

Abstract
Meridians constitute the theoretical foundation of acupuncture in traditional Chinese medicine (TCM), and they have been described for 2000 years. Classical TCM advocates for the directionality of meridians. Finding an accurate method to verify this directionality is an important goal of TCM doctors and researchers. In this study, we objectively explored the physical properties of meridians, such as response current from electrical stimulation, to explore their directionality. The Agilent B1500A semiconductor measurement analyzer was utilized to input the alternating current waveforms and detect the response current on the meridians. The results showed that the direction of the meridians influences the intensity of the response current. Therefore, the mechanisms behind the directions of ion transportation and the meridians were investigated using the response time and the intensity of the response current. Thereafter, we propose a model to explain this mechanism. Afterward, a comparison between the direction of the meridian in this experiment and ancient Chinese medicine classics was performed.
Keywords: Traditional Chinese medicine (TCM), Electrical acupuncture, Meridian directionality, Drift current
Introduction
Since 1979, the World Health Organization (WHO) has published indications of acupuncture, which has become a commonly accepted method for treatment. As complementary alternative medicine, acupuncture has been applied for decades, and it has been established to be therapeutically effective by modern researches [1]. Regardless of the acupuncture method, such as needle insertion, manual pressure, electrical stimulation, magnets, and low-power lasers, the theoretical bases are meridians. Meridians provide an important foundation for traditional Chinese medicine (TCM) and guidelines for clinical practice. The “meridian theory" was described in the Yellow Emperor's Classic of Internal Medicine for 2000 years [2]. Finding an accurate method to verify the existence of meridians is an important goal for TCM doctors and researchers [3–8].
For example, many anatomical structures have been proposed to describe meridians, such as tendinomuscular meridians or primo vascular systems (or Bonghan Ducts) [9, 10]. Various studies have revealed the different parts of the meridian. Gerhard Litscher’s group found that infrared thermography cannot visualize stimulation-induced meridian-like structures [11]. Wei et al. constructed a meridian acupoint temperature map by reporting the characteristics of the meridian acupoint temperatures in healthy medical students [12].
In addition, the Ryodoraku theory explores the utilization of electric conductivity to identify meridians. The Ryodoraku theory was proposed by Dr. Yoshio Nakatani in the 1950s. This theory states that there are some points on the skin that have a high electric conductivity, and the energy change of these points could represent the condition of the body, i.e., the inner viscera or the balance of qi and blood. These points are called Ryodoten, and studies have shown that they connect to form a line, which is called Ryodoraku. The location of the Ryodoraku is almost identical to the location of the meridian distribution. Consequently, the energy of a Ryodoraku is considered to represent the energy of the corresponding meridian [13, 14].
The meridian energy analysis device (MEAD) is an instrument developed based on the Ryodoraku theory [15]. MEAD detects the electrical conductivity of the skin over meridian lines. It is believed that the electrical conductivity of the meridian reflects the biological energy or balance of qi and blood in the body [15]. Due to the therapeutic effects of some treatments, such as analgesic response or control of blood pressure, acupuncture is thought to be related to the central or peripheral nervous system [16, 17]. Thus, in this research, the existence of the meridian was fully confirmed [18].
However, the Ryodoraku theory only detects the electrical conductivity of the skin over a single acupoint of the meridian. Meanwhile, the anatomical or morphological pieces of evidence on the existence of the meridian are still lacking, and the exploration of the meridian with modern physical devices has been minimally investigated. A previous study was referenced [19], and the characteristics of the current–time (I–t) curve measuring body meridians are similar to those obtained by the isothermal transient ionic current (ITIC) theory. Based on the drift and diffusion currents of the theory, the method of conducting electricity in the meridians is mainly through ions. Electrical stimulation was used to determine the electrical characteristics of the meridian, which serves as a precedent for meridian research in the field of physical electronics.
Based on the intrinsic properties of meridians, in this study, we investigated the mechanism of the direction of ion transport and transmission of the meridians mentioned above. The effectiveness of the meridian direction is studied utilizing electrical characteristics, and the results are compared to those in TCM. The meridian direction is based on ancient Chinese medicine classics. It is generally believed that the course of the three Yin meridians of the hand is from the thorax to the hand; the course of the three Yang meridians of the hand is from the hand to the head; the course of the three Yang meridians of the foot is from the head to the foot; and the course of the three Yin meridians of the foot is from the foot to the thorax [20, 21]. In this study, a semiconductor measurement analyzer (Agilent B1500A) was utilized to input the waveforms with different voltage polarities on the three Yin meridians of the hand (Taiyin lung meridian of the hand, Jueyin pericardium meridian of the hand, and Shaoyin heart meridian of the hand) and the three Yang meridians of the foot (Yangming stomach meridian of the foot, Shaoyang gallbladder meridian of the foot, and Taiyang bladder meridian of the foot). Two acupoints were chosen over each meridian, and the differences between the acupoints on each meridian were recorded. Finally, the correlation between the experimental results and the meridian direction recorded in the TCM classics was shown. This study provides the basis for meridian directionality for further research and clinical treatment choices.
Experimental Methods
Participant Selection
The Institutional Review Board of the Chang Gung Medical Foundation approved this clinical trial (IRB permit no. 201901601A3). Before enrollment, all participants received informed consent forms, which they completed signed after understanding the project. Thereafter, the experiments commenced. Thirty volunteers who met the inclusion criteria of being healthy and above 18 years were recruited (15 men and 15 women). Pregnant and lactating women, people who were fasting, people with idiopathic thrombocytopenic purpura (ITP), and people who take sleeping pills or psychiatric drugs were excluded. No specific acupoints were targeted; instead, the acupoints were chosen from convenient locations which are favorable for acupuncture.
Inclusion and Exclusion Criteria
According to a prospective survey, acupuncture can have some side effects despite its benefits [22]. As an invasive treatment, it may sometimes induce local or systemic adverse reactions [22–24]. Moreover, a systemic review showed that life-threatening events may also develop, albeit rarely. Consequently, the exclusion criteria were stringent. Bleeding and hematoma are the most common adverse reactions; therefore, volunteers with bleeding tendencies (platelet count of less than 20,000 and/or thrombocytopenic purpura) were excluded. Volunteers with chronic medical conditions, who were prescribed anticoagulants, were also excluded. Pregnant women and volunteers with pacemakers were excluded. No adverse reaction was observed throughout the experiment.
Measurement Machine and Equipment
In this study, all electrical signals were obtained using an Agilent B1500A semiconductor parameter analyzer and a Cascade M150 microprobe station. The acupuncture needles used were produced under the same conditions, in the same factory (Dong Bang Acupuncture Inc.), and on the same day to minimize experimental error.
Experiment Process
The decision of the left- or right hand and the left- or right foot provided by each subject to participate in this experiment was categorized as random. We chose two acupoints over each Yin meridian of the hand: LU5 (Chize) and LU6 (Kongzui) from the Taiyin lung meridian of the hand, PC3 (Quze) and PC6 (Neiguan) from the Jueyin pericardium meridian of the hand, and HT3 (Shaohai) and HT7 (Shenmen) from the Shaoyin heart meridian of the hand; two acupoints over each Yang meridian of the foot: ST36 (Zusanli) and ST37 (Shangjuxu) from the Yangming stomach meridian of the foot, GB34 (Yanglingquan) and GB39 (Xuanzhong) from the Shaoyang gallbladder meridian of the foot, and BL40 (Weizhong) and BL57 (Chengshan) from the Taiyang bladder meridian of the foot. The detailed locations are featured in Fig. 1 and Table 1.
Fig. 1.

Selected acupoints: a Yin meridians of the hand and b Yang meridians of the foot
Table 1.
Selected acupoints with detailed locations
| Acupoints | Location |
|---|---|
| Taiyin Lung Meridian of the Hand | |
| LU5(Chize) | Located in the transverse cubital crease, on the radial side (laternal side) of the tendon of musculus biceps branchii |
| Lu6(Kongzui) | On the line between LU5(Chize) and LU9 (Tasiyuang), 7 cm above the transverse crease of the twist |
| Jueyin Pericardium Meridian of the Hand | |
| PC3 (Quze) | Located in the transverse cubital crease, on the ulnar side (medial side) of the tendon of musculus biceps branchii |
| PC6 (Neiguan) | Between the tendons of m. palmaris longus and m. flexor carpi radialis, 2 cun above the transverse crease of the twist |
| Shaoyin Heart Meridian of the Hand | |
| HT3 (Shaohai) | At the middle part of the line between the medial end of the transverse cubital crease and medial epicondyle of the humerus when the elbow is flexed. Flex the elbow to locate the point |
| HT7 (Shenmen) | At the ulnar end of the transverse crease of the wrist, on the radial side of the tendon of m. flexor carpi ulnaris |
| Yangming Stomach Meridian of the Foot | |
| ST36 (Zusanli) | 3 cun below Dubi (ST35), one finger width laternal to the anterior crest of the tibia |
| ST37(Shangjuxu) | 3 cun below ST35 one finger width laternal from the anterior crest of the tibia |
| Shaoyang Gallbladder Meridian of the Foot | |
| GB34 (Yanglingquan) | In a depression anterior and inferior to the head of the fibula |
| GB39 (Xuanzhong) | 3 cun above the tip of the laternal malleolus, in the depression of the anterior border of the fibula |
| Taiyang Bladder Meridian of the Foot | |
| BL40 (Weizhong) | Midpoint of the transverse cubital of the popliteal fossa between the biceps femoris and semitendinosus tendons |
| BL57 (Chengshan) | In the depression below the gastrocnemius muscle, 8 cun inferior to BL40 |
After fully explaining the experimental procedures, the consent forms were signed, and acupuncture was performed by a certified TCM doctor. Disposable 1 cun (C.M.S. acupuncture needles, 0.30 × 25 mm) and 1.5 cun sterilized acupuncture needles were employed for the upper and lower limbs, respectively. All acupoints were sterilized using 75% alcohol. The locations of the acupoints were detected based on clinical experience and ancient classics. After the acupuncture needles were inserted, acupuncture manipulation was performed to achieve deqi-soreness, numbness, or distension, as described by participants, and heaviness, tension, tightness, or fullness, as described by the acupuncturist [9, 25]. After deqi, alligator clips were used to clip the acupuncture needles. Meanwhile, the Agilent B1500A parameter analyzer inputted the alternating current (AC) waveforms on two acupoints. In this study, the AC waveform considered was a continuous square wave oscillating between 2 and − 2 V with a frequency of 2 Hz. The first acupoint was near the heart (called the near heart point (NHP)), while the second was far from the heart (called the far heart point (FHP)). Conversely, the analyzer received the response current, Iresponse, from the grounded FHP/NHP. A schematic of the experiment is shown in Fig. 2.
Fig. 2.
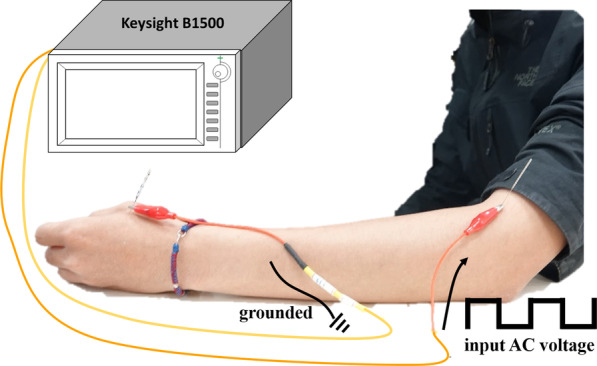
Schematic of the electrical acupuncture
The order of the upper limb acupoints is as follows: the Taiyin lung meridian of the hand, Jueyin pericardium meridian of the hand, and Shaoyin heart meridian of the hand. After the completion of the hand experiments, the foot experiments were performed in the following order: the Yangming stomach meridian of the foot, Shaoyang gallbladder meridian of the foot, and Taiyang gallbladder meridian of the foot. The relationship between the input wave and Iresponse is shown in Fig. 3.
Fig. 3.
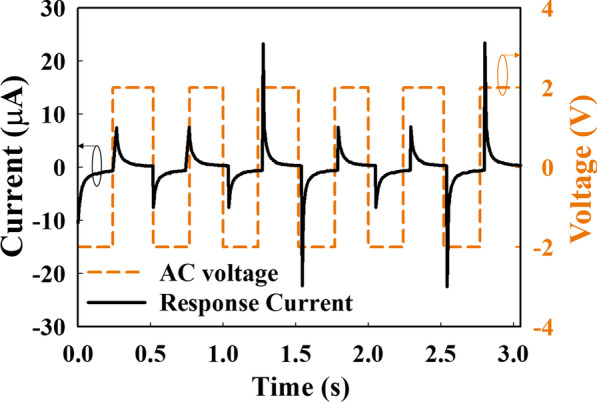
The relationship between the input wave and Iresponse
Result and Discussion
An external force, such as an electric field, is utilized to determine the properties of the current, such as direction and intensity, which is a conventional technique in semiconductor studies. In this study, the direction of the meridians was identified using the external electric field. Electrical acupuncture was utilized to control the flow of ions, which produced current; thereafter, the current was enhanced or countervailed by the force of the meridian. The intensity of the current increased when the direction of the meridians and the extra current forward flow. The described current is defined as the direction of positive ions. Before the electrical signal input, the ions in the meridian were uniformly distributed and underwent diffusion, as shown in Fig. 4. When an AC wave was inputted on an acupoint using the parameter analyzer, the ions drifted along the direction of the electric field, which is called the drift current (Idrift). When the drifting ions create an ion concentration gradient due to the electric field, a diffusion current is also generated. Hung et al. reported that the response current of ion flux includes ion drift and diffusion currents with an applied square AC wave [19]. However, the contribution of the diffusion current to the response current can be ignored. Thus, herein, only the effect of drift current is discussed.
Fig. 4.

Uniform distribution and diffusion of ions in the meridian without the electron field
When a negative voltage was inputted on the FHP, positive ions were attracted to the FHP (along the electric field direction) and negative ions were repelled to the NHP (opposite the electric field direction). Meanwhile, the received Iresponse is higher and lower since the direction of the meridian is identical and opposite direction, respectively.
Based on the applied electric field and the mechanism of the drift current [26], the Iresponse shown in Fig. 5, one period of Iresponse can be divided into three regions according to the change in current with increasing time. At the beginning of the I–t measurement, the current increases gradually in the − V region when a negative voltage (VLow) is inputted. Thereafter, Iresponse reaches point L, and the current increases dramatically in the transition region (point L to point R). The τrising parameter represents the time from the negative saturation of Iresponse to the positive maximum of Iresponse, which responds to the input wave switch from a negative voltage to a positive voltage (VHigh). Subsequently, the current decreases gradually and approaches a flat condition in the + V region.
Fig. 5.
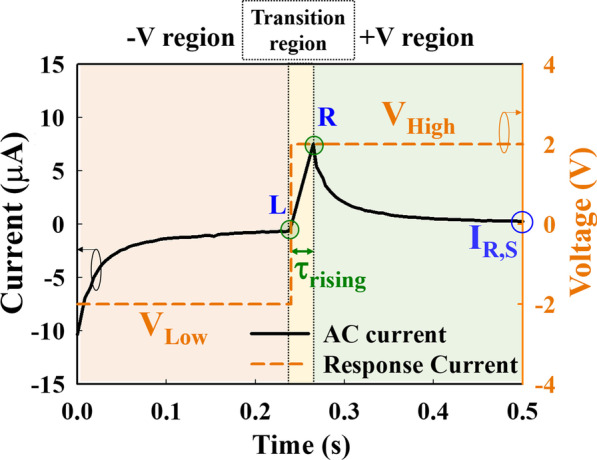
Time evolution of Iresponse and the input voltage. VLow and VHigh represent the negative and positive voltages of the input AC voltage, respectively
In the − V region, because a negative voltage was applied, the positive ions drifted along the electric field direction and removed the grounded acupoint; thus, the Iresponse value was negative. Therefore, with increasing time, ions accumulate near the acupoints (negative ions near the grounded acupoint and positive ions near the input acupoint), causing the received Iresponse to approach a flat. In the transition region, the input voltage changes from a negative to a positive value in an ultrashort time, causing a large number of ions to exchange suddenly, as shown in Fig. 6. Finally, with increasing the input time of the positive voltage in the + V region, most ions tend to accumulate near the acupoints, and the parameter analyzer receives a decreased and saturated Iresponse (IR,S), as shown in Fig. 7. The peak of Iresponse was received with different peak high when a voltage (AC square waveform) was input to the acupoint. To reduce the variation factor in the experiment, the comparison of Iresponse was used at the saturation point.
Fig. 6.

The direction of the positive and negative ions when the inputted negative voltage changes to a positive voltage of AC wave. Many positive and negative ions exchange instantaneously
Fig. 7.

The direction of the positive and negative ions after applying positive voltage for a long time. The ions accumulate at the acupoint
To analyze the relationship between the meridian direction and the Iresponse, the τrising and IR,S were examined, and the differences between the meridians were compared. The average τrising of the Taiyin lung meridian of the hand in Fig. 8a is 23.3 ms when the wave input is on NHP and 28.8 ms when wave input is on FHP. The average τrising of the Yangming stomach meridian of the foot in Fig. 8b is 23.3 ms when the wave input is on NHP and 26.5 ms when the wave input is on FHP. According to Fig. 8, the average τrising with an input wave on the NHP is less than that on the FHP. Contrary to the above τrising results, the average IR,S with an input wave on the NHP is higher than that on the FHP, as shown in Fig. 9. The average IR,S value of the Taiyin lung meridian of the hand in Fig. 9a is 0.49 μs when the wave input is on NHP and 0.38 μs when the wave input is on FHP. The average IR,S of the Yangming stomach meridian of the foot in Fig. 9b is 0.65 μs when the wave input is on NHP and 0.57 μs when wave input is on FHP. The τrising and IR,S values of the Taiyin lung meridian of the hand, Jueyin pericardium meridian of the hand, Shaoyin heart meridian of the hand, Yangming stomach meridian of the foot, Shaoyang gallbladder meridian of the foot, and Taiyang bladder meridian of the foot are shown in Tables 2 and 3, respectively. According to Tables 2 and 3, when the wave input is applied from NHP to FHP, the τrising is lower and IR,S is higher of six meridians. The box plots show that the statistics of the meridian data in this study are concentrated around the central tendency and without extreme values. All data evaluations in this study were repeated three times and are presented as the mean ± standard deviation.
Fig. 8.

Box plot of τrising of the a Taiyin lung meridian and b Yangming stomach meridian. The red line in the box plot is the mean value of the data
Fig. 9.

Box plot of the mean current of the a Taiyin lung meridian and b Yangming stomach meridian. The red line in the box plot is the mean value of the data
Table 2.
The arithmetic means and standard deviation of the τrising values of the Sanyang meridian of the hand and Sanyin meridian of the foot
| Raising time (ms) | NHP | FHP | P value |
|---|---|---|---|
| Meridians | |||
| Taiyin Lund Meridian | 23.3 ± 0.8 | 28.8 ± 2.7 | 8.7e − 08 |
| Jueyin Pericardium Meridian | 24.2 ± 1.5 | 29.0 ± 1.9 | 2.5e − 05 |
| Shaoyin Heart Meridian | 24.5 ± 1.7 | 30.9 ± 3.2 | 1.3e − 05 |
| Yangming Stomach Meridian | 23.3 ± 0.8 | 26.5 ± 0.1 | 1.4e − 10 |
| Shaoyang Gallbladder Meridian | 23.6 ± 1.1 | 27.0 ± 1.0 | 3.6e − 05 |
| Taiyang Bladder Meridian | 23.8 ± 1.7 | 28.5 ± 2.2 | 1.9e − 05 |
Table 3.
The arithmetic means and standard deviation of the IR,S of the Sanyang meridian of the hand and the Sanyin meridian of the foot
| Mean Current (μA) | NHP | FHP | P value |
|---|---|---|---|
| Meridians | |||
| Taiyin Lund Meridian | 0.49 ± 0.11 | 0.38 ± 0.13 | 1.3e − 05 |
| Jueyin Pericardium Meridian | 0.74 ± 0.27 | 0.62 ± 0.21 | 2.8e − 05 |
| Shaoyin Heart Meridian | 0.23 ± 0.18 | 0.21 ± 0.12 | 7.7e − 05 |
| Yangming Stomach Meridian | 0.65 ± 0.13 | 0.57 ± 0.07 | 1.1e − 05 |
| Shaoyang Gallbladder Meridian | 0.77 ± 0.14 | 0.63 ± 0.19 | 8.5e − 05 |
| Taiyang Bladder Meridian | 0.80 ± 0.25 | 0.70 ± 0.12 | 4.5e − 05 |
A physical model is proposed in which the meridians assist in the ion drift based on statistics. The direction of the meridian can be considered as a built-in force that assists the movement of ions. The high velocity of the ions indicates that the ions drift from one acupoint to another in a short time. According to the current density formula [26], the short arrival time of ions between two acupoints leads to an increase in the Iresponse. For example, the direction of the Sanyang meridian of the hand and the inputted electric field are the same, and positive ions drift because of two forces. Thus, a short τrising and a high IR,S are observed. Figure 10 also shows the schematic of the flow direction of the meridian, the direction of Idrift, and the Iresponse relationship.
Fig. 10.

Relationship between the direction of Idrift and the direction of the meridian of a the hand and b the foot. The reverse and the forward relationships between the Idrift and the meridian direction caused a decrease and an increase in the Iresponse
The results illustrate that the meridian direction can be measured and prove that the meridian direction is identical to that inferred in this work and mentioned in TCM. Notably, the findings of this study can be applied to clinical practices. When there is chest/heart discomfort, acupuncture over the Taiyin lung meridian of the hand and electric acupuncture from FHP to NHP can be applied. However, the association between the clinical therapeutic effect and meridian direction requires further research.
Conclusion
In this study, we analyzed the response current, which relies on the input AC voltage on the meridians. Based on the parameters, τrising and IR,S, relating to the response current of the meridians, the model of meridians assisting in ionic drift was proposed, and the meridian direction was also inferred. The result showed that the direction of the meridian obtained in this work was consistent with those in TCM. This study affords more analytical methods for use in clinical practices.
Acknowledgements
This study was supported by the Chang Gung Medical and National Sun Yat-sen University Research Fund (CMRPG8I0321 and CMRPG8K0251). The authors wish to thank Chen-ting Dai for his help with this study.
Abbreviations
- TCM
Traditional Chinese medicine
- WHO
World Health Organization
- MEAD
Meridian energy analysis device
- I–t
Current–time
- ITIC
Isothermal transient ionic current
- ITP
Idiopathic thrombocytopenic purpura
- LU
Taiyin lung meridian in hand
- PC
Jueyin pericardium meridian in hand
- HT
Shaoyin heart meridian in hand
- ST
Yangming stomach meridian in foot
- GB
Shaoyang gallbladder meridian in foot
- BL
Taiyang bladder meridian in foot
- AC
Alternating current
- NHP
Near heat point
- FHP
Far heat point
- Iresponse
Response current
- Idrift
Drift current
- VLow
Negative voltage
- VHigh
Positive voltage
- IR,S
Saturated Iresponse
Author Contributions
CWK, TCC, CCW, and TMT performed the electrical measurements; TCC and YCH were involved in the planning and supervision of the work; CWK, YWL, YFT, and WCC processed the experimental data, performed the analysis, drafted the manuscript, and designed the figures. WLH and YWL performed the acupuncture.
Funding
This study was supported by the Chang Gung Medical Hospital and National Sun Yat-sen University Research Fund (CMRPG8I0321, CMRPG8K0251). The funder had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of Data and Materials
All data are fully available without restriction.
Declarations
Ethics Approval and Consent to Participate
The Institutional Review Board of the Chang Gung Medical Foundation approved this clinical trial (IRB permit no. 201800392A3). Before enrollment, all participants received informed consent forms, which they completed signed after understanding the project.
Consent for Publication
All authors discussed the results and commented on the manuscript. The author(s) read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yan-Wen Liu and Chuan-Wei Kuo have contributed equally
Contributor Information
Ting-Chang Chang, Email: tcchang3708@gmail.com.
Yu-Chiang Hung, Email: hungyuchiang@gmail.com.
References
- 1.Wang H, Yang G, Wang S, Zheng X, Zhang W, Li Y. The most commonly treated acupuncture indications in the United States: a cross-sectional study. Am J Chin Med. 2018;46(07):1387–1419. doi: 10.1142/S0192415X18500738. [DOI] [PubMed] [Google Scholar]
- 2.Liu P, Guo Y, Qian X, Tang S, Li Z, Chen L. China's distinctive engagement in global health. Lancet. 2014;384(9945):793–804. doi: 10.1016/S0140-6736(14)60725-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wang TH, Wang MH, Shih CC, Lu YH, Zheng HX, Tseng YT, Hu WL, Chang TC, Hung YC (2021) Comparison of physical electrical conductivity and acupuncture deqi sensation between stainless steel needling and supercritical fluid-treated needling. Biomed J 44:S267-S274< [DOI] [PMC free article] [PubMed]
- 4.Hao JJ, Mittelman M. Acupuncture: past, present, and future. Glob Adv Health Med. 2014;3(4):6–8. doi: 10.7453/gahmj.2014.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Luo H, Meng F, Jia Y, Zhao X. Clinical research on the therapeutic effect of the electro-acupuncture treatment in patients with depression. Psychiatry Clin Neurosci. 1998;52(S6):S338–S340. doi: 10.1111/j.1440-1819.1998.tb03262.x. [DOI] [PubMed] [Google Scholar]
- 6.Chen ZJ, Guo YP, Wu ZC. Observation on the therapeutic effect of acupuncture at pain points on cancer pain. Zhongguo zhen jiu Chin Acupunct Moxib. 2008;28(4):251–253. [PubMed] [Google Scholar]
- 7.Kaptchuk TJ. Acupuncture: theory, efficacy, and practice. Ann Intern Med. 2002;136(5):374–383. doi: 10.7326/0003-4819-136-5-200203050-00010. [DOI] [PubMed] [Google Scholar]
- 8.VanderPloeg K, Yi X. Acupuncture in modern society. J Acupunct Meridian Stud. 2009;2(1):26–33. doi: 10.1016/S2005-2901(09)60012-1. [DOI] [PubMed] [Google Scholar]
- 9.Longhurst JC. Defining meridians: a modern basis of understanding. J Acupunct Meridian Stud. 2010;3(2):67–74. doi: 10.1016/S2005-2901(10)60014-3. [DOI] [PubMed] [Google Scholar]
- 10.Zhou W, Benharash P. Effects and mechanisms of acupuncture based on the principle of meridians. J Acupunct Meridian Stud. 2014;7(4):190–193. doi: 10.1016/j.jams.2014.02.007. [DOI] [PubMed] [Google Scholar]
- 11.Litscher G. Infrared thermography fails to visualize stimulation-induced meridian-like structures. Biomed Eng Online. 2005;4(1):1–8. doi: 10.1186/1475-925X-4-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wei HN, Jiang LP, Xiong B, Zhou S, Yu L, Huang YM, Liu DG, Ling W, Song XN, Zhang XX, Zhao HL. Characteristic patterns of normal meridian acupoint temperature. J Chin Med Assoc. 2017;80(7):419–426. doi: 10.1016/j.jcma.2016.12.007. [DOI] [PubMed] [Google Scholar]
- 13.Chiang CM, Liu CC, Lin FM, Wang W, Chou PC. Using ryodoraku measurement to evaluate the impact of environmental noise on human physiological response. Indoor Built Environ. 2012;21(2):241–252. doi: 10.1177/1420326X11409448. [DOI] [Google Scholar]
- 14.Nakatani Y, Oiso T. A guide for the application of ryodoraku autonomous nerve regulatory therapy. Alhambra: Chan's Books & Products; 1972. pp. 1–25. [Google Scholar]
- 15.Tsai MY, Chen SY, Lin CC. Theoretical basis, application, reliability, and sample size estimates of a meridian energy analysis device for traditional chinese medicine research. Clinics. 2017;72(4):254–257. doi: 10.6061/clinics/2017(04)10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Li P, Tjen-A-Looi S, Longhurst JC. Rostral ventrolateral medullary opioid receptor subtypes in the inhibitory effect of electroacupuncture on reflex autonomic response in cats. Auton Neurosci. 2001;89(1–2):38–47. doi: 10.1016/S1566-0702(01)00247-8. [DOI] [PubMed] [Google Scholar]
- 17.Toyama PM, Nishizawa M. The physiological basis of acupuncture therapy. J Natl Med Assoc. 1972;64(5):397. [PMC free article] [PubMed] [Google Scholar]
- 18.Wang GJ, Ayati MH, Zhang WB. Meridian studies in China: a systematic review. J Acupunct Meridian Stud. 2010;3(1):1–9. doi: 10.1016/S2005-2901(10)60001-5. [DOI] [PubMed] [Google Scholar]
- 19.Hung YC, Chen WC, Chang TC, Zheng HX, Liu YW, Tan YF, Lin SK, Lu YH, Hu WL, Tsai TM. Meridian study on the response current affected by electrical pulse and acupuncture. Nanoscale Res Lett. 2020;15(1):1–6. doi: 10.1186/s11671-020-03373-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Irnich D, Euler D, Gleditsch J, Banzer W, Bachmann J. Chapter 22 - Acupuncture and related procedures. In: Irnich D, editor. Myofascial trigger points. Oxford: Churchill Livingstone; 2013. pp. 179–232. [Google Scholar]
- 21.Giovanni M. The foundations of Chinese medicine: a comprehensive text for acupuncturists and herbalists. Edinburgh: Churchill Livingstone; 1989. pp. 219–268. [Google Scholar]
- 22.Yamashita H, Tsukayama H, Hori N, Kimura T, Tanno Y. Incidence of adverse reactions associated with acupuncture. J Altern Complement Med. 2000;6(4):345–350. doi: 10.1089/10755530050120718. [DOI] [PubMed] [Google Scholar]
- 23.MacPherson H, Thomas K, Walters S, Fitter M. A prospective survey of adverse events and treatment reactions following 34,000 consultations with professional acupuncturists. Acupunct Med. 2001;19(2):93–102. doi: 10.1136/aim.19.2.93. [DOI] [PubMed] [Google Scholar]
- 24.Ernst E. Life-threatening adverse reactions after acupuncture? A systematic review. Pain. 1997;71(2):123–126. doi: 10.1016/S0304-3959(97)03368-X. [DOI] [PubMed] [Google Scholar]
- 25.Yang XY, Shi GX, Li QQ, Zhang ZH, Xu Q, Liu CZ. Characterization of deqi sensation and acupuncture effect. Evid Based Complement Altern Med. 2013 doi: 10.1155/2013/319734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sze SM, Ng KK (2007) Physics of semiconductor devices, 3rd edn. Wiley-Interscience, New York
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data are fully available without restriction.