

Abstract
Background
The radial head is anatomically complex, making fracture fixation challenging because of the difficult visualization of the articular surface. As a result, screw penetration into the radiocapitellar joint can often occur. To facilitate safe placement of screws tangential to the joint surface, we define an approximate and reliable distance from the articular rim of the radial head that can minimize the risk of articular breach.
Methods
A Kirschner wire for cannulated drilling was placed tangential to the articular surface in 15 cadaveric proximal radii. The distance from the wire to the articular rim was measured 3 times. After insertion of a 3.5-mm compression screw, the radial head was divided in the coronal plane, bisecting the screw track, to visualize the cross section of the screw's position. Headless compression screws of 3.5 mm were placed the distance from the most proximal edge of the screw track to the radial head's articular surface was measured 3 times.
Results
The average distance from the articular rim to the distal surface of the Kirschner wire was 5.1 mm. The average distance from the articular rim to the proximal edge of the cavity was 1.7 mm. The screw placement was subchondral and extra-articular in all cases.
Conclusion
When fixing Mason type 2 articular radial head fractures with 3.5-mm headless compression screws placed tangential to the articular surface, maintaining a screw entry point about 5 mm distal to the articular surface of the radial head will minimize the possibility of articular screw breach. This position also places the screw into subchondral bone, providing the best bone quality for mechanical support.
Keywords: Articular screw penetration, Headless compression screws, Fracture fixation, Open reduction internal fixation, Radial head fracture, Radiocapitellar screw breach
Fractures of the radial head are common injuries that comprise a third of all elbow fractures.2 The mechanism of injury is often a fall onto a pronated outstretched arm,16 and patients tend to be active and aged between 20 to 60 years. Surgical fixation is indicated in displaced articular fractures with significant loss of joint congruity or restricted elbow motion.17 Open reduction and fixation of unstable and displaced radial head fractures are generally recommended to preserve the radiocapitellar joint and allow early motion to minimize elbow stiffness.
The Mason Classification is the most common classification system for radial head fractures, categorized as Types 1, 2, and 3. Type 1 fractures are minimally displaced and are often treated nonoperatively with early range of motion. Type 2 fractures can be treated with or without surgery, but internal fixation may be indicated when displacement is >2 mm with loss of articular congruity and loss of elbow range motion. Headless compression screw fixation with 2.5 or 3.5 mm screws is an option when articular fractures extend into the joint with a plane perpendicular to the articular surface. Anatomical landmarks can be used intraoperatively to maximize the use of subchondral bone support and prevent articular screw penetration.8,21
The radial head is anatomically complex. The articular surface of the radial head is deeply concave and articulates with the convexity of the capitellar articular surface (Fig. 1).20,22 Consequently, the whole of the articular surface of the radial head may be difficult to visualize as it is obscured by the proximal projection of the articular rim of the radial head. This can give the impression of radiocapitellar joint congruity when viewed on radiograph. Computerized tomography scans can be helpful in preoperative planning operative fixation is mainly performed under fluoroscopic guidance without direct visualization of the radial head concavity. Operative fixation of radial head fractures can be technically difficult, and screw trajectory can be challenging. The screws are straight, and the joint surface is curved. Consequently, the screws cannot be placed parallel to the joint surface but should be placed tangential to the joint surface to avoid articular breach.
Figure 1.
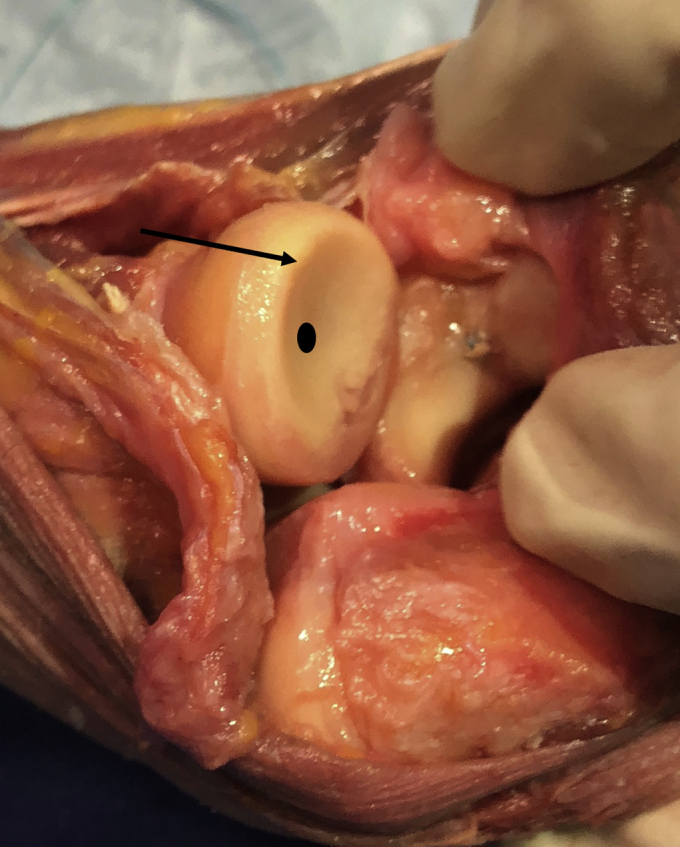
Anatomical dissection of the radial head showing the deep concavity ( ) that may be breached by the screw during radial head fracture fixation. The base of the concavity sits approximately 5 mm distal to the radial head rim (
) that may be breached by the screw during radial head fracture fixation. The base of the concavity sits approximately 5 mm distal to the radial head rim ( ).
).
Visualizing articular breach is difficult and may not be recognized. The distance of the articular concavity from the articular rim has not been defined. The screw location should be optimized to position the screw within the subchondral bone, which maximizes articular support.25 The aim of our study was to define an optimal distance from the articular rim of the radial head for screws tangential to the articular surface that (1) prevents articular breach of radial head screws and (2) places the screws within the subchondral bone.
Materials and methods
Fifteen cadaveric proximal radii were used from donors aged between 50 and 88 years with a weight range of 37.65-81.65 kilograms, allowing for various radial head sizes. Under anteroposterior fluoroscopic view, we used 0.062-inch Kirschner wires (K-wire) to drill tangential to the radiocapitellar joint and as close as possible to the deep surface of the subchondral bone plate (Fig. 2, a and b). This region is the ideal location for screw placement. The subchondral bone plate is darker than the metaphyseal bone and thus easily visualized on fluoroscan. The distance from the distal surface of the K-wire to the articular rim of the radial head was measured 3 times using a digital caliper. The average of the 3 measurements was reported.
Figure 2.

(a) Kirschner wire insertion and (b) headless compression screw placement under fluoroscopic guidance.
Using the K-wire as a guide, we used a cannulated 2.7-mm drill to create a trajectory for placement of the 3.5-mm headless compression screw (REDUCT; Skeletal Dynamics, Miami, FL, USA). Screws that are 2.5 mm or 3.5 mm are appropriate for fixation of large radial head fracture fragments. We chose a 3.5-mm screw because it is the largest diameter screw that may be used for fixation of radial head fractures, so it maximized the possibility of articular breach (Fig. 3). An osteotomy was performed at the level of the radial neck cut, and the radial head was removed. The screws were then removed, and the radial head was sectioned in the coronal plane, bisecting, and exposing the screw track (Fig. 3, a). Next, we measured the most proximal edge of the screw track to the articular surface of the radial head (Fig. 3, b). The distance from the rim of the radial head to the subchondral bone was determined by visualization on fluoroscan and after sectioning the radial head coronally and observing the distance from the subchondral bone to the edge of the outer articular surface. The specimens were randomized at 3 separate times and presented to the surgeon to obtain measurements.
Figure 3.

The isolated radial head. (a) An osteotomy in line with the screw track (shown with screw placed in concavity). (b) The distance from the most proximal edge of the screw track to the deepest part of the articular surface.
Statistical analysis
All data are reported as an average plus or minus standard deviation. Grubbs's outlier tests were used to remove outliers with 95% confidence intervals (alpha value 0.05). The intrarater reliability was estimated using the intraclass correlation coefficient (ICC). The ICC was calculated using the “psych” package in R. The ICC is reported along with the 95% confidence interval. The ICC was calculated based on a mean-rating (k = 3), absolute-agreement, 2-way mixed effects model.19
Results
The average distance from the articular rim to the distal surface of the K-wire was 5.1 mm ± 0.7 mm (range, 3.6-6.3 mm). None of the 3.5 mm variable pitched screws breached the articular surface, and all the K-wire were located in subchondral bone. The average distance from the most proximal edge of the screw track to the deepest part of the articular surface was 1.7 mm ± 0.4 mm (range 0.9-2.6 mm). The distance from the articular surface to the proximal edge of the screw track versus the distance from the articular rim to the distal surface of the K-wire is shown in Fig. 4. The graph and linear regression model of the data did not show a linear relationship between the 2 measurements (P = .95). The screw track did not breach the joint. The K-wire measurement ICC was 0.77 (0.60, 0.89). The screw measurement ICC was 0.86 (0.74, 0.94). These values for the ICC are considered good reliability (0.75-0.90).19
Figure 4.
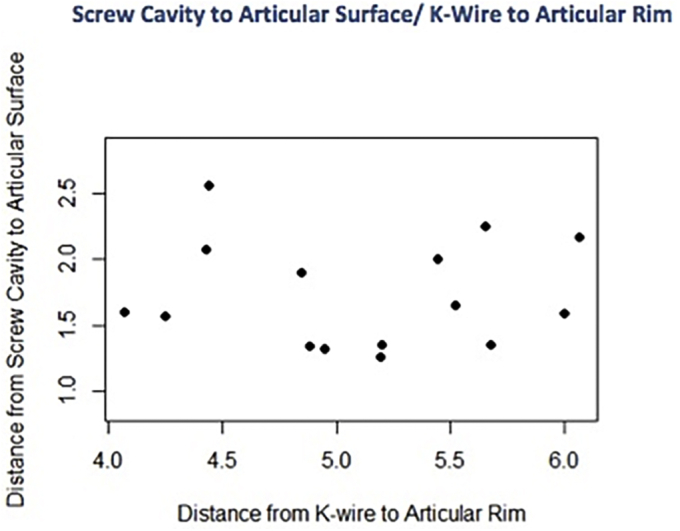
Scatter plot of distance from deepest part of the articular surface to the proximal edge of the screw track versus distance from the articular rim to the distal surface of the K-wire, showing no linear relationship between the 2 measurements.
Discussion
Operative fixation of radial head fractures can be a challenge because of the anatomy of the radial head.17,20 The articular surface is a concavity not well visualized in Mason type 2 fractures on flouroscan, with an accuracy of detection of implant breach of 73%. 9 This is due to the rim of the radius projecting past the base of the center of the radial head (Fig. 5).To ensure screws are subchondral and extra-articular, the surgeon should place them approximately 5 mm distal to the articular rim (5.1 mm ± 0.7 mm). With this entry point, the average distance of these screws to subchondral bone was 1.7 ± 0.4 mm. It is important to place the screws subchondral because the subchondral bone provides the best fixation to axial load.
Figure 5.
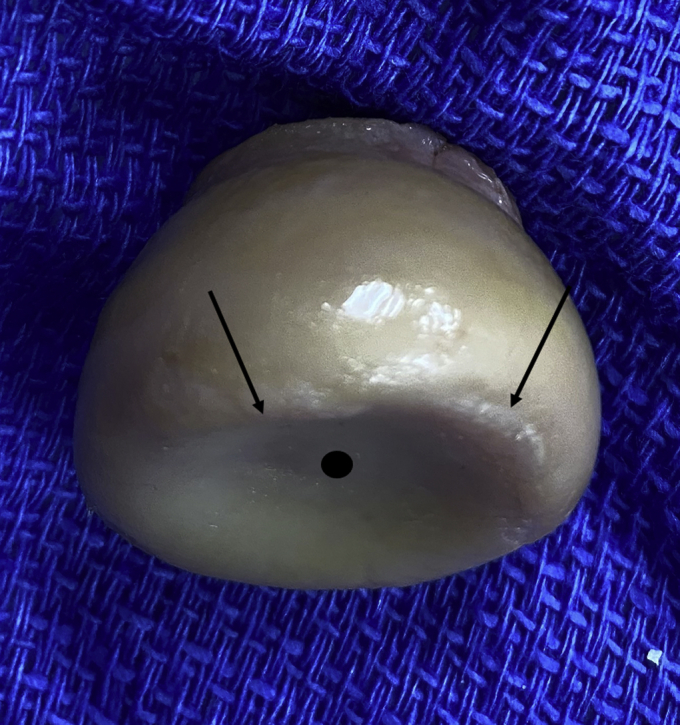
Anatomical specimen example of radial head irregularities illustrating the multiple planes of bony surfaces (), which may overlap on the lateral view and the depth of concavity of the articular surface ().
To our knowledge, this is the first study examining optimal screw placement of radial head fixation in relation to breakthrough of the articular radiocapitellar surface. Although radial head fractures are often partial articular with an anterolateral fragment, studies have found that equal screw purchase can be achieved across all 4 quadrants of subchondral bone.11,12 Therefore, tangential screw placement is ideal for achieving good reduction. Although fluoroscopy greatly improves the accuracy of screw placement and fracture reduction, having a distance guideline to aim for would likely decrease the amount of radiation exposure in the operating room and decrease operative time. Most studies looking at screw placement avoid screw abutment into the proximal radioulnar joint.6,7,10,12,24,26,27,29 Although the proximal radioulnar joint is involved in pronation and supination, both this joint and the radiocapitellar joint are involved in elbow stabilization to valgus stress.3,15 Post-traumatic arthritis and elbow instability can result from malalignment of the radiocapitellar joint.5 Patients with arthritis from screw breakthrough have few options for revision or operative treatments for their pain. Anconeous interposition and radial head resection are well-known salvage options; however, they have limitations because of the loss of the lateral column of the elbow.1,13 Newer salvage procedures include radiocapitellar hemiarthroplasty using a custom metallic capitellar resurfacing implant, prosthetic arthroplasty with a metal capitellar resurfacing implant, and a polyethylene-articulating surface.13,14,18,28 Although preliminary studies show promising results, no studies followed patients for longer than 6 years, and approximately one-third of patients required a second surgery.4,28
Radial head fracture patterns may require a variety of screw trajectories to gain adequate reduction. In cases with a concomitant transverse radial neck fracture, compression and reduction may be best achieved with a perpendicular screw trajectory across the fracture line. Previous research has described an entry point just off the articular surface of the rim of the radial head for a proximal-to-distal screw trajectory in these fracture patterns.23 With countersinking, screws are placed subchondral to prevent complications associated with screw head prominence. In these constructs, the screw will start more proximal than 5 mm but will not breach the articular surface as they are angled distally.
There were some limitations to the present study. This study used cadavers, which have the inherent problem of limited sample. Although age of the cadaver is a consideration, this study focused on subchondral screw placement, and articular cartilage thickness was not considered. In general, the specimens were older. The number of radii was limited to 15, but we deemed this quantity adequate to consider anatomic variations and be comparable to other published studies. We acknowledge that this 5 mm distance may not always be applicable in a variety of fracture patterns, but having a distance guideline can be helpful intraoperatively. In addition, screw trajectory is an important consideration. In spite of adherence to the recommendation of a 5 mm distance, articular breach may still occur with a suboptimal screw trajectory.
Conclusion
Intra-articular placement of screws during operative fixation of radial head fractures can lead to radiocapitellar joint damage. In this study, we have shown that a minimum distance of 5 mm from the articular rim of the radial head can be used reliably to avoid intra-articular screw penetration from screws placed tangential to the articular surface. Giving the surgeon a distance guideline that can be measured intraoperatively can minimize the risk of articular breach and decrease the potential for implant-related radiocapitellar trauma. Often, as surgeons, we rely on prior experience and the use of fluoroscan to confirm correct implant placement. However, combining this method with a defined distance will further reduce the potential for articular damage and improve the likelihood of a satisfactory outcome.
Disclaimers
Funding: No funding was disclosed by the authors.
Conflicts of interest: The authors, their immediate families, and any research foundation with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Acknowledgments
The authors would like to thank Angelique Tapia and Abby Alaine Heifner for editorial assistance and Laurie Wells, PhD, for statistical assistance.
Footnotes
Institutional review board approval was not required for this study.
References
- 1.Baghdadi Y.M., Morrey B.F., Sanchez-Sotelo J. Anconeus interposition arthroplasty: mid- to long-term results. Clin Orthop Relat Res. 2014;472:2151–2161. doi: 10.1007/s11999-014-3629-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Beingessner D.M., Dunning C.E., Beingessner C.J., Johnson J.A., King G.J.W. The effect of radial head fracture size on radiocapitellar joint stability. Clin Biomech (Bristol, Avon) 2003;18:677–681. doi: 10.1016/s0268-0033(03)00115-3. [DOI] [PubMed] [Google Scholar]
- 3.Bennett J.B. Radial head fractures: diagnosis and management. J Shoulder Elbow Surg. 1993;2:264–273. doi: 10.1016/S1058-2746(09)80088-8. [DOI] [PubMed] [Google Scholar]
- 4.Bigazzi P., Biondi M., Ceruso M. Radiocapitellar prosthetic arthroplasty in traumatic and post-traumatic complex lesions of the elbow. Eur J Orthop Surg Traumatol. 2016;26:851–858. doi: 10.1007/s00590-016-1837-0. [DOI] [PubMed] [Google Scholar]
- 5.Biswas D., Wysocki R.W., Cohen M.S. Primary and posttraumatic arthritis of the elbow. Arthritis. 2013;2013:473259. doi: 10.1155/2013/473259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Captier G., Canovas F., Mercier N., Thomas E., Bonnel F. Biometry of the radial head: biomechanical implications in pronation and supination. Surg Radiol Anat. 2002;24:295–301. doi: 10.1007/s00276-002-0059-9. [DOI] [PubMed] [Google Scholar]
- 7.Caputo A.E., Mazzocca A.D., Santoro V.M. The nonarticulating portion of the radial head: anatomic and clinical correlations for internal fixation. J Hand Surg Am. 1998;23:1082–1090. doi: 10.1016/S0363-5023(98)80020-8. [DOI] [PubMed] [Google Scholar]
- 8.Drobetz H., Black A., Davies J., Buttner P., Heal C. Screw placement is everything: risk factors for loss of reduction with volar locking distal radius plates. World J Orthop. 2018;9:203–209. doi: 10.5312/wjo.v9.i10.203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dizdarevic I., Eden C.M., Bengard M., Barron O.A., Catalano L.W., III, Glickel S.Z. Assessment of intra-articular screw penetration during radial head and olecranon locking plate fixation: a cadaveric study. Hand (N Y) 2016;11:65–71. doi: 10.1177/1558944715614862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Giannicola G., Manauzzi E., Sacchetti F.M., Greco A., Bullitta G., Vestri A., et al. Anatomical variations of the proximal radius and their effects on osteosynthesis. J Hand Surg Am. 2012;37:1015–1023. doi: 10.1016/j.jhsa.2012.02.005. [DOI] [PubMed] [Google Scholar]
- 11.Gordon K.D., Duck T.R., King G.J., Johnson J.A. Mechanical properties of subchondral cancellous bone of the radial head. J Orthop Trauma. 2003;17:285–289. doi: 10.1097/00005131-200304000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Haverstock J.P., Katchky R.N., Lalone E.A., Faber K.J., King G.J., Athwal G.S. Regional variations in radial head bone volume and density: implications for fracture patterns and fixation. J Shoulder Elbow Surg. 2012;21:1669–1673. doi: 10.1016/j.jse.2012.07.002. [DOI] [PubMed] [Google Scholar]
- 13.Heijink A., Morrey B.F., Cooney W.P., III Radiocapitellar hemiarthroplasty for radiocapitellar arthritis: a report of three cases. J Shoulder Elbow Surg. 2008;17:e12–e15. doi: 10.1016/j.jse.2007.04.009. [DOI] [PubMed] [Google Scholar]
- 14.Heijink A., Morrey B.F., Eygendaal D. Radiocapitellar prosthetic arthroplasty: a report of 6 cases and review of the literature. J Shoulder Elbow Surg. 2014;23:843–849. doi: 10.1016/j.jse.2014.01.042. [DOI] [PubMed] [Google Scholar]
- 15.Hotchkiss R.N., Weiland A.J. Valgus stability of the elbow. J Orthop Res. 1987;5:372–377. doi: 10.1002/jor.1100050309. [DOI] [PubMed] [Google Scholar]
- 16.Jackson J.D., Steinmann S.P. Radial head fractures. Hand Clin. 2007;23:185–193. doi: 10.1016/j.hcl.2007.01.009. vi. [DOI] [PubMed] [Google Scholar]
- 17.Kaas L., van Riet R.P., Vroemen J.P., Eygendaal D. The epidemiology of radial head fractures. J Shoulder Elbow Surg. 2010;19:520–523. doi: 10.1016/j.jse.2009.10.015. [DOI] [PubMed] [Google Scholar]
- 18.Kachooei A.R., Heesakkers N.A.M., Heijink A., The B., Eygendaal D. Radiocapitellar prosthetic arthroplasty: short-term to midterm results of 19 elbows. J Shoulder Elbow Surg. 2018;27:726–732. doi: 10.1016/j.jse.2017.12.013. [DOI] [PubMed] [Google Scholar]
- 19.Koo T.K., Li M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15:155–163. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Koslowsky T.C., Beyer F., Germund I., Jergas M., Koebke J. Morphometric parameters of the radial neck: an anatomical study. Surg Radiol Anat. 2007;29:279–284. doi: 10.1007/s00276-007-0206-4. [DOI] [PubMed] [Google Scholar]
- 21.Koslowsky T.C., Mader K., Brandenburg A., Hellmich M., Koebke J. Subchondral bone density of the radial head measured with subtraction densitometry. Surg Radiol Anat. 2008;30:113–118. doi: 10.1007/s00276-007-0299-9. [DOI] [PubMed] [Google Scholar]
- 22.Kuhn S., Burkhart K.J., Schneider J., Muelbert B.K., Hartmann F., Mueller L.P., et al. The anatomy of the proximal radius: implications on fracture implant design. J Shoulder Elbow Surg. 2012;21:1247–1254. doi: 10.1016/j.jse.2011.11.008. [DOI] [PubMed] [Google Scholar]
- 23.Lipman M.D., Gause T.M., Teran V.A., Chhabra A.B., Deal D.N. Radial head fracture fixation using tripod technique with headless compression screws. J Hand Surg Am. 2018;43:575.e1–575.e6. doi: 10.1016/j.jhsa.2018.03.009. [DOI] [PubMed] [Google Scholar]
- 24.Mcdougall A., White J. Subluxation of the inferior radio-ulnar joint complicating fracture of the radial head. J Bone Joint Surg Br. 1957;39-B:278–287. doi: 10.1302/0301-620X.39B2.278. [DOI] [PubMed] [Google Scholar]
- 25.Orbay J.L. The treatment of unstable distal radius fractures with volar fiaxation. Hand Surg. 2000;5:103–112. doi: 10.1142/s0218810400000223. [DOI] [PubMed] [Google Scholar]
- 26.Ries C., Müller M., Wegmann K., Pfau D.B., Müller L.P., Burkhart K.J. Is an extension of the safe zone possible without jeopardizing the proximal radioulnar joint when performing a radial head plate osteosynthesis? J Shoulder Elbow Surg. 2015;24:1627–1634. doi: 10.1016/j.jse.2015.03.010. [DOI] [PubMed] [Google Scholar]
- 27.Smith G.R., Hotchkiss R.N. Radial head and neck fractures: anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg. 1996;5(2 Pt 1):113–117. doi: 10.1016/s1058-2746(96)80005-x. [DOI] [PubMed] [Google Scholar]
- 28.Spross C., Jak W., van Riet R.P. Radiocapitellar arthroplasty: a consecutive case series with 2 to 6 years' follow-up. J Shoulder Elbow Surg. 2019;28:131–136. doi: 10.1016/j.jse.2018.08.009. [DOI] [PubMed] [Google Scholar]
- 29.Weiss A.P., Hastings H., II The anatomy of the proximal radioulnar joint. J Shoulder Elbow Surg. 1992;1:193–199. doi: 10.1016/1058-2746(92)90013-S. [DOI] [PubMed] [Google Scholar]