

Abstract
As adolescence is a time characterized by rapid changes in social relationships as well as an increase in risk-taking behaviors, this prospective longitudinal study examined whether social involvement and social alienation are associated with changes in alcohol use from adolescence into young adulthood moderated by organizational and personal religiousness. Participants were 167 adolescents (53% male) assessed five times between ages 14 and 18 years old. Latent change score modeling analyses indicated that social alienation was positively associated with greater increases in alcohol use among those with low organizational religiousness and those with low personal religiousness in early adolescence and during the transition into young adulthood. The findings demonstrate the detrimental effects of social relationship risk factors that promote alcohol use during adolescence into young adulthood. The results further highlight the protective roles of organizational and personal religiousness acting as additional sources of social engagement experiences to modulate the effects of social alienation predicting alcohol use progression and provide evidence for the positive impact religiousness has on healthy adolescent development.
Keywords: Social relationships, Social involvement, Social alienation, Religiousness, Substance use, Alcohol use
Introduction
As a period characterized by salient neurobiological changes, the adolescent years present a great threat of risk-taking behavior (Steinberg, 2010). One such risk-taking behavior is substance use, which is a major public health concern as it is often linked to long-term difficulties with health and well-being, including heightened mental health concerns such as depression (Walters et al., 2018) and premature involvement in risky sexual behavior (Benotsch et al., 2013). Among the risk factors associated with the use of any substance, alcohol use in particular has been linked to neurocognitive impairments including alterations in the development of grey and white matter, attention and verbal learning, and visuospatial processing (Spear, 2018) as well as prefrontal cortex functioning involved in cognitive control which is critical to risky decision making such as substance use (Feldstein Ewing et al., 2015; Squeglia et al., 2009). Further, during adolescence, peers typically replace parents as adolescents’ main source of social support (Rosenthal & Kobak, 2010), and friendships during adolescence become increasingly important, providing companionship and a sense of self-worth (Erdley & Day, 2017). Some adolescents thrive in this new social environment, gaining widespread acceptance, whereas other adolescents find this to be a period of alienation, having experienced low-quality friendships, rejection, and even peer victimization (Erdley & Day, 2017). As discussed in the following sections, social relationship risk factors are a common catalyst for the use of substances, both in young people who have high social involvement, as well as in those who are alienated from their peers (Copeland et al., 2018; Moody et al., 2011). However, there remains a gap in the literature regarding protective factors that interface with social relationship risk factors. Thus, the present study examines whether religiousness buffers against longitudinal links between social relationship risk factors and substance use development.
Social Involvement and Substance Use
Research has demonstrated associations between social involvement and substance use such that the more popular an adolescent is among peers, the greater the likelihood of substance use (Ali et al., 2014; Moody et al., 2011). While social involvement during adolescence is often a sign of healthy adjustment, it also plays a dual function as a risk factor for deviant behavior. Bandura’s social learning theory (Bandura & McClelland, 1977) offers some explanation for a positive link between social involvement and substance use among adolescents, as it emphasizes that the social environment has the potential to affect behavior through modeling. If adolescents observe their peers showing favorable attitudes towards substance use or engaging in substance use, then they are more likely to take part in such behaviors themselves (Trucco, 2020). Peer socialization may be responsible for social learning of substance use, in that affiliation with delinquent or substance-using peers amplifies substance use in adolescence and young adulthood (Otten et al., 2017; Van Ryzin et al., 2012). In particular, Allen et al. (2005) provided evidence supporting a popularity-socialization hypothesis demonstrating that popular adolescents exhibit behavior that adheres to peer norms, resulting in increased substance use behaviors. Further, socially involved adolescents may have easier access to substances because they engage in social situations and peer interactions more frequently. Indeed, a primary source through which adolescents obtain alcohol is social resources, such as a friend or older sibling of legal age (Friese et al., 2013). Taken together, socially involved adolescents may be subject to social influences such as peer modeling and increased access to alcohol, explaining the greater prevalence of alcohol use among socially involved youth.
Social Alienation and Substance Use
Though socially involved adolescents are more likely to engage in substance use, somewhat ironically, the same also rings true for socially alienated adolescents. That is, adolescents who experience alienation from their peers have been found to engage in higher levels of substance use (Copeland et al., 2018). A possible explanation for this association could be the use of substances as a coping mechanism for social relationships that induce negative affect, such as loneliness (Skrzynski & Creswell, 2020). Loneliness is an emotional experience, characterized by sadness or dejection due to lack of companionship, which is especially salient during adolescence and young adulthood due to the rapid social changes that define this period. Indeed, prior research suggests that social isolation is associated with self-medication to cope with feelings of loneliness (Osgood et al., 2014). Neuroimaging research provides further insights into the association between emotional pain derived from negative social relationships and the use of substances for self-medication by demonstrating a shared activation in the brain between physical and social pain. Specifically, the dorsal anterior cingulate cortex and the anterior insula, areas of the brain that respond to physical pain, were activated during a computer game that simulated social rejection (Eisenberger et al., 2003, Eisenberger, 2012), demonstrating that pain stemming from social relationships stimulated the same regions of the brain as physical pain, thus supporting the notion that substances may be used as a form of self-medication against the pain of social alienation.
Indeed, research suggests that substance use may be a form of self-medication for those whose alienation is associated with mental health concerns. For example, social anxiety and depression have been shown to be both predictors (Biggs et al., 2012; Maughan et al., 2013) and outcomes (Katz et al., 2012; Tillfors et al., 2012) of social alienation. In turn, cross-sectional studies indicate that young people who experience mental health concerns (such as social anxiety and depression) self-medicate through the use of substances (Lemyre et al., 2019; Tomlinson & Brown, 2012). Taken together, as young people who are socially alienated may experience both feelings of loneliness as well as related mental health problems, they may use substances as a coping mechanism to alleviate these emotional concerns.
Religiousness as a Protective Factor
Given the long-term detrimental effects of substance use during adolescence (Morin et al., 2019), research identifying protective factors that may modify developmental processes underlying this association is crucial. One such factor is religiousness, which has been identified as deterring maladjustment outcomes during adolescence, including substance use (see Holmes & Kim-Spoon, 2016 for a review). Prior research has shown that more religious adolescents are less likely to engage in risk-taking behaviors, such as substance use, risky sexual behaviors, and criminal activity (Kim-Spoon et al., 2015; Pirutinsky, 2014). Theoretically, protective effects of religiousness are in part due to its faciliatory effect on self-regulation (McCullough & Willoughby, 2009). Indeed, research has shown that more religious adolescents show better self-regulation abilities (Kim-Spoon et al., 2014b; Holmes et al., 2019). Further, there is evidence suggesting buffering roles of religiousness against detrimental effects of parental and peer risk factors (i.e., substance-using peers and harsh parenting) on substance use behaviors, in that these behaviors were attenuated among adolescents with higher religiousness compared to those with lower religiousness (Kim-Spoon et al., 2014a; Peviani et al., 2019). However, prior work examining the moderation between religiousness and substance use focused on parental relationships and peer substance use, and this study fills a gap in literature by examining the moderating effect of religiousness on the association between social relationship factors and alcohol use. Here, it is proposed that more religious adolescents may be better prepared to resist social pressures toward substance use (grown out of social involvement) as well as resist self-medication urges to cope with negative affect (grown out of social alienation).
The present study examined potentially differential roles of two distinct dimensions of religiousness: organizational and personal. Organizational religiousness encompasses an adolescent’s involvement in religious institutions (e.g. attending services or youth group) and personal religiousness encompasses the importance of faith to the adolescent’s life. Different theoretical accounts explain why organizational versus personal religiousness would affect negative health behaviors such as substance use. In the reformulated social control theory, Gottfredson and Hirschi (1990) proposed that the root of delinquent behaviors is low self-control, rather than social control. According to this perspective, youth should be taught the rules of their societies by their parents and other adults to understand the full range of the consequences of their behaviors. Thus, strongly religious adolescents are more likely to internalize these rules and values through their relationships with older adults in their religious communities, and thus they are less likely to use substances facing social pressures and social rejections. Further, being an active participant in religion allows young people to define their own personal religiousness, or the personal importance of their faith. The divine interaction theory provides accounts for the beneficial effects of personal religiousness by suggesting that religious people create relationships with the divine similar to how they would form social relationships, seeking out guidance and solace from a divine being in private (Ellison, 1991; Pollner, 1989). It follows that as adolescents and young adults strengthen their personal relationship with the divine, they are expected to receive support from this relationship in a way that helps them to resist social pressures and cope with social rejections so that they are less likely to turn to substance use.
Current Study
The current study used longitudinal prospective data to examine associations between social relationships (i.e., social involvement and social alienation) and alcohol use during adolescence and into young adulthood. Factors promoting resilience towards social relationship risks were considered by testing the protective role of organizational and personal religiousness within this association. Specifically, it is hypothesized that the link between social relationships and alcohol use may be moderated by religiousness, such that the associations between social relationships and subsequent alcohol use will be weaker for those with higher organizational and personal religiousness, even after controlling for the contribution of parent–adolescent relationship quality (a protective factor within a family context) and other demographic covariates.
Methods
Participants
The sample used in the present study consisted of 167 adolescents (53% males) from a southeastern state in the United States of America who participated in five annual assessments across six years (with a two-year gap between Time 4 and Time 5). Adolescents were 13 to 14 years of age at Time 1 (M = 14.07, SD = 0.54 for Time 1, M = 15.05, SD = 0.54 for Time 2, M = 16.07, SD = 0.56 for Time 3, and M = 17.01, SD = 0.55 for Time 4, and M = 18.39, SD = 0.67 for Time 5). About 78% of adolescents identified as Caucasian, 14% African–American, 6% as more than one race, and 2% as other. The median annual family income was in the $35,000–$50,000 range, with varying levels of family economic status (50% “poor/near poor” and 50% “non-poor” according to income-to-needs ratio). At Time 1, 157 families participated. At Time 2, 10 families were added for a final sample of 167 parent–adolescent dyads. However, 24 families (14%) did not participate at all possible time points for reasons including: ineligibility for tasks (n = 2), declined participation (n = 17), and lost contact (n = 5) during the follow-up assessments. Attrition analyses using univariate General Linear Modeling (GLM) were performed to determine the presence of systematic predictors of missing data. Results indicated that rate of participation (indexed by proportion of years participated to years invited to participate) was not significantly predicted by age, income, sex, or race (ps > 0.307).
Procedures
Data included in the present study was collected as part of a larger longitudinal project. Adolescent participants and their primary caregivers were recruited via flyers, email announcements, and snowball sampling (word-of-mouth). Data collection was administered at university offices where participants completed a combination of self-report questionnaires, behavioral and neuroimaging tasks, and interviews by experienced research assistants. The study sessions lasted on average five hours and participants were compensated monetarily for their time. All procedures were approved by the institutional review board of the university and all participants gave written informed consent or assent.
Measures
Social involvement
Social involvement was measured at Times 1–4 via six items that make up the Social Scale of the Youth Self-Report (YSR; Achenbach & Rescorla, 2001). Adolescents reported (1) the names of organizations, teams or other activities they are involved in, (2) their average participation in each of the listed activities compared to others using a three-point scale including “less than average”, “average” and “more than average”, (3) the number of their close friends using a four-point scale including “none”, “1”, “2 or 3”, and “4 or more”, as well as, (4) frequency of contact with friends outside of school, (5) how well they get along with friends, siblings, and parents, and (6) how well they did things alone compared to others using a three point-scale including “worse”, “average”, and “better”. T-scores of the Social Scale each time were used in the analyses. Internal consistency was relatively low (α ranges from 0.43 to 0.52 across Times 1–4 in the current sample) but consistent with what has previously been reported by Achenbach and Rescorla (2001) (α = 0.55). The low reliability may reflect the nature of the variable, which can be seen as an index variable (Streiner, 2003). That is, the variable has multiple indicators that reflect social involvement in different areas. For instance, an adolescent having multiple close friends may not necessarily indicate that he or she would be a member of multiple organizations, yet both clearly fit within the construct of social involvement.
Social Alienation
Social alienation was measured at Times 1- 4 via the Peer Alienation subscale of the Inventory of Parent and Peer Attachment (Armsden & Greenberg, 1987). Adolescents responded to four statements regarding their feelings of alienation from their peers using a five-point Likert scale from “1 = Almost Never or Never True” to “5 = Almost Always or Always True”. Sample items include “My friends don’t understand what I’m going through these days” and “I feel alone or apart when I am with my friends”. The mean score was calculated to create an overall alienation score, such that higher scores indicated greater feelings of alienation (α ranges from 0.60 to 0.72 across Times 1–4; all factor loadings of the confirmatory factor analyses were significant and greater than 0.44).
Religiousness
Religiousness was measured using adolescent self-report on organizational and personal religiousness subscales at Times 1–4 using six items from: the Multidimensional Measure of Religiousness/ Spirituality (Fetzer & NIA, 1999) and Jessor’ s Value on Religion Scale (Jessor & Jessor, 1977). Two subscales of religiousness, organizational and personal, were used. Organizational religiousness was measured by averaging two items reflecting participation in organized religious activities (e.g., how often they attend religious services; α ranges from 0.83 to 0.87 across Times 1–4; all factor loadings of the confirmatory factor analyses were significant and greater than 0.64). Personal religiousness was assessed by averaging four items indicating the importance of religious faith (e.g., how important they think it is “to believe in God”; α ranges from 0.69 to 0.74 across Times 1–4, all factor loadings of the confirmatory factor analyses were significant and greater than 0.88).
Alcohol use
Alcohol use was measured at Times 1–5 with a question asking a typical frequency: “Which is most true for you about using alcohol?” using a 6-point Likert scale ranging from “1 = never used” to “6 = usually use every day” (α = 0.70 at Time 5).
Sex
At Time 1, adolescents completed a demographic interview which included a question asking for their biological sex, with 0 representing male and 1 representing female.
Race
At Time 1, adolescents completed a demographic interview which included a question asking for their race. This variable was then dummy coded into 0 representing White and 1 representing Non-White.
Income-to-needs ratio
At Time 1, caregivers completed a demographic interview which included questions about their and their spouse’s (if applicable) income. Total household income before taxes for the previous year was used to calculate an income-to-needs (ITN) ratio for each family. Specifically, income was divided by the poverty threshold for the given family size (according to guidelines by the U.S. Census Bureau).
Parent–adolescent relationship quality
Parent–adolescent relationship quality was added as a covariate in the models. Parent–adolescent relationship quality was measured using adolescent self-report via the mean of Parent subscale of the Inventory of Parent and Peer Attachment (Armsden & Greenberg, 1987). Adolescents responded to 12 items each regarding their feelings of attachment to both their mother and father using a five-point Likert scale from “1 = Almost Never or Never True” to “5 = Almost Always or Always True”. Sample items include “My mother/father helps me understand myself better” and “I wish I had a different mother/father”. The mean of the mother and father attachment scores was taken to represent overall parent-adolescent relationship quality at each time point, and the grand mean was calculated across Time 1–4, such that higher scores indicate a more supportive relationship (mean α for mother across Times 1–4 = 0.86; mean α for father across Times 1–4 = 0.88).
Data Analytic Plan
For all variables, descriptive statistics were used to assess for outliers and normal distributions. Skewness and kurtosis were also examined, and levels less than 3 and 10, respectively, were considered acceptable (Kline, 2011). All study variables demonstrated acceptable levels of skewness and kurtosis. Outliers (N = 6) were identified as values deviating more than 3.29 SD from the mean and were Winsorized to retain statistical power and attenuate bias resulting from elimination.
Latent Change Score (LCS) Modeling (McArdle & Hamagami, 2001) using Structural Equation Modeling (SEM) in Mplus statistical software version 8 (Muthén & Muthén, 1998–2018) was used to predict dynamic changes in alcohol use from repeatedly measured social relationships. One clear advantage of the LCS model was to estimate time-based dynamic relations, where the effect on change in one variable (i.e., alcohol use) depends on the state of another variable (i.e., social relationship) as well as any prior change within the system over time (i.e., proportional change which cannot be represented by other longitudinal models such as multivariate growth curve models). Additionally, the LCS model represents changes in perfectly reliable scores over a time series by partitioning true scores from measurement error, reducing the likelihood of biased change parameters while enhancing power. The hypothesized LCS model included the time-varying predictor of social relationship to examine how earlier social involvement and social alienation would predict subsequent changes in alcohol use. Further, whether religiousness moderates the associations between social acceptance and social alienation at Times 1–4 and alcohol use at Times 1–5 was tested by using a two-group SEM with the low and high religiousness groups (n = 85 low, n = 82 high for organizational religiousness, n = 84 low, n = 83 high for personal religiousness, defined by a median split). A grand mean of the religiousness variables (average of Times 1–4) was used to capture longitudinal levels of religiousness (moderator) to create high versus low religiousness groups, separately for organizational and personal religiousness.
Model fit was assessed by χ2 value, degrees of freedom, corresponding p-value, Root Mean Square Error of Approximation (RMSEA), and Confirmatory Fit Index (CFI). For RMSEAs, values less than 0.05 and 0.08 were taken to reflect good and acceptable fits, respectively; and the CFI values greater than 0.90 and 0.95 were taken to reflect acceptable and good fits, respectively (Little, 2013). Full Information Maximum Likelihood (FIML) estimation with robust standard errors (MLR) was used as it is known to account for missing data (three scores of substance use were missing) and non-normal distributions better than maximum likelihood (ML) estimation.
Results
Descriptive statistics and correlations for study variables are presented in Table 1. In the hypothesized LCS models, associations between social involvement/alienation and alcohol use were tested by estimating the effects of social relationships from Time 1 through Time 4 (manifest variables representing time series data) on changes in alcohol use from Time 1 through Time 5, separately for social involvement and social alienation (see Fig. 1 for conceptual model).
Table 1.
Descriptive statistics and bivariate correlations for social involvement, social alienation, alcohol use, organizational religiousness, and personal religiousness
| M | SD | Min | Max | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. SI Time 1 | 47.03 | 9.00 | 25.00 | 65.00 | |||||||||||||||||||
| 2. SI Time 2 | 48.37 | 8.77 | 28.00 | 65.00 | 0.39* | ||||||||||||||||||
| 3. SI Time 3 | 49.05 | 9.08 | 29.00 | 65.00 | 0.34* | 0.62* | |||||||||||||||||
| 4. SI Time 4 | 48.51 | 9.06 | 28.00 | 65.00 | 0.33* | 0.45* | 0.52* | ||||||||||||||||
| 5. SA Time 1 | 4.17 | 0.64 | 2.25 | 5.00 | −0.07 | 0.08 | 0.03 | 0.14 | |||||||||||||||
| 6. SA Time 2 | 4.09 | 0.72 | 1.75 | 5.00 | .04 | 0.08 | −0.01 | 0.11 | 0.49* | ||||||||||||||
| 7. SA Time 3 | 4.05 | 0.62 | 2.25 | 5.00 | 0.14 | 0.14 | −0.03 | 0.10 | 0.49* | 0.59* | |||||||||||||
| 8. SA Time 4 | 4.10 | 0.65 | 2.50 | 5.00 | 0.11 | 0.15 | −0.06 | 0.06 | 0.44* | 0.49* | 0.56* | ||||||||||||
| 9. AL Time 1 | 1.38 | 0.58 | 1.00 | 3.00 | −0.08 | 0.01 | −0.06 | −0.18* | −0.08 | −0.16 | −0.12 | 0.01 | |||||||||||
| 10. AL Time 2 | 1.58 | 0.87 | 1.00 | 4.00 | −0.05 | 0.06 | 0.05 | −0.11 | 0.05 | −0.03 | −0.06 | −0.07 | 0.58* | ||||||||||
| 11. AL Time 3 | 1.91 | 1.02 | 1.00 | 4.00 | −0.02 | 0.02 | 0.05 | −0.05 | −0.08 | −0.09 | −0.08 | −0.10 | 0.51* | 0.66* | |||||||||
| 12. AL Time 4 | 2.32 | 1.06 | 1.00 | 4.00 | −0.01 | 0.01 | 0.05 | −0.07 | 0.03 | 0.08 | 0.00 | 0.00 | 0.42* | 0.59* | 0.72* | ||||||||
| 13. AL Time 5 | 3.02 | 1.12 | 1.00 | 5.00 | 0.06 | 0.18* | 0.22* | 0.02 | −0.01 | 0.08 | −0.02 | 0.20* | 0.24* | 0.41* | 0.48* | 0.60* | |||||||
| 14. OR GM | 5.23 | 2.00 | 1.20 | 9.00 | 0.20* | 0.10 | 0.14 | 0.07 | −0.02 | 0.13 | 0.01 | 0.10 | −0.21* | −0.21* | −0.17* | −0.23* | −0.15 | ||||||
| 15. PR GM | 2.62 | 0.70 | 1.43 | 3.53 | 0.14 | 0.10 | 0.09 | 0.02 | 0.05 | 0.10 | 0.00 | 0.09 | −0.05 | −0.09 | −0.06 | −0.09 | −0.15 | 0.78* | |||||
| 16. Sex | 0.47 | 0.50 | 0.00 | 1.00 | 0.07 | −0.09 | 0.11 | 0.09 | −0.15 | −0.16* | −0.22* | −0.22* | −0.08 | −0.03 | 0.03 | 0.06 | −0.03 | 0.03 | 0.09 | ||||
| 17. Race | 0.22 | 0.41 | 0.00 | 1.00 | 0.09 | 0.02 | −0.01 | 0.07 | 0.09 | 0.04 | 0.06 | 0.09 | 0.03 | 0.06 | 0.06 | 0.13 | −0.08 | −0.01 | 0.08 | 0.06 | |||
| 18. ITN Ratio | 2.49 | 1.89 | 0.00 | 8.39 | 0.02 | 0.06 | 0.16 | 0.16 | −0.16* | −0.09 | −0.04 | 0.06 | −0.04 | −0.08 | 0.01 | 0.07 | 0.03 | −0.14 | −0.21* | −0.02 | −0.20* | ||
| 19. PAR | 3.86 | 0.53 | 2.22 | 4.86 | 0.03 | 0.05 | 0.09 | 0.20* | 0.26* | 0.32* | 0.33* | 0.18* | −0.10 | −0.11 | −0.21* | −0.21* | −0.08 | 0.07 | 0.11 | −0.01 | −0.11 | 0.13 |
SI social involvement, SA social alienation, AL alcohol use, OR organizational religiousness, PR personal religiousness, GM grand mean, ITN income-to-needs, PAR parent–adolescent relationship quality.
p < 0.05.
Fig. 1.
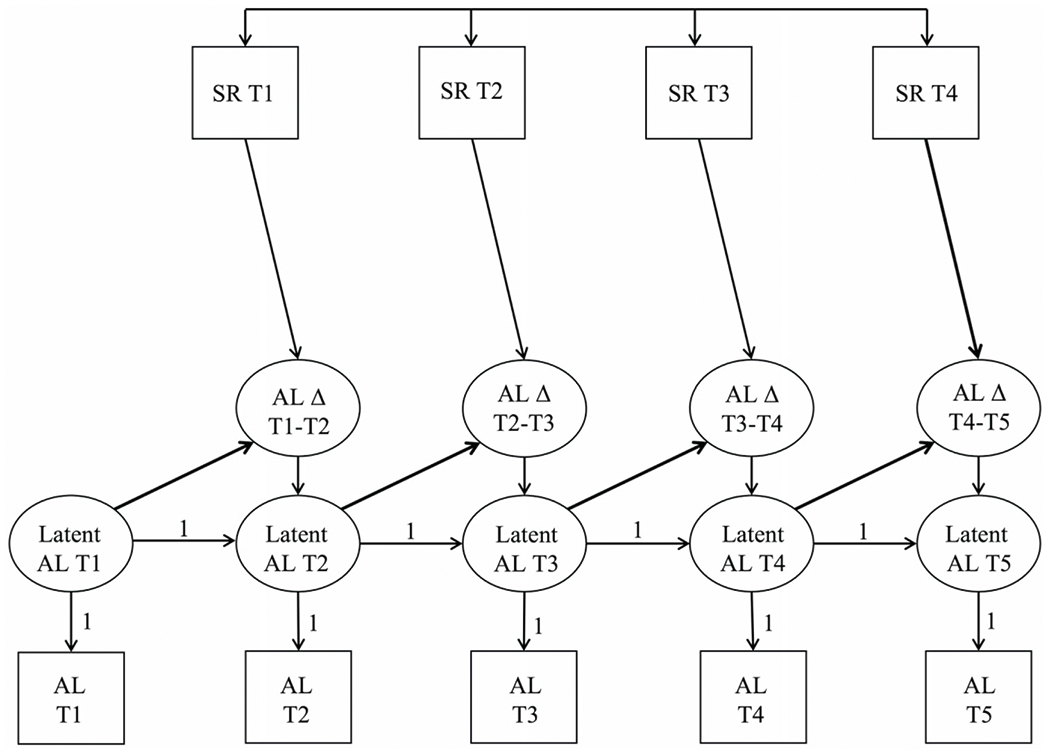
Latent Change Score Model of the Moderation of Religiousness between Social Relationships and Alcohol Use. Note. SR = social relationship; AL = alcohol use; T1 = Time 1 (age 14); T2 = Time 2 (age 15); T3 = Time 3 (age 16); T4 = Time 4 (age 17); T5 = Time 5 (age 18). Demographic variables sex, race, income, and parent-adolescent relationship quality are included but not depicted in conceptual model for clarity of presentation
Univariate Latent Change Score Modeling of Alcohol Use
The univariate LCS model of alcohol use change did not display acceptable model fit (χ2 = 19.53, df = 5, p < 0.001, RMSEA = 0.13, CFI = 0.94). To further improve the model fit based on modification indices, a residual correlation between alcohol use Time 2 and Time 4, was added, and the variances of alcohol use Time 1 and Time 5 were fixed to 0 to account for small, nonsignificant negative residual variances. The resulting model fit was good (χ2 = 5.12, df = 6, p = 0.528, RMSEA = 0.00, CFI = 1.00). The mean (M = 1.38, SE = 0.05, p < 0.001) and variance (σ2 = 0.34, SE = 0.04, p < 0.001) of the intercept factor were significant. Further, proportional changes were positive and significant (b = 0.42, SE = 0.13, p = 0.001), indicating that higher alcohol use at an earlier time point predicted subsequent increases in alcohol use. Next, a two-group univariate LCS models of alcohol use was tested.
The two-group LCS model of alcohol use by organizational religiousness demonstrated good fit (χ2 = 10.20, df = 12, p = 0.598, RMSEA = 0.00, CFI = 1.00). In both the low and high groups, the means (M = 1.43, SE = 0.06, p < 0.001 for the low group; M = 1.25, SE = 0.05, p < 0.001 for the high group) and variances (σ2 = 0.32, SE = 0.05, p < 0.001 for the low group; σ2 = 0.22, SE = 0.04, p < 0.001 for the high group) of the intercept factor were significant. Further, proportional changes were positive and significant in the high group (b = 0.64, SE = 0.23, p = 0.005), but not significant in the low group (b = 0.21, SE = 0.14, p = 0.138).
The two-group LCS model of alcohol use by personal religiousness demonstrated good fit (χ2 = 11.15, df = 12, p = 0.516, RMSEA = 0.00, CFI = 1.00). In both the low and high groups, the means (M = 1.43, SE = 0.06, p < 0.001 for the low group; M = 1.33, SE = 0.07, p < 0.001 for the high group) and variances (σ2 = 0.32, SE = 0.05, p < 0.001 for the low group; σ2 = 0.35, SE = 0.07, p < 0.001 for the high group) of the intercept factor were significant. Further, proportional changes were positive and significant in both the low group (b = 0.41, SE = 0.18, p = 0.022) and the high group (b = 0.50, SE = 0.19, p = 0.009).
Longitudinal Associations of Social Involvement and Social Alienation with Alcohol Use Moderated by Religiousness
Next, the hypothesis that religiousness plays a protective role against the detrimental effects of social relationship risk factors on alcohol use was tested using a two-group SEM based on the high vs. low religious groups. Specifically, religiousness was tested as a moderator for longitudinal associations between social relationships (social involvement and social alienation) and alcohol use for a total of four models. In order to test possible covariates, adolescent sex (0 = male, 1 = female) and race (0 = white and 1 = non-white), income-to-needs ratio, and parent-adolescent relationship quality were added to all four moderation models.
Organizational Religiousness as a Moderator
The two-group LCS models of the moderation of organizational religiousness between social involvement and alcohol use change displayed acceptable fit (χ2 = 83.09, df = 64, p = 0.055, RMSEA = 0.06, CFI = 0.94). As shown in Table 2, there were no significant associations between social involvement nor covariates and change in alcohol use.
Table 2.
Latent change score model of the moderation of organizational religiousness between social relationships and alcohol use
| Parameter | Social Involvement |
Social Alienation |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Religiousness |
High Religiousness |
Low Religiousness |
High Religiousness |
|||||||||
| Est. | SE | p | Est. | SE | p | Est. | SE | p | Est. | SE | p | |
| Regression Effects | ||||||||||||
| SR T1 → AL Δ T1-T2 | 0.01 | 0.01 | 0.175 | −0.01 | 0.01 | 0.191 | −0.03 | 0.12 | 0.823 | 0.04 | 0.11 | 0.757 |
| SR T2 → AL Δ T2-T3 | 0.01 | 0.01 | 0.544 | 0.01 | 0.01 | 0.109 | 0.22* | 0.09 | 0.019 | 0.09 | 0.11 | 0.416 |
| SR T3 → AL Δ T3-T4 | 0.00 | 0.01 | 0.857 | 0.00 | 0.01 | 0.968 | 0.08 | 0.16 | 0.606 | −0.08 | 0.15 | 0.611 |
| SR T4 → AL Δ T4-T5 | 0.01 | 0.01 | 0.526 | −0.01 | 0.01 | 0.667 | 0.33* | 0.13 | 0.010 | −0.16 | 0.18 | 0.369 |
| SEX T1 → AL Δ T1-T2 | 0.01 | 0.19 | 0.955 | 0.06 | 0.15 | 0.692 | 0.03 | 0.19 | 0.875 | 0.05 | 0.15 | 0.720 |
| SEX T2 → AL Δ T2-T3 | 0.21 | 0.24 | 0.375 | 0.00 | 0.19 | 0.985 | 0.27 | 0.22 | 0.226 | 0.02 | 0.20 | 0.933 |
| SEX T3 → AL Δ T3-T4 | −0.11 | 0.23 | 0.623 | 0.05 | 0.21 | 0.809 | −0.04 | 0.22 | 0.868 | 0.03 | 0.23 | 0.912 |
| SEX T4 → AL Δ T4-T5 | −0.37 | 0.25 | 0.131 | 0.18 | 0.28 | 0.520 | −0.26 | 0.23 | 0.251 | 0.12 | 0.29 | 0.668 |
| RAC T1 → AL Δ T1-T2 | −0.20 | 0.22 | 0.341 | 0.26 | 0.20 | 0.183 | −0.17 | 0.22 | 0.430 | 0.18 | 0.20 | 0.367 |
| RAC T2 → AL Δ T2-T3 | 0.42 | 0.27 | 0.125 | −0.27 | 0.20 | 0.171 | 0.33 | 0.25 | 0.188 | −0.22 | 0.23 | 0.337 |
| RAC T3 → AL Δ T3-T4 | −0.02 | 0.30 | 0.955 | 0.12 | 0.32 | 0.702 | 0.02 | 0.26 | 0.951 | 0.14 | 0.35 | 0.696 |
| RAC T4 → AL Δ T4-T5 | −0.54 | 0.35 | 0.123 | −0.50 | 0.44 | 0.261 | −0.61 | 0.34 | 0.068 | −0.51 | 0.46 | 0.258 |
| ITN T1 → AL Δ T1-T2 | −0.04 | 0.04 | 0.414 | −0.04 | 0.03 | 0.185 | −0.03 | 0.05 | 0.471 | −0.04 | 0.03 | 0.149 |
| ITN T2 → AL Δ T2-T3 | 0.05 | 0.05 | 0.328 | 0.09 | 0.05 | 0.063 | 0.06 | 0.05 | 0.223 | 0.01* | 0.05 | 0.045 |
| ITN T3 → AL Δ T3-T4 | 0.02 | 0.05 | 0.619 | 0.04 | 0.06 | 0.544 | 0.03 | 0.04 | 0.503 | 0.03 | 0.06 | 0.618 |
| ITN T4 → AL Δ T4-T5 | −0.02 | 0.07 | 0.775 | −0.16 | 0.09 | 0.061 | −0.02 | 0.07 | 0.779 | −0.17 | 0.09 | 0.059 |
| PAR T1 → AL Δ T1-T2 | −0.02 | 0.10 | 0.830 | 0.09 | 0.09 | 0.322 | 0.10 | 0.13 | 0.438 | −0.06 | 0.13 | 0.683 |
| PAR T2 → AL Δ T2-T3 | −0.11 | 0.12 | 0.352 | −0.21 | 0.11 | 0.062 | −0.28* | 0.12 | 0.024 | −0.16 | 0.10 | 0.123 |
| PAR T3 → AL Δ T3-T4 | 0.03 | 0.11 | 0.799 | −0.05 | 0.13 | 0.711 | −0.04 | 0.17 | 0.831 | 0.03 | 0.17 | 0.886 |
| PAR T4 → AL Δ T4-T5 | 0.02 | 0.14 | 0.915 | 0.26 | 0.16 | 0.107 | −0.21 | 0.13 | 0.093 | 0.36* | 0.18 | 0.050 |
| Proportional Effects | ||||||||||||
| AL T1 → AL Δ T1-T2 | 0.33 | 0.26 | 0.203 | 0.26 | 0.24 | 0.277 | 0.12 | 0.23 | 0.608 | 0.39 | 0.31 | 0.209 |
| AL T2 → AL Δ T2-T3 | 0.33 | 0.26 | 0.203 | 0.26 | 0.24 | 0.277 | 0.12 | 0.23 | 0.608 | 0.39 | 0.31 | 0.209 |
| AL T3 → AL Δ T3-T4 | 0.33 | 0.26 | 0.203 | 0.26 | 0.24 | 0.277 | 0.12 | 0.23 | 0.608 | 0.39 | 0.31 | 0.209 |
| AL T4 → AL Δ T4-T5 | 0.33 | 0.26 | 0.203 | 0.26 | 0.24 | 0.277 | 0.12 | 0.23 | 0.608 | 0.39 | 0.31 | 0.209 |
| Latent Change Score Mean | ||||||||||||
| AL Δ T1–T2 | 44.90* | 1.04 | 0.000 | 49.23* | 0.93 | 0.000 | 4.20* | 0.08 | 0.000 | 4.14* | 0.07 | 0.000 |
| AL Δ T2–T3 | 46.67* | 0.99 | 0.000 | 49.63* | 0.99 | 0.000 | 4.00* | 0.09 | 0.000 | 4.17* | 0.07 | 0.000 |
| AL Δ T3–T4 | 47.36* | 1.08 | 0.000 | 50.10* | 0.99 | 0.000 | 4.07* | 0.07 | 0.000 | 4.04* | 0.07 | 0.000 |
| AL Δ T4–T5 | 48.12* | 1.02 | 0.000 | 48.60* | 1.81 | 0.000 | 4.05* | 0.08 | 0.000 | 4.15* | 0.07 | 0.000 |
| Latent Change Score Variance | ||||||||||||
| AL Δ T1–T2 | 84.08* | 11.14 | 0.000 | 68.11* | 9.35 | 0.000 | 0.47* | 0.08 | 0.000 | 0.37* | 0.05 | 0.000 |
| AL Δ T2–T3 | 76.19* | 10.96 | 0.000 | 74.35* | 10.82 | 0.000 | 0.61* | 0.11 | 0.000 | 0.41* | 0.08 | 0.000 |
| AL Δ T3–T4 | 87.61* | 11.98 | 0.000 | 72.26* | 10.43 | 0.000 | 0.40* | 0.07 | 0.000 | 0.37* | 0.05 | 0.000 |
| AL Δ T4–T5 | 78.24* | 11.76 | 0.000 | 83.44* | 11.62 | 0.000 | 0.48* | 0.07 | 0.000 | 0.36* | 0.06 | 0.000 |
SR social relationship, AL alcohol use, RAC race, ITN income-to-needs ratio, PAR parent–adolescent relationship quality, T1 Time 1 (age 14), T2 Time 2 (age 15); T3 Time 3 (age 16); T4 Time 4 (age 17); T5 Time 5 (age 18). Est. unstandardized parameter estimate, SE standard error.
p < 0.05.
The two-group LCS models of the moderation of organizational religiousness between social alienation and alcohol use change displayed acceptable fit (χ2 = 65.35, df = 64, p = 0.430, RMSEA = 0.02, CFI = 1.00). As can be seen in Table 2, adolescents with low organizational religiousness demonstrated a significant positive association between social alienation at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3, and a significant positive association between social alienation at Time 4 and the subsequent change in alcohol use from Time 4 to Time 5 indicating that high social alienation was associated with greater increases in alcohol use. Significant group differences were found for Time 4 social alienation effects on alcohol use change from Time 4 to Time 5 (Wald test χ2 = 5.00, df = 1, p = 0.025). However, testing numerical invariance for the significant social alienation effects between the two groups did not indicate significant group differences for Time 2 social alienation effects (Wald test χ2 = 0.81, df = 1, p = 0.369).
In the social alienation model, some effects of family income and parent-adolescent relationship quality were found (see Table 2). In the low religiousness group, there was a significant negative association between parent-adolescent relationship quality at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3, indicating that lower relationship quality was associated with greater increases in alcohol use. In the high religiousness group, there was a significant positive association between income-to-needs ratio at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3, indicating that higher family income was associated with greater increases in alcohol use. In addition, there was a significant positive association between parent-adolescent relationship quality at Time 4 and the subsequent change in alcohol use from Time 4 to Time 5, indicating that higher parent-adolescent relationship quality was associated with greater changes in alcohol use. Thus, the data indicated differential effects of the parent-adolescent relationship quality between low and high religiousness groups.
Personal Religiousness as a Moderator
The two-group LCS of the moderation of personal religiousness between social involvement and alcohol use change displayed acceptable fit (χ2 = 88.83, df = 63, p = 0.018, RMSEA = 0.07, CFI = 0.92). As can be seen in Table 3, there were no significant associations between social involvement and change in alcohol use.
Table 3.
Latent change score model of the moderation of personal religiousness between social relationships and alcohol use
| Parameter | Social Involvement |
Social Alienation |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Religiousness |
High Religiousness |
Low Religiousness |
High Religiousness |
|||||||||
| Est. | SE | p | Est. | SE | p | Est. | SE | p | Est. | SE | p | |
| Regression Effects | ||||||||||||
| SR T1 → AL Δ T1-T2 | 0.00 | 0.01 | 0.467 | −0.01 | 0.01 | 0.254 | 0.00 | 0.12 | 0.985 | 0.08 | 0.09 | 0.387 |
| SR T2 → AL Δ T2-T3 | 0.01 | 0.01 | 0.162 | 0.01 | 0.01 | 0.362 | 0.17* | 0.08 | 0.036 | 0.07 | 0.10 | 0.484 |
| SR T3 → AL Δ T3-T4 | 0.01 | 0.01 | 0.341 | 0.00 | 0.01 | 0.987 | 0.14 | 0.19 | 0.455 | −0.02 | 0.14 | 0.911 |
| SR T4 → AL Δ T4-T5 | 0.01 | 0.01 | 0.437 | −0.01 | 0.02 | 0.739 | 0.30* | 0.14 | 0.037 | −0.01 | 0.16 | 0.950 |
| SEX T1 → AL Δ T1-T2 | 0.18 | 0.20 | 0.367 | −0.09 | 0.13 | 0.504 | 0.18 | 0.21 | 0.385 | −0.11 | 0.14 | 0.438 |
| SEX T2 → AL Δ T2-T3 | 0.06 | 0.24 | 0.808 | 0.15 | 0.21 | 0.461 | 0.12 | 0.22 | 0.591 | 0.15 | 0.20 | 0.441 |
| SEX T3 → AL Δ T3-T4 | −0.25 | 0.24 | 0.296 | 0.13 | 0.26 | 0.620 | −0.11 | 0.24 | 0.656 | 0.13 | 0.24 | 0.577 |
| SEX T4 → AL Δ T4-T5 | −0.14 | 0.30 | 0.640 | −0.07 | 0.32 | 0.822 | 0.03 | 0.27 | 0.899 | −0.07 | 0.28 | 0.810 |
| RAC T1 → AL Δ T1-T2 | −0.19 | 0.23 | 0.404 | 0.27 | 0.20 | 0.180 | −0.21 | 0.23 | 0.362 | 0.19 | 0.19 | 0.335 |
| RAC T2 → AL Δ T2-T3 | 0.23 | 0.31 | 0.458 | −0.08 | 0.24 | 0.738 | 0.13 | 0.30 | 0.662 | 0.02 | 0.24 | 0.930 |
| RAC T3 → AL Δ T3-T4 | 0.17 | 0.32 | 0.596 | −0.10 | 0.40 | 0.810 | 0.16 | 0.28 | 0.554 | −0.02 | 0.34 | 0.952 |
| RAC T4 → AL Δ T4-T5 | −0.42 | 0.46 | 0.361 | −0.76 | 0.44 | 0.085 | −0.43 | 0.43 | 0.313 | −0.67 | 0.40 | 0.091 |
| ITN T1 → AL Δ T1-T2 | −0.05 | 0.05 | 0.339 | −0.02 | 0.03 | 0.456 | −0.05 | 0.05 | 0.331 | −0.02 | 0.03 | 0.423 |
| ITN T2 → AL Δ T2-T3 | 0.06 | 0.05 | 0.237 | 0.12* | 0.05 | 0.021 | 0.06 | 0.04 | 0.184 | 0.12* | 0.05 | 0.014 |
| ITN T3 → AL Δ T3-T4 | 0.01 | 0.05 | 0.927 | 0.02 | 0.07 | 0.766 | 0.02 | 0.05 | 0.624 | 0.03 | 0.06 | 0.590 |
| ITN T4 → AL Δ T4-T5 | −0.02 | 0.07 | 0.739 | −0.19 | 0.10 | 0.052 | −0.03 | 0.07 | 0.675 | −0.15 | 0.09 | 0.097 |
| PAR T1 → AL Δ T1-T2 | 0.04 | 0.09 | 0.676 | 0.06 | 0.07 | 0.414 | 0.08 | 0.14 | 0.594 | −0.07 | 0.10 | 0.510 |
| PAR T2 → AL Δ T2-T3 | −0.17 | 0.10 | 0.107 | −0.16 | 0.11 | 0.130 | −0.22* | 0.10 | 0.034 | −0.13 | 0.10 | 0.221 |
| PAR T3 → AL Δ T3-T4 | −0.04 | 0.12 | 0.765 | −0.06 | 0.15 | 0.680 | −0.10 | 0.20 | 0.629 | −0.02 | 0.15 | 0.903 |
| PAR T4 → AL Δ T4-T5 | 0.00 | 0.14 | 0.996 | 0.22 | 0.17 | 0.217 | −0.18 | 0.15 | 0.250 | 0.18 | 0.16 | 0.259 |
| Proportional Effects | ||||||||||||
| AL T1 → AL Δ T1-T2 | 0.46 | 0.35 | 0.187 | 0.51 | 0.36 | 0.160 | 0.23 | 0.30 | 0.436 | 0.38 | 0.26 | 0.140 |
| AL T2 → AL Δ T2-T3 | 0.46 | 0.35 | 0.187 | 0.51 | 0.36 | 0.160 | 0.23 | 0.30 | 0.436 | 0.38 | 0.26 | 0.140 |
| AL T3 → AL Δ T3-T4 | 0.46 | 0.35 | 0.187 | 0.51 | 0.36 | 0.160 | 0.23 | 0.30 | 0.436 | 0.38 | 0.26 | 0.140 |
| AL T4 → AL Δ T4-T5 | 0.46 | 0.35 | 0.187 | 0.51 | 0.36 | 0.160 | 0.23 | 0.30 | 0.436 | 0.38 | 0.26 | 0.140 |
| Latent Change Score Mean | ||||||||||||
| AL Δ T1–T2 | 46.40* | 0.97 | 0.000 | 47.88* | 1.05 | 0.000 | 4.14* | 0.08 | 0.000 | 4.18* | 0.07 | 0.000 |
| AL Δ T2–T3 | 47.88* | 0.99 | 0.000 | 48.34* | 1.01 | 0.000 | 4.01* | 0.09 | 0.000 | 4.17* | 0.07 | 0.000 |
| AL Δ T3–T4 | 48.09* | 1.05 | 0.000 | 49.23* | 1.03 | 0.000 | 4.06* | 0.07 | 0.000 | 4.05* | 0.07 | 0.000 |
| AL Δ T4–T5 | 47.71* | 1.10 | 0.000 | 48.96* | 0.97 | 0.000 | 4.06* | 0.08 | 0.000 | 4.15* | 0.07 | 0.000 |
| Latent Change Score Variance | ||||||||||||
| AL Δ T1–T2 | 76.56* | 10.47 | 0.000 | 84.05* | 11.71 | 0.000 | 0.46* | 0.08 | 0.000 | 0.41* | 0.06 | 0.000 |
| AL Δ T2–T3 | 78.62* | 12.77 | 0.000 | 79.02* | 10.31 | 0.000 | 0.61* | 0.12 | 0.000 | 0.41* | 0.08 | 0.000 |
| AL Δ T3–T4 | 84.84* | 11.68 | 0.000 | 77.74* | 11.03 | 0.000 | 0.42* | 0.08 | 0.000 | 0.36* | 0.05 | 0.000 |
| AL Δ T4–T5 | 90.87* | 12.50 | 0.000 | 67.14* | 9.48 | 0.000 | 0.47* | 0.07 | 0.000 | 0.36* | 0.06 | 0.000 |
SR social relationship, AL alcohol use, RAC race, ITN income-to-needs ratio, PAR parent–adolescent relationship quality, T1 Time 1 (age 14), T2 Time 2 (age 15), T3 Time 3 (age 16); T4 Time 4 (age 17); T5 Time 5 (age 18). Est. unstandardized parameter estimate, SE standard error.
p < 0.05.
The two-group LCS of the moderation of personal religiousness between social alienation and alcohol use change displayed acceptable fit (χ2 = 81.90, df = 62, p = 0.046, RMSEA = 0.06, CFI = 0.94). As can be seen in Table 3, adolescents with low personal religiousness demonstrated a significant positive association between social alienation at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3, and a significant positive association between social alienation at Time 4 and the subsequent change in alcohol use from Time 4 to Time 5 indicating that high social alienation was associated with greater increases in alcohol use. However, testing numerical invariance indicated non-significant group differences for Time 2 (Wald test χ2 = 0.581, df = 1, p = 0.446) or Time 4 (Wald test χ2 = 2.208, df = 1, p = 0.154) social alienation effects, thus these results should be interpreted with caution.
As can be seen in Table 3, in both the social involvement and the social alienation models, there was a significant positive association between income-to-needs ratio at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3 in the high personal religiousness group, indicating that higher income was associated with greater increases in alcohol use. Additionally, in the social alienation model, there was a significant negative association between parent–adolescent relationship quality at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3 in the low religiousness group, indicating that lower relationship quality was associated with greater increases in alcohol use.
Sensitivity Analyses
An alternative approach was taken to examine the robustness of the findings. In contrast to a median split as used in the primary analysis, the data were split by level of religiousness by contrasting the lowest 25% of religiousness (n = 40 for organizational religiousness; n = 42 for personal religiousness) against the remaining 75% (n = 127 for organizational religiousness; n = 125 for personal religiousness) to evaluate whether the buffering effects of religiousness are beneficial to most people while leaving those with notably low levels of religiousness particularly vulnerable to increasing use of alcohol. Results of these analyses are presented in Appendix A.
First, for organizational religiousness, the two-group LCS of social involvement and alcohol use change displayed acceptable fit (χ2 = 95.64, df = 64, p = 0.006, RMSEA = 0.08, CFI = 0.90). As can be seen in Table 4, consistent with the two-group LCS based on the median split, there were no significant associations between social involvement and change in alcohol use. The two-group LCS of the moderation of organizational religiousness between social alienation and alcohol use change displayed acceptable fit (χ2 = 96.49, df = 64, p = 0.005, RMSEA = 0.08, CFI = 0.89), and findings were consistent with the two-group LCS based on the median split. Specifically, as can be seen in Table 4, adolescents with low organizational religiousness demonstrated a significant positive association between social alienation at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3, and a marginally significant association between social alienation at Time 4 and alcohol use change from Time 4 to Time 5.
Table 4.
Latent change score model of the moderation of organizational religiousness (Lowest 25% vs. Others) between social relationships and alcohol use
| Parameter | Social Involvement |
Social Alienation |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Religiousness |
High Religiousness |
Low Religiousness |
High Religiousness |
|||||||||
| Est. | SE | p | Est. | SE | p | Est. | SE | p | Est. | SE | p | |
| Regression Effects | ||||||||||||
| SR T1 → AL Δ T1-T2 | 0.01 | 0.01 | 0.548 | 0.00 | 0.01 | 0.623 | 0.04 | 0.21 | 0.865 | 0.02 | 0.07 | 0.767 |
| SR T2 → AL Δ T2-T3 | 0.01 | 0.01 | 0.527 | 0.01 | 0.01 | 0.294 | 0.36* | 0.17 | 0.032 | 0.10 | 0.08 | 0.162 |
| SR T3 → AL Δ T3-T4 | 0.01 | 0.01 | 0.281 | 0.00 | 0.01 | 0.880 | −0.06 | 0.31 | 0.841 | −0.02 | 0.12 | 0.897 |
| SR T4 → AL Δ T4-T5 | −0.01 | 0.02 | 0.647 | 0.00 | 0.01 | 0.799 | 0.40† | 0.23 | 0.081 | 0.04 | 0.13 | 0.790 |
| SEX T1 → AL Δ T1-T2 | 0.08 | 0.32 | 0.813 | 0.01 | 0.19 | 0.957 | 0.13 | 0.33 | 0.701 | 0.01 | 0.12 | 0.969 |
| SEX T2 → AL Δ T2-T3 | 0.33 | 0.41 | 0.429 | 0.05 | 0.16 | 0.772 | 0.53 | 0.41 | 0.196 | 0.05 | 0.16 | 0.750 |
| SEX T3 → AL Δ T3-T4 | −0.46 | 0.35 | 0.195 | 0.10 | 0.18 | 0.578 | −0.37 | 0.40 | 0.354 | 0.10 | 0.18 | 0.574 |
| SEX T4 → AL Δ T4-T5 | −0.40 | 0.36 | 0.264 | −0.02 | 0.23 | 0.941 | −0.28 | 0.37 | 0.446 | −0.03 | 0.23 | 0.884 |
| RAC T1 → AL Δ T1-T2 | −0.75* | 0.32 | 0.018 | 0.22 | 0.15 | 0.156 | −0.78* | 0.32 | 0.014 | 0.20 | 0.16 | 0.210 |
| RAC T2 → AL Δ T2-T3 | 0.72 | 0.51 | 0.154 | −0.12 | 0.19 | 0.536 | 0.50 | 0.49 | 0.309 | −0.11 | 0.20 | 0.587 |
| RAC T3 → AL Δ T3-T4 | 0.43 | 0.43 | 0.310 | −0.10 | 0.26 | 0.704 | 0.32 | 0.39 | 0.414 | −0.09 | 0.27 | 0.747 |
| RAC T4 → AL Δ T4-T5 | −0.72 | 0.48 | 0.138 | −0.55 | 0.36 | 0.128 | −0.60 | 0.46 | 0.199 | −0.57 | 0.37 | 0.124 |
| ITN T1 → AL Δ T1-T2 | 0.00 | 0.06 | 0.966 | −0.04 | 0.03 | 0.141 | 0.02 | 0.06 | 0.745 | −0.04 | 0.03 | 0.149 |
| ITN T2 → AL Δ T2-T3 | 0.08 | 0.09 | 0.405 | 0.05 | 0.04 | 0.146 | 0.10 | 0.08 | 0.228 | 0.06 | 0.04 | 0.098 |
| ITN T3 → AL Δ T3-T4 | 0.00 | 0.07 | 0.987 | 0.04 | 0.04 | 0.400 | 0.03 | 0.07 | 0.714 | 0.04 | 0.04 | 0.384 |
| ITN T4 → AL Δ T4-T5 | 0.00 | 0.11 | 0.984 | −0.11 | 0.07 | 0.100 | −0.01 | 0.11 | 0.898 | −0.11 | 0.07 | 0.113 |
| PAR T1 → AL Δ T1-T2 | 0.07 | 0.15 | 0.645 | 0.02 | 0.06 | 0.775 | 0.16 | 0.20 | 0.427 | −0.02 | 0.08 | 0.794 |
| PAR T2 → AL Δ T2-T3 | −0.17 | 0.17 | 0.339 | −0.13 | 0.09 | 0.166 | −0.43* | 0.20 | 0.035 | −0.15 | 0.08 | 0.066 |
| PAR T3 → AL Δ T3-T4 | −0.08 | 0.22 | 0.727 | −0.05 | 0.10 | 0.570 | 0.22 | 0.31 | 0.485 | −0.02 | 0.13 | 0.882 |
| PAR T4 → AL Δ T4-T5 | 0.28 | 0.19 | 0.133 | 0.10 | 0.13 | 0.462 | −0.16 | 0.27 | 0.563 | 0.10 | 0.13 | 0.447 |
| Proportional Effects | ||||||||||||
| AL T1 → AL Δ T1-T2 | 0.29 | 0.39 | 0.457 | 0.37 | 0.27 | 0.163 | 0.17 | 0.34 | 0.615 | 0.41 | 0.26 | 0.112 |
| AL T2 → AL Δ T2-T3 | 0.29 | 0.39 | 0.457 | 0.37 | 0.27 | 0.163 | 0.17 | 0.34 | 0.615 | 0.41 | 0.26 | 0.112 |
| AL T3 → AL Δ T3-T4 | 0.29 | 0.39 | 0.457 | 0.37 | 0.27 | 0.163 | 0.17 | 0.34 | 0.615 | 0.41 | 0.26 | 0.112 |
| AL T4 → AL Δ T4-T5 | 0.29 | 0.39 | 0.457 | 0.37 | 0.27 | 0.163 | 0.17 | 0.34 | 0.615 | 0.41 | 0.26 | 0.112 |
| Latent Change Score Mean | ||||||||||||
| AL Δ T1–T2 | 46.30* | 1.46 | 0.000 | 47.42* | 0.83 | 0.000 | 4.19* | 0.10 | 0.000 | 4.16* | 0.06 | 0.000 |
| AL Δ T2–T3 | 47.79* | 1.62 | 0.000 | 48.23* | 0.79 | 0.000 | 3.87* | 0.12 | 0.000 | 4.15* | 0.06 | 0.000 |
| AL Δ T3–T4 | 47.67* | 1.54 | 0.000 | 49.02* | 0.84 | 0.000 | 4.02* | 0.09 | 0.000 | 4.08* | 0.06 | 0.000 |
| AL Δ T4–T5 | 48.60* | 1.43 | 0.000 | 48.31* | 0.86 | 0.000 | 3.94* | 0.11 | 0.000 | 4.17* | 0.06 | 0.000 |
| Latent Change Score Variance | ||||||||||||
| AL Δ T1–T2 | 84.08* | 17.21 | 0.000 | 80.43* | 9.33 | 0.000 | 0.34* | 0.07 | 0.000 | 0.44* | 0.06 | 0.000 |
| AL Δ T2–T3 | 93.76* | 18.31 | 0.000 | 72.58* | 8.77 | 0.000 | 0.53* | 0.12 | 0.000 | 0.48* | 0.08 | 0.000 |
| AL Δ T3–T4 | 94.97* | 16.23 | 0.000 | 77.54* | 9.43 | 0.000 | 0.34* | 0.07 | 0.000 | 0.39* | 0.06 | 0.000 |
| AL Δ T4–T5 | 79.62* | 17.24 | 0.000 | 81.74* | 9.67 | 0.000 | 0.45* | 0.09 | 0.000 | 0.39* | 0.05 | 0.000 |
SR social relationship, AL alcohol use, RAC race, ITN income-to-needs ratio, PAR parent–adolescent relationship quality, T1 Time 1 (age 14), T2 Time 2 (age 15), T3 Time 3 (age 16), T4 Time 4 (age 17), T5 Time 5 (age 18). Est. unstandardized parameter estimate, SE standard error.
p < 0.10;
p < 0.05.
Next, for personal religiousness, the two-group LCS of the moderation of personal religiousness between social involvement and alcohol use change displayed acceptable fit (χ2 = 90.25, df = 63, p = 0.014, RMSEA = 0.07, CFI = 0.91). As can be seen in Table 5, consistent with the two-group LCS based on the median split, there were no significant associations between social involvement and change in alcohol use. The two-group LCS of the moderation of personal religiousness between social alienation and alcohol use change displayed acceptable fit (χ2 = 86.99, df = 62, p = 0.020, RMSEA = 0.07, CFI = 0.92), and the findings were consistent with the two-group LCS based on the median split. Specifically, significant positive associations were found between social alienation at Time 2 and the subsequent change in alcohol use from Time 2 to Time 3, as well as between social alienation at Time 4 and the subsequent change in alcohol use from Time 4 to Time 5 (see Table 5).
Table 5.
Latent change score model of the moderation of personal religiousness (Lowest 25% vs. Others) between social relationships and alcohol use
| Parameter | Social Involvement |
Social Alienation |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Religiousness |
High Religiousness |
Low Religiousness |
High Religiousness |
|||||||||
| Est. | SE | p | Est. | SE | p | Est. | SE | p | Est. | SE | p | |
| Regression Effects | ||||||||||||
| SR T1 → AL Δ T1-T2 | 0.00 | 0.01 | 0.707 | 0.00 | 0.00 | 0.785 | 0.11 | 0.20 | 0.589 | 0.05 | 0.09 | 0.596 |
| SR T2 → AL Δ T2-T3 | 0.01 | 0.01 | 0.453 | 0.01 | 0.01 | 0.233 | 0.34* | 0.17 | 0.044 | 0.10 | 0.09 | 0.247 |
| SR T3 → AL Δ T3-T4 | 0.01 | 0.01 | 0.254 | 0.00 | 0.01 | 0.846 | −0.04 | 0.33 | 0.902 | 0.04 | 0.11 | 0.694 |
| SR T4 → AL Δ T4-T5 | 0.01 | 0.01 | 0.470 | 0.00 | 0.01 | 0.716 | 0.52* | 0.23 | 0.024 | 0.05 | 0.13 | 0.676 |
| SEX T1 → AL Δ T1-T2 | 0.32 | 0.27 | 0.232 | −0.02 | 0.13 | 0.883 | 0.40 | 0.28 | 0.162 | −0.02 | 0.13 | 0.874 |
| SEX T2 → AL Δ T2-T3 | 0.10 | 0.32 | 0.743 | 0.06 | 0.18 | 0.723 | 0.34 | 0.36 | 0.344 | 0.06 | 0.17 | 0.740 |
| SEX T3 → AL Δ T3-T4 | −0.47 | 0.34 | 0.172 | 0.13 | 0.19 | 0.500 | −0.41 | 0.42 | 0.327 | 0.14 | 0.17 | 0.414 |
| SEX T4 → AL Δ T4-T5 | −0.15 | 0.39 | 0.690 | −0.10 | 0.25 | 0.686 | 0.02 | 0.35 | 0.956 | −0.06 | 0.22 | 0.805 |
| RAC T1 → AL Δ T1-T2 | −0.29 | 0.31 | 0.354 | 0.10 | 0.17 | 0.565 | −0.34 | 0.31 | 0.261 | 0.07 | 0.17 | 0.688 |
| RAC T2 → AL Δ T2-T3 | 0.19 | 0.37 | 0.604 | 0.07 | 0.20 | 0.711 | 0.08 | 0.43 | 0.859 | 0.12 | 0.19 | 0.541 |
| RAC T3 → AL Δ T3-T4 | 0.30 | 0.46 | 0.513 | −0.07 | 0.29 | 0.821 | 0.15 | 0.42 | 0.716 | −0.02 | 0.25 | 0.927 |
| RAC T4 → AL Δ T4-T5 | −0.35 | 0.57 | 0.543 | −0.67 | 0.36 | 0.058 | −0.15 | 0.52 | 0.779 | −0.64 | 0.33 | 0.053 |
| ITN T1 → AL Δ T1-T2 | −0.06 | 0.06 | 0.344 | −0.01 | 0.03 | 0.711 | −0.04 | 0.06 | 0.475 | −0.01 | 0.03 | 0.704 |
| ITN T2 → AL Δ T2-T3 | 0.08 | 0.06 | 0.179 | 0.05 | 0.04 | 0.267 | 0.10 | 0.06 | 0.068 | 0.05 | 0.04 | 0.200 |
| ITN T3 → AL Δ T3-T4 | 0.01 | 0.06 | 0.867 | 0.03 | 0.05 | 0.540 | 0.03 | 0.06 | 0.676 | 0.04 | 0.04 | 0.377 |
| ITN T4 → AL Δ T4-T5 | 0.01 | 0.08 | 0.952 | −0.14* | 0.07 | 0.039 | 0.01 | 0.08 | 0.951 | −0.13 | 0.07 | 0.053 |
| PAR T1 → AL Δ T1-T2 | 0.01 | 0.12 | 0.932 | 0.01 | 0.07 | 0.901 | −0.01 | 0.19 | 0.949 | −0.04 | 0.10 | 0.707 |
| PAR T2 → AL Δ T2-T3 | −0.14 | 0.16 | 0.389 | −0.15 | 0.08 | 0.063 | −0.37 | 0.22 | 0.093 | −0.15 | 0.09 | 0.085 |
| PAR T3 → AL Δ T3-T4 | −0.09 | 0.22 | 0.663 | −0.04 | 0.10 | 0.715 | 0.18 | 0.38 | 0.632 | −0.07 | 0.12 | 0.547 |
| PAR T4 → AL Δ T4-T5 | −0.01 | 0.23 | 0.964 | 0.20 | 0.14 | 0.158 | 0.39 | 0.24 | 0.098 | 0.13 | 0.13 | 0.336 |
| Proportional Effects | ||||||||||||
| AL T1 → AL Δ T1-T2 | 0.26 | 0.34 | 0.443 | 0.43 | 0.33 | 0.195 | 0.26 | 0.33 | 0.427 | 0.27 | 0.22 | 0.218 |
| AL T2 → AL Δ T2-T3 | 0.26 | 0.34 | 0.443 | 0.43 | 0.33 | 0.195 | 0.26 | 0.33 | 0.427 | 0.27 | 0.22 | 0.218 |
| AL T3 → AL Δ T3-T4 | 0.26 | 0.34 | 0.443 | 0.43 | 0.33 | 0.195 | 0.26 | 0.33 | 0.427 | 0.27 | 0.22 | 0.218 |
| AL T4 → AL Δ T4-T5 | 0.26 | 0.34 | 0.443 | 0.43 | 0.33 | 0.195 | 0.26 | 0.33 | 0.427 | 0.27 | 0.22 | 0.218 |
| Latent Change Score Mean | ||||||||||||
| AL Δ T1-T2 | 45.27* | 1.41 | 0.000 | 47.72* | 0.82 | 0.000 | 4.15* | 0.10 | 0.000 | 4.17* | 0.06 | 0.000 |
| AL Δ T2-T3 | 47.18* | 1.30 | 0.000 | 48.41* | 0.84 | 0.000 | 3.91* | 0.13 | 0.000 | 4.16* | 0.06 | 0.000 |
| AL Δ T3-T4 | 48.68* | 1.49 | 0.000 | 48.64* | 0.86 | 0.000 | 4.02* | 0.10 | 0.000 | 4.08* | 0.06 | 0.000 |
| AL Δ T4-T5 | 48.75* | 1.50 | 0.000 | 48.22* | 0.85 | 0.000 | 4.00* | 0.10 | 0.000 | 4.16* | 0.06 | 0.000 |
| Latent Change Score Variance | ||||||||||||
| AL Δ T1-T2 | 86.75* | 17.66 | 0.000 | 78.52* | 8.96 | 0.000 | 0.40* | 0.09 | 0.000 | 0.42* | 0.05 | 0.000 |
| AL Δ T2-T3 | 70.89* | 15.04 | 0.000 | 80.06* | 9.17 | 0.000 | 0.61* | 0.13 | 0.000 | 0.45* | 0.07 | 0.000 |
| AL Δ T3-T4 | 91.54* | 19.39 | 0.000 | 80.34* | 9.35 | 0.000 | 0.41* | 0.09 | 0.000 | 0.36* | 0.05 | 0.000 |
| AL Δ T4-T5 | 87.62* | 17.35 | 0.000 | 75.98* | 9.06 | 0.000 | 0.43* | 0.09 | 0.000 | 0.41* | 0.05 | 0.000 |
SR social relationship, AL alcohol use, RAC race, ITN income-to-needs ratio, PAR parent–adolescent relationship quality, T1 Time 1 (age 14), T2 Time 2 (age 15), T3 Time 3 (age 16), T4 Time 4 (age 17), T5 Time 5 (age 18). Est. unstandardized parameter estimate, SE standard error.
p < 0.05.
To summarize, results from sensitivity analyses solidified how religiousness and the risk factor of social alienation interface to predict developmental changes in substance use behaviors during adolescence into young adulthood, although statistical significance (i.e., p levels) was not always consistent with the main analysis results, likely due to the nature of decreased sample size for the lowest religiousness group (i.e., 25% of the sample).
Discussion
Adolescence is a developmental period characterized by heightened susceptibility to social influences, particularly by peers (Albert et al., 2013). Adolescents are more sensitive to acceptance and rejection by peers, and their risk-taking behaviors are also influenced by peers (Dishion & Tipsord, 2011). Yet, some adolescents are more vulnerable than others to the effects of social relationships. As such, the identification of factors that may buffer against adverse effects of social relationship risks is helpful in informing preventive intervention efforts to reduce adolescent substance use and prevent its associated outcomes (Spear, 2018). The present longitudinal study documents the protective role of religiousness in the link between the effects of social relationship risk factors (both being involved with and alienated from social relationships) on substance use across adolescence into young adulthood.
The effect of social alienation on alcohol use was consistent with prior work suggesting a link between loneliness and social isolation with greater substance use (Copeland et al., 2018; Osgood et al., 2014). Importantly, the findings of the function of social relationships align with Cooper’s (1994) four factor model of alcohol use motivators: Those who are socially alienated with high alcohol use can be internally motivated by coping drinking motives (e.g. to forget about their problems) or enhancement motives (e.g., to get high). Internally motivated alcohol users have different clinical implications. For example, drinking as a form of self-medication is often done alone. These solitary drinkers—who are internally motivated—are more concerning, as solitary drinking motivated by the need to cope with emotional pain presents a greater risk of substance use disorders in later life (Mason et al., 2020; Skrzynski & Creswell, 2020). It follows that identifying protective factors against social alienation related drinking is particularly important.
However, the nonsignificant effect of social involvement on alcohol use was not in line with previous research indicating a link between sociometric popularity and substance use culminating in socially motivated drinking behaviors (Ali et al., 2014; Allen et al., 2005; Hussong et al., 2020). The discrepancy between the previous and the current findings may be due to the nature of the social involvement measure used in the current study that mainly captured involvement in groups as well as number of friends and frequency of contacts with friends. Our finding suggests that these quantitative aspects of social involvement may not be a critical predictor of alcohol use. Instead, as alluded by social identity theory (Tajfel & Turner, 1979), adolescents’ risky decision making may depend on the social norms espoused by their social groups such that the attitude that those friends and groups hold toward alcohol use may matter more than quantity of social interactions with respect to influencing adolescents’ alcohol use behaviors.
The study hypothesized that both organizational and personal religiousness would act as a protective factor against social relationship effects on alcohol use, and the findings provide supportive evidence of the protective role of religiousness. Specifically, the alcohol use of adolescents who were low in organizational and personal religiousness was more heavily impacted by the social relationship risk factor of alienation than those high in organizational and personal religiousness. Organizational religiousness is characterized by an adolescent’s engagement in religious institutions, such as attending church services or youth group. The reduced social alienation effects among adolescents with high organizational religiousness are consistent with the reformulated social control theory, as strongly religious adolescents are more likely to internalize these rules and values through their relationships with older adults in their religious communities (Gottfredson & Hirschi, 1990) and thus are less likely to engage in substance use as a coping mechanism.
Personal religiousness is characterized by the personal importance of faith to an adolescent. Consistent with the divine interaction theory (Ellison, 1991; Pollner, 1989), an adolescent who has high personal religiousness forms a relationship with a divine being similar to that of a social relationship, thus seeking out guidance and solace from the divine. The reduced social alienation effects among adolescents with high personal religiousness suggest that their experience of a supportive relationship with a divine being can then help them to resist desires to drink driven by coping motives, such as drinking to achieve the negative, internally generated reinforcement of forgetting pain from feeling lonely. The current finding of the buffering role of personal religiousness is also consistent with prior work suggesting the role of personal religiousness in promoting self-regulation and in turn reducing substance use among adolescents (Kim-Spoon et al., 2015).
Collectively, our findings suggest that both an adolescent’ s frequent involvement in religious institutions, as well as an adolescent’s personal relationship with a divine being, serve as protective factors against alcohol use fueled by the risk factor of social alienation. However, it is important to note that, because the rigorous numeric invariance tests of group differences regarding the social alienation effects at Time 2 for organizational religiousness and the social alienation effects at Time 2 and at Time 4 for personal religiousness were not statistically significant, the results should be interpreted with caution and replication of the findings is warranted.
In light of extant literature implying potential developmental differences with respect to the influences of social relationships, it is important to examine longitudinal analyses to explore differential timing of social relationships contributing to substance use behaviors. The pattern of findings suggested significant effects of social alienation in early adolescence as well as late adolescence into young adulthood. Early adolescence is a time characterized by both social and school changes, as youth transition from middle to high school, spend more time with peers than they do parents, and are exposed to social groups with older peers (Blum et al., 2014). Similarly, late adolescence into young adulthood is a time characterized by social role transitions, including graduating high school and going to college or joining the workforce or military (Shanahan, 2000). These social transitions open the door to increased substance use behaviors within the social context, especially for those who feel alienated from their peers. Stress during a time of social transition (e.g., starting a high school or leaving home to attend college) can prompt self-medication via alcohol use as a way of coping (Creswell et al., 2014; Tomlinson & Brown, 2012). Further, in line with existing literature indicating that the transition to high school is a time often associated with increased loneliness (Benner et al., 2017) and that young adults are particularly sensitive to the effects of loneliness and social isolation (Murthy, 2020), the data suggest that the influence of social alienation on alcohol use is prominent during high school years and for those transitioning into young adulthood.
The contributions of the current study should be considered in light of several limitations. First, study variables were assessed through self-reports. There is evidence that self-report measures are particularly revealing for behaviors that are related to private or internal experience (e.g., Kendall et al., 1989) such as certain aspects of religiousness, alcohol use, and social relationships. Yet, the associations among the study variables may have been enhanced due to method variance and within-subject bias, thus replications of the findings utilizing multiple-informant multi-method assessments are warranted. In particular, sociometric assessment of popularity may represent some important aspects of social involvement (e.g., popularity) in relation to alcohol use. Further, including an assessment of peer substance use or peer delinquency to capture the nuanced role of social involvement would enhance clearer understanding of the role of adolescents’ social network. Indeed, a rich body of empirical work suggests that affiliation with substance-using peers increases substance use throughout adolescence and young adulthood (e.g., Otten et al., 2017). Second, it is important to state the potential limitations of the sample used in this study. The sample involved a homogeneously aged sample of both male and female adolescents who were annually assessed throughout adolescence. Such an intensive longitudinal data collection provided suitable data for examining fast-moving changes in social relationships and substance use behaviors. Yet, given the relatively small sample size and the nature of being regionally representative, future research should replicate the results with larger, nationally representative samples.
These limitations notwithstanding, the current study had notable strengths, including five waves of data with a prospective design that allowed testing timing of the social relationship effects and latent change score models that permitted more precise estimation of the dynamic change in alcohol use affected by preceding social relationship risk factors. The findings have implications useful for health professionals to assist youth at risk for substance use. First, one way to utilize the social effects toward preventing alcohol use is to guide young people to healthy social affiliations. For example, studies using at-risk adult populations have reported positive effects of social network intervention in which participants examine their own social networks to identify people who trigger their substance use in comparison to people who support healthier choices (Kennedy et al., 2018), and actively choose to spend more time with the latter (Eddie & Kelly, 2017). Second, the data provide preliminary support suggesting important roles of religiousness in shaping substance use behaviors among young people. For example, positive religious coping mechanisms (e.g., seeking social support from faith groups) have been found to be associated with positive affect and greater life satisfaction in adolescents (Van Dyke et al., 2009). Indeed, this is consistent with the use of religious and spiritual practices in groups such as Alcoholics Anonymous that have provided strong evidence for the potential of religious values in overcoming substance use (Hahn, 2019) as well as loneliness (Murthy, 2020).
Conclusion
Within the current literature, the moderating effect of religiousness on specifically peer-related social relationship factors is not well known. The present study presents a longitudinal investigation seeking to elucidate how social relationship risk factors and religiousness protective factors interface to predict developmental changes in alcohol use during adolescence and into young adulthood. The findings demonstrate protective effects of organizational and personal religiousness against the detrimental effect of social alienation risk factor that promotes alcohol use during adolescence into young adulthood. The results highlight the protective roles of religiousness acting as additional sources of social engagement experiences to modulate the effects of social alienation predicting alcohol use progression and provide further evidence for the positive impact religiousness has on healthy adolescent development.
Supplementary Material
Acknowledgements
The authors thank the former and current members of the JK Lifespan Development Lab at Virginia Tech for their help with data collection. We are grateful to the adolescents and parents who participated in our study.
Funding
This work was supported by grants from the National Institutes of Health awarded to Jungmeen Kim-Spoon and Brooks King-Casas (DA036017) and Joe Allen (HD058305).
Biographies
Jordan Gamache is a PhD student at Virginia Tech. Her major research interests include social relationships throughout adolescence, primarily peer and romantic relationships, and their influence longitudinally on risk-taking behaviors.
Toria Herd is a postdoctoral research fellow at Penn State. Her major research interests include individual, family, and system level risk and protective factors associated with child maltreatment as well as the longitudinal physical and mental health outcomes associated with child maltreatment.
Joseph Allen is the Hugh P. Kelley Professor of Psychology and Education at the University of Virginia. His research focuses on the predictors and long-term outcomes of social development processes from adolescence into adulthood. He also develops and examines socially-focused interventions for adolescents designed to improve long-term academic and mental health outcomes.
Brooks King-Casas is an Associate Professor at the Fralin Biomedical Research Institute at Virginia Tech Carilion. His major research interests include neural underpinnings of valuation and learning in social settings, and how social and economic preferences influence valuation and learning.
Jungmeen Kim-Spoon is a Professor of Psychology at Virginia Tech. Her research focuses on risk and resilience in the development of psychopathology and health risk behaviors during adolescence and young adulthood.
Footnotes
Conflict of interest The authors declare no competing interests.
Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent Informed consent was obtained from all individual participants included in the study.
Data Sharing and Declaration
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
- Achenbach TM, & Rescorla L (2001). Manual for the ASEBA School-Age Forms and Profiles. Burlington, VT: Department of Psychiatry, University of Vermont. [Google Scholar]
- Albert D, Chein J, & Steinberg L (2013). The teenage brain: Peer influences on adolescent decision making. Current Directions in Psychological Science, 22(2), 114–120. 10.1177/0963721412471347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ali MM, Amialchuk A, & Nikaj S (2014). Alcohol consumption and social network ties among adolescents: Evidence from Add Health. Addictive Behaviors, 39(5), 918–922. 10.1016/j.addbeh.2013.11.030. [DOI] [PubMed] [Google Scholar]
- Allen JP, Porter MR, McFarland FC, Marsh P, & McElhaney KB (2005). The two faces of adolescents’ success with peers: Adolescent popularity, social adaptation, and deviant behavior. Child Development, 76(3), 747–760. 10.1111/j.1467-8624.2005.00875.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armsden GC, & Greenberg MT (1987). The Inventory of Parent and Peer Attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16(5), 427–454. 10.1007/BF02202939. [DOI] [PubMed] [Google Scholar]
- Bandura A, & McClelland DC (1977). Social learning theory (Vol. 1). Englewood cliffs: Prentice Hall. [Google Scholar]
- Benner AD, Boyle AE, & Bakhtiari F (2017). Understanding students’ transition to high school: Demographic variation and the role of supportive relationships. Journal of Youth and Adolescence, 46(10), 2129–2142. 10.1007/s10964-017-0716-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benotsch EG, Snipes DJ, Martin AM, & Bull SS (2013). Sexting, substance use, and sexual risk behavior in young adults. Journal of Adolescent Health, 52(3), 307–313. 10.1016/j.jadohealth.2012.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biggs BK, Vernberg EM, & Wu YP (2012). Social anxiety and adolescents’ friendships: The role of social withdrawal. The Journal of Early Adolescence, 32(6), 802–823. 10.1177/0272431611426145. [DOI] [Google Scholar]
- Blum RW, Astone NM, Decker MR, & Mouli VC (2014). A conceptual framework for early adolescence: a platform for research. International Journal of Adolescent Medicine and Health, 26(3), 321–331. 10.1515/ijamh-2013-0327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper ML (1994). Motivations for alcohol use among adolescents: development and validation of a four-factor model. Psychological Assessment, 6(2), 117. [Google Scholar]
- Copeland M, Fisher JC, Moody J, & Feinberg ME (2018). Different kinds of lonely: Dimensions of isolation and substance use in adolescence. Journal of Youth and Adolescence, 47(8), 1755–1770. 10.1007/s10964-018-0860-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creswell KG, Chung T, Clark DB, & Martin CS (2014). Solitary alcohol use in teens is associated with drinking in response to negative affect and predicts alcohol problems in young adulthood. Clinical Psychological Science: A Journal of the Association for Psychological Science, 2(5), 602–610. 10.1177/2167702613512795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, & Tipsord JM (2011). Peer contagion in child and adolescent social and emotional development. Annual Review of Psychology, 62, 189–214. 10.1146/annurev.psych.093008.100412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eddie D, & Kelly JF (2017). How many or how much? Testing the relative influence of the number of social network risks versus the amount of time exposed to social network risks on post-treatment substance use. Drug and Alcohol Dependence, 175, 246–253. 10.1016/j.drugalcdep.2017.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberger NI, Lieberman MD, & Williams KD (2003). Does rejection hurt? An fMRI study of social exclusion. Science, 302 (5643), 290–292. 10.1126/science.1089134. [DOI] [PubMed] [Google Scholar]
- Eisenberger NI (2012). The neural bases of social pain: evidence for shared representations with physical pain. Psychosomatic Medicine, 74(2), 126 10.1097/PSY.0b013e3182464dd1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellison CG (1991). Religious involvement and subjective well-being. Journal of Health & Social Behavior, 32(1), 80–99. 10.2307/2136801. [DOI] [PubMed] [Google Scholar]
- Erdley CA, & Day HJ (2017). Friendship in childhood and adolescence. The psychology of friendship, 3–19. [Google Scholar]
- Feldstein Ewing SW, Houck JM, & Bryan AD (2015). Neural activation during response inhibition is associated with adolescents’ frequency of risky sex and substance use. Addictive Behaviors, 44, 80–87. 10.1016/j.addbeh.2014.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fetzer Institute & National Institute on Aging Working Group. (1999). Multidimensional measurement of religiousness/spirituality for use in health research. Kalamazoo, MI: Fetzer Institute. [Google Scholar]
- Friese B, Grube JW, & Moore RS (2013). Youth acquisition of alcohol and drinking contexts: An in-depth look. Journal of Drug Education, 43(4), 385–403. 10.2190/DE.43.4.f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gottfredson MR, & Hirschi T (1990). A general theory of crime. Stanford University Press. [Google Scholar]
- Hahn JL (2019). “God as we understood Him”: Being “spiritual but not religious” in Alcoholics Anonymous past and present. Implicit Religion, 22(2). 10.1558/imre.37778 [DOI] [Google Scholar]
- Holmes C, & Kim-Spoon J (2016). Why are religiousness and spirituality associated with externalizing psychopathology? A literature review. Clinical Child and Family Psychology Review, 19, 1–20. 10.1007/s10567-015-0199-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holmes CH, Brieant A, King-Casas, & Kim-Spoon J (2019). How is religiousness associated with adolescent risk taking? The roles of emotion regulation and executive function. Journal of Research on Adolescence, 29, 334–344. 10.1111/jora.12438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong AM, Ennett ST, McNeish DM, Cole VT, Gottfredson NC, Rothenberg WA, & Faris RW (2020). Social network isolation mediates associations between risky symptoms and substance use in the high school transition. Development and psychopathology, 32(2), 615–630. 10.1017/S095457941900049X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor R, & Jessor SL (1977). Problem behavior and psychosocial development: A longitudinal study of youth. New York, NY: Academic Press. 10.15288/jsa.1978.39.948 [DOI] [Google Scholar]
- Katz J, Porath M, Bendu C, & Epp B (2012). Diverse voices: Middle years students’ insights into life in inclusive classrooms. Exceptionality Education International, 22(1), 2–16. 10.5206/eei.v22i1.7685. [DOI] [Google Scholar]
- Kendall PC, Cantwell DP, & Kazdin AE (1989). Depression in children and adolescents: Assessment issues and recommendations. Cognitive Therapy and Research, 13, 109–146. 10.1007/BF01173268. [DOI] [Google Scholar]
- Kennedy DP, Osilla KC, Hunter SB, Golinelli D, Hernandez EM, & Tucker JS (2018). A pilot test of a motivational interviewing social network intervention to reduce substance use among housing first residents. Journal of Substance Abuse Treatment, 86, 36–44. 10.1016/j.jsat.2017.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim-Spoon J, McCullough ME, Bickel WK, Farley JP, & Longo GS (2015). Longitudinal associations among religiousness, delay discounting, and substance use initiation in early adolescence. Journal of Research on Adolescence, 25(1), 36–43. 10.1111/jora.12104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim-Spoon J, Farley JP, Holmes CJ, & Longo GS (2014a). Does adolescents’ religiousness moderate links between harsh parenting and adolescent substance use? Journal of Family Psychology, 28(6), 739–748. 10.1037/a0037178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim-Spoon J, Farley JP, Holmes CJ, Longo GS, & McCullough ME (2014b). Processes linking parents’ and adolescents’ religiousness and adolescent substance use: Monitoring behaviors and self-regulation. Journal of Youth and Adolescence, 43, 745–756. 10.1007/s10964-013-9998-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB (2011). Principles and practice of structural equation modeling (3rd ed). New York, NY: Guilford. [Google Scholar]
- Lemyre A, Gauthier-Légaré A, & Bélanger RE (2019). Shyness, social anxiety, social anxiety disorder, and substance use among normative adolescent populations: a systematic review. The American Journal of Drug and Alcohol Abuse, 45(3), 230–247. 10.1080/00952990.2018.1536882. [DOI] [PubMed] [Google Scholar]
- Little TD (2013). Longitudinal structural equation modeling. Guilford press. [Google Scholar]
- Mason WA, Stevens AL, & Fleming CB (2020). A systematic review of research on adolescent solitary alcohol and marijuana use in the United States. Addiction, 115(1), 19–31. 10.1111/add.14697. [DOI] [PubMed] [Google Scholar]
- Maughan B, Collishaw S, & Stringaris A (2013). Depression in childhood and adolescence. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 22(1), 35. [PMC free article] [PubMed] [Google Scholar]
- McArdle JJ, & Hamagami F (2001). Latent difference score structural models for linear dynamic analyses with incomplete longitudinal data. In Collins LM & Sayer AG (Eds.), New methods for the analysis of change (pp. 139–175). Washington, DC: American Psychological Association. [Google Scholar]
- McCullough ME, & Willoughby BL (2009). Religion, self-regulation, and self-control: Associations, explanations, and implications. Psychological Bulletin, 135(1), 69 10.1037/a0014213. [DOI] [PubMed] [Google Scholar]
- Moody J, Brynildsen WD, Osgood DW, Feinberg ME, & Gest S (2011). Popularity trajectories and substance use in early adolescence. Social Networks, 33(2), 101–112. 10.1016/j.socnet.2010.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morin JFG, Afzali MH, Bourque J, Stewart SH, Séguin JR, O’Leary-Barrett M, & Conrod PJ (2019). A population-based analysis of the relationship between substance use and adolescent cognitive development. American Journal of Psychiatry, 176(2), 98–106. 10.1176/appi.ajp.2018.18020202. [DOI] [PubMed] [Google Scholar]
- Murthy VH (2020). Together: The healing power of human connection in a sometimes lonely world. (HarperCollins; ). [Google Scholar]
- Muthén LK, & Muthén BO (1998). Mplus User’s Guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén. 2021. [Google Scholar]
- Osgood DW, Feinberg ME, Wallace LN, & Moody J (2014). Friendship group position and substance use. Addictive Behaviors, 39(5), 923–933. 10.1016/j.addbeh.2013.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Otten R, Mun CJ, & Dishion TJ (2017). The social exigencies of the gateway progression to the use of illicit drugs from adolescence into adulthood. Addictive Behaviors, 73, 144–150. 10.1016/j.addbeh.2017.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peviani K, Brieant A, Holmes C, King-Casas B, & Kim-Spoon J (2019). Religious social support protects against social risks for adolescent substance use. Journal of Research on Adolescence, 30, 361–371. 10.1111/jora.12529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pirutinsky S (2014). Does religiousness increase self-control and reduce criminal behavior? A longitudinal analysis of adolescent offenders. Criminal Justice and Behavior, 41(11), 1290–1307. 10.1177/0093854814531962. [DOI] [Google Scholar]
- Pollner M (1989). Divine relations, social relations, and well-being. Journal of Health and Social Behavior, 30, 92–104. 10.2307/2136915. [DOI] [PubMed] [Google Scholar]
- Rosenthal NL, & Kobak R (2010). Assessing Adolescents’ attachment hierarchies: differences across developmental periods and associations with individual adaptation. Journal of Research on Adolescense, 20(3), 678–706. 10.1111/j.1532-7795.2010.00655.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shanahan MJ (2000). Pathways to adulthood in changing societies: Variability and mechanisms in life course perspective. Annual Review of Sociology, 26(1), 667–692. 10.1146/annurev.soc.26.1.667. [DOI] [Google Scholar]
- Skrzynski CJ, & Creswell KG (2020). Associations between solitary drinking and increased alcohol consumption, alcohol problems, and drinking to cope motives in adolescents and young adults: a systematic review and meta-analysis. Addiction, 115 (11), 1989–2007. 10.1111/add.15055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spear LP (2018). Effects of adolescent alcohol consumption on the brain and behaviour. Nature Reviews Neuroscience, 19(4), 197 10.1038/nrn.2018.10. [DOI] [PubMed] [Google Scholar]
- Squeglia LM, Jacobus J, & Tapert SF (2009). The influence of substance use on adolescent brain development. Clinical EEG and Neuroscience, 40(1), 31–38. 10.1177/155005940904000110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L (2010). A dual systems model of adolescent risk-taking. Developmental Psychobiology: The Journal of the International Society for Developmental Psychobiology, 52(3), 216–224. 10.1002/dev.20445. [DOI] [PubMed] [Google Scholar]
- Streiner DL (2003). Being inconsistent about consistency: when coefficient alpha does and doesn’t matter. Journal of Personality Assessment, 80(3), 217–222. [DOI] [PubMed] [Google Scholar]
- Tajfel H, & Turner JC (1979). An integrative theory of intergroup conflict. In Austin WG & Worchel S (Eds.), The social psychology of intergroup relations (pp. 33–37). Monterey, CA: Brooks/Cole. [Google Scholar]
- Tillfors M, Persson S, Willén M, & Burk WJ (2012). Prospective links between social anxiety and adolescent peer relations. Journal of Adolescence, 35(5), 1255–1263. 10.1016/j.adolescence.2012.04.008. [DOI] [PubMed] [Google Scholar]
- Tomlinson KL, & Brown SA (2012). Self-medication or social learning? A comparison of models to predict early adolescent drinking. Addictive Behaviors, 37(2), 179–186. 10.1016/j.addbeh.2011.09.016. [DOI] [PubMed] [Google Scholar]
- Trucco EM (2020). A review of psychosocial factors linked to adolescent substance use. Pharmacology Biochemistry and Behavior. 172969. 10.1016/j.pbb.2020.172969 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Dyke CJ, Glenwick DS, Cecero JJ, & Kim SK (2009). The relationship of religious coping and spirituality to adjustment and psychological distress in urban early adolescents. Mental Health, Religion and Culture, 12(4), 369–383. 10.1080/13674670902737723. [DOI] [Google Scholar]
- Van Ryzin MJ, Fosco GM, & Dishion TJ (2012). Family and peer predictors of substance use from early adolescence to early adulthood: an 11-year prospective analysis. Addictive Behaviors, 37, 1314–1324. 10.1016/j.addbeh.2012.06.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walters KS, Bulmer SM, Troiano PF, Obiaka U, & Bonhomme R (2018). Substance use, anxiety, and depressive symptoms among college students. Journal of Child & Adolescent Substance Abuse, 27(2), 103–111. 10.1080/1067828X.2017.1420507. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.