

Abstract
Background
Executive functioning (EF) varies in children with autism spectrum disorder (ASD) and is associated with clinical symptoms, academic, and adaptive functioning. Here, we examined whether middle‐childhood EF mediates associations between early‐childhood autism symptoms and adolescent outcomes in children with ASD.
Methods
The Pathways in ASD Cohort comprising children recruited at the time of ASD diagnosis (at 2–4 years‐of‐age) and followed prospectively across eight subsequent timepoints over ~10 years was used. A subset of Pathways participants (n = 250) with Behavior Rating Inventory of Executive Function (BRIEF)‐Parent Form data from at least one timepoint when participants were school‐aged was analyzed. A mediation framework was used to examine whether BRIEF‐measured EF across age 7–10 years (middle‐childhood) mediated associations between early‐childhood autism symptoms (measured using the parent‐report Social Responsiveness Scale across age 2–6 years) and clinical, academic, and functional outcomes, indexed at age >10–11.8 years (early‐adolescence) using the Child Behavior Checklist (CBCL)‐Internalizing and Externalizing Scales, Academic Performance from the Teacher's Report Form, and Vineland Adaptive Behavior Scales. Models were rerun substituting clinician‐rated and teacher‐rated measures, where possible.
Results
Mediation models indicated a significant indirect effect of middle‐childhood EF on associations between early‐childhood autism symptoms and externalizing behavior, academic performance, or adaptive functioning in early adolescence; kappa squared (κ2) effect sizes ranged from large to small. Model findings were stable across raters. Middle‐childhood EF did not mediate associations between early‐childhood autism symptoms and adolescent internalizing behavior.
Conclusions
Among children with an ASD diagnosis, middle‐childhood EF may be one pathway through which early‐childhood autism symptoms influence a variety of outcomes in early‐adolescence. An experimental study targeting middle‐childhood EF to improve adolescent academic, emotional/behavioral, and adaptive functioning is needed to evaluate the clinical meaningfulness of these findings.
Keywords: Executive function, autism spectrum disorder, academic performance, adaptive functioning, mental health, internalizing/externalizing behavior, longitudinal studies
Introduction
The clinical presentations and long‐term outcomes of autism spectrum disorder (ASD) are highly variable (Howlin & Moss, 2012). A recent priority setting initiative indicated that improvement of mental health, educational, and everyday performance outcomes are top research priorities identified by the autism communities (https://www.jla.nijr.ac.uk). General intellectual ability and early autism symptom severity have each been linked to longitudinal outcomes in ASD (e.g., adaptive functioning, independence, IQ; Bal, Kim, Cheong, & Lord, 2015; Eaves & Ho, 2008; Howlin, Goode, Hutton, & Rutter, 2004; Szatmari, Bryson, Boyle, Streiner, & Duku, 2003). However, recent findings suggest that these variables (measured in early‐ to middle‐childhood) may be better predictors of adult cognitive and functional outcomes than mental health outcomes (i.e. depressive symptoms, negative emotions; Pickles, McCauley, Pepa, Huerta, & Lord, 2020). This study examined whether executive functioning (EF) skills may influence priority outcomes for the autism communities, underscoring the importance of this domain for interventional research and to inform care.
Executive functioning is an important component of cognitive ability that predicts later academic performance, mental, and physical health in typically developing children (Diamond, 2013). In community samples, EF skills in early‐ and middle‐childhood predict later math and literacy skills (Blair, Raver, & Finegood, 2016; Cameron et al., 2012), school performance (Diamantopoulou, Rydell, Thorell, & Bohlin, 2007), externalizing (hyperactivity, oppositionality, conduct/peer problems; Belsky, Pasco Fearon, & Bell, 2007; Sulik, Blair, Mills‐Koonce, Berry, & Greenberg, 2015), and internalizing (anxiety, depression) behaviors (Kertz, Belden, Tillman, & Luby, 2016; Nelson et al., 2018). Evidence also suggests that EF may be one pathway through which early life factors, such as socioeconomic status, maternal depression, and parenting factors contribute to educational achievement and externalizing behaviors in typical development (Albert et al., 2020; Roman, Ensor, & Hughes, 2016; Sulik et al., 2015).
Three main EF subcomponents include: (a) inhibition (self/interference control), (b) set‐shifting (shifting between topics/mental sets), and (c) working memory (retaining/manipulating information over time; Diamond, 2013; Miyake et al., 2000; Pellicano, 2012). A recent meta‐analysis of ASD‐control differences found evidence for a global EF deficit in ASD that is present throughout development (Demetriou et al., 2018). The Behavior Rating Inventory of Executive Function (BRIEF) was developed as an ecologically valid measure of everyday EF performance (Gioia, Isquith, Guy, & Kenworth, 2000). Cross‐sectional studies in ASD have demonstrated associations between BRIEF‐measured EF with: (a) autism symptoms (Leung, Vogan, Powell, Anagnostou, & Taylor, 2016; Torske, Naerland, Oie, Stenberg, & Andreassen, 2017), (b) adaptive functioning (Gilotty, Kenworthy, Sirian, Black, & Wagner, 2002; Pugliese et al., 2015), (c) internalizing symptoms (Gardiner & Iarocci, 2018; Wallace et al., 2016), and (d) learning behaviors (e.g. learning attitudes, task persistence, flexibility; Rosello, Berenguer, Baixauli, Colomer, & Miranda, 2018). A retrospective cohort study also found that earlier measurement of metacognitive skills (a BRIEF‐EF sub‐domain) in children with ASD contributed uniquely to the variance in later measured adaptive functioning, beyond IQ effects (Pugliese et al., 2016). BRIEF‐measured set‐shifting has also been found to mediate the relation between ASD (vs. ADHD) diagnostic status and anxious/depressed behaviors in a cross‐sectional study of children and youth (Lawson et al., 2015).
While the aforementioned literature provides evidence that EF in ASD is associated with clinical symptoms, academic, and everyday performance, less is known about plausible temporal relations between these variables. Drawing on a large inception cohort of preschool children followed prospectively from the time of ASD diagnosis (at 2–4 years) into early adolescence, this study examined whether relations between early‐childhood autism symptoms (measured across age 2–6 years) and priority outcomes (mental health symptoms, academic performance, and adaptive functioning) measured in early‐adolescence (at age greater than 10 to less than 12 years) may be mediated by middle‐childhood EF (measured at age 7–10 years). We tested the hypothesis that, in ASD, EF in middle‐childhood may be one pathway through which early autism symptom severity contributes to adolescent mental health, academic, and everyday performance outcomes.
Methods
Participants
Participants were part of a Canadian multisite longitudinal study (http://www.asdpathways.ca; n = 421) recruited at a single timepoint and assessed longitudinally at five ASD referral centers (Halifax, Nova Scotia; Montreal, Quebec; Hamilton, Ontario; Edmonton, Alberta; Vancouver, British Columbia). Inclusion was based on: (a) age 2–4 years, 11 months and (b) clinical diagnosis of ASD assigned by a clinician using DSM‐IV criteria within 4 months of enrollment, confirmed using the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2012) and the Autism Diagnostic Interview–Revised (Rutter, LeCouteur, & Lord, 2003). Exclusion criteria included: (a) cerebral palsy or other neuromotor disorder, (b) severe vision or hearing impairment interfering with study participation, (c) known genetic or chromosomal abnormality. One child per family could be recruited (Mirenda et al., 2010). Participants were assessed across eight timepoints: time of ASD diagnosis (T1), 6 months post‐T1 (T2), 12 months post‐T1 (T3), at age 6 years (T4), with subsequent assessments (T5–T8) scheduled ~12 months after the preceding one (see Figure 1, Table S1). This study included 250 children from the Pathways sample for which BRIEF–Parent Form data during middle‐childhood (T5–T7; Table 1), as well as any predictor or outcome variable of interest (see below) were available.
Figure 1.
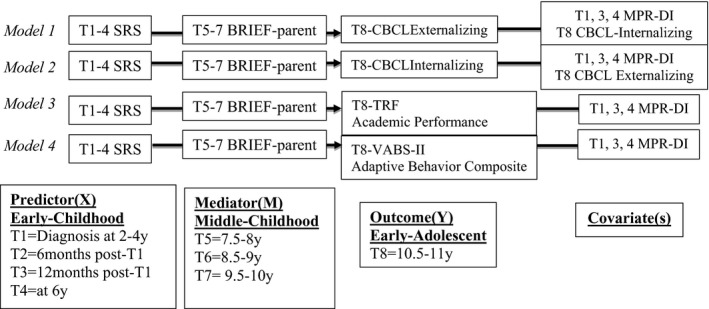
Primary mediation models examined
Table 1.
Sample characteristics across timepoints
| Time | N | Variables | Mean ± SD |
|---|---|---|---|
| 1 | 250 | Number/Percent male | 211 (84.4%) |
| 250 | Age (months) | 40.65 ± 9.0 | |
| 248 | ADOS calibrated severity score | 7.66 ± 1.69 | |
| 215 | MPR developmental index | 59.55 ± 24.90 | |
| 246 | VABS adaptive behavior composite | 73.44 ± 10.41 | |
| 237 | CBCL internalizing T‐score | 59.74 ± 9.27 | |
| 237 | CBCL externalizing T‐score | 55.88 ± 10.1 | |
| 1–4 | 249 | SRS T‐score | 73.26 ± 12.64 |
| 248 | RBS‐R total score | 22.92 ± 16.12 | |
| 5–7 | 250 | BRIEF‐BRI T‐score | 59.05 ± 11.55 |
| 249 | BRIEF‐MCI T‐score | 59.26 ± 11.51 | |
| 8 | 192 | Number/Percent male | 165 (84.4%) |
| 192 | Age (months) | 129.15 ± 3.0 | |
| 158 | CBCL internalizing T‐score | 53.23 ± 10.51 | |
| 158 | CBCL externalizing T‐score | 50.33 ± 11.11 | |
| 120 | TRF academic performance T‐Score | 41.03 ± 8.14 | |
| 181 | VABS adaptive behavior composite | 76.20 ± 16.21 |
Ethical considerations
All study procedures were approved by the Hamilton Integrated Research Ethics Board (REB; project number 04‐353, McMaster University) and each participating site REB. Written informed consent was obtained from all participating families.
Measures
Mediator variable—middle‐childhood (T5–7)
Executive functioning was indexed using the 86‐item BRIEF parent‐report or teacher‐report versions. The Behavior Regulation Index (BRI), derived from the inhibit, shift/flexibility, and emotional control subscales and Metacognition Index (MCI), derived from the initiate, working memory, plan/organize, organization of materials, and monitor subscales were used to capture two EF subdomains. Standardized T‐scores were used (over raw scores) to account for variability in age across assessment timepoints.
Predictor variables—early‐childhood (T1–4)
Autistic symptoms were indexed using: the Social Responsiveness Scale (SRS) Parent‐Report Form total T‐score (Bölte, Poustka, & Constantino, 2008; Constantino et al., 2003) and the Calibrated Severity Score (Gotham, Pickles, & Lord, 2009) of the ADOS, which provided an alternate (non‐parent‐report, interview‐based) measure of autistic symptoms (Venker, Ray‐Subramanian, Bolt, & Ellis Weismer, 2014). The Repetitive Behaviors Scale–Revised (RBS‐R), a parent‐report measure, was used to examine repetitive behaviors (Bodfish, Symons, Parker, & Lewis, 2000).
Outcome variables—early‐adolescence (T8)
The Child Behavior Checklist 6–18 (CBCL; Achenbach & Rescorla, 2001) and Teacher Report Form 6–18 (TRF) Externalizing and Internalizing scales provided a parent‐ or teacher‐reported index of mental health symptoms, respectively. Internalizing T‐scores were derived from Anxious/Depressed, Withdrawn‐Depressed, and Somatic Complaints subscales. Externalizing T‐scores were derived from Rule‐Breaking and Aggressive Behavior subscales. The TRF Academic Performance Scale provided a real‐world measure of grade‐level academic functioning. Adaptive functioning was indexed from the Adaptive Behavior Composite (ABC) of the Vineland Adaptive Behavior Scale, Second Edition (a clinician‐administered caregiver‐report; VABS‐II; Sparrow, Cicchetti, & Balla, 2005).
Covariate
The Merrill‐Palmer–Revised Developmental Index (MPR‐DI), available at T1, T3, and T4 (Dempsey et al., 2020; Roid & Sampers, 2004) was selected as a proxy for general intellectual/cognitive ability (Dempsey et al., 2020).
Analytic plan
Evaluation of missing data
Participants that were included versus excluded from the original baseline sample due to missing data were compared across variables of interest. Little's MCAR test (Little, 1988) was used to evaluate the type of missingness present for the current subsample of the original baseline sample (Hughes, Heron, Sterne, & Tilling, 2019; Lewin, Brondeel, Benmarhnia, Thomas, & Chaix, 2018; Sterne et al., 2009).
Initial analysis
Zero‐order correlations were run among analyzed variables (Table 2). Sequential multivariable regressions were run to examine the relative importance of early‐childhood RBS‐R and SRS on middle‐childhood BRIEF‐BRI/MCI and of middle‐childhood BRIEF‐BRI/MCI on early‐adolescent CBCL‐internalizing/externalizing, TRF Academic Performance, and VABS‐II ABC scores.
Table 2.
Zero‐order correlations between predictor, mediator, outcome, and covariates (sample size included below each correlation, **p = .01, *p = .05)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. MPR‐DI (T1, 3, 4) | − | −.15* | −.04 | −.04 | .03 | .18* | −.04 | .59** | .65** | −.23** |
| 233 | 232 | 234 | 233 | 151 | 151 | 113 | 172 | 234 | ||
| 2. SRS (T1–4) | ‐ | .67** | .63** | .55** | .38** | .48** | −.34** | −.46** | .19** | |
| 248 | 249 | 248 | 158 | 158 | 119 | 181 | 249 | |||
| 3. RBS‐R (T1–4) | ‐ | .60** | .41** | .39** | .51** | −.29** | −.34** | .07 | ||
| 248 | 247 | 158 | 158 | 119 | 181 | 248 | ||||
| 4. BRIEF‐BRI (T5–7) | ‐ | .76** | .45** | .59** | −.17 | −.33** | .18 | |||
| 249 | 158 | 158 | 120 | 182 | 250 | |||||
| 5. BRIEF‐MCI (T5–7) | ‐ | .41** | .42** | −.31** | −.27** | .15* | ||||
| 157 | 157 | 119 | 181 | 249 | ||||||
| 6. Internalizing (T8) | ‐ | .67** | −.08 | −.15 | .09 | |||||
| 158 | 104 | 154 | 158 | |||||||
| 7. Externalizing (T8) | ‐ | −.13 | −.27** | .21** | ||||||
| 104 | 154 | 158 | ||||||||
| 8.TRFAcademic (T8) | ‐ | .55** | −.27** | |||||||
| 111 | 120 | |||||||||
| 9. VABS ABC (T8) | ‐ | −.29** | ||||||||
| 182 | ||||||||||
| 10. ADOS | ‐ | |||||||||
Analysis of indirect effects
We first tested the hypothesis that middle‐childhood EF would mediate associations between early‐childhood ASD symptoms and early‐adolescent emotional/behavioral, academic, and functional outcomes (Figure 1) using mainly parent‐rated measures that were selected a priori based on prior relations found between BRI/MCI and SRS total score (Leung et al., 2016; Torske et al., 2017), BRI and externalizing/internalizing (Lawson et al., 2015), and MCI with learning behaviors (Rosello et al., 2018), or adaptive functioning (Pugliese et al., 2016). Two models examined the indirect effect of middle‐childhood BRIEF‐BRI (parent‐report) on the associations between early‐childhood SRS and early‐adolescent CBCL‐externalizing (Model 1) or internalizing (Model 2) scores. Two models examined the indirect effect of middle‐childhood BRIEF‐MCI (parent‐report) on the associations between early‐childhood SRS and early‐adolescent TRF Academic Performance (Model 3) or VABS‐II ABC (Model 4). The MPR‐DI composite was included in each model as a covariate to control for the effects of general cognitive ability on variables of interest (Havdahl et al., 2016). Given the high intercorrelation of internalizing and externalizing behaviors, the alternate variable was also included as a covariate in Models 1 and 2 (Achenbach, Ivanova, Rescorla, Turner, & Althoff, 2016).
Stability of indirect effects across raters/measurement(s)
We undertook a second set of mediation models that tested the same theoretical model after substituting original measures used (above) for measures completed by alternate raters and in different settings (where possible), to control for common method variance in the original mediation models tested (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). Models where significant indirect effects were found were rerun substituting: clinician‐administered ADOS Calibrated Severity Score for parent‐report SRS as the predictor variable, and teacher‐report versus parent‐report BRIEF‐BRI/MCI as the mediator variable. TRF‐internalizing/externalizing scores were also used instead of parent‐report CBCL scores. Other outcome measures remained the same due to lack of alternate measures for substitution (Figure S1).
Mediation in a regression framework
Mediation models were estimated using the bootstrap method of inference (Fritz & Mackinnon, 2007; Hayes, 2009, 2017) chosen over the causal steps approach based on a number of criticisms, including that preconditions for mediation testing with the causal steps approach (e.g. significant direct effect of X on Y needed for mediation testing) may lead to type II error (Hayes, 2017; Meule, 2019). Using the bootstrap method of inference, the indirect effect was tested for each model regardless of the significance of the direct effect. A significant indirect effect was inferred when the confidence interval did not include zero (tested using bootstrapping at 5,000 resamples). SPSS v25 was used for all analyses. Bootstrapping mediation analyses were conducted using the PROCESS macro v3.2 for SPSS (www.processmacro.org; Hayes, 2017). For each significant mediation model, kappa squared (κ2) was calculated for a basic model with no covariates. The κ2 metric (range = 0–1) expresses the indirect effect as a ratio between the observed effect and the maximum possible indirect effect that could have been found given the study design (κ2 of .01, .09, .25 indicative of small, medium, large mediation effects, respectively; Preacher & Kelley, 2011).
Post‐hoc sensitivity analyses
As early‐childhood SRS scores may be contaminated by behavioral problems (Havdahl et al., 2016) and due to potential item overlap across BRIEF‐BRI and CBCL‐externalizing, based on strong correlations across measures (Table 2), sensitivity analyses were run to examine whether mediation effects remained after controlling for covariance between early‐childhood internalizing/externalizing (CBCL‐measured) and SRS, and between middle‐childhood EF and early‐adolescent externalizing symptoms. Sensitivity analyses were also run to examine whether mediation effects remained for Model 1 when early‐childhood RBS‐R was used in place of SRS as the predictor variable, and whether specific BRI subdomains (inhibition, emotional control, set‐shifting) accounted for Model 1 mediation effects.
Results
Missing data
The analyzed sample (Table 1) differed from the full Pathways baseline sample on SES (Table S2), enrollment age (mean in months, included = 40.65/excluded = 38.74; t = −2.14, p = .03), and on the MPR‐DI (mean included = 59.55/excluded = 52.21; t = −2.54, p = .01). Other variables of interest did not differ significantly in the complete versus baseline sample. Missingness for each assessment timepoint varied from 4.8% (RBS‐R) to 52.0% (TRF Academic Performance). Little's MCAR test (Little, 1988) was nonsignificant, indicating that missingness appeared to be consistent with the missing‐completely‐at‐random(MCAR) category (χ2 (1601) = 1,614.1, p = .4). Complete case analysis was therefore deemed appropriate (as complete cases should provide an unbiased representative subsample of the baseline sample) and was selected over multiple imputation (Hughes et al., 2019; Lewin et al., 2018; Sterne et al., 2009).
Initial analysis
We found moderate to strong correlations (Table S3) among measures administered repeatedly across early‐ (T1–4) and middle‐childhood (T5–7) timepoints. To obtain more stable estimates of constructs of interest, we averaged data across timepoints to create early‐ or middle‐childhood composite measures for predictor, mediator, and covariates used in our models. In the event of missing data for a single timepoint, the composite was calculated using data from available timepoints. See Tables S4–S9 for results of sequential multivariable regression analyses.
Indirect effects
Of the four models that tested for mediation, mainly using parent‐report measures, models 1, 3, and 4 were significant (see Table 3). Model 1 indicated a statistically significant indirect effect of middle‐childhood EF (BRIEF‐BRI) on the association between early‐childhood autism symptoms and early‐adolescent externalizing behaviors (β = .15, 95% CI [0.07, 0.23], κ2 = .27; large effect). Models 3 and 4 indicated a significant indirect effect of middle‐childhood EF (BRIEF‐MCI) on the associations between early‐childhood autism symptoms and either early‐adolescent academic performance (Model 3: β = −.19, 95% CI [−0.29, −0.09]; κ2 = .09, moderate effect) or adaptive functioning (Model 4: β = −.07, 95% CI [−0.14, −0.01]; κ2 = .02, small effect). No significant mediation effect for middle‐childhood EF on the association between early autism symptoms and adolescent internalizing behavior was found (Model 2: β = .01, 95% CI [−0.05, 0.08]).
Table 3.
Mediational model regression results summary
| Model 1 (n = 151; MPR‐DI composite, T8 CBCL Internalizing covaried) | |||||
|---|---|---|---|---|---|
| Path | b (SE) | β | t | p | |
| Total effect | C | 0.24 (0.06) | 0.24 | 3.68 | .003 |
| Direct effect | C’ | 0.09 (0.07) | 0.09 | 1.31 | .19 |
| SRS (X) on BRI (M) | A | 0.45 (0.07) | 0.47 | 6.54 | <.001 |
| BRI (M) on Externalizing (Y) | B | 0.33 (0.07) | 0.31 | 4.51 | <.001 |
| Indirect effect of SRS on Externalizing (path A × B) | |||||
| Unstandardized | Completely standardized | ||||
| b (Boot SE) | Boot CI (LL, UL) | β (Boot SE) | Boot CI (LL, UL) | ||
| Bootstrapping | 0.15 (0.04) | 0.07, 0.24 | 0.15 (0.04) | 0.07, 0.23 | |
| Model 2 (n = 151; MPR‐DI composite, T8 CBCL Externalizing covaried) | |||||
|---|---|---|---|---|---|
| Path | b (SE) | β | t | p | |
| Total effect | C | 0.10 (0.06) | 0.11 | 1.57 | .12 |
| Direct effect | C′ | 0.09 (0.07) | 0.09 | 1.27 | .21 |
| SRS (X) on BRI (M) | A | 0.36 (0.07) | 0.38 | 5.46 | <.001 |
| BRI (M) on Internalizing (Y) | B | 0.03 (0.08) | 0.03 | 0.39 | .70 |
| Indirect effect of SRS on Internalizing (path A × B) | |||||
| Unstandardized | Completely standardized | ||||
| b (Boot SE) | Boot CI (LL, UL) | β (Boot SE) | Boot CI (LL, UL) | ||
| Bootstrapping | 0.01 (0.03) | −0.05, 0.07 | 0.01 (0.03) | −0.05, 0.08 | |
| Model 3 (n = 111; MPR‐DI composite covaried) | |||||
|---|---|---|---|---|---|
| Path | b (SE) | β | t | p | |
| Total effect | C | −0.11 (0.05) | −0.16 | −2.13 | .04 |
| Direct effect | C′ | −0.02 (0.06) | −0.03 | −0.31 | .76 |
| SRS (X) on MCI (M) | A | 0.52 (0.07) | 0.58 | 7.04 | <.001 |
| MCI (M) on Academic (Y) | B | −0.24 (0.06) | −0.33 | −3.90 | .002 |
| Indirect effect of SRS on Academic Performance (path A × B) | |||||
| Unstandardized | Completely standardized | ||||
| b (Boot SE) | Boot CI (LL, UL) | β (Boot SE) | Boot CI (LL, UL) | ||
| Bootstrapping | −0.13 (0.03) | −0.20, −0.06 | −0.19 (0.05) | −0.29, −0.09 | |
| Model 4 (n = 170; MPR‐DI composite covaried) | |||||
|---|---|---|---|---|---|
| Path | b (SE) | β | t | p | |
| Total effect | C | −0.35 (0.06) | −0.30 | −5.43 | <.001 |
| Direct effect | C′ | −0.27 (0.07) | −0.23 | −3.70 | .003 |
| SRS (X) on MCI (M) | A | 0.47 (0.07) | 0.49 | 7.11 | <.001 |
| MCI (M) on VABS‐II ABC (Y) | B | −0.17 (0.07) | −0.14 | −2.32 | .02 |
| Indirect effect of SRS on VABS‐II ABC (path A × B) | |||||
| Unstandardized | Completely standardized | ||||
| b (Boot SE) | Boot CI (LL, UL) | β (Boot SE) | Boot CI (LL, UL) | ||
| Bootstrapping | −0.08 (0.04) | −0.15, −0.01 | −0.07 (0.03) | −0.14, −0.01 | |
Stability of indirect effects
When significant mediation effects (Models 1, 3, 4) were retested after substituting measures completed by alternate raters, models 1, 3, and 4 remained significant with similar effect sizes found overall (Model 1: β = .08, 95% CI [0.02, 0.17]; κ2 = .12; Model 3: β = −.09, 95% CI [−0.17, −0.03]; κ2 = .12; Model 4: β = −.06, 95% CI [−0.11, −0.02]; κ2 = .08, Tables S10–S13).
Post‐hoc sensitivity analyses
The same patterns of significance remained across sensitivity analyses. A significant indirect effect of middle‐childhood BRIEF‐BRI on the association between early‐childhood repetitive behaviors and early‐adolescent externalizing symptoms was found, and of middle‐childhood EF on the association between early‐childhood autism symptoms and early‐adolescent externalizing symptoms remained when BRIEF‐inhibit or emotional control subscales were used in place of the BRI, but not the set‐shifting subscale (See Tables S13–S20).
Discussion
In a large inception cohort of newly diagnosed preschoolers with ASD that were followed prospectively over a ~10‐year period, this study suggests that EF in middle‐childhood may be one pathway through which early‐childhood autism symptoms associate with early‐adolescent mental health, academic, and everyday performance outcomes in children with ASD.
In this study, middle‐childhood behavior regulation mediated the association between early‐childhood autism symptoms and early‐adolescent externalizing (but not internalizing) behavior (Model 1). It is important to note that although large effect sizes were found for the main model examined, more moderate effect sizes were found for substitution and sensitivity model analyses that controlled for common method variance and baseline externalizing behaviors, respectively. As in typical development, our results indicate that stronger middle‐childhood EF in ASD may buffer against development of externalizing symptoms (Sulik, 2017). Our study suggests that this effect may be based on relations between inhibitory and emotional control on behavioral regulation (Compas, Connor‐Smith, Saltzman, Thomsen, & Wadsworth, 2001) and that the same mediation effect is present for the relation between early‐childhood repetitive behaviors (as a subdomain of ASD symptoms) and adolescent externalizing behavior. Our longitudinal findings differ from a prior cross‐sectional study that found an indirect effect of BRIEF‐measured shift/flexibility skills on the relation between having an ASD (vs. ADHD) diagnosis and CBCL‐measured anxious/depressed behaviors in children and youth (Lawson et al., 2015). Differences in our results may stem from the longitudinal nature of our study or the younger upper age limit of our sample upon outcome measurement. A recent Pathways in ASD cohort study found evidence for subgroups of children with different developmental trajectories for both insistence on sameness and anxiety symptoms (that were associated but incongruous in a third of participants; Baribeau et al., 2020). These findings suggest that analyses accounting for heterogeneity of associations over development may be needed to better understand predictors of internalizing symptoms in children diagnosed with ASD as toddlers.
Our results also indicated the presence of a significant indirect effect of the BRIEF metacognitive domain on the relations between early‐childhood autism symptoms and early‐adolescent academic performance or adaptive functioning in our sample, with medium and small effect sizes found, respectively. In typical development, longitudinal studies have linked EF with later academic achievement and general school functioning (Cameron et al., 2012; Diamantopoulou et al., 2007; McClelland et al., 2007; Séguin, Boulerice, Harden, Tremblay, & Pihl, 1999). In prior work in ASD, BRIEF metacognitive skills (e.g. monitoring, planning, working memory) have been shown to influence academic/everyday performance (Gardiner & Iarocci, 2018; Gilotty et al., 2002; McLean, Harrison, Zimak, Joseph, & Morrow, 2014; Pugliese et al., 2015), potentially by affecting motivation and willingness to engage and persist to task completion (Rosello et al., 2018).
This study has a number of strengths and limitations. First, the rich participant characterization available in the Pathways sample enabled us to demonstrate that our mediation results were stable across different raters and measurement tools. However, due to missing data, only a subsample (~60%) of the original cohort could be examined, with higher attrition for some models (e.g. those relying on teacher ratings). Second, mediation models are based on strong assumptions about the directionality of associations. While the models applied to our temporally organized longitudinal data support our hypothesized mechanistic flow of effects, early‐childhood EF was not measured in the Pathways cohort. A recent study using developmentally sensitive EF tests provides evidence of a global EF deficit that is present in preschoolers with ASD (Garon, Smith, & Bryson, 2018). Based on prior longitudinal studies in ASD, an early neurodevelopmental event that causes large‐scale alterations in cortical development affecting multiple neural networks (Hazlett et al., 2017) may contribute to both the emergence of ASD symptoms in early life as well as EF deficits that become more prominent over time (Garon, Bryson, & Smith, 2008). Moreover, parent/teacher‐rated and performance‐based EF are weakly correlated and may measure different aspects of EF (Toplak, West, & Stanovich, 2013). Moderate to large correlations were found among many of the variables included in this study. Further, additional variables that were not explored here may also influence behavioral outcomes in ASD (Tormala, Falces, Brinol, & Petty, 2007), such as socio‐economic factors (Lansford et al., 2019). Thus, future work building on the present findings and evaluating their clinical impact in an experimental framework would benefit from multimodal measurement of each of the constructs of interest, across timepoints, including measurement of additional related variables (e.g. SES) that may influence outcomes. Finally, although use of the large Pathways inception cohort suggests that our findings are translatable to the general population of children diagnosed with ASD in early life, findings may not be generalizable to some girls on the autism spectrum or more subtly affected children who are diagnosed later in life.
Conclusions
This is the first longitudinal study in participants with ASD indicating that middle‐childhood EF may mediate associations between early‐childhood autism symptoms and multiple functional outcomes in early‐adolescence. The potential clinical implications of our findings are that interventions that target middle‐childhood EF may improve adolescent outcomes in autistic children. Our work provides insight into the potential pathways through which very early ASD symptom intervention (e.g. in at‐risk children; Green et al., 2017) or childhood EF training in ASD (Kenworthy et al., 2014) could mitigate developmental risk for impairment across a variety of priority outcomes later in life. An experimental interventional study targeting middle‐childhood EF in an effort to improve adolescent academic, emotional/behavioral, and adaptive functioning is now needed to evaluate the clinical meaningfulness of our findings.
Key points.
Executive functioning (EF) is a component of cognitive ability that predicts later academic performance and mental health in typically developing children.
EF deficits are present in ASD and EF performance has been associated with autism symptoms, mental health, academic, and functional outcomes.
This longitudinal study is the first to show that middle‐childhood EF may be one pathway through which early‐childhood autism symptoms influence early adolescent externalizing behaviors, academic performance, and everyday functioning in children with ASD followed prospectively over ~10 years.
Our work provides support for developing interventions that target EF to mitigate developmental risk for impairment on a variety of outcomes.
Supporting information
Figure S1. Schematic of the mediation models used to evaluate stability of indirect effects across raters.
Table S1. Measurement timepoints for each of the Pathways measures used in the current study.
Table S2. Comparison of socioeconomic status in included versus excluded Pathways in ASD sample.
Table S3. Measurement cross‐timepoint correlations and internal consistency.
Table S4. Sequential multivariable regression examining predictive effect of early‐childhood autism symptoms on middle‐childhood behavior regulation (T5–7 BRI: dependent variable).
Table S5. Sequential multivariable regression examining predictive effect of early‐childhood autism symptoms on middle‐childhood metacognition (T5–7 MCI: dependent variable).
Table S6. Sequential multivariable regression analysis predicting CBCL Externalizing Problems (T8) from middle‐childhood EF skills.
Table S7. Sequential multivariable regression analysis predicting CBCL Internalizing Problems (T8) from middle‐childhood EF skills.
Table S8. Sequential multivariable regression analysis predicting TRF Academic Performance (T8) from middle‐childhood EF skills.
Table S9. Sequential multivariable regression analysis predicting VABS Adaptive Behavior Composite (T8) from middle‐childhood EF skills.
Table S10. Mediation model regression examining indirect effect of teacher‐rated BRIEF‐BRI on the relation between clinician‐rated early autism symptoms (ADOS Calibrated Severity Score) and teacher‐rated Externalizing Behavior in early‐adolescence covarying for teacher‐rated Internalizing Symptoms and general cognitive ability (Model 1).
Table S11. Mediation model regression examining indirect effect of teacher‐rated BRIEF‐MCI on the relation between clinician‐rated early autism symptoms (ADOS Calibrated Severity Score) and teacher‐rated Academic Performance in early adolescence covarying for general cognitive ability (Model 3).
Table S12. Mediation model regression examining indirect effect of teacher‐rated BRIEF‐MCI on the relation between clinician‐rated early autism symptoms (ADOS Calibrated Severity Score) and parent‐rated VABS in early adolescence covarying for general cognitive ability (Model 4).
Table S13. Path coefficients and indirect effects for Model 1 with residualized SRS predictor controlling for baseline externalizing and internalizing symptoms.
Table S14. Path coefficients and indirect effects for Model 3 with residualized SRS predictor controlling for baseline externalizing and internalizing symptoms.
Table S15. Path coefficients and indirect effects for Model 4 with residualized SRS predictor controlling for baseline externalizing and internalizing symptoms.
Table S16. Path coefficients and indirect effects for Model 1 using residualized CBCL‐externalizing outcome controlling for Middle‐Childhood BRIEF‐BRI.
Table S17. Mediational model regressions examining indirect effect of parent‐rated BRIEF‐BRI on the relation between early‐childhood repetitive behaviours and later externalizing problems (variation on Model 1), covarying cognitive ability and internalizing problems.
Table S18. Summary of mediational model regressions examining mediation effects of inhibition subdomain of the BRIEF‐BRI on the association between early autism symptoms and early‐adolescent externalizing problems.
Table S19. Summary of mediational model regressions examining mediation effects of set‐shifting subdomain of the BRIEF‐BRI on the association between early autism symptoms and early‐adolescent externalizing problems.
Table S20. Summary of mediational model regressions examining mediation effects of emotional control subdomain of the BRIEF‐BRI on the association between early autism symptoms and early‐adolescent externalizing problems.
Acknowledgements
This study was supported by the Canadian Institutes of Health Research (P.S., grant numbers HDF‐70333 and FDN 93621), Kids Brain Health Network (formerly NeuroDevNet) (P.S.), Autism Speaks (P.S.), the Government of British Columbia (P.M.), Alberta Innovates Health Solutions (L.Z.), the Sinneave Family Foundation (P.S.), and the Mayberry Family (P.S.). W.J.U. is supported by a Canada Research Chair in Economic Evaluation and Technology Assessment in Child Health. M‐C.L. is supported in part by the Ontario Brain Institute via the Province of Ontario Neurodevelopmental Disorders (POND) Network (IDS‐I l‐02), the Canadian Institutes of Health Research (CIHR) Sex and Gender Science Chair (GSB 171373) and project grant (PJT 173351), the Innovation Fund of the Alternative Funding Plan for the Academic Health Sciences Centres of Ontario (CAM‐18‐004, CAM‐20‐004), and the CAMH Foundation. M‐C.L. and S.H.A. receive funding from the Academic Scholars Award from the Department of Psychiatry, University of Toronto. S.H.A. currently receives funding from the National Institute of Mental Health (R01MH114879), CIHR, and CAMH Foundation. P.S. has received royalties from Guilford Press and Simon & Schuster. The authors thank all the children and families who have participated in the Pathways in ASD study. The authors also acknowledge the Pathways in ASD Study Team (research staff members and trainees) who have contributed to this study. The remaining authors have declared that they have no competing or potential conflicts of interest.
Conflict of interest statement: See Acknowledgements for full disclosures.
References
- Achenbach, T.M. , Ivanova, M.Y. , Rescorla, L.A. , Turner, L.V. , & Althoff, R.R. (2016). Internalizing/externalizing problems: Review and recommendations for clinical and research applications. Journal of the American Academy of Child and Adolescent Psychiatry, 55, 647–656. [DOI] [PubMed] [Google Scholar]
- Achenbach, T.M. , & Rescorla, L. (2001). ASEBA school‐age forms & profiles. Burlington, VT: Aseba. [Google Scholar]
- Albert, W.D. , Hanson, J.L. , Skinner, A.T. , Dodge, K.A. , Steinberg, L. , Deater‐Deckard, K. , … & Lansford, J.E. (2020). Individual differences in executive function partially explain the socioeconomic gradient in middle‐school academic achievement. Developmental Science, 23, e12937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bal, V.H. , Kim, S.‐H. , Cheong, D. , & Lord, C. (2015). Daily living skills in individuals with autism spectrum disorder from 2 to 21 years of age. Autism, 19, 774–784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baribeau, D.A. , Vigod, S. , Pullenayegum, E. , Kerns, C.M. , Mirenda, P. , Smith, I.M. , … & Zwaigenbaum, L. (2020). Repetitive behavior severity as an early indicator of risk for elevated anxiety symptoms in autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 59, 890–899.e893. [DOI] [PubMed] [Google Scholar]
- Belsky, J. , Pasco Fearon, R.M. , & Bell, B. (2007). Parenting, attention and externalizing problems: Testing mediation longitudinally, repeatedly and reciprocally. Journal of Child Psychology and Psychiatry and Allied Disciplines, 48, 1233–1242. [DOI] [PubMed] [Google Scholar]
- Blair, C. , Raver, C.C. , & Finegood, E.D. (2016). Self‐regulation and developmental psychopathology: Experiential canalization of brain and behavior. In Cicchetti D. (Ed.), Developmental psychopathology (pp. 484–522). New York: John Wiley & Sons. [Google Scholar]
- Bodfish, J.W. , Symons, F.J. , Parker, D.E. , & Lewis, M.H. (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30, 237–243. [DOI] [PubMed] [Google Scholar]
- Bölte, S. , Poustka, F. , & Constantino, J.N. (2008). Assessing autistic traits: cross‐cultural validation of the Social Responsiveness Scale (SRS). Autism Research, 1, 354–363. [DOI] [PubMed] [Google Scholar]
- Cameron, C.E. , Brock, L.L. , Murrah, W.M. , Bell, L.H. , Worzalla, S.L. , Grissmer, D. , & Morrison, F.J. (2012). Fine motor skills and executive function both contribute to kindergarten achievement. Child Development, 83, 1229–1244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas, B.E. , Connor‐Smith, J.K. , Saltzman, H. , Thomsen, A.H. , & Wadsworth, M.E. (2001). Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychological Bulletin, 127, 87. [PubMed] [Google Scholar]
- Constantino, J.N. , Davis, S. , Todd, R. , Schindler, M. , Gross, M. , Brophy, S. , … & Reich, W. (2003). Validation of a brief quantitative measure of autistic traits: Comparison of the Social Responsiveness Scale with the Autism Diagnostic Interview‐Revised. Journal of Autism and Developmental Disorders, 33, 427–433. [DOI] [PubMed] [Google Scholar]
- Demetriou, E.A. , Lampit, A. , Quintana, D.S. , Naismith, S.L. , Song, Y.J.C. , Pye, J.E. , … & Guastella, A.J. (2018). Autism spectrum disorders: A meta‐analysis of executive function. Molecular Psychiatry, 23, 1198–1204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dempsey, E.E. , Smith, I.M. , Flanagan, H.E. , Duku, E. , Lawrence, M.A. , Szatmari, P. , … & Bennett, T. (2020). Psychometric properties of the merrill‐palmer‐revised scales of development in preschool children with autism spectrum disorder. Assessment, 27, 1796–1809. [DOI] [PubMed] [Google Scholar]
- Diamantopoulou, S. , Rydell, A.M. , Thorell, L.B. , & Bohlin, G. (2007). Impact of executive functioning and symptoms of attention deficit hyperactivity disorder on children's peer relations and school performance. Developmental Neuropsychology, 32, 521–542. [DOI] [PubMed] [Google Scholar]
- Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64, 135–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eaves, L.C. , & Ho, H.H. (2008). Young adult outcome of autism spectrum disorders. Journal of Autism and Developmental Disorders, 38, 739–747. [DOI] [PubMed] [Google Scholar]
- Fritz, M.S. , & Mackinnon, D.P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18, 233–239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gardiner, E. , & Iarocci, G. (2018). Everyday executive function predicts adaptive and internalizing behavior among children with and without autism spectrum disorder. Autism Research, 11, 284–295. [DOI] [PubMed] [Google Scholar]
- Garon, N. , Bryson, S.E. , & Smith, I.M. (2008). Executive function in preschoolers: A review using an integrative framework. Psychological Bulletin, 134, 31–60. [DOI] [PubMed] [Google Scholar]
- Garon, N. , Smith, I.M. , & Bryson, S.E. (2018). Early executive dysfunction in ASD: Simple versus complex skills. Autism Research, 11, 318–330. [DOI] [PubMed] [Google Scholar]
- Gilotty, L. , Kenworthy, L. , Sirian, L. , Black, D.O. , & Wagner, A.E. (2002). Adaptive skills and executive function in autism spectrum disorders. Child Neuropsychology, 8, 241–248. [DOI] [PubMed] [Google Scholar]
- Gioia, G.A. , Isquith, P.K. , Guy, S.C. , & Kenworth, L. (2000). Behavior rating inventory of executive function. Lutz, FL: Psychological Assessment Resources. [Google Scholar]
- Gotham, K. , Pickles, A. , & Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 693–705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green, J. , Pickles, A. , Pasco, G. , Bedford, R. , Wan, M.W. , Elsabbagh, M. , … & The British Autism Study of Infant Siblings (BASIS) Team (2017). Randomised trial of a parent‐mediated intervention for infants at high risk for autism: longitudinal outcomes to age 3 years. Journal of Child Psychology and Psychiatry, 58, 1330–1340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Havdahl, K.A. , Hus Bal, V. , Huerta, M. , Pickles, A. , Øyen, A.‐S. , Stoltenberg, C. , … & Bishop, S.L. (2016). Multidimensional influences on autism symptom Measures: Implications for use in etiological research. Journal of the American Academy of Child and Adolescent Psychiatry, 55, 1054–1063.e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes, A.F. (2009). Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs, 76, 408–420. [Google Scholar]
- Hayes, A.F. (2017). Introduction to mediation, moderation, and conditional process analysis a regression‐based approach (2nd edn). New York: Guillford Press. [Google Scholar]
- Hazlett, H.C. , Gu, H. , Munsell, B.C. , Kim, S.H. , Styner, M. , Wolff, J.J. , … & Statistical Analysis (2017). Early brain development in infants at high risk for autism spectrum disorder. Nature, 542, 348–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howlin, P. , Goode, S. , Hutton, J. , & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry and Allied Disciplines, 45, 212–229. [DOI] [PubMed] [Google Scholar]
- Howlin, P. , & Moss, P. (2012). Adults with autism spectrum disorders. Canadian Journal of Psychiatry, 57, 275–283. [DOI] [PubMed] [Google Scholar]
- Hughes, R.A. , Heron, J. , Sterne, J.A.C. , & Tilling, K. (2019). Accounting for missing data in statistical analyses: Multiple imputation is not always the answer. International Journal of Epidemiology, 48, 1294–1304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenworthy, L. , Anthony, L.G. , Naiman, D.Q. , Cannon, L. , Wills, M.C. , Luong‐Tran, C. , … & Wallace, G.L. (2014). Randomized controlled effectiveness trial of executive function intervention for children on the autism spectrum. Journal of Child Psychology and Psychiatry and Allied Disciplines, 55, 374–383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kertz, S.J. , Belden, A.C. , Tillman, R. , & Luby, J. (2016). Cognitive control deficits in shifting and inhibition in preschool age children are associated with increased depression and anxiety over 7.5 years of development. Journal of Abnormal Child Psychology, 44, 1185–1196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lansford, J.E. , Malone, P.S. , Tapanya, S. , Tirado, L.M.U. , Zelli, A. , Alampay, L.P. , … & Steinberg, L. (2019). Household income predicts trajectories of child internalizing and externalizing behavior in high‐, middle‐, and low‐income countries. International Journal of Behavioral Development, 43, 74–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawson, R.A. , Papadakis, A.A. , Higginson, C.I. , Barnett, J.E. , Wills, M.C. , Strang, J.F. , … & Kenworthy, L. (2015). Everyday executive function impairments predict comorbid psychopathology in autism spectrum and attention deficit hyperactivity disorders. Neuropsychology, 29, 445–453. [DOI] [PubMed] [Google Scholar]
- Leung, R.C. , Vogan, V.M. , Powell, T.L. , Anagnostou, E. , & Taylor, M.J. (2016). The role of executive functions in social impairment in Autism Spectrum Disorder. Child Neuropsychology, 22, 336–344. [DOI] [PubMed] [Google Scholar]
- Lewin, A. , Brondeel, R. , Benmarhnia, T. , Thomas, F. , & Chaix, B. (2018). Attrition bias related to missing outcome data. Epidemiology, 29, 87–95. [DOI] [PubMed] [Google Scholar]
- Little, R.J.A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83, 1198–1202. [Google Scholar]
- Lord, C. , Rutter, M. , DiLavore, P.C. , Risi, S. , Gotham, K. , Bishop, S.L. , … & Guthrie, W. (2012). Autism diagnostic observation schedule—Second edition (ADOS‐2). Torrence, CA: Western Psychological Services. [Google Scholar]
- McClelland, M.M. , Cameron, C.E. , Connor, C.M. , Farris, C.L. , Jewkes, A.M. , & Morrison, F.J. (2007). Links between behavioral regulation and preschoolers' literacy, vocabulary, and math skills. Developmental Psychology, 43, 947–959. [DOI] [PubMed] [Google Scholar]
- McLean, R.L. , Harrison, A.J. , Zimak, E. , Joseph, R.M. , & Morrow, E.M. (2014). Executive function in probands with autism with average IQ and their unaffected first‐degree relatives. Journal of the American Academy of Child and Adolescent Psychiatry, 53, 1001–1009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meule, A. (2019). Contemporary understanding of mediation testing. Meta‐Psychology, 3, 1–7. [Google Scholar]
- Mirenda, P. , Smith, I.M. , Vaillancourt, T. , Georgiades, S. , Duku, E. , Szatmari, P. , … & Pathways in ASD Study Team (2010). Validating the Repetitive Behavior Scale‐revised in young children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40, 1521–1530. [DOI] [PubMed] [Google Scholar]
- Miyake, A. , Friedman, N.P. , Emerson, M.J. , Witzki, A.H. , Howerter, A. , & Wager, T.D. (2000). The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cognitive Psychology, 41, 49–100. [DOI] [PubMed] [Google Scholar]
- Nelson, T.D. , Kidwell, K.M. , Nelson, J.M. , Tomaso, C.C. , Hankey, M. , & Espy, K.A. (2018). Preschool executive control and internalizing symptoms in elementary school. Journal of Abnormal Child Psychology, 46, 1509–1520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pellicano, E. (2012). The development of executive function in autism. Autism Research and Treatment, 2012, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pickles, A. , McCauley, J.B. , Pepa, L.A. , Huerta, M. , & Lord, C. (2020). The adult outcome of children referred for autism: Typology and prediction from childhood. Journal of Child Psychology and Psychiatry, 61, 760–767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Podsakoff, P.M. , MacKenzie, S.B. , Lee, J.‐Y. , & Podsakoff, N.P. (2003). Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology, 88, 879–903. [DOI] [PubMed] [Google Scholar]
- Preacher, K.J. , & Kelley, K. (2011). Effect size measures for mediation models: Quantitative strategies for communicating indirect effects. Psychological Methods, 16, 93–115. [DOI] [PubMed] [Google Scholar]
- Pugliese, C.E. , Anthony, L. , Strang, J.F. , Dudley, K. , Wallace, G.L. , & Kenworthy, L. (2015). Increasing adaptive behavior skill deficits from childhood to adolescence in autism spectrum disorder: Role of executive function. Journal of Autism and Developmental Disorders, 45, 1579–1587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pugliese, C.E. , Anthony, L.G. , Strang, J.F. , Dudley, K. , Wallace, G.L. , Naiman, D.Q. , & Kenworthy, L. (2016). Longitudinal examination of adaptive behavior in autism spectrum disorders: Influence of executive function. Journal of Autism and Developmental Disorders, 46, 467–477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roid, G.H. , & Sampers, J.L. (2004). Merrill‐palmer‐revised scales of development. Wood Dale, IL: Stoelting Company. [Google Scholar]
- Roman, G.D. , Ensor, R. , & Hughes, C. (2016). Does executive function mediate the path from mothers' depressive symptoms to young children's problem behaviors? Journal of Experimental Child Psychology, 142, 158–170. [DOI] [PubMed] [Google Scholar]
- Rosello, B. , Berenguer, C. , Baixauli, I. , Colomer, C. , & Miranda, A. (2018). ADHD symptoms and learning behaviors in children with ASD without intellectual disability. A mediation analysis of executive functions. PLoS One, 13, e0207286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutter, M. , LeCouteur, A. , & Lord, C. (2003). Autism diagnostic interview‐revised manual. Los Angeles: Western Psychological Services. [Google Scholar]
- Séguin, J.R. , Boulerice, B. , Harden, P.W. , Tremblay, R.E. , & Pihl, R.O. (1999). Executive functions and physical aggression after controlling for attention deficit hyperactivity disorder, general memory, and IQ. Journal of Child Psychology and Psychiatry and Allied Disciplines, 40, 1197–1208. [PubMed] [Google Scholar]
- Sparrow, S.S. , Cicchetti, D.V. , & Balla, D.A. (2005). Vineland adaptive behavior scales (2nd edn). Circle Pines: American Guidance Service. [Google Scholar]
- Sterne, J.A.C. , White, I.R. , Carlin, J.B. , Spratt, M. , Royston, P. , Kenward, M.G. , … & Carpenter, J.R. (2009). Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ, 338, b2393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sulik, M.J. (2017). Introduction to the special section on executive functions and externalizing symptoms. Journal of Abnormal Child Psychology, 45, 1473–1475. [DOI] [PubMed] [Google Scholar]
- Sulik, M.J. , Blair, C. , Mills‐Koonce, R. , Berry, D. , & Greenberg, M. (2015). Early parenting and the development of externalizing behavior problems: Longitudinal mediation through children's executive function. Child Development, 86, 1588–1603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szatmari, P. , Bryson, S.E. , Boyle, M.H. , Streiner, D.L. , & Duku, E. (2003). Predictors of outcome among high functioning children with autism and Asperger syndrome. Journal of Child Psychology and Psychiatry and Allied Disciplines, 44, 520–528. [DOI] [PubMed] [Google Scholar]
- Toplak, M.E. , West, R.F. , & Stanovich, K.E. (2013). Practitioner review: Do performance‐based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry, 54, 131–143. [DOI] [PubMed] [Google Scholar]
- Tormala, Z.L. , Falces, C. , Brinol, P. , & Petty, R.E. (2007). Ease of retrieval effects in social judgment: The role of unrequested cognitions. Journal of Personality and Social Psychology, 93, 143–157. [DOI] [PubMed] [Google Scholar]
- Torske, T. , Naerland, T. , Oie, M.G. , Stenberg, N. , & Andreassen, O.A. (2017). Metacognitive aspects of executive function are highly associated with social functioning on parent‐rated measures in children with autism spectrum disorder. Frontiers in Behavioral Neuroscience, 11, 258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Venker, C.E. , Ray‐Subramanian, C.E. , Bolt, D.M. , & Ellis Weismer, S. (2014). Trajectories of autism severity in early childhood. Journal of Autism and Developmental Disorders, 44, 546–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, G.L. , Kenworthy, L. , Pugliese, C.E. , Popal, H.S. , White, E.I. , Brodsky, E. , & Martin, A. (2016). Real‐world executive functions in adults with autism spectrum disorder: Profiles of impairment and associations with adaptive functioning and co‐morbid anxiety and depression. Journal of Autism and Developmental Disorders, 46, 1071–1083. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Schematic of the mediation models used to evaluate stability of indirect effects across raters.
Table S1. Measurement timepoints for each of the Pathways measures used in the current study.
Table S2. Comparison of socioeconomic status in included versus excluded Pathways in ASD sample.
Table S3. Measurement cross‐timepoint correlations and internal consistency.
Table S4. Sequential multivariable regression examining predictive effect of early‐childhood autism symptoms on middle‐childhood behavior regulation (T5–7 BRI: dependent variable).
Table S5. Sequential multivariable regression examining predictive effect of early‐childhood autism symptoms on middle‐childhood metacognition (T5–7 MCI: dependent variable).
Table S6. Sequential multivariable regression analysis predicting CBCL Externalizing Problems (T8) from middle‐childhood EF skills.
Table S7. Sequential multivariable regression analysis predicting CBCL Internalizing Problems (T8) from middle‐childhood EF skills.
Table S8. Sequential multivariable regression analysis predicting TRF Academic Performance (T8) from middle‐childhood EF skills.
Table S9. Sequential multivariable regression analysis predicting VABS Adaptive Behavior Composite (T8) from middle‐childhood EF skills.
Table S10. Mediation model regression examining indirect effect of teacher‐rated BRIEF‐BRI on the relation between clinician‐rated early autism symptoms (ADOS Calibrated Severity Score) and teacher‐rated Externalizing Behavior in early‐adolescence covarying for teacher‐rated Internalizing Symptoms and general cognitive ability (Model 1).
Table S11. Mediation model regression examining indirect effect of teacher‐rated BRIEF‐MCI on the relation between clinician‐rated early autism symptoms (ADOS Calibrated Severity Score) and teacher‐rated Academic Performance in early adolescence covarying for general cognitive ability (Model 3).
Table S12. Mediation model regression examining indirect effect of teacher‐rated BRIEF‐MCI on the relation between clinician‐rated early autism symptoms (ADOS Calibrated Severity Score) and parent‐rated VABS in early adolescence covarying for general cognitive ability (Model 4).
Table S13. Path coefficients and indirect effects for Model 1 with residualized SRS predictor controlling for baseline externalizing and internalizing symptoms.
Table S14. Path coefficients and indirect effects for Model 3 with residualized SRS predictor controlling for baseline externalizing and internalizing symptoms.
Table S15. Path coefficients and indirect effects for Model 4 with residualized SRS predictor controlling for baseline externalizing and internalizing symptoms.
Table S16. Path coefficients and indirect effects for Model 1 using residualized CBCL‐externalizing outcome controlling for Middle‐Childhood BRIEF‐BRI.
Table S17. Mediational model regressions examining indirect effect of parent‐rated BRIEF‐BRI on the relation between early‐childhood repetitive behaviours and later externalizing problems (variation on Model 1), covarying cognitive ability and internalizing problems.
Table S18. Summary of mediational model regressions examining mediation effects of inhibition subdomain of the BRIEF‐BRI on the association between early autism symptoms and early‐adolescent externalizing problems.
Table S19. Summary of mediational model regressions examining mediation effects of set‐shifting subdomain of the BRIEF‐BRI on the association between early autism symptoms and early‐adolescent externalizing problems.
Table S20. Summary of mediational model regressions examining mediation effects of emotional control subdomain of the BRIEF‐BRI on the association between early autism symptoms and early‐adolescent externalizing problems.