

Abstract
Docetaxel is a cytotoxic taxane frequently used to treat patients with various cancers, including non‐small cell lung cancer (NSCLC). Docetaxel is known to cause acute myalgias, arthralgias, and neuropathy, but there have been few published case reports of myositis. Here, we describe a rare case of docetaxel‐induced myositis diagnosed based on laboratory data, thigh magnetic resonance imaging (MRI), and electromyography (EEG). A 66‐year‐old male was admitted for thigh pain and fatigue that onset 1 week prior. He had been diagnosed with stage IVA (cT4N0M1a) NSCLC 3 years ago and had been started on docetaxel (60 mg/m2 intravenously every 3 weeks; fourth‐line chemotherapy) 1 month earlier. After the second cycle, he developed both thigh pain and fatigue. On admission, his creatinine phosphokinase (CPK) level was elevated, thigh MRI revealed diffuse muscle edema, and EEG showed myogenic changes. We found no plausible cause for myositis except docetaxel. He was diagnosed with myositis and treated with oral prednisolone. His symptoms were relieved and the CPK level declined. Although rare, this case indicates that clinicians should consider the possibility of myositis as a complication in patients on docetaxel.
Keywords: docetaxel, lung cancer, myositis
Docetaxel, a cytotoxic taxane frequently used to treat patients with various cancers, is known to cause acute myalgias, arthralgias, and neuropathy, but there have been few case reports of myositis.
We describe a case of docetaxel‐induced myositis that developed after two cycles of docetaxel, and diagnosed based on laboratory data, thigh magnetic resonance imaging, and electromyography.
Clinicians should consider this possibility when patients complain of muscle pain or the CPK level is elevated.

Docetaxel‐induced myositis developed after two cycles of docetaxel in a patient with a lung adenocarcinoma.
INTRODUCTION
Docetaxel is a cytotoxic taxane frequently prescribed for patients with various cancers, including non‐small cell lung cancer (NSCLC). Docetaxel is well‐known to cause peripheral edema, myalgias, arthralgias, and neuropathy. Myositis (muscle inflammation) can be caused by autoimmune diseases, infection, injury, exercise, or drugs, but docetaxel‐induced myositis is extremely rare. Herein, we present a case of myositis that developed after two cycles of docetaxel.
CASE REPORT
A 66‐year‐old male had been diagnosed with a stage IV (cT4N0M1a) lung adenocarcinoma (without any mutation) 3 years prior. His medical history included noninsulin‐dependent type 2 diabetes mellitus, hypertension, and hypercholesterolemia, which were all well controlled with sitagliptin phosphate hydrate, atenolol, and atorvastatin calcium hydrate. The only new treatment introduced in the previous 3 months had been chemotherapy. Docetaxel was started (60 mg/m2 intravenously every 3 weeks; fourth‐line chemotherapy). He completed two cycles without any notable side‐effects except febrile neutropenia. However, he developed thigh pain and fatigue 2 weeks after the second infusion. He had no joint pain or pigmenturia.
On physical examination, he had a high fever and mild pain in both thighs, without peripheral edema. Muscle weakness was symmetrical (i.e., affected both legs) during active resistance to movement. Joint examination was unremarkable and there was no skin lesions. Leukocytosis was evident (9.41 × 103/μl) together with an elevated C‐reactive protein level (3.57 mg/dl). The creatinine phosphokinase (CPK) level was 2515 U/l, but had previously been normal. The aldolase level was 138.8 U/l. Acute myositis was suspected and he was admitted. Magnetic resonance imaging (MRI) of his thigh revealed diffuse muscular edema involving the bilateral gluteal and thigh muscles (Figure 1). Needle electromyography (EMG) revealed fibrillation, positive sharp waves at rest, and early recruitment during voluntary contraction (myogenic changes). Autoantibody tests for antinuclear antibody, anti‐SSA, anti‐SSB, anti‐ARS, anti‐Jo‐1, anti‐TIF1‐γ, anti Mi‐2, and anti‐MDA‐5 were all negative. The high fever persisted and the CPK level increased to 8715 U/l even after discontinuation of all oral drugs (including the statin). We diagnosed nonspecific myositis. Given his recent medication, docetaxel‐induced myositis was considered.
FIGURE 1.

Coronal T2‐weighted MRI of the thighs revealed diffuse muscular edema involving the bilateral gluteal and thigh muscles
Chemotherapy was discontinued and prednisolone (PSL) 60 mg/day (1 mg/kg/day) was initiated. The CPK level gradually normalized and the high fever and thigh pain were relieved (Figure 2). PSL was tapered over 4 weeks. One month later, the patient remains asymptomatic without any recurrence of myositis.
FIGURE 2.
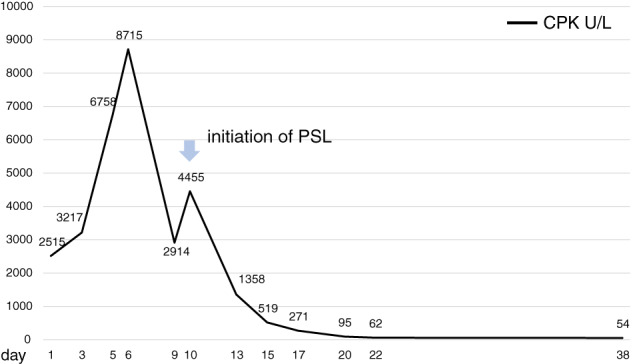
Shows the time course of CPK values during steroid therapy
DISCUSSION
Docetaxel is a well‐known cytotoxic agent frequently used to treat various cancers, including NSCLC. Docetaxel promotes the polymerization (and inhibits the depolymerization) of microtubes that interfere with cell division. It causes several side‐effects including myelosuppression, peripheral effusion, myalgias, arthralgias, and neuropathy. 1 However, myositis (direct muscle inflammation) is rare; there are only a few case reports.
Myositis can develop due to injury, infection, certain medications, toxin ingestion, exercise, autoimmune diseases, diabetes mellitus, or paraneoplastic syndrome. 1 Our patient was not injured and had not exercised to excess. Dermatomyositis is associated with certain skin lesions such as a heliotropic rash, Gottron papules, a shawl sign, and/or erythematous plaques. Dermatomyositis is often evident on initial cancer presentation and improves with treatment. 2 , 3 Our patient lacked any specific sign of dermatomyositis, and all autoantibody tests were negative. Pyomyositis is a rare cause of muscle pain and swelling triggered by a deep muscular infection, accompanied by fever and leukocytosis. Our patient had a high fever and leukocytosis, but MRI did not reveal an abscess. Statin‐induced myopathy can range from myalgia (muscle pain without CPK elevation) to myositis (muscle inflammation with CPK elevation). However, statin‐induced myositis is extremely rare (rate of <0.001%). 1 In our patient, the statin was stopped during hospitalization and not restarted. Although statin‐induced myositis can develop at any time, the temporal association between docetaxel treatment and myopathy suggests that docetaxel‐induced myopathy is the more likely diagnosis.
Docetaxel‐induced myositis has been described in six case reports (Table 1). 1 , 4 , 5 , 6 , 7 , 8 The patient characteristics were similar among all of the reports. First, myositis developed within the first four docetaxel cycles. Second, myositis affected the lower limbs. Third, all cases (except one for whom data were lacking) had diabetes mellitus. However, only our case exhibited a high fever. Three of the other six cases were afebrile; data were lacking for the others. The cause of the fever remains unknown, but the peak CPK level was higher than those of the six previous cases, indicating strong inflammation that may have triggered the fever.
TABLE 1.
Literature review of previous reported cases of docetaxel‐induced myositis
| Case | Sex, age(years) | Comorbidities | Tumor site | Chemotherapy regimen | Times of DT administration | Myositis location | Treatment |
|---|---|---|---|---|---|---|---|
| Alexandros S. et al. 4 | M, 57 | Hypertension, diabetes | Lung | Docetaxel, Gemcitabine | 4 cycles | Lower limbs | methylprednisolone |
| Hughes et al. 7 | F, 47 | Hypertension, diabetes | Breast | Docetaxel | 1 cycle | Proximal legs | dexamethasone |
| Rajeev Saini D. et al. 6 | F, 62 | Hypertension, diabetes | Breast | Docetaxel, Carboplatin | 2 cycles | Lower limbs | prednisolone |
| Alexandra Perel‐Winkler et al. 1 | F, 65 | Hypertension, diabetes | Breast | Docetaxel, Cyclophosphamide | 3 cycles | Right thigh | prednisolone |
| Philippe Rochigneux et al. 8 | M, 52 | diabetes | Prostate | Docetaxel | 2 cycles | Lower limbs / left arm | Morphinic |
| Girish Kumar Parida et al. 5 | F, 44 | unknown | Breast | Docetaxel, transtuzumab | 4 cycles | Shoulder / hip | Prednisolone |
| This case | M, 66 | Hypertension, diabetes | Lung | Docetaxel | 2 cycles | Both thighs | Prednisolone |
In all but one described case, systemic steroids were started after chemotherapy was discontinued. In our case, PSL relieved the fever and thigh pain, and reduced the CPK level.
Studies on diabetic myonecrosis have shown that time to resolution doubled from 29 to 60 days after biopsy was performed. In our case, muscle biopsy was not performed due to the disadvantage of muscle biopsy. There is no biopsy to support the diagnosis of myositis both in our case and in other published cases. To date, the mechanism of docetaxel‐induced myositis is unclear due to the small sample size and the lack of biopsy reports. However, it may become clear in future clinical practice as the cases of docetaxel‐induced myositis increases.
In conclusion, docetaxel‐induced myositis is a rare but severe side‐effect. Clinicians should consider this possibility when patients complain of muscle pain or the CPK level is elevated.
CONFLICT OF INTEREST
The authors have nothing to disclose.
Ishida A, Ushio A, Hashimoto M, Ishii S, Naka G, Iikura M, et al. A rare case of docetaxel‐induced myositis in a patient with a lung adenocarcinoma. Thorac Cancer. 2022;13(14):2075–2077. 10.1111/1759-7714.14480
REFERENCES
- 1. Perel‐Winkler A, Belokovskaya R, Amigues I, Larusso M, Hussain N. A case of docetaxel induced myositis and review of the literature. Case Rep Rheumatol. 2015;795242:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Callen JP. Myositis and malignancy. Curr Opin Rheumatol. 1996;6(6):590–4. [DOI] [PubMed] [Google Scholar]
- 3. Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208–15. [DOI] [PubMed] [Google Scholar]
- 4. Ardavanis AS, Ioannidis GN, Rigatos GA. Acute myopathy in a patient with lung adenocacrinoma treated with gemcitabine and docetaxel. Anticancer Res. 2005;25:523–6. [PubMed] [Google Scholar]
- 5. BGM H, Stuart‐Harris R. Docetaxel‐induced myositis: report of a novel side‐effect. Intern Med J. 2005;35:369–270. [DOI] [PubMed] [Google Scholar]
- 6. Saini R, Chandragouda D, Talwar V, Rajpurohit S. Grade IV myositis: a rare complication of docetaxel. J Can Res Ther. 2015;11:664. [DOI] [PubMed] [Google Scholar]
- 7. Rochigneux P, Schleintiz N, Ebbo M, Aymonier M, Pourroy B, Boissier R, et al. Acute myositis: an unusual and severe side effect of docetaxel: a case report and literature review. Anticancer Drugs. 2018;29:477–81. [DOI] [PubMed] [Google Scholar]
- 8. Parida GK, Upadhyay A, Mitra S, Suman A, Muthu GS, et al. Rare case of docetaxel‐induced myositis detected on fluorodeoxyglucose positron emission tomography/computed tomography in a patient with carcinoma breast. Indian J of Nucl Med. 2020;35:248–50. [DOI] [PMC free article] [PubMed] [Google Scholar]