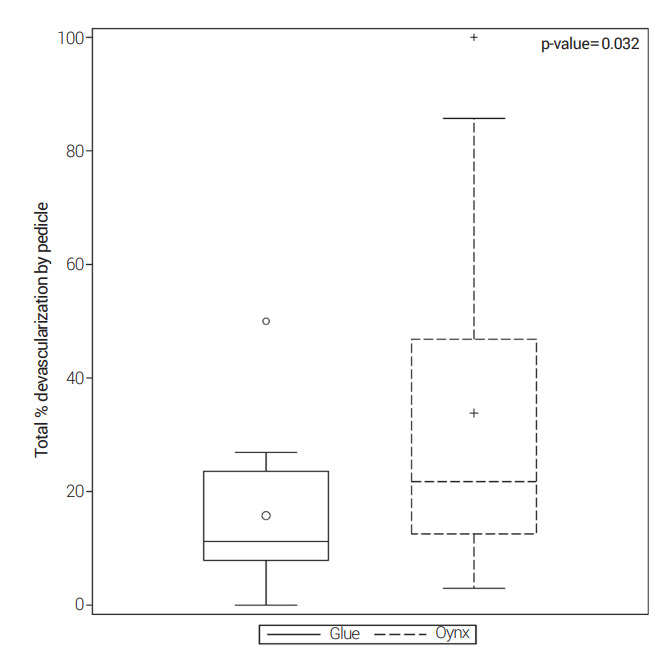
Boxplot graph comparing the percent devascularization per pedicle between n-BCA and Onyx. n-BCA, n-butyl cyanoacrylate
Fig. 3.
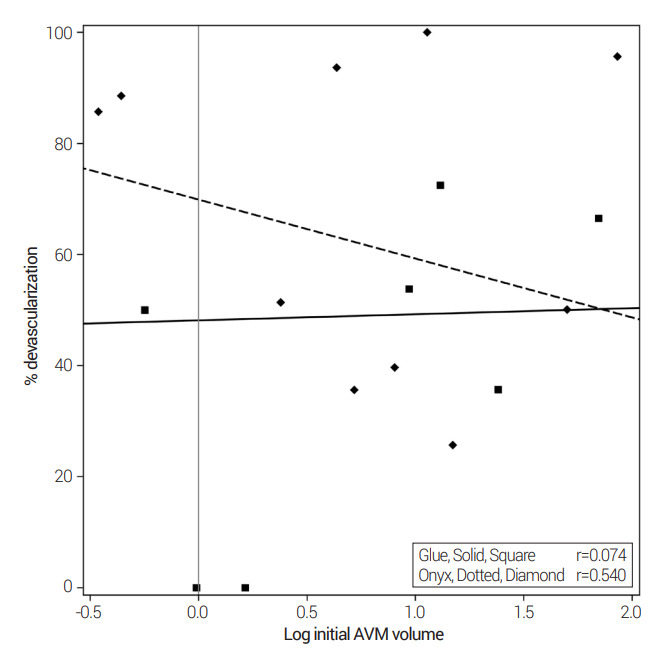
Demonstrating the correlation of percent devascularization to the initial volume of the AVM in both the n-BCA and the Onyx groups. AVM, arteriovenous malformations; n-BCA, n-butyl cyanoacrylate
Fig. 4.
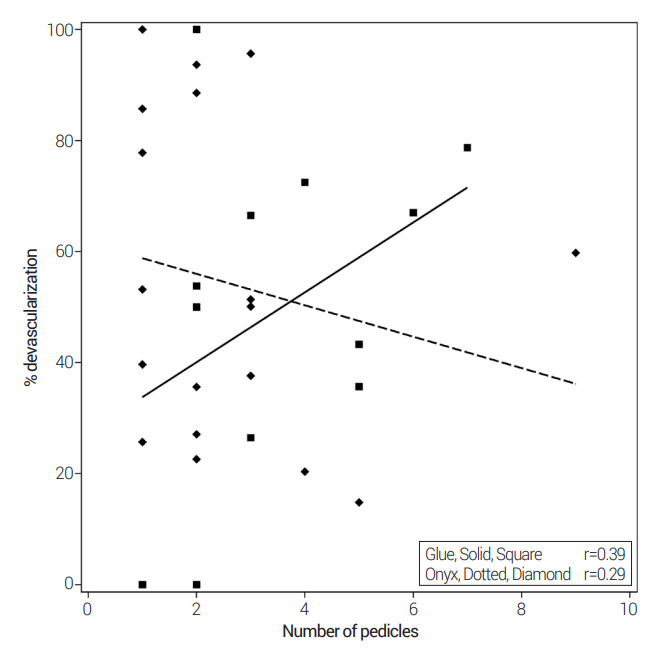
Demonstrating the correlation of percent devascularization and the number of AVM pedicles embolized in the n-BCA and Onyx groups. AVM, arteriovenous malformations; n-BCA, n-butyl cyanoacrylate
DISCUSSION
This single center retrospective analysis of AVM embolization demonstrates similar final nidal reduction results whether using n-BCA or Onyx liquid embolic agents. However, more pedicles and more sessions were required to achieve similar embolization results with n-BCA. Additionally, it does appear that even though achieving the benchmark embolization result of 50% is the same for both groups, achieving a >75% embolization result may slightly favor Onyx. Most importantly, with the caveat of including patients over a 18-year period amongst 8 interventionalists, the use of both agents appears relatively safe and effective.
Trans-arterial embolization of AVMs warrants continued study given the high complications seen in the ARUBA (a randomised trial of unruptured brain arteriovenous malformations) trial amongst AVMs receiving embolization. Of the 3 arms of intervention (microsurgery, stereotactic radiotherapy, and embolization), embolization was used the most commonly (62% of cases) and had the highest occurrence of a primary event (50% of cases) [17]. During the ARUBA enrollment years, 2007-2013, all practitioners would have had substantial experience with n-BCA and/or Onyx. Little granular data is available from the trial about the embolizations, but overall, the results were disparaging and suggests the field needs improvement.
Nidal reduction slightly favors Onyx
Onyx appears slightly superior at achieving nidal volume reduction compared to n-BCA. The industry supported randomized trial comparing Onyx to n-BCA defined the primary endpoint as achievement of 50% volumetric nidal reduction. This trial was not able to blind interventionalists since catheter selection and preparation requires knowledge of the agents and the visual and radiographic appearance are starkly different. With those caveats, Onyx achieved a 50% volume reduction in 96% cases compared to 85% of AVMs treated with n-BCA. These non-inferior results were achieved with a nearly identical number of sessions per AVM and pedicles per AVM [16].
In our study, a 50% volume reduction was less impressive, but similar between n-BCA and Onyx (58 and 56%, respectively), and a 75% volumed reduction may favor Onyx (17% vs 33%) (Fig. 1). Most importantly, n-BCA required 32% more sessions and 37% more pedicles embolized to achieve these results. In a similar single center retrospective analysis, Crowley et al. found the same occlusion results comparing n-BCA to Onyx, but conversely found that more sessions were performed and more pedicles embolized in the Onyx group [5]. Sahlein et al. reported their exclusive n-BCA experience and described a more aggressive approach of embolizing 3.4 pedicles per session and 4.4 pedicles per AVM compared to our 1.9 and 2.9, respectively. This more aggressive approach with n-BCA resulted in an 84% overall devascularization compared to our 52% [22]. Lastly, in a large meta-analysis, Elsenousi et al. found that the angiographic results trended towards Onyx over n-BCA. It is likely that results with these agents will vary by operator.
Lower complications with less aggressive embolization
All complications were infrequent in our series, and this may be a function of the less aggressive nidal reduction during embolization. Our endovascular major complication rate of 3% is at the lower end of that reported in the literature (3.8-14%) [9,10]. A cursory look at our data and the literature suggests that less aggressive embolization with less focus on trans-arterial curative intent may be a superior strategy (Fig. 5). This conservative embolization approach was recently endorsed by See et al. who observed a reduction in hemorrhagic complications with a flow reduction strategy minimizing nidal penetration with n-BCA [23]. These authors have previously reported the usefulness of non-invasive analysis of the AVM flow volume in quantifying embolization results. This method of assessing embolization is perhaps more significant than angiographic volume reduction [1].
Fig. 5.

Ruptured right parietal AVM, pre-surgical Onyx embolization. A ruptured right parietal AVM with intercranial hemorrhage and brain swelling requiring a decompressive hemicraniectomy (A). A pre-embolization right internal carotid artery angiogram with AP (B) and lateral (C) views show AVM dimensions of 1.9 cm×1.8 cm×1.1 cm with a calculated volume of 1.89 mL. Microcatheter angiography showing nidus and draining vein from the first MCA branch before onyx injection (D). Lateral right internal carotid angiogram after 1 MCA pedicle embolization showing 28% volume reduction (E). A second MCA feeding artery microcatheter angiogram with nidus and draining vein (F). The objective of this embolization was adjuvant pre-surgical. Final lateral right internal carotid artery angiogram shows a 94% volume embolization with delayed filling of the 2 embolized MCA pedicles (G) and delayed filling of the draining vein (white arrow) (H). AVM, arteriovenous malformations; AP, anteroposterior; MCA, middle cerebral artery
A trend toward higher Onyx complications rates was seen in the Onyx trial with an adverse event in 9.3% of Onyx treatments compared to 4.8% with n-BCA. The meta-analysis by Elsenousi et al. also had a non-significant trend toward higher complications with Onyx [7]. The brain arteriovenous malformations embolization with Onyx (BRAVO) trial pursued very aggressive AVM Onyx embolization with >50% occlusion occurring in 85% of cases and cures occurring in 24% of cases, but incurred a treatment-related morbidity and mortality of 5 and 4%, respectively [20]. Our data offers little on the comparison of complications between these 2 agents, but more suggestion that a less aggressive nidal occlusion may be preferential.
n-BCA vs Onyx is a matter of preference over evidence
There are numerous differences between these two agents. Most of the differences amount to a higher convenience factor for Onyx since no mixing is required, it is better optically and radiographically visualized, and the injections are slower with less requirement for split second decision making. Whether there is true benefit of Onyx over n-BCA is not settled. Some techniques combine the agents such as the pressure cooker technique in which a coil and n-BCA plug is made to better penetrate Onyx into the nidus [4]. Selection of each agent based on the lesion angioarchitecture and operator experience is likely best practice. Further analysis of these liquid embolic agents and other emerging agents with the use of better balloons and detachable tip microcatheters will be of future interest.
Limitations
There are several limitations to our study. First, it is a retrospective analysis at a relatively low volume practice over 18 years amounting to only 1.7 embolized AVMs per year treated by 8 different practitioners. Although the care is diluted over time and practitioners, this may be a truer reflection of real-world AVM embolizations. Volumetric analysis was performed by an ABC/2 analysis which is a linear assessment based on assumptions of ellipsoidal nidal morphology. Our method was identical to that used by both the Onyx Trial Investigators and n-BCA Trial Investigators [16,18]. Although it is correlative to planimetric volume analysis, it has shown inaccuracies with absolute AVM nidal volume [15,21]. Since we did a relative comparison, this method is likely satisfactory although a planimetric or 3-dimensional assessment may be been more accurate [12]. Variables that were not available but potentially relevant are the concentrations of Onyx and n-BCA. Also, since n-BCA was used in the early portion of this series (2002-2008) and Onyx in the later portion (2009-2019), other advances in imaging and endovascular devices would favor better results with Onyx. Lastly, the small sample size does limit our statistical analysis to discover small differences in the analyzed variables that may have been seen with a larger sample size.
CONCLUSIONS
Continued analysis of AVM embolization experience is needed to identify risk factors for complications and improved embolization results. In this small retrospective series, Onyx and n-BCA achieved similar occlusion results although n-BCA required more session and pedicles embolized to do so. Both agents had low complications which may be related to less aggressive embolization strategies.
Footnotes
Disclosure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
REFERENCES
- 1.Alaraj A, Amin-Hanjani S, Shakur SF, Aletich VA, Ivanov A, Carlson AP, et al. Quantitative assessment of changes in cerebral arteriovenous malformation hemodynamics after embolization. Stroke. 2015 Apr;46(4):942–7. doi: 10.1161/STROKEAHA.114.008569. [DOI] [PubMed] [Google Scholar]
- 2.Alexander MD, Hippe DS, Cooke DL, Hallam DK, Hetts SW, Kim H, et al. Targeted embolization of aneurysms associated with brain arteriovenous malformations at high risk for surgical resection: A case-control study. Neurosurgery. 2018 Mar;82(3):343–49. doi: 10.1093/neuros/nyx167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Atkinson RP, Awad IA, Batjer HH, Dowd CF, Furlan A, Giannotta SL, et al. Reporting terminology for brain arteriovenous malformation clinical and radiographic features for use in clinical trials. Stroke. 2001 Jun;32(6):1430–42. doi: 10.1161/01.str.32.6.1430. [DOI] [PubMed] [Google Scholar]
- 4.Chapot R, Stracke P, Velasco A, Nordmeyer H, Heddier M, Stauder M, et al. The pressure cooker technique for the treatment of brain AVMs. J Neuroradiol. 2014 Mar;41(1):87–91. doi: 10.1016/j.neurad.2013.10.001. [DOI] [PubMed] [Google Scholar]
- 5.Crowley RW, Ducruet AF, Kalani MY, Kim LJ, Albuquerque FC, McDougall CG. Neurological morbidity and mortality associated with the endovascular treatment of cerebral arteriovenous malformations before and during the Onyx era. J Neurosurg. 2015 Jun;122(6):1492–7. doi: 10.3171/2015.2.JNS131368. [DOI] [PubMed] [Google Scholar]
- 6.Debrun GM, Aletich V, Ausman JI, Charbel F, Dujovny M. Embolization of the nidus of brain arteriovenous malformations with n-butyl cyanoacrylate. Neurosurgery. 1997 Jan;40(1):112–20. discussion 120-1. [PubMed] [Google Scholar]
- 7.Elsenousi A, Aletich VA, Alaraj A. Neurological outcomes and cure rates of embolization of brain arteriovenous malformations with n-butyl cyanoacrylate or Onyx: a meta-analysis. J Neurointerv Surg. 2016 Mar;8(3):265–72. doi: 10.1136/neurintsurg-2014-011427. [DOI] [PubMed] [Google Scholar]
- 8.Foroni R, Gerosa M, Pasqualin A, Hoch J, Giri G, Pasoli A, et al. Shape recovery and volume calculation from biplane angiography in the stereotactic radiosurgical treatment of arteriovenous malformations. Int J Radiat Oncol Biol Phys. 1996 Jun 1;35(3):565–77. doi: 10.1016/s0360-3016(96)80020-4. [DOI] [PubMed] [Google Scholar]
- 9.Frizzel RT, Fisher WS. Cure, morbidity, and mortality associated with embolization of brain arteriovenous malformations: a review of 1246 patients in 32 series over a 35-year period. Neurosurgery. 1995 Dec;37(6):1031–9. doi: 10.1227/00006123-199512000-00001. discussion 1039. [DOI] [PubMed] [Google Scholar]
- 10.Haw CS, terBrugge K, Willinsky R, Tomlinson G. Complications of embolization of arteriovenous malformations of the brain. J Neurosurg. 2006 Feb;104(2):226–32. doi: 10.3171/jns.2006.104.2.226. [DOI] [PubMed] [Google Scholar]
- 11.Heidenreich JO, Hartlieb S, Stendel R, Schlattmann P, Wolf K-J, Schilling AM. Bleeding complications after endovascular therapy of cerebral arteriovenous malformations. AJNR Am J Neuroradiol. 2006 Feb;27(2):313–6. [PMC free article] [PubMed] [Google Scholar]
- 12.Imbesi SG, Knox K, Kerber CW. Reproducibility analysis of a new objective method for measuring arteriovenous malformation nidus size at angiography. AJNR Am J Neuroradiol. 2002 Mar;23(3):412–5. [PMC free article] [PubMed] [Google Scholar]
- 13.Jayaraman MV, Marcellus ML, Hamilton S, Do HM, Campbell D, Chang SD, et al. Neurologic complications of arteriovenous malformation embolization using liquid embolic agents. AJNR Am J Neuroradiol. 2008 Feb;29(2):242–6. doi: 10.3174/ajnr.A0793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jayaraman MV, Meyers PM, Derdeyn CP, Fraser JF, Hirsch JA, Hussain MS, et al. Reporting standards for angiographic evaluation and endovascular treatment of cerebral arteriovenous malformations. J Neurointerv Surg. 2012 Sep;4(5):325–30. doi: 10.1136/neurintsurg-2011-010173. [DOI] [PubMed] [Google Scholar]
- 15.Kashanian A, Sparks H, Kaprealian T, Pouratian N. Assessing the volume of large cerebral arteriovenous malformations: Can the ABC/2 formula reliably predict true volume? J Clin Neurosci. 2019 Jul;65:1–5. doi: 10.1016/j.jocn.2019.04.038. [DOI] [PubMed] [Google Scholar]
- 16.Loh Y, Duckwiler GR. Onyx Trial Investigators. A prospective, multicenter, randomized trial of the Onyx liquid embolic system and N-butyl cyanoacrylate embolization of cerebral arteriovenous malformations. Clinical article. J Neurosurg. 2010 Oct;113(4):733–41. doi: 10.3171/2010.3.JNS09370. [DOI] [PubMed] [Google Scholar]
- 17.Mohr JP, Overbey JR, Hartmann A, von Kummer R, Salman RA, Kim H, et al. Medical management with interventional therapy versus medical management alone for unruptured brain arteriovenous malformations (ARUBA): final follow-up of a multicentre, non-blinded, randomised controlled trial. Lancet Neurol. 2020 Jul;19(7):573–81. doi: 10.1016/S1474-4422(20)30181-2. [DOI] [PubMed] [Google Scholar]
- 18.n-BCA Trail Investigators N-butyl cyanoacrylate embolization of cerebral arteriovenous malformations: results of a prospective, randomized, multi-center trial. AJNR Am J Neuroradiol. 2002 May;23(5):748–55. [PMC free article] [PubMed] [Google Scholar]
- 19.Pasqualin A, Barone G, Cioffi F, Rosta L, Scienza R, Da Pian R. The relevance of anatomic and hemodynamic factors to a classification of cerebral arteriovenous malformations. Neurosurgery. 1991 Mar;28(3):370–9. doi: 10.1097/00006123-199103000-00006. [DOI] [PubMed] [Google Scholar]
- 20.Pierot L, Cognard C, Herbreteau D, Fransen H, van Rooij WJ, Boccardi E, et al. Endovascular treatment of brain arteriovenous malformations using a liquid embolic agent: results of a prospective, multicentre study (BRAVO) Eur Radiol. 2013 Oct;23(10):2838–45. doi: 10.1007/s00330-013-2870-6. [DOI] [PubMed] [Google Scholar]
- 21.Roark C, Vadlamudi V, Chaudhary N, Gemmete JJ, Seinfeld J, Thompson BG. ABC/2 method does not accurately predict cerebral arteriovenous malformation volume. Neurosurgery. 2018 Feb;82(2):220–5. doi: 10.1093/neuros/nyx139. [DOI] [PubMed] [Google Scholar]
- 22.Sahlein DH, Mora P, Becske T, Nelson PK. Nidal embolization of brain arteriovenous malformations: rates of cure, partial embolization, and clinical outcome. J Neurosurg. 2012 Jul;117(1):65–77. doi: 10.3171/2012.3.JNS111405. [DOI] [PubMed] [Google Scholar]
- 23.See AP, Mohammaden MH, Rizko M, Stapleton CJ, Amin-Hanjani S, Charbel FT, et al. Morbidity and mortality associated with sequential flow reduction embolization technique of cerebral arteriovenous malformations using n-butyl cyanoacrylate. J Neurointerv Surg. 2021 Mar;13(3):237–41. doi: 10.1136/neurintsurg-2020-016223. [DOI] [PubMed] [Google Scholar]
- 24.Solomon RA, Connolly ES. Arteriovenous malformations of the brain. N Engl J Med. 2017 May;376(19):1859–66. doi: 10.1056/NEJMra1607407. [DOI] [PubMed] [Google Scholar]
- 25.Vinuela F, Dion JE, Duckwiler G, Martin NA, Lylyk P, Fox A, et al. Combined endovascular embolization and surgery in the management of cerebral arteriovenous malformations: experience with 101 cases. J Neurosurg. 1991 Dec;75(6):856–64. doi: 10.3171/jns.1991.75.6.0856. [DOI] [PubMed] [Google Scholar]
- 26.Weber W, Kis B, Siekmann R, Kuehne D. Endovascular treatment of intracranial arteriovenous malformations with onyx: technical aspects. AJNR Am J Neuroradiol. 2007 Feb;28(2):371–7. [PMC free article] [PubMed] [Google Scholar]