

Abstract
Background
Instability in the upper cervical spine, although rare, can be devastating. This spectrum of conditions includes occipitocervical instability, atlantoaxial instability and atlantoaxial rotatory displacement. Knowledge of the literature can provide better understanding of disease processes and management, and aid in clinical decision making. The objective of this study was to perform a bibliometric analysis to formulate a comprehensive review of the most cited publications.
Methods
A systematic search of the literature was conducted using the Clarivate Web of Science database. The search query was ‘“Atlanto-occipital dislocation” OR “atlanto-occipital dissociation” OR “atlantoaxial rotatory displacement” OR “atlantoaxial instability”’. The top 100 articles based on frequency of citation were included in our study. Data extracted from articles included frequency of citation, year of publication, country of origin, journal of publication, level of evidence and article type.
Results
Our initial search yielded 257 results that met the criteria. Articles not pertaining to atlanto-occipital instability were removed. Citation frequency ranged from 15 to 195. The most cited article was “Traumatic Anterior Atlanto-Occipital Dislocation” published by Powers et al. in 1979. The most productive decade was 2000–2009 with 45 publications. All decades showed a progressive increase in the number of papers published except for 2010–2019. Overall, 19 countries contributed and the most productive was the United States (n=61). The articles found in our search were cited a total of 4,095 times (3,463 without self-citations) averaging 40.95 citations per publication.
Discussion
The goal of a bibliometric study is to assess trends in a specific field of study, provide evidence for the impact of an individual or field of study’s research, and highlight potential areas for future research. While the number of citations does not necessarily reflect publication quality, it reflects overall influence based on recognition by peers in the field. Publications from the last 20 years have emphasized the use of newer technologies such as computed tomography (CT) and magnetic resonance imaging (MRI) to aid in diagnosis. Our study highlights the lack of high-level evidence articles and underscores that our understanding of these conditions in both pediatric and adult patients is maturing.
Keywords: Upper, cervical, occipitocervical, atlantoaxial, instability
Introduction
The upper cervical spine is an anatomic region consisting of the occiput to the C2-3 disk space and includes the occipitoatlantal and atlantoaxial joints (1). While instability in this spine segment is rare, this spectrum of conditions that includes occipitocervical instability, atlantoaxial instability and atlantoaxial rotatory displacement can cause devastating neurologic compromise in both pediatric and adult patients (2-4). Both occipitocervical and atlantoaxial instability can be either traumatic or acquired. Conditions that predispose patients to acquired upper cervical spine instability include Down’s Syndrome, Morquio syndrome as well as Rheumatoid arthritis (5-7).
Radiographs, computed tomography (CT) and magnetic resonance imaging (MRI) are all useful tools to diagnose these conditions (8-10). Options for management of these conditions range from nonoperative treatment in a collar to halo orthosis and potentially posterior fusion. Spine surgeons, trauma surgeons and pediatric surgeons must take a multitude of patient factors into account as well as an abundance of literature for the proper diagnosis and management of upper cervical spine instability.
Evidence based medicine is becoming an increasingly important component in the practice of the modern surgeon. Knowledge of the literature not only can provide better understanding of disease processes and management, but also can aid in clinical decision making and direct future investigations. However, given this increased focus on evidence-based medicine, the number of publications has been increasing rapidly over the past 100 years (11). Maintaining knowledge based on recent literature can be a daunting task for the modern surgeon.
The increasing volume of publications has given birth to the field of citation analysis, also known as bibliometric study. This refers to the analysis of publications that have had a significant impact on a specific field in medicine (12). In the past, literature reviews and bibliometric analyses have been used to summarize a topic and provide a complete picture of a disease process in spine surgery (10,13-16). Key findings from these studies showed that citations of individual articles ranged from 66 to 1,748. Additionally, these studies showed that the United States tends to yield the most influential and highly cited articles across a field of orthopedic and neurosurgical subspecialties. These bibliometric studies highlight the immense amount of interest garnered from spinal management and treatment. Topics of interest in the field of spinal surgery, as identified in these bibliometric studies, include imaging, clinical descriptions, basic science research and advanced surgical techniques. There is a consensus that the increased citation frequency directly correlates with influence of the findings pertaining to the study. However, many of these bibliometric studies concluded that the field of spinal surgery, pain management, and imaging is saturated with lower level evidence articles. To our knowledge, there is no comprehensive review of the most cited publications pertaining to upper cervical spine instability. Although the number of citations is not the only variable that determines an article’s impact in a field, it can help provide insight into establishing the ‘classic’ articles. Additionally, it can provide residency and fellowship directors with articles that may be important to include in a standardized reading curriculum. Lastly, a thorough understanding of the most cited articles allows investigators to identify the most active areas for research and guide future endeavors (17). Here we present the most cited publications over the past 100 years relating to the epidemiology, anatomy, diagnosis, and treatment of upper cervical spine instability. We present the following article in accordance with the PRISMA reporting checklist (available at https://jss.amegroups.com/article/view/10.21037/jss-21-132/rc).
Methods
Literature search
A systematic search of the literature was conducted using the Clarivate Web of Science database. The search query was ‘“Atlanto-occipital dislocation” OR “atlanto-occipital dissociation” OR “atlantoaxial rotatory displacement” OR “atlantoaxial instability”’. The complete collection of Boolean searches is provided. Initial input of queries yielded 315 distinct articles as shown in Figure 1. Notes, editorials, letters, book chapters, meeting abstracts and early access materials were excluded. There were 285 papers remaining. Non-English studies and animal studies were excluded and we were left with 257 articles. Articles were then sorted from high to low by number of citations as noted by Web of Science. The top 100 articles listed were included in our study.
Figure 1.

PRISMA flow diagram.
Data extraction
Data extracted from articles included article title, total citations, frequency of citation, year of publication, country of origin, journal of publication, level of evidence, article type, affiliated institution, institution of the corresponding author and names of contributing authors. Articles were grouped by decade of publication. Articles were categorized into biomechanics, case reports, classifications, clinical descriptions, clinical outcomes, imaging, natural history, surgical techniques or pathology. Articles were classified based on their abstract. If an article’s category was unclear from the abstract, the complete paper was assessed to determine the proper category. The articles were also classified based on whether they involved pediatric or adult patients. We recorded all authors on each paper as well as their affiliated institutions. Lastly, articles were grouped by decade of publication.
Level of evidence was assigned based on a 5-tier system (19). Level one literature included randomized control trials and meta-analyses. Level two studies were experimental studies with or without literature reviews. Level three articles included systematic reviews, non-experimental and qualitative studies. Level four papers were literature reviews, clinical guidelines, related descriptions, and outcome articles. Finally, level five categorization was dominated by case reports, small sample size studies, opinion pieces and expert recommendation articles. Article type and level of evidence was assigned after careful review of abstracts and full-text. The classification of these articles was completed by 2 separate authors and their results were compared. Any discrepancies between the levels of evidence assigned were discussed until a level of evidence was agreed upon.
Results
The most cited article was “Traumatic Anterior Atlanto-Occipital Dislocation” published by Powers et al. in 1979. The most productive decade was 2000–2009 followed by 1990–1999 with 45 and 26 publications respectively. All decades showed a progressive increase in the number of papers published except for 2010–2019 as shown in Figure 2. The range of publication years included articles from 1959 to 2018. The most popular year of publication was 2011 with 11 publications. The article published the earliest was non-traumatic atlanto-occipital and atlanto-axial dislocation: a case report by Washington. The most recent article was Motion and dural sac compression in the upper cervical spine during the application of a cervical collar in case of unstable craniocervical junction-A study in two new cadaveric trauma models by Liao et al. published in 2018.
Figure 2.
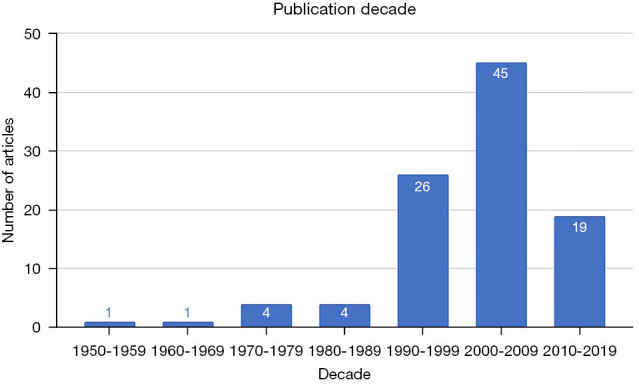
Number of publications based on decade.
The country of origin was also assessed for all articles in our list. All countries affiliated with the authors were included. If multiple countries were listed, they were included as separate entries. Overall, 19 countries contributed and the most prominent country featured was the United States (n=61) followed by Canada (n=7) with England, Japan and Germany tied for third (n=5). Notably, there were 8 countries that contributed to three or more articles on the list as shown in Figure 3.
Figure 3.
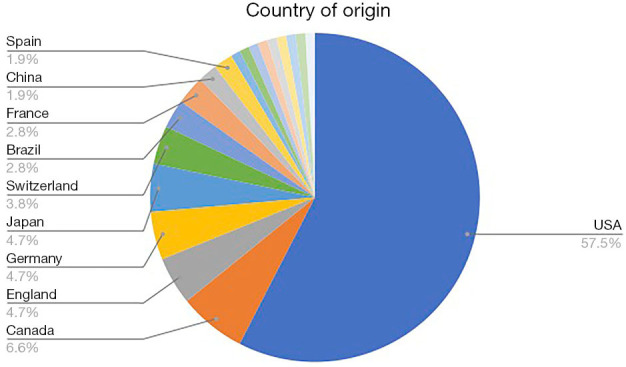
Proportion of publications based on country of origin.
The articles found in our search were collectively cited a total of 4,095 times (3,463 times without self-citations). This averaged out to 40.95 citations per publication. The most cited paper on our list was Traumatic Anterior Atlanto-Occipital Dislocation, cited a total of 195 times according to Web of Science. In second place is Pathological Anatomy of Fatal Atlanto-occipital dislocations by Buchholz et al. The third most cited article found in our search was Pediatric Cervical Spine Injuries: Defining the Disease by Patel et al.
The most productive authors were Dickman with 4 publications followed by Vaccaro and Woodring with 3 publications each. The institutions tied for the most articles on our list were Barrow Neurological Institute and the University of California with five publications each. Many institutions were tied for second place with 3 publications from our list. The journal that published the majority of articles on our list was Spine with 14 publications followed by Neurosurgery and The Journal of Bone and Joint Surgery with 10 and 6 publications respectively. A total of 46 journals contributed to our list. The most prominent level of evidence was level 4 (n=55) followed by level 5 with 39 articles. The most common article type was tied between case reports and clinical descriptions with 31 articles each. In second place was imaging with 15 articles followed by clinical outcomes as seen in Figure 4.
Figure 4.
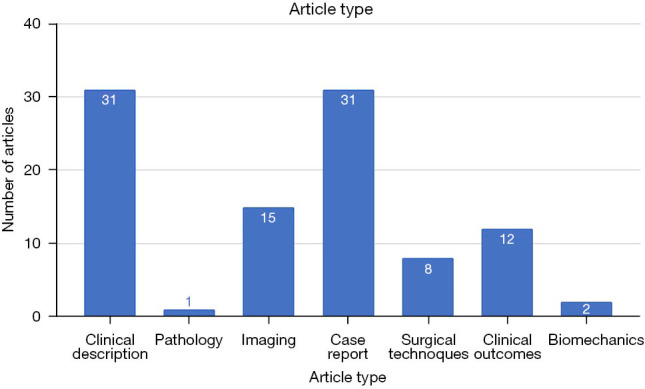
Number of publications based on article type.
Discussion
The goal of a bibliometric study is to assess trends in a specific field of study, provide evidence for the impact of an individual or field of study’s research, and highlight potential areas for future research (12). Article subjects presented from our database are provided in Figure 5. A bibliometric study can prove particularly useful when evaluating a topic with a wide body of literature. While the number of citations does not necessarily reflect publication quality, it reflects overall influence based on recognition by peers in the field. The number of times an article is cited depends on the quality of the work, overall interest in the topic discussed, and the ability of the article to inspire further research or to change the way physicians practice. Upper cervical instability is a topic that can have a devastating effect if it is not recognized and treated promptly.
Figure 5.
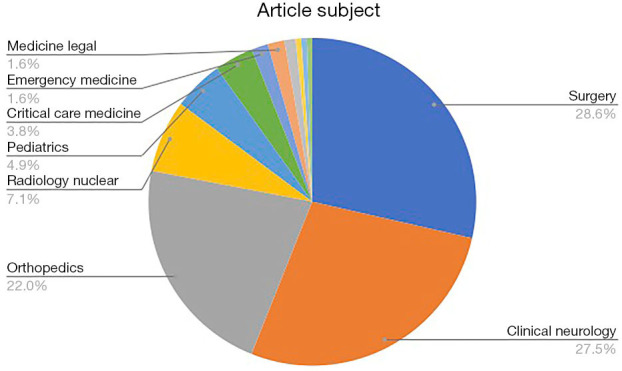
Proportion of publications based on subject of articles.
In pediatric patients, three commonly recognized pathologies in the upper cervical spine are atlanto-occipital dislocation, atlanto-axial instability and atlantoaxial rotatory subluxation. The atlanto-occipital joint is a condylar joint with minimal bony stability, primarily stabilized by ligaments including the tectorial membrane, anterior longitudinal ligament, nuchal ligament and paired alar ligaments. The mechanism typically involves a deceleration mechanism, causing separation of the condyles and the atlas. CT has become the gold standard for diagnosis, with the condyle-C1 interval greater than 4 mm being cited as valuable in the diagnosis in recent studies. Initial treatment involves immobilization in a halo or Minerva cast but unstable injuries should be managed with posterior occipitoatlantal fusion with internal fixation (20,21).
Atlantoaxial instability can be caused by traumatic ligamentous injury or chronic disease processes; associations with Downs syndrome is well documented with the frequency of atlantoaxial instability approaching 10% to 30% by adolescence (22-25). Other sources have associated Reiter syndrome, Larsen syndrome, juvenile rheumatoid arthritis, Morquio syndrome and Kniest syndrome (22,26-30). In traumatic injuries, the transverse ligament is disrupted. Diagnosis is made with lateral cervical radiographs or a CT scan to measure the atlanto-dens interval. The spine is reduced in extension followed by surgical stabilization of C1-2 and a prolonged period of immobilization in a halo, Minerva cast or cervical orthosis.
Atlantoaxial rotatory subluxation in children typically results from minor trauma or infection. If due to an infectious etiology, it is known as Grisel syndrome and typically occurs after an upper respiratory tract infection. In contrast to muscular torticollis, the chin will be pointed towards the side on which the sternocleidomastoid is contracted. Diagnosis may be challenging due to positioning difficulties (31). On anteroposterior and open-mouth odontoid views, the lateral masses appear different in size because one is rotated anteriorly and one posteriorly. CT has also proven useful and can show the atlas superimposed on the axis in a rotated position (32,33). Treatment of atlantoaxial rotatory subluxation depends on timing of injury and duration of symptoms (34). Many children will not require medical attention due to spontaneous reduction. Those with symptoms less than 1 week in duration can be treated in a soft collar with anti-inflammatories and home exercises. Halter traction and bed rest is required if spontaneous reduction does not occur after 1 week. In subluxations greater than 1 month in duration, reduction with halter traction is unlikely and may require the use of a halo (35).
In adults, the spectrum of upper cervical spine instability encompasses atlanto-occipital injuries, atlantoaxial subluxation and dislocation and finally rupture of the transverse ligament. Atlanto-occipital injury typically occurs as the result of a motor vehicle accident. Children are predisposed to this injury because their occipitoatlantal joints are flatter and because their head weight to bodyweight ratio is greater than adults. There are multiple radiographic methods described to diagnose atlanto-occipital injuries that utilize the relationship between the occiput and C1 to assess any instability including the Powers ratio (36). The mortality is extremely high from this injury and only 20% of patients will have a normal neurologic examination (37). All atlanto-occipital injuries should be treated with immediate halo application.
Atlantoaxial subluxation and dislocation in adults is most common after motor vehicle accidents. Similar to children, adults will present with a ‘cock robin’ appearance with the head tilted toward and rotated away from the side of dislocation. X-rays commonly demonstrate asymmetry of the lateral masses on an open-mouth odontoid view. Skull tong traction is used for reduction. Should closed reduction fail, open reduction is performed and a posterior C1-C2 fusion is performed. There are multiple ways of accomplishing this including the Gallie technique, the Brooks technique, and C1-C2 transarticular screws supplemented by posterior fusion.
Lastly ruptures of the transverse ligament can cause instability in the upper cervical spine. Diagnosis is most commonly performed using a combination of MRI, CT and dynamic radiographs (38). Insufficiency of the transverse ligament is suspected if the atlantodens interval is greater than 3.5 mm in adults and 5 mm in children. Treatment typically involves C1-C2 fusion using the aforementioned techniques.
Atlanto-occipital instability was first documented in the literature by Bell in 1830 (39). This was the first reported subluxation of the atlas on the axis. This event occurred following an infection that developed from a pharyngeal ulcer. Subsequently, multiple cases reported subluxation events following infection or ligamentous laxity (40-43). Blackwood documented the first case of atlanto-occipital dislocation due to traumatic injury in 1908 (44). The article published the earliest on our list of the 100 most cited articles was Non-Traumatic Atlanto-Occipital and Atlanto-Axial Dislocation by Washington. This article provided a unique case report of dislocation of both the atlanto-occipital and atlanto-axial joints after pharyngitis in a young female patient and correlated her condition with radiographic findings (45).
The most cited article found in our search was Traumatic Anterior Atlanto-occipital Dislocation by Powers et al. In this landmark review, Powers et al. reported 4 cases of traumatic atlanto-occipital dislocation and established new radiographic criteria to diagnose this condition based on the ratio of the distances between the basion and posterior arch of C1 to the distance between the opisthion and the anterior arch of C1. While traumatic atlanto-occipital instability had been documented in the literature 4 times prior to this paper, previous studies had used the relationship between the atlas, odontoid, and basion for radiographic diagnosis, as first documented by Wholey et al. in 1958 (46). Powers developed new diagnostic criteria based on a relationship between two anatomic structures as opposed to absolute measurements between structures. The new diagnostic criteria established by Powers is still used today (36).
Bucholz et al. authored the article with the second most citations, providing a post-mortem examination of 9 patients with fatal atlanto-occipital dislocations after motor vehicle accidents (47). In this study, they found that 6 of their 9 patients had no fracture in the cervical spine and postulated that ligamentous injury can be a significant factor in the development of atlanto-occipital dislocation.
The third most-cited article on upper cervical spine instability was Pediatric Cervical Spine Injuries: Defining the Disease by Patel et al. In this retrospective review, the incidence and characteristics of pediatric cervical spine injuries as well as the impact of age and level of injury on mortality rate was assessed. One key finding was that 23% of children with upper cervical spine injury died compared to only 4% with lower cervical spine injury. Additionally, mortality rate was highest (48%) in those children diagnosed with atlanto-occipital dislocation (48). Interestingly, despite this high mortality rate, only 9% of the 100 most cited publications pertained specifically to pediatric patients according to Web of Science. This suggests that the literature on pediatric upper cervical instability is either newer and has not had the chance to accumulate citations or there is a lack of articles being published compared to the adult population.
The year with the most articles on our list was 2001 with 11 publications followed by 2005 and 2007 with 8 and 7 publications respectively. These three years contributed to making 2000–2009 the most productive decade with 45 publications followed by 1990–1999 and 2010–2019 with 26 and 19 publications respectively. This reflects the time delay in which newer literature gains citations, putting more recent articles at a disadvantage. The lack of articles on our list from earlier decades including 1970–1979, 1980–1989, and 1990–1999 can likely be attributed to more recent articles creating a lasting impact with the incorporation of advanced imaging such as CT and MRI. The internet has also allowed practitioners to share research data and established treatment guidelines and we believe this is part of the reason why 2000–2009 was the most productive decade. Lastly, the number of publications increasing in later decades may be attributed to an overall increase in publication rate and citations (49,50).
Level of evidence is substantially impacted by the article type. This is evident in that case reporting generates lower level evidence studies while biomechanical evaluations, clinical outcomes and clinical descriptions produce higher level evidence. The collective level of evidence regarding upper cervical instability is analyzed and the effector size of each type of study on the pooled level of evidence is shown in Figure 6. There was a lack of high level of evidence articles found in our search, with 55 articles being classified as level 4 and 39 articles being classified as level 5 as seen in Figure 7. These findings are consistent with other studies regarding craniovertebral dislocation discussed in Klepinowski et al. In this meta-analysis, the first limitation cited is the lack of studies categorized as high-level evidence. In fact, in the 46 full text articles analyzed, the highest-level evidence studies were level IV (51). The paucity of randomized controlled trials or experimental studies provides insight into what type of studies are needed in the future to advance our understanding of upper cervical spine instability.
Figure 6.
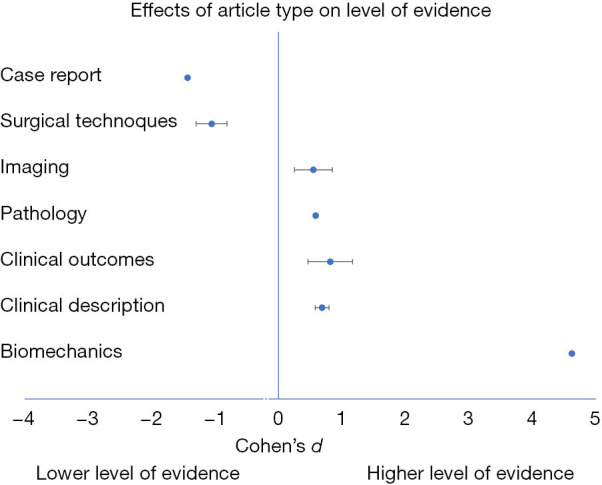
Effect size of article type on the level of evidence.
Figure 7.
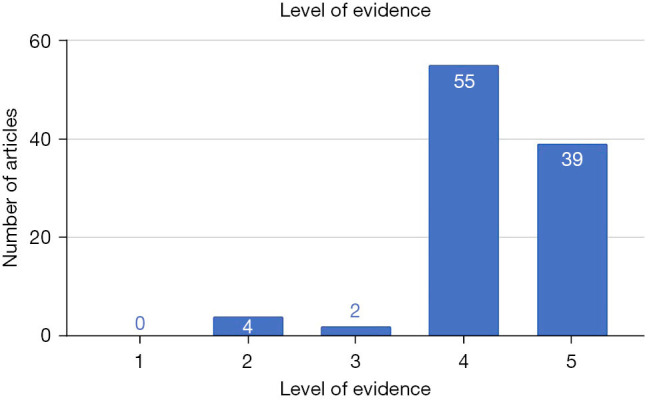
Number of publications based on level of evidence. Assigned levels of criteria was determined by multiple authors and consensus agreements.
There are several limitations to our bibliometric analysis. Firstly, newer articles published after our literature search was completed could change the order of citations. This is unlikely given that it takes several years to accumulate citations. In addition, including 100 articles was an arbitrary decision. However, the authors felt that 100 articles was an adequate number to provide a complete picture of the classic literature regarding the diagnosis and management of upper cervical spine instability. Furthermore, high impact articles that were written in languages other than English were excluded. It is possible that there are high impact articles in other languages that may have been pertinent to include.
Another limitation was the main criterion we used to assess which articles were the most influential, the number of citations. While the number of citations is a useful indicator regarding the popularity of an article, it may not be a reliable indicator of article quality as it can be affected by multiple factors including journal impact, author reputation and research specialty. We also did not account for author self-citations, and as such higher volume authors may be more likely to cite their own work or to cite articles in journals where they are seeking publication. Also not accounted for were citations in textbooks, lectures or other non-peer-reviewed and web-based literature that is not included in Web of Science.
A ‘snowball effect’ has been hypothesized where authors are more likely to cite an article based on its number of citations rather than the content or quality of the article (52). We do not believe this hypothesis severely altered our results. Lastly, this is a cross-sectional study. Future studies would benefit from tracking the number of citations an article has received over time to reflect paradigm shifts in the diagnosis and treatment of upper cervical spine instability.
Conclusions
Upper cervical spine instability is a complex spectrum of pathology that can affect both pediatric and adult patients. The diagnosis and management of this spectrum of conditions has been studied by orthopedic surgeons, neurosurgeons, trauma surgeons and neurologists alike. In this article, we attempted to provide a comprehensive review of the most influential literature pertaining to this topic published over the last 100 years. Publications from the last 20 years have emphasized the use of newer technologies such as computed tomography and magnetic resonance imaging to aid in the diagnosis of upper cervical spine instability. Our article highlights the lack of high level of evidence articles pertaining to this topic and underscores the fact that our understanding of these conditions is still maturing. We believe this article can help practitioners as well as future investigators navigate the wide body of literature surrounding this topic and aid in future discovery.
Acknowledgments
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Open Access Statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
Footnotes
Reporting Checklist: The authors have completed the PRISMA reporting checklist. Available at https://jss.amegroups.com/article/view/10.21037/jss-21-132/rc
Peer Review File: Available at https://jss.amegroups.com/article/view/10.21037/jss-21-132/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jss.amegroups.com/article/view/10.21037/jss-21-132/coif). The authors have no conflicts of interest to declare.
References
- 1.Wills BP, Dormans JP. Nontraumatic upper cervical spine instability in children. J Am Acad Orthop Surg 2006;14:233-45. 10.5435/00124635-200604000-00005 [DOI] [PubMed] [Google Scholar]
- 2.Greenberg AD. Atlanto-axial dislocations. Brain 1968;91:655-84. 10.1093/brain/91.4.655 [DOI] [PubMed] [Google Scholar]
- 3.Sun PP, Poffenbarger GJ, Durham S, et al. Spectrum of occipitoatlantoaxial injury in young children. J Neurosurg 2000;93:28-39. [DOI] [PubMed] [Google Scholar]
- 4.McGrory BJ, Klassen RA, Chao EY, et al. Acute fractures and dislocations of the cervical spine in children and adolescents. J Bone Joint Surg Am 1993;75:988-95. 10.2106/00004623-199307000-00004 [DOI] [PubMed] [Google Scholar]
- 5.Schwarze M, Akbar M. Atraumatic Atlantoaxial Subluxation-Grisel Syndrome. Dtsch Arztebl Int 2020;117:773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Takahata M, Abumi K, Sudo H, et al. Cervical myelopathy due to atraumatic odontoid fracture in patients with rheumatoid arthritis: A case series. Mod Rheumatol 2017;27:901-4. 10.3109/14397595.2015.1029222 [DOI] [PubMed] [Google Scholar]
- 7.Larsson SE, Toolanen G. Posterior fusion for atlanto-axial subluxation in rheumatoid arthritis. Spine (Phila Pa 1976) 1986;11:525-30. 10.1097/00007632-198607000-00004 [DOI] [PubMed] [Google Scholar]
- 8.Perovic MN, Kopits SE, Thompson RC. Radiological evaluation of the spinal cord in congenital atlanto-axial dislocation. Radiology 1973;109:713-6. 10.1148/109.3.713 [DOI] [PubMed] [Google Scholar]
- 9.Weng MS, Haynes RJ. Flexion and extension cervical MRI in a pediatric population. J Pediatr Orthop 1996;16:359-63. 10.1097/01241398-199605000-00013 [DOI] [PubMed] [Google Scholar]
- 10.Das JP, Aherne E, Kavanagh E. Imaging of the Spine: A Bibliometric Analysis of the 100 Most-Cited Articles. Spine (Phila Pa 1976) 2019;44:1593-8. 10.1097/BRS.0000000000003131 [DOI] [PubMed] [Google Scholar]
- 11.Larsen PO, von Ins M. The rate of growth in scientific publication and the decline in coverage provided by Science Citation Index. Scientometrics 2010;84:575-603. 10.1007/s11192-010-0202-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Elder A. Library Guides:Research Methodologies Guide: Bibliometrics. Available online: https://instr.iastate.libguides.com/c.php?g=49332&p=318077
- 13.Huang W, Wang L, Wang B, et al. Top 100 Cited Articles on Back Pain Research: A Citation Analysis. Spine (Phila Pa 1976) 2016;41:1683-92. 10.1097/BRS.0000000000001736 [DOI] [PubMed] [Google Scholar]
- 14.Lefaivre KA, Shadgan B, O'Brien PJ. 100 most cited articles in orthopaedic surgery. Clin Orthop Relat Res 2011;469:1487-97. 10.1007/s11999-010-1604-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Namdari S, Baldwin K, Kovatch K, et al. Fifty most cited articles in orthopedic shoulder surgery. J Shoulder Elbow Surg 2012;21:1796-802. 10.1016/j.jse.2011.11.040 [DOI] [PubMed] [Google Scholar]
- 16.Zhao T, Shen J, Zhang J, et al. Top 100 Cited Articles on Spinal Disc Arthroplasty Research. Spine (Phila Pa 1976) 2020;45:1530-6. 10.1097/BRS.0000000000003608 [DOI] [PubMed] [Google Scholar]
- 17.Zhang Y, Wumaier M, He D, et al. The 100 Top-Cited Articles on Spinal Deformity: A Bibliometric Analysis. Spine (Phila Pa 1976) 2020;45:275-83. 10.1097/BRS.0000000000003247 [DOI] [PubMed] [Google Scholar]
- 18.Haddaway NRAUPCC, McGuinness LA. PRISMA2020: R package and ShinyApp for producing PRISMA 2020 compliant flow diagrams (Version 0.0.2). Zenodo 2021. [DOI] [PMC free article] [PubMed]
- 19.A P. Research Hub: Evidence Based Practice Toolkit: Levels of Evidence.
- 20.Theodore N, Aarabi B, Dhall SS, et al. The diagnosis and management of traumatic atlanto-occipital dislocation injuries. Neurosurgery 2013;72 Suppl 2:114-26. 10.1227/NEU.0b013e31827765e0 [DOI] [PubMed] [Google Scholar]
- 21.MD SRG MF, MD GRB, MD CMB, et al. Rothman-Simeone and Herkowitz’s The Spine. 7 ed. Elsevier, editor2017. [Google Scholar]
- 22.Burke SW, French HG, Roberts JM, et al. Chronic atlanto-axial instability in Down syndrome. J Bone Joint Surg Am 1985;67:1356-60. 10.2106/00004623-198567090-00008 [DOI] [PubMed] [Google Scholar]
- 23.Pueschel SM, Scola FH. Atlantoaxial instability in individuals with Down syndrome: epidemiologic, radiographic, and clinical studies. Pediatrics 1987;80:555-60. 10.1542/peds.80.4.555 [DOI] [PubMed] [Google Scholar]
- 24.Winell J, Burke SW. Sports participation of children with Down syndrome. Orthop Clin North Am 2003;34:439-43. 10.1016/S0030-5898(03)00010-5 [DOI] [PubMed] [Google Scholar]
- 25.Atlantoaxial instability in Down syndrome: subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-4. 10.1542/peds.96.1.151 [DOI] [PubMed] [Google Scholar]
- 26.Dawson EG, Smith L. Atlanto-axial subluxation in children due to vertebral anomalies. J Bone Joint Surg Am 1979;61:582-7. 10.2106/00004623-197961040-00015 [DOI] [PubMed] [Google Scholar]
- 27.Hammerschlag W, Ziv I, Wald U, et al. Cervical instability in an achondroplastic infant. J Pediatr Orthop 1988;8:481-4. 10.1097/01241398-198807000-00021 [DOI] [PubMed] [Google Scholar]
- 28.Kobori M, Takahashi H, Mikawa Y. Atlanto-axial dislocation in Down's syndrome. Report of two cases requiring surgical correction. Spine (Phila Pa 1976) 1986;11:195-200. 10.1097/00007632-198604000-00003 [DOI] [PubMed] [Google Scholar]
- 29.Kransdorf MJ, Wehrle PA, Moser RP, Jr. Atlantoaxial subluxation in Reiter's syndrome. A report of three cases and review of the literature. Spine (Phila Pa 1976) 1988;13:12-4. 10.1097/00007632-198801000-00004 [DOI] [PubMed] [Google Scholar]
- 30.Miz GS, Engler GL. Atlanto-axial subluxation in Larsen's syndrome. A case report. Spine (Phila Pa 1976) 1987;12:411-2. 10.1097/00007632-198705000-00024 [DOI] [PubMed] [Google Scholar]
- 31.Maheshwaran S, Sgouros S, Jeyapalan K, et al. Imaging of childhood torticollis due to atlanto-axial rotatory fixation. Childs Nerv Syst 1995;11:667-71. 10.1007/BF00262228 [DOI] [PubMed] [Google Scholar]
- 32.Geehr RB, Rothman SL, Kier EL. The role of computed tomography in the evaluation of upper cervical spine pathology. Comput Tomogr 1978;2:79-97. 10.1016/0363-8235(78)90006-6 [DOI] [PubMed] [Google Scholar]
- 33.Scapinelli R. Three-dimensional computed tomography in infantile atlantoaxial rotatory fixation. J Bone Joint Surg Br 1994;76:367-70. 10.1302/0301-620X.76B3.8175835 [DOI] [PubMed] [Google Scholar]
- 34.Phillips WA, Hensinger RN. The management of rotatory atlanto-axial subluxation in children. J Bone Joint Surg Am 1989;71:664-8. 10.2106/00004623-198971050-00004 [DOI] [PubMed] [Google Scholar]
- 35.Burkus JK, Deponte RJ. Chronic atlantoaxial rotatory fixation correction by cervical traction, manipulation, and bracing. J Pediatr Orthop 1986;6:631-5. 10.1097/01241398-198609000-00021 [DOI] [PubMed] [Google Scholar]
- 36.Powers B, Miller MD, Kramer RS, et al. Traumatic anterior atlanto-occipital dislocation. Neurosurgery 1979;4:12-7. 10.1227/00006123-197901000-00004 [DOI] [PubMed] [Google Scholar]
- 37.Hadley MN, Zabramski JM, Browner CM, et al. Pediatric spinal trauma. Review of 122 cases of spinal cord and vertebral column injuries. J Neurosurg 1988;68:18-24. 10.3171/jns.1988.68.1.0018 [DOI] [PubMed] [Google Scholar]
- 38.Dickman CA, Greene KA, Sonntag VK. Injuries involving the transverse atlantal ligament: classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50. 10.1097/00006123-199601000-00012 [DOI] [PubMed] [Google Scholar]
- 39.Charles Bell "The nervous system of the human body" 1830. Brain Nerve 2007;59:440-1. [PubMed] [Google Scholar]
- 40.Berkheiser EJ, Seidler F. Nontraumatic dislocations of the atlanto-axial joint. J Am Med Assoc 1931;96:517-23. 10.1001/jama.1931.02720330037010 [DOI] [Google Scholar]
- 41.Lippmann RK. Arthropathy due to adjacent inflammation. J Bone Joint Surg Am 1953;35-A:967-79. 10.2106/00004623-195335040-00015 [DOI] [PubMed] [Google Scholar]
- 42.STEIN F , BLOCH H, KENIN A. Nontraumatic subluxation of the atlanto-axial articulation. J Am Med Assoc 1953;152:131-2. 10.1001/jama.1953.63690020005004b [DOI] [PubMed] [Google Scholar]
- 43.Jones RW. Spontaneous Hyperæmic Dislocation of the Atlas 1932. Available online: https://journals.sagepub.com/doi/abs/10.1177/003591573202500499
- 44.Blackwood NJ. III. Atlo-Occipital Dislocation: A Case of Fracture of the Atlas and Axis, and Forward Dislocation of the Occiput on the Spinal Column, Life being Maintained for Thirty-four Hours and Forty Minutes by Artificial Respiration, during which a Laminectomy was Performed upon the Third Cervical Vertebra. Ann Surg 1908;47:654-8. 10.1097/00000658-190805000-00003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Washington ER. Non-traumatic atlanto-occipital and atlanto-axial dislocation; a case report. J Bone Joint Surg Am 1959;41-A:341-4. 10.2106/00004623-195941020-00015 [DOI] [PubMed] [Google Scholar]
- 46.Wholey MH, Bruwer AJ, Baker HL, Jr. The lateral roentgenogram of the neck; with comments on the atlanto-odontoid-basion relationship. Radiology 1958;71:350-6. 10.1148/71.3.350 [DOI] [PubMed] [Google Scholar]
- 47.Bucholz RW, Burkhead WZ. The pathological anatomy of fatal atlanto-occipital dislocations. J Bone Joint Surg Am 1979;61:248-50. 10.2106/00004623-197961020-00014 [DOI] [PubMed] [Google Scholar]
- 48.Patel JC, Tepas JJ, 3rd, Mollitt DL, et al. Pediatric cervical spine injuries: defining the disease. J Pediatr Surg 2001;36:373-6. 10.1053/jpsu.2001.20720 [DOI] [PubMed] [Google Scholar]
- 49.Garner RM, Hirsch JA, Albuquerque FC, et al. Bibliometric indices: defining academic productivity and citation rates of researchers, departments and journals. J Neurointerv Surg 2018;10:102-6. 10.1136/neurintsurg-2017-013265 [DOI] [PubMed] [Google Scholar]
- 50.Jones LB, Goel S, Hung LY, et al. Objective Methodology to Assess Meaningful Research Productivity by Orthopaedic Residency Departments: Validation Against Widely Distributed Ranking Metrics and Published Surrogates. J Orthop Trauma 2018;32:e139-44. 10.1097/BOT.0000000000001106 [DOI] [PubMed] [Google Scholar]
- 51.Klepinowski T, Limanówka B, Sagan L. Management of post-traumatic craniovertebral junction dislocation: A PRISMA-compliant systematic review and meta-analysis of casereports. Neurosurg Rev 2021;44:1391-400. 10.1007/s10143-020-01366-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Khatra O, Shadgan A, Taunton J, et al. A Bibliometric Analysis of the Top Cited Articles in Sports and Exercise Medicine. Orthop J Sports Med 2021;9:2325967120969902. 10.1177/2325967120969902 [DOI] [PMC free article] [PubMed] [Google Scholar]