

Abstract
Introduction
After extensive research, this study explored whether high‐dose prescriptions and polypharmacy remain more frequent in Japan than elsewhere. If confirmed, we aimed to identify the factors that contributed to this unique trend.
Methods
The psychotropic drug prescription patterns for patients with schizophrenia in Japan were reviewed. This was based on a large sample collected from surveys of the Research on Asian Psychotropic Prescription Patterns, an international collaborative research project conducted by Asian psychiatrists to monitor prescriptions of psychotropic drugs for people with mental disorders, in 2001, 2004, 2008, and 2016.
Results
The 2016 Research on Asian Psychotropic Prescription Patterns survey revealed that Japan continued to demonstrate the highest rate of polypharmacy and the highest dosages of psychotropic prescription drugs for patients with schizophrenia among the 15 countries and areas that participated in the survey.
Discussion
The Research on Asian Psychotropic Prescription Patterns surveys demonstrated that science plays a limited role in the decision‐making process for prescriptions of psychotropic medications. Such prescriptions are influenced by a wide range of factors, such as the national mental health policy, prescription‐financing systems, the history of psychiatry in each country, and the prevailing culture. Hospital‐based national mental health policies and mental health financing systems have been the primary obstacles to reducing polypharmacy in Japan.
Keywords: high‐dose prescription, Japan, polypharmacy, REAP, schizophrenia
1. INTRODUCTION
In 2001, an international collaborative survey, using a uniform research protocol and a common questionnaire, was conducted by Asian psychiatrists. The survey was designated as REAP, which is an acronym for “Research on Asian Psychotropic Prescription Patterns.” REAP examined 2399 prescriptions of inpatients with schizophrenia in six Asian countries and areas: China, Hong Kong, Japan, Korea, Singapore, and Taiwan. High‐dose prescriptions and psychotropic polypharmacy in Japan (Ito et al., 2005) was identified. The average number of psychotropic drugs administered for the treatment of inpatients with schizophrenia in Japan for 627 patients was 5.2 per patient. The average number of antipsychotics administered per patient in Japan was 2.4. The above figures for 2399 patients resulted in an average of 3.4 and 1.6 prescriptions per patient, respectively. The median number of psychotropic and antipsychotic drug prescriptions in Japan was five and two per patient, respectively, while it was three and one per patient, respectively, for the total sample. The chlorpromazine equivalence (CL‐EQ) of antipsychotic prescriptions was the highest in Japan. The average dose of CL‐EQ in Japan was 1003 mg, while the total average dose was 675 mg. The average dose in China is 403 mg. Notably, levomepromazine, known for its strong sedative effects, was prescribed only in Japan (Chong et al., 2004; Ito et al., 2005; Sim et al., 2004). For the first time, these findings provided data regarding high‐dose prescriptions and polypharmacy prescribed by Japanese psychiatrists compared to psychiatrists in other Asian countries. The REAP survey, which was followed up in 2004 and 2008, showed a significant decrease in the CL‐EQ in Japan. However, the CL‐EQ in Japan continued to be the highest among the six countries and areas. This significant decrease from 2001 to 2004 can be attributed to many factors. The revelation of the extremely high dose of CL‐EQ to Japanese psychiatrists could be considered as one of these reasons (Shinfuku & Tan, 2008; Tan et al., 2008; Yoshimura et al., 2006).
The third survey was conducted in 2008. In addition to the original six countries and areas, India, Malaysia, and Thailand participated in the third survey. All investigators collected data based on the same unified questionnaire‐based research protocol. More than 2000 prescriptions each in 2001, 2004, and 2008 were examined. This resulted in a total number of more than 6000 prescriptions. These data were analyzed and compared (López‐Muñoz et al., 2013; Xiang, Kreyenbuhl, Dickerson, Ungvari, Wang, Si, Lee, Chiu, et al., 2012; Xiang, Kreyenbuhl, Dickerson, Ungvari, Wang, Si, Lee, He, et al., 2012). The REAP surveys in 2001, 2004, and 2008 revealed a large international variation in the antipsychotic prescription patterns for individuals with schizophrenia (Ito et al., 2012). The highest doses of psychotropic prescriptions and the highest rates of polypharmacy, per the three surveys, were observed in Japan.
The survey results also showed a high rate of adjunctive use of mood stabilizers, benzodiazepines, and anticholinergic drugs in patients with schizophrenia in Japan (Sim et al., 2011; Tor et al., 2011; Xiang et al., 2011a). Low‐dose antipsychotic drug use was uncommon in Japan, where many patients were long‐term inpatients (Sim et al., 2009). The survey also revealed low recognition of extrapyramidal side effects and a low frequency of reported sexual dysfunction in Asian patients with schizophrenia (Xiang et al., 2011b; Xiang, Dickerson, Kreyenbuhl, Ungvari, Wang, Si, & Chong, 2012d). From 2001 to 2008, there was a major shift from first‐generation antipsychotics to second‐generation antipsychotics (SGA) in all participating countries (Figure 1).
FIGURE 1.
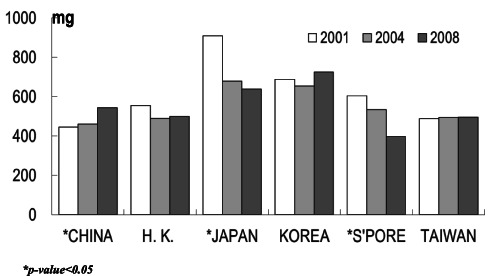
Mean doses of antipsychotics (in CPZ equivalent means*) 2001–2004–2008
The introduction of SGAs resulted in a novel side effect (Xiang et al., 2015). Patients in Japan were no exception to this situation. The three REAP surveys in 2001, 2004, and 2008 revealed continuous antipsychotic polypharmacy in patients with schizophrenia in several Asian countries (Xiang, Dickerson, Kreyenbuhl, Ungvari, Wang, Si, & Chong, 2012d; Xiang, Wang, Si, Lee, He, Ungvari, & Kua, 2012). In addition, the excessive use of adjunctive mood stabilizers and benzodiazepines was continuously observed among older Asian patients with schizophrenia (Xiang, Dickerson, Kreyenbuhl, Ungvari, Wang, Si, & Chong, 2012e). The survey showed that the availability of a specific drug differed greatly between countries. A significant difference was observed when comparing prescription patterns between China and Japan. China used clozapine as the drug of first choice, and the rate of polypharmacy was low, whereas clozapine has not yet been prescribed in Japan. Certain drugs are marketed in some Asian countries and areas, but not in others (Xiang et al., 2017).
The results of the three REAP surveys (2001, 2004, and 2008) that included patients with schizophrenia in Asia showed that Japan had a significant high‐dose antipsychotic prescription trend and a higher frequency of polypharmacy.
2. METHODS
The psychotropic prescription patterns for patients with schizophrenia in Japan were reviewed based on the 2016 REAP survey (Yang et al., 2018), which was a follow‐up survey of the previous REAP surveys conducted in 2001, 2004, and 2008. The REAP survey in 2016 was designed as a hospital‐based cross‐sectional survey to examine the prescription patterns of psychotropic drugs used for inpatients and outpatients in Asia. Data from outpatients were included for the first time in 2016. The research protocol and questionnaire were reviewed and agreed upon by all REAP members. The participants were both inpatients and outpatients with schizophrenia, diagnosed based on either the International Statistical Classification of Diseases and Related Health Problems 10th version (ICD‐10) or the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM‐4). ICD‐10 is used as a basic tool for psychiatric diagnoses. The DSM‐4 has also been used in countries where the ICD system is not commonly used in clinical practice. The Anatomical Therapeutic Chemical system, developed by the World Health Organization, was used to classify psychotropic drugs prescribed by REAP members (Dong, Zeng, Zhang, Ungvari, Ng, Chiu, et al., 2019; Dong, Zeng, Zhang, Yang, Chen, Najoan, et al., 2019; Dong, Zeng, Zhang, Yang, Chen, Sim, et al., 2019). Each participating country was asked to provide 100–500 prescriptions of patients with schizophrenia, depending on the size of their psychiatric resources. The REAP studies were approved by the institutional review boards of all participating centers in each country. A total of 15 countries and areas in Asia participated in the 2016 REAP survey. In addition to the countries and areas that participated in the previous surveys, Bangladesh, Indonesia, Myanmar, Sri Lanka, Pakistan, and Vietnam were included in 2016. The number of prescriptions collected by each participating country or area is attached. Indonesia, India, Taiwan, Malaysia, and Japan collected information on the Brief Psychiatric Rating Scale, Drug Induced Extra‐Pyramidal Symptoms Scale comorbidity, and laboratory data, in addition to the standard requirements.
Table 1 shows the number of prescriptions, number of psychiatrists, and the centers that contributed to the surveys in 2001, 2004, 2008, and 2016.
TABLE 1.
REAP‐AP1, 2, 3, and 4: Participating countries and areas
| Prescription | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2001 | 2004 | 2008 | 2016 | Four surveys all | Psychiatrists | Centers | |||||||||
| Inpatient | Inpatient | Inpatient | Inpatient | outpatient | 2016 All | 2001–2016 | 2001 | 2004 | 2008 | 2016 | 2001 | 2004 | 2008 | 2016 | |
| China | 611 | 504 | 409 | 146 | 14 | 160 | 1684 | 3 | 36 | 3 | 24 | 3 | 4 | 3 | 2 |
| Hong Kong | 108 | 100 | 100 | 31 | 0 | 31 | 339 | 1 | 1 | 10 | 11 | 1 | 1 | 1 | 1 |
| Japan | 627 | 583 | 514 | 129 | 100 | 229 | 1953 | 55 | 77 | 68 | 46 | 10 | 10 | 8 | 8 |
| Korea | 442 | 412 | 284 | 6 | 125 | 131 | 1269 | 51 | 32 | 31 | 17 | 12 | 4 | 4 | 3 |
| Singapore | 300 | 91 | 100 | 128 | 43 | 171 | 662 | 4 | 10 | 2 | 11 | 1 | 1 | 1 | 2 |
| Taiwan | 311 | 446 | 499 | 224 | 179 | 403 | 1659 | 30 | 48 | 58 | 17 | 4 | 5 | 7 | 5 |
| India | 181 | 150 | 329 | 479 | 660 | 5 | 31 | 5 | 5 | ||||||
| Malaysia | 100 | 103 | 202 | 305 | 405 | 2 | 21 | 1 | 10 | ||||||
| Thailand | 39 | 140 | 182 | 322 | 361 | 1 | 51 | 4 | 4 | ||||||
| Bangladesh | 48 | 51 | 99 | 99 | 4 | 1 | |||||||||
| Myanmar | 90 | 74 | 164 | 164 | 25 | 5 | |||||||||
| Pakistan | 142 | 156 | 298 | 298 | 49 | 3 | |||||||||
| Sri Lanka | 50 | 47 | 97 | 97 | 18 | 3 | |||||||||
| Vietnam | 274 | 0 | 274 | 274 | 95 | 10 | |||||||||
| Indonesia | 289 | 292 | 581 | 581 | 66 | 9 | |||||||||
| Total | 2399 | 2136 | 2226 | 1950 | 1794 | 3744 | 10 505 | 144 | 204 | 180 | 486 | 31 | 25 | 34 | 71 |
Note: REAP‐AP 1, 2001; REAP‐AP 2, 2004; REAP‐AP 3, 2008; and REAP‐AP 4, 2016.
In total, 10 505 prescriptions for patients with schizophrenia were collected and analyzed. Notably, in the fourth survey of REAP in 2016, 71 major psychiatric research institutes and more than 400 psychiatrists from 15 countries and areas in Asia contributed to the collection of 3744 prescriptions for patients with schizophrenia.
3. RESULTS
A total of 15 countries and areas in Asia joined the REAP survey in 2016, and 3744 prescriptions of persons with schizophrenia were collected and analyzed.
The REAP survey in 2016 revealed that Japan continued to have the highest rate of polypharmacy and the highest dosages of psychotropic drugs among the 15 countries and areas that participated in the survey (Yang et al., 2018).
Japan continued this trend in the 2016 REAP survey and showed a high rate of polypharmacy. More than 50% of patients with schizophrenia received more than two antipsychotics. However, our REAP data from 2001 to 2016 showed a continuous decrease in the trend for polypharmacy of antipsychotics in Japan (Dong, Zeng, Zhang, Yang, Chen, Sim, et al., 2019; Yang et al., 2018).
The average prescribed daily doses/defined daily dose (PDD/DDD) of antipsychotic use for all 3744 cases was 1.5, with Japan showing the highest PDD/DDD rate (2.29) (Lin et al., 2018). The average psychotropic drug loading for all cases was 2.02. Japan had the highest level at 4.13. The dose of psychotropic drugs in Japan was the highest in the 2016 survey among the 15 countries and areas (Figure 2).
FIGURE 2.
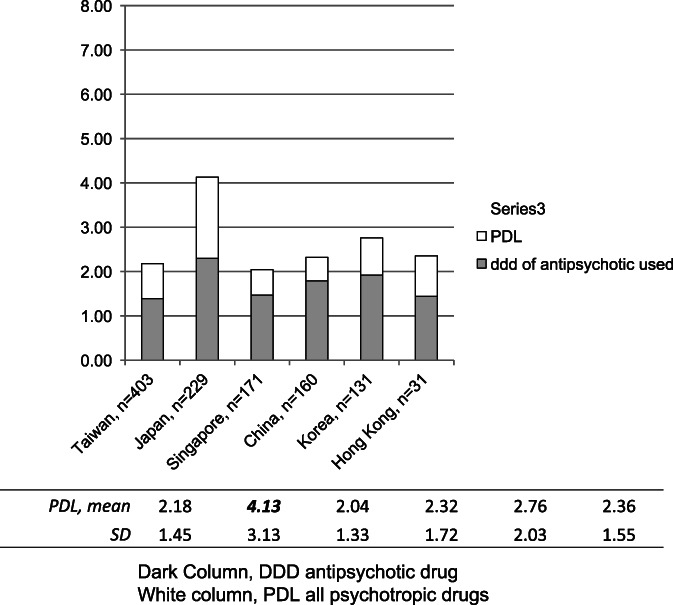
Comparison of psychotropic drug load between countries 2016
In addition to antipsychotic polypharmacy, frequent use of other psychotropic drugs was observed in Japan. Of the 3744 patients with schizophrenia, mood stabilizers were prescribed to 523 patients (14.0%). The combined use of mood stabilizers was high in Japan (30.1%). The rate of combined use with antidepressants was 12.0% for all patients. In Japan, only six cases out of 229 cases (2.6%) were prescribed antidepressants. This indicated that Japanese psychiatrists more frequently prescribed mood stabilizers than antidepressants as combination drugs to patients with schizophrenia (Dong, Zeng, Zhang, Yang, Chen, Najoan, et al., 2019).
The number of combined prescriptions with anxiolytics was 1044 (27.9%) for all cases. In Japan, 73 patients (total 229) with schizophrenia received anxiolytics, with a rate of 31.9%, which was slightly higher than the average value. Of all cases (total 3744), hypnotics were prescribed to 9.3% of patients with schizophrenia. In Japan, 140 out of 229 patients (61.1%) received hypnotics. This rate is the highest among all the countries and areas that participated in the survey (Dong, Zeng, Zhang, Ungvari, Ng, Chiu, et al., 2019).
4. DISCUSSION
4.1. Prescription surveys in Europe and the United States
In Europe and the United States, issues related to prescription behavior have often been highlighted. Gallego et al. conducted a systematic review of psychotropic prescription patterns in Europe, North America, Asia, and Oceania based on 147 research papers published between 1970 and 2009. The review showed a high prevalence of polypharmacy in Asia (Gallego et al., 2012). During the 40 years of this review period, North America was characterized by a lower rate of polypharmacy of antipsychotic drugs, a higher rate of combined prescription with mood stabilizers and antiepileptic drugs, and a lower rate of combined use with anticholinergics compared with those of other regions. European countries revealed a higher rate of antipsychotic polypharmacy, frequent use of anxiolytics and antidepressants, and fewer combined use of anticholinergic drugs. The average polypharmacy rate of antipsychotic drugs was approximately 20% for all regions throughout the survey duration. The polypharmacy rate in each region was 15% in North America, 32% in Asia, 23% in Europe, and 16% in Oceania. In the past 20 years, polypharmacy has decreased in Asia.
4.2. Polypharmacy in Asia
The REAP surveys demonstrated that the prescription of psychotropic drugs was influenced by several factors: the mental health service system, the mental health financing systems, and the training of psychiatrists. These factors contribute to the actual prescription decision‐making process (Dong, Zeng, Zhang, Ungvari, Ng, Chiu, et al., 2019; Dong, Zeng, Zhang, Yang, Chen, Najoan, et al., 2019; Dong, Zeng, Zhang, Yang, Chen, Sim, et al., 2019; Yang et al., 2018). There is a huge difference in the number of mental health resources among the countries that participated in the REAP surveys. Japan has more than 300 000 psychiatric beds in more than 1600 hospitals. Most of these hospitals are privately owned, and more than half of the patients stay at these hospitals for more than 1 year. Therefore, data from Japan include prescriptions for patients with chronic‐stage schizophrenia. Another sampling bias is related to the financing system governing the use of psychotropic drugs. The financing of drugs was significantly different among the 15 countries. The national insurance system in Japan allows psychiatrists to prescribe psychotropic drugs at their discretion without limitations. On the other hand, in countries with limited financial resources, governments control drug expenditures at public hospitals. Psychiatrists are directed to prescribe the minimum amount of psychotropic drugs with the most reasonable prices for cost containment purposes. Additionally, psychiatrists in countries with limited mental health resources are prohibited from prescribing expensive newly introduced psychotropic drugs. When analyzing the REAP data, it is necessary to consider the possible bias resulting from the various mental health financing systems in each Asian country.
4.3. Polypharmacy and high‐dose prescriptions in Japan
The survey findings illustrate that high‐dose prescriptions and polypharmacy continue to be observed more frequently in Japan than elsewhere. These findings are the result of extensive research collected over the past few decades. There are many reasons why psychiatrists in Japan continue to prescribe polypharmacy and high doses of psychotropics. Possible contributing factors are the mental health service system, various stigmas, the national insurance system, physician's culture, patient's attitude, and lack of training in psychopharmacology.
4.3.1. The mental health service system
Japan is known for its unique mental health service system. There are more than 1600 psychiatric hospitals, and more than 90% of patients are hospitalized in privately owned hospitals (Shinfuku, 1998; Shinfuku, 2017). In addition, inpatients with schizophrenia remain hospitalized for extended periods of time. Approximately 100 000 patients stay for more than 1 year (Shinfuku, 2017). Extended‐stay patients tend to receive polypharmacy and high doses of psychotropics. The examples collected by Japanese psychiatrists are representative of a cohort of Japanese inpatients. The rate of polypharmacy decreased slightly from 2001 to 2004 and from 2004 to 2008 (Chong et al., 2004; Shinfuku & Tan, 2008; Xiang, Kreyenbuhl, Dickerson, Ungvari, Wang, Si, Lee, Chiu, et al., 2012; Xiang, Kreyenbuhl, Dickerson, Ungvari, Wang, Si, Lee, He, et al., 2012).
4.3.2. Stigma
There is a concealed strong stigma toward individuals with schizophrenia in Japanese society. The stigma toward patients with mental disorders is deeply rooted in Japanese history. It has been and remains a source of shame for a family to have a member with schizophrenia Therefore, once hospitalized, family members are reluctant to have a sick family member return home (Shinfuku, 1998). They prefer to hide the patient far from the eyes of the community for as long as possible. In Japanese history, individuals with schizophrenia are considered to be dangerous and exhibit bizarre behavior. It is difficult for individuals with schizophrenia to find work post‐discharge. Rehabilitation facilities are poorly developed in the Japanese mental health service system. Given these circumstances, the major objective of pharmacotherapy is the sedation of patients with abnormal behavior, such as aggression. After each episode of abnormal behavior, various types and dosages of medications are added. In the long run, patients with schizophrenia receive polypharmacy and high doses of psychotropic drugs (Shinfuku, 2017).
4.3.3. National insurance system
The Japanese national insurance system has also contributed to polypharmacy and the high dosages of prescriptions. In 1961, the national medical insurance system began to cover and subsidize all medical costs. Generally, medical insurance covers the hospitalization fee for patients with schizophrenia who are hospitalized for extended periods. In the case of private psychiatric hospitals, it is desirable for patients to stay longer. Most of the hospital fees are covered by the national insurance system and other public funding. Families and patients are often exempt from paying for hospitalization costs. The greater the number of patients and the longer their stay, the greater is the financial stability of a private psychiatric hospital. This system encourages polypharmacy and high‐dose prescriptions. Medical fees, including the cost of prescription drugs, are covered by the national insurance system. It is notable that the owner of the hospital may receive a larger reimbursement if the physician prescribes several drugs at higher doses.
4.3.4. Physician's culture
In Japan, the culture surrounding physicians is an important contributing factor to the high dose of prescription medications and polypharmacy. The right of medical doctors to prescribe drugs is protected by law. Few mechanisms exist to control the number of prescriptions.
Furthermore, a weak verification system exists, and it does not prevent polypharmacy and high‐dose prescriptions. The majority of extended‐stay patients receive several drugs for various complaints such as psychotic symptoms, depressive moods, insomnia, and irritability. They are prescribed by different doctors. It is easy to increase the number of drugs prescribed. However, it is cumbersome to reduce the number of previously prescribed drugs. Moreover, it is considered inappropriate for young doctors to discontinue a drug prescribed by senior doctors. When a young doctor wants to change a prescription, the only way is to add a new drug. This Japanese culture of respect for seniority may result in long‐term polypharmacy and high‐dose prescriptions.
4.3.5. Patient's attitude
Japanese patients tend to receive numerous drugs. In traditional herbal medicine, multiple drugs increase the medication's potency and efficacy. Certain Japanese people believe that drugs are good and that multiple drugs are better. This encourages physicians to prescribe high doses of drugs and use polypharmacy. Some experts mention traditional medicine as the origin of polypharmacy. One Chinese herbal medicine typically contains 5–10 ingredients. The philosophy behind polypharmacy is that a higher number of drugs are more effective.
4.3.6. Lack of training in psychopharmacology
The REAP survey results demonstrate poor recognition of the side effects of drugs prescribed by Asian psychiatrists, and Japanese psychiatrists were no exception. The dangers of high‐dose prescriptions and polypharmacy are not sufficiently understood by Japanese psychiatrists. One REAP study showed a rather low recognition of drug side effects by Asian psychiatrists (Xiang et al., 2011a, 2011b; Xiang et al., 2015). This may be true for Japanese psychiatrists as well.
Side effects are not sufficiently considered when a doctor prescribes a new drug. When a doctor adds a psychotropic drug, the existing drug should be reduced. However, this is seldom practiced, and results in polypharmacy and high‐dose prescriptions. Excessive intake of psychotropic drugs damages both the patient's mind and body.
4.3.7. Market factors
Additional factors in the actual decision‐making process for prescribing psychotropic drugs may exist, including the marketing and advertising of drugs. Psychiatrists are urged to prescribe newly approved antipsychotics/psychotropics. It is notable that a number of new drugs entered Asian markets in 2001 (López‐Muñoz et al., 2013; Xiang, Kreyenbuhl, Dickerson, Ungvari, Wang, Si, Lee, Chiu, et al., 2012; Xiang, Kreyenbuhl, Dickerson, Ungvari, Wang, Si, Lee, He, et al., 2012).
4.4. Efforts to improve prescriptions in Japan
Prescription guidelines and scientific data play a limited role in decisions regarding actual prescriptions. In the past 20 years, Japanese psychiatrists have introduced prescription guidelines developed in Europe and the United States to reduce polypharmacy. At present, most Japanese psychiatrists are well aware of the harmful effects of polypharmacy and high‐dose prescriptions. Nevertheless, most patients with schizophrenia continue to receive polypharmacy and high‐dose prescriptions. There are some limitations to reducing polypharmacy and high‐dose prescriptions, including the efficacy of the prescription guidelines and the ethical behavior of the psychiatrist. Past efforts to reduce polypharmacy on a scientific basis can be summarized as having had a limited impact on clinical practice.
The Ministry of Health, Welfare, and Labor introduced changes in the payment system to prevent polypharmacy. However, these do not address high‐dose prescriptions (Hirano & Ii, 2019).
4.5. What we have learned and what should we focus on?
The REAP surveys have demonstrated that science plays a limited role in the decision‐making process for psychotropic prescriptions. These decisions are influenced by a wide range of factors, such as the national mental health policy, financing systems for prescription drugs, and the history of psychiatry in each country as well as the prevailing culture. Hospital‐based national mental health policy and mental health financing systems have been the primary obstacles to reducing polypharmacy in Japan. The development of mental health services in communities separate from hospitals is a prerequisite. High‐dose prescriptions and polypharmacy will continue as long as large numbers of extended‐stay patients with schizophrenia remain in custodial psychiatric hospitals. The situation in Japan clearly demonstrates the abuse of polypharmacy. However, there has been a change in the focus of pharmacotherapy from sedation to rehabilitation. Further training and education of psychiatrists on the side effects of psychotropic medications is essential.
CONFLICT OF INTEREST
The author declares no conflicts of interest.
ACKNOWLEDGMENTS
The REAP surveys were supported by research funds from: (1) Japan Society for Promotion of Science, Japan, (2) Institute of Mental Health, Singapore (CRC 249/2008; Grant 013/2001), (3) Taiwan Bureau of National Health Insurance (DOH92‐NH‐1025); (4) Chang Gung Memorial Hospital (CMRPG83043); and (5) Taipei City Government, Taiwan (97001‐62‐01; 10501‐62‐0120). The author thanks all Asian psychiatrists and pharmacologists who have supported REAP surveys over the past 20 years. Special thanks go to Prof. Shu‐Yu Yang, Taipei City Hospital. Taiwan for her assistance in preparing table and figure.
Shinfuku, N. (2022). Analysis of the trends of polypharmacy and high‐dose prescriptions in Japan. Asia‐Pacific Psychiatry, 14(1), e12488. 10.1111/appy.12488
Funding information Taipei City Government, Taiwan, Grant/Award Numbers: 10501‐62‐0120, 97001‐62‐01; Chang Gung Memorial Hospital, Grant/Award Number: CMRPG83043; Taiwan Bureau of National Health Insurance, Grant/Award Number: DOH92‐NH‐1025; Institute of Mental Health, Singapore, Grant/Award Numbers: 013/2001, CRC 249/2008; Japan Society for Promotion of Science, Japan
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available in the publication list at the REAP homepage website (http://www.reap.asia).
REFERENCES
- Chong, M. Y. , Tan, C. H. , Fujii, S. , Yang, S. Y. , Ungvari, G. S. , Si, T. , Chung, E. K. , Sim, K. , Tsang, H. Y. , & Shinfuku, N. (2004). Antipsychotic drug prescription for schizophrenia in East Asia: Rationale for change. Psychiatry and Clinical Neurosciences, 58, 61–67. 10.1111/j.1440-1819.2004.01194.x [DOI] [PubMed] [Google Scholar]
- Dong, M. , Zeng, L.‐N. , Zhang, Q. , Ungvari, G. S. , Ng, C. H. , Chiu, H. F. , Si, T.‐M. , Sim, K. , Avasthi, A. , Grover, S. , Chong, M.‐Y. , Chee, K.‐Y. , Kanba, S. , Lee, M.‐S. , Yang, S.‐Y. , Udomratn, P. , Kallivayalil, R. A. , Tanra, A. J. , Maramis, M. , … Xiang, Y.‐T. (2019). Concurrent antipsychotic use in older adults treated with antidepressants in Asia. Psychogeriatrics, 19, 333–339. 10.1111/psyg.12416 [DOI] [PubMed] [Google Scholar]
- Dong, M. , Zeng, L. N. , Zhang, Q. , Yang, S. Y. , Chen, L. Y. , Najoan, E. , Kallivalayil, R. A. , Viboonma, K. , Jamaluddin, R. , Javed, A. , Hoa, D. T. Q. , Iida, H. , Sim, K. , Swe, T. , He, Y. L. , Park, Y. , Ahmed, H. U. , De Alwis, A. , Chiu, H. F. K. , … Xiang, Y. T. (2019). Prescription of antipsychotic and concomitant medications for adult Asian schizophrenia patients: Findings of the 2016 research on Asian psychotropic prescription patterns (REAP) survey. Asian Journal of Psychiatry, 45, 74–80. 10.1016/j.ajp.2019.08.010 [DOI] [PubMed] [Google Scholar]
- Dong, M. , Zeng, L. N. , Zhang, Q. , Yang, S. Y. , Chen, L. Y. , Sim, K. , He, Y. L. , Chiu, H. F. , Sartorius, N. , Tan, C. H. , Chong, M. Y. , Shinfuku, N. , Lin, S. K. , Ng, C. H. , Ungvari, G. S. , & Xiang, Y. T. (2019). Antipsychotic polypharmacy in older adult Asian patients with schizophrenia: Research on Asian psychotropic prescription patterns. Journal of Geriatric Psychiatry and Neurology, 32(6), 304–311. 10.1177/0891988719862636 [DOI] [PubMed] [Google Scholar]
- Gallego, J. A. , Bonetti, J. , Zhang, J. , Kane, J. M. , & Correll, C. U. (2012). Prevalence and correlates of antipsychotic polypharmacy: A systematic review and meta‐regression of global and regional trends from the 1970s to 2009. Schizophrenia Research, 138(1), 18–28. 10.1016/j.schres.2012.03.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirano, Y. , & Ii, Y. (2019). Changes in prescription of psychotropic drugs after the introduction of polypharmacy reduction policy in Japan based on a large‐scale claims database. Clinical Drug Investigation, 39(11), 1077–1092. 10.1007/s40261-019-00838-w [DOI] [PubMed] [Google Scholar]
- Ito, H. , Koyama, A. , & Higuchi, T. (2005). Polypharmacy and excessive dosing: psychiatrists' perceptions of antipsychotic drug prescriptions. The British Journal of Psychiatry, 187, 243–247. 10.1192/bjp.187.3.243 [DOI] [PubMed] [Google Scholar]
- Ito, H. , Okumura, Y. , Higuchi, T. , Tan, C. H. , & Shinfuku, N. (2012). International variation in antipsychotic prescription for schizophrenia: Pooled results from research on East Asia psychotropic prescription (reap) studies. Open Journal of Psychiatry, 2, 340–346. 10.4236/ojpsych.2012.224048 [DOI] [Google Scholar]
- Lin, S. K. , Lin, Y. F. , Yang, S. Y. , He, Y. L. , Kato, T. A. , Hayakawa, K. , & Chong, M. Y. (2018). Comparison of the defined daily dose and chlorpromazine equivalent methods in antipsychotic drug utilization in six Asian countries neuropsychiatry, 8(6). [Google Scholar]
- López‐Muñoz, F. , Shinfuku, N. , Shen, W. W. , Moreno, R. , Molina Martín, J. D. D. , Rubio, G. , Huelves, L. , Noriega, C. , Perez Nieto, M. , & Álamo González, C. (2013). Thirty years of scientific research on second‐generation antipsychotic drugs in Japan: A bibliometric analysis. Open Journal of Psychiatry, 3, 18–25. 10.4236/ojpsych.2013.31004 [DOI] [Google Scholar]
- Shinfuku, N. (1998). Mental health services in Asia: International perspectives and challenges for the coming years. Psychiatry and Clinical Neurosciences, 52(3), 269–274. 10.1046/j.1440-1819.1998.00400.x [DOI] [PubMed] [Google Scholar]
- Shinfuku, N. (2017). Mental health system in Japan after the Meiji restoration: Historical observations. Springer. [Google Scholar]
- Shinfuku, N. , & Tan, C. H. (2008). Pharmacotherapy for schizophrenic inpatients in East Asia: Changes and challenges. International Review of Psychiatry, 20, 460–468. 10.1080/09540260802397560 [DOI] [PubMed] [Google Scholar]
- Sim, K. , Chuan Su, H. , Fujii, S. , Yang, S. Y. , Chong, M. Y. , Si, T. , Ling He, Y. , Kee Chung, E. , Huak Chan, Y. , Shinfuku, N. , & Hoon Tan, C. (2009). Low doses of antipsychotic drugs for hospitalized patients with schizophrenia in East Asia: 2004 vs. 2001. International Journal of Neuropsychopharmacology, 12, 117–123. 10.1017/s1461145708009280 [DOI] [PubMed] [Google Scholar]
- Sim, K. , Su, A. , Fujii, S. , Yang, S. Y. , Chong, M. Y. , Ungvari, G. S. , Si, T. , Chung, E. K. , Tsang, H. Y. , Chan, Y. H. , & Heckers, S. (2004). Antipsychotic polypharmacy in patients with schizophrenia: A multicenter comparative study in East Asia. British Journal of Clinical Pharmacology, 58, 178–183. 10.1111/j.1365-2125.2004.02102.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sim, K. , Yong, K. H. , Chan, Y. H. , Tor, P. C. , Xiang, Y. T. , Wang, C. Y. , Lee, E. H. M. , Fujii, S. , Yang, S. Y. , Chong, M. Y. , & Ungvari, G. S. (2011). Adjunctive mood stabilizer treatment for hospitalized schizophrenia patients: Asia psychotropic prescription study (2001–2008). International Journal of Neuropsychopharmacology, 14, 1157–1164. 10.1017/S1461145711000563 [DOI] [PubMed] [Google Scholar]
- Tan, C. H. , Shinfuku, N. , & Sim, K. (2008). Psychotropic prescription practices in East Asia: Looking back and peering ahead current opinion in psychiatry, 21, 645–650. 10.1097/YCO.0b013e32830e6dc4 [DOI] [PubMed] [Google Scholar]
- Tor, P. C. , Ng, T. P. , Yong, K. H. , Sim, K. , Xiang, Y. T. , Wang, C. Y. , Lee, E. H. M. , Fujii, S. , Yang, S. Y. , Chong, M. Y. , & Ungvari, G. S. (2011). Adjunctive benzodiazepine treatment of hospitalized patients with schizophrenia in Asia from 2001 to 2008. International Journal of Neuropsychopharmacology, 14, 735–745. 10.1017/S146114571000163X [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Chiu, H. F. , Ungvari, G. S. , Correll, C. U. , Lai, K. Y. , Wang, C. Y. , & Chong, M. Y. (2015). QTc prolongation in schizophrenia patients in Asia: Clinical correlates and trends between 2004 and 2008/2009. Human Psychopharmacology: Clinical and Experimental, 30(2), 94–99. 10.1002/hup.2458 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Dickerson, F. , Kreyenbuhl, J. , Ungvari, G. S. , Wang, C. Y. , Si, T. M. , & Chong, M. Y. (2012d). Common use of antipsychotic polypharmacy in older Asian patients with schizophrenia (2001–2009). Journal of Clinical Psychopharmacology, 32(6), 809–813. 10.1177/0891988719862636 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Dickerson, F. , Kreyenbuhl, J. , Ungvari, G. S. , Wang, C. Y. , Si, T. M. , & Chong, M. Y. (2012e). Adjunctive mood stabilizer and benzodiazepine use in older Asian patients with schizophrenia, 2001–2009. Pharmacopsychiatry, 45(06), 217–222. 10.1055/s-0031-1301292 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Kato, T. A. , Kishimoto, T. , Ungvari, G. S. , Chiu, H. F. , Si, T. M. , & Shinfuku, N. (2017). Comparison of treatment patterns in schizophrenia between China and Japan (2001–2009). Asia‐Pacific Psychiatry, 9(4), e12277. 10.1111/appy.12277 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Kreyenbuhl, J. , Dickerson, F. B. , Ungvari, G. S. , Wang, C. Y. , Si, T. M. , Lee, E. H. , Chiu, H. F. , Lai, K. Y. , He, Y. L. , & Yang, S. Y. (2012). Antipsychotic treatment in older schizophrenia patients with extrapyramidal side effects in Asia (2001–2009). International Journal of Clinical Pharmacology and Therapeutics, 50, 500–504. 10.5414/cp201683 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Kreyenbuhl, J. , Dickerson, F. B. , Ungvari, G. S. , Wang, C. Y. , Si, T. M. , Lee, E. H. , He, Y. L. , Chiu, H. F. , Yang, S. Y. , & Chong, M. Y. (2012). Use of first‐and second‐generation antipsychotic medications in older patients with schizophrenia in Asia (2001–2009). Australian & New Zealand Journal of Psychiatry, 46, 1159–1164. 10.1177/0004867412453625 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Wang, C. Y. , Si, T. M. , Lee, E. H. M. , He, Y. L. , Ungvari, G. S. , Chiu, H. F. K. , Yang, S. Y. , Chong, M. Y. , Tan, C. H. , & Kua, E. H. (2011a). Use of anticholinergic drugs in patients with schizophrenia in Asia from 2001 to 2009. Pharmacopsychiatry, 44, 114–118. 10.1055/s-0031-1275658 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Wang, C. Y. , Si, T. M. , Lee, E. H. M. , He, Y. L. , Ungvari, G. S. , Chiu, H. F. K. , Yang, S. Y. , Chong, M. Y. , Tan, C. H. , & Kua, E. H. (2011b). The low frequency of reported sexual dysfunction in Asian patients with schizophrenia (2001–2009): Low occurrence or ignored side effects? Human Psychopharmacology: Clinical and Experimental, 26, 352–357. 10.1002/hup.1213 [DOI] [PubMed] [Google Scholar]
- Xiang, Y. T. , Wang, C. Y. , Si, T. M. , Lee, E. H. M. , He, Y. L. , Ungvari, G. S. , & Kua, E. H. (2012). Antipsychotic polypharmacy in inpatients with schizophrenia in Asia (2001–2009). Pharmacopsychiatry, 45(01), 7–12. 10.1055/s-0031-1286345 [DOI] [PubMed] [Google Scholar]
- Yang, S.‐Y. , Chen, L. Y. , Najoan, E. , Kallivayalil, R. A. , Viboonma, K. , Jamaluddin, R. , & Swe, T. (2018). Polypharmacy and psychotropic drug loading in patients with schizophrenia in Asian countries: A fourth survey of research on Asian prescription patterns on antipsychotics. Psychiatry and Clinical Neurosciences, 72(8), 572–579. 10.1111/pcn.12676 [DOI] [PubMed] [Google Scholar]
- Yoshimura, R. , Okamoto, T. , Nakamura, J. , Tateno, M. , Otsuka, K. , Takahashi, H. , Fujisawa, D. , Takamatsu, T. , Fujii, S. , Sato, S. , Inoue, M. , Sasaki, H. , Kuroki, T. , & Shinfuku, N. (2006). Prescription pattern of antipsychotic drugs for inpatients with schizophrenia in Japan: Research on East Asia psychotropic prescription pattern‐antipsychotics study. Psychiatry and Clinical Neurosciences, 60, 778779. 10.1111/j.1440-1819.2006.01601 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are openly available in the publication list at the REAP homepage website (http://www.reap.asia).