

Abstract
Greater physical fitness may lead to greater left ventricular mass (LVM) and reduce the effect of cardiometabolic risk factors on LVM. However, the cardiometabolic biomarkers associations for LVM have not been clarified in physically active young adults. This study included 2019 men and 253 women, aged 18–43 years, from the military in Taiwan. All participants underwent anthropometric and blood metabolic markers measurements, and completed a 3000-m run test for assessing fitness. LVM was calculated on the basis of an echocardiography. Multiple linear regression was used to determine the sex-specific associations between cardiometabolic risk markers and LVM indexed for the body height (g/m2.7). In men, age, systolic blood pressure (SBP), 3000-m running time, serum triglycerides, serum uric acid and waist circumference (WC) were correlated with LVM index (β = 0.07, 0.10, − 0.01, 0.01, 0.24 and 0.24, respectively; all p-values < 0.05). The correlations were not significant for fasting plasma glucose, total cholesterol and high-density lipoprotein cholesterol (HDL-C). In women, SBP, HDL-C and WC were correlated with LVM index in the univariate analysis (β = 0.07, − 0.05 and 0.32, respectively; all p-values < 0.05), whereas the correlation was only significant for WC in the multiple linear regression analysis (β = 0.20; p-value < 0.001). In physically active adults, the associations of cardiometabolic risk markers with LVM might vary by sex. Better endurance exercise performance associated with greater LVM was noted only in men, while greater WC was the only metabolic risk marker for greater LVM in both men and women.
Subject terms: Cardiology, Risk factors
Introduction
Cardiometabolic risk markers are a collection of abnormalities characterized by abdominal obesity, hypertension, dyslipidemia, hyperglycemia and increased oxidative stress1. The risk markers may contribute to end-organ damage, such as left ventricular hypertrophy (LVH)2,3. Cigarette smoking, alcohol intake, low physical fitness and cardiometabolic abnormalities have been considered as the modifiable risk factors of CVD4–8. LVH may act as a role of mediator to CVD9, and can be a sign of patients with increased risk of CVD where physicians may take a more aggressive action on CVD prevention. Prior studies have revealed that the contributions of the cardiometabolic risk markers to LVH or CVD may vary by age and sex10,11. For instance, serum triglycerides have been associated with left ventricular mass (LVM) in hypertensive individuals, which might be only observed in men rather than women11. Therefore, it is critical to investigate the associations between the cardiometabolic risk markers and LVH in specific populations.
As is known, endurance and muscular strength exercises can modulate cardiac structure, resulting in greater LVM, and improve cardiac diastolic function12. The degree of cardiac remodeling related to exercises may vary by race and sex13–15. Prior studies have uncovered that for a given level of physical training, African/Afro-Caribbean athletes show more prominent LVM changes than do Asian and Caucasian athletes12–15, due in part to genetic variations. In addition, male athletes have been observed with a more marked increase in LVM after training compared to female athletes13,16. The effect and interplay between physical fitness and the risk factors of CVD on LVM changes have been rarely examined in physically active individuals, such as athletes and military recruits. We hypothesized that physical fitness could reduce the association between the cardiometabolic risk markers and LVM assessed by electrocardiography (ECG) and echocardiography. The purpose of the study was to clarify the associations in military men and women in Taiwan.
Methods
Study population
The cardiorespiratory fitness and health in eastern armed forces (CHIEF)-heart study included 2688 military personnel, aged 18–43 years, in whom 2386 were men and 302 were women in Eastern Taiwan of R.O.C., 2018–202117–19. All male and female participants were physically active, and received daily aerobic and resistance exercise training. All subjects underwent annual military health examinations, including laboratory tests and a self-reported questionnaire for their behavior of toxic substances use, i.e., cigarette smoking and alcohol intake (former or never vs. active) in the Hualien Armed Forces General Hospital. All subjects participated annual fitness exams in the Military Physical Training and Testing Center in Hualien for examining endurance capacity by the time for a 3000-m run test. All participants received a 12-lead ECG and transthoracic echocardiography for evaluating cardiac structure following the exercise test and before the end of index year19,20. Participants who had serum triglycerides ≥ 400 mg/dL (N = 38), blood pressure (BP) ≥ 140/90 mmHg (N = 346), or body mass index (BMI) ≥ 35 kg/m2 (N = 32) were excluded, leaving a sample of 2019 men and 253 women for analysis.
Anthropometric, hemodynamic and blood test measurements
Body height, body weight and WC measurements of all study subjects were carried out in a standing position. BMI was calculated as body weight (kg) divided by square of body height (m2). The blood pressure (BP) of each subject at rest was measured over right arm in a sitting position by the automatic BP monitor machine (FT201 Parama-Tech Co., Ltd, Fukuoka, Japan), which used the oscillometric method. Routine blood tests, including fasting plasma glucose, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), serum uric acid (SUA) and serum triglycerides were measured by an Olympus AU640 auto analyzer (Olympus, Kobe, Japan). All blood samples were collected after an overnight 12-h fast at the same blood drawing station.
The 3000-m run test
The participants ran a 3-km distance on a flat playground at the Hualien Military Physical Training and Testing Center without bearing a load. The run test was performed outdoor at 16:00 PM after at least a 1-h rest. The weather for the run test was restricted to the condition when there was no heavy raining and the heat stroke risk coefficient, defined as the outdoor temperature on the Celsius scale × relative humidity (%) × 0.1, was < 4020.
Cardiometabolic risk markers for LVM
Based on the latest criteria of International Diabetes Federation for Chinese21, metabolic syndrome was defined as having three or more clinical features: (1) central obesity: WC ≥ 90 cm for men, and ≥ 80 cm for women; (2) fasting plasma glucose ≥ 100 mg/dL, or with anti-diabetic medications; (3) serum triglycerides ≥ 150 mg/dL, or with lipid-lowering medications; (4) HDL-C < 40 mg/dL for men, and < 50 mg/dL for women; (5) systolic BP ≥ 130 mmHg and/or diastolic BP ≥ 85 mmHg, or with antihypertensive medications. SUA has been associated with levels of oxidative stress and systemic inflammation in the body22,23. Hyperuricemia was defined as SUA ≥ 7.0 mg/dL for men and ≥ 6.0 mg/dL for women.
ECG and echocardiographic measurements
Twelve-lead surface ECGs were obtained from CARDIOVIT MS-2015 machine (the Schiller AG, Baar, Switzerland) until a high-quality output image available. The ECG reports were reviewed and approved by an experienced cardiologist. The Sokolow-Lyon voltage criterion for LVH was defined as if the maximum of (S-V1 or V2 + R-V5 or V6) ≥ 35 mm24, and the Cornell voltage criterion for Asian young men was defined as if (R-aVL + S-V3) ≥ 18 mm25.
The transthoracic echocardiography (iE33; Philips Medical Systems, Andover, MA, USA) with a 1–5 MHz transducer, was reviewed by the same cardiologist at the Hualien-Armed Forces General Hospital. Based on the recommendations of the American Society of Echocardiography26, LVM was calculated at end diastole using the corrected formula proposed by Devereux et al.27: 0.8 × {1.04 × [(LV internal diameter (LVIDd) + posterior wall thickness + interventricular septal thickness]3 − LVIDd3} + 0.6. Echocardiographic LVH was defined as the highest 5% of the LVM indexed for the body height (m2.7)28, corresponding to 46.0 g/m2.7 (5.99%) for men and 38.0 g/m2.7 for women in this study25,29.
Statistical analysis
Demographic, anthropometric, time for a 3000-m run (endurance exercise performance), cardiometabolic risk markers, ECG and echocardiography characteristics of the military male and female personnel were presented as numbers (%) for categorical variables and mean ± standard deviation for continuous variables, respectively. Univariate linear regression was used to determine sex-specific correlation of each cardiometabolic risk marker with LVM index. Multiple linear regression was used to determine the independent cardiometabolic risk markers of LVM index in men and women, respectively. Furthermore, multiple logistic regression was used to determine the odds ratio (OR) of cardiometabolic risk markers with echocardiographic LVH (in model 1 without adjustment for endurance exercise performance, and in model 2 with adjustment for endurance exercise performance, and in model 3 with further adjustment for body weight) and with ECG-based LVH (model 1 and model 2) in men. As the number of outcome of interests (LVH) was too small (N < 15) for women to be analyzed, the results were only provided in supplemental tables. A value of P < 0.05 was regarded significant. All analyses were performed using SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA). This study has been reviewed and approved by the Institutional Review Board of the Human Research Ethics Committee (HREC) of the Mennonite Christian Hospital (No. 16-05-008) in Hualien City, Taiwan, and written informed consent was obtained from all participants. In addition, all methods were performed in accordance with the relevant guidelines and regulations.
Ethics approval and consent to participate
The Institutional Review Board (IRB) of the Mennonite Christian Hospital (No. 16-05-008) in Hualien of Taiwan approved access to the data for the CHIEF study, and written informed consent was obtained from all participants.
Results
Clinical features and laboratory findings
The clinical characteristics of men and women are provided in Table 1. The age of men and women were 27.5 and 26.0 years, respectively. In general, men had a greater level of BMI, WC, BP, fasting plasma glucose, total cholesterol, serum triglycerides, SUA, exercise performance (shorter time for a run test) and LVM, and a higher prevalence of active cigarette smoking, alcohol intake, metabolic syndrome and ECG-based LVH, compared to women. In contrast, men had a lower level of HDL-C level than women.
Table 1.
Baseline Characteristics of the Military Men and Women (N = 2272.
| Men (N = 2019) |
Women (N = 253) |
|
|---|---|---|
| Age, years | 27.53 ± 5.93 | 26.02 ± 4.95 |
| Smoking, active (%) | 892 (44.18) | 56 (22.13) |
| Alcohol intake, active (%) | 854 (42.30) | 44 (17.39) |
| 3000-m running time, second | 873.15 ± 93.58 | 1035.98 ± 117.68 |
| Body mass index, kg/m2 | 24.88 ± 3.72 | 22.65 ± 2.89 |
| Waist circumference, cm | 83.56 ± 9.63 | 74.50 ± 7.77 |
| Systolic blood pressure, mmHg | 118.60 ± 13.14 | 106.79 ± 10.66 |
| Diastolic blood pressure, mmHg | 70.12 ± 10.28 | 64.72 ± 8.08 |
| Total cholesterol, mg/dl | 174.22 ± 34.09 | 168.55 ± 28.92 |
| High-density lipoprotein, mg/dl | 49.36 ± 10.44 | 60.70 ± 12.82 |
| Serum triglycerides, mg/dl | 108.29 ± 82.20 | 66.09 ± 29.35 |
| Fasting plasma glucose, mg/dl | 93.58 ± 11.61 | 90.37 ± 7.50 |
| Serum uric acid, mg/dl | 6.74 ± 1.35 | 4.75 ± 0.93 |
| Metabolic syndrome (%) | 255 (12.63) | 8 (3.16) |
| LVM, gram | 148.34 ± 32.01 | 103.34 ± 18.94 |
| ECG voltage criteria | ||
| Sokolow-Lyon based LVH (%) | 1039 (51.46) | 14 (5.53) |
| Cornell based LVH (%) | 199 (9.86) | 3 (1.19) |
| Echocardiographic criteria | ||
|
LVM index ≥ 46 g/m2.7 for men (%), or ≥ 38 g/m2.7 for women (%) |
121 (5.99) | 11 (4.30) |
ECG Electrocardiography, LVH Left ventricular hypertrophy, LVM Left ventricular mass.
The correlations of cardiometabolic risk markers with LVM index
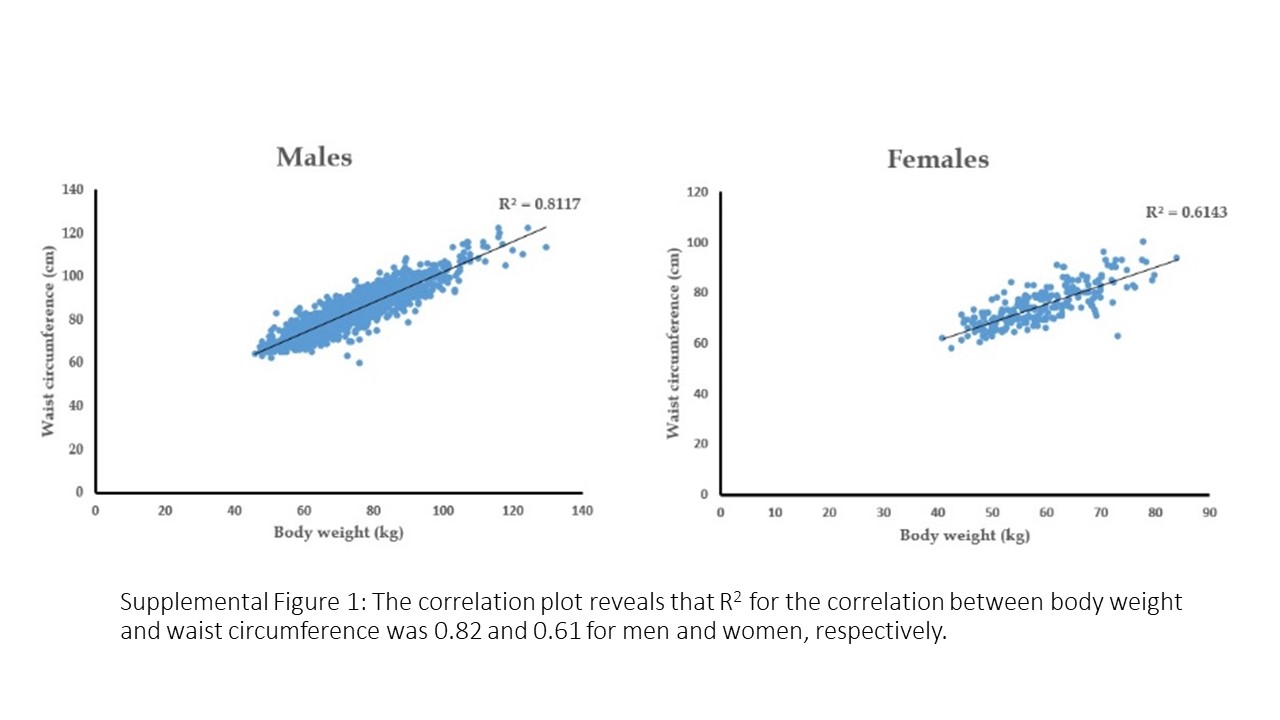
The results of univariate and multiple linear regressions of cardiometabolic risk markers with LVM index in men and women are shown in Table 2. For men, in the univariate analysis, each cardiometabolic risk marker, except the endurance exercise performance, was significantly correlated with LVM index, whereas in the multiple linear regression, only age, systolic BP, time for a 3000-m run, serum triglycerides, SUA and WC were correlated with LVM index (β = 0.07, 0.10, − 0.01, 0.01, 0.24 and 0.24, respectively; all p-values < 0.05). For women, systolic BP, HDL-C and WC were correlated with LVM index in the univariate analysis (β = 0.07, − 0.05 and 0.32, respectively; all p-values < 0.05), whereas the correlation was merely significant for WC in the multivariable model (β = 0.20; p < 0.01). If body weight was further included in the multiple linear regression analysis, the association for WC was reduced more in women (β = 0.06, p = 0.36) than in men (β = 0.15, p < 0.01), indicating the effect of body weight higher than WC for LVM in women (R2 for the correlation between body weight and WC: 0.82 and 0.61 for men and women, respectively in supplemental Fig. 1).
Table 2.
Sex-Specific Correlations between Cardiometabolic Risk Factors and LVMI.
| LVM/height2.7 (Men) | LVM/height2.7 (Women) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Multivariate | Univariate | Multivariate | Multivariate | |||||||||
| R | β | p | β | p | β | p | R | β | p | β | p | β | p | |
| Age | 0.18 | 0.23 | < 0.01 | 0.07 | < 0.01 | 0.08 | < 0.01 | 0.002 | − 0.002 | 0.97 | − 0.05 | 0.43 | − 0.05 | 0.45 |
| 3000-m running time | 0.04 | 0.003 | 0.07 | − 0.01 | < 0.01 | − 0.01 | < 0.01 | 0.03 | − 0.001 | 0.67 | − 0.003 | 0.26 | − 0.004 | 0.11 |
| Systolic BP | 0.33 | 0.18 | < 0.01 | 0.10 | < 0.01 | 0.10 | < 0.01 | 0.14 | 0.07 | 0.02 | 0.05 | 0.20 | 0.04 | 0.28 |
| Diastolic BP | 0.25 | 0.18 | < 0.01 | 0.01 | 0.50 | 0.01 | 0.49 | 0.05 | 0.03 | 0.39 | − 0.02 | 0.62 | − 0.02 | 0.68 |
| Total cholesterol | 0.12 | 0.03 | < 0.01 | − 0.01 | 0.29 | − 0.004 | 0.42 | 0.03 | 0.006 | 0.60 | 0.01 | 0.35 | 0.02 | 0.22 |
| HDL-C | 0.15 | − 0.11 | < 0.01 | − 0.01 | 0.51 | − 0.01 | 0.47 | 0.13 | − 0.05 | 0.04 | − 0.05 | 0.09 | − 0.05 | 0.07 |
| Serum triglycerides | 0.20 | 0.02 | < 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.10 | 0.02 | 0.11 | − 0.003 | 0.79 | − 0.002 | 0.86 |
| Fasting glucose | 0.11 | 0.07 | < 0.01 | − 0.004 | 0.73 | − 0.005 | 0.71 | 0.07 | − 0.05 | 0.29 | − 0.07 | 0.10 | − 0.07 | 0.09 |
| Serum uric acid | 0.19 | 1.01 | < 0.01 | 0.24 | 0.04 | 0.22 | 0.06 | 0.10 | 0.52 | 0.13 | 0.009 | 0.97 | 0.06 | 0.87 |
| Waist circumference | 0.42 | 0.32 | < 0.01 | 0.24 | < 0.01 | 0.15 | < 0.01 | 0.32 | 0.21 | < 0.01 | 0.20 | < 0.01 | 0.06 | 0.36 |
| Body weight | 0.41 | 0.242 | < 0.01 | 0.08 | < 0.01 | 0.34 | 0.21 | < 0.01 | 0.17 | < 0.01 | ||||
Multiple linear regression analysis was used to determine the association of LVM index with age, 3000-m running time, systolic BP, diastolic BP, total cholesterol, HDL-C, serum triglycerides, fasting glucose, serum uric acid, waist circumference, cigarette smoking and alcohol intake status, with and without body weight.
BP Blood pressure, HDL-C High-density lipoprotein cholesterol, LVM Left ventricular mass.
Cardiometabolic risk markers for echocardiographic LVH in men
Table 3 reveals the results of multiple logistic regression analysis for the risk markers of echocardiographic LVH in men. Further adjustment for endurance exercise performance in model 2 did not alter the main results from model 1. Prehypertension, hypertriglyceridemia, hyperuricemia, abdominal obesity and metabolic syndrome were the independent risk markers of echocardiographic LVH in men in model 2 [ORs: 4.15 (95% confidence intervals (CI): 2.83–6.08), 1.78 (95% CI: 1.18–2.70), 2.28 (95% CI: 1.56–3.34), 3.38 (95% CI: 2.28–5.02) and 2.96 (95% CI: 1.94–4.52), respectively]. In model 3, with further adjustment for body weight, prehypertension and hyperuricemia remained the independent risk markers of echocardiographic LVH in men [ORs: 2.83 (95% CI: 1.89–4.23) and 1.67 (95% CI: 1.12–2.48), respectively], and there was a marginal association for metabolic syndrome [OR: 1.58 (95% CI: 0.99–2.50)]. However, the association for abdominal obesity was reduced and became insignificant (OR: 1.22, p = 0.46), probably due to a high correlation between body weight and WC. The results for women were provided in supplemental Table 1, which shows no significant associations for all cardiometabolic risk markers.
Table 3.
Associations between Cardiometabolic Risk Factors and Echocardiographic Left Ventricular Hypertrophy in Men.
| LVM/height2.7 ≥ 46 g/m2.7 | ||||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||||
| OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | |
| BP ≥ 130/85 mmHg | 4.24 (2.90–6.21) | < 0.01 | 4.15 (2.83–6.08) | < 0.01 | 2.83 (1.89–4.23) | < 0.01 |
| Total cholesterol ≥ 200 mg/dl | 1.10 (0.71–1.69) | 0.67 | 1.10 (0.71–1.70) | 0.67 | 1.00 (0.64–1.55) | 0.98 |
| HDL-C < 40 mg/dl | 1.42 (0.92–2.19) | 0.11 | 1.36 (0.88–2.10) | 0.16 | 0.96 (0.61–1.52) | 0.86 |
| Serum triglycerides ≥ 150 mg/dl | 1.82 (1.20–2.75) | < 0.01 | 1.78 (1.18–2.70) | < 0.01 | 1.38 (0.90–2.11) | 0.14 |
| Fasting glucose ≥ 100 mg/dl | 1.13 (0.73–1.76) | 0.58 | 1.13 (0.73–1.76) | 0.58 | 0.90 (0.57–1.43) | 0.66 |
| Serum uric acid ≥ 7.0 mg/dl | 2.32 (1.59–3.40) | < 0.01 | 2.28 (1.56–3.34) | < 0.01 | 1.67 (1.12–2.48) | 0.01 |
| Waist circumference ≥ 90 mg/dl | 3.53 (2.39–5.22) | < 0.01 | 3.38 (2.28–5.02) | < 0.01 | 1.22 (0.71–2.10) | 0.46 |
| Metabolic syndrome | 3.11 (2.04–4.73) | < 0.01 | 2.96 (1.94–4.52) | < 0.01 | 1.58 (0.99–2.50) | 0.05 |
Multiple logistic regressions were used to determine the association of cardiometabolic risk factors with echocardiographic left ventricular hypertrophy.
Model 1 adjusted for age, BP ≥ 130/85 mmHg, total cholesterol ≥ 200 mg/dl, HDL-C < 40 mg/dl, serum triglycerides ≥ 150 mg/dl, fasting glucose ≥ 100 mg/dl, serum uric acid ≥ 7.0 mg/dl, waist circumference ≥ 90 mg/dl, metabolic syndrome status, cigarette smoking status and alcohol intake status.
Model 2 adjusted for the covariates in model 1 and 3000-m running time.
Model 3 adjusted for the covariates in model 2 and body weight.
BP Blood pressure, HDL-C High-density lipoprotein cholesterol, LVM Left ventricular mass.
Cardiometabolic risk markers for ECG-LVH in men
The results of multiple logistic regression analysis for the cardiometabolic risk markers of ECG-LVH in men are shown in Table 4. Additional adjustment for endurance exercise performance in model 2 yielded similar results compared to model 1. In model 2, prehypertension was the only independent risk marker of Sokolow-Lyon based ECG-LVH [ORs: 1.28 (95% CI: 1.03–1.60)]. However, abdominal obesity and metabolic syndrome uncovered an inverse association with Sokolow-Lyon based ECG-LVH [ORs: 0.54 (95% CI: 0.43–0.66) and 0.74 (95% CI: 0.56–0.97), respectively]. Prehypertension and hypertriglyceridemia were independent risk markers of Cornell based ECG-LVH [ORs: 1.65 (95% CI: 1.19–2.29) and 1.44 (95% CI: 1.01–2.04), respectively], whereas the associations of abdominal obesity and metabolic syndrome with Cornell based ECG-LVH were null. The results for women were demonstrated in supplemental Table 2, which revealed prehypertension to be the independent risk marker of both Sokolow-Lyon and Cornell based ECG-LVH, and metabolic syndrome to be another risk marker of Cornell based ECG-LVH.
Table 4.
Associations between Cardiometabolic Risk Factors and Electrocardiographic Left Ventricular Hypertrophy in Men.
| Sokolow-Lyon based ECG-LVH | Cornell based ECG-LVH | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | |
| BP ≥ 130/85 mmHg | 1.26 (1.01–1.57) | 0.04 | 1.28 (1.03–1.60) | 0.03 | 1.66 (1.19–2.30) | < 0.01 | 1.65 (1.19–2.29) | < 0.01 |
| Total cholesterol ≥ 200 mg/dl | 0.87 (0.70–1.10) | 0.24 | 0.87 (0.70–1.10) | 0.24 | 0.95 (0.65–1.37) | 0.76 | 0.95 (0.65–1.37) | 0.76 |
| HDL-C < 40 mg/dl | 0.82 (0.65–1.03) | 0.09 | 0.84 (0.67–1.06) | 0.13 | 0.91 (0.62–1.33) | 0.62 | 0.90 (0.61–1.32) | 0.58 |
| Serum triglycerides ≥ 150 mg/dl | 1.00 (0.79–1.27) | 0.98 | 1.02 (0.80–1.29) | 0.89 | 1.44 (1.01–2.05) | 0.04 | 1.44 (1.01–2.04) | 0.04 |
| Fasting glucose ≥ 100 mg/dl | 0.83 (0.66–1.05) | 0.12 | 0.84 (0.67–1.06) | 0.13 | 0.89 (0.61–1.31) | 0.55 | 0.89 (0.61–1.31) | 0.55 |
| Serum uric acid ≥ 7.0 mg/dl | 0.83 (0.69–1.00) | 0.05 | 0.84 (0.70–1.01) | 0.07 | 1.03 (0.76–1.39) | 0.87 | 1.02 (0.75–1.38) | 0.90 |
| Waist circumference ≥ 90 mg/dl | 0.52 (0.43–0.65) | < 0.01 | 0.54 (0.43–0.66) | < 0.01 | 1.26 (0.91–1.74) | 0.16 | 1.25 (0.90–1.73) | 0.18 |
| Metabolic syndrome | 0.71 (0.54–0.94) | 0.01 | 0.74 (0.56–0.97) | 0.03 | 1.29 (0.86–1.95) | 0.22 | 1.28 (0.85–1.93) | 0.24 |
Multiple logistic regressions were used to determine the association of cardiometabolic risk factors with electrocardiographic LVH.
Model 1 adjusted for age, BP ≥ 130/85 mmHg, total cholesterol ≥ 200 mg/dl, HDL-C < 40 mg/dl, serum triglycerides ≥ 150 mg/dl, fasting glucose ≥ 100 mg/dl, serum uric acid ≥ 7.0 mg/dl, waist circumference ≥ 90 mg/dl, metabolic syndrome status, cigarette smoking status and alcohol intake status.
Model 2 adjusted for the covariates in model 1 and 3000-m running time.
BP Blood pressure, HDL-C High-density lipoprotein cholesterol, LVH Left ventricular hypertrophy.
Discussion
The principal findings in the present study were that in physically active Asian young adults, the associations between cardiometabolic risk markers and LVM index may vary by sex. Greater age, systolic BP, serum triglycerides, SUA, body weight and WC, and superior endurance exercise performance were correlated with greater LVM index in men, whereas only greater WC or body weight was correlated with greater LVM index in women. In addition, in our male subjects, prehypertension, hypertriglyceridemia, hyperuricemia, abdominal obesity and metabolic syndrome were the independent risk markers of echocardioghraphic LVH. Prehypertension was the independent risk marker of both Sokolow-Lyon and Cornell based ECG -LVH. Hypertriglyceridemia was found as another risk marker of Cornell based LVH; however abdominal obesity and metabolic syndrome had a lower risk of Sokolow-Lyon based ECG-LVH.
Most prior studies were designed to investigate the association between cardio-metabolic risk markers and LVM index in hypertensive or diabetic individuals, who were at middle or old ages2,30, and the physical activity or fitness was rarely taken into account6. The independent cardiometabolic risk markers of LVM may vary according to the subjects selected. In hypertensive patients, age, systolic BP, fasting glucose, serum triglycerides and SUA were correlated with LVM2,6,8; however, the relationship for serum triglycerides might be only present in men, and the predictor of LVM in the overweight or obese was only systolic BP31. In contrast, in type 2 diabetic patients, Jørgensen et al. reported a correlation of systolic BP and HDL-C with LVM30, whereas there were no associations for hemoglobin A1c. With regard to the impact of physical activity, Joseph et al. showed the association between physical activity and LVM merely in the normotensive individuals6. In this present study, we further found a sex difference that the association for endurance exercise performance, an estimate for physical fitness, was present in men but not in women free of hypertension. Moreover, for physically active premenopausal women, we revealed that body weight or WC rather than systolic BP was the only independent metabolic risk marker for greater LVM.
Hypertension, abdominal obesity and metabolic syndrome have been revealed as the risk biomarkers of Cornell based ECG-LVH in the general population32. Similarly, the present study revealed that prehypertension was the metabolic risk marker of Sokolow-Lyon and Cornell based ECG-LVH in both physically active young men and women. Hypertriglycerdemia and metabolic syndrome were the independent risk biomarkers of Cornell based ECG-LVH in physically active men and women, respectively. On the contrary, our prior and present works revealed an inverse association with Sokolow-Lyon based ECG-LVH for men10. As compared to men, premenopausal women were thinner, and affected more by the breast than the chest wall thickness, which might result in the sex differences. In addition, the Cornell based ECG-LVH, unlike the Sokolow-Lyon based ECG-LVH, used the limb lead aVL voltage as a part of the criterion, and might reduce the effect of greater chest wall thickness in obesity on diminishing the electrical signals, which has shown a higher accuracy to echocardiographic LVH for both young men and women in prior studies10. Furthermore, using the Cornell based ECG-LVH was superior to using the Sokolow-Lyon based ECG-LVH to predict incident CVD, which has been shown in prior studies as well33,34. Accordingly, using the Cornell based ECG criterion for LVH is suggestive for identifying those who were at greater cardiometabolic risk from the physically young adults in the present study.
Study strengths and limitations
The major strength of the CHIEF heart study was that the study subjects were included from the military in Taiwan, where the training was standardized. As the military base is a closed system, the environment and daily life for the study subjects are similar, which could reduce the unmeasured confounders. By contrast, there had some limitations in the present study. First, the sample size of women had an insufficient power for the multiple logistic regression analysis. Second, since this was a cross-sectional study, the temporal changes in cardiac structure could not be assessed.
Conclusion
The study suggests that in physically active young adults, the associations of cardiometabolic risk markers with LVM and ECG-LVH may vary by sex. In men, there was an association of endurance exercise performance with LVM, however the associations of cardiometabolic risk markers with LVM were not much modified by the exercise performance. In addition, greater body weight or WC, indicating obesity, was a powerful risk marker of greater LVM in both men and women. Thus, weight reduction is suggested to reduce LVM and for a prevention of incident CVD. On the other respect, prehypertension was the risk marker of Cornell and Sokolow-Lyon based ECG-LVH for both men and women, while not the risk marker of echocardiographic LVH for women. This sex difference reflects that a mildly elevated BP level may increase the power of cardiac electricity prior to the structural change of LVH, particularly for the physically young women. Further studies are required to clarify this finding.
Supplementary Information
{kind=link}
Abbreviations
- CHIEF
Cardiorespiratory fitness and health in eastern armed forces study
- LVH
Left ventricular hypertrophy
- LVM
Left ventricular mass
Author contributions
K.Z.T. wrote the paper and made the statistical analyses; P.Y.L. collected and interpreted the data; W.C.H., J.A.C.L. and C.J.L. raised critical comments and edited the manuscript; G.M.L. was the principal investigator for the study.
Funding
The study was supported by the Medical Affairs Bureau Ministry of National Defense (MND-MAB-D-11115) and Hualien Armed Forces General Hospital (HAFGH-D-111003), where was the main place involved in the study design, data collection, analyses and writing of this research.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to materials obtained from the military in Taiwan, which were confidential, but are available from the corresponding author on reasonable request.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-022-15818-y.
References
- 1.Jakubiak GK, et al. “Obesity and Insulin Resistance” is the component of the metabolic syndrome most strongly associated with oxidative stress. Antioxidants (Basel) 2021;11:79. doi: 10.3390/antiox11010079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Visco V, et al. Serum uric acid and left ventricular mass in essential hypertension. Front. Cardiovasc. Med. 2020;7:570000. doi: 10.3389/fcvm.2020.570000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee HJ, et al. Subclinical alterations in left ventricular structure and function according to obesity and metabolic health status. PLoS ONE. 2019;14:e0222118. doi: 10.1371/journal.pone.0222118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dekker JM, et al. Metabolic syndrome and 10-year cardiovascular disease risk in the Hoorn Study. Circulation. 2005;112:666–673. doi: 10.1161/CIRCULATIONAHA.104.516948. [DOI] [PubMed] [Google Scholar]
- 5.Mottillo S, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010;56:1113–1132. doi: 10.1016/j.jacc.2010.05.034. [DOI] [PubMed] [Google Scholar]
- 6.Benowitz NL, Liakoni E. Tobacco use disorder and cardiovascular health. Addiction. 2022;117:1128–1138. doi: 10.1111/add.15703. [DOI] [PubMed] [Google Scholar]
- 7.Ikehara S, Iso H. Alcohol consumption and risks of hypertension and cardiovascular disease in Japanese men and women. Hypertens. Res. 2020;43:477–481. doi: 10.1038/s41440-020-0417-1. [DOI] [PubMed] [Google Scholar]
- 8.Barbiellini Amidei C, et al. Association of physical activity trajectories with major cardiovascular diseases in elderly people. Heart. 2022;108:360–366. doi: 10.1136/heartjnl-2021-320013. [DOI] [PubMed] [Google Scholar]
- 9.Yildiz M, Oktay AA, Stewart MH, Milani RV, Ventura HO, Lavie CJ. Left ventricular hypertrophy and hypertension. Prog. Cardiovasc. Dis. 2020;63:10–21. doi: 10.1016/j.pcad.2019.11.009. [DOI] [PubMed] [Google Scholar]
- 10.Feng P, et al. Analysis of the associations between obesity indices and left ventricular mass. Cardiology. 2018;141:183–189. doi: 10.1159/000496177. [DOI] [PubMed] [Google Scholar]
- 11.Pietri P, et al. Triglycerides are related to left ventricular mass in hypertensive patients independently of other cardiometabolic risk factors: the effect of gender. Sci. Rep. 2020;10:13253. doi: 10.1038/s41598-020-70237-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Liu PY, Tsai KZ, Lima JAC, Lavie CJ, Lin GM. Athlete’s heart in Asian military males: The CHIEF heart study. Front. Cardiovasc. Med. 2021;8:725852. doi: 10.3389/fcvm.2021.725852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lin YK, Tsai KZ, Han CL, Lee JT, Lin GM. Athlete’s heart assessed by sit-up strength exercises in military men and women: The CHIEF heart study. Front. Cardiovasc. Med. 2021;8:737607. doi: 10.3389/fcvm.2021.737607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Papadakis M, Wilson MG, Ghani S, Kervio G, Carre F, Sharma S. Impact of ethnicity upon cardiovascular adaptation in competitive athletes: Relevance to preparticipation screening. Br. J. Sports Med. 2012;46(Suppl 1):i22–i28. doi: 10.1136/bjsports-2012-091127. [DOI] [PubMed] [Google Scholar]
- 15.Sheikh N, Sharma S. Impact of ethnicity on cardiac adaptation to exercise. Nat. Rev. Cardiol. 2014;11:198–217. doi: 10.1038/nrcardio.2014.15. [DOI] [PubMed] [Google Scholar]
- 16.Barnes JN, Fu Q. Sex-specific ventricular and vascular adaptations to exercise. Adv. Exp. Med. Biol. 2018;1065:329–346. doi: 10.1007/978-3-319-77932-4_21. [DOI] [PubMed] [Google Scholar]
- 17.Lin GM, Lu HH. A 12-lead ECG-based system with physiological parameters and machine learning to identify right ventricular hypertrophy in young adults. IEEE. J. Transl. Eng. Health. Med. 2020;8:1900510. doi: 10.1109/JTEHM.2020.2996370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lin GM, Liu K. An electrocardiographic system with anthropometrics via machine learning to screen left ventricular hypertrophy among young adults. IEEE. J. Transl. Eng. Health. Med. 2020;8:1800111. doi: 10.1109/JTEHM.2020.2990073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chao WH, Su FY, Lin F, Yu YS, Lin GM. Association of electrocardiographic left and right ventricular hypertrophy with physical fitness of military males: The CHIEF study. Eur. J. Sport Sci. 2019;19:1214–1220. doi: 10.1080/17461391.2019.1595741. [DOI] [PubMed] [Google Scholar]
- 20.Lin GM, et al. Rationale and design of the cardiorespiratory fitness and hospitalization events in armed forces study in Eastern Taiwan. World. J. Cardiol. 2016;8:464–471. doi: 10.4330/wjc.v8.i8.464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Grundy SM, et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 22.Kurajoh M, et al. Uric acid shown to contribute to increased oxidative stress level independent of xanthine oxidoreductase activity in MedCity21 health examination registry. Sci. Rep. 2021;11:7378. doi: 10.1038/s41598-021-86962-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lyngdoh T, et al. Elevated serum uric acid is associated with high circulating inflammatory cytokines in the population-based Colaus study. PLoS ONE. 2011;6:e19901. doi: 10.1371/journal.pone.0019901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am. Heart. J. 1949;37:161–186. doi: 10.1016/0002-8703(49)90562-1. [DOI] [PubMed] [Google Scholar]
- 25.Su FY, et al. A comparison of Cornell and Sokolow-Lyon electrocardiographic criteria for left ventricular hypertrophy in a military male population in Taiwan: The Cardiorespiratory fitness and HospItalization Events in armed Forces study. Cardiovasc. Diagn. Ther. 2017;7:244–251. doi: 10.21037/cdt.2017.01.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lang RM, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015;28:1–39.e14. doi: 10.1016/j.echo.2014.10.003. [DOI] [PubMed] [Google Scholar]
- 27.Devereux RB, Casale PN, Eisenberg RR, Miller DH, Kligfield P. Electrocardiographic detection of left ventricular hypertrophy using echocardiographic determination of left ventricular mass as the reference standard. Comparison of standard criteria, computer diagnosis and physician interpretation. J. Am. Coll. Cardiol. 1984;3:82–87. doi: 10.1016/S0735-1097(84)80433-7. [DOI] [PubMed] [Google Scholar]
- 28.de Simone G, et al. Normalization for body size and population-attributable risk of left ventricular hypertrophy: The Strong Heart Study. Am. J. Hypertens. 2005;18:191–196. doi: 10.1016/j.amjhyper.2004.08.032. [DOI] [PubMed] [Google Scholar]
- 29.Su FY, et al. Comparisons of traditional electrocardiographic criteria for left and right ventricular hypertrophy in young Asian women: The CHIEF heart study. Medicine (Baltimore) 2020;99:e22836. doi: 10.1097/MD.0000000000022836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jørgensen PG, et al. Burden of uncontrolled metabolic risk factors and left ventricular structure and function in patients with type 2 diabetes mellitus. J. Am. Heart. Assoc. 2018;7:e008856. doi: 10.1161/JAHA.118.008856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Guerra F, et al. The association of left ventricular hypertrophy with metabolic syndrome is dependent on body mass index in hypertensive overweight or obese patients. PLoS ONE. 2011;6:e16630. doi: 10.1371/journal.pone.0016630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ahmad MI, Li Y, Soliman EZ. Association of obesity phenotypes with electrocardiographic left ventricular hypertrophy in the general population. J. Electrocardiol. 2018;51:1125–1130. doi: 10.1016/j.jelectrocard.2018.10.085. [DOI] [PubMed] [Google Scholar]
- 33.Porthan K, et al. ECG left ventricular hypertrophy as a risk predictor of sudden cardiac death. Int. J. Cardiol. 2019;276:125–129. doi: 10.1016/j.ijcard.2018.09.104. [DOI] [PubMed] [Google Scholar]
- 34.Ishikawa J, et al. Cornell product left ventricular hypertrophy in electrocardiogram and the risk of stroke in a general population. Hypertension. 2009;53:28–34. doi: 10.1161/HYPERTENSIONAHA.108.118026. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to materials obtained from the military in Taiwan, which were confidential, but are available from the corresponding author on reasonable request.