

Abstract
Objectives
This review aims to identify types of the existing fall prevention education (FPE) and their effectiveness in promoting fall risk awareness, knowledge and preventive fall behaviour change among community‐dwelling older people.
Background
FPE is a cost‐effective and helpful tool for reducing fall occurrences.
Evaluation
This is a systematic review study using electronic searches via EBSCOHost® platform, ScienceDirect, Scopus and Google Scholar in March 2021. The review protocol was registered with PROSPERO (CRD42021232102). The Preferred Reporting Items for Systematic reviews and Meta‐Analyses (PRISMA) statement flow chart guided the search strategy. Articles published from January 2010 to March 2021 were included for quality appraisal using the ‘Transparent Reporting of Evaluations with Non‐randomised Designs’ (TREND) and the ‘Consolidated Standards of Reporting Trials’ (CONSORT) statement for randomised controlled trial studies.
Key issues
Six FPE studies selected emphasised on personal health status, exercise and environmental risk factors. These studies reported an increase in fall risk awareness or knowledge and a positive change in fall preventive behaviours. Two studies included nurses as educators in FPE.
Conclusion
FPE evidently improved awareness or knowledge and preventive fall behaviour change among older adults. Nurses are in great potential in planning and providing FPE for older adults in community settings.
Implications for Nursing Management
Expand nurses' roles in fall prevention programmes in community settings by using high‐quality and evidence‐based educational tools. Highlight the nurse's role and collaborative management in FPE.
Keywords: community‐dwelling older adult, fall, fall prevention education, fall risk, older adult
1. INTRODUCTION
Fall prevention education (FPE) is one of the strategies that is an inexpensive, less activity involvement and helpful tool for reducing fall occurrences (Kamei et al., 2015; Ott, 2018). In addition, it is essential that initiation of awareness begins with education. It will evidently improve the awareness and knowledge of older adults in recognising their fall threats so that early preventions can be prioritised (Ott, 2018). Furthermore, evaluating older individuals' knowledge deficits is the initial step to implement individualised and appropriate instruction (Ott, 2018). Providing FPE also enhances positive health care outcomes in older individuals (Chaudhry, 2020; Chidume, 2021). This is because they are becoming more independently sustained within their perceived quality of life to perform daily activities and live in safer environment (Minnier et al., 2019).
2. BACKGROUND
Despite that, many older individuals who live in rural or urban neighbourhoods are still unaware of their odds of falling or denying that they are at risk of falling (Loganathan et al., 2015; Mihaljcic et al., 2015). This lack of awareness and denial created more hindrances for unreported falls, poor help‐seeking after fall injuries and refusal to accept that they are the higher group at risk of fall (Greenberg, 2020; Mihaljcic et al., 2015). Due to these concerns, there has been an inadequate translation of this focus into the community settings on older adults' fall risk awareness, knowledge and fall preventive behaviour change after FPE (Heng et al., 2020; Hill et al., 2015; King et al., 2018). Most FPE studies and reviews pay attention to older patients in hospital settings (Hill et al., 2015; Williams & Hadler, 2015) or nursing homes (Uymaz & Nahcivan, 2016).
Promoting fall risk awareness and knowledge will enhance their attention about their potential for falls, encourage them to analyse their current situation at risk of falls and possibly apply or engage in behaviour or lifestyle changes (Flint et al., 2020; Kiegaldie & Farlie, 2019). Thus, fall risk awareness and knowledge indirectly influence older individuals' decision to participate in preventive behaviour change. Contrarily, most FPE studies demonstrated fall risk scores or falls or fall injurious as the primary outcomes instead of fall risk awareness or knowledge and fall preventive behaviour (Chidume, 2021; Harrison, 2017; Hill et al., 2017; Kuhirunyaratn et al., 2019).
Although abundant studies were conducted in education interventions, little is known that some studies had poorly expressed their evidence base for educational design (Kiegaldie & Farlie, 2019). Hence, researchers have to be conversant in determining a high‐quality education design to have a robust, well‐organised and proper measure of the expected outcomes in their studies (Kiegaldie & Farlie, 2019).
3. METHODS
3.1. Aims
This review aims to (i) identify types of the existing FPE and their effectiveness in promoting fall risk awareness, knowledge and preventive fall behaviour change among community‐dwelling older people; (ii) identify theoretical frameworks underpinned in educational designs; (iii) review the quality of educational programmes; (iv) identify nurses' role or involvement in providing FPE in the community settings.
3.2. Design
This systematic review was referred from the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) (Moher, Liberati, et al., 2010). A review protocol was created and the PROSPERO has approved and registered on 3 April 2021 with the registration number CRD42021232102.
3.3. Inclusion and exclusion criteria
A PICO framework was created (Moher, Liberati, et al., 2010), which considered population (P), community‐dwelling older adults; interest area/Intervention (I), fall prevention awareness or education; comparator interventions (C), usual care; outcomes (O), fall prevention knowledge or fall risk awareness and fall prevention behaviour change.
The target population was (a) the older adult of 60 years and older, (b) those older people who were living independently in the communities, (c) research studies on fall risks awareness or FPEs and (d) studies that adopt an experimental design and (e) the outcomes measure was fall risk awareness or knowledge and fall prevention behaviour change. The study excluded (a) older people living in a long‐term care facility or assisted living facility and who have been hospitalised, (b) older adults suffering from medical illnesses such as Parkinson's disease, severe dementia, post‐stroke and mental illnesses such as schizophrenia and psychotic disorders and (d) intervention studies that do not report the outcome of fall risk awareness, knowledge and fall preventive behaviour. (e) Any types of report, abstracts and conference posters are excluded and studies that have been available in non‐English were omitted.
3.4. Search strategy
The study's literature review integrated articles that were published from 2010 to March 2021 via the EBSCOHost® platform, ScienceDirect, Google Scholar and Scopus databases during the search dates of 3–18 March 2021.
3.5. Search selection
Researchers used the PRISMA flow diagram to guide the selection process (Moher, Liberati, et al., 2010) as shown in Figure 1. Ultimately, six studies were eventually selected for the review (Figure 1). The corresponding researcher had contacted the authors of two articles for the full text. However, one of the authors was on sabbatical leave (Minnier et al., 2019), and another author was unavailable (Azzarello & Hall, 2016). One article that recruited an older adult of 56 years old has been included in this review because their actual inclusion for older adults age was 60 years and above (Howard et al., 2016).
FIGURE 1.
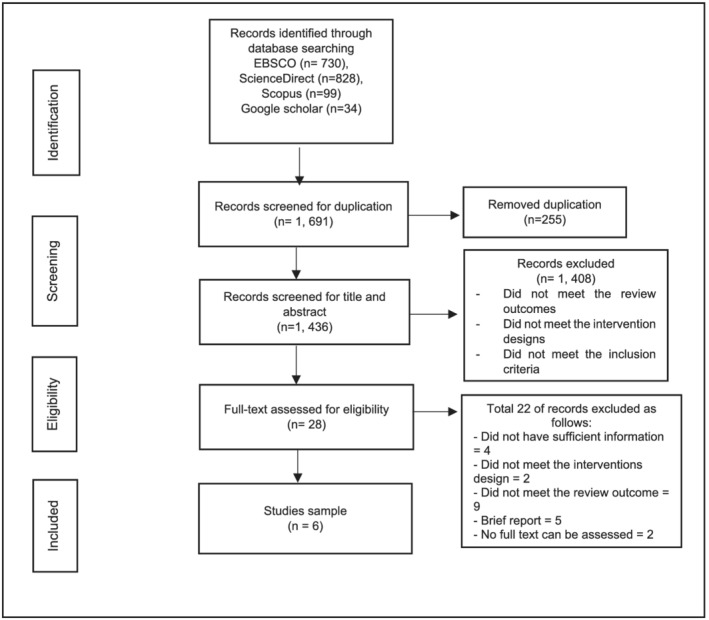
The Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) diagram of the article search
3.6. Quality appraisal
TREND statement (Des Jarlais, Lyles, Crepaz,, & the TREND Group, 2004) and CONSORT statement (Moher, Hopewell, et al., 2010) used for quality appraisal. As a result, it proves that four studies consist good quality assessments (Howard et al., 2016; Khong et al., 2017; Ott, 2018; Kamei et al., 2015) and another two studies with low‐quality assessments respectively (Chen, 2013; Schepens et al., 2011).
3.7. The risk of bias assessment
Table 1 shows risk of bias assessment for randomised studies using Cochrane Collaboration's tool (Higgins et al., 2011). Table 2 assesses the non‐randomised studies using a tool from Kim et al. (2013). Overall, two randomised and non‐randomised studies have low‐risk biases, and another two non‐randomised studies are assessed to have a high‐risk bias respectively.
TABLE 1.
The risk of Bias assessment in selected randomised studies (from the assessment tool of Higgins et al., 2011)
| No. | Bias | Schepens et al. (2011) | Support evidence | Kamei et al. (2015) | Support evidence |
|---|---|---|---|---|---|
| 1 |
Random sequence generation (selection bias) |
Unclear risk | ‘Participants were randomised to one of two multimedia intervention groups or a control group using a block randomisation technique.’ However, their fallers and non‐fallers were not equally distributed among the three groups, and no further details of the randomisation procedure were explained. | Low risk | Flow diagram for randomisation was given, with description details in participants' age, gender, physical status, fall risks, a person who performed housing repair in the past, and a number of fallers over the previous year were similar in both the groups. |
| 2 | Allocation concealment (selection bias) | High risk | No information was provided. | High risk | No information was provided. |
| 3 | Blinding of participants and researchers (performance bias) | Low risk | ‘Participants, but not the primary investigator, were unaware of group allocation and differences in intervention protocols.’ | Unclear risk | ‘Research assistants allocated participants randomly into either the HHMP group or the control group and without the presence of the researchers.’ There was no further explanation about the procedure. |
| 4 | Blinding of outcome assessment (detection bias) | Low risk | ‘Participants were unaware of differences in intervention protocols.’ | High risk | No information was provided. |
| 5 | Incomplete outcome data (attrition bias) | Low risk | All losses to follow up and the number of participants who remained for analyses was demonstrated in the flow diagram. Reporting of 1–2 participants either dropped for the group or lost to follow‐up. The number of about 17–18 participants in one group remained. The attrition rate was low and not expected to affect the result. | Low risk | Kaplan–Meier survival analysis with the log‐rank (Mantel–Cox) test undertaken on an intention‐to‐treat basis. The original number of participants for the intervention/control group analysed for intention‐to‐treat. A total of 63 and 67 participants |
| 6 | Selective reporting (reporting bias) | Low risk | Most outcomes reported | Low risk | All outcomes reported, inclusive of participants intended to treat. |
| 7 | Other bias | Unclear risk | A small number of participants in each group may give rise to challenge in the conclusion of the finding. | Low risk | Retained the original number of participants for intention‐to‐treat, analysed, and report as its final findings. |
| Overall | Low risk | Low risk |
TABLE 2.
The risk of Bias assessment in selected non‐randomised studies (using the assessment tool of Kim et al., 2013)
| No. | Bias | Chen (2013) | Howard et al. (2016) | Ott (2018) | Khong et al. (2017) |
|---|---|---|---|---|---|
| 1 | Selection of participants | Low risk | High risk | High risk | Low risk |
| 2 | Confounding variables | Unclear risk | Unclear risk | Low risk | Low risk |
| 3 | Measurement of exposure | Unclear risk | High risk | Low risk | Low risk |
| 4 | Blinding of outcome assessments | High risk | High risk | High risk | Low risk |
| 5 | Incomplete outcome data | Low risk | Low risk | Low risk | Low risk |
| 6 | Selective outcome reporting | High risk | Low risk | Low risk | Low risk |
| Overall | High risk | High risk | Low risk | Low risk |
3.8. Data abstraction and data analysis
Data were extracted from the selected eligible studies into a table. Table 3 summarises the tabulated information. The team members then reviewed the tabulated data to ensure accuracy. Table 4 assesses the quality of educational programmes using a metric tool by Heng et al. (2020). The scoring was categorised for ‘yes’ response as ‘1’ and ‘0’ or ‘not stated’ response as ‘0’. The range of 0–6 points denotes low quality, whereas 7–12 points indicate moderate quality and 13–17 represent high quality. The corresponding author and the team members discussed to achieve a consensus on the assessment.
TABLE 3.
Characteristics of included studies
| Intervention/control group | ||||||
|---|---|---|---|---|---|---|
| Author | Objective | Participant characteristics | Participant gender |
(i) Knowledge (ii) Fall risk behaviour or fall rate |
Major findings | Quality assessment |
| Chen (2013), Taiwan | To examine the outcome of a health education programme intervention of elderly fall prevention at home |
Aged between 65–80 years old; treatment group: n = 80; control group: n = 79 |
Female: 108 (67.9%); male 51 (32.1%) |
(i) Knowledge: F: 2.607; p = .233; 95% CI (1.127–0.277) (pre‐test); F: 57.873; p < .001; 95% CI (−2.068 to −1.093) (post‐test) (ii) Behaviour: F: 103.751; p < .001; 95% CI (−2.386 to −1.083) |
A different mean was reported in the fall education group, and the intervention group shows an improvement in prevention knowledge and fall prevention behaviour instead of the control group. |
Low |
|
Howard et al. (2016), USA |
To determine if a two‐visit, personalised fall prevention educational intervention affected awareness of fall risk and to assess new learning in a cross‐cultural context and willingness tomake lifestyle changes to reduce fall risk. |
Age from 56 to 92 years of age, with a mean age of 77 years; all lived in home; 16 reported had fallen in the previous 1 year; Most participants received elementary education (n = 8); comorbidities of hypertension, cataract, arthritis, diabetes and stroke. |
Four males and 14 females had participated in the study. |
(i) FRAQ scores increased from pre‐test to post‐test from 27.18 to 27.47, p = .704 (after removing an outlier). (ii) Willingness to make lifestyle changes related to fall prevention. |
There was a slight increase in the means of the total post‐test by 0.29 FRAQ scores over pre‐test scores (with the outlier removed) and the statistically significant result of the behaviour question grouping, with the outlier removed. |
Good |
|
Schepens et al. (2011), USA |
To compare the effectiveness of two tailored multimediafall prevention educational interventions in improving fall threats knowledge and engagement in fall prevention behaviours in community‐dwelling older adults. | The overall mean age: 79.2 (1); authentive: 78.3 (1.8); motivation: 80.1 (1.8); control: 79.2 (1.8). | Female: 43 (81%); male: 10 (19%). |
(i) Authentive group: post‐test 21.7 (1.7), pre‐test 17.1 (1.1), p = .004. Motivation group post‐test 23.0 (1.5), pre‐test 16.6 (2.3), p = 0.002. Control group: post‐test 15.7 (1.4), pre‐test 15.6 (2.3), p = .96. (ii) The authenticity group identified significantly more fall threats than the control group (p = .29), as did the motivation group (p = .07). (iii) Fall risk behaviour: authenticity vs. control: (p = .029); motivation vs. control: (p = .007); motivation group (7.5 ± 1.0) was significantly greater than that reported by both the authenticity (4.3 ± 0.8, p = .05) and the control (2.1 ± 1.0, p = .001). A total of 82.9% engaged in at least two new behaviours (authenticity group, 77.8%; motivation group, 88.2%), and >65% of both intervention groups engaged in at least four or more behaviours. |
Combining motivational strategies with multimedia education increased the effectiveness of the intervention in encouraging fall prevention behaviours. The multimedia‐based and tailored fall prevention education shows an effective intervention for improving fall threat knowledge and engagement in fall. | Low |
|
Ott (2018), USA |
To evaluate the impact of a fall prevention educational session on fall risk knowledge, use of fall prevention interventions, and the number of falls in community‐dwelling older persons attending physical therapy. |
The mean age of 65. 75% (N = 6) of the individuals lived in a private residence with another person. Education level, 50% (4) graduated from high school. Participants perceived their overall health status was good (62.5%). The majority had comorbidities consisting of arthritis/rheumatism and hypertension (62.5%). One participant had a fall with injuries, and three had non‐injuries falls in the past 2 years. |
Female: 6 (75%); male 2 (25%) |
(i) The means of the pre‐test and post‐test interventional FRAQ scores increased pre‐test to post‐test 0.096 (22.85–26.5), p = .031 Increased awareness of medications related to fall risks was observed by having a 50% increase in scores from pre‐test to post‐test. (ii) Fifty percent (N = 4) of the participants have made lifestyle changes based on their strategies. At the 60‐day post‐education, one participant (12.5%) experienced a fall without injuries. |
The educational intervention older adults show an increased fall risk knowledge score indicated in the post‐FRAQ scores increases. It also revealed that the same population had a higher number of participants using fall prevention interventions at home, reducing the number of falls noted compared with previous years. Powerpoint presentation and oral information will retain the information. |
Good |
|
Khong et al. (2017), Australia |
To evaluate the effect ofdelivering a peer‐led falls prevention presentation on community‐dwelling older adults' beliefs and knowledge about falls prevention, and their motivation and intention to engage in falls prevention strategies. |
Overall mean age: 78.55. The mean age in control group was 77.9 (6.9); intervention group was 79.2 (7.0). A previous 12‐month fall, n = 40 (40.4%) and intervention: n = 45 (33.8%). A self‐rated health: control: good n = 52 (52.5%); intervention: n = 22 (16.5%). |
Total female: 143 (61.6%); male: 89 (38.4%). Control: female n: 71(71.7%) and male 28 (28.3%). Intervention: female: 72 (54.1%); male: 61 (45.9%) |
(i) Participants in both control and intervention groups showed increased self‐perceived knowledge, increased self‐belief that falls prevention would be useful, and increased motivation levels to prevent falls at post‐presentation and at 1‐month follow‐up, but not significant. Female in both groups reported increased levels of knowledge about falls prevention after the presentation. (OR = 1.82, 95% CI: 1.02–3.270). Intervention (n = 133); baseline (IQR): 4.1(0.79); post‐test: 4.5 (0.53); 1 month: 4.6 (0.53). Control (n = 99); baseline: 4.2 (0.77); post‐test: 4.6 (0.53); 1 month: 4.6 (0.53) (ii) Participants in both groups also reported higher levels of intention (control median 4.4, intervention median 4.5). The intervention group reported that they had developed a clear action plan that they intended to implement to reduce their risk of falling compared to the control group (OR = 1.69, 95% CI: 1.03–2.78), a significant. Female in both groups report to plan action plan to reduce their risk of falling. (OR = 2.47, 95% CI: 1.51–4.02). |
Providing peer education raises older adults' levels ofbeliefs, knowledge, and intention to engage in fall prevention. | Good |
|
Kamei et al. (2015), Japan |
To evaluate the potential improvement of fall prevention awareness and home modification behaviours and to decrease indoor falls by applying a home hazard modification programme (HHMP) in community‐dwelling older adults followed up to 1 year in this randomised controlled trial | Overall mean age: 75.75. The mean age in intervention and control group: 75.7 (6.7) and 75.8 (6.4) respectively. The previous fall in the intervention & control group: 10 (28.4%) and 18 (28.6%), respectively. | Female: 110; male: 20; intervention: female 56 (83.6%) and male 11 (16.4); control: female 54 (85.7%) and male 9 (14.3%). |
(i) Increased knowledge in‐home hazard modification programme (HHMP) started increased at week 12 and fall prevention awareness between baseline and the 52‐week follow‐up ( p < .05). Control group: the knowledge of the control group dropped at 12 weeks, but there were no significant changes between baseline, 12 weeks, and 52 weeks; thus, this change had no effects. (ii) The HHMP group decreases fall risks. HHMP 10.9% reduction in overall falls compared with the control group (hazard ratio [HR] = 0.591, 95% CI: 0.305–1.147; log‐rank test, p = .116. The aged 75 years and older group showed a reduction in falls of 18.5% (95% CI: 0.043–0.277) and a 13.2% reduction in indoor falls (95% CI: 0.004–0.175) at 12 weeks. |
The HHMP was successful in improving fall prevention awareness and home modification behaviours in the HHMP group. There was a significant increase in fall prevention awareness in the HHMP group between baseline and 52 weeks (p < .05). |
Good |
TABLE 4.
The metric quality of education programme (adopted from Heng et al., 2020)
| Chen (2013) | Howard et al. (2016) | Schepens et al. (2011) | Ott (2018) | Khong et al. (2017) | Kamei et al. (2015) | ||
|---|---|---|---|---|---|---|---|
| Purpose (4) | Is the purpose and rationale of the education programme stated? | 1 | 1 | 1 | 1 | 1 | 1 |
| Is there a clear direction to the programme? | 1 | 1 | 1 | 1 | 1 | 1 | |
| Is there a satisfactory description of the significance of the programme? | 1 | 1 | 1 | 1 | 1 | 1 | |
| Is the education conducted in a suitable setting? | 1 | 1 | 1 | 1 | 1 | 1 | |
| Learner characteristics (2) | Is the programme pitched towards an appropriate audience? | 1 | 1 | 1 | 1 | 1 | 1 |
| Is there recognition of learner's/co‐learner's prior knowledge/experience? | 0 | 1 | 1 | 0 | 1 | 0 | |
| Teacher characteristics (4) | Is there a description of who is teaching the programme? | 0 | 1 | 1 | 1 | 1 | 1 |
| Are the teachers qualified and/or experienced on the topic? | 0 | 1 | 1 | 1 | 1 | 1 | |
| Are the teachers qualified and/or experienced in teaching? | 0 | 1 | 1 | 1 | 0 | 1 | |
| Is training on the programme offered? | 0 | 1 | 1 | 0 | 1 | 0 | |
| Learning activities (3) | Is there a description of the learning activities? | 0 | 1 | 1 | 1 | 1 | 1 |
| Are the learning activities suitable for supporting learners/co‐learners to meet the learning objectives? | 0 | 1 | 1 | 1 | 1 | 1 | |
| Is there an assessment of learner's/co‐learner's achievement of learning objectives (knowledge, skills, attitudes) | 1 | 1 | 1 | 1 | 1 | 1 | |
| Evaluation (4) | Has an evaluation been planned? | 1 | 1 | 1 | 1 | 1 | 1 |
| Is the evaluation method appropriate? | 1 | 1 | 1 | 1 | 1 | 1 | |
| Has an evaluation been conducted? | 1 | 1 | 1 | 1 | 1 | 1 | |
| Are the education outcomes reported for process (learner's/co‐learner's views on the teaching) | 1 | 1 | 1 | 1 | 1 | 1 | |
| Total (17) | 10 | 17 | 17 | 15 | 16 | 15 | |
|
0–6: low 7–12: moderate 13–17: high |
Moderate | High | High | High | High | High |
4. RESULTS
4.1. FPE, fall risk awareness and knowledge outcomes
All studies reported an evidence in improving fall risk awareness and knowledge after FPE (Tables 3 and 5). Table 3 shows the mean score of fall prevention knowledge with a p value less than .05 after post‐test interventions (Chen, 2013; Kamei et al., 2015; Ott, 2018; Schepens et al., 2011). These findings suggested a significant increase in fall risk awareness and knowledge after the post‐test interventions. Although an increased mean or median was demonstrated in fall prevention knowledge, the results were insignificant in two studies (Howard et al., 2016; Khong et al., 2017). Hence, the documented findings in Howard et al. (2016) and Khong et al. (2017) were inconclusive to indicate if FPE improves older adults' fall prevention knowledge in their studies.
TABLE 5.
The characteristics of educational programmes
| Group versus single | Content of the education programme | Mode of delivery | Duration/frequency of a session | Educational design principles and models | Education‐specific outcomes | Behaviour Change‐related outcomes | Measure used to assess fall risk awareness/knowledge | Assessor/teacher | |
|---|---|---|---|---|---|---|---|---|---|
| Chen (2013) | Not stated | Environment changes, exercise programmes | A DVD presentation: Visual and audio | Not stated | Health belief model | Increased | Increased | A self‐developed; Cronbach's alpha: .619 | Not stated |
| Howard et al. (2016) | Group education and individual home visit |
(i) Exercises, home hazards, behaviours leading to falls, medication use, vision, footwear, and foot care, blood pressure and heart issues leading to falls, and Vitamin D supplements. (ii) Centers for Disease Control and Prevention (CDC) home falls prevention checklist |
(i) An original workbook provides a visual aid. (ii) CDC home falls prevention checklist—home visit with personalised instruction |
(i) Fall prevention topics: 2–3 h. (ii) Home visit with personalised instruction: 1.5 h |
Not stated | Increased | Increased |
(i) FRAQ: fall risk awareness (ii) semi‐structured interview |
Occupational therapists, a PhD and master students in an occupational programme |
| Schepens et al. (2011) | Group education | Everyday situations in familiar environments. | Multimedia presentation: using vignettes of scenarios or video clips |
Vignettes presented brief, approximately 30‐min educational Session (45‐s scenarios × 5 pairs of video clips) in specific environments, simultaneous with first‐person narration. |
(i) Authenticity group: situated learning theory (ii) Motivation group: Attention–Relevance–Confidence–Satisfaction (ARCS) model |
Increased in interventions groups (authenticity and motivation group) |
Increased (in interventions group) |
Fall threats knowledge: 10 video clips (approximately 10 s each) presenting everyday situations in familiar environments. The pre‐ to post‐test did not duplicate intervention content. |
A licensed occupational therapist and instructional technologist. |
| Ott (2018) | Not stated |
The definition of a fall, prevalence of falls, the complication of falls, where older adults tend to fall the most, high‐fall risk‐associated diseases, common risk factors with emphasis on pertinent fall risk factors identified for each participant, and fall prevention interventions |
(i) PowerPoint presentation (ii) Booklet |
The 1st session: 1.5 h | Health belief model | Increased | Increased |
(i) FRAQ: awareness of fall risk factors (ii) The second post‐test assessment: (a) questionnaire by Lord et al. (2001), ( b) post‐discharge questionnaire by Hill et al. (2009) |
Family nurse practitioner and physical therapist |
| Khong et al. (2017) | A peer‐led for group education | Falls‐related content knowledge such as risk factors for falls and strategies for reducing the risk of falls, including managing one's medications, improving balance by undertaking exercises, checking feet and footwear and completing environmental modifications | Videotape, booklet, flyers and presentation |
1‐h presentation for each session |
behaviour change wheel theory and educational and adult learning principles | Increased |
Enhanced in behaviour engagement. |
Based on the framework of behaviour change wheel theory (Michie et al., 2011), namely, capability (awareness and knowledge), opportunity, and motivation (Michie et al., 2011). |
Community engagement officer, physical therapist and peer educator |
| Kamei et al. (2015) | Group education (20 pax) |
(i) A residential safety self‐assessment consisting of a 33 item self‐checklist and the CDC (2005) home fall prevention checklist for older adults modified for Japanese settings with added items. (ii) A home hazard awareness programme and education: using a displayed 60 cm × 60 cm residential mock‐up |
Non‐specific presentation (lecture). Another practical session using the mock‐up. | Weekly for 2 h/session for a total of 4 weeks | Not stated |
Increased knowledge of in‐home hazard modification programme (HHMP) |
Improved in home modification behaviour |
A 10‐item original questionnaire on falls that developed and used in another study (Kamei et al., 2010) by researchers to assess older adults' fall prevention awareness. |
Public health nurse researcher for home hazard modifications education |
Howard et al. (2016) revealed that discrepancies exist in health literacy among older participants in their study when they could not understand fall risks or fall risk concepts and the questionnaires, whereas in Khong et al. (2017), their participants stated that the information was irrelevant since they never experience a fall. However, the females in both intervention and control groups had greater knowledge levels than their counterparts after FPE (Khong et al., 2017). Khong et al. (2017) justified that those who had previously discussed fall prevention with their health care providers or received falls prevention information demonstrated to have superior knowledge than the others.
One randomised control trial (RCT) reported a significant finding and increased mean score in fall risk knowledge for the intervention groups. It may be explained from a combination of evidence‐based theoretical frameworks and approaches of tailoring multimedia‐based enhancing their interventions' general design and presentations (Schepens et al., 2011). Another RCT indicates improved knowledge in the home hazard modification programme after using a mock‐up home setting and a hands‐on session to contextualise the real‐life home setting with average participants scores almost at the highest point of the knowledge indicator (Kamei et al., 2015). Furthermore, Ott (2018) revealed that increased knowledge levels are becoming a protective factor in reducing older persons from falling. This finding explained that their fall risk awareness promotes them to recognise their fall threats and prevent them from experience falls. Unfortunately, Chen (2013) did not report any details for the significant finding.
4.2. FPE and behaviour change‐related outcome
All studies revealed a positive change in intention or engagement of fall preventive behaviours (Tables 3 and 5) (Chen, 2013; Howard et al., 2016; Kamei et al., 2015; Khong et al., 2017; Ott, 2018; Schepens et al., 2011). Four out of six studies demonstrated a significant finding in older adults' behaviour change (Chen, 2013; Howard et al., 2016; Khong et al., 2017; Schepens et al., 2011), except in Kamei et al. (2015) and Ott (2018). The mean age of participants in Kamei et al. (2015) was 76 years. This contributed to their restrictions in physical functions to adopt specific behaviour changes and compromise in the home modifications. Another study was probably due to a relatively small total number of participants (n = 8), physical constraints and needing assistance installing grab bars or railings (Ott, 2018).
More than half of the participants in a study for both intervention groups (authenticity and motivational) participated in four or more fall prevention behaviours than the control group (Schepens et al., 2011). However, no details reported on the adopted new behaviours but are referred to modifications on the home environment, walking aids and daily living activities (ADLs). Whereas, the motivational group was allowed to choose their own set of goals that excite them to be involved and accomplished more new behaviours. The participants in Howard et al. (2016) intended to make lifestyle changes by performing simple home modifications, using appropriate assistive devices or footwears, exercise, health monitoring (management and maintenance) and a healthy routine. On the contrary, Khong et al. (2017) believed that the education shared by peers motivated the learners' participation in fall preventive behaviours.
On the other hand, the experiential learning experienced by older adult learners via a mock‐up home and the practical sessions in identifying fall threat sources has successfully impacted on their fall preventive behaviour (Kamei et al., 2015). Examples of behaviour changes reported were avoiding obstacles on the floor or pathway (newspapers, books and electrical cords), securing throw rugs or mats in various places, installing grab bars in the room or bathroom, adjusting the bed height and being cautious on pets. Another study revealed that half of the participants were positively involved in lifestyle changes after receiving FPE (n = 4) (Ott, 2018). Unfortunately, there was no further explanation in a study by Chen (2013).
4.3. FPE and its contents
Table 5 demonstrates that three studies have almost similar fall risk topics reporting in FPE such as the definition of a fall, prevalence and risk factors of falls, the common myths about falls, the complication of falls, places of frequent fall and fall prevention or reducing the risk of falls strategies (managing medications, balance training, choosing suitable footwear, modifications of the home environment) (Howard et al., 2016; Khong et al., 2017; Ott, 2018). Two studies focused on home or environmental risks (Kamei et al., 2015; Schepens et al., 2011), and another study provided education on environmental risks and exercise information (Chen, 2013). Kamei et al. (2015) introduced and demonstrated their 60 × 60 cm residential mock‐up to the older community to educate and practise real‐life situations on home hazard awareness to modify and create safety in a residential environment. In addition, Schepens et al. (2011) aimed at educating the community older persons to recognise the environmental fall risks using everyday situations in familiar environments through vignettes of video clips.
A few studies employed an established checklist such as from the Centers for Disease Control and Prevention (CDC) of home fall prevention checklist for older adults and the Prevention of Falls in Older Persons from the American Geriatrics Society as well as British Geriatrics Society for Clinical Practice Guideline.
4.4. Educational design principles and theoretical frameworks
Health belief model (HBM) was mainly attributed as educational design principles underpinned in two education studies (Chen, 2013; Ott, 2018) (Table 5). Chen (2013) referred to the model by presenting the findings according to individuals' perceived susceptibility, perceived severity, perceived barrier and perceived benefits. Ott (2018) also adopted this theory in formulating the educational tool to evaluate its relationship between individual beliefs and application to positive behaviours. Schepens et al. (2011) also assumed two theories in their programmes: the situated learning theory for the authenticity group. It was claimed that knowledge is best learned based on real‐life situations represented through an actual setting, a virtual surrogate or a multimedia presentation. Another Attention–Relevance–Confidence–Satisfaction (ARCS) model in the motivation group used the principle of satisfying learners' fundamental desires or values to drive individuals' motivation. Khong et al. (2017) emphasised the behaviour change wheel theory, an education and adult learning principles embedded in the education programme, including goal setting and developing an interactive presentation to encourage learners' motivation to learn. In contrast, the remaining two studies did not specify any theoretical frameworks underpinning their education designs (Howard et al., 2016; Kamei et al., 2015).
4.5. Quality and appropriateness of fall education programmes
Table 4 shows the metric quality assessment for educational programmes. The majority of the provided education programmes proved to have high quality (Howard et al., 2016; Kamei et al., 2015; Khong et al., 2017; Ott, 2018; Schepens et al., 2011) except one with a moderate quality (Chen, 2013). Unfortunately, Chen (2013) did not report any information on the learning activities and characteristics of the educators or the learners.
All studies had well stated on their educations' purposes and justification for education settings as the first component in the metric assessment. All studies targeted the appropriate audiences but two out of these studies did not elaborate on their learners' knowledge or experience. Five studies and except Chen (2013) described the educators' knowledge, experience in the topic or teaching and involvement in the training prior to the education interventions.
Overall, the educators across five studies had experienced as family/public health nurses, physical therapists and occupational therapists (OTs). Meanwhile, peer educators in peer‐led interventions received a 5‐h training demonstration and lecture. They also went through another 4 h comprised of group works or discussion and mock presentation practice by two different professionals prior to peer educations (Khong et al., 2017). The leading researcher of an OT in Howard et al. (2016) has led and trained the other co‐researchers (a PhD and master students of OT) related to the intervention information. Another OT in Schepens et al. (2011) has received training using vignettes from one of the most accomplished instructional technologist.
In addition, most authors adequately described the process for each learning activity. For example, the estimated duration for the FPE to take place ranges from 30 min to 3 h per session across studies and the sessions have been divided into a few phases. Kamei et al. (2015) adopted a flow diagram to illustrate their teaching and learning activities. Overall, all studies successfully evaluated their older individuals' outcomes for fall prevention awareness or knowledge and behaviour change.
4.6. Nurses' role in collaborating with other professionals
There were only two studies involving nurses as the investigators and delivering education (Kamei et al., 2015; Ott, 2018). The occupational and physical therapists mainly engaged in the educational programmes on fall risk or fall (Howard et al., 2016; Khong et al., 2017; Ott, 2018; Schepens et al., 2011). However, no educator was mentioned in a study (Chen, 2013). The lack of participation among nurses suggested that nurses still had inadequate roles in providing FPE to older adults in the community settings.
5. DISCUSSION
The six articles in this review highlighted that providing FPE promotes older adults' fall risk awareness or knowledge and behaviour change. On the contrary, all studies did not report any association between fall risk awareness or knowledge and fall preventive behaviour. Despite that, theoretical principles supported the relationship of knowledge to behaviour change as demonstrated in numerous studies (Miller, 2010; Ott, 2018; Punlomso et al., 2020).
Howard et al. (2016) reported no significant difference found in fall prevention knowledge among their learners. Demographic findings, education and memory retention were the main contribution to knowledge gain among older adults, especially when their participants only completed elementary schools and came from cross‐cultural communities. Older individuals in Khong et al. (2017) demonstrated a non‐significant knowledge due to irrelevant perception towards at risk of falls. Whereas, added motivation strategies prove to enhance their engagement in behaviour change (Kiyoshi‐Teo et al., 2020).
Using an interactive and familiar activity to conduct FPE may increase the likelihood of older individuals' behaviour participation in the prevention process and learning (Flint et al., 2020). According to Kiyoshi‐Teo et al. (2020), older individuals are keen to participate in fall prevention behaviour if they perceived that their fall risk is modifiable. Most studies included various fall risk topics from personal factors to the modifications of a home environment as supported in other findings (Cerilo, 2016; Chaudhry, 2020).
The included theoretical frameworks underpinned in the selected studies have limited approaches in predicting preventive behaviours. Alternatively, use the protection motivation theory (PMT) to predict protective behaviours (Rogers, 1975; Taheri‐Kharameh et al., 2020). Furthermore, the educational design approach can be improved using a framework of the 4Ps proposed by Kiegaldie and Farlie (2019).
Interestingly, only two studies mentioned the involvement of the nurses as educators or investigators. However, the essential participation of registered nurses, community nurses, public health nurses, nurse assistants and home care nurses are responsible for providing FPE to community older adults, promoting and enhancing their fall risk awareness.
5.1. Limitations
The present research study's limitation was the older subjects were older than 60, only included experimental studies and thus did not include all FPE interventions used in practice. The inclusion of only six studies with some studies that consist of small sample participants may not be generalised to the entire older population.
6. CONCLUSIONS
In this systematic review, FPE adequately serves as one of the fall preventions approaches in enhancing fall risk awareness, knowledge and preventive behaviour change. However, an association between fall risk awareness or knowledge and fall preventive behaviours should require further investigation. The use of theoretical frameworks should be applied in education designs to help improve the educational programme's quality. Nurses are in great potential in planning and providing FPE for older adults in community settings.
6.1. Implications for nursing management
Expand nurses' roles in fall prevention programmes in community settings by using high‐quality and evidence‐based educational tools. Highlight the nurse's role and collaborative management in FPE and prior to this; nurses should equip themselves with knowledge of fall risk factors in older adults. Encourage the use of theoretical frameworks in designing fall prevention programmes for older adults in community settings. Apply motivational strategy combined with various educational techniques when providing FPE to older people.
FUNDING INFORMATION
This research did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors.
AUTHOR CONTRIBUTIONS
MFO, KLS, RS, MWW, MM and KGS made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. MFO, RS, MWW, KLS and MM involved in drafting the manuscript or revising it critically for important intellectual content. MFO, KLS, RS, WWM, MM and KGS gave the final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. MFO, KLS, RS, MWW, MM and KGS agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
ETHICAL APPROVAL
This is a systematic review. However, a registration number has been obtained from the PROSPERO (CRD42021232102).
Supporting information
Table S1. The Assessment of Article Quality Using the TREND Statement
Table S2. The Assessment of Article Quality Using the CONSORT Statement
Ong MF, Soh KL, Saimon R, Wai MW, Mortell M, Soh KG. Fall prevention education to reduce fall risk among community‐dwelling older persons: A systematic review. J Nurs Manag. 2021;29:2674-2688. 10.1111/jonm.13434
Contributor Information
Mei Fong Ong, Email: mfong@unimas.my.
Kim Lam Soh, Email: sklam@upm.edu.my.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available in repository.
REFERENCES
- Azzarello, J. , & Hall, B. (2016). Describing older adults' awareness of fall risk using situation awareness research techniques: A pilot study. Research in Gerontological Nursing, 9(4), 161–166. 10.3928/19404921-20160504-01 [DOI] [PubMed] [Google Scholar]
- Cerilo, P. C. (2016). Effectiveness of fall prevention multimedia program on patient awareness, self‐efficacy, and engagement. University of Phoenix
- Chaudhry, R. (2020). Education on fall risk prevention strategies. (28022610 D.N.P.), Grand Canyon University, Ann Arbor. Retrieved from https://search.proquest.com/docview/2427497219?accountid=40705 ProQuest Dissertations & Theses Global; Publicly Available Content Database database.
- Chen, S. F. (2013). Intervention to prevent falls through health education for elderly in Taiwan. Pakistan Journal of Statistics, 29(5). [Google Scholar]
- Chidume, T. (2021). Promoting older adult fall prevention education and awareness in a community setting: A nurse‐led intervention. Applied Nursing Research, 57, 151392. 10.1016/j.apnr.2020.151392 [DOI] [PubMed] [Google Scholar]
- Des Jarlais, D. , Lyles, C. , Crepaz, N. , & the TREND Group . (2004). Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. American Journal of Public Health, 94, 361–366. 10.2105/AJPH.94.3.361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flint, J. , Morris, M. , Nguyen, A. T. , Keglovits, M. , Somerville, E. K. , Hu, Y.‐L. , & Stark, S. L. (2020). Fall prevention bingo: Effects of a novel community‐based education tool on older adults knowledge and readiness to reduce risks for falls. American Journal of Health Education, 51(6), 406–412. 10.1080/19325037.2020.1822236 [DOI] [Google Scholar]
- Greenberg, S. A. (2020). Falls in older adults: Prevention and assessment of risk in primary care. Advances in Family Practice Nursing, 2, 1–9. 10.1016/j.yfpn.2019.12.001 [DOI] [Google Scholar]
- Harrison, B. E. (2017). Fall prevention program in the community: A nurse practitioner's contribution. The Journal for Nurse Practitioners, 13(8), e395–e397. 10.1016/j.nurpra.2017.06.017 [DOI] [Google Scholar]
- Heng, H. , Jazayeri, D. , Shaw, L. , Kiegaldie, D. , Hill, A.‐M. , & Morris, M. E. (2020). Hospital falls prevention with patient education: A scoping review. BMC Geriatrics, 20(1), 140. 10.1186/s12877-020-01515-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins, J. P. T. , Altman, D. G. , Gøtzsche, P. C. , Jüni, P. , Moher, D. , Oxman, A. D. , Sterne, J. A. C. , & etal . (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ, 343, d5928. 10.1136/bmj.d5928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill, A. M. , Etherton‐Beer, C. , McPhail, S. M. , Morris, M. E. , Flicker, L. , Shorr, R. , & Haines, T. (2017). Reducing falls after hospital discharge: A protocol for a randomised controlled trial evaluating an individualised multimodal falls education programme for older adults. BMJ Open, 7(2), e013931. 10.1136/bmjopen-2016-013931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill, A.‐M. , McPhail, S. M. , Francis‐Coad, J. , Waldron, N. , Etherton‐Beer, C. , Flicker, L. , & Haines, T. P. (2015). Educators' perspectives about how older hospital patients can engage in a falls prevention education programme: A qualitative process evaluation. BMJ Open, 5(12), e009780. 10.1136/bmjopen-2015-009780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howard, B. S. , Beitman, C. L. , Walker, B. A. , & Moore, E. S. (2016). Cross‐cultural educational intervention and fall risk awareness. Physical and Occupational Therapy in Geriatrics, 34(1), 1–20. 10.3109/02703181.2015.1105344 [DOI] [Google Scholar]
- Kamei, T. , Kajii, F. , Yamamoto, Y. , Irie, Y. , Kozakai, R. , Sugimoto, T. , Niino, N. , et al. (2015). Effectiveness of a home hazard modification program for reducing falls in urban community‐dwelling older adults: A randomized controlled trial. Japan Journal of Nursing Science, 12(3), 184–197. 10.1111/jjns.12059 [DOI] [PubMed] [Google Scholar]
- Khong, L. A. M. , Berlach, R. G. , Hill, K. D. , & Hill, A. M. (2017). Can peer education improve beliefs, knowledge, motivation and intention to engage in falls prevention amongst community‐dwelling older adults? European Journal of Ageing, 14(3), 243–255. 10.1007/s10433-016-0408-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiegaldie, D. & Farlie, M (2019). Using education interventions in falls research: A framework for evidence‐based education design. Retrieve from https://holmesglen.intersearch.com.au/holmesglencrisjspui/handle/20.500.11800/172
- Kim, S. Y. , Park, J. E. , Lee, Y. J. , Seo, H. J. , Sheen, S. S. , Hahn, S. , Jang, B. H. , & Son, H. J. (2013). Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. Journal of Clinical Epidemiology, 66(4), 408–414. 10.1016/j.jclinepi.2012.09.016 [DOI] [PubMed] [Google Scholar]
- King, B. , Pecanac, K. , Krupp, A. , Liebzeit, D. , & Mahoney, J. (2018). Impact of fall prevention on nurses and care of fall risk patients. The Gerontologist, 58(2), 331–340. 10.1093/geront/gnw156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiyoshi‐Teo, H. , Northrup‐Snyder, K. , Robert Davis, M. , Garcia, E. , Leatherwood, A. , & Izumi, S. (2020). Qualitative descriptions of patient perceptions about fall risks, prevention strategies and self‐identity: Analysis of fall prevention motivational interviewing conversations. Journal of Clinical Nursing, 29(21–22), 4281–4288. 10.1111/JOCN.15465 [DOI] [PubMed] [Google Scholar]
- Kuhirunyaratn, P. , Prasomrak, P. , & Jindawong, B. (2019). Effects of a health education program on fall risk prevention among the urban elderly: A quasi‐experimental study. Iranian Journal of Public Health, 48(1), 103‐111. PMCID: PMC6401575 [PMC free article] [PubMed] [Google Scholar]
- Loganathan, A. , Ng, C. J. , Tan, M. P. , & Low, W. Y. (2015). Barriers faced by healthcare professionals when managing falls in older people in Kuala Lumpur, Malaysia: A qualitative study. BMJ Open, 5(11), e008460. 10.1136/bmjopen-2015-008460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mihaljcic, T. , Haines, T. P. , Ponsford, J. L. , & Stolwyk, R. J. (2015). Self‐awareness of falls risk among elderly patients: Characterizing awareness deficits and exploring associated factors. Archives of Physical Medicine and Rehabilitation, 96(12), 2145–2152. 10.1016/j.apmr.2015.08.414 [DOI] [PubMed] [Google Scholar]
- Miller, K. S. (2010). Older adults' perceptions of fall‐prevention education: A qualitative study. Western Carolina University. [Google Scholar]
- Minnier, W. , Leggett, M. , Persaud, I. , & Breda, K. (2019). Four smart steps: Fall prevention for community‐dwelling older adults. Creative Nursing, 25(2), 169–175. 10.1891/1078-4535.25.2.169 [DOI] [PubMed] [Google Scholar]
- Moher, D. , Hopewell, S. , Schulz, K. , Montori, V. , Gøtzsche, P. , Devereaux, P. , for the CONSORT Group ., et al. (2010). CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trial. BMJ , 340(c869). doi: 10.1136/bmj.c869 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moher, D. , Liberati, A. , Tetzlaff, J. , & Altman, D. G. (2010). Preferred reporting items for systematic reviews and meta‐analyses: The PRISMA statement. International Journal of Surgery, 8(5), 336–341. 10.1016/j.ijsu.2010.02.007 [DOI] [PubMed] [Google Scholar]
- Ott, L. D. (2018). The impact of implementing a fall prevention educational session for community‐dwelling physical therapy patients. Nursing Open, 5(4), 567–574. 10.1002/nop2.165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Punlomso, S. , Srimuang, P. , & Tudpor, K. (2020). Fall prevention by Otago exercise program based on health belief model in community‐dwelling older persons. Indian Journal of Physiotherapy & Occupational Therapy, 14(1), 245–252. 10.5958/0973-5674.2020.00044.1 [DOI] [Google Scholar]
- Rogers, R. W. (1975). A protection motivation theory of fear appeals and attitude change. The Journal of Psychology, 91(1), 93–114. 10.1080/00223980.1975.9915803 [DOI] [PubMed] [Google Scholar]
- Schepens, S. L. , Panzer, V. , & Goldberg, A. (2011). Randomized controlled trial comparing tailoring methods of multimedia‐based fall prevention education for community‐dwelling older adults. American Journal of Occupational Therapy, 65(6), 702–709. 10.5014/ajot.2011.001180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taheri‐Kharameh, Z. , Bashirian, S. , Heidarimoghadam, R. , Poorolajal, J. , Barati, M. , & Rásky, É. (2020). Predictors of fall protective behaviors among Iranian community‐dwelling older adults: An application of the protection motivation theory. Clinical Interventions in Aging, 15, 123–129. 10.2147/CIA.S224224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uymaz, P. E. , & Nahcivan, N. O. (2016). Evaluation of a nurse‐led fall prevention education program in Turkish nursing home residents. Educational Gerontology, 42(5), 299–309. 10.1080/03601277.2015.1109403 [DOI] [Google Scholar]
- Williams, M. E. , & Hadler, N. M. (2015). In hospital rehabilitation units, adding individualized fall‐prevention education to usual care reduced falls. Annals of Internal Medicine, 163(4), JC13. 10.7326/ACPJC-2015-163-4-013 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. The Assessment of Article Quality Using the TREND Statement
Table S2. The Assessment of Article Quality Using the CONSORT Statement
Data Availability Statement
The data that support the findings of this study are openly available in repository.