

Abstract
A rapid outbreak of monkeypox is ongoing in non-endemic countries since May 2022. We report the first case of monkeypox in the Republic of Korea. This occurred in a 34-year-old male patient who traveled to Europe in June 2022. On the day of his return to the Republic of Korea (June 21, 2022), the patient presented with a genital lesion. The results of the monkeypox real-time polymerase chain reaction tests were positive in the penile ulcer, oropharyngeal and nasopharyngeal specimens. The patient subsequently developed fever and skin rash after hospital admission. Careful history taking along physical examination should be conducted in the patients who have epidemiologic risk factors for monkeypox. Moreover, appropriate specimens should be obtained from lesions and tested for the monkeypox virus.
Keywords: Monkeypox, Diagnosis, Republic of Korea
Graphical Abstract
An outbreak of monkeypox in nonendemic countries was first reported in Europe in May 20221; further cases continued to be reported worldwide. In the majority of cases, patients had no travel history to the endemic areas of central and western Africa, and were diagnosed through primary care and sexual health services. The cases were mainly reported in homosexual, bisexual or other men who have sex with men.2,3
Here we report the first case of monkeypox in an individual diagnosed in the Republic of Korea after returning from Europe.
A 34-year-old Korean man arrived from Germany at Incheon International Airport, Republic of Korea on June 21, 2022. He had experienced a headache 3 days before arrival, and on the day of arrival he found some skin lesions. On the day of arrival, he also learned that his male friend in Germany undergone a diagnostic test for monkeypox at a German hospital. The patient alerted the Korea Disease Control and Prevention Agency (KDCA) about his medical condition and contact history with the person suspected of having monkeypox, and reported this information at the airport. He was quarantined at the airport, then moved to Incheon Medical Center, and hospitalized in a designated isolation room.
The patient was bisexual, and had no relevant medical history. He visited Germany from June 1 to June 21, 2022, and stayed with a male friend during his stay in Germany from June 1 to June 14, 2022. He denied having sexual intercourse with anyone, including his male friend, or interactions with animals or animal carcasses during his trip. He did not know that he had skin lesions until he discovered them on the day of arrival.
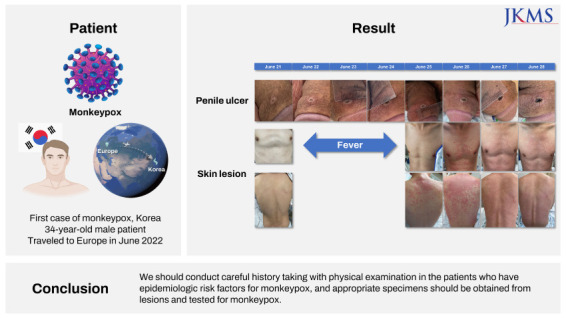
On examination at Incheon Medical Center (hospital day 1), perioral erosive lesions covered with black crusts were found on his face and some tiny papules scattered across his back and lower abdomen, but there were no vesicular or pustular eruptions. There was one painless ulcer on the dorsum of the distal one-third of his penile shaft, measuring 7 mm in diameter and well-circumscribed with central umbilication (Fig. 1). Bilateral enlarged and tender lymph nodes were observed in his groin. On hospital day 2, he began experiencing chilling, sore throat, subjective fever (up to 38.6°C), which are characteristic signs and symptoms of the monkeypox prodrome. On hospital day 5, an erythematous, maculopapular rash appeared on his upper back that extended down his body to involve the extremities (Fig. 1).
Fig. 1. Photographs of the penile ulcer and the skin lesions. Non-tender ulcer on the dorsum of the penile shaft, measuring 7 mm in diameter with central umbilication. Erythematous, maculopapular lesions appreaed on the upper back and proceeded down the body. Red-colored line indicates the period of fever (≥ 37.5°C). The figures are published under agreement of the patient.

His blood electrolytes and glucose levels were normal, as were the results of liver and kidney function test. A blood test result for syphilis and human immunodeficiency virus was negative, and urinary test result for Neisseria gonorrhoeae and Chlamydia trachomatis nucleic acids were negative. Specimens from skin lesions for polymerase chain reaction (PCR) testing were collected as follows: the central dry base of the penile ulcer was scratched with a disposable scalpel after sanitizing the lesion and then the base of the lesion brushed with a sterile polyester swab several times; swabs and crusts were obtained from the perioral erosion after crust removal. Nasopharyngeal and oropharyngeal swabs were also collected. These clinical specimens, and blood samples were sent to the KDCA for detection of the monkeypox virus.
For diagnostic confirmation of the monkeypox, viral DNAs were isolated from the eight specimens of the patient by using the QIAamp DNA blood Mini Kit (QIAGEN, Crawley, UK) and real-time PCR assays specific to the monkeypox virus were performed with the viral DNAs using a laboratory-developed real-time PCR kit. The monkeypox virus real-time PCR test result were positive in viral transport medium (VTM) of skin lesion from penis and oropharyngeal plus nasopharyngeal swabs in VTM and dry swabs. In addition, conventional PCR detecting the two genes (B2R and ATI) of the monkeypox viruses showed that the skin lesion swab in VTM from the penis of eight specimens were positive. Subsequent sequencing of the PCR amplicons (F3L, A39R, B2R and ATI genes) showed that the sequences of the amplicons were identical with those of the monkeypox viruses (Supplementary Table 1). Collectively, these data confirmed the diagnosis of monkeypox; this patient was the first in the Republic of Korea.
Monkeypox usually causes a characteristic rash that is differentiated from other vesicular eruptions. However, during the outbreak of monkeypox outside endemic areas in Africa since May 2022, some patients have presented with genital or rectal lesions without the characteristic rash of monkeypox.2,3,4,5 Moreover, most cases were identified in homosexual, bisexual, or other men who had sex with men. One hypothesis is that monkeypox may be spread by close contact during sexual activity.1,5,6 The initial presentation of a penile ulcer before prodrome in this case as well as the patient’s contact history also suggests that close contact during sexual exposure might have been the route of acquisition. However, this theory warrants further research with a larger numbers of patients.
The early clinical presentation of monkeypox may be similar to that of some sexually transmitted infections, such as syphilis, herpes, or lymphogranuloma venereum.5 In this case, the rash, which occurred about 4 days after the fever, was different from that of typical monkeypox and was similar to that of other viruses such as measles or of noninfectious etiologies such as adverse drug reactions.7 Therefore, a careful history taking should be undertaken along with physical examination in the patients who have epidemiologic risk factors for monkeypox; in addition, appropriate specimens should be obtained from lesions and tested for the monkeypox virus.
Ethics statement
The patient provided informed consent and agreed to publication of the images.
Footnotes
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Jang YR, Kim JY.
- Data curation: Jang YR, Kim JY, Kim J, Na HK.
- Formal analysis: Jang YR, Lee M, Shin H, Kim JW, Choi MM, Kim YM, Lee MJ, Kim JY.
- Investigation: Jang YR, Lee M, Shin H, Kim JW, Choi MM, Kim YM, Lee MJ, Kim JY.
- Visualization: Jang YR, Kim JY.
- Writing - original draft: Jang YR, Lee M, Shin H, Kim JW, Choi MM, Kim YM, Lee MJ, Kim JY.
- Writing - review & editing: Jang YR, Kim JY.
SUPPLEMENTARY MATERIAL
The real-time and conventional PCR results with DNAs extracted from different types of clinical specimens of the monkeypox patient
References
- 1.European Centre for Disease Prevention and Control. Monkeypox cases reported in UK and Portugal. [Accessed June 28, 2022]. https://www.ecdc.europa.eu/en/news-events/monkeypox-cases-reported-uk-and-portugal .
- 2.World Health Organization. Monkeypox. [Accessed June 28, 2022]. https://www.who.int/news-room/fact-sheets/detail/monkeypox .
- 3.Center for Disease Control and Prevention. U.S. monkeypox outbreak 2022. [Accessed June 28, 2022]. https://www.cdc.gov/poxvirus/monkeypox/response/2022/index.html .
- 4.UK Health Security Agency. Monkeypox cases confirmed in England. [Accessed June 28, 2022]. https://www.gov.uk/government/news/monkeypox-cases-confirmed-in-england-latest-updates .
- 5.Minhaj FS, Ogale YP, Whitehill F, Schultz J, Foote M, Davidson W, et al. Monkeypox outbreak - nine states, May 2022. MMWR Morb Mortal Wkly Rep. 2022;71(23):764–769. doi: 10.15585/mmwr.mm7123e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vivancos R, Anderson C, Blomquist P, Balasegaram S, Bell A, Bishop L, et al. Community transmission of monkeypox in the United Kingdom, April to May 2022. Euro Surveill. 2022;27(22):2200422. doi: 10.2807/1560-7917.ES.2022.27.22.2200422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hübschen JM, Gouandjika-Vasilache I, Dina J. Measles. Lancet. 2022;399(10325):678–690. doi: 10.1016/S0140-6736(21)02004-3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The real-time and conventional PCR results with DNAs extracted from different types of clinical specimens of the monkeypox patient