

Abstract
Suicide is the second leading cause of death among youth ages 10–19 in the USA. While suicide has long been recognized as a multifactorial issue, there is limited understanding regarding the complexities linking adverse childhood experiences (ACEs) to suicide ideation, attempt, and fatality among youth. In this paper, we develop a map of these complex linkages to provide a decision support tool regarding key issues in policymaking and intervention design, such as identifying multiple feedback loops (e.g., involving intergenerational effects) or comprehensively examining the rippling effects of an intervention. We use the methodology of systems mapping to structure the complex interrelationships of suicide and ACEs based on the perceptions of fifteen subject matter experts. Specifically, systems mapping allows us to gain insight into the feedback loops and potential emergent properties of ACEs and youth suicide. We describe our methodology and the results of fifteen one-on-one interviews, which are transformed into individual maps that are then aggregated and simplified to produce our final causal map. Our map is the largest to date on ACEs and suicide among youth, totaling 361 concepts and 946 interrelationships. Using a previously developed open-source software to navigate the map, we are able to explore how trauma may be perpetuated through familial, social, and historical concepts. In particular, we identify connections and pathways between ACEs and youth suicide that have not been identified in prior research, and which are of particular interest for youth suicide prevention efforts.
Keywords: Fuzzy cognitive map, Knowledge map, Network analysis, Participatory modeling, Suicide
1. Introduction
Suicide is the second leading cause of death, after unintentional injuries, for youth in the USA. 19.1% of all deaths among youth aged 10–14 and 23.2% of all deaths among youth aged 15–19 were suicides. This percentage then marginally decreases across age categories, from 19.3% of all deaths among 20–24-year-old to 3.1% among 45–64-year-old, and it is not among the top ten causes of death for those aged 65 years and above (Heron 2019, p. 10). Between 2009 and 2018, suicide rates among high school youth aged 14–18 years increased by 61.3% (Ivey-Stephenson 2020). The strongest predictors of eventual suicide fatality among youth are suicidal ideation or previous suicide attempt (Plemmons et al. 2018). In an analysis of hospital data from 31 US children’s hospitals, 1.2% of all children’s hospital admissions between 2008 and 2015 were the result of suicide ideation or attempt with the largest annual increase in admissions occurring between 12 and 14 years. Overall hospitalizations due to suicide ideation and attempt more than doubled during this time period (Plemmons et al. 2018). The most recent data from the Centers for Disease Control and Prevention’s (CDC) Youth Risk Behavior Surveillance Survey show that 18.8% of high school students reported having seriously considered attempting suicide and 15.7% reported having made a suicide plan (Ivey-Stephenson 2020). To address the public health challenge of steadily increasing suicide rates among youth (Heron 2019; Ivey-Stephenson 2020; Plemmons et al. 2018; Hedegaard et al. 2020), it is thus essential to understand what drives the increase in youth suicide ideation and implement interventions to reduce ideation and prevent attempts. This challenge partly stems from the complexity of suicide, as it is rarely caused by a single factor (Centers for Disease Control and Prevention 2018). Although suicide has long been recognized as a multifactoral issue (Bilsen 2018; Cleary et al. 2019; Cash and Bridge 2009), there is still limited understanding regarding the complex relationships between the factors contributing to, or affected by, intentional self-harm.
Ideation-to-action theories of suicide such as the Cultural Theory and Model of Suicide (Chu et al. 2010) or the Interpersonal Theory of Suicide (Chu et al. 2017) have enabled important advances to suicidal behaviors (e.g., based on burdensomeness and belongingness, or a threshold of tolerance to life stressors) and continue to provide the foundational framework for modeling studies (Rogers and Joiner 2019). Researchers have also used the social ecological model, which considers the complex interaction of factors at the individual, relationship, community, and societal levels in order to better understand risk and protective factors for suicide and the effect of prevention initiatives targeting these levels of intervention (World Health Organization 2014; Centers for Disease Control and Prevention 2015). However, these theories and frameworks do not cover several of the features that define complex problems such as suicide: nonlinearity (e.g., cumulative stress grows faster than the number of adverse experiences), large number of interrelationships (e.g., across personal, family, community, and societal domains), and loops (i.e., when a change in one factor eventually impacts the same factor).
Several recent studies have each focused on one of these limitations. For instance, the new Fluid Vulnerability Theory of suicide uses nonlinearity, which can explain how suicidal behavior may suddenly emerge without planning (Bryan et al. 2020). System Dynamics models (and their conceptual foundations as causal loop diagrams) have often be applied to injury and violence prevention (Page et al. 2017), allowing the capture of short loops between stages (e.g., an individual may abort suicide planning and go back to ideation before planning again) or longer loops (e.g., attempts reduce fear of death, which fuels capability for suicide and results in more attempts) (Naumann et al. 2019; Chung 2016). Systems maps have also been created to summarize relationships in the form of a network, where key factors within the problem space (e.g., suicide ideation, depression) can be connected when there is a functional dependence from one onto the other (e.g., one factor increases the risk of another). An expert-developed systems map, as studied in this paper, views ‘causality’ as a shared perception among experts that a change in one factor will impact another. Such maps include causal maps, which characterize an impact as either increasing or decreasing another factor. This category is the focus of this paper and will be detailed within the next section. Maps also include ontologies, which characterize relationships between factors in terms of properties, as exemplified by the ontology of Adverse Childhood Experiences (ACEs), which includes 297 factors as varied as emotional neglect, witnessing neighborhood violence, or parental separation (Brenas et al. 2019).1
In this paper, we describe the process for developing a system map of suicide for youth, with the objectives of accounting for a large number of factors and the many loops involved in this problem. Our three specific contributions are as follows:
We combine the benefits of causal loop diagrams of suicide and ontologies of ACEs, as both notions are extensively covered in our system map, thus contributing to the needs for more comprehensive tools guiding suicide prevention planning (Page et al. 2018).
Our system map includes causal weights for most relationships, which allow us to go beyond purely logical qualitative models (e.g., homelessness causes trauma) and support quantitative lines of inquiries (e.g., what are key causes of suicide ideation?) (Brenas and Shaban-Nejad 2020).
The design of a comprehensive map is an ambitious effort that then supports the research community to achieve various goals, from guiding future data collection efforts (Epstein 2008) to navigating the complexity of a large system. In this paper, we exemplify how the map can be utilized via existing network visualization software to quickly identify causes and consequences.
Note that the first objective aforementioned was partially achieved in our extended abstract (Giabbanelli et al. 2021) at the 2021 IEEE/ACM International Conference on Advances in Social Networks Analysis and Mining (ASONAM). This manuscript is a significant extension as we detail the multiple levels of validations used in creating the map (with an emphasis on network structure) and also achieve the last two contributions.
The design of large system maps for complex problems typically faces two obstacles. First, data may come in different types (e.g., qualitative, quantitative risk ratios or odds ratios) and from various sources (e.g., longitudinal studies, meta-reviews). While creating a model from a single type and source of data simplifies the assessment of its validity, our study demonstrates that the fragmentation of data would drastically limit the content of such a model. Consequently, our study uses mixed methods to achieve a large, comprehensive system map: we perform one-on-one mapping interviews with 15 Subject Matter Experts (SMEs) to identify the causal structure, and we use Fuzzy Cognitive Mapping (FCM) to assign causal weights (Firmansyah et al. 2019; Giabbanelli et al. 2012; Mkhitaryan et al. 2020).2 Second, it is challenging to produce and use large system maps. The design of large maps can result in the same construct being inadvertently included under equivalent terminologies (Gupta et al. 2018; Giabbanelli and Tawfik 2019) or failing to notice causal pathways that do not lead to any problem-relevant constructs due to missing connections. Such concerns are often solved by only allowing SMEs to draw causal connections between a small predetermined list of concepts (Giabbanelli et al. 2012; Gray et al. 2015), but this prevents the creation of comprehensive, cross-domain system maps. To illustrate difficulties in usability, consider the Foresight Obesity System map, which was created in 2007 as an expert-developed systems map (similarly to this paper) to understand the relationships between weight-related factors (e.g., pertaining to social psychology, physiology, or the built environment). This “representation of expert opinion on the obesity causal system” (McGlashan et al. 2018) contains over one hundred concepts and three hundred interrelationships (Morris et al. 2018): looking at the whole map on paper sends the message that the problem is complex rather than manageable (Hall et al. 2011), as users view the diagram as an “almost incomprehensible web of interconnectedness [in which] the scale and number of interactions make it difficult to see how one might use it in any practical way to develop systemic approaches” (Siokou et al. 2014). To address such challenges in producing our system map and ensure its usability, we use computational techniques from network science: we automatically analyze the structure of the map and we provide it as an interactive visualization using tools previously tested with policymakers (Giabbanelli and Baniukiewicz 2018; Giabbanelli et al. 2016).
The remainder of this paper is organized as follows. In Sect. 2, we explain our five key steps (Fig. 1): identifying and inviting SMEs, structuring an individual map through one-on-one interviews, assembling the maps into a single one, simplifying it, and finally adding weights through Fuzzy Cognitive Mapping. Methods for validity are summarized within each of these steps. Section 3 presents the system map using our interactive visualization (accessible on the thirdparty repository at https://osf.io/7nxp4/) and details several of the loops that have emerged as a result of our combined SME interviews. Section 4 contextualizes our results and concludes with further suggestions for the use of the map.
Fig. 1.
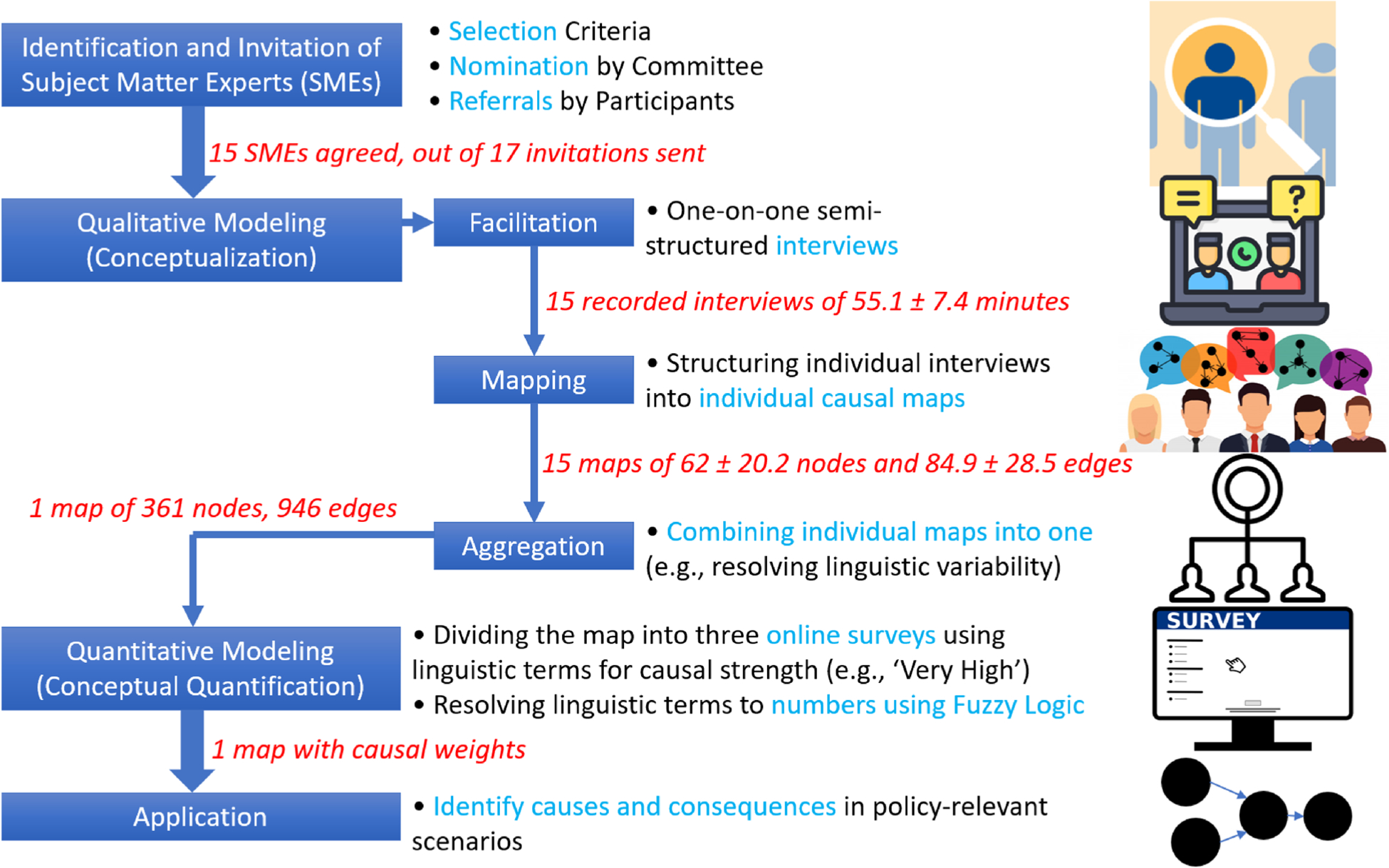
Complete process workflow
2. Methods
2.1. Identification and invitation of subject matter experts
Systematic approaches to identify participants in a participatory modeling study include the application of selection criteria, nomination by a committee, and referral by the participants (i.e., ‘snowball sampling’) (Hedelin et al. 2021). We use these three strategies as follows. Selection criteria for the SMEs included having an established track record in research and public health prevention of suicide and/or ACEs and/or clinical expertise in the therapy and treatment of youth presenting suicidal behavior. The inclusion of therapists, clinical practitioners, and public health experts is essential to obtain a comprehensive coverage of risks and protective factors for suicide, which include but are not limited to ACEs. Our participants were experts within (n = 10) and outside the CDC (n = 5). A track record consists of graduate-level training (e.g., MS, MPH, PhD) and a minimum of 6 years of experience either in research or practice. Based on these criteria, a committee created a purposeful sample of SMEs to ensure we would engage with participants who could communicate experiences and expertise related to suicide in a comprehensive and reflective manner, and who were available and willing to participate within the study time frame. The committee included CDC experts from the National Center for Injury Prevention and Control’s (NCIPC) Division of Injury Prevention Suicide Prevention Team and Division of Violence Prevention Child Abuse Neglect and Adversity Team. Given the cross-sectoral nature of ACEs and suicide risks or preventative factors, the committee assembled an interdisciplinary team of SMEs including behavioral scientists, health scientists and epidemiologists, and physicians. Referrals from participating SMEs served to recruit additional colleagues across other divisions within NCIPC and outside the CDC (i.e., SMEs from other federal agencies, non-profit organizations, private practice, and universities). After each SME was identified, an email invitation was sent with proposed calendar dates within the next two weeks for scheduling.
We note that participatory modeling studies do not have a ‘typical’ or one-size-fits-all number of participants. On the one hand, several studies using mapping and quantification methods have been conducted with fewer than 10 participants (Giabbanelli et al. 2012; van Vliet et al. 2010) or at most 15 (Penn et al. 2013; Henly-Shepard et al. 2015; Isaac et al. 2009) participants. On the other hand, a previous study included 264 participants (Lavin et al. 2018). The number of participants partly depends on the task (Giabbanelli and Tawfik 2020) (e.g., if we want to compare the perspectives of participants and group them, then we may need a larger sample) and the complexity of the problem (e.g., saturation of ideas is obtained faster in problems with a smaller domain space and well-accepted evidence). In line with our previous study on a similar task (developing a map of a system) and cross-disciplinary problem (Firmansyah et al. 2019), we use validation methods (including structural network analysis and assessment of saturation) in each step to ensure that the participatory modeling process is sound.
2.2. One-on-one interviews
A common approach to create a system map with SMEs is to perform semi-structured interviews. Examples include the study of Owen et al. (2018) on obesity with 16 SMEs or our previous study on smart cities (Firmansyah et al. 2019). Interviews can either be performed with a group, which directly leads into a group-level model, or with individuals, whose models are later combined into a single group-level model. Many variables drive the choice of one approach or the other: manpower and associated timeline (the additional work of combining individual models takes longer), the availability of the SMEs (a later combination of individual models requires the SME to provide feedback on the resulting group-level model), the possibility that SMEs have different viewpoints which would need to be preserved (thus avoiding the standardization or power imbalances that occur in a group), or a preference for transparency by tracking how the knowledge of each SME exactly impacts the model (Voinov et al. 2018; Jordan et al. 2018; Andersen et al. 1997). We chose the individual approach as the interdisciplinary nature of suicide research involves SMEs from different fields, thus raising the possibility of individual differences and the need to reflect them into a group-level model. The approach was feasible as SMEs were available for a follow-up and as we included two team members to cope with the additional work of model combination.
Before conducting an individual interview, a mapping approach requires an identification of the problem of interest and a definition of the system’s boundaries (Allender et al. 2019; De Pinho 2017). The problem must be sufficiently isolated to avoid ambiguities, which can lead to seemingly contradictory answers from the SMEs and raise issues in data analysis. Asking “what causes suicide?” would potentially be ambiguous as SMEs may think of different stages, from suicidal thoughts to suicide attempt and completion. In line with other models (Page et al. 2017), we thus decomposed suicide into four problems for the suicide SMEs: suicide ideation, suicide planning, suicide attempt, and suicide. In other words, the causes and consequences of each of the four interrelated problems was discussed during the semi-structured interviews with the suicide SMEs. With experts on ACEs, we set ACEs as the problem of interest. Given different definitions of ACEs in the literature, we did not decompose ACEs into mandatory categories; in other words, each participant was allowed to share their operational definition of ACEs without being restricted to one by the research team.
Complex systems are often highly interactive and cannot be considered fully in isolation. For instance, suicide is partly shaped by the family context, the community, and society. As an analogy, it is difficult to model the behavior of the respiratory system by ignoring the rest of the body, yet the complete body should not be included if the model’s focus is only on breathing (Murray-Smith 2012, p. 10). In our case, we set the boundaries on factors that shape, or are affected by, ACEs and suicide for youth in the U.S. Situations that would not be representative of the target population (e.g., trauma of famine or civil war) were thus considered beyond the scope of this project, similarly to situations encountered in adulthood (e.g., health consequences of ACEs). While the situation of parents was relevant to ACEs and suicide (e.g., mental health in the family, adversity), our model only captures it as it pertains to understanding dynamics in the child. For instance, parental separation or divorce would be relevant for the child, but the complex reasons underlying a divorce would be out of scope for our child focused model.
Each interview is conducted and recorded using WebEx video conferencing after receiving informed consent from the SME. The interview starts with a description of our project, which also serves as an opportunity to reiterate the system boundaries. SMEs are asked if they have any questions, which are then answered either by the modeler (to explain how the interview proceeds and the data are used) or by the project manager (to explain how the interview fits into the portfolio of CDC projects). Then, the interview proceeds with eliciting the map. Our process is briefly described below and shown in Fig. 2. For additional information on the flow of such interviews, we refer the reader to Reddy et al. (2019); for the cognitive underpinnings of the process, we refer to the overview in McNeese and Ayoub (2011).
Fig. 2.
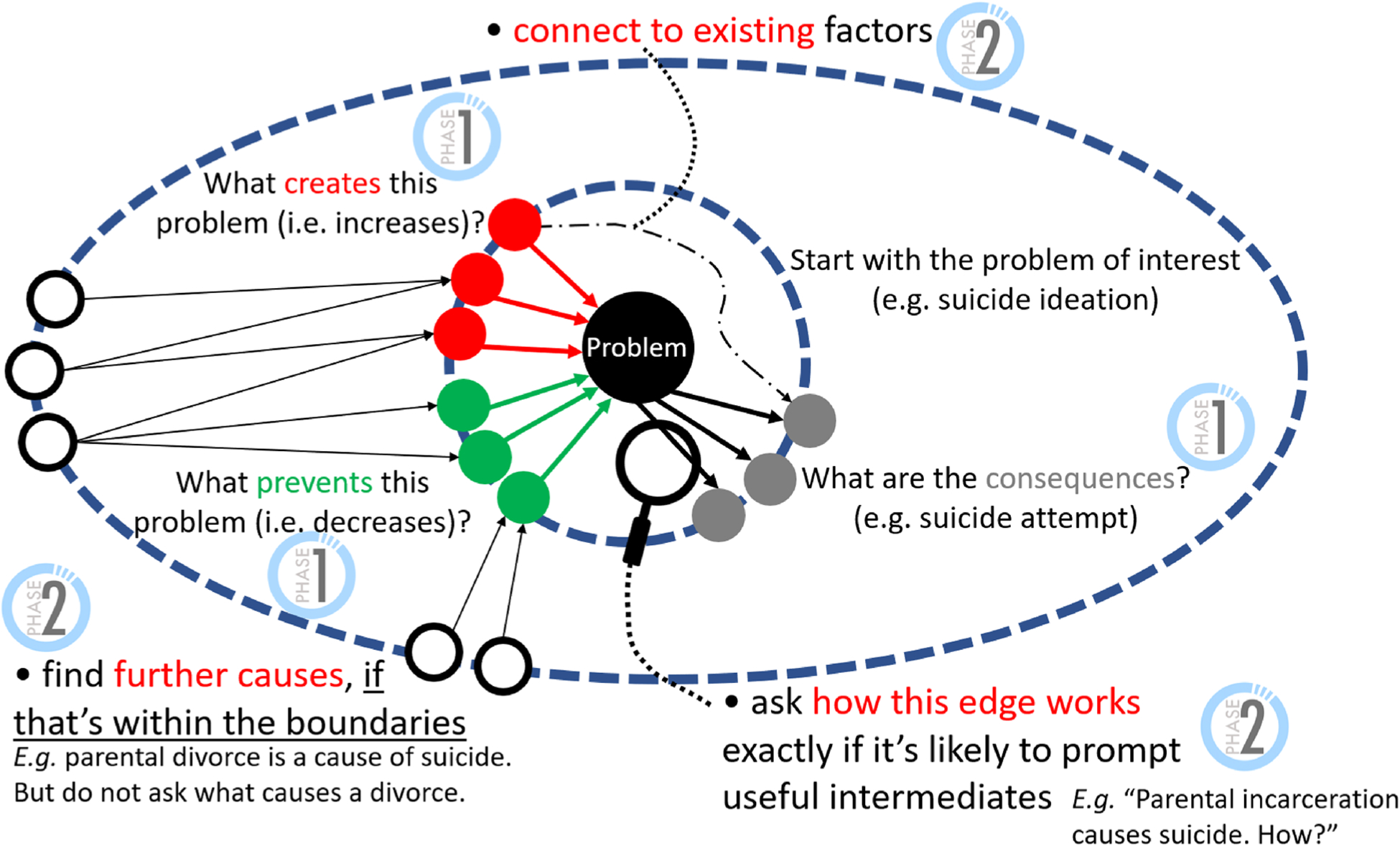
A semi-structured interview starts with immediate causes and consequences for the problem of interest (phase 1). In the next phase, we form connections between the proximal factors, identify intermediate steps, or identify more distal causal drivers
We begin with the problem of interest and systematically ask the participant for causes and consequences, while clarifying with the participant whether the causal link they mentioned leads to an increase (e.g., internalized trauma increases the risk of suicide ideation) or a decrease (e.g., connectedness lowers the risk of suicide ideation). We do not ask confirmatory questions (e.g., “do you think homelessness increases suicide ideation?”), as they may bias an SME in endorsing an idea that would not have otherwise been present in their perspective. The list of factors is frequently read back to the SME such that they can identify any additional ones (e.g., “You mentioned alcohol abuse and mental health in the family—are there any other risk factors in the family?”). Once the proximal causes and consequences are identified, we shift into a second phase to identify mediators, more distal factors, or interrelationships. Questions include identifying how causal links work, particularly where there appears to be a logical gap; forming connections between existing factors; and identifying additional causes. The order in which these questions are asked depends on the conversation, as we avoid ‘jumping’ across parts of the map through successive questions (which can come across as disordered) and instead fully characterize one area before moving onto a closely related one. To establish a positive rapport with each SME, we avoid interrupting them even when they cross the system’s preferred boundaries, and instead bring them back within the boundaries through the next question. One hour was allocated for each interview such that SMEs do not need to be rushed or interrupted by lack of time.
There are several related approaches that elicit the perception of SMEs through an interview and later organize it as a network (Voinov et al. 2018). In a causal map or Causal Loop Diagram (CLD), each causal link has a type (it either increases or decreases its target) and any two factors can be connected by a link. In contrast, mind maps do not have types and only extend radially, while perception graphs also have types but cannot represent loops (Düspohl and Döll 2016). In this project, we use causal maps as this type of causation helps us to better characterize the system and because causal loops are present in complex problems such as suicide (Naumann et al. 2019; Chung 2016). As a causal map summarizes the logical impact of each factor onto others, every relationship has a cause and a consequent. To avoid confusion across disciplines, note that the terminology may differ in studies on suicide, in which a causation is the direct reason for death (e.g., gunshot wounds) while concepts such as ‘parental divorce’ would be categorized as risk factors rather than causes. In addition, the notion of ‘causation’ depends on fields and the context: here, we study the logical connections perceived by subject matter experts (e.g., “in my view, an increase in A will create a change in B”); this participatory approach to determining causation differs from demonstrating causations in health through the use of randomized controlled trials.
As case studies have abundantly demonstrated that cognitive limitations prevent stakeholders from identifying loops (Axelrod 2015), the facilitator actively monitors the structure of the network as the interview unfolds. The network is approximately structured by the modeler during the discussion using MentalModeler (Gray et al. 2013) to track what has been said and prepare the next questions.
We note that an alternative approach is to identify variables and directly connect them, for instance, by drawing them on a circle and asking participants to draw connections as well as specify their type (increasing or decreasing). This approach is feasible and promotes transparency when the causal maps are small, as exemplified by the work of Waqa et al. (2017) in which maps have about 20 connections. When the maps are larger (as in our study where each map averages 83.6 connections), visualizations can be challenging to use for participants; thus, we used the approach of interviewing and then transcribing into maps. That is, only the facilitator sees the ‘sketch’ of the map used to keep track of the conversation; a participant does not see this network during the interview and hence remains focused on the conversation rather than potentially distracted by a visual artifact.
2.3. Transcribing an interview into an individual map
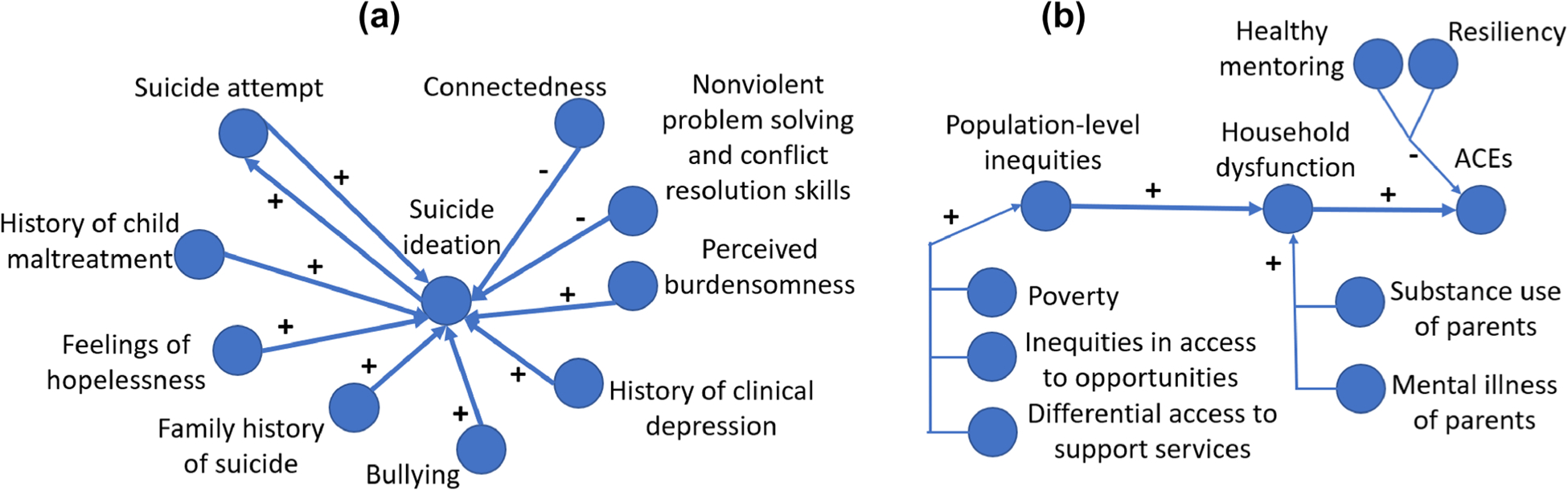
We use the systematic method from Kim and Andersen (2012) to structure a recorded interview into a causal map. We identify the concepts in the discussion (e.g., homelessness, suicide ideation, untreated mental illness in the family) and track their causal connections (e.g., homelessness increases the risk of suicide ideation). In a causal map, concepts are represented as nodes while connections are represented as typed directed edges. In other words, each part of the interview is transformed into a schematic description of a cause variable, an effect variable, and a relationship polarity. Three sample transformations are shown in Fig. 3. In Fig. 3a, the SME provides a list of causes for separation. Rather than simplifying, we capture all such causes, as they may later connect to parts mentioned by other SMEs (e.g. on racial differences in parental incarceration). In Fig. 3b, we note that a causal mechanism may have both a positive and negative impact, which is a common sign that the mechanism depends on additional constructs. Once these constructs are brought into the conversation, we see indirect and direct pathways, which capture the difference between the positive and negative impacts. In Fig. 3c, we note that parts of a conversation may consist of examples or reflections rather than new causal mechanisms, thus not every sentence results in a node or edge. We also strictly use the vocabulary of the SME in a transcription; thus, we would not include the construct of ‘hopelessness’ based on Fig. 3c (“there is no end to it”) until and unless the SME states it. Occasionally, a logical connection is made such as how the ability or barriers to perform a task will impact this task (e.g., the ability to connect impacts connectedness).
Fig. 3.
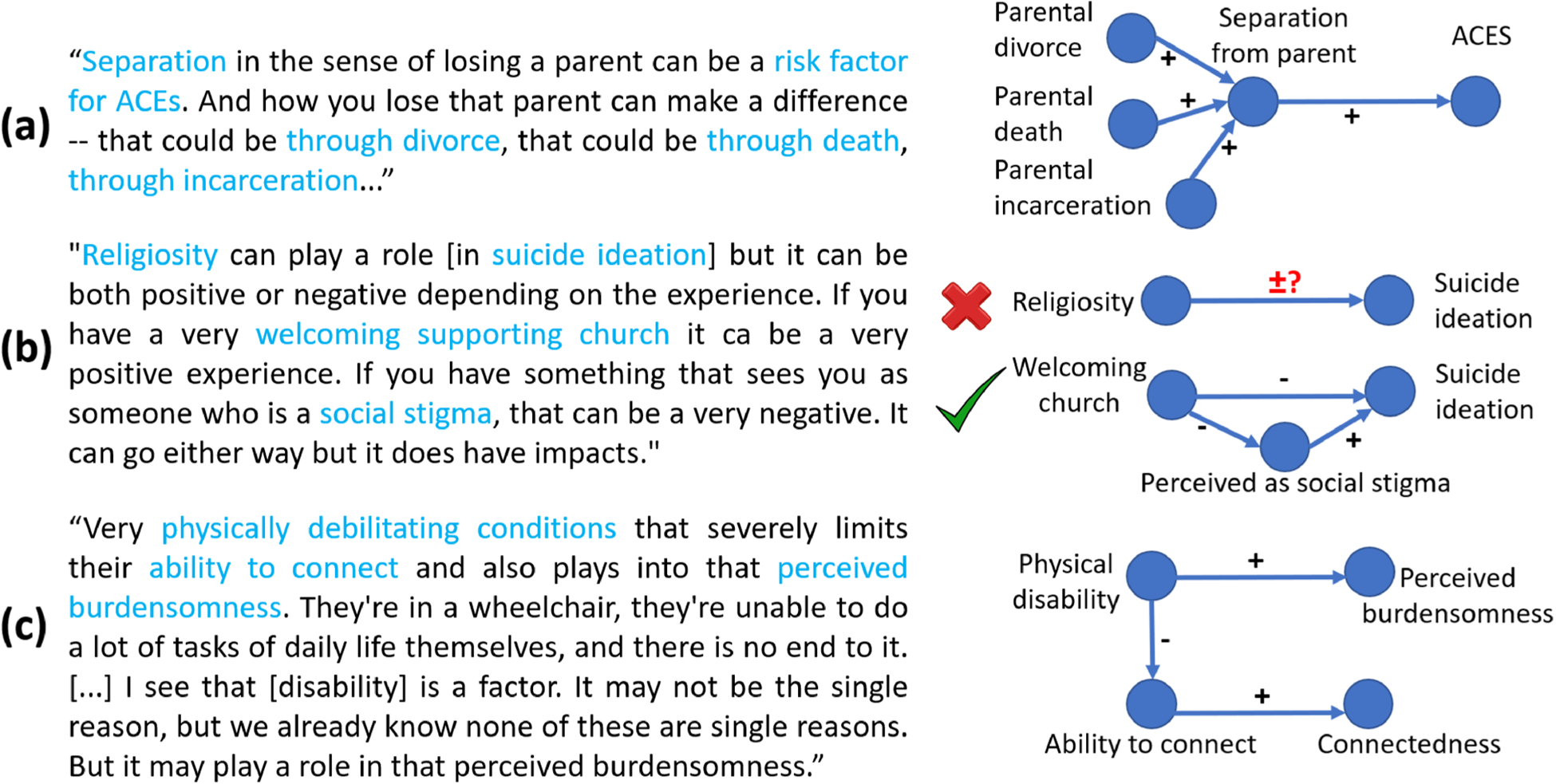
Transformation of three samples collected from our interviews into networks. Factors identified from the transcript are shown in blue within the text and correspond to nodes (blue circles) in the map
After each interview has been transformed into a map, we examine the structure of the map for validation. Although many studies proceed without structural validation (Owen et al. 2018), causal maps can be assessed with respect to their structure or ‘fundamental causal patterns’ (Gray et al. 2019; Levy et al. 2018) to validate the interview process (Firmansyah et al. 2019). Note that ‘validation’ should be interpreted here as the presence of a quality control to ensure that the trained facilitator followed the process in Sect. 2.2. We analyze the structure of each map in terms of:
Types of nodes. As shown in Fig. 4 (colored circles), causal impacts can end at a node (receiver; typically used as output), start at a node (source; typically used as parameter), or pass through a node (transmitter). We generally observe more sources than receivers, as models tend to have few outputs of interest but many parameters driving the model’s behavior (Vasslides and Jensen 2016). Most nodes are neither sources nor receivers, as they constitute the core of the model logic that transforms parameters into outputs. When an SME categorizes a variable as a source, “this means that he perceives the relative causal relationship as a ‘forcing’ function, which cannot be controlled by any other variables. In contrast, a receiver variable is seen as not affecting any of the other variables in the system” (Papageorgiou and Areti 2012). Although an early model may have a lot of parameters, we expect this to be reduced in more elaborate models as SMEs start to capture that such parameters are in fact partly driven by other concepts.
Diameter. When sequences of causal links tend to be short (e.g., A → B → C), there is a risk that the arguments have not been well elaborated (Eden et al. 1992). For instance, stating that “poverty causes parental incarceration which causes suicide” is a short sequence of two causal links which lacks clarity in the exact causal mechanisms. To assess the quality of a map, we thus study the shortest distance between its concepts (Ifenthaler et al. 2011); for example in Fig. 4a, the distance between ACEs and compounded trauma is 1. The maximum shortest distance between any pair of concepts is the diameter of the map, which intuitively represents how much it spans across the problem space.
Feedback loops. Research has shown that there are feedback loops in suicide (Page et al. 2017; Naumann et al. 2019; Chung 2016) and cognitive limitations prevent SMEs from identifying such loops (Axelrod 2015). A map created with a trained facilitator should thus exhibit loops. We monitor three statistics of the loops: their total number, maximum length (e.g., to distinguish reciprocal structures in Fig. 4b from longer loops as shown in Fig. 4a), and average length (Rozenfeld et al. 2005).
Degree. The number of links in which a factor is involved is known as its degree. This is an essential notion for other measures (e.g., a receiver node has a positive in-degree but an out-degree of 0) and often serves to determine the importance of a node (Papageorgiou and Areti 2012). We monitor the maximum degree and the average degree, where the ‘degree’ of a concept is obtained by counting all causal links involving this concept (a.k.a., total degree). The maximum degree can reveal how many of the causal links are concentrated around a single concept. To contextualize this number, we also record the total number of causal links.
Density. The notion captures the overall level of interconnectedness in the map. It is computed as the ratio of edges present to the total number of possible edges. For instance, in a map of three nodes, each one could be linked to the other two, which makes a total of six possible edges. If there are only three, then the ratio is 3/6 = 0.5. Generally, we expect very sparse maps with very low ratios (Vasslides and Jensen 2016), since participants are selective in the causal connections that they perceive. As maps cover more of the problem space (e.g., larger diameter), this ratio decreases.
Fig. 4.
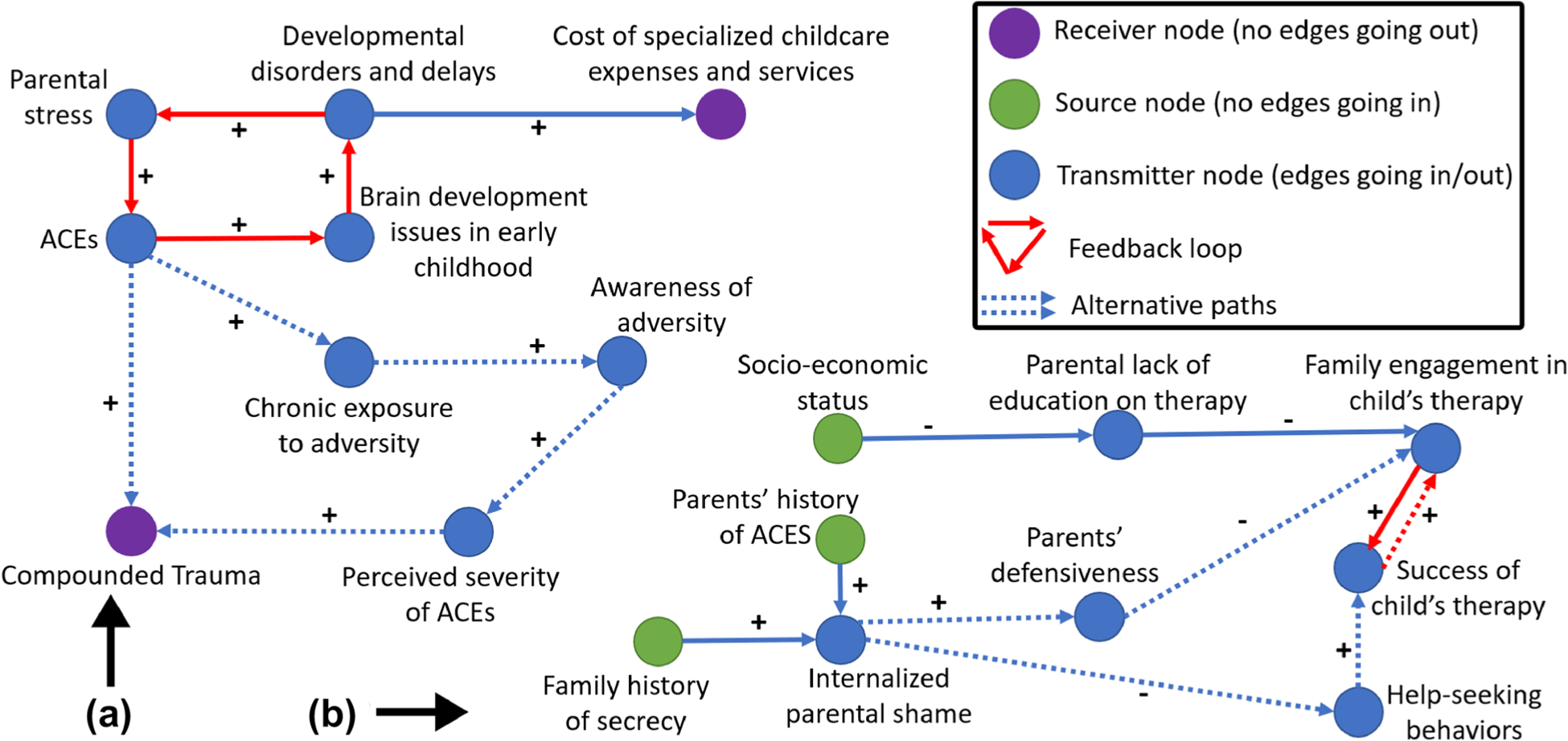
A map can be analyzed with respect to its type of nodes (receivers, sources, transmitters) or the existence of structures involving multiple edges (e.g., feedback loops, alternative paths)
We note that there is a plethora of measures for the structure of a causal map, as evidenced by a summary of 20 years of research in the area (Yoon and Jetter 2016). Additional measures would include whether SMEs see many alternatives (Fig. 4), or assessments of centrality, which can be done in dozens of ways. We thus focused on measures that are commonly adopted and can be interpreted in the context of structural validation (Giabbanelli and Tawfik 2021). Such measures can reveal problematic causal structures indicative of issues in the facilitation or expertise of the participants (Fig. 5).
Fig. 5.
The ‘star’ a views one central concept as being driven by a large number of independent concepts. A map may contain such structure when a large share of the causal links are centered on one concept, as indicated by the high ratio of maximum degree and total links. The ‘list of determinants’ b is a linear cause-and-effect thinking whereby one category affects the next one and so on, without feedback or relationships involving factors within a category
2.4. Assembling individual maps into a single map
Combining all individual maps into one is a challenge due to variations in language across the SMEs (Fig. 6). Some studies prevent this problem from appearing by limiting the SMEs to only designate concepts from a pre-established list (Gray et al. 2015), possibly including ‘distractors’ or ‘misleading’ concepts to ensure careful selection (Ruiz-Primo 2000). However, such limitations may force SMEs to artificially think alike and prevent the emergence of concepts that were not previously considered (Lavin et al. 2018). After adding all causal links and concepts across individual maps into a single one, we manually identify all equivalent forms of a concept and resolve them into a single term. Figure 6 exemplifies how variations (nodes of the same color) are resolved. Although some of the resolutions are straightforward (e.g., “mental illness of the parents” vs “parents’ mental illness”), others require an expert understanding of the context (e.g., terminology for mental health disorders). Note that some of the changes may require inverting the causal direction of a link (e.g., a ‘lack of connectedness’ is a risk factor but, ‘connectedness’ is a protective factor), as shown in Fig. 6 for hopelessness.
Fig. 6.
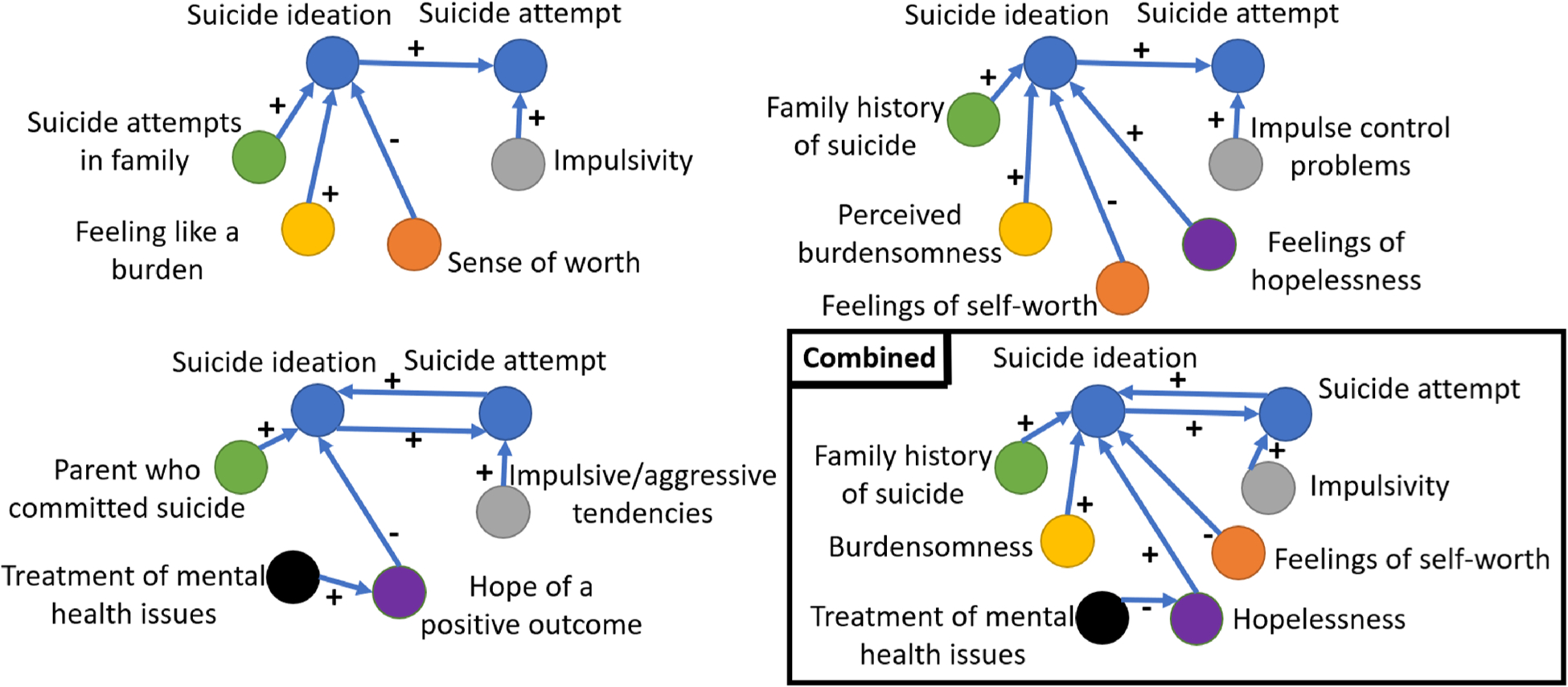
Combining three individual maps into one (bottom-right). Colors show matching concepts
Five of the authors (including a suicide SME and an ACE SME) thus identify and reduce variations in language iteratively, until each concept appears through a unique term. Variations are tracked and documented in a ‘thesaurus,’ available on our repository (https://osf.io/7nxp4/). The thesaurus can be reused by other researchers needing to reduce variability in similar qualitative inquiries featuring open-ended coding schemes (Naumann et al. 2019; Chung 2016; Giabbanelli et al. 2019).
Based on previous studies, the first aggregate map of a complex system can be ‘large and unwieldy’ (Owen et al. 2018); thus, it needs to undergo a simplification process. We simplify the model based on consultations with SMEs, guided by an analysis of the network to identify possible candidates for simplification: (i) source concepts, characterized as having no incoming link, whose removal would reduce the number of model parameters; (ii) receive concepts, defined as having no outgoing link, whose removal would reduce the number of model outputs; and (iii) intermediate concepts on a chain of causation, defined as having exactly one incoming and one outgoing link, which can be simplified by rewiring their endpoints. As an unfiltered aggregate map can be challenging to navigate, network analysis served to automatize the identification of candidates, using the scripts openly available at https://osf.io/7nxp4/.
The main drawback of this approach is that it is very time-consuming, as an SME on ACEs or suicide needs to be involved to validate each of the decision to remove, and several iterations are necessary. The key advantages are that such changes do not affect the existence of feedback loops (i.e., any loop present before simplification will be preserved afterward) (Owen et al. 2018) and the model remains entirely connected unlike in some extensive pruning methods (Hayward et al. 2020).
2.5. Quantitative modeling using fuzzy cognitive mapping
By the end of the previous section, we obtain one map. The map is directed as it represents causality, and its concept nodes have unique labels identified by resolving linguistic variations. However, every link that potentially matters is put together without any simple way to filter or prioritize. In other words, every link mentioned was included regardless of whether it was stated by a single SME or multiple ones. Indeed, the aggregation process includes a link in the final map if it was present in any of the individual maps, without counting the number of maps that included it. This treats SMEs equally, but a systematic filtering is necessary to analyze and navigate the system. This is akin to having a road map that lists every path between all locations without differentiating whether they are highways or trails, hence preventing effective navigation. Two broad approaches can be then considered. One approach is to filter the map by including links between nodes that either occur at least at a certain user-defined frequency (e.g., only retain connections made by at least two experts) or at a frequency that is statistically significant (e.g., the use of z-scores by Bakeman and Gottman (1997), which also requires at least five experts). Another approach is to extend the map by equipping each edge with information that characterizes its nature, function, or level of endorsement (Lavin et al. 2018). For instance, they can be characterized in terms of causal intensity (when connectedness increase, how strongly does it impact suicide ideation?), timing (is the impact immediate and sustained through time or is there a lag and gradual decrease?), and previous history. The use of a follow-up survey to quantify the links thus makes up for a deficiency at the aggregation stage (not counting the endorsement of each link in individual models) and potentially goes further depending on the items on the survey.
Modeling approaches such as System Dynamics (SD) can represent all these characteristics, but the issue is then to obtain data: there are neither sufficient data to populate all aspects of the model (as evidenced by our analysis), nor the possibility to ask subject matter experts to precisely state the duration of every time lag. In contrast, Fuzzy Cognitive Mapping (FCM) can represent knowledge domains with high complexity and without a single accepted theory. In this situation, an FCM combines the qualitative information provided by different sources, thus aggregating their partial knowledge to achieve an overall understanding of the system (Hester and Adams 2017). We thus adopt the FCM methodology to characterize the causal intensity/strength of the links in the map. For a broader discussion on FCM in comparison with other network-based methods, we refer the reader to (Hester and Adams 2017).
The process is depicted in Fig. 7 and proceeds in three steps. First, we decompose the set of causal links in the map into three groups matching the expertise of the SMEs in the problem domain (ACEs, suicide, therapy/clinical practice). This avoids the creation of an overwhelmingly long questionnaire where most questions may be skipped. Second, we create an online questionnaire for each group. One question is asked for each causal edge, focusing on its causal strength. The answers are qualitative and allow for a skip pattern as well as to report that the SME disagrees with the existence of the proposed causal mechanism. The third step uses fuzzy logic to transform the qualitative constructs (e.g., ‘very low’ or ‘high’ strength) into quantitative weights.3 Fuzzy Logic was designed to deal with imprecise concepts in real-world problems, thus providing a mathematical tool that also deals with the degree or partiality of truth. Concepts such as ‘very low’ or ‘high’ are defined mathematically through fuzzy membership functions (triangular functions in Fig. 7) which partly overlap, thus indicating that an SME’s perception of a ‘medium’ strength can partly resemble what another may label a ‘high’ strength. After SMEs have completed a questionnaire, we count the proportion of respondents for each of the options (Fig. 7, Step 3a). Then, we apply fuzzy logic, which projects the ratio of each response onto its fuzzy membership function (Fig. 7, Step 3b). These responses are aggregated by ‘clipping’ the prorated parts of each function and then a consensus response is established by identifying the center of gravity (Step 3c) which results in a number in the range [−1, 1] where −1 indicates the most negative causal strength and 1 the highest one.4
Fig. 7.
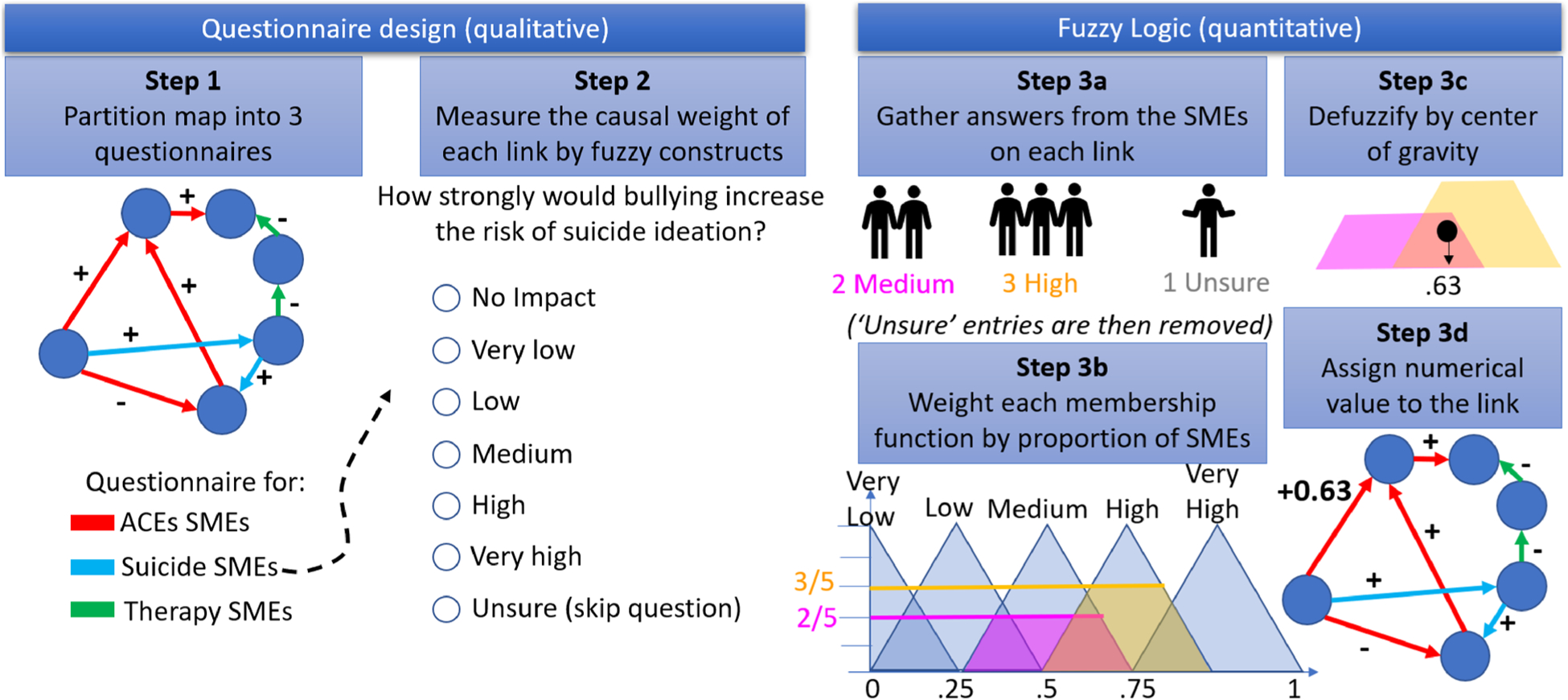
Applying Fuzzy Logic on questionnaires to quantify causal impacts in the map
3. Development of the systems map
3.1. Overview
All data reported in this section are openly accessible without registration on the third-party Open Science Framework repository (OSF) at https://osf.io/7nxp4/. The repository is organized in numbered subfolders following the progress of the model building process, from (1) individual maps and the subsequent completion of (2) individual questionnaires, to the creation of (3) the complete map. As a large map is best explored through interactive visualizations, we provide the map together with (4) an open-source visualization software and a brief tutorial. The key application demonstrating the usefulness of the map consists of (5) examining the data landscape. The remainder of this section reports key results on the model building process, complete map, and application.
3.2. Map building process
A total of 17 invitations were emailed, with 15 affirmative responses, and 2 non-responses. Their professional characteristics are summarized in Table 1, and their complete list together with professional affiliations is provided in the Acknowledgements section. The fifteen SMEs accepting to participate were interviewed for the study between June 29, 2020, and July 21, 2020. Interviews lasted 55.1 ± 7.4 min. Characteristics of the individual maps (transcribed from the interview recordings) are shown in Fig. 8. As the importance and definition of metrics was provided under section ‘Transcribing an interview into an individual map,’ we now briefly analyze these results as they pertain to the validation of the model building process. Participants aptly saw the system as being composed of loops, rather than as a list of determinants (Fig. 5b). Rather than focused on direct causes or consequences, participants addressed distal factors as evidence by an average diameter of 8. On average, 15 out of the 85 causal links are concentrated around a single factor (i.e., max degree), which indicates a small level of centralization and is far away from the problematic case of the ‘star graph’ (Fig. 5a).
Table 1.
Characteristics of the 15 subject matter experts
| Professional characteristic | Value |
|---|---|
| Area of expertise | |
| …Suicide | 46.67% (n = 7) |
| …ACEs | 46.67% (n = 7) |
| …Both | 6.67% (n = 1) |
| Affiliation | |
| …Internal to CDC | 66.67% (n = 10) |
| …External to CDC | 33.33% (n = 5) |
| Years of experience | |
| …Suicide | 23 ± 17 years, range 7–50 |
| …ACEs | 14.2 ± 6 years, range 6–20 |
| …Therapy | 7 ± 1 years, range 6–8 |
| Primary role | |
| …Behavioral scientist | 46.67% (n = 7) |
| …Clinician, licensed therapist | 26.67% (n = 4) |
| …Health scientist, analyst, epidemiolo-gist | 20.00% (n = 3) |
| …Child abuse prevention advocacy | 6.67% (n = 1) |
Fig. 8.
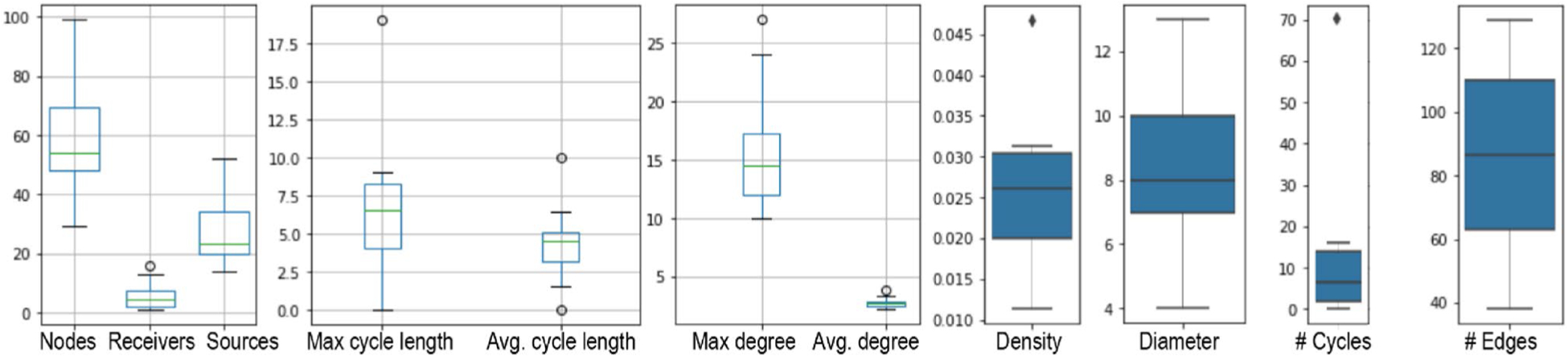
Distribution of structural characteristics across the 15 individual maps
In the process of combining the fifteen individual maps into a single one, we found that 131 terms appeared in several maps under different names. These differences were resolved by adopting a single name, such as “racism” instead of “structural racism,” “racism and discrimination,” “racial injustice,” or “racism and forms of systemic oppression.” Each of the 131 terms had an average of 4 linguistic variations. Eight concepts had over ten linguistic variations, which indicates their importance across interviews: mental health disorders (e.g., mental health issues, mental illness, child with mental illnesses, emerging psycho-pathologies), ‘connectedness’ (e.g., social support, friends, social connections), coping skills (e.g., healthy coping strategies, problem-solving skills), family financial stress (e.g., financial distress, economic stressors on families), economic policies for ACEs, parents’ substance use, protective factors, and child abuse or neglect.
When simplifying the combined map, we emphasize that network science only serves to identify potential areas for simplifications, but decisions are ultimately made by SMEs. For example, the vast majority (62 out of 71) of concepts serving as intermediate on a chain were preserved by SMEs. Such concepts are considered as important to understand ACEs and suicide, or as potential targets for prevention. For example, we have a chain stipulating that ACEs arise when a child engaging in conflicts is harshly disciplined. Although ‘harsh discipline’ only plays the role of an intermediate from a network perspective, it is an important target in suicide prevention. Similarly, we see a chain noting that exposure to violence is followed by normalization of violence, ultimately contributing to suicide fatality. The concept of normalization was preserved, as a noteworthy social construct. Among the nine concepts that were simplified, some were merged (e.g., ‘ruminative thoughts about dying’ subsumed ‘repeated suicide ideation,’ ‘access to immediate effective clinical cares’ subsumed ‘requires medical intervention’ in the context of saving life by treatment following an attempt), and others were rewired such as directly connecting in-patient treatment to mental health treatment, without noting the ‘short stay’ intermediate (as going into a hospital triage model is out of scope).
Characteristics of the map after simplification are presented in Table 2. We note its total of 946 edges and 361 concepts, which makes it the largest map on ACEs and suicide (Brenas et al. 2019). There are only two receiver nodes, which stand for consequences that go ‘beyond’ the life of a child or adolescent. One is the consequence of a suicide, which results in exposing the community to suicide. The other is an increased propensity to be involved in violence in adulthood. The most important factor in the map in terms of degree are Adverse Childhood Experiences (ACEs). As the concept encompasses a large number of forms of abuse, it has a total of 92 antecedents and consequents. The existence of a few such ‘hub’ concepts with many connections and a majority of concepts with few connections evokes a power-law degree distribution, which is the hallmark of scale-free network. We confirmed this hypothesis by fitting a power-law degree distribution to the map (Fig. 9) with a p-value of 0.008, which is statistically significant (< 0.05). Although we see that the power-law distribution does not perfectly match our empirical distribution, such deviations from a perfect fit are commonplace in empirical data (Broido and Clauset 2019).
Table 2.
Characteristics of the whole system map
| Structural characteristic | Value |
|---|---|
| Number of nodes | 361 |
| Number of source nodes | 113 |
| Number of receiver nodes | 2 (community exposure to suicide, involvement in violence) |
| Number of edges | 946 |
| Density | 0.007 |
| Average degree | 5.240 |
| Maximum degree | 92 (ACEs) |
| Diameter | 12 |
Fig. 9.
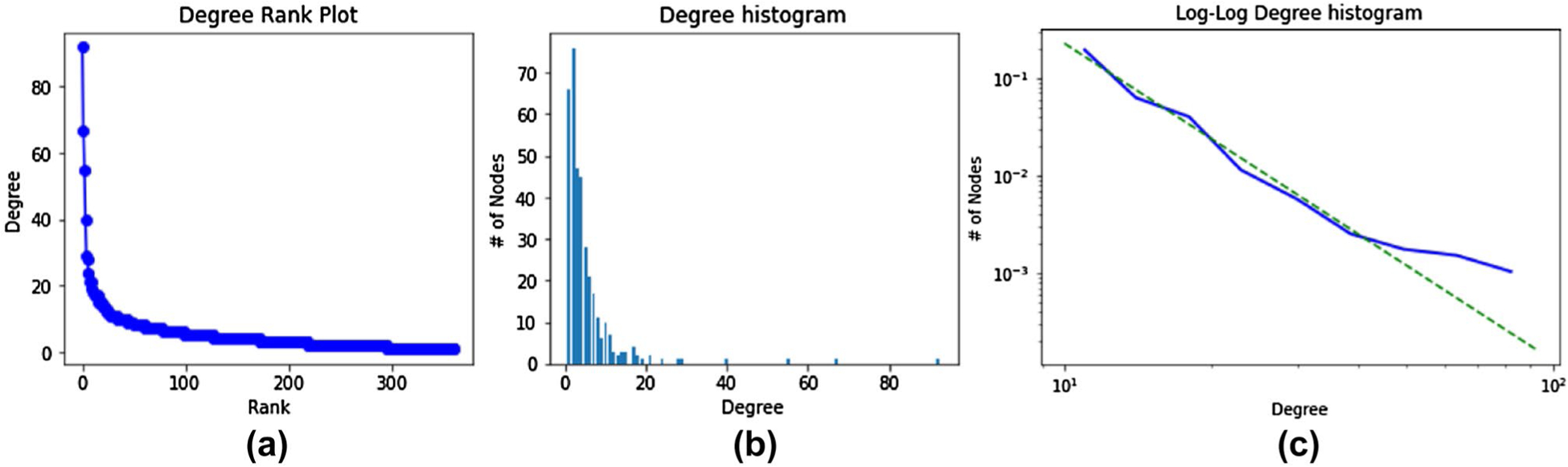
Degrees in the overall map as a rank plot (a) or linear histogram (b), and on a log–log scale to fit a power-law distribution (c)
Previous Fuzzy Cognitive Maps related to suicide or Adverse Childhood Experiences were able to quantify all causal connections either because they were much smaller, such as 12 concepts in Merlin et al. (2020), or because they used fully automated techniques rather than a participatory approach, such as White and Mazlack (2011) who detected suicide notes based on connections between words. In contrast, our participatory modeling approach resulted in 361 nodes, connected by 946 edges. We thus selected small subsets for further quantification with the SMEs through three questionnaires: an ACE questionnaire (116 links; n = 6 respondents), a suicide questionnaire (114 links; n = 5 respondents), and a therapy questionnaire (108 links; n = 2 respondents). Twelve questions were asked to two groups of SMEs, as the questions were related to the expertise of both groups. When a large difference was observed (≥ 0.10), the group on the receiving end of the causal link always saw it as larger (Table 3). In other words, when a causal link ‘left’ the domain of expertise of a group, they tended to see it as less important.
Table 3.
Perceptions of cross-domain causal strengths across groups of experts
| Causal link | Causal strength | ||
|---|---|---|---|
| ACEs SMEs | Suicide SMEs | Therapy SMEs | |
| ACEs → suicide ideation | 0.67 | 0.81 | |
| ACEs → suicide attempt | 0.62 | 0.74 | |
| ACEs → suicide fatality | 0.44 | 0.61 | |
| Mental illness in the family → ACEs | 0.72 | 0.62 | |
| ACEs → mental health disorders | 0.66 | 0.79 | |
| ACEs → psychological pain | 0.66 | 0.79 | |
| Suicide ideation → mental health disorders | 0.48 | 0.79 | |
| Mental health disorders → suicide attempt | 0.71 | 0.76 | |
| Mental health disorders → suicide fatality | 0.71 | 0.76 | |
| Mental health disorders → suicide ideation | 0.71 | 0.76 | |
| ACEs → self-esteem | − 0.61 | − 0.62 | |
| Mental health disorders → coping skills and resiliency | − 0.65 | − 0.62 | |
Although the use of a follow-up questionnaire to quantify weights with the participants is a common practice (Firmansyah et al. 2019; Giabbanelli et al. 2012; Mkhitaryan et al. 2020), a recurring concern is whether participants will see ‘everything as important’ and hence score every link as Very High instead of providing nuances. We do not see this concern in the data as the (defuzzified) scores had a large range: from 0.34 to 0.86 (average 0.63 ± 0.09) for ACEs SMEs, from 0.29 to 0.86 (average 0.61 ± 0.13) for suicide SMEs, and 0.37 to 0.79 (average 0.67 ± 0.10) for therapy SMEs. This indicates that SMEs carefully reflected on the nuances of causal strengths.
The option of labeling a causal edge as inexistent (i.e., ‘no causality’) was extremely rare. Across all three questionnaires, no edge was labeled as inexistent by more than one participant. In addition, only one respondent within each of the three groups ever categorized edges as inexistent, with four edges receiving this label for suicide, 5 for ACEs, and 6 for therapy. There is thus a large consensus that most edges in the map do play a role in the ACEs and suicide system.
3.3. Examination of the final weighted map
Given its large size (Table 2), the final map is not meant to be visualized all at once. Rather, it provides a decision support tool that can be utilized to address asking specific questions such as “in which ways does factor A eventually impact factor B,” or “what are the direct and indirect consequences of an intervention on factor A.” In this section, we selected some common queries in consultation with SMEs. In Fig. 10, we examined the many ways in which ACEs of parents eventually cause suicide fatality of the child, thus highlighting intergenerational effects. In Fig. 11, we selected a sample of six feedback loops covering different domains, from the benefits of therapy and changes in parental practices (Fig. 11a or c) to the many loops involving parental frustration and coping via substance abuse or perpetration of ACEs (Fig. 11b or d). Thanks to its broad coverage of proximal and distal factors, the loops also include high-level societal constructs such as poverty, thus demonstrating the perpetuation of social issues (Fig. 11e). Finally, we examined opportunities for interventions via structural changes focused on one factor, and the rippling effects through the broader map. Economic policies (Fig. 12a) can directly improve financial stability and lower stress, which ultimately reduces ACEs. Social support for parents (Fig. 12b) also reduces ACEs, in addition to preventing suicide ideation. Additional analyses provided in S1 Table list all of the quantified links contributing to suicide ideation, attempt, and fatality. When a direct link is not present, we measured indirect effects through paths and whether such paths all acted via factors such as ACEs, or included ACEs among other mediating variables.
Fig. 10.
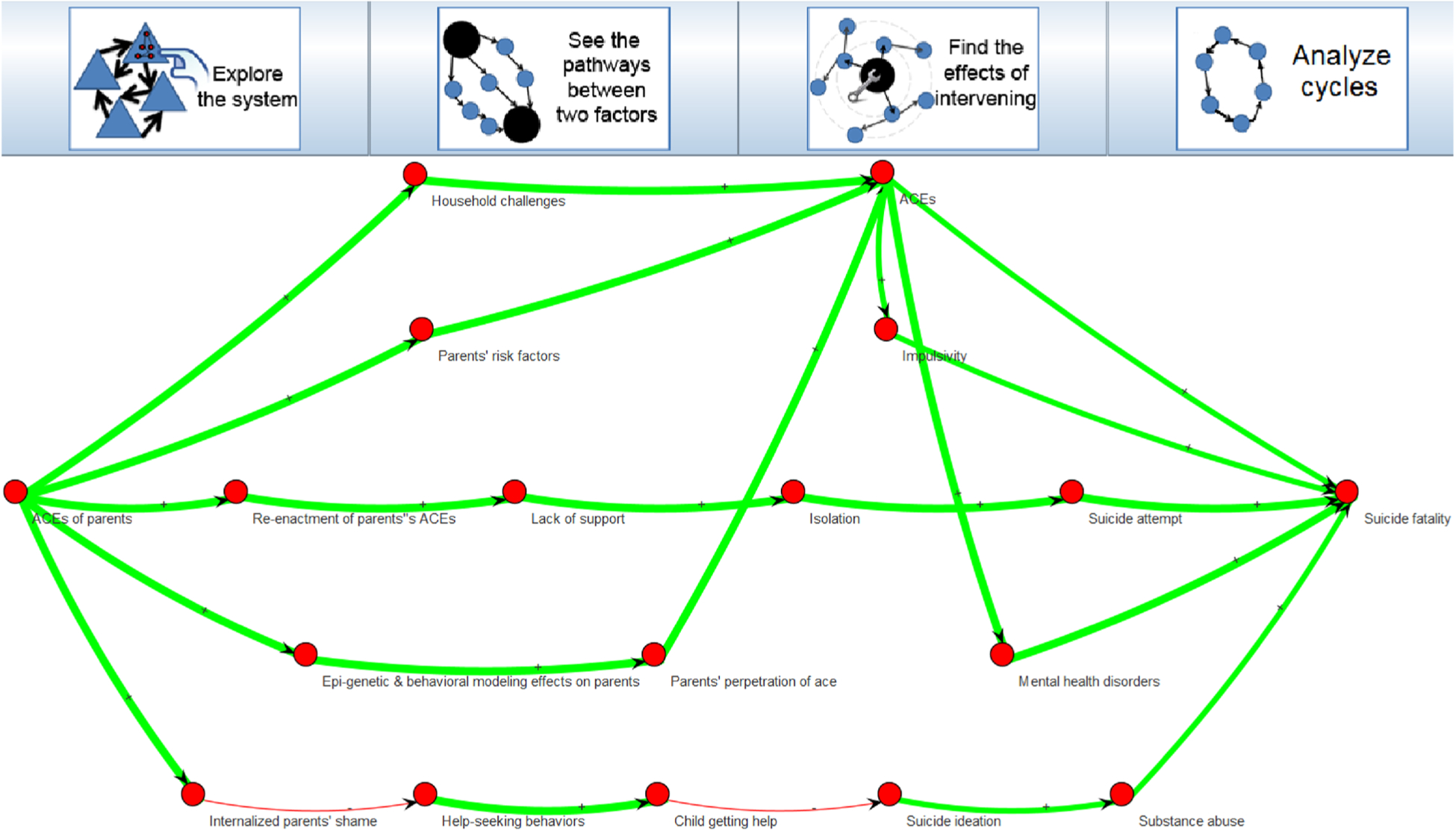
ActionableSystems software (available on our repository) allows to automatically identify all pathways from one concept to another, as exemplified here from ACEs of parents (left) to suicide fatality (right). The software also identifies all loops and rippling effects of an intervention
Fig. 11.
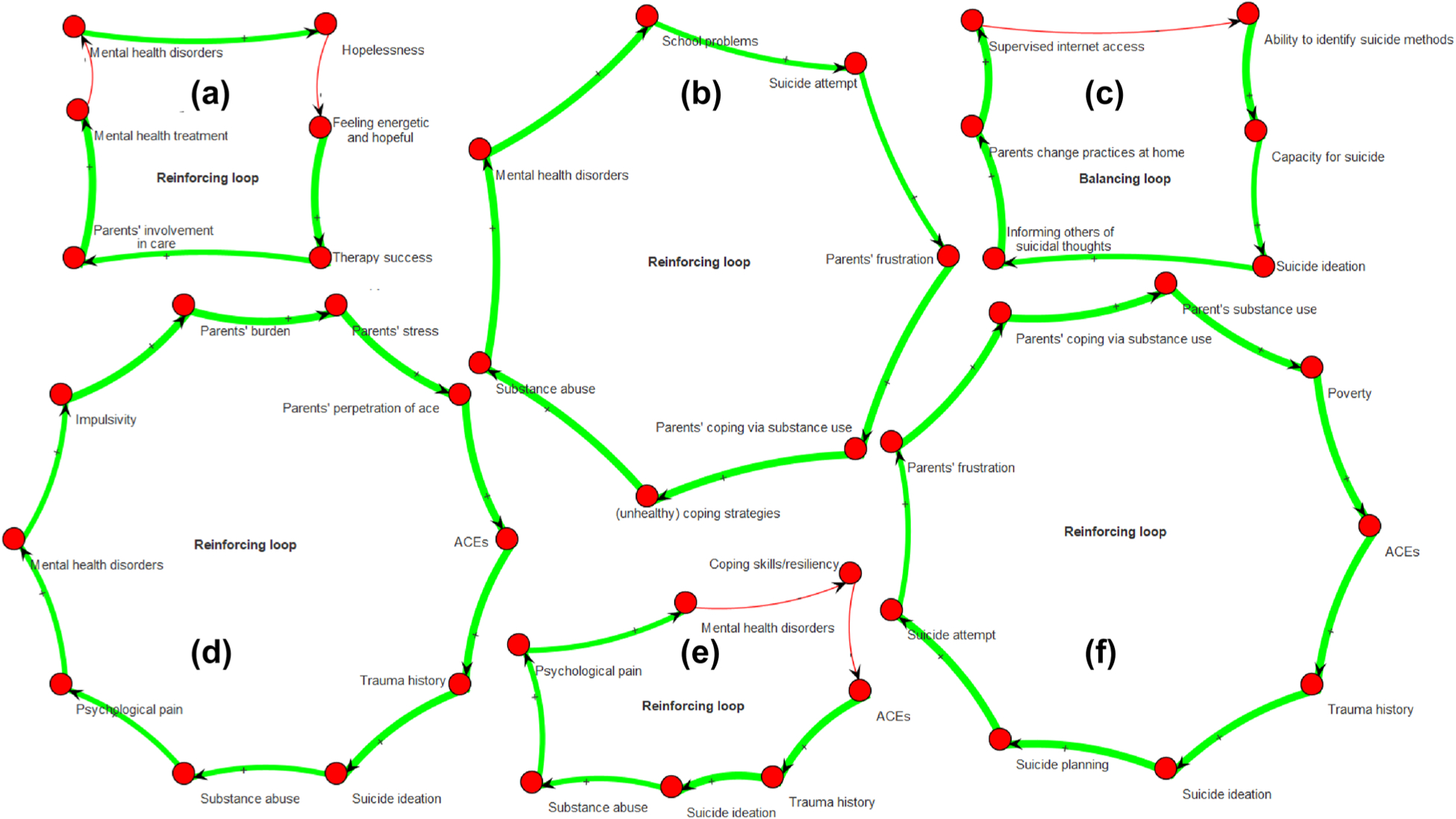
Sample loops from the map including a the benefits of therapy, b parental frustration and coping via substance use, c positive changes in practices that decrease capacity for suicide, d parental perpetration of ACEs, e mental health disorders, and e poverty
Fig. 12.
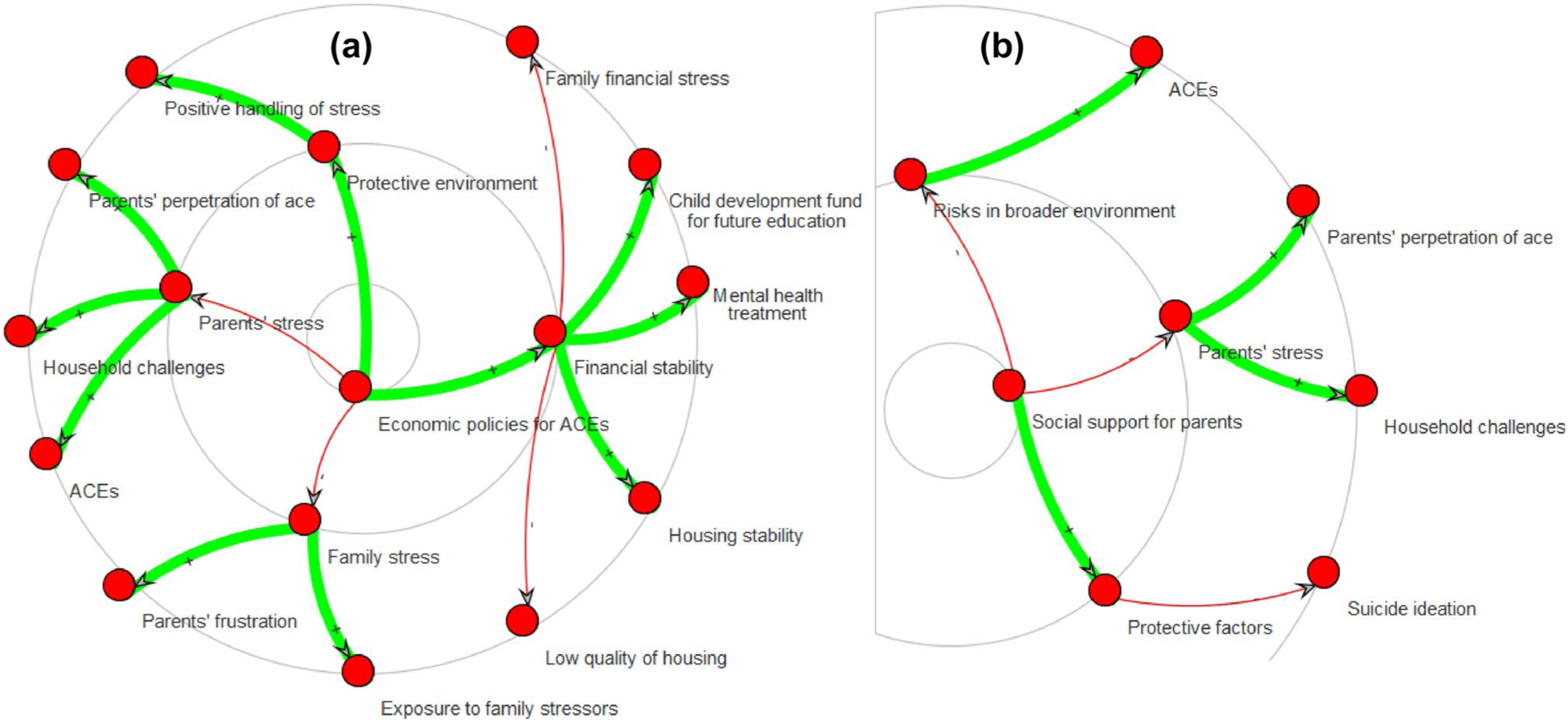
Rippling effects of interventions on economic policies (a) and social support for parents (b). Effects are shown in concentric circles from most proximal to more distal
4. Discussion
Suicide among youth in the USA has increased 56% from 2007 to 2017 and now represents the second leading cause of death. Despite its necessity, designing effective interventions for suicide prevention among youth is a challenging task given our limited understanding of the many factors and interrelationships that characterize suicide as a multifactoral problem (Centers for Disease Control and Prevention 2018; Bilsen 2018; Cleary et al. 2019; Cash and Bridge 2009). Although several frameworks have demonstrated their usefulness (Chu et al. 2010, 2017; Rogers and Joiner 2019; World Health Organization 2014; Centers for Disease Control and Prevention 2015), they do not comprehensively cover the very large number of concepts involved across domains (e.g., individual, family, community, society) or the feedback loops that are essential to understand both intergenerational effects and the perpetuation of risk factors. In this paper, we developed the largest system map to date on suicide and Adverse Childhood Experiences (ACEs), totaling 361 concepts and 946 interrelationships. As large system maps are decision support tools, we demonstrated the potential value of such a map by exploring it through a software. We focused on the pathways between factors, the impacts of interventions, and feedback loops. We further exemplified the benefits of a map, not only to explore a complex system but also to guide data collection by contrasting it with several large datasets commonly used in suicide research. This guidance and improvement in data linkages was mentioned among key data science efforts for violence and injury prevention (Ballesteros et al. 2020).
Given the interdisciplinary knowledge of subject matter experts, we were able to disentangle pathways and assemble concepts across domains (e.g., economy, mental health) and socio-ecological levels (e.g., individual, family, community, society). We identified factors of importance and used a mathematically rigorous approach to evaluate their perceived causal strength among experts, whether the factors could be concretely measured or are abstract. In line with best practices for systems mapping, we validated our approach throughout model development and provided full transparency into our steps by making our intermediate data available together with the final map. An advantage of our approach is the ability to identify and quantify relationships that we may not have otherwise identified in the published literature, or for which data are not available at a national level. For example, the literature is limited on the connections between ACEs and youth suicide fatality; however, by mapping out connections we are able to see pathways that potentially connect these factors. Once we identify these pathways, we can guide data collection processes to better characterize these relationships. This process also helps us identify linkages where prevention efforts may be most impactful. For example, we identified inter-generational transmission of ACEs from the parent to the child that was a direct pathway leading to an increased likelihood of youth suicide ideation. Identifying this linkage offers opportunities for interventions at the parental level as a potential suicide prevention strategy at the child level.
Trauma is not just an individual trait or behavior. Trauma is perpetuated through familial, social, and historical context. In our map linking ACEs and suicide risk, families and parents appear to be an important contributor to the intergenerational transmission of ACEs, as evidenced in Figs. 10 and 11 where both parental mental health and financial instability partially explain the interrelationship between exposure to ACEs and suicidal thoughts and behaviors. Thus, our findings underscore the importance of trauma-informed care and a 2-generation approach to addressing social determinants of health such as poverty, housing instability, and social disadvantage. Policies that increase access to mental health services (particularly for parents) and economic supports for families are critical for interrupting the intergenerational transmission of ACEs and suicide risk.
Research on the associations between ACEs and suicide has typically been limited to suicidal thought and behaviors, since research on the relationship between ACEs and suicide completion has been limited by methodological constraints. The systems map developed here, as exemplified in Fig. 9, can help researchers and policy makers better understand possible intermediary processes between ACEs and suicide. Programs and policies that address substance use, mental health disorders, isolation, impulsivity, and suicide attempts may help interrupt the effects of ACEs on suicide fatality, while programs and policies that prevent parental ACEs and improve the home environment may prevent both ACEs and suicide fatality.
As shown by the many steps of our methodology, the development of a comprehensive systems map is a large undertaking. Other researchers may be interested in conducting similar participatory modeling studies by following the steps detailed here, but they may lack in-house capacity (e.g., time, availability of trained facilitators). Several software packages have been released that support some or all of the tasks performed here (e.g., creating a map, aggregating, simplifying). For example, jMAP allows to construct causal maps, aggregate them, or perform comparisons (Jeong 2016). jMAP has been used in several studies in educational technology, where students viewed a short video and then used the system on their own (Jeong 2020). Unlike a trained facilitator, the role of jMAP is not to guide a participant (e.g., avoiding out-of-scope topics, prompting them to examine connections between important concepts), but rather to examine the reasoning processes of learners. When switching from the context of educational technology to participatory modeling, software packages such as MentalModeler tend to be used together either by participants with facilitators (Gray et al. 2013) or solely by the facilitators, as a tool to record interviews (Blacketer et al. 2021), as we did here. In this case, the software alleviates the time spent on certain activities, but the involvement of facilitators still results in significant time commitment.
Prototypes (with various degrees of maturity and reusability) are emerging to use AI in replacement of the time-consuming tasks performed by trained facilitators. Given the time-consuming nature of the semi-structured one-on-one interviews, our research group released the prototype for an ‘artificial facilitator’ that uses algorithms (e.g., network science and Natural Language Processing) to manage the conversation. The algorithms were embedded in Amazon Alexa, hence the device acted as a facilitator (Reddy et al. 2019). Experiments showed that individuals were able to use the system even if they had no prior experience in interacting with Voice Activated Personal Assistants, or no prior experience in building systems maps (Reddy et al. 2020). However, such a prototype still needs significant improvements before it can measure up with a trained facilitator, in specific domains. After the facilitation stage, we need to transform the (transcribed) individual interviews into maps, which requires the identification of key concepts and their interrelationships. This task can partly be achieved by prototypes, built through a combination of Natural Language Processing and Visual Analytics. Specifically, we posited that analysts can be supported by creating a feedback loop between the identification of entities in the text and the map (Pillutla and Giabbanelli 2019). Newer tools such as Discussoo further illustrate the potential of eliciting mental models from discussions (Anjum et al. 2021). Finally, the challenge of linguistic variability in the aggregation step has been examined from complementary perspectives. The field of ontology matching has long been interested in handling variations in meaning when combined different graph-based descriptions of a domain. Processes from ontology matching have recently inspired techniques to aggregate causal maps (Freund and Giabbanelli 2021), based on the observations that concepts are more likely to match if they share links (i.e., structural information: similar consequents or antecedents) or overlap in meaning (i.e., semantic information: relationships such as synonymy). However, accuracy is not currently comparable to a trained facilitator performing the aggregation with subject matter experts.
Similar to how the Foresight Obesity Map shaped conversations and guided numerous efforts in obesity research (McPherson et al. 2007; Ulijaszek 2015), the investment that we made in developing a systems map on ACES and suicide among youth provides a decision support tool that can be benefit researchers and public health practitioners in ACEs and youth suicide prevention. That is, the ultimate function of a map is to help experts articulate and view the shared problem space. Applications include, but are not limited to, deciding where to directed limited resources to either address or further investigate aspects of suicide and ACEs. Given previous reports on the difficulty of end users in navigating the Foresight Obesity Map as a picture (Hall et al. 2011; Siokou et al. 2014), we have actively facilitated future reuse by releasing the map together with a visualization software (and tutorials) on a third-party repository. The case of the Foresight Obesity Map exemplifies how numerous future studies become possible once a map is provided to the research community. For instance, a dedicated study examined the structure of the Foresight Obesity Map from a network perspective by reducing it to core ‘groups’ or components (Finegood et al. 2010) and their implications for solutions. In another case, the authors compared the map developed from subject-matter experts (as built here) with another one, developed by members of the community who experience the issues covered by the map (Giles et al. 2007). Our methodological step of quantifying causal connections (with fuzzy logic) can be particularly useful for such a comparison, as we can examine differences not only in the existence of causal relationships but also in their strength (Allender et al. 2015). Comparative studies can also be developed across groups of experts, as our study already exemplifies how disciplinary boundaries may shape perspectives on ACEs and suicide (Table 3). As suicide is an interdisciplinary problem, a comparison of maps built by sizeable subgroups can serve to investigate potential expert biases (e.g., from training or practice) toward the importance of their own field over others (Giles et al. 2007). In sum, there are numerous instances in which the release of a comprehensive map (Allender et al. 2015) is followed by an extensive analysis (McGlashan et al. 2016) with implications for the field. The development of our map and its release with a software thus provides the first step in a longer vision of using systems science methods in suicide research to cope with the complexity of the problem, and more effectively identify connections between ACEs and youth suicide and identify interventions for supporting young people at risk.
Supplementary Material
Acknowledgements
We are indebted to all fifteen subject-matter experts for engaging in this process and sharing their perspectives: Sarah Bacon, Margaret Brown, Eric Caine, Monica Chambers, Alexander Crosby, Beverly Fortson, Christopher Harper, Kristin Holland, Asha Ivey-Stephenson, Cheryl King, Melissa Merrick, Marilyn Metzler, Kelly Quinn, Deb Stone, and Elizabeth Swedo. The complete list including affiliations and fields of expertise is provided in Appendix A.
Funding
This publication was supported by the Centers for Disease Control and Prevention (CDC), National Center for Injury Prevention and Control (NCIPC), Intergovernmental Personnel Act (IPA) Assignment Agreement 20IPA2009427.
Abbreviations
- ACEs
Adverse childhood experiences
- CDC
Centers for disease control and prevention
- FCM
Fuzzy cognitive map
- SME
Subject matter expert
Appendix A: Affiliations of the subject matter experts (SMEs) who were interviewed
Sarah Bacon, PhD.
Behavioral Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Office of the Director.
Margaret Brown, DrPH.
Behavioral Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Injury Prevention, Suicide Prevention Team.
Eric Caine, MD.
Psychiatrist.
University of Rochester Medical Center.
Monica Chambers, MS.
Mental Health Counselor.
Odyssey Family Counseling Center.
Alexander Crosby, MD, MPH.
Medical Epidemiologist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Office of the Director.
Beverly Fortson, PhD.
Behavioral Scientist.
U.S. Department of Defense, Sexual Assault Prevention and Response Office.
Christopher Harper, PhD.
Behavioral Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, Child Abuse Neglect and Adversity Team.
Kristin Holland, PhD, MPH.
Health Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Overdose Prevention, Office of the Director.
Asha Ivey-Stephenson, PhD.
Behavioral Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Injury Prevention, Suicide Prevention Team.
Cheryl King, PhD.
Professor.
University of Michigan, Youth and Young Adult Depression and Suicide Prevention Research Program.
Melissa Merrick, PhD.
President and CEO.
Prevent Child Abuse America.
Marilyn Metzler, MPH.
Public Health Analyst.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, Office of the Director.
Kelly Quinn, PhD, MPH.
Behavioral Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, Child Abuse Neglect and Adversity Team.
Deb Stone, ScD, MSW, MPH.
Behavioral Scientist.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Injury Prevention, Suicide Prevention Team.
Elizabeth Swedo, MD, MPH.
Physician.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, Morbidity and Behavioral Surveillance Team.
Footnotes
Conflict of interest The authors declare that they have no competing interests.
Consent for publication The manuscript received clearance from publication from relevant divisions within the Centers for Disease Control and Prevention (CDC): the National Center for Injury Prevention and Control (NCIPC) Division of Injury Prevention (DIP)—Data Analytics Branch (DAB), and the National Center for Injury Prevention and Control (NCIPC) Office of Strategy and Innovation (OSI). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Ethics approval and consent to participate The study protocol was examined given the CDC guidelines to determine the need for approval by the Institutional Review Board (IRB) and Office of Management and Budget (OMB). The study received exemption from both as it does not involve clinical investigations (e.g., drugs, biologics, devices) and the number of non-federal interviewees included in the study is under the threshold requiring a review by the Human Research Protection Office. Each interview was conducted and recorded using WebEx video conferencing after receiving informed consent from the SME.
ACEs are preventable, potentially traumatic events that occur in childhood such as neglect, experiencing or witnessing violence, and having a family member attempt or die by suicide. This also includes aspects of a child’s environment that can undermine their sense of safety, stability, and bonding, such as growing up in a household with substance use, mental health problems, or instability due to parental separation or incarceration of a parent, sibling or other member of the household. ACEs have complex and negative influences on individual health outcomes throughout the life course, including increased risk of suicidal behaviors (World Health Organization 2014).
Fuzzy Cognitive Mapping (FCM) is “a powerful means to represent knowledge domains that are characterized by high complexity, by widespread knowledge sources that usually only have partial knowledge, by qualitative information that frequently changes, and by a lack of a commonly accepted ‘theory’ or ‘truth’” (Jetter 2006).
Fuzzy Logic can produce highly accurate estimates, as demonstrated by the use of FCMs in settings highly sensitive to errors such as radiotherapy treatment, diagnostics of brain tumor (where the system was above 90% accurate) (Amirkhani et al. 2017), or drug therapy management (Bevilacqua et al. 2018).
For the mathematical foundations of Fuzzy Logic and standard operations involved (Mamdani, Algebraic Sum, Center of Gravity), we refer the reader to (Xu and Da 2003; Kruse et al. 2016; Mamdani 1977).
Availability of data and materials
Our data are provided on a thirdparty repository by the Open Science Framework (OSF), which can be publicly accessed without registration at https://osf.io/7nxp4/In particular, the online repository includes the individual map from each SME, the questionnaires used to assign weights to causal relationships, the overall map, and the software used to visualize the map.
References
- Allender S, Brown AD, Bolton KA, Fraser P, Lowe J, Hovmand P (2019) Translating systems thinking into practice for community action on childhood obesity. Obes Rev 20:179–184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allender S, Owen B, Kuhlberg J, Lowe J, Nagorcka-Smith P, Whelan J, Bell C (2015) A community based systems diagram of obesity causes. PLoS ONE 10(7):e0129683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amirkhani A, Papageorgiou EI, Mohseni A, Mosavi MR (2017) A review of fuzzy cognitive maps in medicine: taxonomy, methods, and applications. Comput Methods Programs Biomed 142:129–145 [DOI] [PubMed] [Google Scholar]
- Andersen DF, Richardson GP, Vennix JA (1997) Group model building: adding more science to the craft. Syst Dyn Rev: J Syst Dyn Soc 13(2):187–201 [Google Scholar]
- Anjum M, Voinov A, Taghikhah F, Pileggi SF (2021) Discussoo: towards an intelligent tool for multi-scale participatory modeling. Environ Model Softw 140:105044 [Google Scholar]
- Axelrod R (ed.) (2015) Structure of decision: the cognitive maps of political elites. Princeton University Press [Google Scholar]
- Bakeman R, Gottman JM (1997) Observing interaction: an introduction to sequential analysis. Cambridge University Press [Google Scholar]
- Ballesteros MF, Sumner SA, Law R, Wolkin A, Jones C (2020) Advancing injury and violence prevention through data science. J Saf Res 73:189–193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bevilacqua M, Ciarapica FE, Mazzuto G (2018) Fuzzy cognitive maps for adverse drug event risk management. Saf Sci 102:194–210 [Google Scholar]
- Bilsen J (2018) Suicide and youth: risk factors. Front Psych 9:540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blacketer MP, Brownlee MT, Baldwin ED, Bowen BB (2021) Fuzzy cognitive maps of social-ecological complexity: applying mental modeler to the Bonneville salt flats. Ecol Complex 47:100950 [Google Scholar]
- Brenas JH, Shaban-Nejad A (2020) Health intervention evaluation using semantic explainability and causal reasoning. IEEE Access 8:9942–9952 [Google Scholar]
- Brenas JH, Shin EK, Shaban-Nejad A (2019) Adverse childhood experiences ontology for mental health surveillance, research, and evaluation: advanced knowledge representation and semantic web techniques. JMIR Ment Health 6(5):e13498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broido AD, Clauset A (2019) Scale-free networks are rare. Nat Commun 10(1):1–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryan CJ, Butner JE, May AM, Rugo KF, Harris JA, Oakey DN et al. (2020) Nonlinear change processes and the emergence of suicidal behavior: a conceptual model based on the fluid vulnerability theory of suicide. New Ideas Psychol 57:100758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cash SJ, Bridge JA (2009) Epidemiology of youth suicide and suicidal behavior. Curr Opin Pediatr 21(5):613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (2015) The social-ecological model: a framework for prevention. CDC, Atlanta. https://www.cdc.gov/violenceprevention/publichealthissue/social-ecologicalmodel.html. Accessed 9 May 2015 [Google Scholar]
- Centers for Disease Control and Prevention (2018) Vital signs: suicide rising across the US. https://www.cdc.gov/vitalsigns/pdf/vs-0618-suicide-H.pdf Centers for Disease Control and Prevention. NCHS Data Brief, No. 362. National Center for Health Statistics, Hyattsville. Accessed June 2018 [Google Scholar]
- Chu C, Buchman-Schmitt JM, Stanley IH, Hom MA, Tucker RP, Hagan CR et al. (2017) The interpersonal theory of suicide: a systematic review and meta-analysis of a decade of cross-national research. Psychol Bull 143(12):1313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chu JP, Goldblum P, Floyd R, Bongar B (2010) The cultural theory and model of suicide. Appl Prev Psychol 14(1–4):25–40 [Google Scholar]
- Chung SY (2016) Suicide attempts from adolescence into young adulthood: a system dynamics perspective for intervention and prevention. Dissertation, Washington University in St Louis [Google Scholar]
- Cleary M, Visentin DC, Neil A, West S, Kornhaber R, Large M (2019) Complexity of youth suicide and implications for health services. J Adv Nurs 75(10):2056–2058 [DOI] [PubMed] [Google Scholar]
- De Pinho H (2017) Generation of systems maps. In: El-Sayed AM, Galea S (eds) Systems science and population health. Oxford University Press, Oxford, United Kingdom, p 61–76 [Google Scholar]
- Düspohl M, Döll P (2016) Causal networks and scenarios: participatory strategy development for promoting renewable electricity generation. J Clean Prod 121:218–230 [Google Scholar]
- Eden C, Ackermann F, Cropper S (1992) The analysis of cause maps. J Manage Stud 29(3):309–324 [Google Scholar]
- Epstein JM (2008) Why model? J Artif Soc Soc Simul 11(4):12 [Google Scholar]
- Finegood DT, Merth TD, Rutter H (2010) Implications of the foresight obesity system map for solutions to childhood obesity. Obesity 18(n1s):S13. [DOI] [PubMed] [Google Scholar]
- Firmansyah HS, Supangkat SH, Arman AA, Giabbanelli PJ (2019) Identifying the components and interrelationships of smart cities in Indonesia: Supporting policymaking via fuzzy cognitive systems. IEEE Access 7:46136–46151 [Google Scholar]
- Freund AJ, Giabbanelli PJ (2021) Automatically combining conceptual models using semantic and structural information. In: 2021 annual modeling and simulation conference (ANNSIM). IEEE, pp 1–12 [Google Scholar]
- Giabbanelli PJ, Baniukiewicz M (2018) Navigating complex systems for policymaking using simple software tools. In: Advanced data analytics in health. Springer, Cham, pp 21–40 [Google Scholar]
- Giabbanelli PJ, Flarsheim R, Vesuvala C, Drasic L (2016) Developing technology to support policymakers in taking a systems science approach to obesity and well-being: T6: S41: 31. Obes Rev 17:194–195 [Google Scholar]
- Giabbanelli PJ, Galgoczy MC, Nguyen DM, Foy R, Rice KL, Nataraj N, Brown MM, Harper CR (2021) Mapping the complexity of suicide by combining participatory modeling and network science. In: Proceedings of the IEEE/ACM international conference on advances in social network analysis and mining (ASONAM) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giabbanelli PJ, Tawfik AA (2019) Overcoming the PBL assessment challenge: Design and development of the incremental thesaurus for assessing causal maps (ITACM). Technol Knowl Learn 24(2):161–168 [Google Scholar]
- Giabbanelli PJ, Tawfik AA (2020) Reducing the gap between the conceptual models of students and experts using graph-based adaptive instructional systems. In: International conference on human-computer interaction. Springer, Cham, pp 538–556 [Google Scholar]
- Giabbanelli PJ, Tawfik AA (2021) How perspectives of a system change based on exposure to positive or negative evidence. Systems 9(2):23 [Google Scholar]
- Giabbanelli PJ, Tawfik AA, Gupta VK (2019) Learning analytics to support teachers’ assessment of problem solving: a novel application for machine learning and graph algorithms. In Utilizing learning analytics to support study success, pp 175–199 [Google Scholar]
- Giabbanelli PJ, Torsney-Weir T, Mago VK (2012) A fuzzy cognitive map of the psychosocial determinants of obesity. Appl Soft Comput 12(12):3711–3724 [Google Scholar]
- Giles BG, Findlay CS, Haas G, LaFrance B, Laughing W, Pembleton S (2007) Integrating conventional science and aboriginal perspectives on diabetes using fuzzy cognitive maps. Soc Sci Med 64(3):562–576 [DOI] [PubMed] [Google Scholar]
- Gray SA, Gray S, Cox LJ, Henly-Shepard S (2013) Mental modeler: a fuzzy-logic cognitive mapping modeling tool for adaptive environmental management. In: 2013 46th Hawaii international conference on system sciences. IEEE, pp 965–973 [Google Scholar]
- Gray S, Hilsberg J, McFall A, Arlinghaus R (2015) The structure and function of angler mental models about fish population ecology: the influence of specialization and target species. J Outdoor Recreat Tour 12:1–13 [Google Scholar]
- Gray S, Sterling EJ, Aminpour P, Goralnik L, Singer A, Wei C et al. (2019) Assessing (social-ecological) systems thinking by evaluating cognitive maps. Sustainability 11(20):5753 [Google Scholar]
- Gupta VK, Giabbanelli PJ, Tawfik AA (2018) An online environment to compare students’ and expert solutions to ill-structured problems. In: International conference on learning and collaboration technologies. Springer, Cham, pp 286–307 [Google Scholar]
- Hall KD, Sacks G, Chandramohan D, Chow CC, Wang YC, Gortmaker SL, Swinburn BA (2011) Quantification of the effect of energy imbalance on bodyweight. Lancet 378(9793):826–837 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayward J, Morton S, Johnstone M, Creighton D, Allender S (2020) Tools and analytic techniques to synthesise community knowledge in CBPR using computer-mediated participatory systemmodelling. NPJ Digit Med 3(1):1–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedegaard H, Curtin SC, Margaret W (2020) Increase in suicide mortality in the United States, 1999–2018 [PubMed]
- Hedelin B, Gray S, Woehlke S, Todd KB, Alison S, Jordan R, Moira Z et al. (2021) What’s left before participatory modeling can fully support real-world environmental planning processes: A case study review. Environ Model Softw 143:105073 [Google Scholar]
- Henly-Shepard S, Gray SA, Cox LJ (2015) The use of participatory modeling to promote social learning and facilitate community disaster planning. Environ Sci Policy 45:109–122 [Google Scholar]
- Heron MP (2019) Deaths: leading causes for 2017 [USA]. In: National vital statistics reports: from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System, vol 68, no 6, pp 1–77 [PubMed] [Google Scholar]
- Hester PT, Adams KM (2017) Complex systems modeling. In: Systemic decision making. Springer, Cham, pp 101–125 [Google Scholar]
- Ifenthaler D, Masduki I, Seel NM (2011) The mystery of cognitive structure and how we can detect it: tracking the development of cognitive structures over time. Instr Sci 39(1):41–61 [Google Scholar]
- Isaac ME, Dawoe E, Sieciechowicz K (2009) Assessing local knowledge use in agroforestry management with cognitive maps. Environ Manage 43(6):1321–1329 [DOI] [PubMed] [Google Scholar]
- Ivey-Stephenson AZ (2020) Suicidal ideation and behaviors among high school students—youth risk behavior survey, USA. MMWR Suppl 69:47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeong AC (2020) Developing computer-aided diagramming tools to mine, model and support students’ reasoning processes. Educ Tech Res Dev 68(6):3353–3369 [Google Scholar]
- Jeong A (2016) Facilitating collaborative problem-solving with computer-supported causal mapping. In: Proceedings of the 19th ACM conference on computer supported cooperative work and social computing companion, pp 57–60 [Google Scholar]
- Jetter AJ (2006) Fuzzy cognitive maps for engineering and technology management: What works in practice? In: 2006 technology management for the global future-PICMET 2006 conference, vol 2. IEEE, pp 498–512 [Google Scholar]
- Jordan R, Gray S, Zellner M, Glynn PD, Voinov A, Hedelin B et al. (2018) Twelve questions for the participatory modeling community. Earth’s Fut 6(8):1046–1057 [Google Scholar]
- Kim H, Andersen DF (2012) Building confidence in causal maps generated from purposive text data: mapping transcripts of the Federal Reserve. Syst Dyn Rev 28(4):311–328 [Google Scholar]
- Kruse R, Borgelt C, Braune C, Mostaghim S, Steinbrecher M (2016) Introduction to fuzzy sets and fuzzy logic. In: Computational intelligence. Springer, London, pp 329–359 [Google Scholar]
- Lavin EA, Giabbanelli PJ, Stefanik AT, Gray SA, Arlinghaus R (2018) Should we simulate mental models to assess whether they agree? In: Proceedings of the annual simulation symposium, pp 1–12 [Google Scholar]
- Levy MA, Lubell MN, McRoberts N (2018) The structure of mental models of sustainable agriculture. Nat Sustain 1(8):413–420 [Google Scholar]
- Mamdani EH (1977) Application of fuzzy logic to approximate reasoning using linguistic synthesis. IEEE Trans Comput 26(12):1182–1191 [Google Scholar]
- McGlashan J, Hayward J, Brown A, Owen B, Millar L, Johnstone M et al. (2018) Comparing complex perspectives on obesity drivers: action-driven communities and evidence-oriented experts. Obes Sci Pract 4(6):575–581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGlashan J, Johnstone M, Creighton D, de la Haye K, Allender S (2016) Quantifying a systems map: network analysis of a childhood obesity causal loop diagram. PLoS ONE 11(10):e0165459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McNeese MD, Ayoub PJ (2011) Concept mapping in the analysis and design of cognitive systems: a historical review. Appl Concept Mapp, Captur, Anal Organ Knowl 47:3–21 [Google Scholar]
- McPherson K, Marsh T, Brown M (2007) Foresight report on obesity. Lancet 370(9601):1755. [DOI] [PubMed] [Google Scholar]
- Merlin MMM, Mary MFJ, Aishwarya R (2020) A Pythagorean FCM Analysis on the impacts of adverse childhood experiences in learning of school children. Eur J Mol Clin Med 7(9):2020 [Google Scholar]
- Mkhitaryan S, Giabbanelli PJ, de Vries NK, Crutzen R (2020) Dealing with complexity: How to use a hybrid approach to incorporate complexity in health behavior interventions. Intell-Based Med 3:100008 [Google Scholar]
- Morris MA, Wilkins E, Timmins KA, Bryant M, Birkin M, Griffiths C (2018) Can big data solve a big problem? Reporting the obesity data landscape in line with the Foresight obesity system map. Int J Obes 42(12):1963–1976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray-Smith DJ (2012) Continuous system simulation. Springer [Google Scholar]
- Naumann RB, Austin AE, Sheble L, Lich KH (2019) System dynamics applications to injury and violence prevention: a systematic review. Curr Epidemiol Rep 6(2):248–262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Owen B, Brown AD, Kuhlberg J, Millar L, Nichols M, Economos C, Allender S (2018) Understanding a successful obesity prevention initiative in children under 5 from a systems perspective. PLoS ONE 13(3):e0195141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Page A, Atkinson JA, Heffernan M, McDonnell G, Hickie IB (2017) A decision-support tool to inform Australian strategies for preventing suicide and suicidal behaviour. Public Health Res Pract 27(2):e2721717. [DOI] [PubMed] [Google Scholar]
- Page A, Atkinson JA, Heffernan M, McDonnell G, Prodan A, Osgood N, Hickie I (2018) Static metrics of impact for a dynamic problem: The need for smarter tools to guide suicide prevention planning and investment. Aust N Z J Psych 52(7):660–667 [DOI] [PubMed] [Google Scholar]
- Papageorgiou E, Areti K (2012) Using fuzzy cognitive mapping in environmental decision making and management: a methodological primer and an application. In: Young S, Silvern S (eds) International perspectives on global environmental change. InTech, Rijeka, Croatia, p 427–450 [Google Scholar]
- Penn AS, Knight CJ, Lloyd DJ, Avitabile D, Kok K, Schiller F et al. (2013) Participatory development and analysis of a fuzzy cognitive map of the establishment of a bio-based economy in the Humber region. PLoS ONE 8(11):e78319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pillutla VS, Giabbanelli PJ (2019) Iterative generation of insight from text collections through mutually reinforcing visualizations and fuzzy cognitive maps. Appl Soft Comput 76:459–472 [Google Scholar]
- Plemmons G, Matthew H, Stephanie D, James G, Charlotte B, Whitney B, Robert C et al. (2018) Hospitalization for suicide ideation or attempt: 2008–2015. Pediatrics 141(6):e20172426. [DOI] [PubMed] [Google Scholar]
- Reddy T, Giabbanelli PJ, Mago VK (2019) The artificial facilitator: guiding participants in developing causal maps using voice-activated technologies. In: International conference on human-computer interaction. Springer, Cham, pp 111–129 [Google Scholar]
- Reddy T, Srivastava G, Mago V (2020) Testing the causal map builder on Amazon Alexa. In: World conference on information systems and technologies. Springer, Cham, pp 449–461 [Google Scholar]
- Rogers ML, Joiner TE (2019) Exploring the temporal dynamics of the interpersonal theory of suicide constructs: a dynamic systems modeling approach. J Consult Clin Psychol 87(1):56. [DOI] [PubMed] [Google Scholar]
- Rozenfeld HD, Kirk JE, Bollt EM, Ben-Avraham D (2005) Statistics of cycles: How loopy is your network? J Phys a: Math Gen 38(21):4589 [Google Scholar]
- Ruiz-Primo MA (2000) On the use of concept maps as an assessment tool in science: What we have learned so far. REDIE Rev Electrón Invest Educ 2(1):29–53 [Google Scholar]
- Siokou C, Morgan R, Shiell A (2014) Group model building: a participatory approach to understanding and acting on systems. Public Health Res Pract 25(1):e2511404. [DOI] [PubMed] [Google Scholar]
- Ulijaszek S (2015) With the benefit of Foresight: obesity, complexity and joined-up government. BioSocieties 10(2):213–228 [Google Scholar]
- van Vliet M, Kok K, Veldkamp T (2010) Linking stakeholders and modellers in scenario studies: the use of Fuzzy Cognitive Maps as a communication and learning tool. Futures 42(1):1–14 [Google Scholar]
- Vasslides JM, Jensen OP (2016) Fuzzy cognitive mapping in support of integrated ecosystem assessments: developing a shared conceptual model among stakeholders. J Environ Manage 166:348–356 [DOI] [PubMed] [Google Scholar]
- Voinov A, Jenni K, Gray S, Kolagani N, Glynn PD, Bommel P et al. (2018) Tools and methods in participatory modeling: selecting the right tool for the job. Environ Model Softw 109:232–255 [Google Scholar]
- Waqa G, Moodie M, Snowdon W, Latu C, Coriakula J, Allender S, Bell C (2017) Exploring the dynamics of food-related policymaking processes and evidence use in Fiji using systems thinking. Health Res Policy Syst 15(1):1–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- White E, Mazlack LJ (2011) Discerning suicide notes causality using fuzzy cognitive maps. In: 2011 IEEE international conference on fuzzy systems (FUZZ-IEEE 2011). IEEE, pp 2940–2947 [Google Scholar]
- World Health Organization (2014) Preventing suicide: a global imperative. World Health Organization, Geneva [Google Scholar]
- Xu Z, Da QL (2003) An overview of operators for aggregating information. Int J Intell Syst 18(9):953–969 [Google Scholar]
- Yoon BS, Jetter AJ (2016) Comparative analysis for fuzzy cognitive mapping. In: 2016 Portland international conference on management of engineering and technology (PICMET). IEEE, pp 1897–1908 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Our data are provided on a thirdparty repository by the Open Science Framework (OSF), which can be publicly accessed without registration at https://osf.io/7nxp4/In particular, the online repository includes the individual map from each SME, the questionnaires used to assign weights to causal relationships, the overall map, and the software used to visualize the map.