

Abstract
Families play an important role in the lives of people with intellectual disability as they do for everyone. However, little research has addressed the views of people with intellectual disability about their families by using self‐report. Individual family members may hold different views about their family relationships. Therefore, we used a social capital theoretical perspective to examine (a) how perceptions of people with mild intellectual disability (MID) about their family support networks compare to those of their family members and (b) what factors are associated with any diverging perceptions. Randomly selected participants with MID (n = 111) and their family members (n = 111) were interviewed individually at their homes using the Family Network Method—Intellectual Disability (FNM‐ID). The FNM‐ID examines how people define their family groups and how they perceive existing supportive relationships within this group. The findings showed that participants with MID perceived that they had somewhat denser family networks (i.e., bonding social capital) than family members perceived them to have and were more likely to report bridging social capital. They reported more relationships that involved them providing support to family members. This difference in estimation was greater when the participant with MID displayed higher levels of externalizing behaviour problems. They also perceived more reciprocity in their relationships with family. No differences were found in the estimated numbers of significant family members and relationships in which support was received. It is concluded that people with MID and their family members have different perceptions on several aspects of the family support network. Family professionals and services should seek the views of people with intellectual disability and their family members when carrying out assessments or organizing supports.
Keywords: emotional support, family relationships, perceptions, reciprocity, social capital, social networks
What is known about this topic?
People with MID have become more reliant on their families for their support.
Previous family research has tended to focus on the perceptions of family members of people with MID.
Perceptions about the family are often not shared by individual family members.
What this paper adds?
Participants with MID and their family members held similar views about supportive resources available to the person with intellectual disability
They differed in their views about the support that was contributed by the person with MID.
This difference was greater when the person with MID displayed higher levels of externalising behaviour.
1. INTRODUCTION
The informal supportive networks of people with mild intellectual disability (MID) have become increasingly important in a time of austerity and cuts to services. However, the levels of informal support provided to people with MID are often low (Sanderson et al., 2019). Their informal support networks are found to mainly consist of family members (Van Asselt‐Goverts et al., 2013), with parents as the main provider of practical (Sanderson et al., 2017) and emotional support (Giesbers et al., 2020a). Accordingly, due to cuts to services, people with MID have become more reliant on their families for their support (e.g., Malli et al., 2018), and families may play an important role in facilitating the social participation and inclusion of people with MID (Simplican et al., 2015). As such, the research literature requires a theoretical foundation and associated method to build knowledge on the supportive resources within families of people with MID.
Several studies have shown that social capital is a useful theoretical framework to examine support in the family relationships of people with MID (Giesbers et al., 2019; Kramer et al., 2013; Widmer et al., 2013). Broadly defined, social capital is about human relationships and networks (Bourdieu, 1986). There has been much debate on what constitutes social capital and how it should be measured (Tzanakis, 2013), though there seems to be a growing consensus that “social capital stands for the ability of actors to secure benefits by virtue of membership in social networks or other social structures” (Portes, 1998, p. 6). Social capital centres on the mutual exchange of supports or resources (i.e., reciprocal supportive relationships) between network members (Bullen & Onyx, 1999). The social capital available to individuals has been frequently linked to factors such as the individual's sex (e.g., Van Emmerik, 2006), subjective well‐being (e.g., Umberson & Montez, 2010), and internalizing and externalising behaviour problems (e.g., McPherson et al., 2014).
As families are social structures in which supportive relationships are typically provided, they are considered a significant source of social capital (Furstenberg & Kaplan, 2004). The two main types of social capital are relevant with respect to family networks: bonding and bridging social capital. Bonding social capital refers to a family with a high density of relationships in which all or most family members are interconnected (Coleman, 1988). As dense networks enhance expectations, obligations, and trust among members, support within such a network becomes collective. Bridging social capital refers to weaker connections between subgroups of a network that give some members (i.e., brokers) the potential to mediate the flow of resources between family members (Burt, 1995). A “broker” role may lead to feelings of autonomy, competence, and control (Burt, 1995).
To characterize individuals' perceptions of their social capital, Krackhardt (1987) conceptualized social networks as cognitive structures, based on the assumption that “perceptions are real in their consequences, even if they do not map one‐to‐one onto observed behaviors” (p. 128). By defining social networks as cognitive structures, the focus is not on the actual configuration of relationships surrounding individuals, but on the pattern of relationships as perceived by the different individuals. It is assumed that family network data from a single informant may be the idiosyncratic view of that individual family member, rather than a consensual reflection from multiple family members (Bartle‐Haring et al., 1999). As such, Krackhardt's (1987) conceptualization stresses the importance of gaining insight into the individual's perception of their family relationships, and underlines the importance of including the perceptions of people with intellectual disability themselves.
When examining the family‐based social capital of people with MID from their own perspective, people with MID reported fewer family relationships with given and received support than people without disability (Widmer et al., 2008). Their family support networks were also less dense (i.e., bonding social capital), and they had a less central position in their network (i.e., bridging social capital). These findings imply that their family‐based social capital is lower on average, and this finding was even stronger for those who also have psychiatric problems (Widmer et al., 2008). However, people with MID may experience different types of family networks with different levels of social capital. For one, their family support networks may be dependent on living situations (Kozma et al., 2009; Widmer et al., 2013). For example, people with MID who lived in community settings had a larger share of professionals and friends in their family network than those who lived with their parents (Widmer et al., 2013).
Thus, previous research has included the perceptions of people with MID about their family support experiences. Even though family data derived from people with MID themselves is of great value, as stated, a perspective from a single informant within the family may be the view only of that individual family member. Several studies have shown that perceptions about the family are often not shared, and that family members experience the same events in different ways (Henggeler et al., 1987; Jager et al., 2012, 2014; Van Heel et al., 2019). For example, Henggeler et al. (1987) assessed intrafamilial agreement concerning three dimensions (i.e., affect, conflict, dominance) of family relations and found that individual family members' reports showed low‐moderate agreement. Moreover, Jager et al. (2012) demonstrated that each family member's unique perspective on family dysfunction was associated with his or her own adjustment.
These findings underline Barnes and Olson's (1985) idea that it may be advantageous to examine the extent that informants differ in their views of family relations, as the description of these differences may advance our understanding about the nature of family functioning. Therefore, it is of interest to explore differences in the perceptions of people with MID and their family members about their family relationships and social capital, to examine the extent of (dis)agreement between family members and the extent to which they share a reality. Widmer et al. (2010) found that, compared with a non‐clinical sample, 17 people with MID and psychiatric disorders perceived less support within their families. Their family members held the same view about a lack of family support. However, there were also differences in the perceptions of people with MID and their family members; family members perceived the family network to be smaller and denser than people with MID perceived.
Widmer et al.'s study (2010) focused on a relatively small, purposive sample of people with MID and psychiatric disorders residing in a psychiatric unit of a hospital. Our study adds to this previous work by recruiting a much larger and randomly selected sample of 111 people with MID (and a family member) with, but also without, comorbid psychopathology, who received support of mainstream intellectual disability services. All participants with MID lived apart from their birth family. Moreover, our study explored factors associated with any divergence in perceptions of the person with MID and their family member.
Specifically, the first aim of the study was to examine support in the family networks of a randomly selected sample of people with MID, by assessing both their own perceptions, and the perceptions of their family members about the network of the person with MID, and comparing both perceptions on key social capital measures. Second, this study aimed to explore factors associated with any divergence in perceptions of the person with MID and their family member to obtain a broader understanding of the nature of converging versus diverging perceptions. Potential correlates of divergence in perceptions were factors commonly associated with social capital in general: sex (e.g., Van Emmerik, 2006), subjective well‐being (e.g., Umberson & Montez, 2010), and internalizing and externalising behaviour problems (e.g., McPherson et al., 2014), and the social capital of people with intellectual disability in particular: type of support/living setting (Kozma et al., 2009), and the number of years living apart from family with the support of a service provider (Widmer et al., 2013).
2. METHOD
2.1. Participants
Participants were people with MID (IQ 50–70; n = 111) and their family members (n = 111). Inclusion criteria for people with MID were (a) MID (IQ 50–70) initially according to file records (later confirmed), (b) aged 18–40 years, and (c) receiving professional support at least once a week for a minimum of 6 months. The limit for inclusion was set at 40 years old, since parents of older individuals are likely to be elderly and less able to provide support (Grey et al., 2015). Living with their birth family was an exclusion criterion for participants, as family support is found to be associated with living situation (Widmer et al., 2013). Family members were selected by the participants with MID based on the criterion that they felt this family member could best be questioned about their family support experiences. Key support workers (who had supported the individual for at least 6 months) were included in the study as proxy informants on the emotional and behavioural problems of the participants with MID. Demographic characteristics of the three participants groups are described in Table 1 (participants with MID) and Table 2 (family members and key support workers).
TABLE 1.
Demographics of participants with MID (N = 111)
| Variable | n (%) | M (SD) |
|---|---|---|
| Gender | ||
| Male | 62 (55.9) | |
| Female | 49 (44.1) | |
| Age in years | 28.4 (6.08) | |
| Cultural background | ||
| Dutch | 105 (94.6) | |
| Other | 6 (5.4) | |
| Living setting | ||
| Community‐based setting | 94 (84.7) | |
| Facility | 17 (15.3) | |
| Living situation | ||
| Together with other service users | 69 (62.2) | |
| Individually | 35 (31.5) | |
| Together with a partner | 4 (3.6) | |
| Other | 3 (2.7) | |
| Additional diagnoses | ||
| Yes | 50 (45.5) | |
| No | 60 (54.5) | |
| Unknown | 1 (0.9) | |
| Additional diagnoses specified | ||
| Autism | 26 (23.4) | |
| Disorder of impulse‐ or aggression regulation | 9 (8.1) | |
| Genetic syndrome | 7 (6.3) | |
| Personality disorder | 6 (5.4) | |
| Attention deficit hyperactivity disorder | 5 (4.5) | |
| Attachment disorder | 4 (3.6) | |
| Post‐traumatic stress disorder | 2 (1.8) | |
| Other | 5 (4.5) | |
| Physical impairment | ||
| Yes | 28 (25.2) | |
| No | 83 (74.8) | |
| Sensory impairment | ||
| Yes | 15 (13.5) | |
| No | 96 (86.5) | |
| Years of living apart from family | 10.6 (6.19) | |
TABLE 2.
Demographics of family members (N = 111) and key support workers (N = 111)
| Variable | Category | Family members | Key support workers | ||
|---|---|---|---|---|---|
| n (%) | M (SD) | n (%) | M (SD) | ||
| Gender | Male | 37 (33.3) | 21 (18.9) | ||
| Female | 74 (66.7) | 90 (81.1) | |||
| Age in years | 55.7 (11.65) | 41.2 (10.66) | |||
| Cultural background | Dutch | 104 (93.7) | |||
| Other | 7 (6.3) | ||||
| Relation to the participant with MID | Mother | 55 (49.5) | |||
| Father | 25 (22.5) | ||||
| Sibling | 15 (13.5) | ||||
| Extended family | 5 (4.5) | ||||
| Foster parents | 5 (4.5) | ||||
| Step parents | 3 (2.7) | ||||
| Friends | 2 (1.8) | ||||
| Partner | 1 (0.9) | ||||
| Years of working in the field of intellectual disability | 18.2 (10.43) | ||||
| Educated in the field of social work/health care | Yes | 104 (93.7) | |||
| No | 6 (5.4) | ||||
| Unknown | 1 (0.9) | ||||
| Level of education in social work/health care | Intermediate vocational training | 67 (60.4%) | |||
| Higher education | 37 (33.3%) | ||||
2.2. Measures
2.2.1. Family networks
Participants with MID and family members were interviewed individually using the Family Network Method—Intellectual Disability (FNM‐ID; Giesbers et al., 2019). The FNM‐ID is designed to map the family network and to identify significant family members, as well as family members who provide emotional support. Consistent with the FNM‐ID procedure described in Giesbers et al. (2019), participants with MID were asked about their perception of their family support network. Family members were interviewed about their perception of their relative's support network.
The FNM‐ID has four main steps. First, participants are instructed to map the family network. The term ‘family’ is not defined by the researcher; participants are told to use their own definition of ‘family’ and define who they consider to be their (or their relative's) family. Second, participants are invited to define significant family members (according to their own definition) from those listed in the first step. The third step concerns questions about emotional support provision. Participants not only estimate their own relationships with their family members by asking them “If you are feeling ‘out of sorts’, who is there for you?” (or in case of family members: The relationships between their relative and their family members), but also the relationships existing among all family members (e.g., “When grandpa is feeling ‘out of sorts’, who is there for him?”). Key demographic characteristics of all the listed family members (e.g., gender, age, place of residence) are also collected.
2.2.2. Subjective well‐being
A Dutch version of the Personal Wellbeing Index‐Intellectual Disability (PWI‐ID; Cummins & Lau, 2005) was used with the participants with MID. The PWI‐ID contains seven satisfaction items rated on a five‐point Likert scale, each corresponding to a quality of life domain (i.e., satisfaction with standard of living, health, achieving in life, relationships, safety, community‐connectedness, and future security), and one question about “satisfaction with life as a whole”. McGillivray et al. (2009) reported a Cronbach's alpha of 0.76 and the domains form a single stable factor that predicts over 50% of the variance in “satisfaction with life as a whole”. Within the current study, the sum score of the seven quality of life domains was used.
2.2.3. Cognitive ability
Two subtests (i.e., vocabulary and matrix reasoning) of the Dutch Wechsler Adult Intelligence Scale (WAIS‐IV‐NL; Wechsler, 2012) were administered to participants with MID only. These two WAIS‐IV‐NL subtests correspond with the two‐subtest form of the Wechsler Abbreviated Scale of Intelligence (WASI‐II; Wechsler, 2011). As no Dutch WASI‐II is available, an estimation of IQ scores was made based on the subtest standard scores of the two corresponding WAIS‐IV subtests. When both WAIS‐IV‐NL standard scores were indicative of a level of cognitive ability above or below the MID range (taking the standard error into account), a participant was considered to not have MID.
2.2.4. Behavioural and emotional problems
The Dutch Adult Behaviour Check List (ABCL; Achenbach & Rescorla, 2003) was completed by the key support workers. The ABCL consists of 118 items (using a 3‐point scale) and examines a broad range of behavioural and emotional problems. We used the scales concerning internalizing behaviour (i.e., anxious/depressive problems, somatic complaints, and withdrawn behaviour) and externalizing behaviour (aggressive behaviour, rule‐breaking behaviour, and intrusive behaviour). Psychometric data suggest that this instrument can be used with people with MID (Cronbach's alpha ranged from 0.69 to 0.95 (M = 0.84), interrater reliability ranged from 0.57 to 0.76 (mean ICC = 0.68; Tenneij & Koot, 2007).
2.3. Procedure
Ethical approval was obtained from the Ethical Review Board of Tilburg University. Participants with MID were recruited from five intellectual disability services in the Netherlands. To increase the representativeness of the sample, participants who met inclusion criteria were randomly selected from each service provider using a stratified sampling procedure (i.e., stratified by service provider). Service providers were asked to determine the total number of their service users who met the inclusion criteria of the study. From each service provider, 10% of their service users who met inclusion criteria participated in the study to reach the target number of about 150 participants (see Figure 1 for an overview of the sampling procedure).
FIGURE 1.
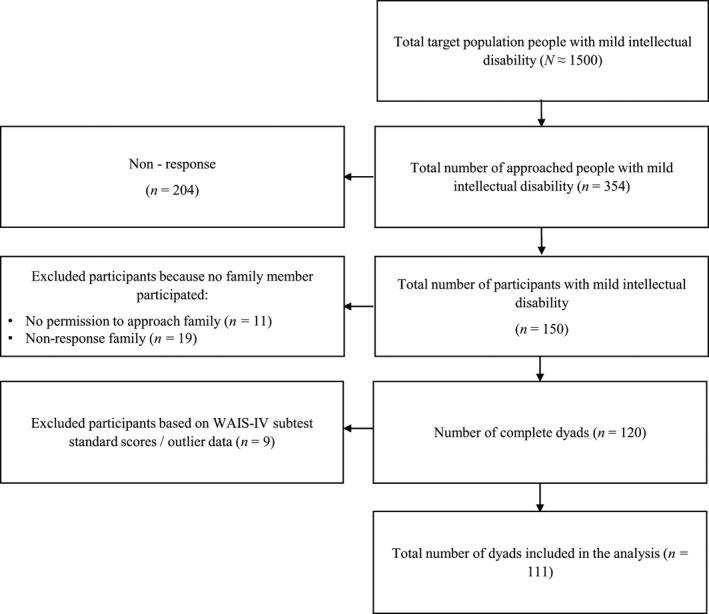
Overview of the sampling procedure
Participants with MID were always approached in consultation with their key worker. The researcher contacted the key workers by telephone and sent an information letter to the key workers to discuss with the potential participants. In total 150 participants with MID participated.
For the service users who were willing to participate in the study, an appointment was made at their home or another location they preferred. Participants with MID were visited individually by a researcher (the first or fifth author, or a research assistant) for 45–60 min per visit. In a few cases (6.7%), not all measures could be completed during one visit (participants showed signs of distractibility or fatigue, or asked to complete the measures at another time), and a second visit was needed. To ensure that participants with MID were able to give their informed consent, a standard consent procedure was followed (Arscott et al., 1998).
After consent was obtained, the WAIS‐IV‐NL subtests were administered. Second, demographic information was gathered using a computer administered set of questions (after the visits, with the consent of participants, the researcher contacted the psychologist or key worker for each participant with MID to ask for possible additional, official diagnoses). Third, the PWI‐ID was computer‐administered to participants, using the same procedure. The main task was completed last and involved interviewing the participants about their family network using the FNM‐ID, following the prescribed interview protocol (Giesbers et al., 2019), and all FNM‐ID interviews were audio recorded. At the end of the FNM‐ID interview, participants were asked to select one of their family members, and were asked permission to approach that family member to participate in the study. Eleven participants did not give their permission to invite a family member for participation.
An information letter was sent to the selected family members and the researchers contacted them by telephone to explain the study. If a family member was willing to participate, an appointment was scheduled at their home or on the service provider's premises. Of the 150 family members that could potentially participate in the study, 139 were invited to participate, and 120 participated (80.0%). Reasons for non‐response included protracted illness of a family member, the expected burden of participation was perceived as too high, or family members had no interest in the study. Family members were visited individually 45–60 min. After informed consent was obtained, family members were questioned about their perceptions of their relative's network. Key demographic information about the family member was also collected.
For each participant with MID, the key support worker was invited by the research team (with the consent of the participant with MID) to complete the ABCL as a proxy informant. Proxy‐report instead of self‐report was used to reduce the demand placed on participants with MID. After informed consent was given, the ABCL was computer‐administrated.
The current analysis only included data from dyads of participants with MID and their family members. Data from an additional nine participants were excluded from the study because both WAIS‐IV‐NL standard scores were indicative of a level of cognitive ability above or below the MID range. In addition, data from the FNM‐ID for one participant were excluded from the study; scores on all but one measures were found to be extreme outliers (3 SDs or more above the mean). Therefore, 111 complete dyads of people with MID and family members were included in the current analysis (see Figure 1).
2.4. Data analysis
2.4.1. (Group differences in) social network measures
Family network data were analysed using UCINET (Version 6.623; Borgatti et al., 2002). First, several social network measures, of interest from a social capital theoretical perspective, were computed (see Table 3). In a second step, Paired samples t‐tests were conducted to examine differences in the characteristics of the family networks perceived by the participants with MID and their family members. A standardized mean difference effect size for paired designs, d was calculated using t[2(1 − r)/n]1/2 (Dunlap et al., 1996). A conservative 0.80 was used to estimate r. For the interpretation of the effect size, d = 0.2 was considered a small effect size, d = 0.5 represents a medium effect size, and d = 0.8 a large effect size (Cohen, 1988).
TABLE 3.
Overview of the computed social network measures
| Network measures—full network | Size | Number of listed family members |
|---|---|---|
| Network measures—significant network | Size | Number of significant family members |
| Density | The number of relationships between network members compared to the maximum possible numbers of relationships that could theoretically exist between all family members. In highly dense connected family networks, most or all family members are connected with each other, providing a bonding type of social capital. | |
| Dyad reciprocity—all relationships | The number of dyads in the network with reciprocal relationships, divided by the total number of adjacent dyads in the network | |
| Individual family network measures for people with MID | In‐degree | Number of relationships in which the person with MID receives support |
| Out‐degree | Number of relationships in which the person with MID provides support | |
| Betweenness centrality | Quantifies the number of times the person with MID acts as a bridge along the shortest path between two other network members. That is, the number of pairs of family members an individual would have to go through to reach another (in the minimum number of steps), thereby describing the intermediary position of a person in the family network. Family members with a high betweenness centrality mediate the flow of support among network members, providing a bridging type of social capital. | |
| Dyad reciprocity—relationships of participant only | Number of dyads (in which the person with MID is an actor) with reciprocal relationships, divided by the total number of adjacent dyads (in which the person with MID is an actor) |
2.4.2. Associating factors with diverging perceptions
As this study focused on factors that may account for divergence in perceptions of people with MID and their family on key social capital measures, dyad difference scores were calculated for the measures that revealed significant differences at the second step (i.e., network density, dyad reciprocity, and out‐degree). That is, for each dyad, scores as estimated by the family member were subtracted from scores as estimated by the participant with MID. Individual scores within a dyad are nested data involving two levels (individual–dyad; Gonzalez & Griffin, 2012). However, when using difference scores only the dyadic level is included in the analysis.
2.4.3. Multiple regression analyses
Next, factors that may account for different perceptions between people with MID and their family on divergent network measures were examined using multiple regression analyses with the dyad's difference score on that network measure as the dependent variable. By using a residual change approach (Castro‐Schilo & Grimm, 2018), it is not assumed that all dyads have the same mean. Therefore, the mean score of the dyad on the dependent variable was included as a covariate, to correct for different dyad mean scores. The other covariates for each regression model were: the sex of the participant with MID, the number of years the participant with MID had lived apart from family, the subjective well‐being of the participant with MID, whether the participant with MID resided in a residential versus community living setting, and the level of internalizing and externalizing behavioural and emotional problems.
2.4.4. McNemar's test for paired data
During the initial inspection of the computed social network measures, two cases with extreme difference scores (3 SDs or more above or below the mean)—one on the size of the significant network and one case with extreme difference scores on out‐degree—were excluded from the analyses. In addition, scores on the individual network measure “betweenness centrality” were found to strongly deviate from a normal distribution, as difference scores were centred around zero (Skewness: 6.86, Kurtosis: 53.54). This finding was related to the fact that 70 (63.1%) participants with MID and 93 (83.8%) family members estimated a betweenness centrality score of zero, resulting in high levels of agreement (difference score of zero). Therefore, the estimates of “betweenness centrality” were dichotomized into zero—not zero, and a McNemar's test for paired data was performed to test differences in the estimation of a zero—nonzero “betweenness centrality” between groups. In a second step, dyad difference scores on “betweenness centrality” were dichotomized into agreement—nonagreement, and factors that may account for (non‐) agreement were tested in a logistic regression analysis.
3. RESULTS
3.1. Group differences in network perception
3.1.1. Network measures
For network measures (concerning the network as a whole), participants with MID perceived their significant family networks to be more dense than did family members, t(110) = 2.12, p = 0.037, with a small effect size (see Table 4). The difference in the estimation of dyad reciprocity was not statistically significant, t(110) = 1.81, p = 0.073.
TABLE 4.
Mean numbers of the network measures for participants, t, df, p, d
| Variable | Mean (SD) | t | df | p | d | ||
|---|---|---|---|---|---|---|---|
| Individuals with MID | Family members | ||||||
| Full network | Size | 11.40 (6.61) | 12.36 (7.63) | −1.34 | 110 | 0.184 | −0.080 |
| Significant network | Size | 7.14 (4.52) | 7.10 (3.86) | 0.08 | 108 | 0.935 | 0.005 |
| Density | 0.36 (0.24) | 0.30 (0.20) | 2.12 | 110 | 0.037 | 0.127 | |
| Dyad reciprocity—all relationships | 0.38 (0.30) | 0.31 (0.25) | 1.81 | 110 | 0.073 | 0.109 | |
| Measures for individuals with MID | In‐degree | 2.37 (1.58) | 2.23 (1.45) | 0.72 | 110 | 0.471 | 0.043 |
| Out‐degree | 2.14 (2.74) | 0.85 (1.72) | 4.41 | 109 | <0.001 | 0.266 | |
| Dyad reciprocity—relationships of participant only | 0.28 (0.33) | 0.15 (0.28) | 3.10 | 110 | 0.002 | 0.186 | |
3.1.2. Individual network measures
Participants with MID perceived that they had more relationships with network members in which they gave support (i.e., out‐degree), than family members perceived, t(109) = 4.41, p < 0.001, with a small effect. Also, they experienced their relationships with network members as more reciprocal than did family members, t(110) = 3.10, p = 0.002, also with a small effect size. Finally, McNemar's test (not in Table 4) showed that participants with MID were significantly more likely (OR 1.10) to report a “Betweenness centrality” that was nonzero, p = 0.001.
3.2. Correlates of divergence
Multiple regression models for network density, F(7,103) = 1.67, p = 0.126, R 2 = 0.10, and dyadic reciprocity F(7,103) = 1.69, p = 0.120, R 2 = 0.10 were not statistically significant overall and none of the individual covariates were significant independent covariates (Table 5). For out‐degree the overall model was significant, F(7,102) = 5.95, p < 0.001, R 2 = 0.29. Externalizing behaviour problems and the dyad's mean score on out‐degree independently added to the prediction. A higher score on externalizing behaviour and a higher mean score of the dyad on out‐degree predicted larger differences in out‐degree estimations.
TABLE 5.
Summary of multiple regression analyses for variables predicting dyad's difference scores
| Variable | Density (n = 111) | Out‐degree (n = 110) | Dyad reciprocity (n = 111) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B (SE) | t | p | B (SE) | t | p | B (SE) | t | p | |
| Sex | 0.073 (0.060) | 1.22 | 0.227 | 0.648 (0.542) | 1.20 | 0.234 | 0.065 (0.088) | 0.74 | 0.459 |
| Years of living apart from family | 0.004 (0.005) | 0.76 | 0.447 | 0.025 (0.043) | 0.59 | 0.558 | 0.011 (0.007) | 1.66 | 0.101 |
| Well‐being | 0.015 (0.009) | 1.78 | 0.079 | 0.025 (0.076) | 0.33 | 0.743 | 0.007 (0.013) | 0.55 | 0.581 |
| Living setting | −0.135 (0.081) | −1.66 | 0.100 | 0.382 (0.733) | 0.52 | 0.604 | 0.005 (0.118) | 0.04 | 0.970 |
| Internalising behaviour | −0.001 (0.004) | −0.19 | 0.850 | −0.025 (0.035) | −0.73 | 0.466 | 0.004 (0.006) | 0.66 | 0.508 |
| Externalising behaviour | 0.003 (0.003) | 1.10 | 0.276 | 0.080 (0.028) | 2.90 | 0.005 | 0.005 (0.004) | 1.07 | 0.287 |
| Dyadic mean score | 0.281 (0.182) | 1.55 | 0.125 | 0.783 (0.158) | 4.95 | <0.001 | 0.293 (0.200) | 1.47 | 0.145 |
Constant = −0.57 (density), −2.30 (out‐degree), −0.44 (dyad reciprocity).
The logistic regression model for betweenness centrality was not statistically significant, χ 2 (6) = 11.70, p = 0.069 (Table 6). The model explained 13.4% (Nagelkerke R 2) of the variance in agreement on betweenness centrality. While the model was not statistically significant overall, women with MID were 3.01 times more likely than men with MID to disagree with family members about whether betweenness centrality is zero or nonzero (p = 0.013).
TABLE 6.
Summary of logistic regression analysis for variables predicting dyad's (non‐)agreement on betweenness centrality of the participant with mild intellectual disability (n = 111)
| Variable | B (SE) | Wald χ 2 | p | OR | 95% CI OR |
|---|---|---|---|---|---|
| Sex | 1.102 (0.444) | 6.17 | 0.013 | 3.01 | [1.26–7.18] |
| Years of living apart from family | −0.036 (0.034) | 1.10 | 0.294 | 0.97 | [0.90–1.03] |
| Well‐being | 0.119 (0.065) | 3.35 | 0.067 | 1.13 | [0.99–1.28] |
| Living setting | 0.103 (0.584) | 0.03 | 0.860 | 1.11 | [0.35–3.48] |
| Internalising behaviour | −0.029 (0.027) | 1.16 | 0.282 | 0.97 | [0.92–1.02] |
| Externalising behaviour | 0.036 (0.022) | 2.63 | 0.105 | 1.04 | [0.99–1.08] |
Constant = −3.82.
4. DISCUSSION
Within this study, a social capital theoretical perspective was used to examine (1) how perceptions of people with MID about their family support networks compare to those of their family members, and (2) what factors are associated with any diverging perceptions. The findings showed that participants with MID and their family members have different perceptions on several aspects of the family support network (i.e., bonding and bridging social capital, support provided by the person with MID, and the reciprocity of the family relationships of the person with MID). No differences in perceptions were found in the estimated numbers of significant family members and relationships in which support was received by the person with MID.
First, contrary to the findings of Widmer et al. (2010), participants with MID in this study perceived their family network to be denser compared to their family members. Participants with MID perceived more relationships among their network members, meaning that they experienced a somewhat higher level of bonding social capital. Bonding social capital is often advantageous (Coleman, 1988), as it provides the norms and trust that facilitates collaborative action, and can fulfill a valuable social function by providing a source of collective support. However, it has also been suggested that bonding social capital can be a source of strain, and a barrier to experiencing individual autonomy, potentially leading to conflicts (Ferlander, 2007).
Participants with MID were also more likely to estimate a betweenness centrality different to zero when compared to their family members. People with MID were thus more likely to report experiences of bridging social capital. Bridging social capital may enhance feelings of competence, control, and autonomy of people with MID within their families (Woolcock, 1998). However, participants with MID and family members most frequently reported no bridging social capital at all (63.1% and 83.8% respectively).
Furthermore, compared to family members, participants with MID reported more relationships that involved them supporting the family member. They were also more likely to report reciprocal relationships with family members. Reciprocity is an essential aspect of social capital (Bullen & Onyx, 1999). Being able to support others may enhance the individual's self‐worth and self‐esteem (e.g., Liang et al., 2001). People with intellectual disability in previous research stressed that reciprocal relationships are of great importance to make them feel useful, and to challenge feelings of dependence (Milner & Kelly, 2009). However, research has shown that people with MID report that only about one third of their relationships are based on reciprocity (Giesbers et al., 2020a), and that they estimate their family relationships to be less often reciprocal compared to the estimations of people without intellectual disability of the same sex and age (Giesbers et al., 2020b). The current findings add to these previous studies by showing that family members did not always share the participants with MID's view of reciprocity within family relationships; family members reported even lower levels of reciprocal family relationships than did the participants with MID themselves, suggesting that family members do not always recognize the participants with MID's sense of reciprocity.
It is important for people with MID to be able to support their family members, but it may also be of great value for family members to receive support from their relative with MID. That is, several studies have shown the positive effects of reciprocity on caregiver well‐being as well (Heller et al., 1997; Reid et al., 2005). For example, Heller et al. (1997) found that when parents experienced greater support from an adult child with intellectual disability they experienced less burden and higher levels of caregiving satisfaction. Though beneficence may be responsible for initiating caregiving actions of family members (Gouldner, 1973), these findings suggest that reciprocity in care and support may be a mechanism that contributes to sustained support from family members. Therefore, when aiming to involve and strengthen family support networks, it is important for services to consider the support that people with MID may be able to offer to their family members, to support people with MID to actively engage in family exchanges, thereby encouraging reciprocity in their family relationships.
In recent years, there has been increasing emphasis on increasing the levels of informal support and social inclusion of people with MID (Simplican et al., 2015). Cuts to the level of professional support have also made people with MID increasingly reliant on their family carers for their social capital (e.g., Malli et al., 2018). However, the culture within disability services, and especially in residential settings, seems often to be one of care, with staff prioritising care tasks over tasks to promote social inclusion (McConkey & Collins, 2010). Staff could support reciprocity in family relationships in simple ways by, for example, encouraging people with MID to invite family members to visit (Francis et al., 2016), by supporting them to take a family member (e.g., nephew, niece) out for a trip (Kramer et al., 2013), or by helping them to send cards/messages or buy presents to mark key occasions in the lives of their family members (Kuis et al., 2018). As the current study showed different perceptions about reciprocity in family relationships, it is important for staff to initiate a dialogue with both people with MID and their significant family members, and encourage them to share their individual experiences, needs, and wishes in this regard.
Perceptions of participants with MID and family members did not diverge on all aspects of family relationships. Contrary to Widmer et al. (2010), no significant differences were found in the perceptions of the number of significant family members that make up the network and the number of family relationships in which support is provided to the person with MID. Participants with MID did not perceive different levels of supportive resources from the family. While family members do not always recognize the supportive behaviours of people with MID (see earlier), they perceived similar levels of supportive behaviours from the family to the person with MID.
An examination of factors that may account for divergence in perceptions between people with MID and their family members found associations between divergence on out‐degree estimates and externalizing behaviour. Several explanations for this finding may exist. First, people who increasingly lack the family's recognition of their supportive behaviours, may develop lower levels of self‐esteem (Liang et al., 2001), which in turn may lead to increased levels of externalizing behaviours (Donnellan et al., 2005). Second, family members of people with intellectual disability who display externalizing behaviours experience increased stress and emotional difficulties (Dreyfus & Dowse, 2018). For these family members, building rewarding or reciprocal relationships, in which their relative's supportive behaviours are recognized, may be challenging or the experienced difficulties may affect their perceptions of their relative's place in the family. Therefore, it seems important for staff and services supporting people with MID who display externalizing behaviour to recognize the additional challenges they and their families might be facing to build positive reciprocal relationships within the family. We also found that women were significantly more likely than men to disagree with family members on their bridging social capital. This might be linked to gender biases: Women's bridging roles in friendship networks were significantly underrecognised by other network members (Brands & Kilduff, 2014).
4.1. Limitations and future research
A number of sampling and methodological issues are important to discuss as they relate to the generalisability of the current findings. First, there is a risk of non‐response bias. Only 42.4% of the invited people with MID accepted the invitation to participate. As no other data were available for the nonrespondents, it was not possible to quantify biases in the sample selection. Additionally, 30 of the eligible 150 family members did not participate in the current study and only the data of people with MID with a participating family member were included (thus, findings should be generalized with caution).
Third, the findings concerned a specific group of people with MID; all lived apart from family and were frequently supported by staff from a service provider. Future research should address the perceptions of individuals with MID who live, for example, at home with and without professional support. Fourth, this study was based on the perceptions of people with MID and one of their family members only. Though this study makes a valuable contribution to our understanding about relationships in families of people with MID, each individual family member may experience the same family relationships in different ways (e.g., Henggeler et al., 1987). As such, perceptions of neither people with MID nor family members can be viewed as the actual patterns of relationships. When viewing social networks as cognitive structures, individuals are said to have accurate views of their social networks to the extent that they perceive a relationship between two individuals that is confirmed by those individuals. To further examine differences in perceptions, future studies could use a multi‐informant network research design in which all members of the family are interviewed on all relationships within the family.
Fifth, the current study included quantitative family network data from the perspective of a relatively large group of participants with MID and their family members. It might be of interest for future research to include an in‐depth exploration of how a smaller group of people with MID and also family members explain their responses to a structured method such as the family network method. Finally, when exploring factors that are associated with divergence in perceptions between people with MID and family members, the current study showed associations with externalizing behaviour and the sex of the person with MID only. Future research could explore other factors such as the closeness and frequency of the contact between the person with MID and the family member, the level of intellectual disability, and adaptive functioning (Schmidt et al., 2010).
Despite these limitations, the current study contributes to our understanding of relationships in the family networks of people with MID by demonstrating how their own perceptions compare to those of their family members. As participants with MID and family members were found to have different perceptions on several aspects of the family support network (i.e., bonding and bridging social capital, support provided by the person with MID, and the reciprocity of the family relationships of the person with MID), family professionals and services should seek the views of both people with MID and family members when carrying out assessments or organizing supports.
CONFLICT OF INETERST
None.
ACKNOWLEDGEMENTS
We would like to thank the individuals who participated in this study and the staff from the service providers who supported recruitment to the research.
Giesbers SAH, Hendriks AHC, Hastings RP, Jahoda A, Tournier T, Embregts PJCM. Perceptions of people with mild intellectual disability and their family members about family‐based social capital in the Netherlands. Health Soc Care Community. 2022;30:341–352. 10.1111/hsc.13407
Funding information
The research was funded by service providers Dichterbij and ASVZ. Dichterbij and ASVZ have not imposed any restrictions on free access to or publication of the research data. All authors declare that they have no conflict of interest. This manuscript has not been previously published and is not under consideration in the same or substantially similar form in any other (peer‐reviewed) media. All authors listed have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline. We have included acknowledgements, conflicts and funding sources on the title page.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study can be requested from the corresponding author upon reasonable request on the basis of a Data Transfer Agreement (DTA).
REFERENCES
- Achenbach, T. , & Rescorla, L. (2003). Manual for the ASEBA adult forms and profiles. University of Vermont. [Google Scholar]
- Arscott, K. , Dagnan, D. , & Stenfert Kroese, B. (1998). Consent to psychological research by people with an intellectual disability. Journal of Applied Research in Intellectual Disabilities, 11(1), 77–83. 10.1111/j.1468-3148.1998.tb00035.x [DOI] [Google Scholar]
- Barnes, H. L. , & Olsen, D. H. (1985). Parent‐adolescent communication and the circumplex model. Child Development, 56(2), 438–447. 10.2307/1129732 [DOI] [Google Scholar]
- Bartle‐Haring, S. , Kenny, D. A. , & Gavazzi, S. M. (1999). Multiple perspectives on family differentiation: Analyses by multitrait multimethod matrix and triadic social relations models. Journal of Marriage and Family, 61(2), 491–503. 10.2307/353764 [DOI] [Google Scholar]
- Borgatti, S. P. , Everett, M. G. , & Freeman, L. C. (2002). UCINET for Windows. Software for social network analysis. Analytic Technologies. [Google Scholar]
- Bourdieu, P. (1986). The forms of capital. In Richardson J. (Ed.), Handbook of theory and research in the sociology of education (pp. 241–568.Greenwood Press. [Google Scholar]
- Brands, R. , & Kilduff, M. (2014). Just Like a Woman? Effects of gender‐biased perceptions of friendship network brokerage on attributions and performance. Organization Science, 25(5), 1530–1548. 10.1287/orsc.2013.0880 [DOI] [Google Scholar]
- Bullen, P. , & Onyx, J. (1999). Social capital: Family support services and neighbourhood and community centres in NSW. [Google Scholar]
- Burt, R. (1995). Structural holes. The social structure of competition. Harvard University Press. [Google Scholar]
- Castro‐Schilo, L. , & Grimm, K. J. (2018). Using residualized change versus difference scores for longitudinal research. Journal of Social and Personal Relationships, 35(1), 32–58. 10.1177/0265407517718387 [DOI] [Google Scholar]
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Erlbaum. [Google Scholar]
- Coleman, J. (1988). Social capital and the creation of human capital. American Journal of Sociology, 94, 95–121. 10.1086/228943 [DOI] [Google Scholar]
- Cummins, R. A. , & Lau, A. D. L. (2005). Personal wellbeing index‐intellectual disability. , 3rd ed. Deakin University. [Google Scholar]
- Donnellan, M. B. , Trzesniewski, K. H. , Robins, R. W. , Moffitt, T. E. , & Caspi, A. (2005). Low self‐esteem is related to aggression, antisocial behavior, and delinquency. Psychological Science, 16(4), 328–335. 10.1111/j.0956-7976.2005.01535.x [DOI] [PubMed] [Google Scholar]
- Dreyfus, S. , & Dowse, L. (2018). Experiences of parents who support a family member with intellectual disability and challenging behaviour: “This is what I deal with every single day”. Journal of Intellectual & Developmental Disability, , 45(1), 12–22. 10.3109/13668250.2018.1510117 [DOI] [Google Scholar]
- Dunlap, W. P. , Cortina, J. M. , Vaslow, J. B. , & Burke, M. J. (1996). Meta‐analysis of experiments with matched groups or repeated measures designs. Psychological Methods, 1(2), 170–177. 10.1037/1082-989X.1.2.170 [DOI] [Google Scholar]
- Ferlander, S. (2007). The importance of different forms of social capital for health. Acta Sociologica, 50(2), 115–118. 10.1177/0001699307077654 [DOI] [Google Scholar]
- Francis, G. L. , Blue‐Banning, M. , Haines, S. J. , Turnbull, A. P. , & Gross, J. M. S. (2016). Building “Our School”: Parental perspectives for building trusting family‐professional partnerships. Preventing School Failure: Alternative Education for Children and Youth, 60(4), 329–336. 10.1080/1045988X.2016.1164115 [DOI] [Google Scholar]
- Furstenberg, F. F. , & Kaplan, S. B. (2004). Social capital and the family. In Richards I. M., Scott J., & Treas J. (Eds.), Blackwell companion to the sociology of families (pp. 218–232). Blackwell Publisher. [Google Scholar]
- Giesbers, S. A. H. , Hendriks, A. H. C. , Hastings, R. P. , Jahoda, A. , Tournier, T. , & Embregts, P. J. C. M. (2020a). Social capital and the reciprocal nature of family relationships: The perspective of individuals with mild intellectual disability. American Journal on Intellectual and Developmental Disabilities, 125(3), 170–185. 10.1352/1944-7558-125.3.170 [DOI] [PubMed] [Google Scholar]
- Giesbers, S. A. H. , Hendriks, A. H. C. , Hastings, R. P. , Jahoda, A. , Tournier, T. , & Embregts, P. J. C. M. (2020b). Family‐based social capital of emerging adults with and without mild intellectual disability. Journal of Intellectual Disability Research, 64(10), 757–769. 10.1111/jir.12764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giesbers, S. A. H. , Tournier, T. , Hendriks, A. H. C. , Hastings, R. P. , Jahoda, A. , & Embregts, P. J. C. M. (2019). Measuring emotional support in family networks: Adapting the Family Network Method for individuals with a mild intellectual disability. Journal of Applied Research in Intellectual Disabilities, 32(1), 94–105. 10.1111/jar.12512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez, R. , & Griffin, D. (2012). Dyadic data analysis. In Cooper H. (Ed.), APA handbook of research methods in psychology: Vol. 3. Data analysis and research publication (pp. 439–450). APA. 10.1037/13621-022 [DOI] [Google Scholar]
- Gouldner, A. W. (1973). The importance of something for nothing. In Gouldner I. A. W. (Ed.), For sociology: Renewal and critique in sociology today (pp. 260–299). Allen Lane. [Google Scholar]
- Grey, J. M. , Griffith, G. M. , Totsika, V. , & Hastings, R. P. (2015). Families' experiences of seeking out‐of‐home accommodation for their adult child with an intellectual disability. Journal of Policy and Practice in Intellectual Disabilities, 12(1), 47–57. 10.1111/jppi.12106 [DOI] [Google Scholar]
- Heller, T. , Miller, A. B. , & Factor, A. (1997). Adults with mental retardation as supports to their parents: Effects on parental caregiving appraisal. Mental Retardation, 35(5), 338–346. 10.1352/0047-6765(1997)035<0338:AWMRAS>2.0.CO;2 [DOI] [PubMed] [Google Scholar]
- Henggeler, S. W. , Borduin, C. M. , & Mann, B. J. (1987). Intrafamily agreement: Association with clinical status, social desirability, and observational ratings. Journal of Applied Developmental Psychology, 8(1), 97–111. 10.1016/0193-3973(87)90023-2 [DOI] [Google Scholar]
- Jager, J. , Bornstein, M. H. , Diane, P. L. , & Hendricks, C. (2012). Family members‘ unique perspectives of the family: Examining their scope, size, and relations to individual adjustment. Journal of Family Psychology, 26, 400–410. 10.1037/a0028330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jager, J. , Yuen, C. X. , Bornstein, M. H. , Diane, P. L. , & Hendricks, C. (2014). The relations of family members‘ unique and shared perspectives of family dysfunction to dyad adjustment. Journal of Family Psychology, 28, 407–414. 10.1037/a0036809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kozma, A. , Mansell, J. , & Beadle‐Brown, J. (2009). Outcomes in different residential settings for people with intellectual disability: A systematic Review. American Journal on Intellectual and Developmental Disabilities, 114(3), 193–222. 10.1352/1944-7558-114.3.193 [DOI] [PubMed] [Google Scholar]
- Krackhardt, D. (1987). Cognitive social structures. Social Networks, 9(2), 109–134. 10.1016/0378-8733(87)90009-8 [DOI] [Google Scholar]
- Kramer, J. , Hall, A. , & Heller, T. (2013). Reciprocity and social capital in sibling relationships of people with disabilities. Intellectual and Developmental Disabilities, 51(6), 482–495. 10.1352/1934-9556-51.6.482 [DOI] [PubMed] [Google Scholar]
- Kuis, E. , Hermsen, M. , Van Heijst, A. , Timmermann, M. , & Embregts, P. (2018). Examining the voluntary deployment of people without a disability on behalf of people with disabilities: “Verwenzorg”(“LC”) as an example. Journal of Social Intervention, 27(1), 48–66. 10.18352/jsi.534 [DOI] [Google Scholar]
- Liang, J. , Krause, N. M. , & Bennett, J. M. (2001). Social exchange and well‐being: Is giving better than receiving? Psychology and Aging, 16(3), 511–523. 10.1037//0882-7974.16.3.511 [DOI] [PubMed] [Google Scholar]
- Malli, M. A. , Sams, L. , Forrester‐Jones, F. , Murphy, G. , & Henwood, M. (2018). Austerity and the lives of people with learning disabilities. A thematic synthesis of current literature. Disability & Society, 33(9), 1412–1435. 10.1080/09687599.2018.1497950 [DOI] [Google Scholar]
- McConkey, R. , & Collins, S. (2010). The role of support staff in promoting the social inclusion of persons with an intellectual disability. Journal of Intellectual Disability Research, 54(8), 691–700. 10.1111/j.1365-2788.2010.01295.x [DOI] [PubMed] [Google Scholar]
- McGillivray, J. A. , Lau, A. L. D. , Cummins, R. A. , & Davey, G. (2009). The utility of the Personal Well‐being Index Intellectual Disability Scale (PWI‐ID) in an Australian sample. Journal of Applied Research in Intellectual Disability, 22(3), 276–286. 10.1111/j.1468-3148.2008.00460.x [DOI] [Google Scholar]
- McPherson, K. E. , Kerr, S. , McGee, E. , Morgan, A. , Cheater, F. M. , McLean, J. , & Egan, J. (2014). The association between social capital and mental health and behavioural problems in children and adolescents: An integrative systematic review. BMC Psychology, 2, 7–23. 10.1186/2050-7283-2-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milner, P. , & Kelly, B. (2009). Community participation and inclusion: People with disabilities defining their place. Disability & Society, 24(1), 47–62. 10.1080/09687590802535410 [DOI] [Google Scholar]
- Portes, A. (1998). Social capital: Its origins and applications in modern sociology. Annual Review of Sociology, 24, 1–24. 10.1146/annurev.soc.24.1.1 [DOI] [Google Scholar]
- Reid, C. E. , Moss, S. , & Hyman, G. (2005). Caregiver reciprocity: The effect of reciprocity, carer self‐esteem and motivation on the experience of caregiver burden. Australian Journal of Psychology, 57(3), 186–196. 10.1080/00049530500141022 [DOI] [Google Scholar]
- Sanderson, K. A. , Burke, M. M. , Urbano, R. C. , Arnold, C. K. , & Hodapp, R. M. (2017). Who helps? Characteristics and correlates of informal supporters to adults with disabilities. American Journal on Intellectual and Developmental Disabilities, 122(6), 492–510. 10.1352/1944-7558-122.6.492 [DOI] [PubMed] [Google Scholar]
- Sanderson, K. A. , Burke, M. M. , Urbano, R. C. , Arnold, C. K. , & Hodapp, R. M. (2019). Getting by with a little help from my friends: Siblings report on the amount of informal support received by adults with disabilities. Journal of Intellectual Disability Research, 63(9), 1097–1110. 10.1111/jir.12622 [DOI] [PubMed] [Google Scholar]
- Schmidt, S. , Power, M. , Green, A. , Lucas‐Carrasco, R. , Eser, E. , Dragomirecka, E. , & Fleck, M. (2010). Self and proxy rating of quality of life in adults with intellectual disabilities: Results from the DISQOL study. Research in Developmental Disabilities, 31(5), 1015–1026. 10.1016/j.ridd.2010.04.013 [DOI] [PubMed] [Google Scholar]
- Simplican, S. C. , Leader, G. , Kosciulek, J. , & Leahy, M. (2015). Defining social inclusion of people with intellectual and developmental disabilities: An ecological model of social networks and community participation. Research in Developmental Disabilities, 38, 18–29. 10.1016/j.ridd.2014.10.008 [DOI] [PubMed] [Google Scholar]
- Tenneij, N. , & Koot, H. (2007). A preliminary investigation into the utility of the Adult Behavior Checklist in the assessment of psychopathology in people with low IQ. Journal of Applied Research in Intellectual Disability, 20(5), 391–400. 10.1111/j.1468-3148.2007.00383.x [DOI] [Google Scholar]
- Tzanakis, M. (2013). Social capital in Bourdieu's, Coleman's and Putnam's theory: Empirical evidence and emergent measurement issues. Educate, 13(2), 2–23. [Google Scholar]
- Umberson, D. , & Montez, D. (2010). Social relationships and health: A flashpoint for health policy. Journal of Health and Social Behavior, 51, S54–S66. 10.1177/0022146510383501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Asselt‐Goverts, A. E. , Embregts, P. J. C. M. , & Hendriks, A. H. C. (2013). Structural and functional characteristics of the social networks of people with mild intellectual disabilities. Research in Developmental Disabilities, 34(4), 1280–1288. 10.1016/j.ridd.2013.01.012 [DOI] [PubMed] [Google Scholar]
- Van Emmerik, I. H. (2006). Gender differences in the creation of different types of social capital: A multilevel study. Social networks, 28(1), 24–37. 10.1016/j.socnet.2005.04.002 [DOI] [Google Scholar]
- Van Heel, M. , Bijttebier, P. , Colpin, H. , Goossens, L. , Den Noortgate, V. , Verschueren, K. , & Van Leeuwen, K. (2019). Adolescent‐parent discrepancies in perceptions of parenting: Associations with adolescent externalizing problem behavior. Journal of Child and Family Studies, 28, 3170–3182. 10.1007/s10826-019-01493-7 [DOI] [Google Scholar]
- Wechsler, D. (2011). Wechsler abbreviated scale of intelligence‐second edition (WASI‐II). NCS Pearson. [Google Scholar]
- Wechsler, D. (2012). Wechsler adult intelligence scale – Fourth, Dutch ed. . Pearson Assessment and Information BV. [Google Scholar]
- Widmer, E. D. , Kempf, N. , Sapin, M. , & Galli‐Carminati, G. (2013). Family beyond parents? An exploration of family configurations and psychological adjustment in you adults with intellectual disability. Research in Developmental Disabilities, 34(4), 207–217. 10.1016/j.ridd.2012.07.006 [DOI] [PubMed] [Google Scholar]
- Widmer, E. D. , Kempf‐Constantin, N. L. , & Galli‐Carminati, G. (2010). Exploring perceptions of family relationships by individuals with intellectual disability and psychiatric disorders. Families in Society: the Journal of Contemporary Social Services, 91(4), 378–384. 10.1606/1044-3894.4041 [DOI] [Google Scholar]
- Widmer, E. D. , Kempf‐Constantin, N. , Robert‐Tissot, C. , Lanzi, F. , & Galli‐Carminati, G. (2008). How central and connected am I in my family? Family‐based social capital of individuals with intellectual disability. Research in Developmental Disabilities, 29(2), 176–187. 10.1016/j.ridd.2007.02.005 [DOI] [PubMed] [Google Scholar]
- Woolcock, M. (1998). Social capital and economic development: Towards a theoretical synthesis and policy framework. Theory and Society, 27(2), 151–208. 10.1023/A:1006884930135 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study can be requested from the corresponding author upon reasonable request on the basis of a Data Transfer Agreement (DTA).