

Abstract
The present article examines how disease anthropomorphism affects compliance with recommendations for preventing the disease. We find that consumers are more likely to comply with health recommendations when the disease is described in anthropomorphic (vs. non-anthropomorphic) terms because anthropomorphism increases psychological closeness to the disease, which increases perceived vulnerability. We demonstrate the effect of disease anthropomorphism on health compliance in seven studies with several diseases (COVID-19, breast cancer), manipulations of anthropomorphism (first person and third person; with and without an image), and participant populations (the US and China). We test the proposed pathway through psychological closeness and perceived vulnerability with sequential mediation analyses and moderation-of-process approaches, and we rule out alternative accounts based on known consequences of anthropomorphism and antecedents of health compliance. This research contributes to the theory and practice of health communication and to the growing literature on how the anthropomorphism of negative entities affects consumers’ judgments and behaviors.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11747-022-00891-6.
Keywords: Disease anthropomorphism, Psychological distance, Perceived vulnerability, Health compliance, Health communication
Introduction
Anthropomorphism is the attribution of human characteristics, motivations, intentions, and behaviors to nonhuman entities such as animals, objects, and abstract concepts (Aggarwal & McGill, 2007; Epley et al., 2007; Guthrie, 1993). In marketing communications, anthropomorphism may influence persuasion and compliance in positive ways (Ahn et al., 2014; Tam et al., 2013; Zhou et al., 2019) and in negative ways (Hur et al., 2015; Puzakova & Aggarwal, 2018). The net effect depends on the context, the type of object, and consumers’ personal characteristics (Aggarwal & McGill, 2012; Touré-Tillery & McGill, 2015).
Anthropomorphizing diseases is a common practice in health communications.1 For example, a popular Chinese medical social media account describes the coronavirus (COVID-19) as a dangerous criminal who can take many disguises to avoid detection. In the US, televised commercials for the cough suppressant and expectorant Mucinex portray mucus as a green, obnoxious, humanlike invader of the nasal and chest cavities; Mucinex is depicted as an effective way to get rid of this unwelcome “guest.” A popular Japanese anime, “Cells at Work!” (based on a manga by the same name), anthropomorphizes cells and diseases such as influenza and pneumococcus to show how they operate within the human body. The popularity of disease anthropomorphism begs the question: How does thinking about a disease in anthropomorphic terms—rather than in non-anthropomorphic terms—influence consumers’ likelihood of complying with medical and public health recommendations for disease protection?
This question is important because, according to a recent report from the World Health Organization (2020), the top three global causes of death and disability are from preventable diseases (ischemic heart disease, stroke, and chronic obstructive pulmonary disease), and many more deaths are caused by detectable and treatable diseases (e.g., some cancers). Almost 50% of cancer diagnoses occur relatively late, which makes treatment less likely to succeed and reduces the patient’s chance of survival. The problem is not necessarily a lack of awareness or access to care but rather a lack of compliance with well-established health recommendations. For example, more than three million people die each year from vaccine-preventable diseases such as tuberculosis, polio, diphtheria, tetanus, pertussis, measles, and hepatitis B; many people still lack access to vaccines, but a substantial number of vaccine-preventable deaths are due to failures to comply with public health recommendations. Similarly, most people in the US are aware that lifestyle changes are critical determinants of their health and longevity, yet 79% of US adults do not meet recommendations for aerobic and muscle-strengthening physical activity (Hellmich, 2013), and about 90% consume too much sodium (Paddock, 2016), which can increase the risk of high blood pressure. Furthermore, every year, efforts to vaccinate at least 70% of the US population against influenza fall short of this target (Centers for Disease Control and Prevention 2020).
The present article explores the link between disease anthropomorphism and health compliance, defined broadly as taking steps to protect oneself from the disease (e.g., vaccination) or to detect the disease early (e.g., cancer screening), as recommended in health communications from public health organizations or medical professionals (see also Brouwers & Sorrentino, 1993; Hovland et al., 1953; Wilson et al., 1988). We predict that communications that present a disease in anthropomorphic (vs. non-anthropomorphic) terms will increase consumers’ compliance. Our rationale for this prediction is that anthropomorphism increases the psychological closeness between the consumer and the disease by taking a nonhuman entity, which otherwise is psychologically distant (Liberman et al., 2007a; Maglio, 2020), and bringing it into a cognitive realm that is more connected with the person’s subjective experience of reality as a human. Greater psychological closeness to an anthropomorphized (vs. non-anthropomorphized) disease, in turn, makes the consumer feel more vulnerable to the disease. Indeed, previous research shows a positive relationship between dimensions of psychological closeness to a disease and perceived vulnerability to the disease (Murdock & Rajagopal, 2017). Finally, greater perceived vulnerability to an anthropomorphized (vs. non-anthropomorphized) disease motivates compliance because when people feel more vulnerable to a disease, they are typically more likely to comply with health recommendations to protect themselves from the disease (Maddux & Rogers, 1983; Rogers, 1975).
Our investigation contributes to the rich literature on anthropomorphism (Aggarwal & McGill, 2007; Puzakova et al., 2013b; Wan et al., 2017) and to the theory and practice of health communication (Berger & Rand, 2008; Han et al., 2016; Yan & Sengupta, 2013). From a theoretical standpoint, first, we contribute to an understanding of the cognitive processes that are triggered by anthropomorphism (Epley et al., 2007) by showing that anthropomorphism increases one’s psychological closeness with the nonhuman entity. Second, our work identifies a positive consequence of the anthropomorphism of negative attitude objects, while most previous research on the anthropomorphism of such objects has found detrimental effects (Hur et al., 2015; Puzakova et al., 2013a; Wan et al., 2022). Third, we extend research on the role of psychological distance in health behavior (Chandran & Menon, 2004; Menon et al., 2002; Murdock & Rajagopal, 2017) by identifying disease anthropomorphism as a novel antecedent to psychological closeness. From a practical standpoint, our findings indicate that anthropomorphizing diseases in health communications may be an effective strategy for promoting disease prevention and detection among people without a known diagnosis of the disease.
Conceptual development
Anthropomorphism increases psychological closeness
Decades of research show that people respond to anthropomorphized entities in ways that mirror their responses to comparable persons (Aggarwal & McGill, 2007; Epley et al., 2007; Guthrie, 1993; Tam et al., 2013; Wan et al., 2017). For example, Aggarwal & McGill (2007) find that participants evaluate an anthropomorphized car acting as a spokesperson more positively when the car appears to be smiling (upturned grill) than when it appears to be frowning (downturned grill) because the former feature is more congruent with the human schema of a spokesperson. Kim & McGill (2011) show that participants high in social power feel a stronger sense of control over anthropomorphized (vs. non-anthropomorphized) risk-bearing entities such as slot machines and skin cancer, and they deem such entities less serious, less life-threatening, and less risky. The effects reverse for participants low in power. The results suggest that assessments of anthropomorphized threats (e.g., skin cancers described as criminals) mirror assessments of comparable social threats (e.g., human criminals).
The tendency to treat anthropomorphized entities as social beings has many consequences. For one, people perceive the actions of anthropomorphized entities as intentional (De Visser et al., 2016; Puzakova et al., 2013a) and potentially disruptive to their own actions and goals (Hur et al., 2015; Kim, Chen, et al., 2016; Kim, Sherman, et al., 2016; Puzakova & Aggarwal, 2018). For example, Kwak et al. (2015) show that brand anthropomorphism heightens the perceived unfairness of price increases and the perceived fairness of price decreases because the actions seem calculated and intentional when coming from an anthropomorphized brand. For another, people feel more moral responsibility, interpersonal connectedness, and empathy toward anthropomorphized (vs. non-anthropomorphized) entities, such that people are more motivated to protect and care for such entities (Ahn et al., 2014; Kim & Yoon, 2021; Koo et al., 2019; Tam et al., 2013; Wang et al., 2022). For example, Chandler & Schwarz (2010) find that participants with a greater tendency to anthropomorphize their car are less willing to replace it; Tam et al. (2013) find that anthropomorphizing nature fosters conservation behavior. Zhu et al. (2019) find that this last effect is even more pronounced when people anthropomorphize an environmental object as someone close to them.
Most effects of anthropomorphism on judgments and behaviors can be explained in terms of the cognitive processes underlying anthropomorphism. Epley et al. (2007) theorized that anthropomorphism is a form of inductive inference about nonhuman agents. In inductive inference, people acquire knowledge, activate stored knowledge, and apply the activated knowledge to a given target (Higgins, 1996). When anthropomorphizing, people activate stored knowledge about humans in general (and themselves in particular) and apply the knowledge to nonhuman entities. The process is consistent with analogical or metaphorical reasoning, whereby people routinely understand and experience one thing in terms of another (Fauconnier & Turner, 2008; Lakoff & Johnson, 1980; Williams & Bargh, 2008). Thus, anthropomorphism is pervasive because people find it easier, more natural, and more automatic to reason about nonhuman entities if they use their own (human) mental states and characteristics as a reference. People have immediate access to the phenomenological experience of being human but not of being a nonhuman entity. Due to the physical constraints inherent to the human sensory apparatus, a person cannot directly experience being a germ, sloth, or any other nonhuman entity (Nagel, 1974).
In sum, anthropomorphism takes a nonhuman entity, which otherwise is psychologically distant (Liberman et al., 2007a; Maglio, 2020), and brings it into a cognitive realm that is more connected with the subjective experience of reality as a human. Thus, we propose that anthropomorphizing a nonhuman entity reduces the psychological distance—i.e., increases the psychological closeness—between the self and the nonhuman entity. Psychological distance is the degree to which an object or event is cognitively separated or removed from oneself, that is, not present in one’s direct, subjective experience of reality. Objects or events may be removed from one’s immediate reality if they occur at a different time (temporal distance), in a different place (spatial distance), to a different person (social distance), or if they are not real (hypotheticality). According to construal level theory (Trope & Liberman, 2010; Trope et al., 2007), psychologically-distant objects are construed more abstractly and at a higher level, whereas psychologically-close objects are construed more concretely and at a lower level. This proposition is consistent with the notion that psychologically-distant objects are more cognitively removed from one’s phenomenological experience, whereas psychologically-close objects are more cognitively connected to one’s phenomenological experience.
Psychological closeness increases perceived vulnerability
For positive entities such as nature or one’s car, the greater psychological closeness elicited by anthropomorphism strengthens one’s affiliation and connectedness with the nonhuman entity (see Heider, 1958; Chandler & Schwarz, 2010; Tam et al., 2013). For negative entities, however, we propose that the increased psychological closeness increases one’s sense of being vulnerable to the nonhuman entity.
Research has established a positive relationship between psychological closeness to a disease and perceived vulnerability to the disease (Murdock & Rajagopal, 2017). Chandran & Menon (2004) test two types of disease framing: “every day” framing and “every year” framing (e.g., “every day/year, a significant number of people fall prey to mononucleosis”). The authors find that “every day” framing (relative to “every year” framing) increases perceived vulnerability to the disease because it decreases the temporal distance between the self and the disease. Similarly, Menon et al. (2002) find that a participant’s perceived vulnerability to a disease is related to the degree to which the participant perceives the possibility of contracting the disease as real/probable rather than hypothetical/improbable. Participants who read that hepatitis C is “often contracted by leaving a cut un-bandaged” (a more frequent and hence more real occurrence for most participants in the study) felt more vulnerable to the disease than those who read that hepatitis C is “often contracted simply by getting a tattoo” (a less frequent and hence more hypothetical occurrence for participants in the study).
In sum, feeling psychologically close to (vs. distant from) a disease or its causes (e.g., germs) increases perceived vulnerability to the disease. If, as we propose, consumers feel psychologically closer to an anthropomorphized (vs. non-anthropomorphized) disease, it follows that consumers will feel more vulnerable to an anthropomorphized (vs. non-anthropomorphized) disease, which we argue will have consequences for health compliance.
Perceived vulnerability increases health compliance
The perception of invulnerability is a critical obstacle to health compliance, which we define as taking steps to protect oneself from the disease (e.g., COVID-19 vaccination) or to detect the disease early (e.g., cancer screening), as recommended in health communications from public health organizations or medical professionals (Brouwers & Sorrentino, 1993; Hovland et al., 1953; Wilson et al., 1988). People tend to be unrealistically optimistic about their own susceptibility to harm and often believe they are less at risk of contracting a disease than their peers (i.e., self-positivity bias; Folkes & Kiesler, 1991; Menon et al., 2002; Pechmann et al., 2003). For example, a study of visitors of a mobile skin-cancer screening unit in Sweden found that people were aware that sun exposure is an important risk factor but underestimated their own vulnerability to skin cancer (Bränström et al., 2006). Thus, people may not initiate preventive behaviors until an intervention reduces or eliminates self-positivity bias (Block & Keller, 1998; Mann, 1967; Menon et al., 2002). For example, Raghubir & Menon (1998) found that participants’ perceived risk of contracting HIV increased when an intervention made the causes of HIV more accessible in participants’ memories. Then, the increase in perceived vulnerability increased participants’ intentions to engage in precautionary behaviors (e.g., getting tested for HIV, using condoms). Similarly, Lisjak & Lee (2014) found that participants who were depleted by a previous self-regulatory task felt more vulnerable to danger and hence were more willing to engage in preventive behaviors (e.g., avoiding unprotected sex, getting tested for kidney disease) relative to non-depleted participants. In sum, when people feel more vulnerable to a disease, they are more likely to comply with health recommendations to protect themselves from the disease (Maddux & Rogers, 1983; Rogers, 1975).
Synthesis and hypotheses
In the previous sections, we presented three causal relationships: First, anthropomorphizing a disease (vs. not; A) causes an increase in psychological closeness to the disease (B), which causes an increase in perceived vulnerability to the disease (C), which causes an increase in health compliance (D). Through causal transitive reasoning (see Egenhofer, 1994; Wolff & Barbey, 2015), we propose a new causal relationship by forming links between the non-adjacent elements of this causal chain. Specifically, given our propositions that A causes B, B causes C, and C causes D, and that these causal relationships are similar (i.e., positive effects), we infer that A causes D (also a positive effect)—that is, anthropomorphizing a disease (vs. not) causes an increase in health compliance. Our first hypothesis is as follows:
H1 Consumers are more likely to comply with health recommendations for preventing or detecting a disease if the disease is presented in anthropomorphic terms than if it is not.
We also test the full causal chain using two methods. First, we test for sequential mediation: that is, we predict that psychological closeness and perceived vulnerability to the disease sequentially mediate the effect of disease anthropomorphism on health compliance. Second, we use moderation-of-process, advanced by Spencer et al. (2005) as a method to provide compelling evidence of a proposed psychological process by manipulating the process to influence the relationship between the independent variable and the dependent variable. We use interventions other than anthropomorphism to heighten psychological closeness and perceived vulnerability in turn, and we test for moderation of the main effect (A causes D). Specifically, we expect anthropomorphism to have no effect on compliance with recommendations for preventing skin cancer when consumers are told that they are physically close to the sun and its carcinogenic effects (i.e., heightened psychological closeness). Similarly, we expect anthropomorphism to have no effect on compliance with recommendations for preventing high blood pressure when consumers are told that their demographics put them at high risk of developing the disease (i.e., heightened perceived vulnerability). In sum, we hypothesize that:
H2 The effect of disease anthropomorphism on health compliance occurs through psychological closeness and perceived vulnerability such that (a) psychological closeness and perceived vulnerability sequentially mediate the effect, and (b) the effect disappears when an intervention other than anthropomorphism heightens psychological closeness or perceived vulnerability to the disease (moderations).
We summarize our conceptual model in Fig. 1.
Fig. 1.
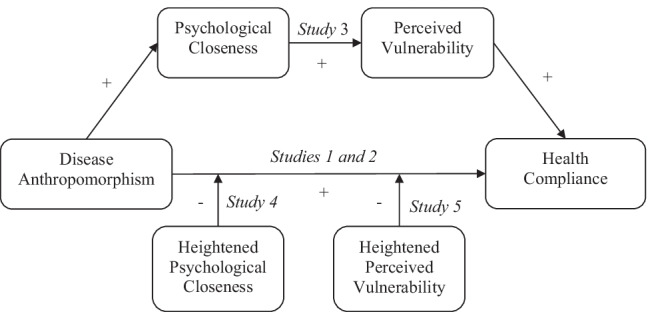
Conceptual model of the effect of disease anthropomorphism on health compliance. Note: Disease anthropomorphism increases health compliance, and the effect occurs through psychological closeness and perceived vulnerability (sequential mediation). Interventions that heighten psychological closeness moderate the effect of disease anthropomorphism on health compliance. Interventions that heighten vulnerability moderate the effect of disease anthropomorphism on health compliance
Empirical overview
In seven studies, we tested our hypotheses about the effect of disease anthropomorphism on health compliance. The first set of studies tested the proposed main effect (H1) in the contexts of COVID-19 (Study 1a; preregistered at AsPredicted.org), yellow fever (Study 1b; preregistered), and breast cancer (Study 2; preregistered). The second set of studies explored our proposed underlying mechanism (H2). Studies 3a (preregistered) and 3b examined the proposed sequential mediating roles of psychological closeness and perceived vulnerability in the effect of disease anthropomorphism on compliance (H2a; disease: breast cancer), and we ruled out alternative explanations. Studies 4 (preregistered; skin cancer) and 5 (high blood pressure) provided additional support for the mechanism using a moderation-of-process approach (H2b) to test the roles of psychological distance and perceived vulnerability, respectively. Table 1 presents a summary of the studies.
Table 1.
Summary of study objectives, designs, and findings
| Objective | Study | Sample | Disease | Manipulation of Anthropo-morphism | Findings |
|---|---|---|---|---|---|
| Main Effect of Disease Anthropomorphism on Health Compliance |
1a (N = 222) |
US Adults | COVID-19 | “Mr. Coronavirus” | Disease anthropomorphism increases health-compliance intentions |
|
1b (N = 150) |
Yellow Fever | “Mr. Yellow Fever” | |||
|
2 (N = 300) |
Chinese Students | Breast Cancer | “I am Breast Cancer” | Disease anthropomorphism increases health-compliance behavior | |
| Mediation through Psychological Closeness and Perceived Vulnerability |
3a (N = 291) |
Chinese Students | Breast Cancer | “I am Breast Cancer” |
• Psychological distance and perceived vulnerability sequentially mediate the effect • Alternative explanations based on known consequences of anthropomorphism (3a) and antecedents of health compliance (3b) cannot explain the effect |
|
3b (N = 159) | |||||
| Moderation by Psychological Closeness |
4 (N = 893) |
Chinese Adults | Skin Cancer | “Mr. Melanoma” | The effect of anthropomorphism on health compliance disappears when psychological distance is heightened by other means |
| Moderation by Perceived Vulnerability |
5 (N = 305) |
US Adults | High Blood Pressure | “I am High Blood Pressure” | The effect of anthropomorphism on health compliance disappears when perceived vulnerability is heightened by other means |
We wish to highlight several ways in which we tested the robustness and generalizability of our findings. As is standard for research on health behavior (Achar et al., 2020; Chandran & Menon, 2004; Menon et al., 2002), we used several diseases because disease characteristics (e.g., infectious or non-infectious; acute or chronic) may influence health compliance by eliciting different levels of fear (Keller & Block, 1996) or affecting assessments of one’s ability to cope with the disease (Block & Keller, 1995). We recruited participants from China and the US because culture, especially the individualism versus collectivism dimension, affects consumers’ responses to health threats (Briley et al., 2017; Kim, Chen, et al., 2016; Kim, Sherman, et al., 2016). Finally, research shows that the way in which an entity is anthropomorphized can influence consumers’ responses to the anthropomorphized entity (Reavey et al., 2018). Considerations for marketing and health communications include the display (image or no image) and voice (third person: May & Monga, 2014; Tam et al., 2013; first person: Puzakova et al., 2013a; Touré-Tillery & McGill, 2015). In our anthropomorphized conditions, we tested first-person and third-person descriptions, with and without an image.
Given the nature of our experiments, all studies ended with a debrief in which participants learned about the objectives of the research project, the purpose and misleading nature of the experimental manipulations, and their random assignment to an experimental condition. Participants were provided with direct contact information for the principal investigator and the monitoring institution in case of questions, issues, or concerns (see Web Appendix A for a sample debriefing form).
In all studies, we excluded participants who had a prior diagnosis of the disease (and, in some studies, those who had been screened for the disease within the past year) because they naturally would have more information about the disease (which might render our experimental message redundant or not applicable) or might feel more psychologically close and vulnerable to the disease. In all cases, to encourage truthful responses to the screening question(s), we chose not to screen out participants at the beginning of the survey (Chandler & Paolacci, 2017). Instead, we presented the screening question(s) within the demographics section at the end of the survey. Participants who were screened out were still compensated for their time. We report the results without exclusions in Web Appendix B; most results are qualitatively unchanged.
For all studies, we estimated a minimum required sample size of 62 participants per experimental condition to achieve a desired power of 0.80 at an alpha level of p = 0.05 with an average effect size of dCohen = 0.51 (based on effect sizes documented in previous research on health compliance; Floyd et al., 2000). To be conservative and maximize power, we aimed to recruit between 75 and 150 participants per experimental condition (after exclusions). Finally, we note that Studies 1b, 3b, and 5 were conducted before the COVID-19 pandemic, whereas Studies 1a, 2, 3a, and 4 were conducted during the pandemic. We used IBM SPSS 21 statistical software to conduct our analyses. The experimental stimuli are available in the Web Appendices. De-identified data for all studies, and preregistration documents, and Web Appendices are available on the Open Science Framework (https://osf.io/tdk47/).
Study 1: Two communicable diseases
In this study, we test our first hypothesis about the effect of disease anthropomorphism on health compliance (H1) using two diseases: COVID-19 in Study 1a and yellow fever (during a hypothetical trip to Panama in Study 1b). In both studies, the disease information was written in the third person and included anthropomorphic or non-anthropomorphic terms (depending on the condition). Participants also received information about the steps required to protect themselves from the disease and then indicated their likelihood of complying with several recommended behaviors; we predicted a higher likelihood of compliance when the disease was anthropomorphized (vs. non-anthropomorphized).
Study 1a: COVID-19
Methods
Participants
We recruited 225 US-based participants on Prolific Academic (Prolific) to complete this experiment for monetary compensation. Prolific is a participant-sourcing platform for online research, and surveys and recent research show that Prolific provides high-quality data when used properly (Eyal et al., 2021; Litman et al., 2021). We ran this study at the beginning of the COVID-19 pandemic in the US (April 2, 2020), when the disease was still relatively unfamiliar. As preregistered, we excluded three participants who reported that they might have had COVID-19 (all in the non-anthropomorphized condition), leaving 222 participants for analyses (128 females, 88 males, 6 non-binary; Median age = 25–34).
Design and procedure
The study employed a two-level (anthropomorphism: yes vs. no) between-subjects design. Participants read a message that described COVID-19 and provided recommendations (presumably from medical or public health authorities) on how to protect themselves and others from this highly contagious virus (see Web Appendix C-I). The beginning of the message varied by condition: “By now, you have certainly heard about the coronavirus” in the non-anthropomorphized condition or “By now, you have certainly heard about Mr. Coronavirus” in the anthropomorphized condition (May & Monga, 2014; Tam et al., 2013).
We measured health compliance by asking participants to indicate their likelihood of engaging in several preventive behaviors (1 = very unlikely, 7 = very likely; α = 0.74) such as “wash your hands regularly for 20 s, with soap and water or an alcohol-based hand rub” (see Web Appendix C-I for the full list of questions). Finally, participants completed a one-item manipulation check (“In the message you just read, to what extent did coronavirus seem nonhuman or human?” 1 = nonhuman, 7 = human) followed by a brief demographic questionnaire that contained the screening question: whether the participant had been told by a medical professional that they (might) have had the coronavirus within the last few weeks (yes, no, or prefer not to answer).
Results
Manipulation check
The anthropomorphism manipulation produced the intended effect (t(220) = -5.23, p < 0.001, dCohen = -0.71): “Mr. Coronavirus” seemed more human than “coronavirus” (Manthropomorphized = 4.45, SD = 2.04 vs. Mnon-anthropomorphized = 3.03, SD = 1.97) (see Fig. 2).
Fig. 2.

Manipulation checks: disease anthropomorphism increases the perceived humanness of the disease (across studies). Notes: (1) Error bars indicate standard errors. (2) *p < .05, ** p < .01, ***p < .001
Health compliance
As expected, participants in the anthropomorphized condition reported a higher likelihood of complying with the health recommendations (M = 5.95, SD = 0.83) than participants in the non-anthropomorphized condition (M = 5.61, SD = 0.85, t(220) = -2.98, p = 0.003; dCohen =—0.40). We note that in this study (and in subsequent ones), the pattern of results was unchanged when we included all demographic variables (e.g., gender, age, whether English was their native language) as covariates in the analysis (see Web Appendix D) and when we included interaction effects between the key variables and gender or age (see Web Appendix E).
Study 1b: Yellow fever
Methods
Participants
We recruited 166 US-based participants from Prolific to complete this experiment online for monetary compensation. As preregistered, we excluded 16 participants (eight in each condition): three reported traveling to Panama (all in the non-anthropomorphized condition), and 15 reported vaccination against yellow fever (seven in the non-anthropomorphized condition and eight in the anthropomorphized condition). We reasoned that both experiences could affect a participant’s assessment of yellow fever and their vulnerability to the disease. The final sample contained 150 participants (70 females, 80 males; Mage = 29.21, SDage = 10.11).
Design and procedure
The study employed a two-level (anthropomorphism: yes vs. no) between-subjects design. Participants read a scenario about traveling to Panama, where there is risk of exposure to yellow fever, described as either “yellow fever is a viral infection spread through mosquito bites” (non-anthropomorphized condition) or “Mr. Yellow Fever is a viral infection spread through mosquito bites” (anthropomorphized condition; see Web Appendix C-II).
The measure of health compliance (1 = very unlikely, 7 = very likely; α = 0.64) included preventive behaviors such as “get the yellow fever vaccine before travelling” (see Web Appendix C-II for the full list of questions). Finally, participants completed a one-item manipulation check (“To what extent did yellow fever seem like a person?” 1 = not at all, 7 = very much) followed by a brief demographic questionnaire, which contained the two screening questions: whether the participant had been to Panama (yes, no) and whether they had been vaccinated against yellow fever (yes, no).
Results
Manipulation check
The anthropomorphism manipulation produced the intended effect (t(148) = -2.71, p = 0.008, dCohen = -0.44): “Mr. Yellow Fever” seemed more like a person than “yellow fever” (Manthropomorphized = 3.19, SD = 2.12 vs. Mnon-anthropomorphized = 2.28, SD = 2.00; see Fig. 2).
Health compliance
Participants in the anthropomorphized condition reported a higher likelihood of complying with the health recommendations (M = 6.36, SD = 0.77) than participants in the non-anthropomorphized condition (M = 6.09, SD = 0.86, t(148) = -2.04, p = 0.043, dCohen = -0.33).
Discussion
Using two communicable diseases, Study 1 provided initial evidence for the effect of disease anthropomorphism on health compliance (H1). Participants reported higher likelihoods of following recommendations to protect themselves from COVID-19 (Study 1a) or yellow fever (Study 1b) when the disease was described in anthropomorphic (vs. non-anthropomorphic) terms.
Study 2: I am breast cancer
Study 2 aimed to replicate the effect of disease anthropomorphism on health compliance (H1) while increasing the robustness, generalizability, and external validity of our findings from Study 1. We used a different type of disease (non-communicable instead of communicable), a different manipulation of anthropomorphism (first person instead of third person), and an experimental design that allowed us to measure a real health behavior (instead of self-reported likelihoods of pursuing recommended behaviors). Specifically, female participants read a message about breast cancer (in non-anthropomorphic terms or anthropomorphized in the first person) and decided whether to take a recommended risk assessment embedded within our study; we expected a higher compliance rate in the anthropomorphized condition.
Methods
Participants
We used wjx, the largest online survey platform based in China, to recruit 313 participants who were prescreened as female (Medianage = 31–40, Modeage = 31–40) to complete the study for monetary compensation. Wjx covers over 2.6 million respondents, allowing for a diverse, authentic, and representative sample (Wang et al., 2020). As preregistered, we excluded one male participant (in the non-anthropomorphized condition), five participants who reported a breast cancer diagnosis (in the non-anthropomorphized condition), and seven participants who reported a clinical breast exam within the last year (one in the anthropomorphized condition and six in the non-anthropomorphized condition). The final sample contained 300 participants (Medianage = 26–30, Modeage = 31–40).
Design and procedure
The study employed a two-level (anthropomorphism: yes vs. no) between-subjects design. Female participants read a message about breast cancer (see Web Appendix C-III); the disease either “talked” about itself in the first person or was discussed in non-anthropomorphic terms (Puzakova et al., 2013a; Touré-Tillery & McGill, 2015).
Participants then read, “The researchers on this project support the efforts of Pink Ribbon International to raise awareness about breast cancer and provide information and resources to aid in the early detection and treatment of breast cancer. The breast cancer risk assessment tool can help you assess your risk of cancer, which can help in the early detection of breast cancer. The Chinese version of the breast cancer risk assessment includes 10 questions and takes about two minutes to complete. You can take this short risk assessment today to learn your personal risk.” The risk assessment was based on the MCCN Clinical Practice Guidelines in Oncology-Breast cancer (Chinese version 2018) and asked about several risk factors (e.g., a family history of breast cancer). Participants learned that the researchers of the wjx survey would not receive participants’ information from their risk assessment, and that their compensation for the wjx survey would not depend on their decision regarding the test. Participants then indicated whether they would like to take the risk assessment (yes, no; our measure of health compliance), and those who answered “yes” proceeded to the test.
Finally, participants completed a one-item manipulation check of disease anthropomorphism (“In the message you just read, to what extent did breast cancer seem nonhuman or human?” 1 = nonhuman, 7 = human) followed by demographics and our screening questions: (a) “Have you been diagnosed with breast cancer in the past?” (yes, no) and (b) “Did you have a clinical breast exam within the past year?” (yes, no).
Results
Manipulation check
The disease-anthropomorphism manipulation produced the intended effect (t(298) =—4.24, p < 0.001, dCohen = -0.49): breast cancer seemed more humanlike in the anthropomorphized condition (Manthropomorphized = 5.07, SD = 1.68) than in the non-anthropomorphized condition (Mnon-anthropomorphized = 4.22, SD = 1.77; see Fig. 2).
Health compliance
A logistic regression of the compliance rate (0 = no, 1 = yes) on anthropomorphism (0 = no, 1 = yes) revealed a positive effect (anthropomorphized condition: 97.96% vs. non-anthropomorphized condition: 92.16%; b = 1.41(0.66); z = 2.14, p = 0.032; odds ratio = 4.09).
Discussion
This study provided a conceptual replication of Studies 1a and 1b, demonstrating the effect of disease anthropomorphism on health compliance (H1) with a different disease, different manipulation of anthropomorphism (first person instead of third person), and a measure of a real health behavior. Female participants who read a health message in which breast cancer was presented in anthropomorphic (vs. non-anthropomorphic) terms were more likely to take a recommended risk assessment. We conducted Study 2 with Chinese participants, and we replicated the result with US-based participants, further demonstrating the robustness of this effect (see Web Appendix F). The remaining studies tested the proposed underlying mechanism of the effect: psychological closeness and perceived vulnerability.
Study 3: Sequential mediation and alternative accounts
We hypothesized that disease anthropomorphism increases health compliance by increasing psychological closeness to the disease, which increases perceived vulnerability to the disease (sequential mediation; H2a). In Studies 3a and 3b, we test this proposed sequential mediation pathway and several alternative accounts. In both studies, female participants read a paragraph about breast cancer and the importance of regular breast self-exams. We measured health compliance as the participant’s interest in performing regular breast self-exams and learning how to screen for the disease.
In Study 3a, we tested alternative explanations based on three documented consequences of anthropomorphism: (a) an increase in the perceived vividness and concreteness (Riva et al., 2015) of the disease, (b) an increase in arousal (Riva et al., 2015), and (c) a decrease in perceived control over the disease (because an anthropomorphized entity seems more agentic; Hur et al., 2015).
In Study 3b, we tested alternative explanations based on three well-known antecedents of health compliance: (a) perceived severity (i.e., the noxiousness of the disease or health concern), (b) self-efficacy (i.e., the belief in one’s own ability to follow health recommendations), and (c) response efficacy (i.e., the belief in the effectiveness of the health recommendations). Indeed, according to protection motivation theory, these three factors (as well as perceived vulnerability) reliably influence health compliance (Rogers, 1975).
Study 3a: Ruling out arousal, vividness/concreteness, and control
Methods
Participants
We recruited 308 female students from a large university in China to participate in this study for monetary compensation. We excluded three participants (two in the non-anthropomorphized condition and one in the anthropomorphized condition) who reported a breast cancer diagnosis and 14 participants (five in the non-anthropomorphized condition and nine in the anthropomorphized condition) who reported breast cancer screening in the last year. The final sample contained 291 participants (Mage = 22.27, SDage = 2.50).
Design and procedure
The study employed a two-level (anthropomorphism: yes vs. no) between-subjects design. Female participants read a message about breast cancer (see Web Appendix C-IV); the disease either “talked” about itself in the first person or was discussed in non-anthropomorphic terms, depending on the condition. Both messages featured the same picture of breast cancer and a health recommendation: “Breast self-exam is an effective way to find breast cancer early, when it’s more likely to be treated successfully. By doing a breast self-exam every month, you can get to know how your breasts normally look and feel, and it will be easier to determine if something has changed.”
We measured health compliance with four questions (α = 0.79), including “How likely are you to perform a breast self-exam in the next week?” (1 = very unlikely, 7 = very likely); see Web Appendix C-IV for the full list of questions). Then, we measured the proposed mediators. We included two measures of psychological closeness: (a) an adapted version of the Inclusion of Other in the Self Scale (Aron et al., 1992), which is a valid measure of the closeness between the participant and another entity (Gächter et al., 2015); and (b) “How close or far do you think breast cancer is from you?” (1 = very far, 7 = very close; r = 0.63, p < 0.001). We measured perceived vulnerability using three questions (α = 0.80) adapted from Cox et al. (2004), including “How likely do you believe it is that you will get breast cancer in the next 10 years?” (1 = very unlikely, 7 = very likely; see Web Appendix C-IV for the full list of questions). These questions were followed by the same manipulation check of disease anthropomorphism used in Study 2.
To test the alternative accounts, we measured arousal (two items; e.g., “I feel aroused,” 1 = strongly disagree, 7 = strongly agree; α = 0.88), vividness/concreteness (“While reading the message, how vividly could you picture breast cancer?” 1 = not at all vividly, 7 = very vividly; “To what extent does breast cancer seem abstract or concrete?” 1 = very abstract; 7 = very concrete; α = 0.83), and perceived control (two items; e.g., “To what extent do you think you are in control of breast cancer?” 1 = not at all, 7 = very much; r = 0.66, p < 0.001; see Web Appendix C-IV for the full list of questions). The survey ended with some basic demographic questions, including whether the participant conducted a breast self-exam regularly (yes, no) and the same screening questions as in Study 2.
Results
We conducted confirmatory factor analysis (see Web Appendix G-I for details), which showed that our measures were adequately distinct,2 with only weak to moderate correlations between the indices (see Table 2).
Table 2.
Descriptive statistics and correlations between all variables measured in Study 3a
| M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|
| 1. Health Compliance | 4.34 (1.17) | 1 | .30*** | .26*** | .26*** | . 40*** | .21*** |
| 2. Psychological Closeness | 3.51 (1.20) | 1 | .46*** | .16** | .23*** | .06 | |
| 3. Perceived Vulnerability | 3.35 (.91) | 1 | .17** | .21*** | -.10 | ||
| 4. Arousal | 3.04 (1.21) | 1 | .34*** | .17** | |||
| 5. Perceived Vividness | 4.36 (1.16) | 1 | .13* | ||||
| 6. Personal Control | 4.24 (1.23) | 1 |
*p < .05, ** p < .01, ***p < .001
Manipulation check
Breast cancer seemed more humanlike in the anthropomorphized condition (M = 3.74, SD = 1.74) than in the non-anthropomorphized condition (M = 3.30, SD = 1.65, t(289) = -2.19, p = 0.029, dCohen = -0.26; see Fig. 2).
Health compliance
As expected, participants in the anthropomorphized condition were more interested in the recommended screening (M = 4.48, SD = 1.10) than those in the non-anthropomorphized condition (M = 4.19, SD = 1.23, t(289) = -2.16, p = 0.032, dCohen = -0.25).
Psychological closeness
Participants in the anthropomorphized condition felt psychologically closer to the disease (M = 3.69, SD = 1.17) than those in the non-anthropomorphized condition (M = 3.32, SD = 1.22, t(289) = -2.60, p = 0.010, dCohen =—0.31).
Perceived vulnerability
Furthermore, participants in the anthropomorphized condition felt marginally more vulnerable to the disease (M = 3.45, SD = 0.93) than those in the non-anthropomorphized condition (M = 3.25, SD = 0.89, t(289) = -1.94, p = 0.053, dCohen = -0.22).
Sequential mediation
We conducted a sequential mediation analysis using the bootstrap test of the indirect effect a1 × d × b2 (Process Model 6; Hayes, 2017; see Fig. 3) and found a positive, significant mean sequential indirect effect (a1 × d × b2 = 0.02(0.02), 95% CI [0.002, 0.06]). We used PROCESS version 3.4 for this analysis. The result indicates that psychological closeness and perceived vulnerability sequentially mediated the effect of disease anthropomorphism on health compliance, consistent with H2a.
Fig. 3.
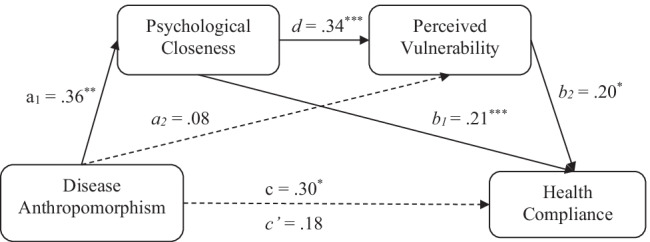
Psychological closeness and perceived vulnerability sequentially mediate the effect of disease anthropomorphism on health compliance (Study 3a, breast cancer). Note: *p < .05, ** p < .01, ***p < .001
Alternative processes
Disease anthropomorphism had no effect on arousal, perceived vividness/concreteness, or perceived control (all ps > 0.35). Furthermore, including the three variables as covariates in the analyses reported above did not qualitatively change the results, so they are unlikely to account for the effect of disease anthropomorphism on health compliance.
We offer some additional thoughts on vividness/concreteness and the relationship between construal level and psychological distance. First our measure of vividness/concreteness might be positively correlated with construal level; objects or events that are represented at a lower level of construal appear more vivid and more concrete than objects or events represented at a higher level. Also, there is a bidirectional positive relationship between psychological distance and construal level; increasing one increases the other (Liberman et al., 2007a), but psychological distance and construal level are distinct constructs, such that the influence of psychological distance on other responses, judgments, and behaviors may occur independently of construal level (see also Williams et al., 2014). The results of Study 3a illustrate the distinction between psychological distance and construal level, as it seems that disease anthropomorphism influences health compliance through psychological distance but not through construal level.
Study 3b: Ruling out perceived severity, self-efficacy, and response efficacy
Methods
Participants
We recruited 161 female students from the graduate business school of a large university in China to participate in this study for monetary compensation. We excluded two participants (both in the non-anthropomorphized condition) who reported a breast cancer diagnosis,3 leaving 159 participants for analysis (Mage = 31.33, SDage = 4.86).
Design and procedure
The study employed a two-level (anthropomorphism: yes vs. no) between-subjects design. The study started with the same manipulated health message and measures of health compliance, psychological closeness (r = 0.51, p < 0.001), and perceived vulnerability (α = 0.83) as in Study 3a.
To test the alternative accounts, we measured the perceived severity of the disease (three items; α = 0.86; e.g., “How serious of a health problem is breast cancer?” 1 = not at all serious, 7 = very serious; see Web Appendix C-V for the full list of questions), self-efficacy (three items; e.g., “To what extent do you feel capable of taking the steps necessary to avoid breast cancer?” 1 = not at all, 7 = very much), and response efficacy (one item; “To what extent do you believe breast self-exam is an effective way to avoid breast cancer?” 1 = not at all, 7 = very much). We merged the responses for self-efficacy and response efficacy because of overlap between the measures; we refer to the combined measure as “perceived efficacy” (α = 0.58). These questions were followed by the same one-item manipulation check of disease anthropomorphism as in Studies 2 and 3a and some basic demographic and health-related questions, including the screening question (whether participants had ever been diagnosed with breast cancer; yes, no).
Results
We conducted confirmatory factor analysis (see Web Appendix G -II for details), which showed that our measures were adequately distinct,4 with only weak to moderate correlations (see Table 3).
Table 3.
Descriptive statistics and correlations between all variables measured in Study 3b
| M (SD) | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
| 1. Health Compliance | 4.79 (1.37) | 1 | .24** | .28*** | .18* | . 27** |
| 2. Psychological Closeness | 3.08 (1.34) | 1 | .50*** | .12 | .04 | |
| 3. Perceived Vulnerability | 3.37 (1.14) | 1 | .07 | -.01 | ||
| 4. Perceived Severity | 5.92 (1.07) | 1 | .11 | |||
| 5. Perceived Efficacy | 4.83 (.99) | 1 |
*p < .05, ** p < .01, ***p < .001
Manipulation check
Breast cancer was rated as more humanlike in the anthropomorphized condition (M = 4.28, SD = 1.93) than in the non-anthropomorphized condition (M = 3.35, SD = 1.82, t(157) = -3.15, p = 0.002, dCohen = -0.50; see Fig. 2).
Health compliance
As expected, participants in the anthropomorphized condition were more interested in the recommended screening (M = 5.02, SD = 1.37) than those in the non-anthropomorphized condition (M = 4.55, SD = 1.33, t(157) = -2.18, p = 0.031, dCohen = -0.35).
Psychological closeness
Participants in the anthropomorphized condition felt psychologically closer to the disease (M = 3.35, SD = 1.35) than those in the non-anthropomorphized condition (M = 2.80, SD = 1.28, t(157) = -2.60, p = 0.010, dCohen = 0.42).
Perceived vulnerability
Furthermore, participants in the anthropomorphized condition felt more vulnerable to the disease (M = 3.58, SD = 1.19) than those in the non-anthropomorphized condition (M = 3.15, SD = 1.05, t(157) = -2.45, p = 0.016, dCohen = 0.38).
Sequential mediation
As in Study 3a, we found a positive, significant mean indirect effect in the bootstrap analysis (a1 × d × b2 = 0.05(0.04), 95% CI [0.002, 0.14]). The result indicates that the effect of disease anthropomorphism on health compliance is sequentially mediated by psychological closeness and perceived vulnerability (H2a; see Fig. 4).
Fig. 4.
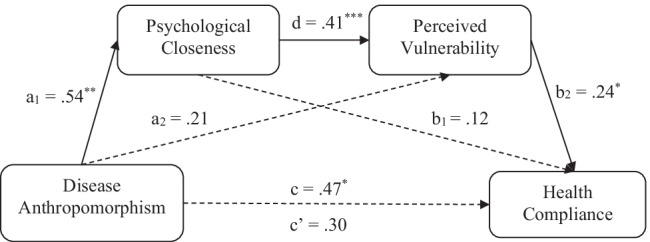
Psychological closeness and perceived vulnerability sequentially mediate the effect of disease anthropomorphism on health compliance (Study 3b, breast cancer). Note: *p < .05, ** p < .01, ***p < .001
Alternative processes
Disease anthropomorphism had no effect on perceived severity or perceived efficacy (all ps > 0.22), and including the two variables as covariates in the analyses reported above did not qualitatively change the results. Nevertheless, we conducted a multiple sequential mediation analysis to test our proposed pathway (through psychological distance and perceived vulnerability) against two alternative pathways: (a) through psychological distance and perceived severity and (b) through psychological distance and perceived efficacy. A bootstrap test of the indirect effect (Model 81; Hayes, 2017) with 5,000 iterations showed that only the sequential mediation path through psychological closeness and perceived vulnerability was significant (b = 0.05(0.04), 95% CI [0.006, 0.15]; see Fig. 5). Neither path (a) through psychological closeness and perceived severity (b = 0.007(0.008), 95% CI [-0.004, 0.03]) nor path (b) through psychological closeness and perceived efficacy (b = 0.007(0.018), 95% CI [-0.019, 0.053]) were significant. The results indicate that the effect of disease anthropomorphism on health compliance is unlikely to occur through assessments of severity or efficacy.
Fig. 5.

Psychological closeness and perceived vulnerability sequentially mediate the effect of breast-cancer anthropomorphism on health compliance controlling for perceived severity and efficacy (Study 3b, breast cancer). Note: *p < .05, ** p < .01, ***p < .001
Discussion
The results of Study 3 support the proposed mechanism: psychological closeness and perceived vulnerability sequentially mediate the effect of disease anthropomorphism on health compliance (H2a). We also ruled out several alternative explanations pertaining to documented consequences of anthropomorphism (arousal, vividness/concreteness, and control; Study 3a) and well-known antecedents of health compliance (perceived severity and efficacy; Study 3b). In the final two studies, we complement the mediation analyses with a moderation-of-process approach, thus identifying theoretically and practically relevant boundary conditions for the effect of disease anthropomorphism on health compliance.
Study 4: Moderation by heightened psychological closeness
In Study 4, we examined the underlying role of psychological closeness in the effect of disease anthropomorphism on health compliance in the setting of a new disease: melanoma (a type of skin cancer). We used a moderation-of-process approach (H2b): we crossed the manipulation of anthropomorphism with a manipulation of psychological distance, for which we explained that the key cause of the disease (the sun) was either physically close (psychologically-close condition) or far away (psychologically-distant condition). We also included a control condition with no information about distance. We expected to replicate the effect of disease anthropomorphism on health compliance in the psychologically-distant and control conditions but not in the psychologically-close condition.
Methods
Participants
We recruited 921 Chinese adults (gender: 494 females, 427 males; age: Median = 26–30) online through wjx to complete this study for monetary compensation. As preregistered, we excluded 28 participants who reported a skin cancer diagnosis (five in the non-anthropomorphized/psychologically-close condition, six in the non-anthropomorphized/psychologically-distant condition, seven in the anthropomorphized/ psychologically-close condition, and 10 in the anthropomorphized/psychologically-distant condition). The final sample contained 893 participants (gender: 484 females, 409 males; age: Median = 26–30).
Design and procedure
This study employed a 2 (anthropomorphism: yes vs. no) × 3 (psychological distance: control vs. close vs. distant) between-subjects design. Participants read a short message about “Mr. Melanoma” (anthropomorphized in the third person) or “melanoma” (non-anthropomorphized; see Web Appendix C-VI). In the psychologically-close [-distant] condition, the message mentioned, “The sun is closer to [farther away from] us than we think,” and it displayed a human stick figure with the sun very nearby [far away]. The sentence and picture were omitted from the control condition.
To measure health compliance, we first prompted participants, “Think about a sunny day in summer, when you are outside for an hour or more between 11am and 3 pm,” and then asked about their likelihood of following sun-protection recommendations (α = 0.56) such as wearing a hat (1 = very unlikely, 7 = very likely; see Web Appendix C-VI for the full list of questions). Finally, participants completed a one-item manipulation check of disease anthropomorphism (similar to the one used in Study 3) and demographic questions, including the screening question: “Have you ever been diagnosed with skin cancer?” (yes, no).
Results
Manipulation check
A 2 (anthropomorphism) × 3 (psychological closeness) analysis of variance (ANOVA) on the manipulation check showed the predicted significant main effect of anthropomorphism (F(1, 887) = 12.84, p < 0.001, ηp2 = 0.014): participants in the anthropomorphized condition (M = 4.07, SD = 1.94) perceived skin cancer as more humanlike than those in the non-anthropomorphized condition (M = 3.62, SD = 1.89). There was no interaction effect (F(2, 887) = 1.12, p = 0.328, ηp2 = 0.003), but there was a marginal main effect of psychological closeness (F(2, 887) = 2.84, p = 0.059, ηp2 = 0.006): participants in the psychologically-close condition (M = 4.04, SD = 1.90) perceived skin cancer as slightly more humanlike than those in the control condition (M = 3.67, SD = 1.97; t(887) = 2.37, p = 0.018).
Health compliance
A 2 (anthropomorphism) × 3 (psychological distance) ANOVA on health compliance revealed no main effect of psychological distance (F(2, 887) = 0.82, p = 0.441, ηp2 = 0.002), a marginal main effect of anthropomorphism (F(1, 887) = 3.68, p = 0.055, ηp2 = 0.004), and, most importantly, a significant anthropomorphism × psychological distance interaction (F(2, 887) = 3.14, p = 0.044, ηp2 = 0.007). Planned contrasts showed a replication of previous findings in the control condition: participants who read about melanoma in anthropomorphic terms reported a higher likelihood of following recommended sun-protection behaviors (M = 5.49, SD = 0.73) than participants who read about melanoma in non-anthropomorphic terms (M = 5.27, SD = 0.97; t(887) = 2.00, p = 0.046, dCohen = 0.26). The same effect of anthropomorphism on compliance occurred in the psychologically-distant condition (Manthropomorphized = 5.40, SD = 0.96 vs. Mnon-anthropomorphized = 5.17, SD = 1.06; t(887) = 2.19, p = 0.029, dCohen = 0.23). By contrast, in the psychologically-close condition, anthropomorphism had no effect on compliance (Manthropomorphized = 5.29, SD = 0.82 vs. Mnon-anthropomorphized = 5.39, SD = 0.98; t(887) = -0.93, p = 0.350, dCohen = -0.11). The results are displayed in Fig. 6.
Fig. 6.
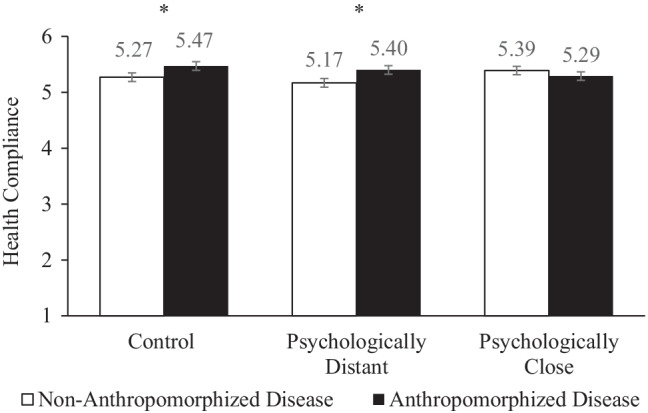
The effect of disease anthropomorphism on health compliance is moderated by a direct manipulation of psychological distance (Study 4, skin cancer). Notes: (1) Error bars indicate standard errors. (2).*p < .05
Discussion
In Study 4, we eliminated the effect of disease anthropomorphism on health compliance in the presence of other information that increased psychological closeness. The result corroborates the conclusion of Study 3 about the underlying role of psychological closeness in the effect of disease anthropomorphism on health compliance: interventions that heighten psychological closeness moderate the effect of disease anthropomorphism on health compliance (H2b). The final study used an analogous moderation-of-process approach to test the underlying role of perceived vulnerability.
Study 5: Moderation by heightened perceived vulnerability
In Study 5, we examined the underlying role of perceived vulnerability in the effect of disease anthropomorphism on health compliance in the context of high blood pressure (HBP). As in Study 4, we used a moderation-of-process approach (H2b): we crossed the manipulation of anthropomorphism with a manipulation of vulnerability to HBP, for which we led some participants to believe that they personally had a high risk of HBP based on their demographics. Participants in the control condition did not receive personal risk information. We expected to replicate the effect of disease anthropomorphism on health compliance in the control condition but not in the high-vulnerability condition.
Methods
Participants
We recruited 393 US-based participants from Amazon’s Mechanical Turk website (MTurk) to complete this experiment for monetary compensation. We pre-screened for participants under the age of 50 using CloudResearch (formerly Turkprime), a participant-sourcing service that draws participants through MTurk (Litman et al., 2017). We restricted the age because we needed to recruit participants with low-to-moderate personal vulnerability to HBP so that we could achieve a strong experimental manipulation of perceived vulnerability. We also excluded participants who reported current HBP issues (34 who responded “yes”) and those whose HBP status we could not confirm (52 who responded “unsure” and 2 who declined to answer), leaving a final sample of 305 responses (120 females; Medianage = 30–34).
Design and procedure
This study employed a 2 (anthropomorphism: yes vs. no) × 2 (vulnerability: high vs. control) between-subjects design. Participants provided some basic information about themselves, including gender, age, race, country of residence, employment status, and income. Participants read a message about HBP that contained information from the website of the American Heart Association (www.heart.org/en/health-topics/high-blood-pressure); HBP either talked about itself in the first person (anthropomorphized condition) or was described in non-anthropomorphic terms (non-anthropomorphized condition; see Web Appendix C-VII for the messages).
We conducted a manipulation check as a post-test with a separate set of participants (N = 301, 245 females; Medianage = 18–24) from the same pool. Participants in the post-test read the same messages as in the main study and indicated the extent to which HBP seemed like a person (1 = not at all, 7 = very much). A 2 (anthropomorphism) × 2 (vulnerability) ANOVA revealed the intended significant main effect of anthropomorphism (F(1, 297) = 170.31, p < 0.001, ηp2 = 0.36): HBP seemed more like a person in the anthropomorphized condition (M = 5.01, SD = 1.56) than in the non-anthropomorphized condition (M = 2.51, SD = 1.75). There was no main effect of the vulnerability manipulation (F(1, 297) = 0.02, p = 0.892, ηp2 < 0.001) and no interaction (F(1, 297) = 0.82, p = 0.367, ηp2 = 0.003).
In the main experiment, the message also contained the vulnerability manipulation immediately after the sentence that ended, “kill almost 1,000 people each day in the US.” In the high-vulnerability condition, the message informed participants that they personally were at high risk of HBP based on their demographic characteristics. Specifically, participants in the anthropomorphized [non-anthropomorphized] condition read, “Given the information you provided earlier, you have a relatively HIGH chance of encountering me [HBP issues] in the near future: > 80.0%.” No information about personal risk appeared in the control condition.
We measured health compliance by asking participants about their likelihood of engaging in a series of behaviors to prevent or control high blood pressure (e.g., “limit your sodium (salt) consumption,” 1 = very unlikely, very likely) and their interest in learning more about high blood pressure (1 = not at all interested, 7 = very interested; α = 0.75; see Web Appendix C-VII for the full list of questions). The survey ended with a full debriefing procedure preceded by two questions, the first of which we used as a screener: (a) “Do you currently have any issues with high blood pressure?” (yes, no, unsure, prefer not to answer), and (b) “Have you checked your blood pressure within the last 6 months?” (yes, no, prefer not to answer). For the screening question, we excluded those who answered “unsure” (as the participant might have a past diagnosis of HBP with an unknown current status) and “prefer not to answer” as well as “yes.”
Results
A 2 (anthropomorphism) × 2 (vulnerability) ANOVA on health compliance revealed no main effects of the anthropomorphism (F(1, 301) = 2.28, p = 0.133, ηp2 = 0.008) or vulnerability manipulations (F(1, 301) = 0.31, p = 0.580, ηp2 = 0.001) but, more importantly, a significant interaction (F(1, 301) = 4.05, p = 0.045, ηp2 = 0.01). Planned contrasts showed that we replicated the positive effect of anthropomorphism in the control condition: participants in the anthropomorphized condition were more interested in recommended behaviors to prevent or control HBP (M = 5.24, SD = 1.14) than participants in the non-anthropomorphized condition (M = 4.77, SD = 1.26; t(301) = -2.46, p = 0.014, dCohen = -0.39). When we artificially heightened personal vulnerability to the disease, however, anthropomorphism had no effect on compliance (Manthropomorphized = 4.90, SD = 1.03; Mnon-anthropomorphized = 4.97, SD = 1.17; t(301) = 0.36, p = 0.718, dCohen = 0.06). The results are displayed in Fig. 7.
Fig. 7.
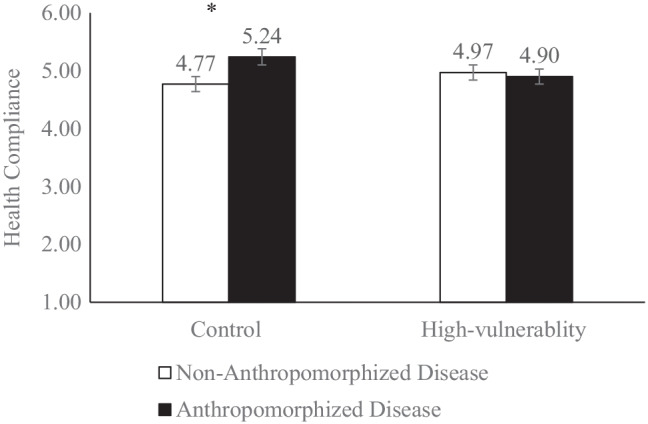
The effect of disease anthropomorphism on health compliance is moderated by a direct manipulation of vulnerability to the disease (Study 5, high blood pressure). Notes: (1) Error bars indicate standard errors. (2).*p < .05
Discussion
In Study 5, we eliminated the effect of disease anthropomorphism on health compliance in the presence of personalized risk information, which was designed to increase perceived vulnerability to the disease. The result corroborates the conclusion of Study 3 about the underlying role of perceived vulnerability in the effect of disease anthropomorphism on health compliance: interventions that heighten perceived vulnerability moderate the effect of disease anthropomorphism on health compliance (H2b).
In Studies 4 and 5, one might have expected higher compliance from participants in the psychologically-close condition (Study 4) and those in the high-vulnerability condition (Study 5) than from those in the control conditions—but we found no main effects of the psychological distance or vulnerability manipulations. We reason that our explicit manipulations of psychological closeness and vulnerability may have increased anxiety about the disease, and anxiety can lead to defensive processing of the health information (e.g., tuning out, downplaying the threat, or denying one’s own vulnerability; Berkowitz & Cottingham, 1960; Janis & Terwilliger, 1962; Morris & Swann, 1996; Pham et al., 2016; Sherman et al., 2000). Furthermore, after learning of their psychological closeness or vulnerability, participants might have felt helpless (Rippetoe & Rogers, 1987); helplessness could cancel out the positive effect of psychological closeness or perceived vulnerability on compliance by decreasing perceived efficacy (Tunner et al., 1989; Wurtele & Maddux, 1987). Our insignificant main effects and the results of prior research underscore the importance of using alternative, indirect approaches—such as disease anthropomorphism—to increase psychological closeness, perceived vulnerability, and hence health compliance.
General discussion
The present article examined how disease anthropomorphism affects consumers’ compliance with health recommendations for preventing or detecting the disease. We demonstrated the beneficial effect of anthropomorphism on compliance with several types of diseases (infectious and non-infectious; acute and chronic), participants from contrasting cultures (China and the US), and several experimental manipulations of anthropomorphism (first- or third-person descriptions; with or without images). After demonstrating the main effect in Studies 1a (COVID-19), 1b (yellow fever), and 2 (breast cancer), we tested the proposed mechanism: disease anthropomorphism makes consumers feel psychologically closer to the disease, which makes them feel more vulnerable to the disease, which increases their motivation to comply with recommendations for disease prevention or detection. We tested the mechanism with sequential mediation analyses in Studies 3a and 3b and with moderation-of-process approaches (Spencer et al., 2005) in Studies 4 and 5. We also ruled out alternative accounts involving documented consequences of anthropomorphism (e.g., vividness/concreteness; Study 3a) and antecedents of health compliance (e.g., perceived efficacy; Study 3b). This research contributes to the growing literature on anthropomorphism and to both the theory and practice of health communication.
Theoretical implications
The present article makes several theoretical contributions. First, by showing that anthropomorphism increases one’s psychological closeness with the nonhuman entity, we contribute to the understanding of the cognitive processes behind anthropomorphism (Epley et al., 2007). The effect of anthropomorphism on psychological closeness may help explain many well-documented consequences of anthropomorphism, such as the greater liking of and caring for anthropomorphized products (Aggarwal & McGill, 2007; Ahn et al., 2014; De Visser et al., 2016; Tam et al., 2013). Indeed, research on psychological distance shows that people experience stronger affective responses to objects and events that are psychologically close (Williams et al., 2014); the closeness may be physical (Williams & Bargh, 2008), temporal (Bruehlman-Senecal & Ayduk, 2015), social (Lin & Utz, 2015), or hypothetical (Buechel et al., 2014).
Second, our work extends the literature on anthropomorphism by identifying a positive consequence of anthropomorphizing a negative attitude object. In previous research, anthropomorphizing negative attitude objects led to negative or maladaptive consequences (Puzakova et al., 2013a). For example, Hur et al. (2015) showed that consumers with a dieting goal were more likely to consume an anthropomorphized (vs. non-anthropomorphized) tempting product (e.g., cookie) because anthropomorphism strengthened consumers’ perceptions that the product was an agent that could be held accountable for the consumers’ behaviors. Similarly, May and Monga (2014) studied participants who were low in social power and found that the anthropomorphism of time made participants less patient, increasing the likelihood of choosing smaller-sooner rewards (e.g., $100 today) over larger-later ones (e.g., $125 in one month). The authors argued that imbuing time with humanlike mental states (e.g., will, intention) made the wait time seem more powerful and aversive to those who felt less powerful. Our research, by contrast, shows that anthropomorphizing a disease increases the likelihood of adaptive responses such as health compliance.
Third, we extend the research on the role of psychological distance in health behavior (Chandran & Menon, 2004; Menon et al., 2002; Murdock & Rajagopal, 2017) by identifying disease anthropomorphism as a novel antecedent to psychological closeness. Consistent with prior research, we find that psychological closeness increases perceived vulnerability, which influences health behaviors. In Study 3b, we go beyond previous investigations by testing the possible influence of psychological closeness on other important drivers of health compliance (perceived severity, self-efficacy, and response efficacy; Maddux & Rogers, 1983; Rogers, 1983). Our comprehensive examination of the mechanism finds no support for the alternative accounts (Studies 3a and 3b) and provides strong support for the proposed mechanism through psychological closeness and perceived vulnerability (Studies 3–5).
Finally, we document the effect of disease anthropomorphism on health compliance with both US participants and Chinese participants, which suggests that the effect is not culture-dependent—although effect sizes might vary. Previous research shows that culture and self-construal moderate the effect of anthropomorphism on judgments and behaviors in some contexts. For example, Kwak et al. (2017) show that consumers with independent self-construal, relative to those with interdependent self-construal, react more negatively to distributive injustice (e.g., price increases) when the brand is anthropomorphized (vs. non-anthropomorphized). By contrast, consumers with interdependent self-construal react more negatively to procedural injustice (e.g., the slow resolution of service failures) when a brand is anthropomorphized (vs. non-anthropomorphized). Hsieh et al. (2021) show that consumers with independent self-construal are more interested in purchasing brands that are anthropomorphized as the consumer’s partner (e.g., “works as your partner and helps ensure a superb experience when you are on the move”) than brands that are anthropomorphized as the consumer’s servant (e.g., “works as your servant and helps ensure a superb user experience when you are on the move”). However, this effect does not occur for consumers with interdependent self-construal. In sum, although culture affects consumers’ responses to anthropomorphized entities in some contexts, we find no difference in the patterns of responses of US and Chinese consumers to anthropomorphized diseases.
Managerial implications
From a practical standpoint, it is no secret that getting the public to comply with health recommendations often is challenging. Global and national public health organizations devote substantial resources to informing people about preventable risk factors—including tobacco use, unhealthy diets, and low physical activity—that lead to many deadly diseases. For example, the US government spent $13 million on anti-smoking ads in 2010 (Creamer, 2012), and in 2014, 890 cancer centers spent about $173 million on advertisements to raise awareness about cancer and cancer prevention (Vater et al., 2014). Furthermore, in 2022, the Centers for Disease Control and Prevention, the leading national public health agency in the US, requested a budget of $15.4 billion5 to fund its various activities, including critical science research and the dissemination of health information.
Even when people are aware of preventable risk factors, they may not be motivated to comply with associated recommendations. For example, although most US consumers understand that exposure to ultraviolet radiation is the most preventable risk factor for all types of skin cancers, only 14.3% of men and 29.9% of women reported using sunscreen regularly in a 2015 survey by the American Academy of Dermatology (Holman et al., 2015). Our findings suggest that healthcare providers and public health organizations can increase compliance with health recommendations by anthropomorphizing diseases in health communications using some of the approaches we take in our studies.
Also, the findings of Studies 4 and 5 may help practitioners identify populations for which disease anthropomorphism may be most effective at increasing compliance. In Study 4, we show that disease anthropomorphism does not increase health compliance when people already feel psychologically close to a key risk factor (the sun, in the context of skin cancer). In Study 5, we find that anthropomorphism does not increase compliance when people already believe they are highly vulnerable to the disease. Thus, anthropomorphism may be most effective in populations of consumers who have (unfounded) perceptions of distance from the disease or its causes and/or who perceive that they are less vulnerable to the disease.
Future directions and limitations
The present article offers several avenues for future explorations. First, our work has focused on using anthropomorphism to motivate healthy people (i.e., those without the focal disease) to reduce their risk of getting the disease. For those who already have the disease (and likely feel close and vulnerable to the disease), however, anthropomorphism might have adverse consequences. For example, the anthropomorphism of cancer might increase the despair felt by cancer patients, and despair might weaken the patients’ will to continue treatment. Future research is needed to investigate how the message recipient’s disease status moderates the effect of disease anthropomorphism. Future research also might consider an interaction effect involving anthropomorphism, disease status, and self-construal. Briley et al. (2017) show that patients with independent self-construal are more likely to follow recommended treatments and are more optimistic about recovering if they adopt an initiator frame (“how will I act?”) than if they adopt a responder frame (“how will I react?”), while the opposite is true for patients with interdependent self-construal. We speculate that disease anthropomorphism might interact with culture and other factors (e.g., initiator vs. responder frame) to influence the health-related behaviors of individuals who already have the disease.
Second, our operationalization of anthropomorphism involved the disease itself (e.g., “I am breast cancer”), but elements of a disease could be anthropomorphized instead. Examples include the germs that cause an infectious disease (e.g., influenza virus), the gene mutation responsible for some cases of a specific cancer (e.g., BRCA1), and symptoms of a disease (e.g., cough, mucus production). Disease elements may be construed at different levels of psychological distance; symptoms may be psychologically closer than the germ or gene mutation responsible for a disease. Given the important role of psychological closeness in health compliance, would it be more effective to anthropomorphize the mucus produced by an influenza infection than to anthropomorphize the influenza virus? Relatedly, future research could explore whether the pathway via psychological closeness and perceived vulnerability can extend to compliance with recommendations regarding other negative or dangerous attitude objects. For example, would people feel more vulnerable to anthropomorphized (vs. non-anthropomorphized) guns or illegal drugs and hence be more willing to follow recommendations to avoid these objects (or support policies that restrict access to these objects)?
Third, future research may test other downstream consequences of the effect of anthropomorphism on psychological closeness in the contexts of product and brand choices beyond health behaviors. For example, people tend to overweigh secondary considerations for psychologically-close choices, whereas they rely more heavily on primary considerations (i.e., act according to their priorities) for psychologically-distant choices (Liberman et al., 2007b; Rim et al., 2013). These findings suggest a possible downside of product or brand anthropomorphism: by increasing psychological closeness, the anthropomorphism of a product or brand (e.g., car) may skew consumers’ considerations toward relatively unimportant factors (e.g., color) instead of top priorities (e.g., safety).
Fourth, the present research does not evaluate the duration of the effect of anthropomorphism on health compliance, but the persistence of preventive health behaviors is crucial to the success of many public health efforts (e.g., consistent mask-wearing for many months during the COVID-19 pandemic). Thus, we urge future research to investigate the long-term effects of interventions like ours and those in prior research (e.g., Chandran & Menon, 2004; Menon et al., 2002; Murdock & Rajagopal, 2017). We believe our study of a short-term effect is still relevant, though: understanding the immediate antecedents of behavioral change is important because past behavior is a strong predictor of future behavior (Ferguson & Bibby, 2002; Ouellette & Wood, 1998), and some public health efforts focus almost exclusively on a discrete, short-term act of compliance (e.g., getting vaccinated).
Finally, we found minimal to no interaction effects involving demographic variables such as gender and age (see Web Appendix E), most likely an artifact of the experimental design and random assignment. We will briefly describe an exception that illustrates an avenue for future research: In Study 4, we found a marginal 3-way interaction of gender, anthropomorphism, and psychological distance on compliance. Specifically, for male participants, we replicated the anthropomorphism × psychological distance interaction that we found in the full sample. However, for female participants, there was no interaction between anthropomorphism and psychological distance. Furthermore, we found a significant main effect of gender: female participants were more willing to comply than male participants, perhaps because, in this specific context, female participants were more likely to have other goals (e.g., skin care, anti-aging) that are compatible with sun protection behaviors. Future research could investigate the contexts in which demographic variables such as age and gender interact with anthropomorphism to influence (health-related) judgments and behaviors.
Supplementary Information
Below is the link to the electronic supplementary material.
Funding
This research was supported by grants from the National Natural Science Foundation of China (Grant No. 71972169) awarded to the first author, and by funding from the Richard M. Clewett Endowed Professorship, Kellogg School of Management, awarded to the second author. All authors contributed equally to this research. The authors’ names are listed in reverse alphabetical order.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
COVID-19: https://mp.weixin.qq.com/s/Yu6AbvDJnmb0_aWKHjBCfA; Mucus/Mucinex: https://www.youtube.com/watch?v=MGltaIqro-g; “Cells at Work!”: https://www.youtube.com/watch?v=Ek39M_lYUtE.
Study 3a included many questions that assessed multiple constructs, so we followed Leung, Kim, and Tse (2020) and conducted confirmatory factor analysis to determine whether the constructs were distinct. Results showed that all items loaded on the intended factor, and the average variance extracted (AVE) exceeded .50 (psychological closeness = .64, perceived vulnerability = .59, arousal = .65, vividness/concreteness = .56, perceived control = .66). Fornell and Larcker’s (1981) test also revealed that all AVEs were higher than the shared variances of .33, confirming that the measures represented distinct constructs.
We conducted Study 3b before Studies 2 and 3a, and unfortunately, we did not think to measure whether participants had received a professional breast screening within the last year.
As in Study 3a, we conducted confirmatory factor analysis for the items measured in Study 3b. Results showed that self-efficacy and response efficacy loaded on a single factor (which we combined into “efficacy”), but all other items loaded on the intended factors. The AVEs exceeded 0.50 for psychological closeness (.60), perceived vulnerability (.66), and perceived severity (.68) but not efficacy (.33). Fornell and Larcker’s (1981) test revealed that the AVEs of the first three variables exceeded the shared variance of .33, but the AVE of efficacy did not. One item in the efficacy measure (“To what extent do you believe that getting breast cancer is inevitable, and there is very little you can do to avoid it?”) exhibited weak correlations with the remaining items, which accounted for the relatively low reliability score. We kept this item in the analysis, but the results are qualitatively the same if we exclude it.
CDC Statement on President’s Fiscal Year 2022 Budget: https://www.cdc.gov/media/releases/2021/s0528-fiscal-year-2022.html.
Martin Mende served as Area Editor for this article.
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Lili Wang, Email: lw122@zju.edu.cn.
Maferima Touré-Tillery, Email: m-touretillery@kellogg.northwestern.edu.
Ann L. McGill, Email: ann.mcgill@chicagobooth.edu
References
- Achar C, Agrawal N, Hsieh MH. Fear of detection and efficacy of prevention: Using construal level to encourage health behaviors. Journal of Marketing Research. 2020;57(3):582–598. doi: 10.1177/0022243720912443. [DOI] [Google Scholar]
- Aggarwal P, McGill AL. Is that car smiling at me? Schema congruity as a basis for evaluating anthropomorphized products. Journal of Consumer Research. 2007;34(4):468–479. doi: 10.1086/518544. [DOI] [Google Scholar]
- Aggarwal P, McGill AL. When brands seem human, do humans act like brands? Automatic behavioral priming effects of brand anthropomorphism. Journal of Consumer Research. 2012;39(2):307–323. doi: 10.1086/662614. [DOI] [Google Scholar]
- Ahn H-K, Kim H-J, Aggarwal P. Helping fellow beings: Anthropomorphized social causes and the role of anticipatory guilt. Psychological Science. 2014;25(1):224–229. doi: 10.1177/0956797613496823. [DOI] [PubMed] [Google Scholar]
- Aron A, Aron EN, Smollan D. Inclusion of Other in the Self Scale and the structure of interpersonal closeness. Journal of Personality and Social Psychology. 1992;63(4):596–612. doi: 10.1037/0022-3514.63.4.596. [DOI] [Google Scholar]
- Berger J, Rand L. Shifting signals to help health: Using identity signaling to reduce risky health behaviors. Journal of Consumer Research. 2008;35(3):509–518. doi: 10.1086/587632. [DOI] [Google Scholar]
- Berkowitz L, Cottingham DR. The interest value and relevance of fear arousing communications. The Journal of Abnormal and Social Psychology. 1960;60(1):37–43. doi: 10.1037/h0045247. [DOI] [PubMed] [Google Scholar]
- Block LG, Keller PA. When to accentuate the negative: The effects of perceived efficacy and message framing on intentions to perform a health-related behavior. Journal of Marketing Research. 1995;32(2):192–203. doi: 10.1177/002224379503200206. [DOI] [Google Scholar]
- Block LG, Keller PA. Beyond protection motivation: An integrative theory of health appeals. Journal of Applied Social Psychology. 1998;28(17):1584–1608. doi: 10.1111/j.1559-1816.1998.tb01691.x. [DOI] [Google Scholar]
- Bränström R, Kristjansson S, Ullen H. Risk perception, optimistic bias, and readiness to change sun related behaviour. The European Journal of Public Health. 2006;16(5):492–497. doi: 10.1093/eurpub/cki193. [DOI] [PubMed] [Google Scholar]
- Briley DA, Rudd M, Aaker J. Cultivating optimism: How to frame your future during a health challenge. Journal of Consumer Research. 2017;44(4):895–915. doi: 10.1093/jcr/ucx075. [DOI] [Google Scholar]
- Brouwers MC, Sorrentino RM. Uncertainty orientation and protection motivation theory: The role of individual differences in health compliance. Journal of Personality and Social Psychology. 1993;65(1):102–112. doi: 10.1037/0022-3514.65.1.102. [DOI] [Google Scholar]
- Bruehlman-Senecal E, Ayduk O. This too shall pass: Temporal distance and the regulation of emotional distress. Journal of Personality and Social Psychology. 2015;108(2):356–375. doi: 10.1037/a0038324. [DOI] [PubMed] [Google Scholar]
- Buechel EC, Zhang J, Morewedge CK, Vosgerau J. More intense experiences, less intense forecasts: Why people overweight probability specifications in affective forecasts. Journal of Personality and Social Psychology. 2014;106(1):20–36. doi: 10.1037/a0034478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandler JJ, Paolacci G. Lie for a dime: When most prescreening responses are honest but most study participants are impostors. Social Psychological and Personality Science. 2017;8(5):500–508. doi: 10.1177/1948550617698203. [DOI] [Google Scholar]
- Chandler JJ, Schwarz N. Use does not wear ragged the fabric of friendship: Thinking of objects as alive makes people less willing to replace them. Journal of Consumer Psychology. 2010;20(2):138–145. doi: 10.1016/j.jcps.2009.12.008. [DOI] [Google Scholar]
- Chandran S, Menon G. When a day means more than a year: Effects of temporal framing on judgments of health risk. Journal of Consumer Research. 2004;31(2):375–389. doi: 10.1086/422116. [DOI] [Google Scholar]
- Cox DN, Koster A, Russell CG. Predicting intentions to consume functional foods and supplements to offset memory loss using an adaptation of protection motivation theory. Appetite. 2004;43(1):55–64. doi: 10.1016/j.appet.2004.02.003. [DOI] [PubMed] [Google Scholar]
- Creamer, M. (2012). Anti-smoking campaigns work, so don’t quit now. Ad Age. Accessed August 15, 2019, from https://adage.com/article/news/funding-anti-tobacco-ads-fell-quitting-rate/232111
- De Visser EJ, Monfort SS, Mckendrick R, Smith MA. Almost human: Anthropomorphism increases trust resilience in cognitive agents. Journal of Experimental Psychology. 2016;22(3):331–349. doi: 10.1037/xap0000092. [DOI] [PubMed] [Google Scholar]
- Egenhofer MJ. Deriving the composition of binary topological relations. Journal of Visual Languages & Computing. 1994;5(2):133–149. doi: 10.1006/jvlc.1994.1007. [DOI] [Google Scholar]
- Epley N, Waytz A, Cacioppo JT. On seeing a human: A three-factor theory of anthropomorphism. Psychological Review. 2007;114(4):864–886. doi: 10.1037/0033-295X.114.4.864. [DOI] [PubMed] [Google Scholar]
- Eyal P, Rothschild DM, Evernden Z, Gordon A, Damer E. Data quality of platforms and panels for online behavioral research. Behavior Research Methods. 2021 doi: 10.3758/s13428-021-01694-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fauconnier G, Turner M. The way we think: Conceptual blending and the mind’s hidden complexities. Basic Books; 2008. [Google Scholar]
- Ferguson E, Bibby PA. Predicting future blood donor returns: Past behavior, intentions, and observer effects. Health Psychology. 2002;21(5):513–518. doi: 10.1037/0278-6133.21.5.513. [DOI] [PubMed] [Google Scholar]
- Floyd DL, Prentice-Dunn S, Rogers RW. A meta-analysis of research on protection motivation theory. Journal of Applied Social Psychology. 2000;30(2):407–429. doi: 10.1111/j.1559-1816.2000.tb02323.x. [DOI] [Google Scholar]
- Folkes VS, Kiesler T. Social cognition: Consumers’ inferences about the self and others. Handbook of Consumer Behavior. 1991;3:281–315. [Google Scholar]
- Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research. 1981;18(1):39–50. doi: 10.1177/002224378101800104. [DOI] [Google Scholar]
- Gächter S, Starmer C, Tufano F. Measuring the closeness of relationships: A comprehensive evaluation of the 'Inclusion of the Other in the Self’ scale. PLoS ONE. 2015;10(6):e0129478. doi: 10.1371/journal.pone.0129478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guthrie, S. E. (1993). Faces in the clouds.Oxford University Press.
- Han D, Duhachek A, Agrawal N. Coping and construal level matching drives health message effectiveness via response efficacy or self-efficacy enhancement. Journal of Consumer Research. 2016;43(3):429–447. doi: 10.1093/jcr/ucw036. [DOI] [Google Scholar]
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis. Guilford Press; 2017. [Google Scholar]
- Heider F. The psychology of interpersonal relations. Wiley; 1958. [Google Scholar]
- Hellmich, N. (2013). Most people aren’t meeting exercise guidelines. USA Today, Accessed July 22, 2019, from https://www.usatoday.com/story/news/nation/2013/05/02/physical-activity-guidelines/2128971/
- Higgins ET. The” self digest”: Self-knowledge serving self-regulatory functions. Journal of Personality and Social Psychology. 1996;71(6):1062–1083. doi: 10.1037/0022-3514.71.6.1062. [DOI] [PubMed] [Google Scholar]
- Hovland C, Janis I, Kelley H. Communication and persuasion. Yale University Press; 1953. [Google Scholar]
- Holman DM, Berkowitz Z, Guy GP, Jr, Hawkins NA, Saraiya M, Watson M. Patterns of sunscreen use on the face and other exposed skin among US adults. Journal of the American Academy of Dermatology. 2015;73(1):83–92. doi: 10.1016/j.jaad.2015.02.1112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsieh MH, Li XB, Jain SP, Swaminathan V. Self-construal drives preference for partner and servant brands. Journal of Business Research. 2021;129:183–192. doi: 10.1016/j.jbusres.2021.02.054. [DOI] [Google Scholar]
- Hur JD, Koo M, Hofmann W. When temptations come alive: How anthropomorphism undermines self-control. Journal of Consumer Research. 2015;42(2):340–358. [Google Scholar]
- Janis IL, Terwilliger RF. An experimental study of psychological resistances to fear arousing communications. The Journal of Abnormal and Social Psychology. 1962;65(6):403–410. doi: 10.1037/h0047601. [DOI] [PubMed] [Google Scholar]
- Keller PA, Block LG. Increasing the persuasiveness of fear appeals: The effect of arousal and elaboration. Journal of Consumer Research. 1996;22(4):448–459. doi: 10.1086/209461. [DOI] [Google Scholar]
- Kim DJM, Yoon S. Guilt of the meat-eating consumer: When animal anthropomorphism leads to healthy meat dish choices. Journal of Consumer Psychology. 2021;31(4):665–683. doi: 10.1002/jcpy.1215. [DOI] [Google Scholar]
- Kim HS, Sherman DK, Updegraff JA. Fear of Ebola: The influence of collectivism on xenophobic threat responses. Psychological Science. 2016;27(7):935–944. doi: 10.1177/0956797616642596. [DOI] [PubMed] [Google Scholar]
- Kim S, McGill AL. Gaming with Mr. Slot or gaming the slot machine? Power, anthropomorphism, and risk perception. Journal of Consumer Research. 2011;38(1):94–107. doi: 10.1086/658148. [DOI] [Google Scholar]
- Kim S, Chen RP, Zhang K. Anthropomorphized helpers undermine autonomy and enjoyment in computer games. Journal of Consumer Research. 2016;43(2):282–302. doi: 10.1093/jcr/ucw016. [DOI] [Google Scholar]
- Koo M, Oh H, Patrick VM. From oldie to goldie: Humanizing old produce enhances its appeal. Journal of the Association for Consumer Research. 2019;4(4):337–351. doi: 10.1086/705032. [DOI] [Google Scholar]
- Kwak H, Puzakova M, Rocereto JF. Better not smile at the price: The differential role of brand anthropomorphization on perceived price fairness. Journal of Marketing. 2015;79(4):56–76. doi: 10.1509/jm.13.0410. [DOI] [Google Scholar]
- Kwak H, Puzakova M, Rocereto JF. When brand anthropomorphism alters perceptions of justice: The moderating role of self-construal. International Journal of Research in Marketing. 2017;34(4):851–871. doi: 10.1016/j.ijresmar.2017.04.002. [DOI] [Google Scholar]
- Lakoff G, Johnson M. Conceptual metaphor in everyday language. The Journal of Philosophy. 1980;77(8):453–486. doi: 10.2307/2025464. [DOI] [Google Scholar]
- Leung FF, Kim S, Tse CH. Highlighting effort versus talent in service employee performance: Customer attributions and responses. Journal of Marketing. 2020;48(3):106–121. doi: 10.1177/0022242920902722. [DOI] [Google Scholar]
- Liberman N, Trope Y, Stephan E. Psychological distance. Guilford Press; 2007. [Google Scholar]
- Liberman N, Trope Y, McCrea SM, Sherman SJ. The effect of level of construal on the temporal distance of activity enactment. Journal of Experimental Social Psychology. 2007;43(1):143–149. doi: 10.1016/j.jesp.2005.12.009. [DOI] [Google Scholar]
- Lin R, Utz S. The emotional responses of browsing Facebook: Happiness, envy, and the role of tie strength. Computers in Human Behavior. 2015;52:29–38. doi: 10.1016/j.chb.2015.04.064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lisjak M, Lee AY. The bright side of impulse: Depletion heightens self-protective behavior in the face of danger. Journal of Consumer Research. 2014;41(1):55–70. doi: 10.1086/674975. [DOI] [Google Scholar]
- Litman, L., Moss, A., Rosenzweig, C., & Robinson, J. (2021). Reply to MTurk, Prolific or panels? Choosing the right audience for online research. SSRN Electronic Journal.10.2139/ssrn.3775075
- Litman L, Robinson J, Abberbock T. Turkprime.com: A versatile crowdsourcing data acquisition platform for the behavioral sciences. Behavior Research Methods. 2017;49(2):433–442. doi: 10.3758/s13428-016-0727-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maddux JE, Rogers RW. Protection motivation and self-efficacy: A revised theory of fear appeals and attitude change. Journal of Experimental Social Psychology. 1983;19(5):469–479. doi: 10.1016/0022-1031(83)90023-9. [DOI] [Google Scholar]
- Maglio SJ. Psychological distance in consumer psychology: Consequences and antecedents. Consumer Psychology Reviewer. 2020;3(1):108–125. doi: 10.1002/arcp.1057. [DOI] [Google Scholar]
- Mann L. The effects of emotional role playing on desire to modify smoking habits. Journal of Experimental Social Psychology. 1967;3(4):334–338. doi: 10.1016/0022-1031(67)90002-9. [DOI] [Google Scholar]
- May F, Monga A. When time has a will of its own, the powerless don’t have the will to wait: Anthropomorphism of time can decrease patience. Journal of Consumer Research. 2014;40(5):924–942. doi: 10.1086/673384. [DOI] [Google Scholar]
- Menon G, Block LG, Ramanathan S. We’re at as much risk as we are led to believe: Effects of message cues on judgments of health risk. Journal of Consumer Research. 2002;28(4):533–549. doi: 10.1086/338203. [DOI] [Google Scholar]
- Morris KA, Swann WB., Jr . Denial and the AIDS crisis: On wishing away the threat of AIDS. In: Oskamp S, Thompson SC, editors. Understanding and preventing HIV risk behavior: Safer sex and drug use. Sage Publications Inc; 1996. pp. 57–79. [Google Scholar]
- Murdock MR, Rajagopal P. The sting of social: How emphasizing social consequences in warning messages influences perceptions of risk. Journal of Marketing. 2017;81(2):83–98. doi: 10.1509/jm.15.0402. [DOI] [Google Scholar]
- Nagel T. What is it like to be a bat? The Philosophical Review. 1974;83(4):435–450. doi: 10.2307/2183914. [DOI] [Google Scholar]
- Ouellette JA, Wood W. Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior. Psychological Bulletin. 1998;124(1):54–74. doi: 10.1037/0033-2909.124.1.54. [DOI] [Google Scholar]
- Paddock C. (2016). CDC: 90% of Americans consume too much salt. Medical News Today, Accessed July 22, 2019, from https://www.medicalnewstoday.com/articles/304833
- Pechmann C, Zhao G, Goldberg ME, Reibling ET. What to convey in antismoking advertisements for adolescents: The use of protection motivation theory to identify effective message themes. Journal of Marketing. 2003;67(2):1–18. doi: 10.1509/jmkg.67.2.1.18607. [DOI] [Google Scholar]
- Pham N, Mandel N, Morales AC. Messages from the food police: How food-related warnings backfire among dieters. Journal of the Association for Consumer Research. 2016;1(1):175–190. doi: 10.1086/684394. [DOI] [Google Scholar]
- Puzakova M, Aggarwal P. Brands as rivals: Consumer pursuit of distinctiveness and the role of brand anthropomorphism. Journal of Consumer Research. 2018;45(4):869–888. doi: 10.1093/jcr/ucy035. [DOI] [Google Scholar]
- Puzakova M, Kwak H, Rocereto JF. When humanizing brands goes wrong: The detrimental effect of brand anthropomorphization amid product wrongdoings. Journal of Marketing. 2013;77(3):81–100. doi: 10.1509/jm.11.0510. [DOI] [Google Scholar]
- Puzakova M, Rocereto JF, Kwak H. Ads are watching me: A view from the interplay between anthropomorphism and customisation. International Journal of Advertising. 2013;32(4):513–538. doi: 10.2501/IJA-32-4-513-538. [DOI] [Google Scholar]
- Raghubir P, Menon G. AIDS and me, never the twain shall meet: The effects of information accessibility on judgments of risk and advertising effectiveness. Journal of Consumer Research. 1998;25(1):52–63. doi: 10.1086/209526. [DOI] [Google Scholar]
- Reavey B, Puzakova M, Larsen Andras T, Kwak H. The multidimensionality of anthropomorphism in advertising: The moderating roles of cognitive busyness and assertive language. International Journal of Advertising. 2018;37(3):440–462. doi: 10.1080/02650487.2018.1438054. [DOI] [Google Scholar]
- Rim S, Hansen J, Trope Y. What happens why? Psychological distance and focusing on causes versus consequences of events. Journal of Personality and Social Psychology. 2013;104(3):457–472. doi: 10.1037/a0031024. [DOI] [PubMed] [Google Scholar]
- Rippetoe PA, Rogers RW. Effects of components of protection-motivation theory on adaptive and maladaptive coping with a health threat. Journal of Personality and Social Psychology. 1987;52(3):596–604. doi: 10.1037/0022-3514.52.3.596. [DOI] [PubMed] [Google Scholar]
- Riva P, Sacchi S, Brambilla M. Humanizing machines: Anthropomorphization of slot machines increases gambling. Journal of Experimental Psychology: Applied. 2015;21(4):313–325. doi: 10.1037/xap0000057. [DOI] [PubMed] [Google Scholar]
- Rogers RW. A protection motivation theory of fear appeals and attitude change. The Journal of Psychology: Interdisciplinary and Applied. 1975;91(1):93–114. doi: 10.1080/00223980.1975.9915803. [DOI] [PubMed] [Google Scholar]
- Rogers RW. Preventive health psychology: An interface of social and clinical psychology. Journal of Social and Clinical Psychology. 1983;1(2):120–127. doi: 10.1521/jscp.1983.1.2.120. [DOI] [Google Scholar]
- Sherman DA, Nelson LD, Steele CM. Do messages about health risks threaten the self? Increasing the acceptance of threatening health messages via self-affirmation. Personality and Social Psychology Bulletin. 2000;26(9):1046–1058. doi: 10.1177/01461672002611003. [DOI] [Google Scholar]
- Spencer SJ, Zanna MP, Fong GT. Establishing a causal chain: Why experiments are often more effective than mediational analyses in examining psychological processes. Journal of Personality and Social Psychology. 2005;89(6):845–851. doi: 10.1037/0022-3514.89.6.845. [DOI] [PubMed] [Google Scholar]
- Tam K, Lee S, Chao MM. Saving Mr. Nature: Anthropomorphism enhances connectedness to and protectiveness toward nature. Journal of Experimental Social Psychology. 2013;49(3):514–521. doi: 10.1016/j.jesp.2013.02.001. [DOI] [Google Scholar]
- The Centers for Disease Control and Prevention (2020). Flu vaccination coverage, United States, 2019–20 Influenza Season. Accessed Feb 24, 2022, from https://www.cdc.gov/flu/fluvaxview/coverage-1920estimates.htm
- Touré-Tillery M, McGill AL. Who or what to believe: Trust and the differential persuasiveness of human and anthropomorphized messengers. Journal of Marketing. 2015;79(4):94–110. doi: 10.1509/jm.12.0166. [DOI] [Google Scholar]
- Trope Y, Liberman N. Construal-level theory of psychological distance. Psychological Review. 2010;117(2):440–463. doi: 10.1037/a0018963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trope Y, Liberman N, Wakslak C. Construal levels and psychological distance: Effects on representation, prediction, evaluation, and behavior. Journal of Consumer Psychology. 2007;17(2):83–95. doi: 10.1016/S1057-7408(07)70013-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tunner JF, Jr, Day E, Crask MR. Protection motivation theory: An extension of fear appeals theory in communication. Journal of Business Research. 1989;19(4):267–276. doi: 10.1016/0148-2963(89)90008-8. [DOI] [Google Scholar]
- Vater LB, Donohue JM, Arnold R, White DB, Chu E, Schenker Y. What are cancer centers advertising to the public? A content analysis. Annals of Internal Medicine. 2014;160(2):813–820. doi: 10.7326/M14-0500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wan EW, Chen RP, Jin L. Judging a book by its cover? The effect of anthropomorphism on product attribute processing and consumer preference. Journal of Consumer Research. 2017;43(6):1008–1030. [Google Scholar]
- Wan J, Kulow K, Cowan K. It’s alive! Increasing protective action against the coronavirus through anthropomorphism and construal. Journal of the Association for Consumer Research. 2022;7(1):81–88. doi: 10.1086/711849. [DOI] [Google Scholar]
- Wang H, Jing R, Lai Z, Zhang J, Lyu Y, Knoll MD, Fang H. Acceptance of COVID-19 vacination during the COVID-19 pandemic in China. Vaccines. 2020;8(3):482. doi: 10.3390/vaccines8030482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang L, Kim S, Zhou Y. Money in a “safe” place: Money anthropomorphism increases saving behavior. International Journal of Research in Marketing, Forthcoming, 2022 doi: 10.1016/j.ijresmar.2022.02.001. [DOI] [Google Scholar]
- Williams LE, Bargh JA. Experiencing physical warmth promotes interpersonal warmth. Science. 2008;322(5901):606–607. doi: 10.1126/science.1162548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams LE, Stein R, Galguera L. The distinct affective consequences of psychological distance and construal level. Journal of Consumer Research. 2014;40(6):1123–1138. doi: 10.1086/674212. [DOI] [Google Scholar]
- Wilson DK, Purdon SE, Wallston KA. Compliance to health recommendations: A theoretical overview of message framing. Health Education Research. 1988;3(2):161–171. doi: 10.1093/her/3.2.161. [DOI] [Google Scholar]
- Wolff P, Barbey AK. Causal reasoning with forces. Frontiers in Human Neuroscience. 2015;9:1–17. doi: 10.3389/fnhum.2015.00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (2020). The top 10 causes of death. Accessed December 12, 2021, from https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
- Wurtele SK, Maddux JE. Relative contributions of protection motivation theory components in predicting exercise intentions and behavior. Health Psychology. 1987;6(5):453–466. doi: 10.1037/0278-6133.6.5.453. [DOI] [PubMed] [Google Scholar]
- Yan D, Sengupta J. The influence of base rate and case information on health-risk perceptions: A unified model of self-positivity and self-negativity. Journal of Consumer Research. 2013;39(5):931–946. doi: 10.1086/666596. [DOI] [Google Scholar]
- Zhou X, Kim S, Wang L. Money helps when money feels: Money anthropomorphism increases charitable giving. Journal of Consumer Research. 2019;45(5):953–972. doi: 10.1093/jcr/ucy012. [DOI] [Google Scholar]
- Zhu H, Wong N, Huang M. Does relationship matter? How social distance influences perceptions of responsibility on anthropomorphized environmental objects and conservation intentions. Journal of Business Research. 2019;95:62–70. doi: 10.1016/j.jbusres.2018.10.008. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.