

Abstract
Background Sickle cell disease (SCD) is associated with oxidative stress due to an imbalance between production and elimination of the reactive oxygen species. It has been reported that SCD patients are at risk of multiple micronutrients' deficiencies, including several trace elements involved in the antioxidation mechanisms. We aimed to assess the status of these micronutrients in SCD patients.
Methods This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. The databases of MedLine, Embase, and PsycInfo were used for the systematic search from time the databases existed until April 2021. A total of 36 studies fulfilled the eligibility criteria. We calculated the pooled standardized mean difference (SMD) of serum zinc, magnesium, or copper levels among patients with SCD and their healthy controls.
Results SCD patients had significantly lower zinc (SMD = −1.27 [95% CI: 1.67−0.87, p 0.001]) and magnesium levels (SMD = −0.53 [95% CI: 1.0−0.06, p 0.026] than their controls. Copper level was found to be significantly higher in SCD patients, with SMD = 0.68 (95% CI: 0.05−1.32, p 0.004).
Conclusion This review showed that SCD patients may potentially prompt to have lower zinc and magnesium levels and higher copper levels compared with those without the disease. Future research need to be directed to investigate clinical outcome of nutritional difficiencies in patients with SCD, as well as the possibility of implementing nutritional supplement programs which may help minimizing the harmful effects of the disease on human body.
Keywords: sickle cell, SCD, zinc, magnesium, copper
Introduction
Sickle cell disease (SCD) is an inherited red blood cell disorder that leads to forming the mutated hemoglobin S, resulting in a wide range of signs and symptoms, including chronic hemolytic anemia, sequestration crisis, susceptibility to repeated infections, and periodic episodes of pain mostly due to vasoocclusive phenomena. 1 2 3 SCD also presents with long-term effects such as cerebrovascular accidents, sickle nephropathy, pulmonary complications, renal impairment, cardiomyopathy, delayed puberty, and reduced growth. 1 2 3 4 5 6 7
The sickling and ischemic reperfusion injury associated with SCD lead to a state of oxidative stress due to an imbalance between production and elimination of the reactive oxygen species. 8 9 Furthermore, hemoglobin S has a high autoxidation rate which contributes to the oxidative stress in SCD patients. 8 9 As a result of the high-energy expenditure associated with the high rate of red cell turnover, SCD patients are at risk of multiple micronutrients deficiencies that could have an impact on SCD severity. 8 9 10 11 It has been reported that the concentrations of multiple micronutrients and trace elements tend to be low in patients with SCD. 8 9 10 11
Many of these micronutrients are involved in antioxidation mechanisms which are further compromised as a result of high oxidative stress in the sickled erythrocytes. 8 9 Of these trace elements, zinc, copper, and magnesium and their roles have been widely described in the literature. 8 9 Zinc and copper are essential cofactors for the optimal performance of superoxide dismutase, a scavengering enzyme responsible for detoxifying anion superoxide to hydrogen peroxide. However, copper could act as a prooxidant and promotes free radicals when it presents in high concentration in the state of impaired zinc bioavailability, a condition that has been previously described in various diseases, including SCD. 8 9 12 13 Also, magnesium has a role in the modulation of endothelial inflammation, besides its roles in regulating heart rhythm, immune system functions, and bone metabolism. 14
Several studies provided data on the status of these micronutrients in SCD but these data require further summary and analyses for better accuracy. This review aimed to provide a quantitative, comprehensive view of the status and extent of zinc, copper, and magnesium levels and deficiencies in SCD patients.
Methods
Search Strategy and Eligibility Criteria
This systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline. 15 16 A systematic search was performed in April 2021 through Medline, Embase, and PsycInfo databases from data of inception up to specified databases up to April 2021. Databases were queried for the terms ((zinc or magnesium or copper) AND (Sickle cell or Sickler)). Duplicate records were removed subsequently. We included studies reported sufficient data on the mean levels of zinc, magnesium, or copper among patients with SCD and their healthy controls for evidence synthesis. Neither age restriction nor specific population criteria were implemented. Studies with insufficient data, case reports, conference presentations, editorials, proposals, and abstracts were excluded.
The titles and abstracts of retrieved articles were screened by two independent reviewers for potential inclusion. Any discrepancy between the reviewers was resolved by consensus with a third reviewer. Full-text screening was done by two independent reviewers and any discrepancy between the reviewers was resolved by consensus with a third reviewer. Appraisal of individual study quality was performed by two independent reviewers using the Newcastle–Ottawa scale, a tool that determines the quality based on the selection of the study group, comparability of groups, and ascertainment of the exposure and outcomes. 17 Data extraction was done with a data collection sheet made in a Microsoft Excel Spreadsheet. When data were presented in medians and interquartile range, we transformed them into means and standard deviations. 18
Statistical Analysis
The standardized mean difference (SMD) was selected as a measurement tool to estimate the difference in serum levels of the targeted micronutrients. SMD was chosen as the included studies reported the results using different tools and measures. Statistical analysis was performed using R language v.4, using the “meta” and “metafor” packages, through the MARVIS app (Elkhidir, Ibrahim (2022): MARVIS. Figshare software). 19 20 21 22 Random effects models were used to pool the individual estimates and to accommodate for the heterogeneity in the reported pooled effect sizes. The effect size selected for statistical computation is the pooled SMD. Statistical heterogeneity was estimated using I 2 statistics and further assessed using subgroup analysis and metaregression. Publication bias was evaluated by both the Egger test and funnel plot visual analysis.
Result
Studies Characteristics
The search yielded a total of 986 records. After eliminating duplicate data, 696 studies were included for the title and abstract screening of which 599 were excluded due to irrelevance. Full texts of the remaining 97 records were screened with a subsequent exclusion of 54 records. A total of 36 studies published from 1974 to 2019 met the eligibility criteria and were further included for evidence synthesis; 15 from Africa, 9 from the United States, 8 from Asia, and 4 from Europe. 8 9 12 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 Details of the selection process are summarized in ( Fig. 1 ).
Fig. 1.
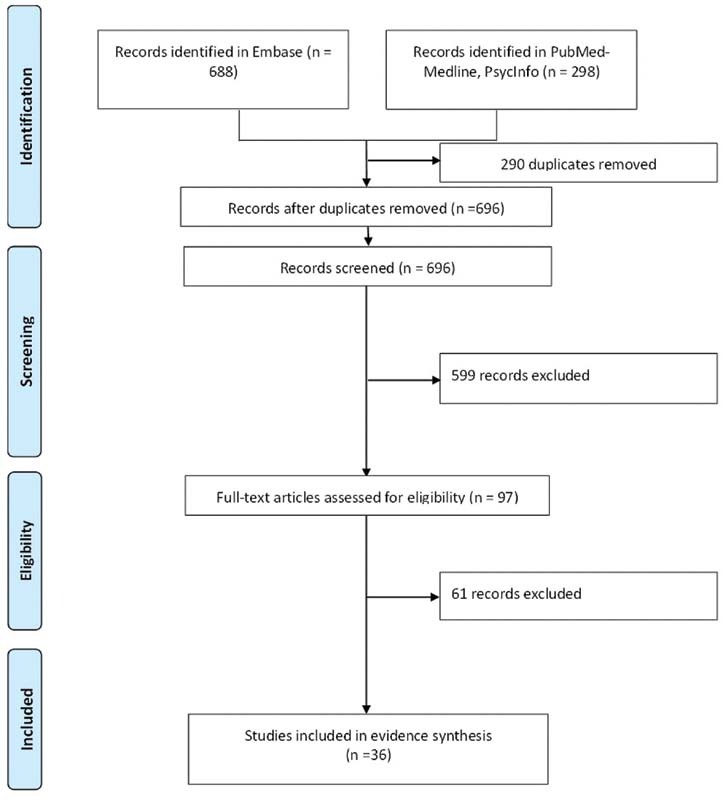
The flow diagram for the process of study selection.
Zinc
Discriptive summary of data for zinc in Table 1 . The pooled SMD of serum zinc across all included studies was −1.27 (95% confidence interval [CI]: −1.67 to −0.87, p < 0.001) with a prediction interval of (−3.44; 0.90; Fig. 2 ). A substantial heterogeneity across studies was noted ( I 2 = 95%, p < 0.001). A potential risk for publication bias was noted on visual examination of funnel plot and the Egger's test = − 2.14; p = 0.042. Subgroup analysis by study location as a grouping variable revealed that the Asian (−1.65), African (−1.63), and American (−0.71) studies have statistically significant SMD, unlike the European studies (−0.82). Year of publication explained approximately 10.34% ( R 2 ) of the total heterogeneity.
Table 1. Data of zinc between sickle cell disease patient(s) and non–sickle cell disease patient(s).
| Study | Location | Design | Sickle cell disease patient(s) | Non–sickle cell disease patient(s) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | |||
| Akinkugbe and Ette (1987) 37 | Africa | Cross-sectional | 53.45 | 25.19 | 40 | 79 | 61.6 | 20 |
| Alayash et al (1987) 49 | Asia | Cross-sectional | 113 | 35.9 | 57 | 117.43 | 34.1 | 45 |
| Al-Naama et al (2016) 51 | Asia | Cross-sectional | 62.2 | 12.6 | 42 | 94.2 | 12.5 | 50 |
| Antwi-Boasiako et al (2019) | Africa | Cross-sectional | 66.5 | 5.8 | 34 | 101.4 | 9.4 | 50 |
| Bashir (1995) 55 | Asia | Cross-sectional | 85.6 | 10.3 | 15 | 107.2 | 11.7 | 25 |
| Canellas et al (2012) 43 | The United States | Cross-sectional | 60 | 10 | 43 | 80 | 20 | 60 |
| Emokpae et al (2019) 59 | Africa | Case control | 46.26 | 1.986 | 74 | 54.6 | 1.237 | 50 |
| Hasanato et al (2019) 9 | Asia | Cross-sectional | 65.5 | 22.5926 | 33 | 94 | 13.75 | 33 |
| Karayalcin et al (1979) 23 | The United States | Cross-sectional | 114.9 | 22.2 | 46 | 133.63 | 24.36 | 46 |
| Karayalcin-zinc et al (1974) 24 | The United States | Cross-sectional | 116 | 33 | 50 | 177 | 49 | 50 |
| Kehinde et al (2011) 25 | Africa | Cross-sectional | 70 | 6 | 20 | 70 | 7 | 20 |
| Kilinç et al (1991) 28 | Europe | Case control | 58 | 18.6529 | 20 | 96.4 | 22.8 | 20 |
| Kudirat et al (2019) 30 | Africa | Descriptive longitidual | 23.4 | 7.4 | 70 | 48.9 | 14.4 | 70 |
| Kuvibidila et al (2006) 31 | The United States | Case control | 96.1 | 20.5 | 90 | 95.1 | 46.1 | 82 |
| Olaniyi et al (2010) 36 | Africa | Case control | 1320 | 230 | 59 | 1170 | 200 | 35 |
| Oliveira et al (2001) 56 | The United States | Case control | 85.15 | 32.18 | 34 | 108.45 | 22.89 | 20 |
| Onukwuli et al (2018) 39 | Africa | Cross-sectional, case control | 58.01 | 10.58 | 81 | 68.37 | 8.67 | 81 |
| Oztas et al (2012) 40 | Europe | Case control | 158.3 | 13.8 | 15 | 154.1 | 22.4 | 10 |
| Phebus et al (1988) 41 | The United States | Case control | 76.3 | 8.9 | 56 | 82.2 | 9.8 | 44 |
| Prasad et al (1976) | The United States | Case control | 104 | 10.5 | 84 | 113 | 13.6 | 70 |
| Smith et al (2019) 42 | Africa | Cross-sectional | 101 | 13.4683 | 80 | 105.7 | 11.5 | 80 |
| Wasnik et al (2017) 44 | Asia | Cross-sectional | 83.09 | 9.26 | 33 | 104.06 | 6.27 | 33 |
| Yousif et al (2018) 45 | Asia | Case control | 67.25 | 17.78 | 87 | 90.34 | 16.38 | 90 |
| Yuzbasiyan et al (1989) 46 | The United States | Case control | 87 | 17 | 7 | 83 | 17 | 8 |
| Arinola et al (2008) 50 | Africa | Case control | 11.2545 | 5.66609 | 44 | 15.94 | 5.51066 | 50 |
| Arcasoy et al (2001) 48 | Europe | Case control | 77.3 | 15.74 | 10 | 90.04 | 13.83 | 20 |
| Durosinmi et al (1993) 57 | Africa | Case control | 2.89 | 0.73 | 18 | 5.21 | 1.97 | 27 |
| Sungu et al (2018) 8 | Africa | Case control | 0.27 | 0.58 | 76 | 1.64 | 0.14 | 76 |
Fig. 2.
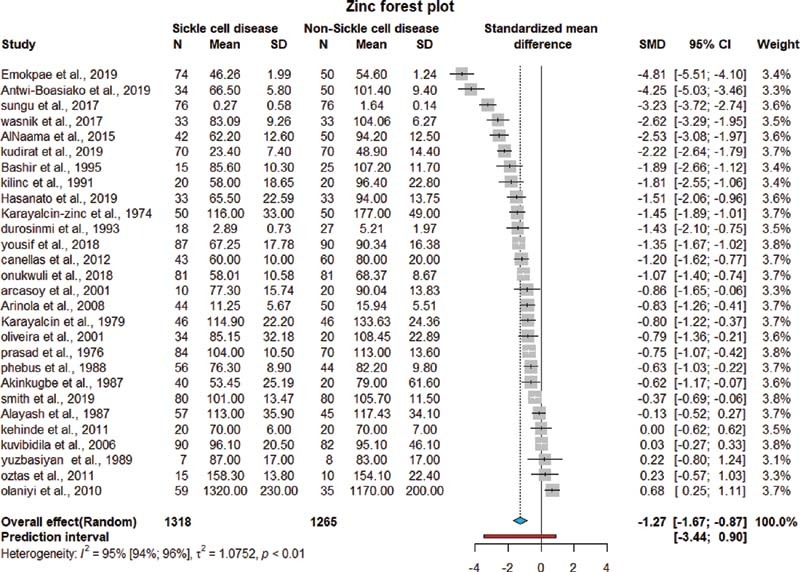
Pooled SMD of zinc levels among patients with SCD. CI, confidence interval; SCD, sickle cell disease; SD, standard deviation; SMD, standardadized mean difference.
Magnesium
Discriptive summary of data for magnesium in Table 2 . The pooled SMD of serum magnesium across all included studies was −0.53 (95% CI: −1.0 to −0.06, p < 0.026) with a prediction interval of (−1.0; 1.25; Fig. 3 ). A substantial heterogeneity across studies was noted ( I 2 = 92%, p < 0.01). No potential risk for publication bias was noted visual examination of the funnel plot and the Egger's test was 0.964, p = 0.36. Subgroup analysis by study location as a grouping variable revealed that SMD was only significant among American studies. Both location and year explained 17.20% ( R 2 ) of the total heterogeneity. Testing for residual heterogeneity was significant (QE [df = 6] = 98.3528, p < 0.001), indicating that there are other factors not included in the model that significantly contributing to the high heterogeneity.
Table 2. Data of magnesium between sickle cell disease patient(s) and non–sickle cell disease patient(s).
| Study | Location | Design | Sickle cell disease patient(s) | Non–sickle cell disease patient(s) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | |||
| Antwi-Boasiako et al (2019) | Africa | Case control | 0.79 | 0.25 | 79 | 0.90 | 0.11 | 48 |
| Elshal et al (2012) 58 | Asia | Case control | 0.79 | 0.13 | 60 | 0.85 | 0.17 | 20 |
| Khan (2003) 27 | Asia | Case control | 0.84 | 0.09 | 51 | 0.78 | 0.05 | 29 |
| Kontessis et al (1992) 29 | Europe | Case control | 0.77 | 0.10 | 8 | 0.85 | 0.10 | 14 |
| Olaniyi et al (2010) 36 | Africa | Case control | 0.39 | 0.09 | 59 | 0.38 | 0.08 | 35 |
| Olukoga et al (1993) 38 | Africa | Case control | 0.76 | 0.10 | 25 | 0.83 | 0.15 | 25 |
| Prasad et al (1976) | The United States | Case control | 0.78 | 0.10 | 29 | 0.82 | 0.08 | 38 |
| Sungu et al (2018) 8 | Africa | Case control | 0.13 | 0.02 | 76 | 0.42 | 0.21 | 76 |
| Yousif et al (2018) 45 | Asia | Case control | 0.55 | 0.19 | 87 | 0.77 | 0.11 | 90 |
| Zehtabchi et al (2004) | The United States | Case control | 0.79 | 0.09 | 74 | 0.81 | 0.07 | 32 |
Fig. 3.
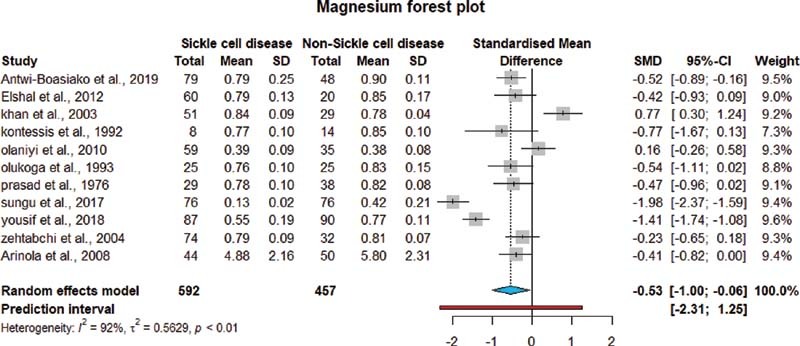
Pooled SMD of magnesium levels among patients with SCD. CI, confidence interval; SCD, sickle cell disease; SD, standard deviation; SMD, standardadized mean difference.
Copper
Discriptive summary of data for copper in Table 3 . The pooled SMD of serum copper across all included studies was 0.68 (95% CI: 0.05–1.32, p < 0.004), with a prediction interval of (−2.29; 3.66; Fig. 4 ). A substantial heterogeneity across studies was noted ( I 2 = 97%, p < 0.001). On visual examination of funnel plot, no potential risk for publication bias was noted and the Egger's test statistics was 0.561, p = 0.58. Subgroup analysis by study location as a grouping variable, revealed that SMD was only significant among Asian studies. Between group difference is significant ( Q = 12.01865, df = 3, p = 0.007). Mixed model of study location and year of publication explained approximately 21.77% ( R 2 ) of the total heterogeneity. Testing for residual heterogeneity was significant (QE [df = 5] = 242.2145, p < 0.001), indicating that there are other factors not included in the model that significantly contributing to the high heterogeneity.
Table 3. Data of copper between sickle cell disease patient(s) and non–sickle cell disease patient(s).
| Study | Location | Design | Sickle cell disease patient(s) | Non–sickle cell disease patient(s) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean.c | SD | n | |||
| Akinkugbe and Ette (1987) 37 | Africa | Cross-sectional | 70.40 | 42.62 | 40 | 89.30 | 61.30 | 20 |
| Alayash et al (1987) 49 | Asia | Cross-sectional | 144.93 | 44.09 | 57 | 148.40 | 44.40 | 45 |
| Al-Naama et al, (2016) 51 | Asia | Cross-sectional | 145.50 | 14.30 | 42 | 100.90 | 13.50 | 50 |
| Antwi-Boasiako et al, 2019 | Africa | Cross-sectional | 220.90 | 27.80 | 34 | 114.00 | 16.30 | 50 |
| Bashir (1995) 55 | Asia | Cross-sectional | 131.30 | 11.50 | 15 | 109.00 | 15.10 | 25 |
| Canellas et al (2012) 43 | The United States | Cross-sectional | 120.00 | 10.00 | 43 | 100.00 | 10.00 | 60 |
| Emokpae et al (2019) 59 | Africa | Case control | 105.80 | 2.46 | 74 | 102.60 | 1.59 | 50 |
| Erhabor et al (2019) 60 | Africa | Case control | 40.40 | 9.66 | 45 | 75.60 | 6.50 | 25 |
| Hasanato et al (2019) 9 | Asia | Cross-sectional | 131.67 | 15.56 | 33 | 88.00 | 10.50 | 33 |
| kehinde et al (2011) 25 | Africa | Cross-sectional | 6.00 | 2.00 | 20 | 7.00 | 3.00 | 20 |
| Kilinç et al (1991) 28 | Europe | Case control | 133.80 | 64.67 | 20 | 168.70 | 39.30 | 20 |
| Mukuku et al (2018) 33 | Africa | Case control | 172.00 | 15.00 | 76 | 189.00 | 20.00 | 76 |
| Olaniyi et al (2010) 36 | Africa | Case control | 67.00 | 10.10 | 59 | 68.50 | 10.00 | 35 |
| Oztas et al (2012) 40 | Europe | Case control | 95.90 | 9.90 | 15 | 96.30 | 9.10 | 10 |
| Prasad et al, 1976 | The United States | Case control | 126.00 | 25.00 | 41 | 116.00 | 19.00 | 60 |
| Smith et al (2019) 42 | Africa | Cross-sectional | 144.00 | 17.09 | 80 | 116.00 | 27.70 | 80 |
| Yousif et al (2018) 45 | Asia | Case control | 142.35 | 49.92 | 87 | 109.66 | 24.42 | 90 |
Fig. 4.
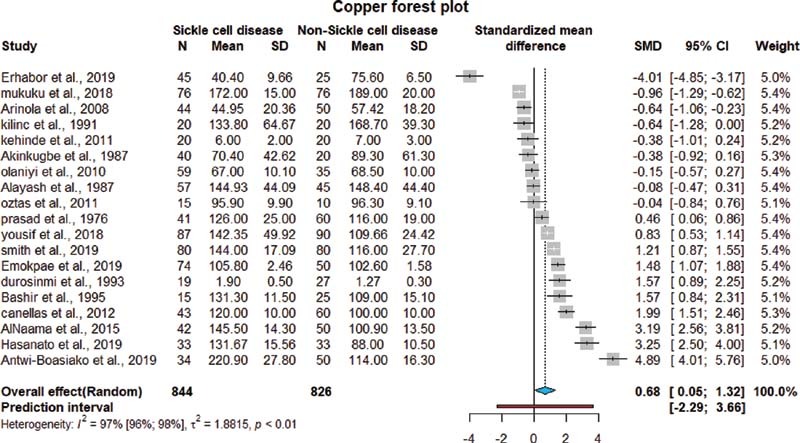
Pooled SMD of copper levels among patients with SCD. CI, confidence interval; SCD, sickle cell disease; SD, standard deviation; SMD, standardadized mean difference.
Discussion
This review aimed to provide an overarching resource about the status of zinc, magnesium, and copper in SCD patients. Most of the studies (28 out of 36) focused on zinc serum level among patients with SCD. The analyses showed that both zinc and magnesium levels were lower in SCD patients, whereas copper level was higher among them. These findings coincide with the known nature of the chronic inflammatory process occurring in SCD associated with ischemia-reperfusion injury, excessive production of free radicals like superoxide, and hydrogen peroxide. 61 62 Additionally, due to the norable heterogeneity in SMD meta-anaylsis, subgroup analysis was done, and the Asian and African descent had significanly lower values than both American and European. This stress on the importance of race and ethnicity on the clinical outcome in SCD patients which is well established in the literature. 63 The high copper values in these patients may be attributed to the chronic hemolysis state and aggravated by the coexisting zinc deficieny. In two studies by Antwi-Boasiako et al and Osredkar and Sustar et al, they discovered that serum copper is influenced by zinc bioavailability, as they observe that zinc deficiency significantly enhance copper absorption from the gut. 12 64 Additionally, high copper may promote a prooxidant state as illustrated by Chirico and Pialoux. 65 Although there is noted heterogenity using I 2 statistics, most of included studies for zinc and magnesium had a pattern of consistency across them that nearly 22 studies out of 28 fall below SMD of 0 for zinc, and 10 out of 12 studies for magnesium that fell below a SMD of 0 which, in fact, explained by Borenstein et al which concluded that not to miss such patterns in expense of high heterogeneity. 66
The differences noted in these trace elements levels between SCD patients and others could be attributed to several peculiar characteristics of SCD such as increased physiological demands due to the fast rate of erythrocytosis and red blood cells turnover in SCD, impact of suboptimal renal function, glomerular injury in SCD, and impaired absorption by the damaged intestinal mucosa as a complication of SCD. 8 42 67 There are implications to the reported findings. From a clinical perspective, the SCD patients might have benefited from nutritional supplementations with these elements, as it has been reported by previous studies 13 68 but nutritional guidelines concerning the performance of these micronutrients in SCD patients are still not broadly available. 13
From a research perspective, the paucity of data on clinical outcomes of trace elements deficiencies needs to be addressed and could benefit from further studies to give a better understanding of the exact pathogenesis and effects of such deficiencies.
Limitations
The results of this review need to be considered in the context of some limitations. The protocol of the study was not registered in PROSPERO which is a well-known review registry portal. 69 The inclusion of observational studies published only in English which might compromise representativeness, as well as the notable heterogeneity among studies, which was partially explained by some demographic variables. In addition, despite the paucity of data on the clinical outcomes associated with these trace element deficiencies, it does not mean that the laboratory findings cannot have implications on clinical significance, but the included studies used different tools making using the raw mean difference difficult to implement.
Conclusion
This review showed that SCD patients may potentially prompt to have lower zinc and magnesium levels and higher copper levels compared with those without the disease. Future research needs to be directed to investigate clinical outcome of nutritional difficiencies in patients with SCD, as well as the possibility of implementing nutritional supplements programs which may help minimizing the harmful effects of the disease on human body.
Funding Statement
Funding None.
Conflict of Interest None declared.
Authors' Contributions'
S.O.O.M. and I.H.E. conceptualized the research idea and designed the study; R.H.S.S., W.M.E., H.R.M., and R.A.B. undertook articles searching, articles assessment, and review; and S.S.A. and W.K.A.) undertook data extraction and analysis. All authors interpreted the results and drafted the manuscript. All authors revised and approved the final manuscript.
Availability of Data and Material
The dataset generated during this study are available from the corresponding author on reasonable request.
References
- 1.Chakravorty S, Williams T N. Sickle cell disease: a neglected chronic disease of increasing global health importance. Arch Dis Child. 2015;100(01):48–53. doi: 10.1136/archdischild-2013-303773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brousse V, Makani J, Rees D C. Management of sickle cell disease in the community. BMJ. 2014;348:g1765. doi: 10.1136/bmj.g1765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wastnedge E, Waters D, Patel S. The global burden of sickle cell disease in children under five years of age: a systematic review and meta-analysis. J Glob Health. 2018;8(02):21103. doi: 10.7189/jogh.08.021103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Farooq S, Testai F D. Neurologic complications of sickle cell disease. Curr Neurol Neurosci Rep. 2019;19(04):17. doi: 10.1007/s11910-019-0932-0. [DOI] [PubMed] [Google Scholar]
- 5.Pinto V M, Balocco M, Quintino S, Forni G L. Sickle cell disease: a review for the internist. Intern Emerg Med. 2019;14(07):1051–1064. doi: 10.1007/s11739-019-02160-x. [DOI] [PubMed] [Google Scholar]
- 6.Kosaraju V, Harwani A, Partovi S.Imaging of musculoskeletal manifestations in sickle cell disease patients Br J Radiol 201790(1073):2.016013E7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Barden E M, Kawchak D A, Ohene-Frempong K, Stallings V A, Zemel B S. Body composition in children with sickle cell disease. Am J Clin Nutr. 2002;76(01):218–225. doi: 10.1093/ajcn/76.1.218. [DOI] [PubMed] [Google Scholar]
- 8.Sungu J K, Mukuku O, Mutombo A M, Mawaw P, Aloni M N, Luboya O N. Trace elements in children suffering from sickle cell anemia: a case-control study. J Clin Lab Anal. 2018;32(01):e22160. doi: 10.1002/jcla.22160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hasanato R. Alterations in serum levels of copper, zinc, and selenium among children with sickle cell anemia. Turk J Med Sci. 2019;49(05):1287–1291. doi: 10.3906/sag-1812-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mandese V, Marotti F, Bedetti L, Bigi E, Palazzi G, Iughetti L. Effects of nutritional intake on disease severity in children with sickle cell disease. Nutr J. 2016;15(01):46. doi: 10.1186/s12937-016-0159-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mohamed S OO, Mohamed Elmugadam F AA, Awadalla H FM. A meta-analysis on vitamin D deficiency in patients with sickle cell disease. Med J. 2020;2(03):95–100. [Google Scholar]
- 12.Antwi-Boasiako C, Dankwah G B, Aryee R. Serum iron levels and copper-to-zinc ratio in sickle cell disease. Medicina (Kaunas) 2019;55(05):1–7. doi: 10.3390/medicina55050180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Delesderrier E, Curioni C, Omena J, Macedo C R, Cople-Rodrigues C, Citelli M.Antioxidant nutrients and hemolysis in sickle cell diseaseClin Chim Acta [DOI] [PubMed]
- 14.Than N N, Soe H HK, Palaniappan S K, Abas A BL, De Franceschi L. Magnesium for treating sickle cell disease. Cochrane Database Syst Rev. 2017;4(04):CD011358. doi: 10.1002/14651858.CD011358.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Liberati A, Altman D G, Tetzlaff J. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi: 10.1136/bmj.b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.PRISMA Group . Moher D, Liberati A, Tetzlaff J, Altman D G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi: 10.1136/bmj.b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wells G, Shea B, O'Connell D, Peterson J.The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analysesAccessed April 21, 2022 at:http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
- 18.Hozo S P, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5(01):13. doi: 10.1186/1471-2288-5-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Viechtbauer W. Conducting meta-analyses in {R} with the {metafor} package. J Stat Softw. 2010;36(03):1–48. [Google Scholar]
- 20.R Core Team R: a language and environment for statistical computingAccessed April 21, 2022 at:https://www.r-project.org/
- 21.Metaprop: meta-analysis of single proportions. In meta: general package for meta-analysis. Accessed June 18, 2020 at:https://rdrr.io/cran/meta/man/metaprop.html
- 22.Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(04):153–160. doi: 10.1136/ebmental-2019-300117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Karayalcin G, Lanzkowsky P, Kazi A B. Zinc deficiency in children with sickle cell disease. Am J Pediatr Hematol Oncol. 1979;1(03):283–284. [PubMed] [Google Scholar]
- 24.Karayalcin G, Rosner F, Kim K Y, Chandra P.Letter: plasma-zinc in sickle cell-anaemia Lancet 19741(7850):217. [DOI] [PubMed] [Google Scholar]
- 25.Kehinde M O, Jaja S I, Adewumi O M, Adeniyi I M, Nezianya M O, Ayinla E O. Liver enzymes and trace elements in the acute phase of sickle cell anaemia. West Afr J Med. 2010;29(04):244–248. doi: 10.4314/wajm.v29i4.68244. [DOI] [PubMed] [Google Scholar]
- 26.Abshire T C, English J L, Githens J H, Hambidge M. Zinc status in children and young adults with sickle cell disease. Am J Dis Child. 1988;142(12):1356–1359. doi: 10.1001/archpedi.1988.02150120110052. [DOI] [PubMed] [Google Scholar]
- 27.Khan J AJ. Vitamin D status and serum level of some elements in children with sickle cell disease in Jeddah, Saudi Arabia. Pak J Med Sci. 2003;19(04):295–299. [Google Scholar]
- 28.Kilinç Y, Kümi M, Yilmaz B, Tanyeli A.A comparative study of zinc and copper values in serum, erythrocytes and urine in sickle cell homozygotes and heterozygotes Acta Paediatr Scand 199180(8-9):873–874. [DOI] [PubMed] [Google Scholar]
- 29.Kontessis P, Mayopoulou-Symvoulidis D, Symvoulidis A, Kontopoulou-Griva I. Renal involvement in sickle cell-beta thalassemia. Nephron. 1992;61(01):10–15. doi: 10.1159/000186827. [DOI] [PubMed] [Google Scholar]
- 30.Kudirat A A, Shehu U A, Kolade E, Ibrahim M. Serum zinc level during and after acute painful episodes in children with sickle cell anemia at the aminu kano teaching hospital, Kano, Northern Nigeria. Niger J Clin Pract. 2019;22(01):16–23. doi: 10.4103/njcp.njcp_169_18. [DOI] [PubMed] [Google Scholar]
- 31.Kuvibidila S R, Sandoval M, Lao J. Plasma zinc levels inversely correlate with vascular cell adhesion molecule-1 concentration in children with sickle cell disease. J Natl Med Assoc. 2006;98(08):1263–1272. [PMC free article] [PubMed] [Google Scholar]
- 32.Leonard M B, Zemel B S, Kawchak D A, Ohene-Frempong K, Stallings V A.Plasma zinc status, growth, and maturation in children with sickle cell disease J Pediatr 1998132(3 Pt 1):467–471. [DOI] [PubMed] [Google Scholar]
- 33.Mukuku O, Sungu J K, Mutombo A M. Albumin, copper, manganese and cobalt levels in children suffering from sickle cell anemia at Kasumbalesa, in Democratic Republic of Congo. BMC Hematol. 2018;18(01):23. doi: 10.1186/s12878-018-0118-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Niell H B, Leach B E, Kraus A P. Zinc metabolism in sickle cell anemia. JAMA. 1979;242(24):2686–2687. [PubMed] [Google Scholar]
- 35.Oladipo O O, Temiye E O, Ezeaka V C, Obomanu P. Serum magnesium, phosphate and calcium in Nigerian children with sickle cell disease. West Afr J Med. 2005;24(02):120–123. doi: 10.4314/wajm.v24i2.28180. [DOI] [PubMed] [Google Scholar]
- 36.Olaniyi J A, Arinola O G. Nitric oxide and trace metals in relation to haemoglobin F concentration in Nigerian sickle cell disease patients. Turk J Med Sci. 2010;40(01):109–113. [Google Scholar]
- 37.Akinkugbe F M, Ette S I. Role of zinc, copper, and ascorbic acid in some common clinical paediatric problems. J Trop Pediatr. 1987;33(06):337–342. doi: 10.1093/tropej/33.6.337. [DOI] [PubMed] [Google Scholar]
- 38.Olukoga A O, Adewoye H O, Erasmus R T, Adedoyin M A. Urinary magnesium excretion in steady-state sickle cell anaemia. Acta Haematol. 1993;90(03):136–138. doi: 10.1159/000204394. [DOI] [PubMed] [Google Scholar]
- 39.Onukwuli V O, Chinawa J, Eke C B, Nwokocha A R, Emodi I J, Ikefuna A N. Impact of zinc on sexual maturation of female sickle cell anemia (SCA) children in Enugu, Southeast Nigeria. Pediatr Hematol Oncol. 2018;35(02):145–155. doi: 10.1080/08880018.2018.1469706. [DOI] [PubMed] [Google Scholar]
- 40.Oztas Y, Durukan I, Unal S, Ozgunes N. Plasma protein oxidation is correlated positively with plasma iron levels and negatively with hemolysate zinc levels in sickle-cell anemia patients. Int J Lab Hematol. 2012;34(02):129–135. doi: 10.1111/j.1751-553X.2011.01369.x. [DOI] [PubMed] [Google Scholar]
- 41.Phebus C K, Maciak B J, Gloninger M F, Paul H S. Zinc status of children with sickle cell disease: relationship to poor growth. Am J Hematol. 1988;29(02):67–73. doi: 10.1002/ajh.2830290203. [DOI] [PubMed] [Google Scholar]
- 42.Smith O S, Ajose O A, Adegoke S A. Plasma level of antioxidants is related to frequency of vaso-occlusive crises in children with sickle cell anaemia in steady state in Nigeria. Pediatr Hematol Oncol J. 2019;4(01):17–22. [Google Scholar]
- 43.Canellas C GL, Carvalho S MF, Anjos M J, Lopes R T. Determination of Cu/Zn and Fe in human serum of patients with sickle cell anemia using radiation synchrotron. Appl Radiat Isot. 2012;70(07):1277–1280. doi: 10.1016/j.apradiso.2011.12.028. [DOI] [PubMed] [Google Scholar]
- 44.Wasnik R R, Akarte N R. Evaluation of serum zinc and antioxidant vitamins in adolescent homozygous sickle cell patients in Wardha, district of central India. J Clin Diagn Res. 2017;11(08):BC01–BC03. doi: 10.7860/JCDR/2017/30855.10320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Yousif O O, Hassan M K, Al-Naama L M. Red blood cell and serum magnesium levels among children and adolescents with sickle cell anemia. Biol Trace Elem Res. 2018;186(02):295–304. doi: 10.1007/s12011-018-1307-0. [DOI] [PubMed] [Google Scholar]
- 46.Yuzbasiyan-Gurkan V A, Brewer G J, Vander A J, Guenther M J, Prasad A S. Net renal tubular reabsorption of zinc in healthy man and impaired handling in sickle cell anemia. Am J Hematol. 1989;31(02):87–90. doi: 10.1002/ajh.2830310203. [DOI] [PubMed] [Google Scholar]
- 47.Zehtabchi S, Sinert R, Rinnert S. Serum ionized magnesium levels and ionized calcium-to-magnesium ratios in adult patients with sickle cell anemia. Am J Hematol. 2004;77(03):215–222. doi: 10.1002/ajh.20187. [DOI] [PubMed] [Google Scholar]
- 48.Arcasoy A, Canata D, Sinav B, Kutlay L, Oğuz N, Şen M.Serum zinc levels and zinc binding capacity in thalassemia J Trace Elem Med Biol 200115(2-3):85–87. [DOI] [PubMed] [Google Scholar]
- 49.Alayash A I, Dafallah A, Al-Quorain A, Omer A H, Wilson M T. Zinc and copper status in patients with sickle cell anemia. Acta Haematol. 1987;77(02):87–89. doi: 10.1159/000205975. [DOI] [PubMed] [Google Scholar]
- 50.Arinola O G, Olaniyi J A, Akiibinu M O. Evaluation of antioxidant levels and trace element status in Nigerian sickle cell disease patients with plasmodium parasitaemia. Pak J Nutr. 2008;7(06):766–769. [Google Scholar]
- 51.Al-Naama L M, Hassan M K, Mehdi J K. Association of erythrocytes antioxidant enzymes and their cofactors with markers of oxidative stress in patients with sickle cell anemia. Qatar Med J. 2016;2015(02):14. doi: 10.5339/qmj.2015.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Aloni M N, Lecerf P, Lê P-Q. Is Pica under-reported in children with sickle cell disease? A pilot study in a Belgian cohort. Hematology. 2015;20(07):429–432. doi: 10.1179/1607845414Y.0000000219. [DOI] [PubMed] [Google Scholar]
- 53.Antwi-Boasiako C, Kusi-Mensah Y A, Hayfron-Benjamin C. Total serum magnesium levels and calcium-to-magnesium ratio in sickle cell disease. Medicina (Kaunas) 2019;55(09):1–8. doi: 10.3390/medicina55090547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Claster S, Wood J C, Noetzli L. Nutritional deficiencies in iron overloaded patients with hemoglobinopathies. Am J Hematol. 2009;84(06):344–348. doi: 10.1002/ajh.21416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bashir N A. Serum zinc and copper levels in sickle cell anaemia and β-thalassaemia in North Jordan. Ann Trop Paediatr. 1995;15(04):291–293. doi: 10.1080/02724936.1995.11747786. [DOI] [PubMed] [Google Scholar]
- 56.Oliveira P M, Póvoa L C, Oliveira M HCF, Pfeiffer W C. Study of zinc and growth hormone in sickle cell disease. J Pediatr Endocrinol Metab. 2001;14(06):773–779. doi: 10.1515/jpem.2001.14.6.773. [DOI] [PubMed] [Google Scholar]
- 57.Durosinmi M A, Ojo J O, Oluwole A F, Akanle O A, Arshed W, Spyrou N M. Trace elements in sickle cell disease. J Radioanal Nucl Chem Article. 1993;168(01):233–242. [Google Scholar]
- 58.Elshal M F, Bernawi A E, Al-Ghamdy M A, Jalal J A. The association of bone mineral density and parathyroid hormone with serum magnesium in adult patients with sickle-cell anaemia. Arch Med Sci. 2012;8(02):270–276. doi: 10.5114/aoms.2012.28554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Emokpae M A, Fatimehin E B, Obazelu P A. Serum levels of copper, zinc and disease severity scores in sickle cell disease patients in Benin City, Nigeria. Afr Health Sci. 2019;19(03):2798–2805. doi: 10.4314/ahs.v19i3.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Erhabor O, Ogar K, Erhabor T, Dangana A. Some haematological parameters, copper and selenium level among children of African descent with sickle cell disease in Specialist Hospital Sokoto, Nigeria. Hum Antibodies. 2019;27(03):143–154. doi: 10.3233/HAB-180360. [DOI] [PubMed] [Google Scholar]
- 61.Ansari J, Gavins F NE. Ischemia-reperfusion injury in sickle cell disease: from basics to therapeutics. Am J Pathol. 2019;189(04):706–718. doi: 10.1016/j.ajpath.2018.12.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Granger D N, Kvietys P R. Reperfusion injury and reactive oxygen species: the evolution of a concept. Redox Biol. 2015;6:524–551. doi: 10.1016/j.redox.2015.08.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Reinier K, Rusinaru C, Chugh S S. Race, ethnicity, and the risk of sudden death. Trends Cardiovasc Med. 2019;29(02):120–126. doi: 10.1016/j.tcm.2018.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Osredkar J, Sustar N. Copper and zinc, biological role and significance of copper/zinc imbalance. J Clin Toxicol. 2011;S3:1. [Google Scholar]
- 65.Chirico E N, Pialoux V. Role of oxidative stress in the pathogenesis of sickle cell disease. IUBMB Life. 2012;64(01):72–80. doi: 10.1002/iub.584. [DOI] [PubMed] [Google Scholar]
- 66.Borenstein M, Hedges L V, Higgins J PT, Rothstein H R. Introduction to meta-analysis. Statistics and Data Science. 2009 doi: 10.1002/9780470743386. [DOI] [Google Scholar]
- 67.Emokpae M, Tijani A. The impact of proteinuria on serum levels of trace elements in sickle cell disease patients. J Med Biomed Sci. 2015;3(03):16–20. [Google Scholar]
- 68.Zemel B S, Kawchak D A, Fung E B, Ohene-Frempong K, Stallings V A. Effect of zinc supplementation on growth and body composition in children with sickle cell disease. Am J Clin Nutr. 2002;75(02):300–307. doi: 10.1093/ajcn/75.2.300. [DOI] [PubMed] [Google Scholar]
- 69.PROSPERO is fast-tracking registration of protocols related to COVID-19. Accessed February 28, 2022 at:https://www.crd.york.ac.uk/prospero/
- 70.Prasad A S, Ortega J, Brewer G J, Oberleas D, Schoomaker E B. Trace elements in sickle cell disease. JAMA. 1976;235(22):2396–2398. [PubMed] [Google Scholar]