

Introduction:
Although single institution studies have analyzed various animal attacks, there has not been multicenter investigation into dog bites in children. The purpose of this study was to characterize national trends and investigate the characteristics of pediatric dog bites.
Methods:
Aretrospective cohort study was conducted of pediatric dog bite injuries in the United States from 2015 to 2020 using the Pediatric Health Information System national database. Patient characteristics, injury locations, and need for intervention were analyzed. Mann–Whitney U test, Pearson chi-square, and Fisher exact test, and linear multivariate regressions were performed for statistical analysis of data values; statistical significance was maintained at P < 0.05.
Results:
A total of 56,106 patients were included, majority male (55.1%) with a median age 6.8 years (interquartile range 3.5–10.6). Incidence peaked in July (median =1217) with nadirs in February (median = 760). A substantial increase in bites was seen per overall Emergency Department presentations during the pandemic. Most common bite location was the head (62.1%), followed by the upper extremity (25.1%). Relative proportions of dog bites to the face gradually decreased with age (B = –3.4%/year, P< 0.001), whereas proportions to the upper extremities (B = + 1.9%/year, P < 0.001) and lower extremities (B = + 1.6%/year, P = 0.002) gradually increased with age. Overall, 8.0% patients required repair in the operating suite. injuries isolated to the head (OR= 2.6, P< 0.001) and those to multiple anatomic regions were more likely to require operative intervention [operating room (OR= 2.6, P< 0.001)].
Conclusions:
Dog bites most commonly occur during the summer in school-aged boys. Toddlers disproportionately suffer injuries to the head, with a trend towards upper extremity bites in teenagers. The coronavirus disease 2019 pandemic ushered a spike in dog bite presentations among Emergency Department visits, further underscoring the need for targeted educational initiatives to halt the persistence of these preventable injuries.
Key Words: Animal bite, COVID-19 pandemic, dog bite, facial trauma, pediatric trauma
An estimated 3.9 million people suffer a dog bite in the United States (US) annually, with nearly 850,000 seeking some degree of medical care. 1,2 Rates of dog-bite related Emergency Department (ED) visits are highest among pediatric patients, representing 158 per 100,000 visits, with a projected annual medical cost of $252 million. 3 Perhaps more detrimental than the cost burden of these preventable injuries is the psychologically traumatic and physically scarring sequalae suffered by the child and their family.
Previous reports have elucidated the epidemiology of dog bite injuries, some of which may be targets for preventative efforts. For example, a disproportionate vulnerability exists for younger boys, those familiar with the attacking canine, and those with an increasing number of dogs in their household. 4–8 Specific dog breeds have been implicated with higher risk, particularly Pitbulls and other mixed breeds. 9,10 Recently it has been suggested that societal shutdowns in the wake of the coronavirus disease 2019 (COVID-19) pandemic have inadvertently precipitated a rise in incidence of dog-bites among pediatric ED visits. 1 As we contend with the unanticipated ramifications of these government directives and their precarious duration, it may be helpful to learn more about their underpinnings.
To date, dog bite data has been predominantly limited to single institution or regional experience alone.12,13 Several reports have drawn from national inpatient samples, 14,15 but as the majority of these injuries are treated in the ED setting, a global perspective on all presenting occurrences at a national scale is lacking. The aim of the present study is to utilize a multicenter dataset of pediatric dog bite injuries in the US, and to elucidate national trends that occurred during the COVID-19 pandemic.
Methods
A retrospective cohort study was conducted of all dog bite injuries presenting to pediatric hospitals in the US from September 2015 to September 2020 using the Pediatric Health Information System. Pediatric Health Information System is an administrative database that contains encounter-level data from over 50 nonprofit tertiary care pediatric hospitals in all representative regions of the US. Data quality and reliability are assured through a joint effort between the Children’s Hospital Association and participating hospitals. Participating hospitals provide encounter data including demographics, diagnoses, procedures, and imaging. Access to the Pediatric Health Information System database is restricted only to participating hospitals. Data are deidentified at the time of data submission. Internal Review Board approval was not required because this dataset only contained deidentified information.
All patients under 18 years of age who presented with a dog bite to the hospital setting. Dog bites were defined as patients having hospital visitations associated with Internal Classification of Diseases (ICD-9 or ICD-10) diagnosis codes including E906.0, W54.0, or W54.0XXA. This is inclusive of all patients presenting to the ED as well as those admitted to an inpatient stay. Demographic information such as patient age, gender, race/ethnicity, geographic location, insurance coverage and median household income was collected. Median household income was based on the zip code of each patient’s home address. Urban was defined as cities or surrounding suburbs. Date of injury and anatomic location affected were also extracted from the database. Radiographic data was searched for any concomitant fractures suffered as a result of a dog attack. Operative procedure was a designation assigned to patients who had an “operating room” charge and excluded any bedside procedures.
Mann-Whitney U test and Kruskal-Wallis test were used to compare continuous nonparametric variables between independent groups. Pearson chi-square test and Fisher exact test were used to compare categorical variables. Haldane-Anscombe correction was applied as indicated when calculating odds ratios. Linear multivari-ate regressions were represented by the beta coefficient of each variable. Binary multivariate regressions were represented by the adjusted odds ratio of each variable. Central tendency was reported using median and its corresponding confidence interval. P values were all 2-tailed, and significance was set at the α < 0.05 level. Statistical analysis was conducted on is a statistical software v27 (IBM Corporation; Armonk, NY), Prism v9 (GraphPad; San Diego, CA), and Tableau v2020.4 (NorthEdge; Seattle, WA).
Results
A total of 56,106 pediatric patients who incurred dog bite injuries were treated at participating hospitals. Annual incidence of presentation significantly increased (P = 0.032) with approximately 82 new cases per year. During the 5-year study period, these injuries represented 0.33% ED visits at included hospitals. In April 2020, following national COVID-19 shelter-in-place mandates, a slight decrease in pediatric dog bites was observed (total 883) compared to presentations in April of preceding years [median 1029, interquartile range (IQR) 903 –1073]. However, in May through September, the absolute number of dog bites was slightly increased compared to corresponding months of prior years. Yet, the rates of injury nearly tripled as a proportion of ED visits, encompassing 0.8% of presenting patients in the ED (Fig. 1). Incidence of presentation followed a cyclical pattern that strongly correlated with seasonal change, with the highest frequency of injury occurring in the summer months and peaks in July (median 1031 patients, IQR 992 – 1149), and declining in the winter reaching lowest points in February (median 704 patients, IQR 483–829).
Figure 1.
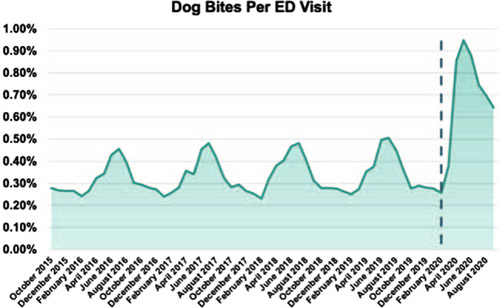
Dog bite injuries as a percentage of all pediatric Emergency Department visits in participating hospitals. Dashed line represents March 2020, indicating the beginnings of the COVID-19 pandemic and initiation of stay-at-home orders in the US. COVID-19, coronavirus disease 2019;US, United States.
Median patient age was 6.8 years (IQR 3.5–10.6) with a slight male dominance (55%), and most frequently identifying within the White/Non-Hispanic race (Supplementary Digital Content, Table 1, http://links.lww.com/SCS/E39). No differences in age or gender were observed over time. Incidence of injury consistently declined with patient age, with infants 0 to 3 years old comprising 28% ofthe cohort. White/Non-Hispanic patients were more susceptible to injury during the pandemic (49% from March to September 2020) compared to other races. Median household income of children’s families was $43,386 (IQR 34,080-56,408), with a small but statistically significant increase seen during the pandemic (P < 0.001, median $42,621 IQR 33,605-55,321 from March to September 2020). The majority of visits were covered by governmental insurance (51%), with a smaller portion paid for by private insurance (38%), self-pay (6%) or other payors (4%). The overwhelming majority of dog bites took place in urban areas (93%). Injuries occurred predominantly in the South (41%), followed by the Midwest (26%), the West (24%), and least commonly the Northeast (9%) areas of the US. The Northeast had the lowest per-capita incidence with 4 per 10,000 children, whereas the Midwest, West, and South had 9, 8, and 8 per 10,000, respectively. Less seasonal variance in dog bite presentations occurred in the South, and compared to the spring/summer a greater percentage of dog bites in the winter months were treated in the South, weighing in regional population density (Fig. 2).
Figure 2.
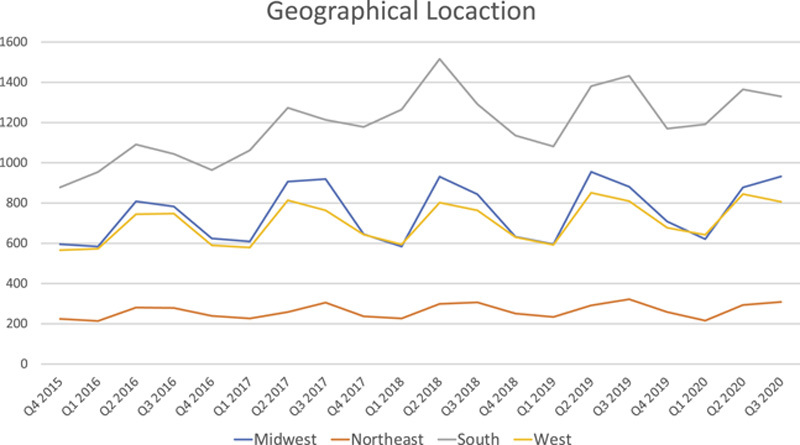
Distribution of dog bites by geographical location.
The most common anatomic location for dog bite injuries overall was the head/face (62.1%, n = 34,835), followed by the upper extremity (25.1%, n = 14,086). Almost half of patients presented with bites to multiple anatomic regions (45%, n= 25,400), with the head and neck are a still being mostcommon(Supplementary Digital Content, Table 2, http://links.lww.com/SCS/E40). The majority of toddlers had facial injuries (age <3 years: 82.5%, n = 9584), whereas the majority of teenagers had upper extremity injuries (age 13 years + : 40.9%, n — 2958). The relative proportions of dog bites to the face gradually decreased with age (P < 0.001, B = –3.4% per year), whereas relative proportions of dog bites to the upper extremities (P < 0.001, B = + 1.9% per year) and lower extremities (P = 0.002, B = + 1.6% per year) gradually increased as patients became older (Fig. 3). Fractures were diagnosed in 1744 (2.9%) patients, with 51% in the head and neck region, 40% in the upper extremity, 5% in the lower extremity, and 3% in the trunk.
Figure 3.
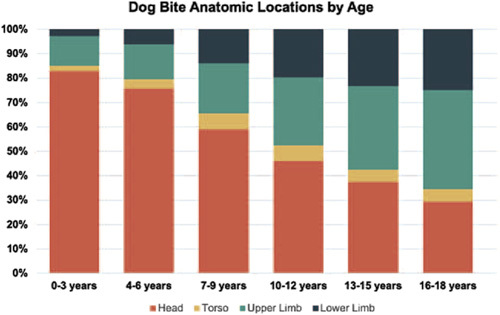
Anatomic location of dog bite by patient age.
Overall, 8.0% (n = 4515) patients required operative intervention. Dog bites to various portions of the body had different risk of requiring surgery, as defined by need for repair in the operating room. Injuries isolated to the head [P< 0.001, OR= 2.6, 95% confidence interval (CI) 2.4–2.9] were significantly more likely to require operative intervention (Fig. 4), whereas isolated injuries to the torso (P< 0.001, OR = 0.5, 95%CI 0.4–0.6), upper extremity (P < 0.001, OR = 0.4, 95%CI 0.4–0.5), and lower extremity (P < 0.001, OR = 0.3, 95%CI 0.3–0.5) were significantly less likely to require operative intervention. Patients with dog bites to multiple anatomic regions were more likely to require operative intervention (P < 0.001, OR = 2.6, 95%CI 2.4–2.8).
Figure 4.
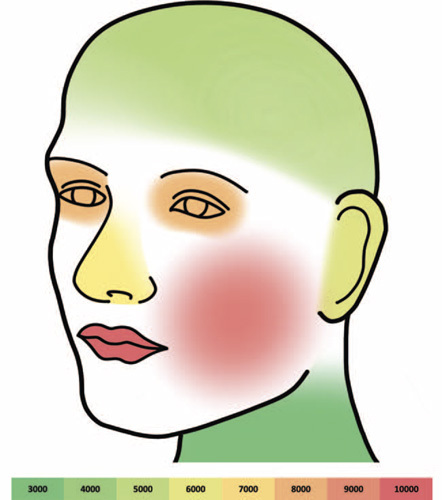
Heat map of anatomic locations in the head and neck region most frequently injured by dog bites.
Discussion
The present study represents the largest cohort of pediatric dog bites extracted from a heterogeneous database representing over 50 pediatric hospitals nationwide. The data indicates that dog bite injuries in children remain a pervasive public health concern in the US, with a steady increase in the rate of dog bite injuries overt he past 5 years and a surge among ED visits during the COVID-19 pandemic. Young boys are particularly vulnerable to dog bites to the head and face, whereas older children tend to be bitten in the upper extremity. Most dog bites are treated at the bedside, with only 8% requiring operative intervention and only 2.9% having an associated fracture. The following paragraphs detail opportunities for education given our data.
Interestingly, there has been a spike in absolute number of pediatric dog bites during the COVID-19 pandemic, the reasons for which are not known but are likely to be associated with stay-at-home orders, bringing dogs and children together for longer periods of time and perhaps in closer quarters. It is alarming to note that the spike in incidence of dog bites has peaked, yet persisted, even as states continue to slowly relax social restrictions. Several explanations of this phenomena can be explored, beginning with the simple fact that urgent/emergent care utilization significantly declined due to the imminent fear of contracting coronavirus in the hospital setting such that dog bites formed a larger percentage of the whole. 16 20 Conceivably, children’s hospitals in particular may have absorbed a higher referral of dog bites from urgent care or adult EDs that were otherwise overwhelmed, during the initial pandemic months. Even yet, the persistence in presentations throughout the summer and fall months suggests a larger phenomenon beyond just a shift in access to healthcare venues. Neither children nor domesticated dogs were accustomed to the uninterrupted co-habitation in close quarters. The compounding stress on caregivers from converting to a virtual workplace, limited social outlets, and economic uncertainty may have left little reserve for the nonstop child supervision demanded of them. Kids themselves were also stripped of their own activities and sought ways to remain engaged while at home, which may inadvertently incite more provoking interactions with otherwise docile pets. Lastly, as data in the US mounted that canines were not potential transmitters of COVID-19 to humans, parents and children were not shielded against playing with dogs outside their household.
Many families embraced their homebound lifestyles by purchasing a dog. In 2020, adoption rates from animal shelters increased by 30% to 40% compared to the preceding year, leaving shelters struggling to even meet the unprecedented demand that remains ongoing. 16 Purebred dogs are seeing an even greater rate of adoption in this past year. 17 Media attention has been drawn to the emotional benefits of newfound companionship to distract from social isolation and the valuable opportunity to provide children with a developed sense of responsibility. But as the “pandemic puppy” grows olderina normalizing world, they will soon lose their attention filled routine and plentiful walks that afforded their owners an opportunity to escape their isolated states. 18,19 Tensions might rise and it can be unpredictable how most of these dogs will react, especially previously abandoned dogs who may inherently be more volatile and ill-equipped to adapt to change. As the over 48 millionU.S. households 20 with a dog slowly return to “normalcy,” educational efforts are needed for the creation of a reasonable post-pandemic routine and vigilance in supervising child-dog interactions.
Onset of the pandemic did not alter the inflictive patterns of dog bites on child age, race, or geographic location; however, the median household income of patient families presenting to the hospital with pediatric dog bites was higher after the onset of social shutdowns. Our findings on dog bite patterns before the pandemic align with previous reports of children from lower-income homes with government-funded insurance more typically falling victims to accidental trauma, such as dog bites. There was, however, a small but statistically significant increase in median household income for dog bites once COVID-19 hit. One hypothesis is that those households in which income earners were able to retain their jobs and financially save from disengaging in social activities were fiscally able to adopt a dog. Perhaps they were also burdened by the 24-hour childcare responsibilities, whereas simultaneously meeting their work demands, lending less availability for supervision. This is an important consideration given that work-from-home practices are likely here to stay in the post-pandemic world. A competing hypothesis that may be more of a concern is if socioeconomically disadvantaged families grew increasingly reluctant to seek medical care during the pandemic, leading to children of low-income families not receiving appropriate medical care. Further education in communities can target awareness for parents and emphasize the importance of prompt evaluation.
Over the entirety of the study period, there was a significant association between child age and anatomic location of injury. A predominance in head/neck wounds was seen for children under the age of 9, when infants, toddlers, and elementary school kids remain in close proximity to the ground and the animal. Young children are curious, unintentionally provoking, and less astute at identifying behavioral cues from the dog indicating aggression. An increase in upper extremity wounds was seen as children grew older, with an inverse relationship to injuries overall. Based on large cohort reports from the late 1990s to early 2000s, the 5 to 9 age range has been regarded as the highest risk 4,6,9 ; however, our findings corroborate more recent, albeit smaller series, indicating that children 0 to 3 years old fall victim to dog-bites more frequently. 12,21 Almost half of included patients suffered bites to multiple body regions, which correlated with greater severity and had a significant association with need for operative repair. Patient age was not predictive of multi-site injuries, though the head and neck area remained the most commonly involved. It is also important to distinguish data sources from ED visits to those analyzing inpatient-only cohorts, as demographic specifics may be contrasting. 14,15,22 One study from a national trauma database described a bimodal age distribution for children suffering dog bites, with increases seen in the 0 to 2 and 6 to 12-year-olds, 23 suggesting that young adolescents may present to adult EDs and were not as readily captured in the pediatric hospital database referenced here.
Seasonal fluctuation in dog bite injuries has been established, with plentiful reports on increased trauma rates during times of warmer weather. 4 Dog bite incidence peaks in July seem most obvious as children are out of school and interfacing more frequently with dogs at home. Contrasting nadirs in February suggest that being sheltered indoors with pets is not in and of itself a great danger for dog attacks. Although geographical incidence of dog bites is evenly distributed across the US by regional population density, the South experienced the greatest number of bites overall and fewer variations between the summer and winter months, where a more consistent outdoor climate is maintained. This stands in contrast to reports of dog bites to majority adult patients who primarily reside in the Northeast, which is the region of fewest per-capita bites in children. Understanding this can help navigate educational directives with a greater concentration in the South given overall higher incidence. The climate factor does raise the question of whether degree of familiarity between the child, the dog, and the supervisor plays a role in likelihood of biting. If fewer injuries occur during cold months when children and dogs of the same household are mutually sheltered, then the rise of bites in the summertime can be subsequent to children playing with known, yet less familiar pets outdoors. Caregivers might underestimate the true risk their neighbor’s dog may pose leading to a false sense of security, another area of educational opportunity.
Coinciding with existing literature, fractures in this database were identified in 2.9% of patients, the majority of which occurred in the craniofacial skeleton. 25,26 Our reported cohort found most fractures located in the midface, which is in contrast to other reports discussing skull, nasal bone, or orbital fractures, though many patients did present with fractures to multiple locations. With an aggressive enough clench and penetrating teeth, the thin cranial and facial bones can easily shatter when juxtaposed by the strong force of a canine’s mandible. Presumably fractures can also be sequelae of a secondary fall after the initial bite and follow age-specific trends, where we can imagine younger children who are already crawling may fall on their head or face and older children may catch a fall with an outstretched hand. Yet much of this is difficult to elucidate given the number of attacks that go unwitnessed. Regardless of specific fracture patterns, diagnosing them are uniquely challenging in the pediatric population as symptomatology in kids are hard to discern and avoidance of unnecessary radiation is always a consideration. Severe presentations of dog bite wounds should always raise a high level of suspicion and prompt diagnostic imaging to avoid missing fractures. Further investigation to more accurately identify predictive factors of fractures should be carried out to better guide clinicians on narrow indications for obtaining computerized tomography imaging.
The nature of this retrospective, observational study poses several limitations to be considered, predominantly that reliance on a large administrative database through diagnostic coding searches may be exclusive of miscoded patients and injuries that do not present to the hospital setting. Extracting from a variety of hospital systems made it unfeasible to standardize variables such as severity of injury, type of soft tissue repair, anesthetic preferences, primary physician specialty, and antibiotic prescribing practices, all of which should be more closely studied. Missing variables such as dog breed, stray or housed dog, or patient-dog familiarity were unable to be ascertained. Exclusively investigating pediatric treatment settings could also present a risk of inclusion bias towards more severe injuries that were beyond the scope of management by adult-practice providers. Nevertheless, this study presents the largest nationally representative data source on pediatric dog bites presenting for acute care. No other reports have discussed the longitudinal implications of COVID-19 on dog bite injuries to our knowledge. This stands as a profound body of evidence that profiles dog bite injuries, which can guide future prevention efforts.
Supplementary Material
Footnotes
The authors report no conflicts of interest.
Supplemental digital contents are available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.jcraniofacialsurgery.com).
References
- 1.Holmquist LEA. Healthcare Cost and Utilization Project, Emergency Department Visits and Inpatient Stays Involving Dog Bites, 2008, November 2010 [PubMed]
- 2.Center for Disease Control and Prevention (CDC). National Center for Injury Prevention and Control Data & Statistics (WIQARS): Non-Fatal Injury Reports, 2000–2019. 2019
- 3.Center for Disease Control Data & Statistics: Cost of Injury Reports.
- 4.Weiss HB Friedman DI Coben JH. Incidence of dog bite injuries treated in emergency departments. JAMA 1998;279:51–53 [DOI] [PubMed] [Google Scholar]
- 5.Jakeman M Oxley JA Owczarczak-Garstecka SC et al. Pet dog bites in children: management and prevention. BMJ Paediatr Open 2020;4:e000726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gilchrist J Sacks JJ White D et al. Dog bites: still a problem? Inj Prev 2008;14:296–301 [DOI] [PubMed] [Google Scholar]
- 7.Ramgopal S Brungo LB Bykowski MR et al. Dog bites in a U.S. county: age, body part and breed in paediatric dog bites. Acta Paediatr 2018;107:893–899 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Avner JR Baker MD. Dog bites in urban children. Pediatrics 1991;88:55–57 [PubMed] [Google Scholar]
- 9.Kaye AE Belz JM Kirschner RE. Pediatric dog bite injuries: a 5-year review of the experience at the Children s Hospital of Philadelphia. Plast Reconstr Surg 2009;124:551–558 [DOI] [PubMed] [Google Scholar]
- 10.O’Brien DC Andre TB Robinson AD et al. Dog bites of the head and neck: an evaluation of a common pediatric trauma and associated treatment. Am J Otolaryngol 2015;36:32–38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dixon CA Mistry RD. Dog bites in children surge during coronavirus disease-2019: a case for enhanced prevention. J Pediatr 2020;225:231–232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Golinko MS Arslanian B Williams JK. Characteristics of 1616 consecutive dog bite injuries at a single institution. Clin Pediatr (Phila) 2017;56:316–325 [DOI] [PubMed] [Google Scholar]
- 13.Alizadeh K Shayesteh A Xu ML. An algorithmic approach to operative management of complex pediatric dog bites: 3-year review of a level I regional referral pediatric trauma hospital. Plast Reconstr Surg Glob Open 2017;5:e1431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McLoughlin RJ Cournoyer L Hirsh MP et al. Hospitalizations for pediatric dog bite injuries in the United States. J Pediatr Surg 2020;55:1228–1233 [DOI] [PubMed] [Google Scholar]
- 15.Cook JA Sasor SE Soleimani T et al. An epidemiological analysis of pediatric dog bite injuries over a decade. J Surg Res 2020;246:231–235 [DOI] [PubMed] [Google Scholar]
- 16.Shelter Animals Count, The National Database. COVID 19-Impact Report: November 2020
- 17.Cooper C. Supply and Demand. In: As devastating as it has been for humans Chbgnfpd, Ed. January 21, 2021, Dog News
- 18.Oliva JL Johnston KL. Puppy love in the time of corona: dog ownership protects against loneliness for those living alone during the COVID-19 lockdown. Int J Soc Psychiatry 2020;67:232–242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Klass P. Got a Pandemic Puppy? Learn How to Prevent Dog Bites. The New York Times; 2021
- 20.U.S. Pet Ownership & Demographics Sourcebook 2017–2018. American Veterinary Medical Association
- 21.Chen HH Neumeier AT Davies BW et al. Analysis of pediatric facial dog bites. Craniomaxillofac Trauma Reconstr 2013;6:225–232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bernardo LM Gardner MJ Rosenfield RL et al. A comparison of dog bite injuries in younger and older children treated in a pediatric emergency department. Pediatr Emerg Care 2002;18:247–249 [DOI] [PubMed] [Google Scholar]
- 23.Fein J Bogumil D Upperman JS et al. Pediatric dog bites: a population-based profile. Inj Prev 2019;25:290–294 [DOI] [PubMed] [Google Scholar]
- 24.Rabbani CC Kao R Shin TJ et al. The association of weather, temperature, and holidays on pediatric maxillofacial trauma. Laryngoscope Investig Otolaryngol 2020;5:846–852 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Saadi R Oberman BS Lighthall JG. Dog-bite-related craniofacial fractures among pediatric patients: a case series and review of literature. Craniomaxillofac Trauma Reconstr 2018;11:249–255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wei LA Chen HH Hink EM et al. Pediatric facial fractures from dog bites. Ophthalmic Plast Reconstr Surg 2013;29:179–182 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.