

Abstract
Nowadays, metabolic syndrome (MetS) represents a global health challenge in developed and developing countries. The sex hormones disorders in males are related to many clinical co-morbidities. This study aimed to evaluate the total testosterone (TT) to estradiol (E2) ratio as a predictor marker of MetS. This case-control study included 88 MetS patients and 88 healthy individuals (control), in the age range of 18-69 years who were selected among patients who were referring to an outpatient clinic, using a convenience sampling method. The study participants were selected based on their medical history and physical examination, which included waist circumference, blood pressure, serum E2, TT, fasting blood glucose (FBG), triglyceride (TG), and high-density lipoprotein-cholesterol (HDL-C). Diagnosis of MetS was confirmed according to the National Cholesterol Education Program Adult Treatment Panel III guidelines. The findings revealed that the mean TT level was significantly lower among patients with MetS (P<0.001), while the mean E2 level was significantly higher among patients with MetS (P<0.001). The mean TT to E2 ratio was significantly lower among patients with MetS (OR=9.6, P<0.001). There was a significant correlation between MetS components and TT to E2 ratio and waist circumference (WC) (r = - 0.49, P<0.0001). The means of weight, WC, blood pressure, and FBG levels were significantly higher in patients with MetS (P<0.001, P<0.001, P<0.001, P=0.04, respectively), and the lipid profile of patients with MetS was abnormal (TG, P<0.001, HDL-C, P<0.001). Eventually, it can be concluded that the TT to E2 ratio can be regarded as a significant predictor of MetS in males.
Keywords: Estradiol, Iraq, Metabolic syndrome, Testosterone
1. Introduction
The metabolic syndrome (MetS) is also known as syndrome X or insulin resistance (IR) syndrome. It is a collection of metabolic disorders composed of central obesity, hypertension (HTN), IR, and atherogenic dyslipidemia that is considered to be the common risk factor in the development of atherosclerotic cardiovascular disease (CVD) ( 1 ). The MetS was first defined by the World Health Organization (WHO) in 1999 as the insulin resistance or hyperglycemia with high-density lipoprotein cholesterol (HDL-C) level, high triglycerides (TG) level, abdominal obesity, and HTN ( 2 ). The global incidence and prevalence of MetS are various and depend on the epidemiology of MetS components, especially obesity. The epidemiology of MetS is affected by differences in the prevalence of age, gender, ethnicity, and diagnostic criteria. It was shown that MetS affected a fifth or more of the American population and one-quarter of the European population. The prevalence of MetS in South-East Asia countries is low; however, the rate is increasing rapidly, and reaching the rates in the Western world.
The high prevalence of MetS in Middle East countries is related to high obesity prevalence among the population of these countries and accounts for 15-60% of CVD risk factors ( 3 ). In Iraq, the prevalence of MetS reached up to 46.6% among the evaluated samples with the predominance of female gender ( 4 ). The common risk factors included abdominal obesity in addition to diabetes mellitus, abnormal lipid profile, and HTN ( 5 ).
The accumulation of adipose tissue in central obesity results in higher conversion rates of total testosterone (TT) to estradiol (E2) by aromatase activation and inhibits the hypothalamic-pituitary unit leading to the vicious cycle of obese estrogenic hypogonadism ( 6 ). Sex hormones play a major role in improving quality of life and decreasing death rates in males ( 7 - 8 ). There was no published study conducted in Iraq to calculate a cutoff point. Therefore, this study aimed to evaluate the TT to E2 ratio as a predictor marker of MetS.
2. Materials and Methods
2.1. Study Design
This case-control study was conducted in the Faiha Specialized Diabetes, Endocrine, and Metabolism Center (FDEMC) in Basrah city of Iraq from 1st of September, 2020 to 30th of September, 2021.
2.2. Sample Size and Patients
A convenient sample of 88 patients with MetS and 88 healthy individuals were selected from an outpatient clinic in FDEMC.
.3. Data Collection
Data were collected through interviews after convenient sampling of participants. The inclusion criteria included adult patients (in the age range of 18- 69 years), male gender, and confirmed MetS. The exclusion criteria included the history of panhypopituitarism or congenital hypogonadotropic hypogonadism, history of extreme depression or mental disorder, history of head trauma, renal dysfunction, history of hemochromatosis, liver disorders, medicinal intake of steroids or opiates, acute illness, malignancy, prostate disease, alcohol consumption, and history of treatment by testosterone hormone supplementation or aromatase inhibitor in the last three months.
2.4. Assessment Tools
The diagnosis of MetS was confirmed by the study supervisor, according to the National Cholesterol Education Program Adult Treatment Panel-III guideline. Accordingly, MetS was considered to be present if three or more of the following five criteria were observed: WC over ≥102 cm (males), blood pressure (BP) over 130/85 mmHg, fasting TG level over 150 mg/dl, fasting HDL-C level less than 40 mg/dl, and fasting blood glucose (FBG) over 100 mg/dl ( 4 , 9 ).
The top of the right iliac crest was located for measuring WC. A measuring tape was placed in a horizontal plane around the abdomen at the level of the iliac crest, and it was ensured that the tape was snug and parallel to the floor but did not compress the skin.. The Omron® HBP -1300-E portable blood pressure monitor was used to check each patient’s blood pressure while they seated properly for at least five minutes. The arms were rested at the level of the instrument, and an appropriate bladder cuff size was placed to their arm with the back supported. The full history of patients was taken, and an eight milliliter venous blood sample was obtained in the early morning (between 8:05 and 10:00 a.m) using the Cobas E-411 analyzer. Subsequently, TT and E2 hormones, lipid profile, and FBG were assayed using COBAS INTEGRA 400 plus analyzer -Roche (Roche Diagnostics, Mannheim, Germany).
2.5. Clinical Assessment
The information collected from each participant included age, weight, height, body mass index (BMI), WC, and BP for each patient.
2.6. Laboratory Assessment
The test values taken from the patients’ database in FDEMC included TG and HDL-C levels, FBG level, and TT and E2 levels.
2.7. Statistical Analysis
Data were analyzed using SPSS software (Version 22) through one-way analysis of variance (ANOVA), and Kolmogorov–Smirnov test was used to determine the normal distribution of data. Descriptive statistics were presented as mean±standard deviation (SD) and percentages. Data (means) were compared using multiple contingency tables, appropriate statistical tests, and an independent sample t-test. Receiver operating characteristic curve (ROC) was used to assess T to E2 ratio cutoff values predicting MetS. Correlation between metabolic syndrome components as continuous variable and testosterone to estradiol ratio was determined using spearman correlation and blotted as a scatter dots figure. A p-values less than 0.05 (P≤ 0.05) was considered statistically significant, and the results were presented in tables and/or graphs.
3. Results
The mean age of study participants was significantly higher in patients with MetS, compared to healthy individuals (P=0.001). Moreover, weight and WC were significantly higher in patients with MetS (P<0.001). The FBG of study participants was significantly higher in patients with MetS (P=0.04), and BP was significantly higher in patients with MetS (P<0.001). Furthermore, TG level was significantly higher among patients with MetS (P<0.001), while HDL-C was significantly lower among these patients (P=0.001).
The TT level was significantly lower among patients with MetS (P<0.001), and the E2 level was significantly increased in these patients (P<0.001). In addition, TT to E2 ratio was significantly lower among patients with MetS, compared to healthy participants (P<0.001). No significant difference was observed between participants with MetS and controls in terms of height (P=0.17) and BMI (P=0.9) (Table 1).
Table 1.
Distribution of participants’ data according to study groups
| Variable | Study groups | P-value | |
|---|---|---|---|
| MetS | Control | ||
| Age (years) | 45.9±10.9 | 37.9±10.4 | <0.001 |
| Weight (Kg) | 94.6±16 | 81.5±19 | <0.001 |
| Height (cm) | 171.9±6 | 173.5±8.3 | 0.17 |
| BMI (kg/m2) | 29.8±5.9 | 29.8±6.2 | 0.9 |
| WC (cm) | 110.2±10.6 | 95±13.2 | <0.001 |
| BP (mm/Hg) | 143.88±18.13 | 123.77±30.8 | <0.001 |
| FBG (mg/dl) | 134.5±82 | 110.5±64 | 0.04 |
| TG (mg/dl) | 195.8±104.7 | 131.5±73 | <0.001 |
| HDL-C (mg/dl) | 38.3±8.9 | 44.9±10.5 | <0.001 |
| T (ng/ml) | 358.7±143.4 | 459.6±199.2 | <0.001 |
| E2 (Pg/ml) | 49.45±10.8 | 38.1±14.2 | <0.001 |
| T to E2 ratio | 7.6±3.6 | 13.8±8.2 | <0.001 |
MetS: Metabolic syndrome; SD: Standard deviation, BMI: Body mass index; WC: Waist circumference; BP: Blood pressure; FBG: Fasting blood glucose; HDL-C: High density lipoprotein; T: Testosterone; E2: Estradiol
The acceptable cut-off points and the corresponding validity values for TT to E2 ratio in the prediction of MetS are presented in table 2 and figure 1. The Cutoff point of T to E2 ratio obtained at 8.4 had acceptable validity (with a sensitivity of 80.9%, specificity of 70.5%, the positive predictive value of 79.7%, the negative predictive value of 71.2%, accuracy of 78.9%, and odds ratio of 9.6) for predicting MetS.
Table 2.
Prediction of metabolic syndrome by T to E2 ratio
| Cutoff point | Sensitivity | Specificity | PPV | NPV | Accuracy | OR (95%CI) |
|---|---|---|---|---|---|---|
| 7.8 | 86.8% | 65.9% | 78.6% | 64.3% | 74.5% | 12 (5.6-25.5) |
| 8.4 | 80.9% | 70.5% | 79.7% | 71.2% | 78.9% | 9.6 (4.8-19.5) |
| 9.1 | 70.6% | 73.9% | 69.5% | 74.2% | 70.2% | 6.0 (3.1-11.5) |
PPV: Positive predictive value; NPV: Negative predictive value; OR: Odds ratio; CI: Confidence interval
Figure 1.
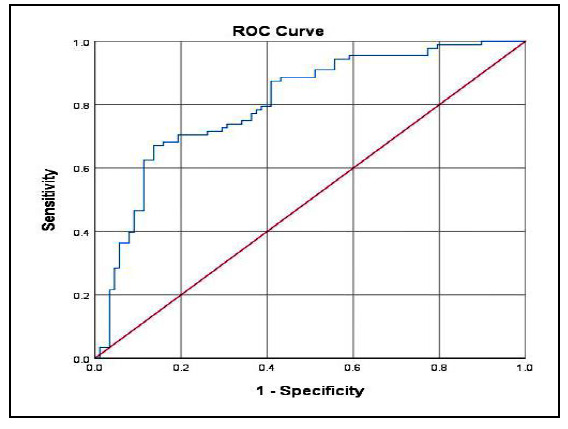
Receiver operating characteristic curve for T to E2 ratio predicting MetS (area under the curve [AUC] =0.8)
TT to E2 ratio had a significant negative correlation with systolic BP, diastolic BP, FBG, WC and TG levels (r=-0.31, P<0.0001; r=-0.22 , P<0.004; r=-0.24, P<0.002; r=-0.49, P<0.0001; r=-0.29, P<0.0001, respectively), and significant positive correlation of HDL-C level (r=0.22, P<0.002) (Figure 2).
Figure 2.
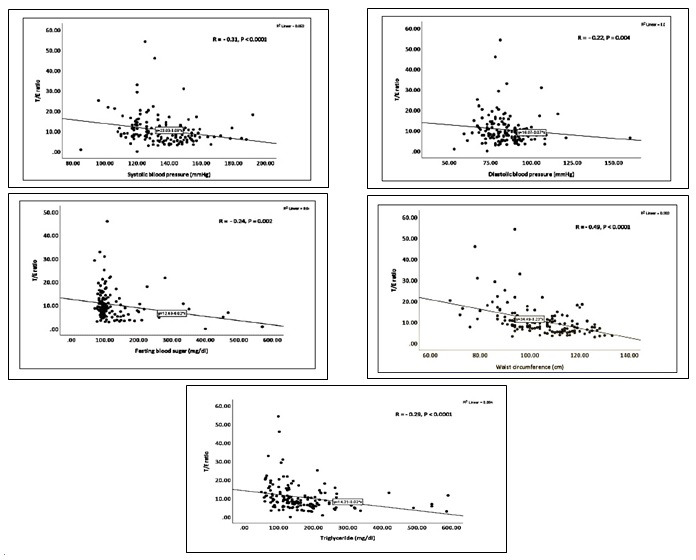
Correlation between testosterone to estradiol ratio and metabolic syndrome components
4. Discussion
Based on the obtained data, the mean TT to E2 ratio of study participants was significantly lower in patients with MetS (P<0.001). This finding was in line with the results of the studies conducted by Bekaert et al. ( 10 ) in Belgium and Hevener et al. ( 11 ) in the United States of America, reporting an obvious decline in TT hormone level with a significant increase in E2 level in patients with MetS. The results of an open-label, non-randomized clinical trial carried out by Alajeely et al. ( 12 ) in Iraq indicated a negative correlation between TT to E2 ratio and male obesity. The results of a cross-sectional study conducted by Kusuma and Siregar ( 13 ) in Indonesia revealed that E2 to TT ratio was elevated in patients with MetS, although the difference was not significant. A multi-center study conducted by Antonio et al. ( 14 ) in eight European countries reported that decreased TT level (but not E2 level) in males was related to a higher risk of developing MetS, regardless of sex hormone binding globulin (SHBG), BMI, or IR. Some studies suggested that reduced levels of TT and SHBG are directly related to development of MetS in males ( 15 - 17 ). Based on the results of present study, mean TT level was significantly lower among patients with MetS (P<0.001). This finding was consistent with those reported by Muraleedharan and Jones ( 18 ) in the UK, indicating that MetS was associated with lower TT levels. Moreover, the mean E2 level was significantly increased among patients with MetS (P<0.001) which confirmed the results obtained in the study conducted by Maggio et al. ( 6 ) in Italy, suggesting a high E2 level in older males with MetS.
The present study showed that means of weight and WC were significantly higher among patients with MetS (P<0.001). This finding was in line with the definition of MetS provided by the International Atherosclerosis Society (IAS) and the International Chair on Cardiometabolic Risk (ICCR) Working Group on Visceral Obesity ( 19 ). The present study showed that the mean FBG of study participants was significantly higher in patients with MetS (P=0.04). This finding was consistent with the results of the study performed by Kurotani et al. ( 20 ) in Japan who reported the importance of FBG in the diagnosis and risk stratification of MetS. In this study, the mean BP of study participants was significantly higher among patients with MetS (P<0.001). This finding was in line with the results of the survey conducted by Zidek et al. ( 21 ) in Germany reporting that HTN was the main component of MetS and that high BP was detected in patients with MetS in the presence and absence of diabetes mellitus.
In the current study, the mean TG level was significantly higher in patients with MetS (P<0.001). Consistently, the results of a longitudinal study performed by Tao et al. ( 22 ) in China revealed a significant longitudinal association between high TG level and other components of MetS. The present study showed that mean HDL-C was significantly lower in patients with MetS (P=0.001). This finding was in line with the results of the study performed by Mani et al. ( 23 ) in the USA, suggesting that low HDL-C level was independently associated with the development of MetS. In the present study, a significant correlation was observed between TT to E2 ratio and WC which confirmed the findings of another study in America, indicating a relationship between obesity and TT and E2 hormone level ( 12 , 24 ).
In the present study, the cutoff value of TT to E2 ratio (8.4) had acceptable validity ( sensitivity of 80.9%, specificity of 70.5%, PPV of 79.7%, NPV of 71.2%, and accuracy of 78.9%) for predicting MetS. These findings were in line with the results of the studies conducted by Miranda et al. ( 25 ) in Brazil and Ahmed et al. ( 26 ) in Egypt, suggesting that TT and E2 levels play a significant role in predicting MetS in males. Although the application of sex hormones levels for screening MetS in males is relatively costly, compared to non-invasive screening measures, such as waist to height ratio, it is highly accurate in diagnosing MetS ( 27 ).
Regarding the limitations of the present study, one can refer to the recruitment of men from a tertiary referral center which might have not been the exact representation of the general population. TT was measured by electrochemiluminescence rather than liquid chromatography, using the tandem mass spectrometry method.
The results revealed that TT to E2 ratio was a significant predictor of MetS in males and that there was a strong relationship between this ratio and MetS parameters, especially in terms of WC. The weight, WC, BP, and FBG levels were higher in patients with MetS, compared to healthy individuals. The abnormal lipid profile of high TG and low HDL -C levels were obvious in patients with MetS. This study can be a pioneer for future studies in the prediction of MetS and indication of its impact on human health.
5. Conclusion
Regarding the obtained results, it is recommended that health policies should enforce MetS screening strategies in primary health care centers, and physicians should be encouraged to perform MetS screening in males, considering TT to E2 ratio. Eventually, further national multi-center studies should be conducted on the role of sex hormones in males in MetS screening.
Authors' Contribution
Study concept and design: M. A. H.
Acquisition of data: M. A. H.
Analysis and interpretation of data: A. A.
Drafting of the manuscript: A. A. M.
Critical revision of the manuscript for important intellectual content: A. A.
Statistical analysis: A. A. M.
Administrative, technical, and material support: A. A.
Ethics
The study protocol was approved by the Ethics Committee at College of Medicine, University of Basrah, Basrah, Iraq. Oral informed consent was taken from patients enrolled in the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- 1.Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9(1):1–13. doi: 10.1186/1741-7015-9-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Parikh RM, Mohan V. Changing definitions of metabolic syndrome. Indian J Endocrinol Metab. 2012;16(1):7. doi: 10.4103/2230-8210.91175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sliem HA, Ahmed S, Nemr N, El-Sherif I. Metabolic syndrome in the Middle East. Indian J Endocrinol Metab. 2012;16(1):67. doi: 10.4103/2230-8210.91193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Azzawi OF. Metabolic syndrome; comparing the results of three definition criteria in an Iraqi sample. AL-Kindy College Medical Journal. 2018;14(2):7–12. [Google Scholar]
- 5.Saleh AA, Hayawi AH, Al-Samarrai AY, Lafta RK. Metabolic syndrome among obese adults in Baghdad, Iraq. Saudi J Obesity. 2017;5(1):8. [Google Scholar]
- 6.Maggio M, Ceda GP, Lauretani F, Bandinelli S, Metter EJ, Artoni A, et al. Estradiol and inflammatory markers in older men. J Clin Endocrinol Metab. 2009;94(2):518–22. doi: 10.1210/jc.2008-0940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Goodpaster BH, Krishnaswami S, Harris TB, Katsiaras A, Kritchevsky SB, Simonsick EM, et al. Obesity, regional body fat distribution, and the metabolic syndrome in older men and women. Arch Intern Med. 2005;165(7):777–83. doi: 10.1001/archinte.165.7.777. [DOI] [PubMed] [Google Scholar]
- 8.Kupelian V, Page ST, Araujo AB, Travison TG, Bremner WJ, McKinlay JB. Low sex hormone-binding globulin, total testosterone, and symptomatic androgen deficiency are associated with development of the metabolic syndrome in nonobese men. J Clin Endocrinol Metab. 2006;91(3):843–50. doi: 10.1210/jc.2005-1326. [DOI] [PubMed] [Google Scholar]
- 9.Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 2009;120(16):1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644. [DOI] [PubMed] [Google Scholar]
- 10.Bekaert M, Van Nieuwenhove Y, Calders P, Cuvelier CA, Batens A-H, Kaufman J-M, et al. Determinants of testosterone levels in human male obesity. Endocrine. 2015;50(1):202–11. doi: 10.1007/s12020-015-0563-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hevener AL, Clegg DJ, Mauvais-Jarvis F. Impaired estrogen receptor action in the pathogenesis of the metabolic syndrome. Mol Cell Endocrinol. 2015;418:306–21. doi: 10.1016/j.mce.2015.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Alajeely MHJ, Abdulkareem DT, Ghazzay HI, Jasim E. Association between serum testosterone-estradiol ratio and body mass index in obese iraqi men. Ann Trop Med Public Health. 2020;23:23–1028. [Google Scholar]
- 13.Kusuma. Kusuma R, Siregar Y, editors. Estradiol to testosterone ratio in metabolic syndrome men aged started 40 years above. IOP Conference Series: Earth and Environmental Science; 2018: IOP Publishing [Google Scholar]
- 14.Antonio L, Wu FC, O'Neill TW, Pye SR, Carter EL, Finn JD, et al. Associations between sex steroids and the development of metabolic syndrome: a longitudinal study in European men. J Clin Endocrinol Metab. 2015;100(4):1396–404. doi: 10.1210/jc.2014-4184. [DOI] [PubMed] [Google Scholar]
- 15.Bhasin S, Jasjua GK, Pencina M, D’Agostino R, Coviello AD, Vasan RS, et al. Sex hormone–binding globulin, but not testosterone, is associated prospectively and independently with incident metabolic syndrome in men: the Framingham heart study. Diabetes care. 2011;34(11):2464–70. doi: 10.2337/dc11-0888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Haring R, Völzke H, Spielhagen C, Nauck M, Wallaschofski H. The role of sex hormone-binding globulin and testosterone in the risk of incident metabolic syndrome. Eur J Prev Cardiol. 2013;20(6):1061–8. doi: 10.1177/2047487312452965. [DOI] [PubMed] [Google Scholar]
- 17.Li C, Ford ES, Li B, Giles WH, Liu S. Association of testosterone and sex hormone–binding globulin with metabolic syndrome and insulin resistance in men. Diabetes care. 2010;33(7):1618–24. doi: 10.2337/dc09-1788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Muraleedharan V, Jones TH. Testosterone and the metabolic syndrome. Therapeutic Advances in Endocrinology and Metabolism. 2010;1(5):207–23. doi: 10.1177/2042018810390258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ross R, Neeland IJ, Yamashita S, Shai I, Seidell J, Magni P, et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol. 2020;16(3):177–89. doi: 10.1038/s41574-019-0310-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kurotani K, Miyamoto T, Kochi T, Eguchi M, Imai T, Nishihara A, et al. Metabolic syndrome components and diabetes incidence according to the presence or absence of impaired fasting glucose: The Japan Epidemiology Collaboration on Occupational Health Study. J Epidemiol. 2017;27(9):408–12. doi: 10.1016/j.je.2016.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zidek W, Naditch-Brûlé L, Perlini S, Farsang C, Kjeldsen SE. Blood pressure control and components of the metabolic syndrome: the GOOD survey. Cardiovasc Diabetol. 2009;8(1):1–9. doi: 10.1186/1475-2840-8-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tao L-X, Yang K, Liu X-T, Cao K, Zhu H-P, Luo Y-X, et al. Longitudinal associations between triglycerides and metabolic syndrome components in a Beijing adult population, 2007-2012. Int J Med Sci. 2016;13(6):445. doi: 10.7150/ijms.14256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mani P, Ren H-Y, Neeland IJ, McGuire DK, Ayers CR, Khera A, et al. The association between HDL particle concentration and incident metabolic syndrome in the multi-ethnic Dallas Heart Study. Diabetes Metab Syndr. 2017;11(1):S175–S9. doi: 10.1016/j.dsx.2016.12.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rohrmann S, Shiels MS, Lopez DS, Rifai N, Nelson WG, Kanarek N, et al. Body fatness and sex steroid hormone concentrations in US men: results from NHANES III. Cancer Causes & Control. 2011;22(8):1141–51. doi: 10.1007/s10552-011-9790-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Miranda EP, Oliveira C, Carvalho E, Rabelo A, Xavier A, Tiraboschi R, et al. MP91-08 Combination Of Metabolic Syndrome Components To Predict Testosterone Deficiency In Men. Urol J. 2017;197(4S): 1221. [Google Scholar]
- 26.Ahmed IZ, Mahdy MM, El Oraby H, Abdelazeem EM. Association of sex hormones with metabolic syndrome among Egyptian males. Diabetes Metab Syndr. 2017;11:S1059–S64. doi: 10.1016/j.dsx.2017.07.042. [DOI] [PubMed] [Google Scholar]
- 27.Liu PJ, Lou HP, Zhu YN. Screening for metabolic syndrome using an integrated continuous index consisting of waist circumference and triglyceride: A preliminary cross-sectional study. Diabetes Metab Syndr Obes. 2020;13:2899. doi: 10.2147/DMSO.S259770. [DOI] [PMC free article] [PubMed] [Google Scholar]