

Abstract
Background and purpose
Modifiable lifestyle factors, including diet, may affect clinical outcomes in multiple sclerosis (MS). This study assessed the relationships between diet, and disability, fatigue, and depression risk in people with MS.
Methods
Participants from the Health Outcomes and Lifestyle In a Sample of people with Multiple sclerosis (HOLISM) international cohort were assessed over 2.5 years. Dietary data were obtained using a modified Diet Habits Questionnaire (DHQ), disability using the calculated Patient‐determined MS Severity Score (P‐MSSS), fatigue using the Fatigue Severity Scale, and depression risk using the Patient Health Questionnaire‐2. Participants reported whether they were experiencing symptoms due to a recent relapse. Cross‐sectional and prospective relationships of diet and disease outcomes were explored, adjusted for relevant confounders.
Results
Among 1,346 participants, higher DHQ scores showed significant dose‐dependent associations with lower frequencies of severe disability, fatigue, and depression risk, cross‐sectionally. Prospectively, higher baseline DHQ scores were associated with a lower risk of increasing disability, those above the median having 41% and 36% lower risk of increasing disability, and 0.30 P‐MSSS points less disability progression, but were not associated with fatigue or depression risk. Meat consumption was associated with 0.22 P‐MSSS points higher disability cross‐sectionally, while prospectively, baseline meat consumption was associated with 76% higher risk of increasing disability and 0.18 P‐MSSS points higher disability progression. Dairy consumption showed mixed associations cross‐sectionally and prospectively.
Conclusions
These results show that better quality of diet, as well as not consuming meat, were associated with reduced disability progression in people with MS. Substantiation of these findings in other settings may inform opportunities to manage disability progression in people with MS using dietary modifications.
Keywords: depression, diet, disability progression, fatigue, multiple sclerosis
In this cohort of 1,346 people with multiple sclerosis, followed over 2.5 years, we found that better diet quality and not consuming meat or dairy were associated with significantly less disability progression. Those with better diet quality or not consuming meat or dairy actually decreased their disability, while those with worse diet practices had static or worse disability. However, no prospective associations of diet quality with fatigue or depression were seen.

INTRODUCTION
Multiple sclerosis (MS) is a chronic, autoimmune, neurodegenerative disorder with an array of symptoms [1]. Sustained inflammation and axonal loss result in progressive and cumulative disability. Fatigue and depression are common symptoms in MS, fatigue affecting approximately 80% and depression 20–50% of people with MS [2, 3].
Of the lifestyle factors implicated in MS progression [4], diet has received increasing interest. There is biological plausibility for diet to affect progression, including via body mass index (BMI), dyslipidaemia, and microbiome changes [5, 6]. In addition, diet is modifiable, with positive benefits to health and well‐being. Diet in MS can be assessed via many instruments, such as the Dietary Questionnaire for Epidemiological Studies [7], food diaries, and shorter measures such as the Short‐Form Food Frequency Questionnaire [8] and the Diet Habits Questionnaire (DHQ) [9], used in the present study. Multiple studies have identified associations between diet and MS risk [10, 11] disability [12], fatigue [12, 13, 14], and depression [12, 15]; others have found no associations [14, 15, 16, 17, 18]. Our group has evaluated the cross‐sectional relationships of diet and disability [19, 20], depression [21], and fatigue [22] at baseline using the Health Outcomes and Lifestyle In a Sample of people with Multiple sclerosis (HOLISM) cohort, finding that a higher DHQ score was associated with better outcomes.
Several diet programmes, some as part of multimodal lifestyle programmes, have been proposed for people with MS, some suggesting improved clinical outcomes in MS [23, 24, 25, 26], and all featuring modified consumption of certain food groups. In particular, the Wahls modified‐Paleolithic diet programme recommends meat consumption [27], while the Swank [27], Overcoming MS [28], and McDougall [29] diet programmes recommend limited or no meat consumption; all of these diets apart from the Swank programme recommend limited or no dairy consumption. The evidence base for the role of meat and dairy consumption in MS is limited and highly heterogeneous, with the authors of some prior work suggesting a harmful relationship [20] and others suggesting beneficial associations [24]. The frequency of adherence to the diet programmes is also quite heterogeneous, as shown in various cohorts [15, 30].
To determine the potential effect of diet on MS clinical outcomes, we undertook a prospective analysis of diet and disability, clinically significant fatigue, and depression risk in an international cohort of people with MS over a 2.5‐year follow‐up.
METHODS
Participants were originally recruited to the HOLISM study, as described elsewhere [31, 32]. Briefly, participants were recruited via online platforms in 2012, surveyed at 2.5‐year intervals, and were required to be at least 18 years of age with a self‐reported physician diagnosis of MS.
Ethical approval was granted by The University of Melbourne (HESC 1545102) and all participants provided informed tacit consent.
Data collection
Survey data
Sociodemographic and clinical factors were queried, including demographics, MS phenotype, clinical outcomes, prescription medications, and lifestyle behaviours. The surveys at baseline and 2.5 years were generally consistent, except for perceived relative socioeconomic status (PRSES), which was assessed only at 2.5 years. PRSES is a nine‐level variable that was consolidated into: below average (1–4); average (5); and above average (6–9); PRSES values at 2.5 years were used for the prospective analyses from baseline. Self‐reported height (m) and weight (kg) were used to calculate BMI and categorized as underweight (<18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2), as per World Health Organization guidelines. Physical activity was measured using the International Physical Activity Questionnaire (IPAQ), categorized as inactive, minimally active, and active as per IPAQ guidelines [33].
Dietary habits
Diet was assessed using a modified DHQ [9], as described previously [19]. Briefly, three questions about salt consumption were omitted and one on alcohol intake was replaced, leaving 20 questions. Response to DHQ questions on the consumption of low‐fat versus full‐fat dairy products, trimming fat/skin from meat, and consumption of processed meats, were modified to include a response of 'I do not consume dairy' and 'I do not consume meat', respectively, from which dichotomous terms about meat and dairy consumption were created. Fish consumption was queried separately, thus, meat consumption in this study refers to land‐based meats including poultry. The DHQ produces seven dietary subscores: cereals; fruit/vegetables; takeaway; fat; fibre; food choices; and food preparation. Each question is measured with a Likert scale from 1 (poor) to 5 (healthy), as per DHQ guidelines [9]. A summary score from 20 DHQ questions was calculated, giving equal weight to all items, with a possible score range of 20–100 (higher scores indicating higher quality of diet). Missing questions within subdomains were imputed with the mean of the non‐missing questions comprising that subdomain, as described previously [31]. Imputation using the median of non‐missing questions did not materially change the values of DHQ scores or subdomains (data not shown).
Clinical outcomes
Disability was assessed via the Patient Determined Disease Steps (PDDS) [34], from which the disease duration‐adjusted Patient‐determined MS Severity Score (P‐MSSS) was calculated [35], categorized as: normal/mild (0–3), moderate (>3–6), and severe (>6) disability.
Fatigue was measured by the Fatigue Severity Scale (FSS) [36]. Responses to nine statements related to fatigue were based on a seven‐point Likert scale, a mean FSS score >5 indicating clinically significant fatigue [36].
Depression was assessed using the Patient Health Questionnaire‐2 (PHQ‐2), with a total PHQ‐2 score > 2 indicating depression risk [37].
Participants reported whether they were experiencing ongoing symptoms from a recent relapse in the preceding 30 days (yes/no).
Data analysis
Cohort characteristics and bias
Characteristics of participants included in the analyses at baseline and 2.5 years were assessed by multinomial logistic regression for categorical, and linear regression for continuous variables, variance adjusted for multiple observations.
Bias in retention was assessed by comparing the baseline characteristics among those with and without data at follow‐up, using multinomial logistic regression for categorical terms and two‐tailed t‐tests for normally distributed and Kruskal−Wallis for non‐normally distributed continuous terms.
Cross‐sectional analyses
Continuous disability was assessed by linear regression. Because disability was significantly skewed, in each model disability was transformed by theta coefficients identified by Box‐Cox regression. The transformed variable was used as the outcome in relevant models. All reported coefficients were back‐transformed at the means of the model covariates to the original scale of the outcome variable. Categories of disability severity (mild/moderate/severe) were assessed by log‐multinomial regression. Dichotomous fatigue and depression risk at 2.5 years were assessed by log‐binomial regression. Outcome models were adjusted for ongoing symptoms due to recent relapse, age, sex, PRSES, and MS phenotype. Disability models were also adjusted for fatigue, fatigue models were adjusted for disability and prescription for anti‐fatigue medication use, and depression risk models were adjusted for disability, fatigue, and prescription antidepressant use.
Prospective analyses
Change in continuous disability between baseline and 2.5 years was estimated as the change in the continuous P‐MSSS between baseline and 2.5 years. Change in disability severity between baseline and 2.5 years was categorized as decreasing, increasing, or stable.
Change in disability severity, fatigue, and depression risk were assessed by log‐multinomial regression. Change in continuous disability was assessed by linear regression.
Change in fatigue and depression risk were evaluated as the proportion of participants without the symptom at baseline who developed the symptom at 2.5 years (gain), or with the symptom at baseline but not at 2.5 years (loss), as per previous analyses [38], and evaluated by log‐multinomial regression.
All models were adjusted for ongoing symptoms due to a recent relapse at baseline and 2.5‐year reviews. Further, the adjusted models included the baseline covariates as in the cross‐sectional models. Change in continuous disability models were also adjusted for baseline P‐MSSS.
All analyses were complete case, constrained to participants with data available for all model covariates.
In addition, imputation of the P‐MSSS, fatigue, and depression risk outcomes at baseline and follow‐up were imputed with the best‐case (mild disability/no fatigue/no depression risk) and worst‐case (severe disability/fatigue/depression risk) where these values were missing for prospective analyses. These did not materially change any associations (data not shown).
Analyses were conducted using STATA/SE 16.0 (StataCorp, College Station, TX, USA).
RESULTS
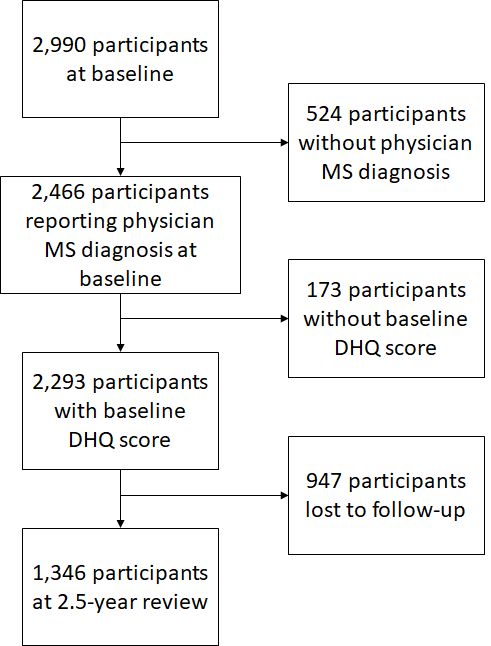
Of 2,466 baseline HOLISM participants, 1,346 participants with baseline DHQ data completed the 2.5‐year survey (Supplemental Figure 1) and were included in the study. Included participants were predominantly female (82.8%), with a mean (SD) age of 48.6 (10.5) years. The majority reported a relapsing‐remitting MS (RRMS) phenotype (67.8%), 61.6% had mild P‐MSSS, 62.1% had fatigue, and 14.1% screened positive for depression risk, and the median duration since onset was 14.0 years. DHQ and subdomain scores were skewed towards higher scores, with a median total DHQ score of 81/100. Over 60% of participants consumed meat and nearly 60% consumed dairy. Other characteristics of the analysis sample are shown in Table 1.
TABLE 1.
Cohort characteristics of analysis sample at 2.5‐year review
| Mean (SD; range) | |
|---|---|
| Age, years | 48.6 (10.5; 20.1–81.5) |
| n (%) | |
|---|---|
| Sex | |
| Male | 232 (17.2) |
| Female | 1,114 (82.8) |
| PRSES | |
| Lower | 256 (19.3) |
| Same | 420 (31.7) |
| Higher | 650 (49.0) |
| (Missing) | (20 [1.5]) |
| BMI | |
| Underweight/normal (<25) | 820 (61.0) |
| Overweight (≥25–30) | 292 (21.7) |
| Obese (>30) | 232 (17.3) |
| (Missing) | (2 [0.2]) |
| Current MS phenotype | |
| RRMS | 910 (67.8) |
| SPMS | 142 (10.6) |
| PPMS | 96 (7.2) |
| PRMS | 18 (1.3) |
| Unsure/other | 176 (13.1) |
| [Missing] | (4 [0.3]) |
| Disability (P‐MSSS) | |
| Normal/mild | 806 (61.6) |
| Moderate | 315 (24.1) |
| Severe | 187 (14.3) |
| (Missing) | (38 [2.8]) |
| Clinically significant fatigue (FSS) | |
| No | 465 (37.9) |
| Yes | 761 (62.1) |
| (Missing) | (120 [8.9]) |
| Depression‐risk (PHQ‐2) | |
| No | 1,089 (85.9) |
| Yes | 179 (14.1) |
| (Missing) | (78 [5.8]) |
| Disease‐modifying therapy use? | |
| No | 772 (57.4) |
| Yes | 574 (42.6) |
| Prescription antidepressant use? | |
| No | 1,149 (82.0) |
| Yes | 252 (18.0) |
| Prescription antifatigue medication use? | |
| No | 1,287 (91.9) |
| Yes | 114 (8.1) |
| Consume meat? | |
| No | 501 (38.9) |
| Yes | 787 (61.1) |
| (Missing) | (58 [4.3]) |
| Consume dairy? | |
| No | 549 (42.8) |
| Yes | 735 (57.2) |
| (Missing) | (62 [4.6]) |
| Median (IQR) | |
|---|---|
| Duration since onset, years | 14.0 (8.1–22.9) |
| DHQ total score | 81 (70–89) |
Missing value percentages are in addition to the 100% of measured values. Where no missing proportion is shown, there were none missing based on how the variable was queried.
Abbreviations: BMI, body mass index; DHQ, Diet Habits Questionnaire; IQR, interquartile range; MS, multiple sclerosis; P‐MSSS, Patient‐determined MS Severity Score; PPMS, primary progressive MS; PRMS, progressive‐relapsing MS; PRSES, perceived relative socioeconomic status; RRMS, relapsing‐remitting MS; SD, standard deviation; SPMS, secondary progressive MS.
Characteristics of the analysis sample at baseline and the 2.5‐year review, including characteristics not shown in Table 1, are shown in Table S1. The only meaningful differences between baseline and 2.5 years were a reduced proportion using disease‐modifying therapies (DMTs), and a higher frequency of depression risk.
Compared to the participants lost to follow‐up (45.4%), the included participants had higher levels of education, higher rates of employment, healthier behaviours (normal BMI, physically active, supplement use), including higher DHQ scores, and less disability, fatigue and depression risk, as well as less antidepressant and anti‐fatigue medication use (Table S2).
Cross‐sectional analyses at 2.5 years
Diet and disability
The DHQ scores did not differ between people with MS reporting moderate versus mild disability (Table 2). However, the higher the DHQ score, the more likely the participants were to have mild versus severe disability, although this attenuated on adjustment for age, sex, PRSES, MS phenotype, and clinically significant fatigue. Participants in the top two quartiles of DHQ scores had 25% (95% CI −3%, 45%) and 29% (95% CI −6%, 53%) a lower frequency of severe disability. DHQ scores also showed a strong inverse association with continuous disability (P‐MSSS); those in the top two quartiles of DHQ scores had 0.33 (95% CI 0.06, 0.59) and 0.37 (95% CI 0.10, 0.64) points lower disability and meat consumption was positively associated with continuous disability (aβ = 0.22, 95% CI 0.03, 0.41; Table 3). Fruit/vegetables, fat, fibre, and food preparation subdomains were inversely associated with disability (Tables S3 and S4).
TABLE 2.
Cross‐sectional relationships of Diet Habits Questionnaire scores and meat and dairy consumption with Patient‐determined Multiple Sclerosis Severity Score severity at 2.5‐year review
| n (%) | Moderate vs. Mild | Severe vs. Mild | |||||
|---|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | aPR1 | aPR2 | aPR1 | aPR2 | |
| DHQ score a | |||||||
| 32–70 | 182/339 (53.7) | 84/339 (24.8) | 73/339 (21.5) | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] |
| >70–80 | 187/324 (57.7) | 91/324 (28.1) | 46/324 (14.2) | 1.03 (0.81, 1.31) | 0.97 (0.77, 1.22) | 0.69 (0.50, 0.95) | 0.81 (0.60, 1.09) |
| >80–89 | 231/351 (65.8) | 76/351 (21.7) | 44/351 (12.5) | 0.81 (0.62, 1.05) | 0.82 (0.64, 1.06) | 0.57 (0.41, 0.80) | 0.75 (0.55, 1.03) |
| >89–100 | 209/308 (67.9) | 73/308 (23.7) | 26/308 (8.4) | 0.85 (0.65, 1.11) | 1.00 (0.78, 1.28) | 0.40 (0.26, 0.60) | 0.71 (0.47, 1.06) |
| Trend | p = 0.083 | p = 0.64 | p < 0.001 | p = 0.042 | |||
| Consume meat? b | |||||||
| No | 346/511 (67.7) | 121/511 (23.7) | 44/511 (8.6) | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 463/812 (57.0) | 203/81 (25.0) | 146/812 (18.0%) | 1.14 (0.94, 1.38) | 1.00 (0.83, 1.19) | 2.09 (1.53, 2.85) | 1.25 (0.92, 1.69) |
| p = 0.19 | p = 0.96 | p < 0.001 | p = 0.16 | ||||
| Consume dairy? c | |||||||
| No | 362/561 (64.5) | 141/561 (25.1) | 58/561 (10.3) | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 447/758 (59.0) | 182/758 (24.0) | 129/758 (17.0) | 1.00 (0.83, 1.21) | 0.90 (0.75, 1.07) | 1.60 (1.21, 2.12) | 1.15 (0.88, 1.51) |
| p = 0.98 | p = 0.23 | p = 0.001 | p = 0.29 | ||||
Analyses by log‐multinomial regression. Model 1 adjusted for ongoing symptoms due to recent relapse. Model 2 further adjusted for age, sex, multiple sclerosis phenotype, clinically significant fatigue, and socioeconomic status.
Results in boldface denote statistical significance (p < 0.05).
Abbreviations: DHQ, Diet Habits Questionnaire; aPR, adjusted prevalence ratio.
Analyses for DHQ score vs. disability in Model 1 includes 1,322 people, thus excluding 24 people with missing data. Model 2 includes 1,235 people, thus excluding 111 people with missing data.
Analyses for meat consumption vs. disability in Model 1 includes 1,323 people, thus excluding 23 people with missing data. Model 2 includes 1,236 people, thus excluding 110 people with missing data.
Analyses for dairy consumption vs. disability in Model 1 includes 1,319 people, thus excluding 27 people with missing data. Model 2 includes 1,232 people, thus excluding 114 people with missing data.
TABLE 3.
Cross‐sectional relationship of Diet Habits Questionnaire scores and meat and dairy consumption with continuous Patient‐determined Multiple Sclerosis Severity Score at 2.5‐year review
| n (%) | aβ (95% CI) a | aβ (95% CI) b | |
|---|---|---|---|
| DHQ score a | |||
| 32–70 | 339 (25.6) | 0.00 [Reference] | 0.00 [Reference] |
| >70–80 | 324 (24.5) | −0.22 (−0.56, 0.13) | −0.17 (−0.44, 0.11) |
| >80–89 | 351 (26.6) | −0.54 (−0.85, −0.23) | −0.33 (−0.59, −0.06) |
| >89–100 | 308 (23.3) | −0.79 (−1.10, −0.49) | −0.37 (−0.64, −0.10) |
| Trend | p < 0.001 | p = 0.003 | |
| Consume meat? b | |||
| No | 511 (38.6) | 0.00 [Reference] | 0.00 [Reference] |
| Yes | 812 (61.4) | 0.54 (0.33, 0.75) | 0.22 (0.03, 0.41) |
| p < 0.001 | p = 0.024 | ||
| Consume dairy? c | |||
| No | 561 (42.5) | 0.00 [Reference] | 0.00 [Reference] |
| Yes | 758 (57.5) | 0.35 (0.14, 0.55) | 0.10 (−0.09, 0.28) |
| p = 0.001 | p = 0.32 | ||
Analyses by linear regression. Model 1 adjusted for ongoing symptoms due to recent relapse. Model 2 further adjusted for age, sex, multiple sclerosis phenotype, socioeconomic status and clinically significant fatigue.
Results in boldface denote statistical significance (p < 0.05).
Abbreviations: DHQ, Diet Habits Questionnaire.
Analyses for DHQ score vs. disability in model 1 includes 1,322 people, thus excluding 24 people with missing data. Model 2 includes 1,235 people, thus excluding 111 people with missing data.
Analyses for meat consumption vs. disability in Model 1 includes 1,323 people, thus excluding 23 people with missing data. Model 2 includes 1,236 people, thus excluding 110 people with missing data.
Analyses for dairy consumption vs. disability in Model 1 includes 1,319 people, thus excluding 27 people with missing data. Model 2 includes 1,232 people, thus excluding 114 people with missing data.
Diet and fatigue and depression‐risk
Higher DHQ scores showed a dose‐dependent inverse association with fatigue (Table 4), those in the top two quartiles having 11% (95% CI −8%, 27%) and 25% (95% CI 6%, 39%) lower frequencies of fatigue on adjustment for age, sex, MS phenotype, P‐MSSS, and anti‐fatigue medication. Associations were strongest for fat, takeaway, and fruit/vegetable subdomains (Table S5). Meat and dairy consumption were positively associated with fatigue but both attenuated on adjustment.
TABLE 4.
Cross‐sectional relationships of Diet Habits Questionnaire scores and meat and dairy consumption with clinically significant fatigue at 2.5‐year review.
| n/N (%) | aPR1 | aPR2 | |
|---|---|---|---|
| DHQ score a | |||
| 32–70 | 237/329 (72.0) | 1.00 [Reference] | 1.00 [Reference] |
| >70–80 | 214/310 (69.0) | 0.96 (0.80, 1.15) | 0.99 (0.82, 1.20) |
| >80–89 | 199/340 (58.5) | 0.83 (0.69, 1.00) | 0.89 (0.73, 1.08) |
| >89–100 | 141/287 (49.1) | 0.70 (0.57, 0.86) | 0.75 (0.61, 0.94) |
| Trend | p < 0.001 | p = 0.007 | |
| Consume meat? b | |||
| No | 267/481 (55.5) | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 52/786 (66.8) | 1.18 (1.02, 1.37) | 1.09 (0.94, 1.27) |
| p = 0.027 | p = 0.25 | ||
| Consume dairy? c | |||
| No | 290/526 (55.1) | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 498/737 (67.6) | 1.21 (1.05, 1.40) | 1.15 (0.99, 1.34) |
| p = 0.010 | p = 0.067 | ||
Analyses by log‐binomial regression.
Model 1 adjusted for ongoing symptoms due to recent relapse. Model 2 further adjusted for age, sex, multiple sclerosis (MS) phenotype, P‐MSSS, and anti‐fatigue medication.
Results in boldface denote statistical significance (p < 0.05).
Abbreviations: aPR, adjusted prevalence ratio; DHQ, Diet Habits Questionnaire; P‐MSSS, Patient‐determined MS Severity Score;.
Analyses for DHQ score vs. clinically significant fatigue in Model 1 includes 1,266 people, thus excluding 80 people with missing data. Model 2 includes 1,196 people, thus excluding 150 people with missing data.
Analyses for meat consumption vs. clinically significant fatigue in Model 1 includes 1,267 people, thus excluding 79 people with missing data. Model 2 includes 1,197 people, thus excluding 149 people with missing data.
Analyses for dairy consumption vs. clinically significant fatigue in model 1 includes 1,263 people, thus excluding 83 people with missing data. Model 2 includes 1,193 people, thus excluding 153 people with missing data.
Higher DHQ score showed an inverse association with depression risk; those in the highest quartile had a 48% (95% CI 13%, 69%) lower frequency of depression risk on adjustment for age, sex, MS phenotype, P‐MSSS, clinically significant fatigue, and prescription antidepressant medication (Table 5); those in the second and third quartiles showed inverse trends, but these were not significant. DHQ subdomains associated with depression risk were cereal, fruit/vegetables, fat, fibre, and food choices (Table S6). Meat and dairy consumption were associated with higher frequencies of depression risk but both attenuated and became nonsignifcant on adjustment.
TABLE 5.
Cross‐sectional relationships of Diet Habits Questionnaire scores and meat and dairy consumption with depression risk at 2.5‐year review
| n/N (%) | aPR1 | aPR2 | |
|---|---|---|---|
| DHQ score a | |||
| 32–70 | 74/335 (22.1) | 1.00 [Reference] | 1.00 [Reference] |
| >70–80 | 51/320 (15.9) | 0.72 (0.51, 1.03) | 0.83 (0.57, 1.21) |
| >80–89 | 46/349 (13.2) | 0.62 (0.43, 0.90) | 0.85 (0.58, 1.25) |
| >89–100 | 19/303 (6.3) | 0.30 (0.18, 0.49) | 0.52 (0.31, 0.87) |
| Trend | p < 0.001 | p = 0.024 | |
| Consume meat? b | |||
| No | 53/505 (10.5) | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 137/803 (17.1) | 1.57 (1.14, 2.16) | 1.20 (0.86, 1.66) |
| p = 0.005 | p = 0.28 | ||
| Consume dairy? c | |||
| No | 58/551 (10.5) | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 131/753 (17.4) | 1.61 (1.18, 2.20) | 1.24 (0.90, 1.71) |
| p = 0.002 | p = 0.19 | ||
Analyses by log‐binomial regression.
Model 1 adjusted for ongoing symptoms due to recent relapse. Model 2 further adjusted for age, sex, multiple sclerosis (MS) phenotype, P‐MSSS, clinically significant fatigue, and prescription antidepressant medication.
Results in boldface denote statistical significance (p < 0.05).
Abbreviations: aPR, adjusted prevalence ratio; DHQ, Diet Habits Questionnaire; P‐MSSS, Patient‐determined MS Severity Score.
Analyses for DHQ score vs. depression risk in Model 1 includes 1,307 people, thus excluding 39 people with missing data. Model 2 includes 1,237 people, thus excluding 109 people with missing data.
Analyses for meat consumption vs. depression risk in Model 1 includes 1,308 people, thus excluding 38 people with missing data. Model 2 includes 1,238 people, thus excluding 108 people with missing data.
Analyses for dairy consumption vs. depression risk in Model 1 includes 1,304 people, thus excluding 42 people with missing data. Model 2 includes 1,234 people, thus excluding 112 people with missing data.
Prospective analyses
Baseline diet and change in disability over 2.5 years
No dietary characteristics were associated with a decrease in the level of disability at 2.5 years. Higher baseline DHQ scores were strongly associated with less accumulation of disability over 2.5 years; participants in the top two quartiles had a 41% (95% CI 1%, 65%) and 36% (95% CI −2%, 60%) lower risk of worse disability at the 2.5‐year follow‐up (Table 6). Assessment of continuous change in P‐MSSS (Table 7) also showed that a higher DHQ score was associated with less disability; those in the top two quartiles had 0.30 (95% CI 0.07, 0.53) and 0.27 (95% CI 0.04, 0.49) points less disability. Of DHQ subdomains, the association was most evident for fat and fibre (Tables S7 and S8).
TABLE 6.
Prospective relationships of baseline Diet Habits Questionnaire scores and meat and dairy consumption with subsequent change in Patient‐determined Multiple Sclerosis Severity Score severity, baseline to 2.5‐year review
| n/N (%) | Decrease disability | Increase disability | |||||
|---|---|---|---|---|---|---|---|
| Decrease | Stable | Increase | aRR1 | aRR2 | aRR1 | aRR2 | |
| DHQ score a | |||||||
| 32–70 | 32/267 (12.0) | 198/267 (74.2) | 37/267 (13.9) | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] |
| >70–80 | 21/302 (7.0) | 251/302 (83.1) | 30/302 (9.9) | 0.70 (0.42, 1.15) | 0.77 (0.45, 1.31) | 0.68 (0.44, 1.05) | 0.77 (0.48, 1.21) |
| >80–89 | 27/351 (7.7) | 301/351 (85.8) | 23/351 (6.6) | 0.85 (0.53, 1.36) | 1.03 (0.65, 1.64) | 0.49 (0.30, 0.80) | 0.59 (0.35, 0.99) |
| >89–100 | 25/385 (6.5) | 331/385 (86.0) | 29/385 (7.5) | 0.83 (0.51, 1.36) | 1.02 (0.62, 1.67) | 0.56 (0.36, 0.88) | 0.64 (0.40, 1.02) |
| Trend | p = 0.61 | p = 0.73 | p = 0.009 | p = 0.048 | |||
| Consume meat? b | |||||||
| No | 29/523 (5.5) | 461/523 (88.2) | 33/523 (6.3) | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 76/781 (9.7) | 619/781 (79.3) | 86/781 (11.0) | 1.28 (0.85, 1.92) | 1.17 (0.78, 1.74) | 1.86 (1.25, 2.75) | 1.76 (1.17, 2.63) |
| p = 0.23 | p = 0.45 | p = 0.002 | p = 0.006 | ||||
| Consume dairy? c | |||||||
| No | 41/565 (7.3) | 483/565 (85.5) | 41/565 (7.3) | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] |
| Yes | 64/730 (8.8) | 589/730 (80.7) | 77/730 (10.6) | 1.00 (0.69, 1.43) | 0.93 (0.75, 1.34) | 1.47 (1.02, 2.11) | 1.36 (0.93, 1.99) |
| p = 0.98 | p = 0.71 | p = 0.039 | p = 0.11 | ||||
Analyses by log‐multinomial regression. Model 1 adjusted for baseline and 2.5‐year ongoing symptoms due to recent relapse. Model 2 further adjusted for age, sex, multiple sclerosis (MS) phenotype, socioeconomic status, and baseline clinically significant fatigue.
Results in boldface denote statistical significance (p < 0.05).
Abbreviations: aRR, adjusted risk ratio; DHQ, Diet Habits Questionnaire; P‐MSSS, Patient‐determined MS Severity Score.
Analyses for DHQ score vs. disability in model 1 includes 1,291 people, thus excluding 55 people with missing data. Model 2 includes 1,207 people, thus excluding 139 people with missing data.
Analyses for meat consumption vs. disability in model 1 includes 1,290 people, thus excluding 56 people with missing data. Model 2 includes 1,206 people, thus excluding 140 people with missing data.
Analyses for dairy consumption vs. disability in Model 1 includes 1,281 people, thus excluding 65 people with missing data. Model 2 includes 1,201 people, thus excluding 145 people with missing data.
TABLE 7.
Prospective relationships of baseline Diet Habits Questionnaire scores and meat and dairy consumption with subsequent change in continuous Patient‐determined Multiple Sclerosis Severity Score, baseline to 2.5‐year review
| n (%) | aβ (95% CI) a | aβ (95% CI) b | |
|---|---|---|---|
| DHQ score a | |||
| 32–70 | 267 (20.5) | 0.00 [Reference] | 0.00 [Reference] |
| >70–80 | 302 (23.1) | −0.13 (−0.36, 0.09) | −0.12 (−0.36, 0.11) |
| >80–89 | 351 (26.9) | −0.31 (−0.53, −0.09) | −0.30 (−0.53, −0.07) |
| >89–100 | 385 (29.5) | −0.27 (−0.49, −0.06) | −0.27 (−0.49, −0.04) |
| Trend | p = 0.006 | p = 0.010 | |
| Consume meat? b | |||
| No | 523 (40.1) | 0.00 [Reference] | 0.00 [Reference] |
| Yes | 781 (59.9) | 0.19 (0.04, 0.35) | 0.18 (0.02, 0.33) |
| p = 0.014 | p = 0.031 | ||
| Consume dairy? c | |||
| No | 565 (43.6) | 0.00 [Reference] | 0.00 [Reference] |
| Yes | 730 (56.4) | 0.19 (0.04, 0.34) | 0.19 (0.04, 0.35) |
| p = 0.015 | p = 0.017 | ||
Analyses by linear regression. Model 1 adjusted for baseline and 2.5‐year ongoing symptoms due to recent relapse and baseline P‐MSSS. Model 2 further adjusted for age, sex, multiple sclerosis (MS) phenotype, socioeconomic status, and baseline clinically significant fatigue.
Results in boldface denote statistical significance (p < 0.05).
Abbreviations: DHQ, Diet Habits Questionnaire; P‐MSSS, Patient‐deterimined MS Severity Score.
Analyses for DHQ score vs. disability in Model 1 includes 1,291 people, thus excluding 55 people with missing data. Model 2 includes 1,207 people, thus excluding 139 people with missing data.
Analyses for meat consumption vs. disability in model 1 includes 1,290 people, thus excluding 56 people with missing data. Model 2 includes 1,206 people, thus excluding 140 people with missing data.
Analyses for dairy consumption vs. disability in Model 1 includes 1,281 people, thus excluding 65 people with missing data. Model 2 includes 1,201 people, thus excluding 145 people with missing data.
Baseline meat consumption was associated with an 86% (95% CI 25%, 175%) higher risk of increasing disability, while for continuous disability progression, meat consumption was associated with 0.19 (95% CI 0.04, 0.35) points higher progression, both robust to adjustment for age, sex, PRSES, MS phenotype, and baseline fatigue. Baseline dairy consumption was associated with 0.19 points higher continuous change in disability, robust to adjustment, though the association of dairy consumption with risk of increasing disability did not persist on adjustment.
Baseline diet and subsequent change in fatigue and depression risk
Baseline DHQ scores were not associated with a change in fatigue (data not shown). The food preparation subdomain showed a positive association with loss of fatigue, while the fat subdomain (>3.9–4.4) showed an inverse association with a gain in fatigue score. Neither meat nor dairy consumption was associated with change in fatigue.
There were no associations between the DHQ total or subdomains scores and depression risk (data not shown).
DISCUSSION
We found that a better quality of diet, as measured by a higher DHQ score, was cross‐sectionally associated with lower levels of disability. Prospective analyses showed that participants in the top two quartiles of the total DHQ scores at baseline had roughly 0.30 points lower disability progression at 2.5 years, most apparent for the fruit/vegetable, fat and fibre subdomains. Meat consumption showed cross‐sectional and prospective associations with disability; baseline consumption was associated with 0.18 points higher disability progression over subsequent follow‐up. DHQ scores were associated with less fatigue and depression risk cross‐sectionally, but not prospectively.
In our previous baseline assessment of this cohort, we found 3% lower PDDS for each 1‐unit higher DHQ score [19], this driven by the fruit/vegetable and fat DHQ subdomains. In the present study, we have substantiated these findings, both cross‐sectionally at 2.5 years and prospectively for change in disability severity and disability progression. We again showed associations were driven by fruit/vegetable and fat subdomains. Associations for severe disability were similar (29% reduction), while for moderate disability no association was found at 2.5 years. This difference may be attributed to differences in the covariates adjusted for, particularly ongoing symptoms due to a recent relapse [23].
Studies using the North American Research Committee on MS (NARCOMS) cohort (n = 6,989), cross‐sectionally showed a dose‐dependent relationship between higher diet quality and lower PDDS; participants in the top quintile had 20% lower odds of higher disability than the bottom quintile, attributed to dairy and wholegrain subdomains [12]. While overall diet quality associations with disability aligns with our results, the subdomain associations differ. This may be attributable to the different tools used to assess diet and disability, statistical models, and cohort differences. In contrast, findings from the Australian MS Longitudinal Study (AMSLS; n = 1,490) found no associations between diet quality and disability [15]. The disparity may reflect differences in methodology, including the different dietary instrument used, as well as cohort characteristics, including BMI, moderate/severe disability, and a higher proportion using DMTs. In addition, the randomized controlled trial (RCT) by Yadav et al. [23], which randomized participants with MS to either a low‐fat plant‐based diet (n = 32) or wait‐listed controls (n = 29), found no difference in disability at the 12‐month time point. This disparity in results can be attributed to differences in methodology (the study by Yadav et al. was an RCT while the present study was observational), the nature of the exposure (in the present study this was overall diet quality whereas in the study by Yadav et al. it was a specific diet programme), and the follow‐up duration and sample size. Further investigation of this relationship in other cohorts would be warranted, preferably using consistent measures of exposure and outcomes between studies.
The magnitude of associations observed for diet quality and meat/dairy consumption with disability are not large relative to the scale of the P‐MSSS (0–9.85), reflecting the relatively limited change in P‐MSSS over the 2.5‐year interval and the low level of disability in the cohort at baseline. Despite this, our prospective analyses found that those in the highest quartiles of baseline DHQ had 41% and 36% lower risks of increasing disability over 2.5 years. It may be that differences in absolute disability by diet may be greater [12] over a longer follow‐up period or in a cohort that is less skewed to lower disability or with a shorter disease duration. Replication of these results is recommended.
For fatigue, our cross‐sectional 2.5‐year results are in line with our prior baseline findings, where those in the lowest quartile of DHQ score had a threefold greater frequency of fatigue, although this attenuated on adjustment [22]. Conversely, others have found no relationship of diet quality with fatigue [12, 15]. This disparity may relate to differences in the cohort or the modes of assessment. The lack of prospective associations between the quality of the diet and fatigue is an interesting conflict since the modified Paleolithic diet proposed by the Wahls group has had success with fatigue as an outcome, both in smaller RCTs compared to wait‐listed controls [24, 39] and in a larger RCT compared to the Swank low‐saturated‐fat diet [25]. Given this conflict, further research using observational study designs to assess the prospective relationship of a healthier diet with fatigue should be undertaken.
For depression risk, our cross‐sectional results are in concordance with our prior findings at baseline, where those in the bottom quartile of DHQ had a 2.7‐fold greater risk of depression [21]. They also align with the studies by Fitzgerald et al. [12] and Marck et al. [15] showing associations between diet quality and depression risk. In the former, participants in the highest quintiles of total diet scores had a 28% lower frequency of severe depression, and in the latter, participants in the top quintiles had a 2.0 and 2.2‐points lower depression score. However, we did not observe prospective associations with depression risk. The extent to which reverse causality may be at play here warrants further study.
There is significant biological plausibility for the observed associations between diet and clinical outcomes [40]. This includes BMI [41], given the deleterious effects of inflammatory adipokines and sequestration of circulating vitamin D metabolites [42, 43]. In parallel with adiposity is dyslipidaemia, as total cholesterol and low density lipoprotein levels have been associated with disability progression [41, 44]. There are also potential roles for specific elements of diet, such as fatty acids, which have been correlated with neuronal function and MS [45, 46]. We were unable to assess serum lipid or fatty acid levels using our cohort but it is a worthwhile investigation for other studies.
Associations seen for the fruit/vegetables and fibre subdomains may suggest immune system impacts via their effect on the gut microbiome [47]. This is in line with recent findings, including a pilot study by Saresella et al. [48] showing a high‐vegetable/low‐protein diet changed the microbiome, increasing Lachnospiraceae flora and altering the fractions of circulating lymphocytes and monocytes. Also, in the experimental autoimmune encephalitis animal model, Berer et al. [49] found that mice on a cellulose‐enriched diet had half the frequency of experimental autoimmune encephalitis compared with mice on a standard diet, attributing this to an altered immune response toward a Th2 profile due to a markedly altered gastrointestinal microbiome. This suggests some promise for healthy and particularly high‐fibre plant‐based diets in altering the immune profile and thereby moderating clinical progression in MS. Of note, the RCT by Yadav et al. [23] did examine a plant‐based diet and found no differences in relapse rate, disability, or MRI outcomes between the two groups. Again, the disparity in results may reflect differences in the study design and it is notable that, while Yadav et al. did examine serum lipid profile and insulin, they did not examine microbiome. Further studies examining the microbiome are warranted.
Meat consumption showed a robust prospective association with disability progression. However, the method of assessment is limited by not explicitly querying whether and how much of various meats, poultry, and seafood were consumed. The mode of assessing dairy consumption was likewise limited. This may account for failure to find consistent associations of dairy consumption with outcomes, while meat associations should be interpreted with caution.
Our study is the first to prospectively examine the relationship of the quality of the diet with disability, fatigue, and depression risk in people with MS. Comprehensive assessment of clinical, demographic and lifestyle factors have enabled a robust assessment of the statistical independence of diet and these outcomes. However, the study has some limitations. All exposure and outcome data were self‐reported. However, patient‐reported outcome measures are an increasingly utilized metric to assess clinical outcomes, and measurement tools used for assessing disability, fatigue and depression have previously been validated [50, 51, 52]. Nonetheless, there is potential for recall bias in self‐reported measures. Our cohort is susceptible to participation bias in lifestyle behaviours due to the websites used for recruitment advocating for a healthy lifestyle programme [31]. This may reduce the generalizability of the cohort although our findings for diet are in broad agreement with the NARCOMS results [12] where specific diet programme adherence was not high [30]. Our cohort experienced appreciable attrition, with 54.6% retained at follow‐up. This retention was greater among those of higher education, employment, less clinical severity, and particularly a tendency toward healthy lifestyle behaviours, including diet. However, we assessed these covariates in multivariable models, showing that the associations of a quality diet persisted on adjustment. A further limitation is the nature of the dietary assessment, which was by recall questionnaire, rather than a prospective recording such as a food record or diet history interview. The DHQ was developed for an Australian cardiac population, and the modifications were not validated for use in an MS patient population. Finally, there is the potential for differential information bias given participants reported both exposure and outcome measures; people with more severe clinical presentation could report behaviour differently. The objective measures of outcomes to quantify and control for this bias could be considered for future studies. This bias could also impact on attrition, persons with greater clinical severity or better health behaviours being differently inclined to participate at follow‐up.
Despite some healthy participant bias, particularly as related to diet quality, with a higher median DHQ score than that seen elsewhere [12, 15], we believe our findings are generalizable to the general MS population, both in terms of clinical and demographic characteristics, as well as including participants from countries with some of the highest frequencies of MS globally. We have endeavoured to control for healthy participant bias in multivariable models.
In conclusion, our results indicate a beneficial relationship between better quality of diet, potentially including reduced meat consumption, and less disability progression. While there was no prospective association between diet and fatigue, there was some evidence that improved diet scores were associated with a decreased depression risk. Taken together, the internal and external consistency, dose‐dependency, and biological plausibility indicate that there is substantial evidence for a relationship between quality of the diet and disability in people with MS. Pending validation with further research, this could inform interventions to reduce disability progression in MS.
CONFLICT OF INTEREST
George A. Jelinek receives royalties for his books, Overcoming Multiple Sclerosis and Recovering from Multiple Sclerosis. George A. Jelinek and Sandra L. Neate received remuneration for conducting lifestyle educational workshops for people with MS.
AUTHOR CONTRIBUTIONS
Steve Simpson‐Yap: Conceptualization (lead); Data curation (lead); Formal analysis (lead); Investigation (lead); Writing − original draft (lead); Writing − review and editing (lead). Nupur Nag: Project administration (equal); Resources (equal); Writing − review and editing (equal). Yasmine Probst: Writing − review and editing (equal). George A. Jelinek: Conceptualization (equal); Funding acquisition (lead); Project administration (supporting); Writing − review and editing (equal). Sandra L. Neate: Project administration (lead); Resources (lead); Writing − review and editing (equal).
Supporting information
{kind=link}
ACKNOWLEDGEMENTS
We express our sincere thanks to Wal Pisciotta and anonymous philanthropic funders for their support for the Neuroepidemiology Unit and the HOLISM Study. We also acknowledge the work of our Honours student, Ms Hafsa Ali, for her work on an earlier version of this project. We are also indebted to the participants of the HOLISM Study, without which this study could not have been conducted.
Simpson‐Yap S, Nag N, Probst Y, Jelinek G, Neate S. Higher‐quality diet and non‐consumption of meat are associated with less self‐determined disability progression in people with multiple sclerosis: A longitudinal cohort study. Eur J Neurol. 2022;29:225–236. 10.1111/ene.15066
Funding information
The study was funded by the Wal Pisciotta, and other anonymous philanthropic funders
DATA AVAILABILITY STATEMENT
Data may not be shared due to the conditions approved by our institutional ethics committee, in that all data are stored as re‐identifiable information at the University of Melbourne in the form of password‐protected computer databases, and only the listed investigators have access to the data. All data have been reported on a group basis, summarizing the group findings rather than individual findings so personal information cannot be identified. Therefore, we can supply aggregate group data on request. Readers may contact Dr Steve Simpson‐Yap.
REFERENCES
- 1. Compston A, McDonald I, Noseworthy JH, et al. McAlpine's Multiple Sclerosis, 4th edn. Churchill Livingston; 2005. [Google Scholar]
- 2. Krupp L. Fatigue is intrinsic to multiple sclerosis (MS) and is the most commonly reported symptom of the disease. Mult Scler. 2006;12:367‐368. [DOI] [PubMed] [Google Scholar]
- 3. Rodgers S, Calabrese P, Ajdacic‐Gross V, et al. Major depressive disorder subtypes and depression symptoms in multiple sclerosis: what is different compared to the general population? J Psychosom Res. 2021;144:110402. [DOI] [PubMed] [Google Scholar]
- 4. Claflin SB, van der Mei IAF, Taylor BV. Complementary and alternative treatments of multiple sclerosis: a review of the evidence from 2001 to 2016. J Neurol Neurosurg Psychiatry. 2018;89:34‐41. [DOI] [PubMed] [Google Scholar]
- 5. Esposito S, Bonavita S, Sparaco M, Gallo A, Tedeschi G. The role of diet in multiple sclerosis: a review. Nutr Neurosci. 2018;21:377. [DOI] [PubMed] [Google Scholar]
- 6. Katz SI. The role of diet in multiple sclerosis: mechanistic connections and current evidence. Curr Nutr Rep. 2018;7:150‐160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ireland P, Jolley D, Giles G, et al. Development of the Melbourne FFQ: a food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pac J Clin Nutr. 1994;3:19‐31. [PubMed] [Google Scholar]
- 8. Bingham SA, Welch AA, McTaggart A, et al. Nutritional methods in the European prospective investigation of cancer in Norfolk. Public Health Nutr. 2001;4:847‐858. [DOI] [PubMed] [Google Scholar]
- 9. McKellar S, Horsely P, Chambers R. Development of the diet habits questionnaire for use in cardiac rehabilitation. Austr J Prim Health. 2008;14:43‐47. [Google Scholar]
- 10. Black LJ, Baker K, Ponsonby AL, van der Mei I, Lucas RM, Pereira G. A higher Mediterranean diet score, including unprocessed red meat, is associated with reduced risk of central nervous system demyelination in a case‐control study of Australian adults. J Nutr. 2019;149:1385‐1392. [DOI] [PubMed] [Google Scholar]
- 11. Black LJ, Rowley C, Sherriff J, Pereira G, Ponsonby AL, Lucas RM. A healthy dietary pattern associates with a lower risk of a first clinical diagnosis of central nervous system demyelination. Mult Scler. 2018;25:1514‐1525. [DOI] [PubMed] [Google Scholar]
- 12. Fitzgerald KC, Tyry T, Salter A, et al. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology. 2018;90:e1‐e11. [DOI] [PubMed] [Google Scholar]
- 13. Mousavi‐Shirazi‐Fard Z, Mazloom Z, Izadi S, Fararouei M. The effects of modified anti‐inflammatory diet on fatigue, quality of life, and inflammatory biomarkers in relapsing‐remitting multiple sclerosis patients: a randomized clinical trial. Int J Neurosci. 2020;131(7):657‐665. [DOI] [PubMed] [Google Scholar]
- 14. Pommerich UM, Brincks J, Christensen ME. Is there an effect of dietary intake on MS‐related fatigue? ‐ A systematic literature review. Mult Scler Relat Disord. 2018;25:282‐291. [DOI] [PubMed] [Google Scholar]
- 15. Marck CH, Probst Y, Chen J, Taylor B, van der Mei I. Dietary patterns and associations with health outcomes in Australian people with multiple sclerosis. Eur J Clin Nutr. 2021. 10.1038/s41430-021-00864-y [DOI] [PubMed] [Google Scholar]
- 16. Rotstein DL, Cortese M, Fung TT, Chitnis T, Ascherio A, Munger KL. Diet quality and risk of multiple sclerosis in two cohorts of US women. Mult Scler. 2018;25:1352458518807061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Machado SB, Cabral R, Murade N, Ares NC, Scorcine C, Fragoso YD. Dietary habits in a group of patients with multiple sclerosis are similar to those of healthy control subjects. Arq Neuropsiquiatr. 2020;78:638‐641. [DOI] [PubMed] [Google Scholar]
- 18. Pommerich UM, Nielsen R, Overvad K, et al. Diet quality is not associated with late‐onset multiple sclerosis risk‐ A Danish Cohort Study. Mult Scler Relat Disord. 2020;40:101968. [DOI] [PubMed] [Google Scholar]
- 19. Hadgkiss EJ, Jelinek GA, Weiland TJ, Pereira NG, Marck CH, van der Meer DM. The association of diet with quality of life, disability, and relapse rate in an international sample of people with multiple sclerosis. Nutr Neurosci. 2015;18:125‐136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Jelinek GA, De Livera AM, Marck CH, et al. Associations of lifestyle, medication, and socio‐demographic factors with disability in people with multiple sclerosis: an international cross‐sectional study. PLoS ONE. 2016;11:e0161701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Taylor KL, Hadgkiss EJ, Jelinek GA, et al. Lifestyle factors, demographics and medications associated with depression risk in an international sample of people with multiple sclerosis. BMC Psychiatry. 2014;14:327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Weiland TJ, Jelinek GA, Marck CH, et al. Clinically significant fatigue: prevalence and associated factors in an international sample of adults with multiple sclerosis recruited via the internet. PLoS ONE. 2015;10:e0115541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Yadav V, Marracci G, Kim E, et al. Low‐fat, plant‐based diet in multiple sclerosis: a randomized controlled trial. Mult Scler Relat Disord. 2016;9:80‐90. [DOI] [PubMed] [Google Scholar]
- 24. Bisht B, Darling WG, White EC, et al. Effects of a multimodal intervention on gait and balance of subjects with progressive multiple sclerosis: a prospective longitudinal pilot study. Degener Neurol Neuromuscul Dis. 2017;7:79‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Wahls T, Watson K, Turpin R, Tsuyuki R. P0208 ‐ Effects of Wahls elimination and swank dietary patterns on multiple sclerosis related fatigue, quality of life, processing speed and waking distance. MSVirtual. 2020;2020. [Google Scholar]
- 26. Hadgkiss EJ, Jelinek GA, Weiland TJ, et al. Health‐related quality of life outcomes at 1 and 5 years after a residential retreat promoting lifestyle modification for people with multiple sclerosis. Neurol Sci. 2013;34:187‐195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Wahls TL, Chenard CA, Snetselaar LG. Review of two popular eating plans within the multiple sclerosis community: low saturated fat and modified paleolithic. Nutrients. 2019;11:352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Jelinek GA. Overcoming multiple sclerosis: the evidence‐based 7 step recovery program, 2nd edn. Allen & Unwin; 2016. [Google Scholar]
- 29. McDougall J, McDougall M. The healthiest diet on the planet. HarperCollins Publishers Inc.; 2016. [Google Scholar]
- 30. Fitzgerald KC, Tyry T, Salter A, et al. A survey of dietary characteristics in a large population of people with multiple sclerosis. Mult Scler Relat Disord. 2018;22:12‐18. [DOI] [PubMed] [Google Scholar]
- 31. Hadgkiss EJ, Jelinek GA, Weiland TJ, Pereira NG, Marck CH, van der Meer DM. Methodology of an International study of people with multiple sclerosis recruited through Web 2.0 platforms. Demographics, Lifestyle, and Disease Characteristics. Neurol Res Int. 2013;2013:580596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Weiland TJ, De Livera AM, Brown CR, et al. Health outcomes and lifestyle in a sample of people with multiple sclerosis (HOLISM): longitudinal and validation cohorts. Front Neurol. 2018;9:1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire: 12‐country reliability and validity. Med Sci Sports Exerc. 2003;35:1381‐1395. [DOI] [PubMed] [Google Scholar]
- 34. Hohol MJ, Orav EJ, Weiner HL. Disease steps in multiple sclerosis: a simple approach to evaluate disease progression. Neurology. 1995;45:251‐255. [DOI] [PubMed] [Google Scholar]
- 35. Kister I, Chamot E, Salter AR, Cutter GR, Bacon TE, Herbert J. Disability in multiple sclerosis: a reference for patients and clinicians. Neurology. 2013;80:1018‐1024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Krupp LB, LaRocca NG, Muir‐Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46:1121‐1123. [DOI] [PubMed] [Google Scholar]
- 37. Kroenke K, Spitzer RL, Williams JB. The patient health questionnaire‐2: validity of a two‐item depression screener. Med Care. 2003;41:1284‐1292. [DOI] [PubMed] [Google Scholar]
- 38. Taylor KL, Simpson S Jr, Jelinek GA, et al. Longitudinal associations of modifiable lifestyle factors with positive depression‐screen over 2.5‐years in an international cohort of people living with multiple sclerosis. Front Psychiatry. 2018;9:526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Irish AK, Erickson CM, Wahls TL, Snetselaar LG, Darling WG. Randomized control trial evaluation of a modified Paleolithic dietary intervention in the treatment of relapsing‐remitting multiple sclerosis: a pilot study. Degener Neurol Neuromuscul Dis. 2017;7:1‐18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Esposito S, Bonavita S, Sparaco M, Gallo A, Tedeschi G. The role of diet in multiple sclerosis: a review. Nutr Neurosci. 2018;21:377‐390. [DOI] [PubMed] [Google Scholar]
- 41. Tettey P, Simpson S, Taylor B, et al. An adverse lipid profile and increased levels of adiposity significantly predict clinical course after a first demyelinating event. J Neurol Neurosurg Psychiatry. 2017;88:395‐401. [DOI] [PubMed] [Google Scholar]
- 42. Guerrero‐García JJ, Carrera‐Quintanar L, López‐Roa RI, Márquez‐Aguirre AL, Rojas‐Mayorquín AE, Ortuño‐Sahagún D. Multiple sclerosis and obesity: possible roles of adipokines. Mediators Inflamm. 2016;2016:4036232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72:690‐693. [DOI] [PubMed] [Google Scholar]
- 44. Tettey P, Simpson S Jr, Taylor B, et al. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult Scler. 2014;20:1737‐1744. [DOI] [PubMed] [Google Scholar]
- 45. Hoare S, Lithander F, van der Mei I, Ponsonby AL, Lucas R. Higher intake of omega‐3 polyunsaturated fatty acids is associated with a decreased risk of a first clinical diagnosis of central nervous system demyelination: results from the ausimmune study. Mult Scler. 2016;22:884‐892. [DOI] [PubMed] [Google Scholar]
- 46. Hon G, Hassan M, van Rensburg SJ, et al. Immune cell membrane fatty acids and inflammatory marker, C‐reactive protein, in patients with multiple sclerosis. Br J Nutr. 2009;102:1334‐1340. [DOI] [PubMed] [Google Scholar]
- 47. Riccio P, Rossano R. Diet, gut microbiota, and vitamins D + A in multiple sclerosis. Neurotherapeutics. 2018;15:75‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Saresella M, Mendozzi L, Rossi V, et al. Immunological and clinical effect of diet modulation of the gut microbiome in multiple sclerosis patients: a pilot study. Front Immunol. 2017;8:1391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Berer K, Martínez I, Walker A, et al. Dietary non‐fermentable fiber prevents autoimmune neurological disease by changing gut metabolic and immune status. Sci Rep. 2018;8:10431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Hohol MJ, Orav EJ, Weiner HL. Disease steps in multiple sclerosis: a longitudinal study comparing disease steps and EDSS to evaluate disease progression. Mult Scler. 1999;5:349‐354. [DOI] [PubMed] [Google Scholar]
- 51. Amtmann D, Kim J, Chung H, et al. Comparing CESD‐10, PHQ‐9, and PROMIS depression instruments in individuals with multiple sclerosis. Rehabil Psychol. 2014;59:220‐229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Flachenecker P, Kumpfel T, Kallmann B, et al. Fatigue in multiple sclerosis: a comparison of different rating scales and correlation to clinical parameters. Mult Scler. 2002;8:523‐526. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data may not be shared due to the conditions approved by our institutional ethics committee, in that all data are stored as re‐identifiable information at the University of Melbourne in the form of password‐protected computer databases, and only the listed investigators have access to the data. All data have been reported on a group basis, summarizing the group findings rather than individual findings so personal information cannot be identified. Therefore, we can supply aggregate group data on request. Readers may contact Dr Steve Simpson‐Yap.