

Abstract
Background
Minimally invasive procedures, such as thread suspension techniques, are a growing trend for facial rejuvenation. However, not enough data are available on the efficacy, outcomes, and morbidity of suture suspension techniques in mid‐face reshaping.
Aims
Our goal was to assess treatment outcomes and patient satisfaction following mid‐face reshaping using threads with bidirectional convergent barbs (DefinisseTM free floating threads).
Patients/Methods
We performed a retrospective analysis of 60 patients who underwent treatment for mid‐face reshaping using DefinisseTM free floating threads. Response to treatment was assessed at 6 months using the mid‐face‐specific Mid‐Face Volume Deficit scale (Allergan®), Global Aesthetic Improvement and FACE‐QTM scales.
Results
Sixty patients underwent mid‐face treatment with the suspension thread technique (mean age 51.3, 90% female). No concomitant procedures were done. A reduction by one point or more in the Mid‐Face Volume Deficit Scale (MDFVS) score treatment was seen in all patients after 6 months. Mean overall MFVDS and FACE‐QTM scores were significantly improved. On the GAIS, most patients were rated as improved or better both by the evaluating investigators and during self‐assessment. No major complications were observed, and none of the patients requested the removal of the threads (mean follow‐up 9.8 months, range 6–14 months).
Conclusion
Our results suggest that mid‐face reshaping with DefinisseTM free floating threads is a safe and reliable procedure characterized by low complication rates and good esthetic results. This minimally invasive procedure is a good alternative for normal or combination skin patients who refuse or want to delay the need for traditional rhytidectomy.
Keywords: bidirectional threads, mid‐face lift, minimally invasive
1. INTRODUCTION
Facial aging is a dynamic process involving dramatic changes in different structures of the face, 1 , 2 including skin, soft tissues, and facial skeleton. 3 , 4 In the last decade, there has been a significant paradigm shift in the field of rejuvenation surgery with the spreading of minimally invasive techniques for facial rejuvenation instead of more invasive surgically oriented modalities. 5 More and more patients ask for procedures with a short recovery time to get rapidly back to work. The growing trend nowadays is to seek high‐quality results with the least invasive treatment possible and with less risk and downtime. In many situations, patients prefer minimally invasive procedures and are willing to trade a more modest degree of esthetic improvement in exchange for decreased morbidity. 6 A large variety of injectable fillers and structural fat grafts may be combined with neurotoxins to resolve superficial wrinkles and restore facial volumes. 7 Indeed, rejuvenation with soft tissue fillers, while providing the opportunity for volumetric restoration to the aging face, often fails to provide adequate soft tissue repositioning and, in certain situations, may result in puffiness with unnatural facial appearance. In recent years, thread lifts are becoming popular since they enable the correction and repositioning of soft tissue laxity and ptosis, ensuring short recovery time, fewer complications, limited scarring, and lower costs. 8 , 9 , 10 These minimally invasive procedures may be performed separately or in combination with other facial surgical interventions. However, there is a lively debate about efficacy, long‐term outcomes, and morbidity of suture suspension techniques, and only a few reliable studies have analyzed its use in large cohorts. 11 , 12
In the present study, we used the suspension thread technique with DefinisseTM free floating threads for facial rejuvenation. DefinisseTM free floating threads are monofilament, absorbable skin support of synthetic origin, belonging to Class III of medical devices according to Rule 8 of Annex IX of the Legislative Decree n.46/1997, as amended, which is the Italian transposition of the Medical Device Directive 93/42 EEC as amended. 13
DefinisseTM free floating threads are characterized by a special kind of barbs, created by a unique technology that does not reduce thread gauge. 11 The presence of these barbs and their tri‐dimensional geometry (length, number per unit of length, angulation, and spatial distribution) are essential for the interaction of the sutures with the surrounding tissue; in fact, their tri‐dimensional geometry is specifically developed to obtain an intense mechanical stimulation of fibroblasts. 14
The interaction of the DefinisseTM free floating threads with the surrounding tissue provides a dual effect. Through a mechanical effect, this interaction gives support and allows the repositioning of tissues, inducing a lifting action, while the barbs and the molecules poly‐L‐lactic acid and caprolactone stimulate the synthesis of collagen, hyaluronic acid, and elastin inducing a revitalizing action. 11 Furthermore, the fibrous capsule formed around the inserted thread prolongs the lifting effect and maintains the skin traction. 14 In addition, it also protects the thread from hydrolysis, extending its permanence in the tissue. This translates into a simultaneous mechanical and histological lifting effect. 11
The goal of this study is to report treatment outcomes and patient satisfaction following mid‐face reshaping with DefinisseTM free floating threads.
2. METHODS
This is a single‐center, observational, retrospective study conducted between May 2018 and September 2019 (enrollment and follow‐up) in patients who underwent treatment for mid‐face reshaping using DefinisseTM free floating threads.
The data collected included the following: age and sex of patients; number of threads used; Mid‐Face Volume Deficit Scale scores; self‐assessed Face‐QTM scores; preoperative and postoperative 3D photographs using the 3D Vectra H2 system (Canfield Scientific, NJ); and intraoperative and postoperative complications. Absolute contraindications to the treatment are recognizable personality disorders; previous injection of non‐absorbable filler in the same treatment area; unrealistic patient expectations; anticoagulant therapy/bleeding disorders; use of illegal medication/substance abuse; intolerance for or allergic to lidocaine or epinephrine; severe systemic illness; intolerance for or allergic to PLL and/or PCL; immunologically compromising diseases; facial and/or scalp eczema or psoriasis; local or systemic infection; history of keloids or hypertrophic scarring; acne/rosacea at or near the thread entry/exit points; uncontrolled diabetes; pregnancy and breastfeeding; and use of blood thinners. Relative contraindications are mild acne; non‐infectious gastrointestinal conditions; conditions affecting skin pigmentation; intolerance for or allergic to lidocaine; or epinephrine. Efficacy assessments were performed at the 6‐month follow‐up visit.
Mid‐face reshaping with DefinisseTM free floating threads was performed under local anesthesia using 2.5 ml of carbocaine with adrenaline (1:200 000) for each side (5 ml in total). Preoperative markings were performed with the patient in the sitting position, and four threads were used for each patient (two on each side), except in two patients with hemifacial paralysis. In these patients, two threads were used on the normal side and four threads on the side with paralysis. Threads were introduced through a 20‐gauge 90 mm needle‐cannula.
We performed the procedure as follows (Figure 1). First, we identified and marked a 1‐cm‐diameter target area with the part of the thread without barbs. The target area is the area in the malar zone in which volume reposition of the collapsed fat compartments needs to be improved. After marking the target area, we mark four symmetrical entry and four exit points crossed at 30 degrees (2 entry and 2 exit points per side). Entry points must be at least 3 cm away from the target area to have enough grip to reposition the compartment. Exit points are marked caudally at the same distance so that the part of the thread without barbs is perfectly in the target area (IN1‐Target=Target‐OUT1 and IN2‐Target=Target‐OUT2, Figure 1). The technique was named Soft Tissue Reshaping‐2 (STR‐2).
FIGURE 1.
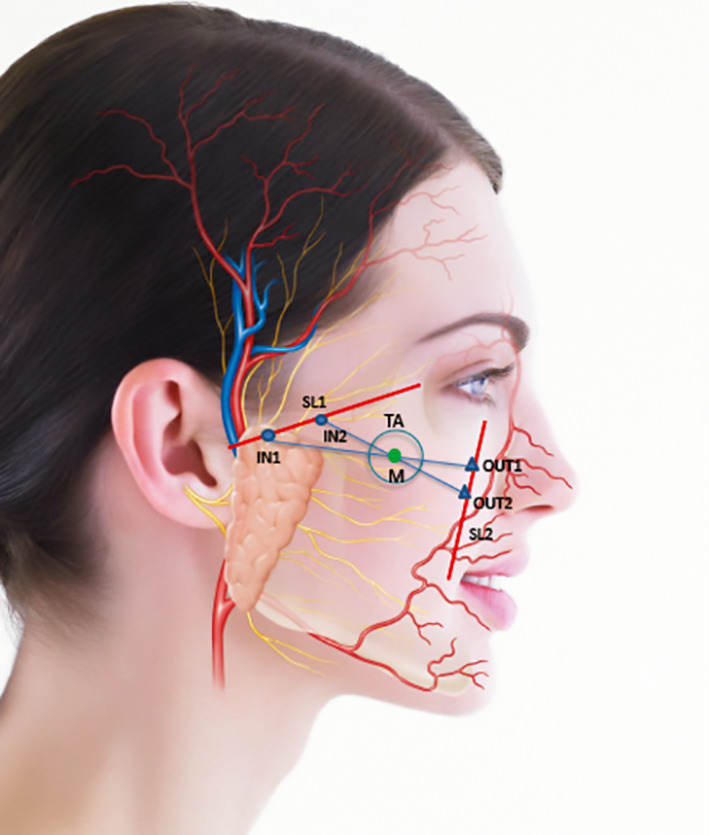
Soft Tissue Reshaping‐2 Technique
All treatment marks were included in the safety area, delimited by two lines excluding dangerous areas: the first line from the tragus to the lateral canthal and the second line from the medial canthus to the corner of the mouth.
Ten minutes after the local anesthesia, the procedure was started. The two threads for each side were crossed between them with an angle between 10 and 70 degrees.
Below the zygomatic arch, the needle‐cannula was introduced deeply in the subcutaneous tissue grasping above the Superficial Muscle Aponeurotic System (SMAS) until the OUT point passing for the target area. The thread was introduced gently in the hole of the cannula. After removing the cannula, we ensured that the thread was perfectly symmetrical to the target area by measuring the distance where it is positioned—this is a critical step. The thread is barbed only laterally. The internal part (1 cm) is barbless. We must ensure that the target area (area depressed bus t) corresponds exactly to the barbless region, so when we open the barbs the entire ptotic compartment is lifted to the depressed area. Then, the barbs were opened by massaging the skin. With a pinch, we confirmed that the barbs had gripped the retinacula ligaments, and we cut the part of the thread in excess. Steri‐strips to cover the entry and exit points and fix the skin on threads’ lines may be useful. No particular dressings were necessary after the intervention.
2.1. Response measures
Response to treatment was assessed by overall mid‐face volume deficit (MFVD) on the validated 6‐point MFVD Scale (MFVDS) at baseline and follow‐up (6 months after the procedure). 15 The MFVDS was used with the prior written consent of Allergan. MFVDS was graded by investigators as severe (5), significant (4), moderate (3), mild (2), minimal (1), and none (0).
In addition, treatment outcome was assessed using the 5‐point Global Aesthetic Improvement Scale (GAIS), 6 months after the procedure by investigators and patients (self‐assessment). 16 For GAIS ratings, evaluating investigators and patients compared the live post‐treatment face with a baseline photograph. The level of improvement in cheek volume was assigned as much improved (2), improved (1), no change (0), worse (−1), or much worse (−2).
Patient satisfaction was also assessed at baseline and 6 months using the self‐assessment FACE‐QTM scale. The FACE‐QTM was used with the prior written consent of Memorial Sloan Kettering Cancer Center.
2.2. Statistics
SPSS software (version 17.00, SPSS, Chicago, USA) was used for statistical analysis. Data are presented as mean, SD, number, or percent. Comparisons between baseline and 6‐month MFVDS and FACE‐QTM were performed using paired samples t‐test. Mean GAIS scores at 6 months were compared using a t‐test (unpaired). A value of p < 0.05 was considered statistically significant.
3. RESULTS
A total of 60 patients underwent mid‐face treatment with the suspension threads technique (Table 1). The mean age was 51.3 years. Most patients were female (90% female vs. 10% male). Four threads (two on each side) were used in most cases (n = 58, Figures 2 and 3); in the remaining two patients, six threads were needed. No concomitant procedures were done. The mean follow‐up period was 9.8 months (range 6–14 months), with a minimum follow‐up of 6 months for all patients.
TABLE 1.
Demographic data and baseline characteristics
| Baseline demographics and characteristics | Total |
|---|---|
| Number of subjects, n | 60 |
| Female, n (%) | 54 (90) |
| Age | |
| Mean+/‐ SD | 51.3 +/‐ 8.2 |
| Min‐max | 32–71 |
| MFVDS | |
| Mean score +/‐ SD | 3.03 +/‐ 0.92 |
| Min‐max | 1.0–5.0 |
| FACE‐QTM | |
| Mean score +/‐ SD | 16.12 +/‐ 5.912 |
| Min‐max | 10.0–32.0 |
FIGURE 2.
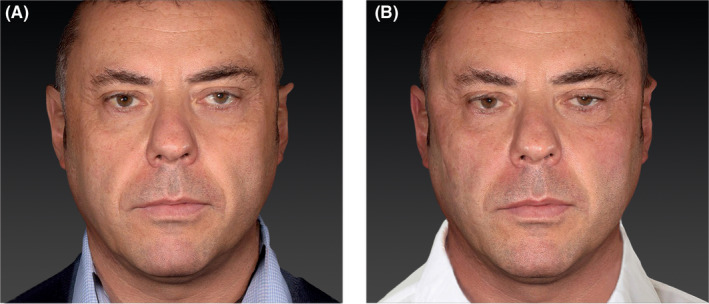
3D photographs of a 47‐year‐old male who underwent mid‐face reshaping using threads with bidirectional convergent barbs. (A) Preoperative photograph. (B) 6 months following the minimally invasive procedure. 3D photographs were taken with the 3D Vectra H2 system
FIGURE 3.
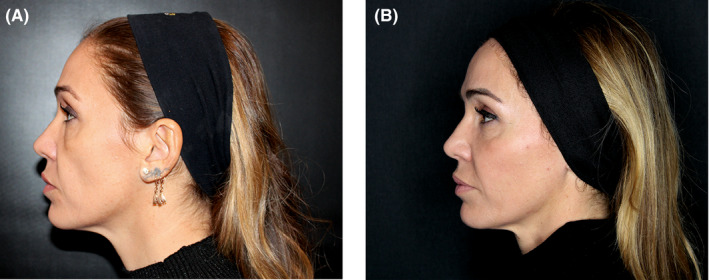
3D photographs of a 42‐year‐old female who underwent mid‐face reshaping using threads with bidirectional convergent barbs. (A) Preoperative photograph. (B) 6 months following the minimally invasive procedure. 3D photographs were taken with the 3D Vectra H2 system
All patients showed a reduction by one point or more in the MDFVS score 6 months after treatment. Changes in mean overall MFVDS scores from baseline were statistically significant (3.03+/‐0.92 vs. 0.63+/‐ 0.581; p < 0.001, Figure 4). On the GAIS, most patients were rated as improved or better both by the evaluating investigators and during self‐assessment (Figure 5). Patient satisfaction with treatment outcome was confirmed with FACE‐QTM grading 6 months after treatment (Figure 6). Mean overall FACE‐QTM scores were significantly increased (improved) at follow‐up in comparison with baseline scores (16.12+/‐5.912 vs. 31.3+/‐5.497, p < 0.001).
FIGURE 4.
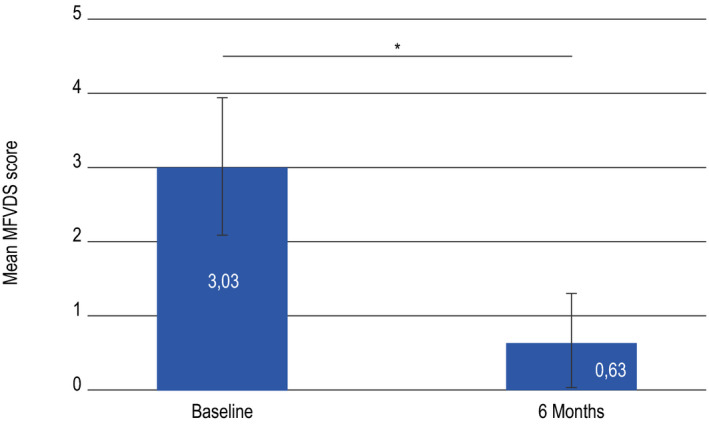
Mean overall Mid‐Face Volume Deficit Scale (MFVDS) Score before treatment (baseline) and at follow‐up (6 months). *p < 0.001
FIGURE 5.
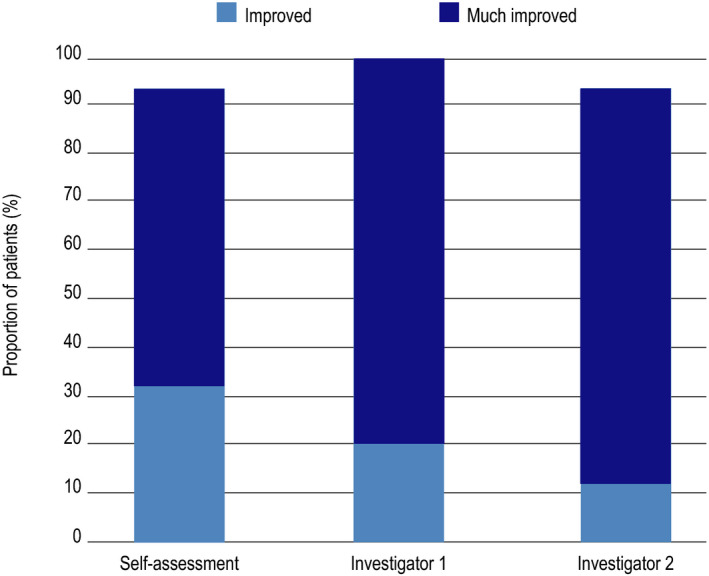
Improvement as assessed by the Global Aesthetic Improvement Scale at 6 months. Proportion of subjects grading themselves as improved or better (self‐assessment) and proportion of subjects graded by investigators as improved or better (investigator 1 and 2)
FIGURE 6.
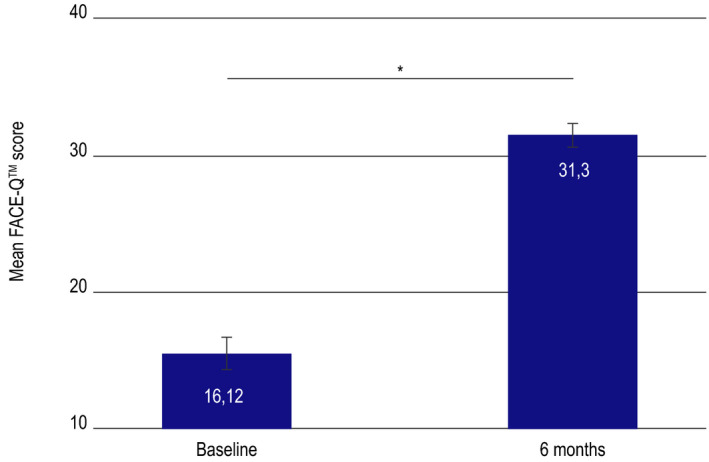
Subject reported self‐satisfaction using the FACE‐QTM scale before treatment (baseline) and at follow‐up (6 months). *p < 0.001
Minor and transient complications were seen in 16 out of 60 patients (26.6%, Table 2). No infection or complete thread extrusion occurred. No major complications were observed. Stable results were obtained in 58 patients. The procedure was redone within 12 months in two patients only, with additional four threads. These patients would have probably benefited from a surgical rhytidectomy since they showed high‐grade ptosis and severe skin laxity. In 4 cases, asymmetry occurred after the first procedure and was spontaneously corrected in 14 days. None of the patients requested the removal of the threads.
TABLE 2.
Complications during mid‐face lift with bidirectional barbs
| Complications | Patients, n (%) |
|---|---|
| No complications | 44 (73.3) |
| Minor and transient complications | 16 (26.6) |
| Dermal pinching a | 7 (11.7) |
| Minor extrusion | 4 (6.7) |
| Bruising | 3 (5.0) |
| Mild edema | 2 (3.3) |
Resolved in 7–10 days.
4. DISCUSSION
This retrospective study assessed treatment outcomes in patients who underwent a mid‐face reshaping procedure with DefinisseTM free floating threads. Our results show that this type of procedure offers high rates of esthetic improvement and patient satisfaction at 6 months and stable results after 6 months. Treatment was well tolerated since most procedures were performed smoothly and no major complications occurred.
Facial thread lifts using blue polypropylene threads with bidirectional barbs anchored in the dermis were popularized in the late 1990 s. Lee and Isse.
illustrated the use of barbed polypropylene threads for correction of the ptotic mid‐face, suturing the proximal end of the thread to the deep temporal fascia. Many variations of the original Aptos thread were utilized in the last decade for lifts of the brow, mid‐face, and the lower face and neck with the promise of excellent results with minimal recovery, less scarring, and low complication rates. 18 , 19
However, in contrast with the excellent results reported by these authors, many plastic surgeons raised numerous doubts about the low morbidity and the long‐term outcome of this type of procedure. 6 Rachel et al. conducted a retrospective review of 29 cosmetic patients who underwent thread lifting with barbed threads, demonstrating that adverse events occurred in 69% and early recurrence in 45% of the patients in the study group. 20 Walton et al. emphasized the need for a more objective measure of the outcome and long‐term follow‐up data. 20 Gampper et al observed that recovery time was similar between Threads lift and a traditional rhytidectomy; they reported postoperative Chevron‐shaped contour irregularities in patients undergoing suture lifts, many days after the intervention. 12 Vazquez described facial percutaneous suspension using 4/0 monofilament nylon in 20 patients with good long‐term results in a 2‐year follow‐up without complications. 19 It is worth stressing the importance of a careful selection of patients undergoing this procedure. Young patients with low‐grade flaccidity are ideal candidates; however, the same results cannot be achieved in patients with thin skin and many wrinkles. The procedure should not be offered to patients as an alternative to surgical rhytidectomy but as a temporary procedure with good esthetic results that can be maintained until more invasive approaches are required due to aging. DefinisseTM free floating threads are composed of a copolymer made from L‐lactide and ε‐caprolactone. 13 L‐lactide is present in a small percentage and provides elasticity to the thread; the ε‐caprolactone is used to ensure longer stability of the thread inside the tissue.
During the past years, research interest in random copolymers of L‐lactide and ε‐caprolactone has been increasingly growing due to a wide range of applications in the biomedical field. These copolymers are biocompatible and biodegradable and have been used to develop controlled‐release drug delivery systems, monofilament surgical threads, and absorbable nerve guides for axon regeneration. 21 In vivo studies have shown that monofilament threads made from poly(lactide‐ co‐caprolactone) cause a very mild tissue reaction. 22 In Japan, a complex of lactic acid‐caprolactone copolymer was used by a group at Kyoto University to develop an artificial dura mater, useful when endo‐cranial defects occur during craniotomy for the treatment of cranial nerves. 23
The thread, if immersed in a physiological solution at pH and temperature comparable to those of the dermis, is completely hydrolyzed in about 9–12 months. In vivo, however, it is supposed to last longer thanks to the fibrosis that protects the thread from degradation. For this reason, the thread is estimated to last up to 12–15 months. The lifting effect is estimated at around 30–36 months. 11
The DefinisseTM free floating threads have a central area, free of barbs, and two distal areas with barbs. The threads can be available with two lengths of barbed sections, 12 and 23.2 cm. In the present study, we used a 12‐cm thread which was inserted through a 20‐G cannula needle (9 cm). The barbs are convergent and bidirectional. 11
The DefinisseTM free floating threads were introduced in flabby tissues of the zygomatic and malar area with a cannula needle (Spinal Needle, 20‐G, 3,50 IN, 0.8 × 90 mm), and subsequently, the cannula was removed, leaving the thread in its place. The thread, with bidirectional and convergent barbs toward the center, was inserted inside the needle carefully so that the barbs that had to maintain their efficiency were not damaged. 7
Our study supports the use of DefinisseTM free floating threads in volume redistribution procedures for mid‐face reshaping. Treatment was successful in all patients who underwent thread lifting with DefinisseTM free floating threads, as seen by a reduction by one or more points in individual MFVDS scores and a significant reduction in overall mean MFVDS scores. Esthetic improvement was not only confirmed by evaluating investigators but also by patients themselves. On the GAIS scale, more than 90% of patients reported improvement after the procedure. Self‐assessment GAIS responder rates were similar to evaluating investigator's GAIS responder rates. A high mean FACE‐QTM score confirmed patient satisfaction with the outcome of the non‐invasive procedure performed in our study.
Older patients with high‐grade flaccidity of the skin and severe ptosis of the mid‐cheek are not good candidates for this procedure. Tissue repositioning with the thread lift technique should not be considered as an alternative to the much more invasive surgical face lift procedures. 13 This method should be considered for patients that refuse or want to delay more invasive procedures as well as an adjunct technique to other less invasive procedures such as endoscopic forehead lift and upper and lower blepharoplasty. 24 In the zygomatic‐malar region, optimal results may also be achieved by combining the thread lift technique with high G‐prime dermal fillers, which are able to fill facial tissue and reduce wrinkles and skin folds. Fillers are the best option in patients who need to restore facial volume, particularly in the malar region. However, in our opinion, filler injection should not be the first option when there is ptotic tissue involved. In such patients, the first step should always be the repositioning of ptotic tissue with threads. Only after this first procedure can high G‐prime hyaluronic acid fillers be used to give volume to the target (ptotic) area, if needed. An interval of at least 2 weeks should be given between procedures.
Limitations of this study include a short follow‐up and a relatively small number of patients. However, none of the patients was lost to follow‐up. Efficacy assessments were performed 6 months after the thread lift procedure in all patients, but the mean follow‐up of the study is 9.8 months. Patients seem satisfied with the outcomes of the procedure, as demonstrated by the lack of new interventions during follow‐up, even in patients with follow‐up periods longer than 6 months (range 6–14 months).
One advantage of the study here presented is the use of more than one scale to assess treatment efficacy and patient satisfaction. To our knowledge, no study has ever used the FACE‐QTM scale to evaluate outcomes in patients undergoing mid‐face reshaping with bidirectional threads.
5. CONCLUSION
Suspension thread technique using DefinisseTM free floating threads with bidirectional convergent barbs is a safe and reliable procedure for suspension of the ptotic mid‐face characterized by low complication rates, short recovery time, and good esthetic results. In our opinion, this approach should not be considered as an alternative to more aggressive procedures but, especially when combined with other less invasive procedures, can delay the need for traditional rhytidectomy.
ACKNOWLEDGEMENTS
Statistical analysis and editorial assistance were provided by ERA ms S.r.l. and funded by Relife S.r.l.
CONFLICT OF INTEREST
Nothing to declare.
AUTHOR CONTRIBUTION
AS, FC, and SA were involved in study design, patient enrollment, and data analysis. AS wrote the original draft of the manuscript. PC and MC provided medical and scientific input to the study. All authors reviewed and contributed to the final manuscript.
ETHICAL APPROVAL
The present study was designed in accordance with the ethical principles of the Declaration of Helsinki. Considering the retrospective design, according to the Italian Law, the study did not require approval by the local ethics committee. All patients who participated in this study signed an informed consent form.
Funding information
Nothing to declare.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Kahn DM, Shaw RB. Overview of current thoughts on facial volume and aging. Facial Plast Surg FPS. 2010;26(5):350‐355. [DOI] [PubMed] [Google Scholar]
- 2. Fitzgerald R, Graivier MH, Kane M, et al. Update on facial aging. Aesthet Surg J. 2010;30(Suppl):11S‐24S. [DOI] [PubMed] [Google Scholar]
- 3. Mendelson B, Wong C‐H. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2012;36(4):753‐760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Tonnard P, Verpaele A. The MACS‐lift short scar rhytidectomy. Aesthet Surg J. 2007;27(2):188‐198. [DOI] [PubMed] [Google Scholar]
- 5. Fedok FG. Advances in minimally invasive facial rejuvenation. Curr Opin Otolaryngol Head Neck Surg. 2008;16(4):359‐368. [DOI] [PubMed] [Google Scholar]
- 6. Atiyeh BS, Dibo SA, Costagliola M, Hayek SN. Barbed sutures “lunch time” lifting: evidence‐based efficacy. J Cosmet Dermatol. 2010;9(2):132‐141. [DOI] [PubMed] [Google Scholar]
- 7. Beer KR. Combined treatment for skin rejuvenation and soft‐tissue augmentation of the aging face. J Drugs Dermatol JDD. 2011;10(2):125‐132. [PubMed] [Google Scholar]
- 8. Sulamanidze MA, Paikidze TG, Sulamanidze GM, Neigel JM. Facial lifting with “APTOS” threads: featherlift. Otolaryngol Clin North Am. 2005;38(5):1109‐1117. [DOI] [PubMed] [Google Scholar]
- 9. Ruff G. Technique and uses for absorbable barbed sutures. Aesthet Surg J. 2006;26(5):620‐628. [DOI] [PubMed] [Google Scholar]
- 10. Isse N. Silhouette sutures for treatment of facial aging: facial rejuvenation, remodeling, and facial tissue support. Clin Plast Surg. 2008;35(4):481‐486. [DOI] [PubMed] [Google Scholar]
- 11. de Benito J, Pizzamiglio R, Theodorou D, Arvas L. Facial rejuvenation and improvement of malar projection using sutures with absorbable cones: surgical technique and case series. Aesthetic Plast Surg. 2011;35(2):248‐253. [DOI] [PubMed] [Google Scholar]
- 12. Garvey PB, Ricciardelli EJ, Gampper T. Outcomes in threadlift for facial rejuvenation. Ann Plast Surg. 2009;62(5):482‐485. [DOI] [PubMed] [Google Scholar]
- 13. Beer K. Delayed complications from thread‐lifting: report of a case, discussion of treatment options, and consideration of implications for future technology: DELAYED COMPLICATIONS FROM THREADLIFTING. Dermatol Surg. 2008;34(8):1120‐1123. [DOI] [PubMed] [Google Scholar]
- 14. Savoia A, Accardo C, Vannini F, Di Pasquale B, Baldi A. Outcomes in thread lift for facial rejuvenation: a study performed with happy LiftTM revitalizing. Dermatol Ther. 2014;4(1):103‐114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Jones D, Murphy DK. Volumizing hyaluronic acid filler for midface volume deficit: 2‐year results from a pivotal single‐blind randomized controlled study. Dermatol Surg. 2013;39(11):1602‐1612. [DOI] [PubMed] [Google Scholar]
- 16. Narins RS, Brandt F, Leyden J, Lorenc ZP, Rubin M, Smith S. A randomized, double‐blind, multicenter comparison of the efficacy and tolerability of restylane versus Zyplast for the correction of nasolabial folds. Dermatol Surg. 2003;29(6):588‐595. [DOI] [PubMed] [Google Scholar]
- 17. Lee S, Isse N. Barbed Polypropylene Sutures for Midface Elevation. Archives of Facial Plastic Surgery. 2005;7(1):55–61. 10.1001/archfaci.7.1.55 [DOI] [PubMed] [Google Scholar]
- 18. Isse NG, Fodor PB. Elevating the midface with barbed polypropylene sutures. Aesthet Surg J. 2005;25(3):301‐303. [DOI] [PubMed] [Google Scholar]
- 19. Vázquez GD. Facial percutaneous suspension. Plast Reconstr Surg. 2005;116(2):656‐660. [DOI] [PubMed] [Google Scholar]
- 20. Rachel JD, Lack EB, Larson B. Incidence of complications and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2010;36(3):348‐354. [DOI] [PubMed] [Google Scholar]
- 21. Baimark Y, Molloy R. Synthesis and characterization of Poly(L‐lactide‐co‐ε‐caprolactone) copolymers: effects of stannous octoate initiator and diethylene glycol coinitiator concentrations. ScienceAsia. 2004;30:327‐334. [Google Scholar]
- 22. Tomihata K, Suzuki M, Oka T, Ikada Y. A new resorbable monofilament suture. Polym Degrad Stab. 1998;59(1–3):13‐18. [Google Scholar]
- 23. Yamada K, Miyamoto S, Takayama M, et al. Clinical application of a new bioabsorbable artificial dura mater. J Neurosurg. 2002;96(4):731‐735. [DOI] [PubMed] [Google Scholar]
- 24. Hochman M. Midface barbed suture lift. Facial Plast Surg Clin N Am. 2007;15(2):201‐207. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.