

Abstract
Objective
The aim of the study was to compare the cleaning efficiency of XP Finisher (FKG Dentaire, La Chaux-de-Fonds, Switzerland), XP Finisher R (FKG Dentaire), and passive ultrasonic irrigation after root canal retreatment.
Methods
A total of 75 single-rooted human teeth were decoronated, instrumented using HyFlex EDM rotary files (Coltène/Whaledent Inc., Altstätten, Switzerland), and filled with gutta-percha and the TotalFill HiFlow bioceramic sealer (FKG Dentaire) using the warm vertical compaction technique. Retreatment was performed with D-Race rotary files (FKG Dentaire). Samples were randomly divided into five groups according to the activation protocol used. Samples were sectioned longitudinally and prepared for the scanning electron microscope. The percentages of cleaned canal walls in each third of the canal were determined using the ImageJ software. The one-way ANOVA test was used to make comparisons among all of the tested groups, with a pairwise comparison made with the Bonferroni correction. The significance level was set at P≤0.05.
Results
Results showed that none of the activation techniques used resulted in complete canal cleanliness. However, XP Finisher R and XP Finisher had better cleaning ability compared with passive ultrasonic irrigation in all thirds of each root canal (P<0.001).
Conclusion
The cleaning efficiency of XP Finisher R and XP Finisher was superior to that of passive ultrasonic irrigation after the retreatment of the hydraulic calcium silicate sealer.
Keywords: Bioceramic sealer, oval canals, passive ultrasonic irrigation, retreatment, XP Finisher R, XP Finisher
HIGHLIGHTS
The percentage of cleaned walls was higher when a supplemental method was used to activate NaOCl and EDTA.
The XP Finisher R and XP Finisher could be used to enhance surface cleanliness after retreatment of hydraulic calcium silicate sealers.
The apical third of the root canal is the most difficult area to clean.
All of the used methods failed to produce completely clean canal walls.
INTRODUCTION
When root canal treatment fails to promote healing, the first option for preserving the tooth is nonsurgical endodontic retreatment. The persistence of microbial infection in the root canal system and/or the periradicular area has been identified as the primary cause of failure (1). A retreatment procedure in such cases aims to disinfect the root canal space and reduce the microbial population through the complete removal of all filling materials (2), and the dentine surface must be cleaned to facilitate the direct action of irrigation and intracanal medications to create conditions conducive to periradicular healing (3).
Several approaches for removing root-filling material have been proposed, including manual instruments with or without chemical solvents, heated instruments, Gates-Glidden drills, and rotary or reciprocation systems (4-7). Although these techniques can be considered effective, no retreatment protocol can completely remove all the filling material, particularly in the apical third (8). Supplementary methods have therefore been advocated for more efficient removal of the remaining filling materials. Passive ultrasonic irrigation (PUI) utilises acoustic microstreaming and cavitation effects without direct contact with the dentine walls (9). PUI can be used to remove dentinal debris, organic tissue, or calcium hydroxide from inaccessible root canal areas and also root canal sealers during retreatment procedures (10, 11). The use of ultrasonics in endodontic retreatment has been previously reported in the literature. One study proposes that irrigant activation using ultrasonics can help in the removal of filling materials in oval canals (12).
The new innovative alloy, MaxWire (Martensite-Austenite Electropolish Flex; FKG Dentaire, La Chaux-de-Fonds, Switzerland), with new properties for transitioning between martensite (M-phase) at room temperature and austenite (A-phase) at body temperature, was used in the manufacturing of both the XP Finisher (XPF) and XP Finisher R (XPR). When exposed to the body temperature, this alloy transforms into the A-phase, assuming a spoon shape of 1.5 mm in depth in the last 10 mm. The A-phase allows the instrument to reach inaccessible areas, activating the irrigating solution without changing the canal shape (13).
Recently, XPR (FKG Dentaire) has been launched to aid in retreatment cases. According to the manufacturer, it has a core diameter of (ISO no. 30), which is bigger than the core diameter of XPF (ISO no. 25). The stiffer core is supposed to be more efficient in removing root filling materials, especially in oval canals (8). The purpose of this file is to scrape the dentine surface and/or root filling material while maintaining the canal’s original shape (14).
The TotalFill HiFlow bioceramic (BC) sealer (FKG Dentaire) is a premixed ready-to-use injectable calcium phosphate silicate-based cement that can be used in warm filling techniques (15, 16). Its major inorganic components include tricalcium silicate, dicalcium silicate, calcium phosphates, colloidal silica, and calcium hydroxide. It uses zirconium oxide as the radiopacifier and contains water-free thickening vehicles to enable the sealer to be delivered in the form of a premixed paste (17, 18). According to the manufacturer, this new sealer has a lower viscosity when heated and is more radiopaque than its predecessor. However, there is no information on its retreatability in the literature (19).
The aim of this study was to compare the cleaning efficiency of XPF, XPR, and PUI after the retreatment of root canals filled with TotalFill Hiflow BC sealer using a warm vertical compaction technique. The null hypothesis tested was that there is no significant difference in the cleanliness of XPF, XPR, and PUI after the removal of obturation material from root canals during root canal retreatment.
MATERIALS AND METHODS
Sample selection and root canal filling
The research proposal was approved by the local Research Ethics Committee (Registration no. 315/2020). Seventy-five freshly extracted human single-rooted lower premolars that had been extracted for orthodontic reasons were used. After extraction, soft tissues, debris, and calculus were removed using an ultrasonic scaler.
Preoperative radiographs were taken in the buccolingual and mesiodistal directions to confirm the presence of a single oval canal Type I Vertucci (20) and curvature of less than 5 degrees measured using the Schneider method (21). Exclusion criteria included teeth that showed calcification or open apices, teeth with previous endodontic treatment or heavily restored teeth, and teeth with signs of resorption (internal or external resorption).
Teeth were decoronated at the level of the cementoenamel junction using a diamond saw mounted on a low-speed micromotor under water coolant to adjust the length of the roots to a standardised length of 13 mm. The tooth length was established using a #10 K-file (MANI, Inc., Utsunomiya, Tochigi, Japan) until the tip of the file was visible from the apex. The working length (WL) was calculated by subtracting 1 mm from the tooth length. Root canal preparation was done using Hyflex EDM rotary nickel-titanium instruments (Coltène/Whaledent Inc., Altstätten, Switzerland). The sequence included orifice opener 25/.12, glide path file size 10/.05, shaping file size 25/.04, and finishing file size 40/.04, all operated at 500 rpm with a torque of 2.5 Ncm, except for the glide path file, which was used at 300 rpm and a torque of 1.8 Ncm according to the manufacturer’s instructions using the X-smart rotary endodontic motor (Dentsply-Sirona Endodontics, Ballaigues, Switzerland). In between each step the canals were thoroughly irrigated with 2 ml of 2.5% sodium hypochlorite (NaOCl; Clorox Company, HC Egypt, Cairo, Egypt) using a 30-gauge NaviTip needle (Ultradent Products, Inc., South Jordan, Utah, USA) adapted to a disposable plastic syringe; it was placed 1 mm short of the WL, and patency was established between every file using a #10 K-file. After the last instrument was used, each canal was irrigated with 5 ml of 2.5% NaOCl, 5 ml distilled water followed by 5 ml of 17% EDTA (Cerkamed, Stalowa Wola, Poland), and a final flush with 5 ml distilled water and dried with paper points (Cerkamed).
Samples were sealed with warm vertical compaction technique using gutta-percha (Cerkamed) size 40/.04 and TotalFill HiFlow BC sealer according to the manufacturer’s instructions. The downpack procedure was performed with the EQ-V Pack (Meta Biomed Co. Ltd., Chungcheongbuk-do, Republic of Korea) set at 180°C with a heater plugger size of 50/.04 until reaching 3 mm from the WL, followed by compaction by hand pluggers (DiaDent, Cheongju, Republic of Korea). The backfill procedure was performed with the EQ-V fill handpiece of the EQ-V obturation unit (Meta Biomed Co. Ltd.) and 23-gauge needle tips containing gutta-percha at a temperature of 200 °C and condensed at the orifice level with hand pluggers. Postoperative radiographs were taken to check the quality of obturation. The access of canals was sealed with Cavit-G (3M ESPE, Seefeld, Germany). Teeth were stored in 100% humidity at 37°C for 4 months (22).
Retreatment technique
D-Race retreatment files (FKG Dentaire) were operated at 800 rpm. The DR1 instrument (size 30/.10) was used to remove the coronal third of the root filling (4 mm). The DR2 instrument (size 25/.04) was used with light apical pressure until the WL was reached. Following the manufacturer’s instructions, the DR2 file was used only for one canal. If the WL was not reached, C+ files (Dentsply-Sirona Endodontics) of sizes 6, 8, 10 and 15 were used to negotiate the canals and maintain patency. Finally, the Hyflex EDM finishing file size 40/.04 (Coltène/Whaledent Inc.) was used at 500 rpm and a torque of 2.5 Ncm. During the retreatment procedure, each canal was irrigated with a total of 10 ml of 2.5% NaOCl. Smooth canal walls and no visible filling material on the instruments were required for the retreatment procedures to be completed, and this was confirmed by radiographic examination.
Samples were randomly divided using the Research Randomizer (https://www.randomizer.org) into five equal groups (n=15) as follows (Fig. 1):
Figure 1.

Schematic representation of different activation protocols used in all groups
XPF: XP Finisher, XPR: XP Finisher R, PUI: Passive ultrasonic irrigation, NaOCI: Sodium hypochlorite, EDTA: Ethylenediaminetetraacetic acid
Syringe irrigation (n=15): 5 ml of 2.5% NaOCl was flushed into the canal using the conventional syringe technique with a 30-gauge NaviTip needle adapted to a disposable plastic syringe placed up to 1 mm short of the WL, with a gentle in-and-out movement. Then, 5 ml of distilled water was flushed, followed by 5 ml of 17% EDTA as a final irrigant and washing with 5 ml of distilled water to serve as a positive control.
Negative control group (n=15): 5 ml of distilled water was used.
XP finisher and XP finisher R groups
For both the XPF and XPR groups, instruments were cooled down (Frost Spray; Macro Group Pharmaceutical S.A.E., Cairo, Egypt) following the manufacturer’s instructions and removed from the plastic tubes. Each canal was filled with 5 ml of 2.5% NaOCl and the file was inserted 1 mm shorter than the WL; adjusted using the plastic tube to fix the rubber stopper and operated at 800 rpm at a torque of 1 Ncm for 1 minute using slow and gentle lengthwise movements of 7 to 8 mm. The instrument was removed from the canal, and then 5 ml of distilled water was flushed, followed by 5 ml of 17% EDTA (the instrument activated the EDTA in the same manner) and then washed with 5 ml of distilled water.
Passive ultrasonic irrigation (PUI) group
The E1 Irrisonic tip, 0.20 mm in diameter (Helse Ultrasonic, Santa Rosa de Viterbo, Brazil), mounted on a pecker ultrasonic unit (Guilin Woodpecker Medical Instrument Co. Ltd., Guilin, China) with the power set at 10% (30 Hz) was used. A total of 5 ml of 2.5% NaOCl was used per canal during a 1-min activation time (3 cycles of 20 seconds), and then 5 ml of distilled water was flushed, followed by 5 ml of 17% EDTA with the same motion. The tip was placed 2 mm coronal to the WL, and an up-and-down motion without touching the walls was applied for 20 seconds with intermittent flux; the area was then washed with 5 ml of distilled water.
The NaOCl solution used in all groups was warmed to 37°C before application to allow the XPF and XPR to work optimally at the A-phase. All root canals were prepared, filled, and retreated by the same experienced operator to reduce inter-operator variability with the aid of an operating microscope (Global Surgical Corp., St. Louis, Missouri, USA) at 5× magnification.
Scanning electron microscopy
A small cotton pellet was placed inside the coronal opening of each sample to prevent dentinal shavings or debris from entering the root canal. Each root was notched longitudinally without penetrating the canal using a diamond disc with a straight handpiece. It was then grooved horizontally at two levels at 4 and 8 mm from the root apices using a diamond bur to define the coronal, middle, and apical thirds. The roots were split gently into two halves with the aid of a chisel, and the optimum half of each root was used for the scanning electron microscope (SEM) examination of the coronal, middle, and apical thirds. The samples were left to dry overnight and were then mounted on copper stubs and coated with gold using a fine coat-sputtering device. They were then examined and photographed using a SEM at magnification 1000 × at 20,000 kV and a low vacuum. Data from SEM images were analysed using the ImageJ software (ImageJ 1.41A; National Institutes of Health, Bethesda, Maryland, USA).
Image analysis
Measurements were done by an examiner who was blinded to the study groups. All images were cropped at fixed dimensions (left, 14; right, 0; top, 3; bottom, 61 pixels) using standardised image editor software. The image was cropped to remove the black edges that would interfere with the measurement of the actual dental tissue. The total surface area of all images measured by the ImageJ software after cropping was of a fixed value of 263,760 pixels. All images were transferred to 8-bit type. The adjust/threshold function was used to identify the area that was to be measured to calculate the area of debris (residual filling material, debris, and smear layer). The create selection function from the edit/selection menus was then used to delineate the area identified in the previous step. The analyse/measure function was used to measure the area of interest (Fig. 2). The percentage of the cleaned area in relation to the total surface area of the image was calculated by the following equation:
Figure 2.

(a) Adjusting the threshold to measure the area of the dentine debris and smear layer. (b) The analyse\measure function was used to measure the area free of smear layer
The surface area of cleaned area × 100/Total surface area of the image.
Statistical analysis
The independent t-test was used to compare the control group with each intervention group. The repeated measures ANOVA test was used to compare sections. The one-way ANOVA test was used to make comparisons among all of the tested groups, and a pairwise comparison was made with the Bonferroni correction. The significance level was set at p≤.05. Statistical analysis was performed with IBM SPSS Statistics Version 25 for Windows (IBM Corp., Armonk, New York, USA).
RESULTS
Among the roots of the five groups, completely cleaned roots were never found. Results presented as mean values and standard deviations indicated that XPR had a higher nonsignificant mean cleaning percentage compared with XPF in all root sections (Fig. 3). Both instruments resulted in better cleaning in the middle root third compared to other sections with XPR achieving (86.49±1.95%) and XPF achieving (85.97±2.1%) cleaned surface areas.
Figure 3.
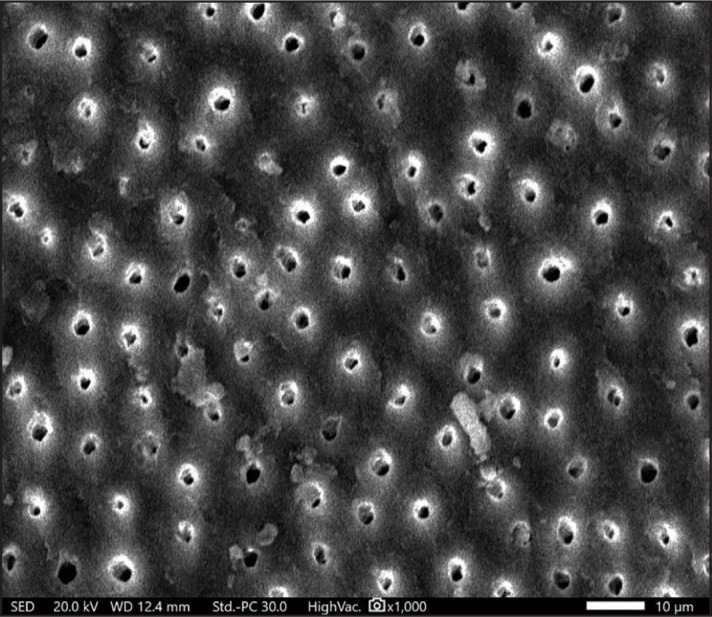
SEM micrographs of the middle third of the dentine surface of the XPR group (x 1000)
SEM: Scanning electron microscope, XPR: XP Finisher R
On the other hand, PUI had a significantly lower mean percentage of cleaned area compared with both XPR and XPF in all root sections. Regarding the XPR group, the coronal third (84.16±2.11%) and middle third (86.49±1.95%) showed a higher significant cleaning percentage compared with the apical third (76.77±3.65%) at P<0.001. PUI group in the apical third showed the lowest mean percentage of cleaned area compared to XPR and XPF (65.85±1.07%) (Fig. 4).
Figure 4.
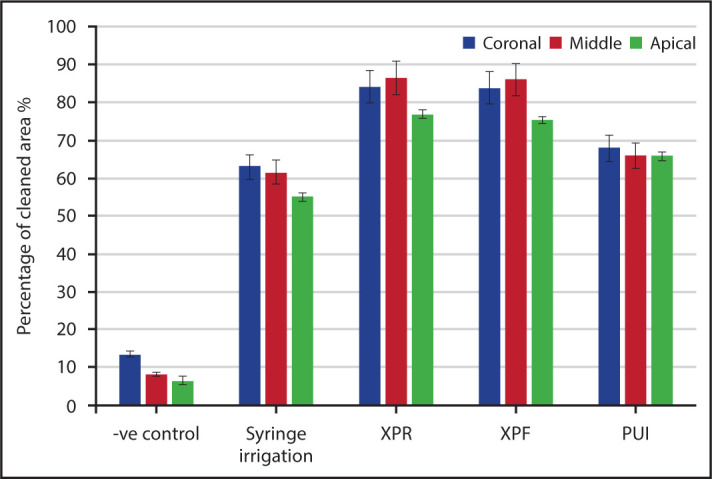
Bar chart showing mean percentage and standard deviations of cleaned area for root sections of different tested groups and comparisons of the cleanliness between different root sections
XPR: XP Finisher R, XPF: XP Finisher, PUI: Passive ultrasonic irrigation
DISCUSSION
Currently, there is rising interest in the use of bioactive materials in endodontics for an extensive variety of applications, ranging from pulp capping to apexification and including root canal sealing. Recent investigations revealed that the TotalFill HiFlow BC sealer had a higher frequency of failure in the reestablishment of patency after retreatment with significantly more residuals, suggesting serious difficulty in removing during retreatment (15, 23, 24). The retreatability of the TotalFill HiFlow BC sealer used in the warm canal filling technique has not been thoroughly investigated. This study compared surface cleanliness using XPF, XPR, and PUI after removal of obturation material from root canals during nonsurgical root canal retreatment.
New instruments and supplementary protocols for the removal of the remaining filling material have been proposed, and the results are currently promising (8, 25). Their use is considered mandatory in the retreatment of oval canals, where the filling material fills the polar areas and its removal is therefore hindered (26-28). Studies showed that when root canals with complex anatomic features were filled with the warm vertical technique and submitted to retreatment, proper cleaning was difficult to accomplish (12).
Warm gutta-percha filling techniques demand the use of root canal sealers that can tolerate the heating process. The TotalFill HiFlow BC sealer has been recently developed as a modification of the hydraulic calcium silicate TotalFill BC sealer, the modified version is claimed by the manufacturer to be able to resist heat and is recommended for use with the warm vertical compaction obturation technique (19, 29).
For this study to have clinical relevance, the teeth filled were stored for 4 months before the retreatment process. Previous studies on the removal of root fillings used a 1- to 2-week storage period to allow for the complete setting of the sealer (15). In clinical scenarios, a patient may seek retreatment several months or years after the original root canal treatment, necessitating a prolonged storage period. Retreatment was done up to size 40/.04, and no attempt was made to increase the apical enlargement beyond the initial preparation size. Thus, the results obtained could merely be due to the effect of the supplemental protocols used.
The results of this study showed large areas of debris and a smear layer in the syringe irrigation group and confirmed that the combination of NaOCl and EDTA is ineffective in rendering root canals completely free from root fillings and a smear layer (22, 30, 31). The mean percentages of cleaned walls were higher in the experimental groups than in the syringe irrigation group, and this indicates that the supplemental methods used to activate NaOCl and EDTA are more effective in debris and smear layer removal. Results also showed that in all studied groups, the apical third showed the least percentage of cleaned walls (Fig. 5). This finding is in line with almost all previously published studies on this subject (11, 12, 31, 32). It is possible that dampening of agitation forces occurred due to contact of the ultrasonic tip against the root canal walls or that the smaller canal size of the apical third compared with the other regions limited the semiactive tip of the XPF and XPR from removing debris and the smear layer in the apical part.
Figure 5.
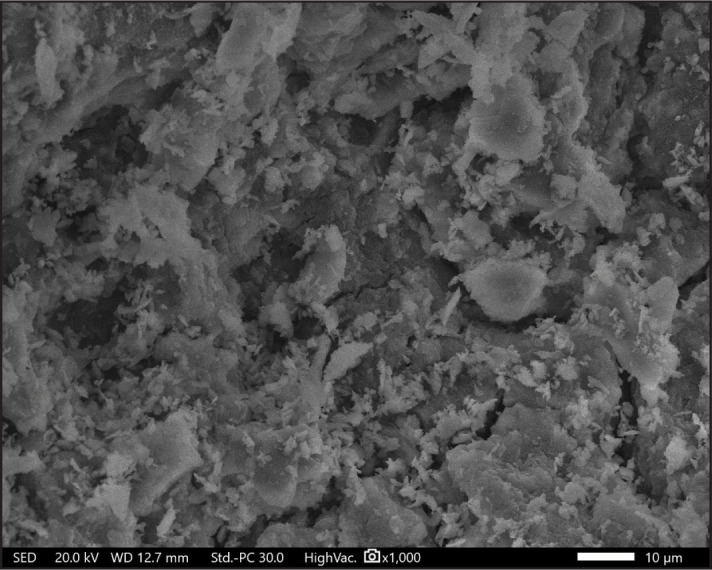
SEM micrographs of the apical third of the dentine surface of the negative control group (x1000)
SEM: Scanning electron microscope
The results showed that the XPR and XPF files had higher significant cleaning efficiency results in all root segments than the PUI; thus, the null hypothesis was rejected. This finding can be attributed to XPR and XPF metallurgy. The development and manufacture of these files are dependent on the shape-memory principles of the NiTi alloy. The file is straight in its M-phase, which is formed when it is cooled. When the file is subjected to body temperature (i.e., the canal), it will transform its shape into the A-phase. Its shape in this phase allows the file to contact and clean areas that are otherwise inaccessible with regular instruments (30). Using microcomputed tomographic (micro-CT) imaging, De-Deus et al. (32) found that XPR was associated with greater root filling removal (32.79%) when compared to PUI (12.81%) (P<0.05). They suggested that the mechanical action of XPR may allow the instrument's tip to touch and dislodge root filling material from the canal walls even in some hard-to-reach areas, which was more effective in displacing existing root filling material than activation of irrigating solutions using PUI.
The XPR group showed a higher percentage of cleaned walls than the XPF group, with no significant differences between them. This result was in agreement with the findings of Silva et al. (8), who found that both files were equally effective for the removal of remaining filling material from straight oval-shaped canals using micro-CT imaging. It is also in agreement with the study of Alzuabi and Abiad (33), who concluded that the XPF and the XPR removed debris from the root canal walls after retreatment with no significant difference. The XPR instrument differs in its core diameter and the angulation of its tip compared with the XPF file, and this makes it potentially more aggressive for removing filling material. However, both the XPR and XPF files can follow the canal morphology owing to their ability to work in a mixed-phase (M-phase/A-phase), which allows them to scout for filling remnants.
PUI had a significantly higher percentage of cleaned walls than syringe irrigation. A previous study showed that ultrasonic activation of the irrigation with Irrisafe tips was effective in eliminating debris and opening up dentinal tubules (34). During PUI, energy is conveyed through ultrasonic waves from the file to the irrigant, producing two physical phenomena: acoustic streaming and cavitation. Acoustic streaming is a rapid movement of fluid in a circular manner like a vortex around the file, and cavitation is the distortion of the existing bubbles in the irrigant. Additionally, the tip vibration could result in gutta-percha plasticisation and sealer debonding, and this would explain the higher cleaning ability than in syringe irrigation (35).
In the present study, the cleaning efficiency was examined based on the numerical evaluation methodology of SEM images of the coronal, middle, and apical thirds of the canals. This was like the descriptions in previously published studies examining the cleaning efficacy of different irrigation protocols and devices (11, 30). SEM examination has various limitations, such as the ability to assess only limited areas of the canal wall. To overcome this limitation, the canal walls were thoroughly inspected by SEM, and the area with the most debris and a smear layer was photographed so that each third of the canal could be examined (36). It is worth mentioning that the amount of debris and smear layer left in the root canal walls may have been affected by the mounting, sectioning, and gold sputtering during the SEM process (37). Another limitation is that the canal anatomy in clinical cases would be much more complex than single-rooted teeth used in this study. Nevertheless, our study may lay a foundation for further studies using teeth with more complex anatomy. Future studies should evaluate if the additional use of solvents in the retreatment of bioceramic sealers would improve the cleaning performance of XPR, XPF, and PUI files.
CONCLUSION
Supplementary techniques are effective tools for increasing the cleanliness of root canals after a retreatment procedure. The cleaning efficiency of XPF and XPR was superior to that of PUI after the retreatment of hydraulic calcium silicate sealers.
Footnotes
Please cite this article as: Hassan R, El Zahar S. Cleaning Efficiency of XP Finisher, XP Finisher R and Passive Ultrasonic Irrigation Following Retreatment of Teeth Obturated with TotalFill HiFlow Bioceramic Sealer. Eur Endod J 2022; 7: 143-9
Disclosures
Conflict of interest:
The authors deny any conflict of interest.
Ethics Committee Approval:
This study was approved by The Minia University Faculty of Dentistry Research Ethics Committee (Date: 12/01/2020, Number: 315/2020).
Peer-review:
Externally peer-reviewed.
Financial Disclosure
This study did not receive any financial support.
Authorship contributions
Concept – R.H.; Design – S.E.Z.; Supervision – R.H.; Funding - S.E.Z.; Materials - R.H.; Data collection and/or processing – R.H.; Analysis and/or interpretation – S.E.Z.; Literature search – R.H.; Writing – R.H.; Critical Review – S.E.Z.
References
- 1.Siqueira JF, Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008;34(11):1291–301. doi: 10.1016/j.joen.2008.07.028. [DOI] [PubMed] [Google Scholar]
- 2.Yılmaz F, Koç C, Kamburoğlu K, Ocak M, Geneci F, Uzuner MB, et al. Evaluation of 3 different retreatment techniques in maxillary molar teeth by using micro-computed tomography. J Endod. 2018;44(3):480–4. doi: 10.1016/j.joen.2017.09.006. [DOI] [PubMed] [Google Scholar]
- 3.Siqueira JF., Jr Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001;34(1):1–10. doi: 10.1046/j.1365-2591.2001.00396.x. [DOI] [PubMed] [Google Scholar]
- 4.Bueno CE, Delboni MG, de Araújo RA, Carrara HJ, Cunha RS. Effectiveness of rotary and hand files in gutta-percha and sealer removal using chloroform or chlorhexidine gel. Braz Dent J. 2006;17(2):139–43. doi: 10.1590/s0103-64402006000200011. [DOI] [PubMed] [Google Scholar]
- 5.Hiltner RS, Kulild JC, Weller RN. Effect of mechanical versus thermal removal of gutta-percha on the quality of the apical seal following post space preparation. J Endod. 1992;18(9):451–4. doi: 10.1016/S0099-2399(06)80848-4. [DOI] [PubMed] [Google Scholar]
- 6.Saad AY, Al-Hadlaq SM, Al-Katheeri NH. Efficacy of two rotary NiTi instruments in the removal of Gutta-Percha during root canal retreatment. J Endod. 2007;33(1):38–41. doi: 10.1016/j.joen.2006.08.012. [DOI] [PubMed] [Google Scholar]
- 7.Zuolo AS, Mello JE, Jr, Cunha RS, Zuolo ML, Bueno CE. Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment. Int Endod J. 2013;46(10):947–53. doi: 10.1111/iej.12085. [DOI] [PubMed] [Google Scholar]
- 8.Silva EJNL, Belladonna FG, Zuolo AS, Rodrigues E, Ehrhardt IC, Souza EM, et al. Effectiveness of XP-endo Finisher and XP-endo Finisher R in removing root filling remnants: a micro-CT study. Int Endod J. 2018;51(1):86–91. doi: 10.1111/iej.12788. [DOI] [PubMed] [Google Scholar]
- 9.Wilcox LR. Endodontic retreatment: ultrasonics and chloroform as the final step in reinstrumentation. J Endod. 1989;15(3):125–8. doi: 10.1016/S0099-2399(89)80133-5. [DOI] [PubMed] [Google Scholar]
- 10.van der Sluis LW, Wu MK, Wesselink PR. The evaluation of removal of calcium hydroxide paste from an artificial standardized groove in the apical root canal using different irrigation methodologies. Int Endod J. 2007;40(1):52–7. doi: 10.1111/j.1365-2591.2006.01182.x. [DOI] [PubMed] [Google Scholar]
- 11.Grischke J, Müller-Heine A, Hülsmann M. The effect of four different irrigation systems in the removal of a root canal sealer. Clin Oral Investig. 2014;18(7):1845–51. doi: 10.1007/s00784-013-1161-6. [DOI] [PubMed] [Google Scholar]
- 12.Cavenago BC, Ordinola-Zapata R, Duarte MA, del Carpio-Perochena AE, Villas-Bôas MH, Marciano MA, et al. Efficacy of xylene and passive ultrasonic irrigation on remaining root filling material during retreatment of anatomically complex teeth. Int Endod J. 2014;47(11):1078–83. doi: 10.1111/iej.12253. [DOI] [PubMed] [Google Scholar]
- 13.Alves FR, Marceliano-Alves MF, Sousa JC, Silveira SB, Provenzano JC, Siqueira JF., Jr Removal of root canal fillings in curved canals using either reciprocating single-or rotary multi-instrument systems and a supplementary step with the XP-Endo finisher. J Endod. 2016;42(7):1114–9. doi: 10.1016/j.joen.2016.04.007. [DOI] [PubMed] [Google Scholar]
- 14.FKG XP Endo Shaper. Available at: https://www.fkgiberia.com/sites/default/files/FKG_Catalogue_EN_WEB_201909.pdf Accessed Jun 16, 2022.
- 15.Hess D, Solomon E, Spears R, He J. Retreatability of a bioceramic root canal sealing material. J Endod. 2011;37(11):1547–9. doi: 10.1016/j.joen.2011.08.016. [DOI] [PubMed] [Google Scholar]
- 16.Candeiro GT, Correia FC, Duarte MA, Ribeiro-Siqueira DC, Gavini G. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J Endod. 2012;38(6):842–5. doi: 10.1016/j.joen.2012.02.029. [DOI] [PubMed] [Google Scholar]
- 17.Ha WN, Nicholson T, Kahler B, Walsh LJ. Mineral trioxide aggregate-a review of properties and testing methodologies. Materials (Basel) 2017;10(11):1261. doi: 10.3390/ma10111261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Loushine BA, Bryan TE, Looney SW, Gillen BM, Loushine RJ, Weller RN, et al. Setting properties and cytotoxicity evaluation of a premixed bioceramic root canal sealer. J Endod. 2011;37(5):673–7. doi: 10.1016/j.joen.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 19.FKG. TotalFill HiFlow. Available at: https://www.fkg.ch/products/endodontics/obturation/totalfill-hiflow Accessed 30 Apr, 2021.
- 20.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 21.Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32(2):271–5. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- 22.Pedullà E, Abiad RS, Conte G, Khan K, Lazaridis K, Rapisarda E, et al. Retreatability of two hydraulic calcium silicate-based root canal sealers using rotary instrumentation with supplementary irrigant agitation protocols: a laboratory-based micro-computed tomographic analysis. Int Endod J. 2019;52(9):1377–87. doi: 10.1111/iej.13132. [DOI] [PubMed] [Google Scholar]
- 23.Uzunoglu E, Yilmaz Z, Sungur DD, Altundasar E. Retreatability of root canals obturated using gutta-percha with bioceramic, MTA and resin-based sealers. Iran Endod J. 2015;10(2):93–8. [PMC free article] [PubMed] [Google Scholar]
- 24.Kontogiannis TG, Kerezoudis NP, Kozyrakis K, Farmakis ET. Removal ability of MTA, bioceramic, and resin-based sealers from obturated root canals, following XP-endo® Finisher R file: An ex vivo study. Saudi Endod J. 2019;9(1):8–13. [Google Scholar]
- 25.Bernardes RA, Duarte MAH, Vivan RR, Alcalde MP, Vasconcelos BC, Bramante CM. Comparison of three retreatment techniques with ultrasonic activation in flattened canals using micro-computed tomography and scanning electron microscopy. Int Endod J. 2016;49(9):890–7. doi: 10.1111/iej.12522. [DOI] [PubMed] [Google Scholar]
- 26.Crozeta BM, Silva-Sousa YT, Leoni GB, Mazzi-Chaves JF, Fantinato T, Baratto-Filho F, et al. Micro-computed tomography study of filling material removal from oval-shaped canals by using rotary, reciprocating, and adaptive motion systems. J Endod. 2016;42(5):793–7. doi: 10.1016/j.joen.2016.02.005. [DOI] [PubMed] [Google Scholar]
- 27.Jiang S, Zou T, Li D, Chang JW, Huang X, Zhang C. Effectiveness of sonic, ultrasonic, and photon-induced photoacoustic streaming activation of NaOCl on filling material removal following retreatment in oval canal anatomy. Photomed Laser Surg. 2016;34(1):3–10. doi: 10.1089/pho.2015.3937. [DOI] [PubMed] [Google Scholar]
- 28.Monguilhott Crozeta B, Damião de Sousa-Neto M, Bianchi Leoni G, Francisco Mazzi-Chaves J, Terezinha Corrêa Silva-Sousa Y, Baratto-Filho F. A micro-computed tomography assessment of the efficacy of rotary and reciprocating techniques for filling material removal in root canal retreatment. Clin Oral Investig. 2016;20(8):2235–40. doi: 10.1007/s00784-016-1728-0. [DOI] [PubMed] [Google Scholar]
- 29.Hadis M, Camilleri J. Characterization of heat resistant hydraulic sealer for warm vertical obturation. Dent Mater. 2020;36(9):1183–9. doi: 10.1016/j.dental.2020.05.008. [DOI] [PubMed] [Google Scholar]
- 30.Elnaghy AM, Mandorah A, Elsaka SE. Effectiveness of XP-endo Finisher, EndoActivator, and File agitation on debris and smear layer removal in curved root canals: a comparative study. Odontology. 2017;105(2):178–83. doi: 10.1007/s10266-016-0251-8. [DOI] [PubMed] [Google Scholar]
- 31.Rossi-Fedele G, Ahmed HM. Assessment of root canal filling removal effectiveness using micro-computed tomography: a systematic review. J Endod. 2017;43(4):520–6. doi: 10.1016/j.joen.2016.12.008. [DOI] [PubMed] [Google Scholar]
- 32.De-Deus G, Belladonna FG, Zuolo AS, Cavalcante DM, Carvalhal JCA, Simões-Carvalho M, et al. XP-endo Finisher R instrument optimizes the removal of root filling remnants in oval-shaped canals. Int Endod J. 2019;52(6):899–907. doi: 10.1111/iej.13077. [DOI] [PubMed] [Google Scholar]
- 33.Alzuabi MA, Abiad R. Ability of XP-Endo Finisher and XP-Endo Finisher-R in removal of debris from the root canal walls after retreatment: An in-vitro study. Int Arab J Dent. 2018;9(2) [Google Scholar]
- 34.Mozo S, Llena C, Chieffi N, Forner L, Ferrari M. Effectiveness of passive ultrasonic irrigation in improving elimination of smear layer and opening dentinal tubules. J Clin Exp Dent. 2014;6(1):e47–52. doi: 10.4317/jced.51297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rached-Júnior FA, Sousa-Neto MD, Bruniera JF, Duarte MA, Silva-Sousa YT. Confocal microscopy assessment of filling material remaining on root canal walls after retreatment. Int Endod J. 2014;47(3):264–70. doi: 10.1111/iej.12142. [DOI] [PubMed] [Google Scholar]
- 36.Plotino G, Colangeli M, Özyürek T, DeDeus G, Panzetta C, Castagnola R, et al. Evaluation of smear layer and debris removal by stepwise intraoperative activation (SIA) of sodium hypochlorite. Clin Oral Investig. 2021;25(1):237–45. doi: 10.1007/s00784-020-03358-6. [DOI] [PubMed] [Google Scholar]
- 37.Virdee SS, Seymour DW, Farnell D, Bhamra G, Bhakta S. Efficacy of irrigant activation techniques in removing intracanal smear layer and debris from mature permanent teeth: a systematic review and meta-analysis. Int Endod J. 2018;51(6):605–21. doi: 10.1111/iej.12877. [DOI] [PubMed] [Google Scholar]