

Abstract
Background
Prenatal alcohol exposure (PAE) is associated with growth deficits and neurodevelopmental impairment including foetal alcohol spectrum disorder (FASD). Difficulties with oral and written communication skills are common among children with PAE; however, less is known about how communication skills of adolescents who have PAE compare with those who do not. Adolescence is a critical time for development, supporting the transition into adulthood, but it is considered a high‐risk period for those with FASD.
Aims
We conducted a systematic review to synthesize evidence regarding oral and written communication skills of adolescents with PAE or FASD and how they compare with those with no PAE.
Methods & Procedures
A comprehensive search strategy used seven databases: Cochrane Library, Cinahl, Embase, Medline, PsycInfo, Eric and Web of Science. Included studies reported on at least one outcome related to oral and written communication for a PAE (or FASD) group as well as a no/low PAE group, both with age ranges of 10–24 years. Quality assessment was undertaken.
Main Contribution
Communication skills most often assessed in the seven studies included in this review were semantic knowledge, semantic processing, and verbal learning and memory. These communication skills, in addition to reading and spelling, were commonly weaker among adolescents with PAE compared with those with no/low PAE. However, the findings were inconsistent across studies, and studies differed in their methodologies.
Conclusions & Implications
Our results emphasize that for adolescents with PAE, communication skills in both oral and written modalities should be comprehensively understood in assessment and when planning interventions. A key limitation of the existing literature is that comparison groups often include some participants with a low level of PAE, and that PAE definitions used to allocate participants to groups differ across studies.
What this paper adds
What is already known on the subject
PAE and FASD are associated with deficits in oral and written communication skills. Studies to date have mostly focused on children with a FASD diagnosis as well as combined groups of children and adolescents with FASD or PAE. There is a gap in what is known about oral and written communication skills of adolescents, specifically, who have PAE or FASD. This has implications for the provision of assessment and supports during a period of increased social and academic demands.
What this study adds to existing knowledge
This review provides systematic identification, assessment and synthesis of the current literature related to oral and written communication skills of adolescents with PAE compared with those with no/low PAE. The review revealed a small knowledge base with inconsistent methodologies and findings across studies. However, the findings overall highlight that adolescents with PAE have weaker skills in oral and written language than those with no/low PAE. Results are discussed in relation to education, social and emotional well‐being, and forensic contexts.
What are the potential or actual clinical implications of this work?
Findings emphasize that for adolescents with PAE, comprehensive assessment of both oral and written communication skills, through both standardized and functional tasks, should be undertaken. Speech–language pathologists have a key role in assessment with individuals who have PAE.
Keywords: language, literacy, communication, prenatal alcohol exposure, foetal alcohol spectrum disorder, adolescence
INTRODUCTION
Prenatal alcohol exposure (PAE) and foetal alcohol spectrum disorder (FASD)
PAE is a global public health concern. Alcohol can affect foetal development, potentially resulting in a range of neurodevelopmental impairments, including FASD (McCormack et al. 2017). Globally, the prevalence of alcohol use in pregnancy is 10%, however variation is considerable within and across countries (Popova et al. 2017). In Australia, for example, one study in which children were randomly selected from a government database and their parents were interviewed face to face reported that 30% of pregnancies involved PAE (Hutchinson et al. 2013). In another Australian study, in which women were from a prospective pregnancy cohort study and interviewed via telephone, PAE was identified in 61% of pregnancies (McCormack et al. 2017). Following pregnancy recognition, just over one in four pregnancies in Australia continue to involve PAE (Muggli et al. 2016). Globally, approximately 8% of children with PAE receive a diagnosis of FASD (Lange et al. 2017). Pooled prevalence estimates of FASD among children and youth in the general community range from < 1% to 2% (Lange et al. 2017). However, the prevalence is much higher among specific sub‐populations, such as in special education (3–8%) and child welfare populations (5–31%) (Popova et al. 2019).
Duration and dose of PAE are associated with risk of psychosocial and behaviour problems which extend into early adulthood (Day et al. 2013), and PAE of ≥ 1 ounce (oz) of absolute alcohol (AA) per week 1 is associated with structural changes and reduced volume of the brain (Chen et al. 2012). Individuals with a FASD diagnosis demonstrate severe impairments across a wide range of neurocognitive domains, including attention, memory, language, executive function, cognition, motor skills and affect regulation (Mattson et al. 2019). These impairments confer additional vulnerability for the acquisition and use of adaptive functioning and academic skills (Lynch et al. 2017, McLachlan et al. 2020). Neurodevelopmental impairment associated with PAE can also be compounded by exposure to childhood trauma and other adversities (Hyter 2007, Kambeitz et al. 2019). While neurodevelopmental impairment can occur among children with trauma alone, it is more common among those with both trauma and FASD (Henry et al. 2007).
PAE and skills related to oral and written communication
Communication skills are a key consideration in FASD diagnostic assessments and in the provision of services to support functioning (Bower and Elliott 2016, Scottish Intercollegiate Guidelines Network 2019). Speech‐sound, word‐ and sentence‐level language difficulties were first observed among children and adolescents of parents with alcohol use problems in France in the late 1960s (Lemoine et al. 2003). In the 1970s, standardized assessment of the communication skills of 45 young children with a diagnosis of foetal alcohol syndrome (FAS: a diagnosis subsumed under the diagnosis of FASD) in the United States revealed that 80% demonstrated speech, language or voice deficits (Iosub et al. 1981). In Australia, parent‐reported language delay at 2 years of age was not associated with PAE at low levels (≤ 20 g of AA per occasion, less than weekly 2 ); however, language delay was more common among those with higher levels of PAE in trimesters two and three of pregnancy (O'Leary et al. 2009). More recently, in Canada, among children of high‐risk drinkers, a 50% increased risk of parent‐reported communication delay in early childhood was identified (Netelenbos et al. 2020).
Several studies show that individuals with FASD or PAE (without a diagnosis of FASD) demonstrate impairments across multiple verbal skills. In general, the research focuses on children with a FASD diagnosis, combined groups of children and adolescents with FASD or PAE, and adolescents with PAE that was assessed for part of the pregnancy, rather than for all three trimesters in pregnancy. Weak verbal memory skills are seen in children with FASD and adolescents with PAE (Becker et al. 1990, Olson et al. 1998, Willford et al. 2004). Hearing loss is also common among children with FASD (McLaughlin et al. 2019). Such deficits affect the encoding and consolidation of speech and language, and in turn, compromise learning within oral language domains of phonology, semantics and syntax (grammar). Individuals with FASD have been found to lack adequate semantic knowledge, including receptive and expressive vocabulary (Wyper and Rasmussen 2011), and those with PAE are slower to access and retrieve vocabulary items based on semantic and phonemic constraints (Mattson and Riley 1999). Using semantic knowledge for language‐related problem‐solving tasks is also difficult for individuals with FASD (Rasmussen and Bisanz 2009, Wyper and Rasmussen 2011). Grammatical skills can also be compromised, impeding both comprehension and formulation of language at sentence and text levels (Kodituwakku et al. 2006, Wyper and Rasmussen 2011).
Oral language skills are foundational to learning how to read, spell and write (Nation 2019, Wagner and Torgesen 1987). Both oral and written language skills are critical for academic and occupational success, therefore it is important to consider both these modalities. Studies with children who have FASD, either separate to or in a combined group with adolescents, have found compromised reading and spelling abilities (Adnams et al. 2007, Glass et al. 2015). These studies have also shown that underlying these difficulties are weaknesses in phonological awareness, phoneme manipulation, decoding (mapping graphemes to phonemes) and encoding (mapping phonemes to graphemes) (Adnams et al. 2007, Glass et al. 2015). According to the Simple View of Reading, skills in both decoding and semantic knowledge are required for reading comprehension (Nation 2019), and weak reading comprehension skills have also been found among individuals with PAE, with and without FASD (Mattson et al. 1998, Vaurio et al. 2011). Further, rapid naming skills, which are strongly associated with reading fluency (Norton and Wolf 2012), were also found to be weak (Glass et al. 2015).
PAE, communication skills and adolescence
Some studies have reported that deficits with communication skills among individuals with FASD or PAE become more severe with increasing age. Increasing deficits in overall receptive and expressive language ability have been identified (de Beer et al. 2010, Proven et al. 2014) as well as in specific skills, such as grammar (Wyper and Rasmussen 2011) and verbal fluency (Rasmussen and Bisanz 2009). It is not surprising that deficits in communication skills become more severe with age given the increasing social and academic demands as well as fewer parent and teacher supports. Individuals with FASD struggle with the complex language and cognitive skills required to navigate learning and social situations (Duquette et al. 2006, Skorka et al. 2020). Consequently, the transition from primary to high school as well as from adolescence into young adulthood is particularly problematic (Lynch et al. 2017, Skorka et al. 2020).
Adolescence begins at the commencement of puberty (a biological event); however, the end of adolescence differs according to country and community, and can align with social and cultural achievements, such as educational attainment, social competence and financial independence (Blakemore 2018). Adolescence is a critical time for the development of neurocognitive skills which support the establishment of greater independence as well as influence social, educational, health and economic trajectories (Dahl et al. 2018). Thus, adolescent health has emerged as an internationally recognized priority area concerned with health and well‐being, encompassing both the adolescent (10–19 years) and youth (15–24 years) age ranges (Patton et al. 2016, Viner et al. 2012).
The development of communication skills is particularly important during adolescence, with growth in skills related to semantic knowledge, morphology and syntax as well as metacognitive verbs, figurative and pragmatic language (Nippold 2016, Spencer 2018). Adolescents become increasingly capable of producing and comprehending more complex oral and written language. This in turn contributes to successful participation in social, academic and occupational contexts. However, during adolescence, the development of communication skills can be often overlooked, and communicative competence assumed, given that development of communication skills is less visible compared with early childhood years (Spencer 2018). Given the significance of oral and written communication skill development within adolescence and beyond, specific attention to the communication skills of adolescents with PAE is warranted.
Previous systematic reviews
Four systematic reviews report communication outcomes as part of their investigation of individuals with FASD or PAE. A systematic review and meta‐analysis, by Popova et al. (2016), of the comorbid conditions among children, adolescents and adults with a diagnosis of FAS established receptive (82%) and expressive language disorder (76%) as two of the most common comorbid conditions. Articulation, motor‐speech and voice problems were also commonly noted; however, detailed communication profiles were not reported given that the focus of the review related to a wide range of comorbidities (Popova et al. 2016). Price et al. (2017) systematically reviewed research related to the impact of both PAE and trauma on development; they identified that for 0–16‐year‐olds, exposure to both trauma and PAE can have a compounding effect, resulting in a higher risk of communication problems, including with phonological awareness, speech, vocabulary, grammar as well as verbal memory, compared with exposure to one of these factors alone. Flak et al. (2014) systematically reviewed and meta‐analysed research related to the association between PAE and child neurodevelopment; they failed to find an association between mild, moderate and binge levels of PAE and expressive vocabulary, verbal intelligence, semantic verbal fluency and reading for 0–14‐year‐olds. Due to the complex and dynamic nature of neurodevelopment, Flak et al. (2014) raised a concern about analysing results from studies with a wide age range of participants. Irner (2012) undertook a systematic review on the association between PAE and other substance exposures in‐utero and developmental outcomes in adolescence. They included studies with and without comparisons between PAE and no/low PAE groups, as well as studies with participant groups with children, adolescents and adults. They concluded that PAE, especially at high levels (more than or equal to five alcohol drinks per occasion), is associated with developmental deficits, including in verbal skills and academic achievement, and highlighted the impact on development that social adversity and other drug exposures may also have.
A further two systematic reviews specifically focused on PAE and communication skills among infants and young children, but are equivocal in their findings as to whether PAE, at varying levels, is associated with weaker communication outcomes (Hendricks et al. 2019, O'Keeffe et al. 2014). The current review aimed to address a gap in previous reviews, namely the need to synthesize nuanced data on communication profiles of adolescents to provide a comprehensive understanding of how both PAE and FASD affect oral and written communication outcomes during this developmental period.
Current study
Our objective was to systematically review and synthesize literature to identify the communication profiles of adolescents (10–24 years) with PAE, and to examine how they compare with those with no/low PAE. Detailed insights into the specific communication profiles of adolescents with PAE can help to drive assessment, support and therapeutic approaches that are developmentally and neurocognitively appropriate for this age group.
Materials and methods
We conducted and report this systematic review following the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) statement (Moher et al. 2009). Our protocol was registered with PROSPERO (ID: CRD42019077187).
Eligibility criteria
This review included only English‐language, peer‐reviewed and published studies that had both a PAE (or FASD) group and a no/low PAE group. For inclusion in this review, PAE needed to have been assessed for each group. In this review, we used the age range consistent with that used in adolescent health (Patton et al. 2016, Viner et al. 2012); all participants in both the PAE and no/low PAE groups needed to be aged 10–24 years. Studies in which the age range of participants fell outside of this age criterion were excluded, unless data were provided specifically for those in the required age range. We contacted the authors if a study did not specify the age range of the participants. Studies were eligible if they included data (mean/SD) from standardized or non‐standardized assessments for at least one outcome related to oral or written communication skills.
Search strategy and information sources
Our search strategy included terms for (1) adolescents, (2) PAE and FASD, (3) control groups and (4) outcomes related to oral and written communication skills examined when a diagnosis of FASD is being considered, for example, speech, language, verbal memory, verbal fluency and literacy (Bower and Elliott 2016, Scottish Intercollegiate Guidelines Network 2019). An example of our search strategy is provided (see table S1 in the additional supporting information). We did not include individual subtest outcomes related to mathematics, social communication or social problem solving. While composite verbal IQ and verbal comprehension scores include data related to these skills, they also include data related to vocabulary, similarities and general knowledge, and are considered to reflect overall verbal ability (Wechsler 1991). Therefore, we have included the verbal IQ and verbal comprehension composite scores. Further, we did not include verbal tasks which require switching and are considered measures of inhibition, for example, the switching subtest scores for verbal fluency and rapid naming.
The databases searched were the Cochrane Library, Cinahl, Embase, Medline, PsycInfo, Eric and Web of Science. We used MeSH headings as well as title and abstract truncation relevant to each electronic database, and our search strategy was reviewed by an experienced university librarian. The search included studies published from 1967 onwards and was conducted in March 2019. Before our final reporting, we conducted the search again for studies published during 2019 and up to 6 July 2020.
Study selection
The search results were exported to Endnote (X8.2) and uploaded to Covidence, a web‐based software program for systematic reviews (Veritas Health, Innovation). Following the removal of duplicates, the first author and a second (SL/RW/AFJ) independently screened 100% of titles and abstracts. The same method was carried out for full‐text screening of 100% of the remaining results. We resolved disagreements by team discussion.
Quality assessment
The first author and a second (RW/AFJ) independently assessed the methodological quality of the included studies using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields (Kmet et al. 2004). Studies were assessed for their design, participant recruitment, assessment and outcomes as well as reporting of results and confounders. Items can be scored 0 = no, 1 = partial, 2 = yes, or N/A if not applicable. Items 5–7 can be excluded for observational studies; however, we included item 6 as it relates to blinding of investigators which is an important item to consider in quality assessment (National Health and Medical Research Council 1999). Raw scores were converted to percentages and used to categorize study quality as strong (> 80%), good (70–80%), adequate (50–69%) or limited (< 50%) (Lee et al. 2008) (table 1). Disagreements were resolved by team discussion.
TABLE 1.
Included study and participant characteristics of five of the eight included studies
| Age (years) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Reference, country | Design | Groups | n | Range | Mean | Male (%) | Ethnicity/Race (%) | Social strata | QA (%) |
| Furtado and de Sa Roriz (2016), Brazil | Cohort | PAE | 28 | 11–13 | 11.9 (0.4) | 43 | – | Low d |
71 Good |
| No/low PAE | 28 | 12.0 (0.3) | 50 | – | Low | ||||
| Lewis et al. (2015), USA a | Cohort | PAE + heavy | 19 | 13–16 | 14.4 (0.6) | 43 | African American: 100 | Medium e |
83 Strong |
| PAE + moderate | 21 | African American: 100 | |||||||
| No/low PAE | 251 | African American: 100 | |||||||
| McLachlan et al. (2014), Canada | Case control | PAE (FASD) | 50 | 12–23 | 17.6 (1.8) | 80 | – | – |
79 Good |
| No/low PAE | 50 | 12–23 | 17.5 (1.3) | 82 | – | – | |||
| Howell et al. (2006), USA b | Cohort | PAE + dysmorphic | 46 | 13–17 | 15.1 (1.1) | 48 | African American: 98 | Low f |
75 Good |
| PAE – dysmorphic | 82 | 14.9 (0.8) | 39 | African American: 96 | Low | ||||
| No/low PAE | 53 | 14.9 (0.8) | 44 | African American: 96 | Low | ||||
| Doyle et al. (2018), USA c | Cohort | PAE | 142 | 10–16 | 12.9 (2.1) | 52 | White: 59; Hispanic: 20 | Medium g |
71 Good |
| No/low PAE | 160 | 13.5 (2.1) | 51 | White: 61; Hispanic: 24 | Medium | ||||
Notes: aDetroit participants only.
The same participants, but different outcomes and ages, are reported by Coles et al. (2010) (see table S2 in the additional supporting information).
The same participants, but different outcomes, are reported by Panczakiewicz et al. (2016) (see table S2 in the additional supporting information).
Based on parent education.
Based on the Hollingshead Four Factor Index of Socioeconomic Status (individual group data not provided).
Based on geographical location.
Based on parent education and SES data provided by Panczakiewicz et al. (2016); QA = quality assessment score.
Data extraction
The first author extracted data related to study characteristics from the included studies, using a template that we developed based on guidelines from the National Health and Medical Research Council (1999). The extracted data were related to study design and participant characteristics (table 1), as well as the definitions used for PAE and the methods used to guide FASD diagnostic decisions (table 2). We extracted outcomes of interest (i.e., mean/SD) and the respective assessments administered (table 3). All extracted data were cross‐checked by a second author (SL/AFJ/RW). We classified outcomes according to oral language domains, verbal processing skills that underlie communication skills, and written language skills. Two speech–language pathologists (NK and SL) reviewed each administered assessment task and classified outcomes accordingly. Discrepancies were resolved through team discussion.
TABLE 2.
Definitions of PAE by group for the included studies
| Group definitions of PAE | ||
|---|---|---|
| Reference | PAE | No/low PAE |
| Furtado and de Sa Roriz (2016) | Any positive answer to alcohol consumption questions; score ≥ 1 on an assessment of high‐risk drinking (T‐ACE); alcohol abuse/dependence | Alcohol abstinence in pregnancy; score of 0 on T‐ACE assessment; no alcohol diagnosis |
| Lewis et al. | Heavy: ≥ 1.0 oz AA per day during pregnancy | < 0.5 oz AA per day during pregnancy |
| Moderate: 0.5–0.99 oz AA per day during pregnancy | ||
| McLachlan et al. (2014) | Participant has a FASD diagnosis | No known, documented, or suspected PAE |
| Howell et al. | ≥ 2 drinks per week during pregnancy | No PAE |
| Doyle et al. | > 4 drinks per occasion or > 13 drinks per week on average during pregnancy; Alcohol abuse/dependence; PAE suspected AND criteria met for FAS | ≤ 1 drink per week on average and never > 2 drinks per occasion during pregnancy d |
Notes: AA, absolute alcohol. A total of 0.6 fluid ounces (fl oz) of AA = one standard drink in the United States (National Institute on Alcohol Abuse and Alcoholism, 2020); FAS, foetal alcohol syndrome (diagnosis subsumed under FASD).
Detroit sample only.
The same participants, but different outcomes and age, are reported by Coles et al. (2010).
The same participants, but different outcomes, are reported by Panczakiewicz et al. (2016).
Definition used by Panczakiewicz et al. (2016): less than one drink per week on average and never more than two drinks per occasion during pregnancy.
TABLE 3.
Assessments and outcomes reported in the included studies
| Reference | Assessment and Subtest | Outcomes |
|---|---|---|
| Oral language | ||
| Semantic knowledge and organization | ||
| Word definitions: Spoken definitions of vocabulary items | ||
| Furtado et al. (2016) | WISC‐III: Language a | PAE (mean = 10.8, SD = 3.3), no/low PAE (mean = 10.3, SD = 2.1), p = 0.48, d = 0.2 |
| McLachlan et al. (2014) | CMR: Vocabulary | FASD (mean = 5.7, SD = 3.2) < no/low PAE (mean = 8.2, SD = 2.4), p < 0.01, d = 0.9 |
| CMR: Vocabulary b | FASD (mean = 11.3, SD = 4.4) < no/low PAE (mean = 14.8, SD = 4.0), p < 0.01, d = 0.9 | |
| Howell et al. (2006) | WISC‐III: Vocabulary |
PAE + dysmorphic (mean = 4.1, SD = 2.4) < no/low PAE (mean = 5.8, SD = 2.4), p < 0.01, d = 0.7 PAE–dysmorphic (mean = 5.4, SD = 3.3), no/low PAE, p = 0.34, d = 0.2 |
| Panczakiewicz et al. (2016) | DAS‐II: Word definitions |
Female: PAE (mean = 44.2, SD = 11.2) < no/low PAE (mean = 51.9, SD = 9.2), p < 0.01, d = 0.8 Male: PAE (mean = 48.3, SD = 8.0) < no/low PAE (mean = 56.1, SD = 9.8), p < 0.01, d = 0.9 |
| General knowledge: Spoken responses to general knowledge questions, such as ‘how many days are there in a week?’ | ||
| Furtado et al. (2016) | WISC‐III: Knowledge a | PAE (mean = 8.1, SD = 3.0), no/low PAE (mean = 8.1, SD = 3.3), p = 0.97, d < 0.1 |
| Similarities: Spoken explanations supported by reasoning, e.g., ‘In what way are milk and water alike?’ | ||
| Furtado et al. (2016) | WISC‐III: Similarities | PAE (mean = 10.8, SD = 3.9), no/low PAE (mean = 10.4, SD = 3.4), p = 0.68, d = 0.1 |
| Howell et al. (2006) | WISC‐III: Similarities |
PAE + dysmorphic (mean = 6.0, SD = 3.3) < no/low PAE (mean = 7.3, SD = 2.6), p = 0.03, d = 0.4 PAE – dysmorphic (mean = 7.4, SD = 3.4), no/low PAE, p = 0.86, d < 0.1 |
| Panczakiewicz et al. (2016) | DAS‐II: Verbal Similarities |
Female: PAE (mean = 41.1, SD = 10.0) < no/low PAE (mean = 49.0, SD = 8.3), p < 0.01, d = 0.9 Male: PAE (mean = 46.2, SD = 8.1) < no/low PAE (mean = 51.1, SD = 9.8), p < 0.01, d = 0.5 |
| Sentence recognition: Recognition of semantically identical sentences related to interrogation warnings | ||
| McLachlan et al. (2014) | CMR: Sentence recognition | FASD (mean = 9.3, SD = 3.2) < no/low PAE (mean = 10.6, SD = 1.2), p < 0.01, d = 0.9 |
| CMR: Sentence recognition b | FASD (mean = 14.3, SD = 2.3) < no/low PAE (mean = 15.7, SD = 1.7), p < 0.01, d = 0.9 | |
| Paraphrasing: Spoken paraphrasing of sentences related to interrogation warnings | ||
| McLachlan et al. (2014) | CMR: Paraphrasing | FASD (mean = 4.9, SD = 2.0) < no/low PAE (mean = 6.3, SD = 1.9), p < 0.01, d = 0.7 |
| CMR: Paraphrasing b | FASD (mean = 7.0, SD = 2.7) < no/low PAE (mean = 9.2, SD = 2.4), p < 0.01, d = 0.9 | |
| Verbal processing skills | ||
| Verbal intelligence | ||
| Verbal IQ and VCI. The combined scores of verbal subtests | ||
| Furtado et al. (2016) | WISC‐III: Verbal IQ | PAE (mean = 95.8, SD = 15.6), no/low PAE (mean = 98.2, SD = 16.6), p = 0.59, d = 0.2 |
| Howell et al. (2006) | WISC‐III: Verbal IQ |
PAE + dysmorphic (mean = 72.4, SD = 14.2) < no/low PAE (mean = 80.3, SD = 10.9), p < 0.01, d = 0.6 PAE – dysmorphic (mean = 80.5, SD = 15.9), no/low PAE, p = 0.93, d < 0.1 |
| WISC‐III: VCI |
PAE + dysmorphic (mean = 73.4, SD = 14.5) < no/low PAE (mean = 81.1, SD = 10.8), p < 0.01, d = 0.6 PAE – dysmorphic (mean = 81.0, SD = 16.1), no/low PAE, p = 0.99, d < 0.1 |
|
| Phonological and semantic processing: Access to and retrieval of lexical items | ||
| Verbal fluency: Spoken production of vocabulary items that meet semantic/phonemic as well as time constraints | ||
| Furtado et al. (2016) | Verbal fluency: F‐A‐S d | PAE (mean = 17.5, SD = 6.0), no/low PAE (mean = 18.0, SD = 7.2), p = 0.79, d < 0.1 |
| Verbal fluency: animals d | PAE (mean = 13.6, SD = 3.6) < no/low PAE (mean = 15.8, SD = 4.4), p = 0.05, d = 0.5 | |
| Doyle et al. (2018) | NEPSY‐II: Word generation (semantic and initial) | PAE (mean = 7.3, SD = 3.0) < no/low PAE (8.3, SD = 3.0), p < 0.01, d = 0.3 |
| Panczakiewicz et al. (2016) | NEPSY‐II: Word generation (semantic) |
Female: PAE (mean = 10.5, SD = 4.1) < no/low PAE (mean = 12.4, SD = 3.2), p < 0.01, d = 0.5 Male: PAE (mean = 9.9, SD = 3.6) < no/low PAE (mean = 11.9, SD = 3.5), p < 0.01, d = 0.7 |
| Rapid naming: Rapid spoken naming of printed letters and numbers | ||
| Doyle et al. (2018) | NEPSY‐II: Speeded naming (letters and numbers) | PAE (mean = 8.2, SD = 2.8) < no/low PAE (mean = 9.0, SD = 2.4), p < 0.01, d = 0.3 |
| Verbal working memory | ||
| Digit span (total): Spoken recall of a sequence of orally presented digits, forwards and backwards | ||
| Furtado et al. (2016) | WISC‐III: Digit span (total) | PAE (mean = 9.3, SD = 3.2), no/low PAE (mean = 8.7, SD = 2.3), p = 0.41, d = 0.2 |
| Howell et al. (2006) | WISC‐III: Digit span (total) |
PAE + dysmorphic (mean = 7.8, SD = 3.2), no/low PAE (mean = 8.0, SD = 3.1), p = 0.85, d < 0.1 PAE – dysmorphic (mean = 8.0, SD = 2.8), no/low PAE, p = 0.91, d < 0.1 |
| Verbal learning and memory | ||
| Memory for names: Listening to and spoken recall of names associated with pictures of faces | ||
| Panczakiewicz et al. (2016) | NEPSY‐II: Memory for names delayed |
Female: PAE (mean = 7.6, SD = 3.8) < no/low PAE (mean = 9.8, SD = 3.1), p < 0.01, d = 0.6 Male: PAE (mean = 7.3, SD = 3.8) < no/low PAE (mean = 10.0, SD = 2.7), p < 0.01, d = 0.8 |
| Narrative memory: Listening to and immediate recall of a verbally provided story (text‐level of language) | ||
| Panczakiewicz et al. (2016) | NEPSY‐II: Narrative memory immediate recall |
Female: PAE (mean = 8.1, SD = 3.2) < no/low PAE (mean = 10.3, SD = 3.2), p < 0.01, d = 0.7 Male: PAE (mean = 8.7, SD = 3.2) < no/low PAE (mean = 10.9, SD = 3.4), p < 0.01, d = 0.7 |
| Word list learning and recall: Listening to and spoken recall of a series of words within different time intervals | ||
| Furtado et al. (2016) | RAVLT: Immediate recall | PAE (mean = 7.1, SD = 1.5), no/low PAE (mean = 6.7, SD = 1.9), p = 0.39, d = 0.2 |
| RAVLT: Total recall | PAE (mean = 57.8, SD = 4.7), no/low PAE (mean = 55.9, SD = 6.7), p = 0.21, d = 0.3 | |
| RAVLT: Recall 30 minute | PAE (mean = 13.5, SD = 1.6), no/low PAE (mean = 13.1, SD = 1.8), p = 0.38, d = 0.2 | |
| RAVLT: Recognition | PAE (mean = 14.9, SD = 0.4), no/low PAE (mean = 14.5, SD = 1.0), p = 0.09, d = 0.5 | |
| RAVLT: Proactive interference | PAE (mean = 1.1, SD = 0.4), no/low PAE (mean = 1.2, SD = 1.0), p = 0.46, d = 0.2 | |
| RAVLT: Retroactive interference | PAE (mean = 0.69, SD = 0.49), no/low PAE (mean = 0.72, SD = 0.06), p = 0.75, d < 0.1 | |
| Coles et al. | VSRT: Learning slope |
PAE + dysmorphic (mean = 0.27, SD = 0.14) < no/low PAE (mean = 0.36, SD = 0.13), p < 0.01, d = 0.7 PAE – dysmorphic (mean = 0.32, SD = 0.14), no/low PAE, p = 0.13, d = 0.3 |
| VSRT: Total recall |
PAE + dysmorphic (mean = 7.1, SD = 2.1) < no/low PAE (mean = 8.5, SD = 1.4), p < 0.01, d = 0.8 PAE – dysmorphic (mean = 7.8, SD = 1.7) < no/low PAE, p < 0.01, d = 0.5 |
|
| VSRT: 8th trial |
PAE + dysmorphic (mean = 8.4, SD = 2.5) < no/low PAE (mean = 10.3, SD = 1.8), p < 0.01, d = 0.9 PAE – dysmorphic (mean = 9.3, SD = 2.1) < no/low PAE, p < 0.01, d = 0.5 |
|
| VSRT: Long‐term storage |
PAE + dysmorphic (mean = 8.3, SD = 3.3) < no/low PAE (mean = 10.5, SD = 2.0), p < 0.01, d = 0.8 PAE – dysmorphic (mean = 9.6, SD = 2.7) < no/low PAE, p = 0.04, d = 0.4 |
|
| VSRT: Consistent long‐term retrieval |
PAE + dysmorphic (mean = 5.8, SD = 3.4) < no/low PAE (mean = 8.6, SD = 2.9), p < 0.01, d = 0.9 PAE – dysmorphic (mean = 7.1, SD = 3.0) < no/low PAE, p < 0.01, d = 0.5 |
|
| VSRT: Delayed recall 30 min |
PAE + dysmorphic (mean = 6.3, SD = 3.0) < no/low PAE (mean = 8.5, SD = 2.6), p < 0.01, d = 0.8 PAE – dysmorphic (mean = 7.6, SD = 2.8), no/low PAE, p = 0.08, d = 0.3 |
|
| Lewis et al. (2015) | CVLT‐C: Immediate |
PAE + heavy (mean = 6.8, SD = 1.8), no/low PAE (mean = 7.1, SD = 1.7), p = 0.46, g = 0.2 PAE + moderate (mean = 6.6, SD = 1.9), no/low PAE, p = 0.20, g = 0.3 |
| CVLT‐C: Total learning |
PAE + heavy (mean = 46.8, SD = 7.3), no/low PAE (mean = 50.4, SD = 8.1), p = 0.06, g = 0.4 PAE + moderate (mean = 49.4, SD = 8.9), no/low PAE p = 0.59, g = 0.1 |
|
| CVLT‐C: Short delay recall |
PAE + heavy (mean = 9.0, SD = 1.9) < no/low PAE (mean = 10.5, SD = 2.3), p < 0.01, g = 0.7 PAE + moderate (mean = 10.3, SD = 2.3), no/low PAE, p = 0.70, g = 0.1 |
|
| CVLT‐C: Long delay recall |
PAE + heavy (mean = 9.4, SD = 1.8) < no/low PAE (mean = 10.9, SD = 2.1), p < 0.01, g = 0.7 PAE + moderate (mean = 10.7, SD = 2.1), no/low PAE, p = 0.68, g = 0.1 |
|
| CVLT‐C: Recognition discrimination |
PAE + heavy (mean = 93.4, SD = 5.7) < no/low PAE (mean = 96.4, SD = 4.1), p = 0.04 e , g = 0.7 PAE + moderate (mean = 94.6, SD = 6.0), no/low PAE, p = 0.18 f , g = 0.4 |
|
| Written language | ||
| Reading | ||
| Letter identification, word reading, and sentence‐level reading comprehension (WRAT‐4); non‐word and word reading (WIAT‐I); receptive vocabulary and text‐level reading (ITBS) | ||
| McLachlan et al. (2014) | WRAT‐4: Reading | FASD (mean = 5.2, SD = 2.2) < no/low PAE (mean = 7.8, SD = 3.0), p < 0.01, d = 1.0 |
| Howell et al. (2006) | WIAT‐I: Basic reading |
PAE + dysmorphic (mean = 78.2, SD = 14.5), no/low PAE (mean = 82.9, SD = 13.7), p = 0.10, d = 0.3 PAE – dysmorphic (mean = 82.5, SD = 15.8), no/low PAE, p = 0.90, d < 0.1 |
| ITBS: Reading |
PAE + dysmorphic (mean = 18.2, SD = 17.1) < no/low PAE (mean = 30.5, SD = 24.0), p < 0.01, d = 0.6 PAE – dysmorphic (mean = 32.8, SD = 25.2), no/low PAE, p = 0.59, d = 0.1 |
|
| Spelling | ||
| Spelling of single words | ||
| Howell et al. (2006) | WIAT‐I: Spelling |
PAE + dysmorphic (mean = 78.5, SD = 15.6) < no/low PAE (mean = 85.0, SD = 15.3), p = 0.04, d = 0.4 PAE – dysmorphic (mean = 83.4, SD = 16.3), no/low PAE, p = 0.55, d = 0.1 |
Notes: WISC‐III, Wechsler Intelligence Scale for Children—Third Edition (scaled/standard scores) (Wechsler 1991); CMR, Grisso's Comprehension of Miranda Rights (score range: 0–12 (vocabulary, recognition) 0–8 (paraphrasing)) (Grisso 1998); DAS‐II, Differential Ability Scales—Second Edition (T‐scores) (Elliott 2007); DKEFS, Delis–Kaplan Executive Function System (scaled scores) (Delis et al. 2001); NEPSY‐II, Developmental Neuropsychological Assessment—Second Edition (scaled scores) (Korkman et al. 2007); RAVLT, Rey Auditory Verbal Learning Test (Brazilian standardization: Diniz et al. 2000); VSRT, Verbal Selective Reminding Test (learning slope/number of words) (Buschke and Fuld 1974); CVLT‐C, California Verbal Learning Test, Children's version (number of words/percentages) (Delis et al. 1994); WRAT‐4, Wide Range Achievement Test, Fourth Edition (combined scaled score) (Wilkinson and Robertson 2006); WIAT‐I, Wechsler Individual Achievement Test, First Edition (standard scores) (Wechsler 1992); and ITBS, Iowa Test of Basic Skills (percentiles) (Hoover et al. 1996).
Equivalent to the Vocabulary and Information subtests.
Canadian supplementary.
Verbal IQ subtests = Information, Similarities, Arithmetic, Vocabulary, Comprehension and Digit span, and Verbal Comprehension. Index subtests = Information, Similarities, Vocabulary and Comprehension.
Brazilian standardization.
Authors reported p = 0.004.
Authors reported p = 0.06; however, in our analysis we accounted for Hartley's test for equal variance, p = 0.008; Cohen's d and Hedge's g effect sizes: small = 0.2, medium = 0.5 and large = 0.8.
Statistical analysis
Pooled samples t‐tests in SPSS were undertaken to examine between group differences when studies reported group comparisons with more than two groups, and when post‐hoc tests were reported without p‐values. Where effect sizes were not reported for between‐group comparisons, we calculated these with Cohen's d, and for one study with unequal group sizes (Lewis et al. 2015), with Hedge's g (d/g: small = 0.2, medium = 0.5, large = 0.8) (Cohen 1988).
Results
Study selection
As shown in figure 1, the initial search yielded 4264 records following the removal of 2577 duplicates. Title and abstract screening resulted in 165 records being retained for full‐text screening from which 158 records were excluded. We achieved interrater agreement of 98% at the title and abstract screening stage and 95% at the full text screening stage. Team discussion resulted in 100% consensus at each stage. Reasons for full‐text exclusion included incorrect participant population (n = 130), comparator group (n = 5), outcomes (n = 21) and language (n = 2). The remaining seven search results were consistent with the inclusion criteria and were included in this review. No further studies were identified as meeting the inclusion criteria when the search was rerun in July 2020.
FIGURE 1.
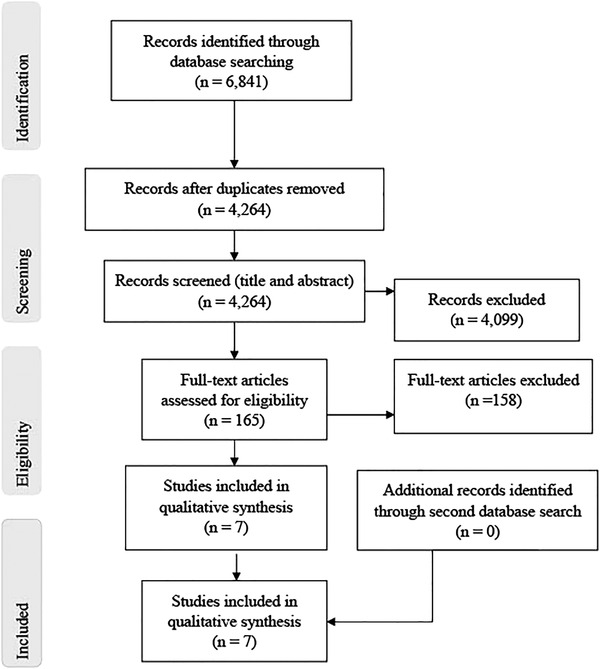
PRISMA flow diagram showing the process and selection of included studies (Moher et al. 2009)
Study and participant characteristics
Study and participant characteristics of five of the seven included studies are reported in table 1. Three of the seven studies contained unique participant groups from Brazil, Canada and the United States (Furtado and de Sa Roriz 2016, Lewis et al. 2015, McLachlan et al. 2014), and are reported in table 1. Two of the seven studies, also from the United States, reported data for the same participants, but on different outcomes and ages (Coles et al. 2010, Howell et al. 2006). We report the study and participant characteristics for the study with the largest sample (Howell et al. 2006) in table 1 while study and participant characteristics for the other study are provided in table S2 in the additional supporting information. The remaining two of seven studies are from the Collaborative Initiative on Fetal Alcohol Spectrum Disorders (CIFASD) research group, also in the United States, who reported data for the same participants, but on different outcomes (Doyle et al. 2018, Panczakiewicz et al. 2016). We include the study and participant characteristics for the study that reported data for one combined PAE and one no/low PAE group (Doyle et al. 2018) in table 1. Study and participant characteristics for the remaining study, with PAE subgroups according to gender, are provided in table S2 in the additional supporting information.
All included studies were observational, and all but one were cohort in design. There was a total of 388 adolescents in the PAE groups, and 542 in the no/low PAE groups (table 1). One study reported on participants who were involved with the criminal justice system (McLachlan et al. 2014), while the remaining reported on participants recruited in clinic (Furtado and de Sa Roriz 2016, Howell et al. 2006, Lewis et al. 2015) or community and clinic (Doyle et al. 2018) settings. Where data are provided, the PAE and no/low PAE groups included a similar percentage of female and male participants. The participant groups reported by Howell et al. (2006) and Lewis et al. (2015) included all or mostly African American participants, while Doyle et al. (2018) included mostly white participants. Data for ethnicity and race were not provided in the remaining two studies. The languages of the participant groups were not reported in any study. However, Furtado and de Sa Roriz (2016) administered tests normed with Brazilian children, and studies from the CIFASD research group excluded participants if English was not their primary language, or if they had been adopted from abroad after 5 years of age or within 2 years of assessment.
Studies that reported sociodemographic data for both the PAE and no/low PAE groups showed that participants were classified as being of low and medium sociodemographic strata (table 1). There were no between‐group differences for the reported variables, with the exception of Furtado and de Sa Roriz (2016) whose groups differed on maternal religion only. Only one study (Howell et al. 2006) reported whether the participants lived with their biological families (PAE + dysmorphic: n = 76%; PAE – dysmorphic: n = 78%; no/low PAE: n = 93%).
Intelligence scores (full‐scale IQ or general conceptual ability) for both the PAE and no/low PAE groups were reported for all the included studies except one (Lewis et al. 2015) in which a score for all participants combined was reported. The IQ scores of the PAE and no/low PAE groups in one study (Furtado and de Sa Roriz 2016) were not different. However, the IQ scores of the PAE groups in two studies (Doyle et al. 2018, McLachlan et al. 2014) were lower than those of the no/low PAE groups. Further, IQ scores of the PAE + dysmorphic group in another study (Howell et al. 2006) were lower than those of both the PAE – dysmorphic and no/low PAE groups. Doyle et al. (2018), who did not adjust for intelligence, cited Dennis et al. (2009) who argues against adjusting for IQ in studies related to populations with neurodevelopmental disorders. For the studies that have controlled for IQ and other variables, details are reported within the results on communication outcomes below.
PAE definitions and FASD determination
Definitions of PAE and no/low PAE groups differed between studies and are based on scores from measures used to assess alcohol dependence or thresholds for daily/weekly alcohol use (table 2). For those studies that used daily/weekly thresholds, the thresholds were reported by number of alcoholic drinks or amount of AA. In the United States, where the studies that used thresholds took place, one standard drink is equal to 0.6 oz of AA (National Institute on Alcohol Abuse and Alcoholism). Based on this definition, PAE thresholds ranged from more than or equal to two standard drinks per week to more than or equal to 13 standard drinks per week during pregnancy for the PAE groups. For the no/low PAE groups, threshold ranged from alcohol abstinence to less than one standard drink per day during pregnancy. The one study with a FASD group, rather than a PAE group (McLachlan et al. 2014), used a published FASD diagnostic guideline (Chudley et al. 2005).
Quality assessment
Quality assessment outcomes of the included studies ranged from good to strong (table 1). Areas of weakness included inadequate description of the study question or objective, limited provision of participant characteristics, lack of investigator blinding and possible measurement errors when assessing PAE (Sayal 2007) (see table S3 in the additional supporting information).
Communication outcomes
Across studies, data were reported for multiple tasks related to oral language skills, verbal processing skills that underlie and support communication skills and written language skills (table 3). Oral communication outcomes predominantly drew on semantic knowledge and organization, with no reported measures of speech or syntactic skills in any study.
Oral language
Semantic knowledge and organization
Four studies reported on five different tasks related to semantic knowledge and organization. McLachlan et al. (2014) compared outcomes among adolescents with FASD to those with no/low PAE, while three studies examined outcomes among those with PAE and no/low PAE. Howell et al. (2006) reported on subgroups within the PAE group (± dysmorphic) and Panczakiewicz et al. (2016) reported on male and female subgroups within both the PAE and no/low PAE groups.
In the comparison of adolescents with FASD with those with no/low PAE, McLachlan et al. (2014) reported between‐group differences for all six measures (vocabulary, sentence recognition and paraphrasing with and without Canadian supplementary versions). In comparisons of adolescents with PAE versus no/low PAE, results were mixed. Furtado and de Sa Roriz (2016) found no differences between groups for vocabulary, general knowledge or similarities. Howell et al. (2006), who conducted post‐hoc between‐group analyses, found a difference between the PAE + dysmorphic subgroup and the no/low PAE group for vocabulary, but not for similarities. However, in our analysis using pooled samples t‐tests, we identified a difference between these two groups for both vocabulary and similarities. Panczakiewicz et al. (2016) identified a difference on word definitions and similarities between the PAE and no/low PAE groups.
McLachlan et al. (2014) identified that IQ was predictive of all six outcomes (vocabulary, sentence recognition and paraphrasing with and without Canadian supplementary versions), and after controlling for IQ that reading was also associated with the six outcomes. However, when controlling for both IQ and reading, group membership was not predictive of any of the six outcomes. Panczakiewicz et al. (2016) identified that among their participants, age did not interact with any of their outcomes for semantics. Overall, within the language domain of semantics, measures of word definitions were the most administered tasks. Group differences on these were common, with those in the PAE groups demonstrating weaker skills than those in the no/low PAE groups in most studies.
Verbal processing skills
Verbal intelligence
Two studies reported on communication‐related skills as measured by verbal IQ and verbal comprehension, comparing outcomes of adolescents with PAE and no/low PAE. Furtado and de Sa Roriz (2016), who excluded participants with an IQ < 70 or a language disorder, reported no group differences for verbal IQ, and both groups scored in the average range. Howell et al. (2006) included participants with intellectual and language disorders; they identified differences for both verbal IQ and verbal comprehension between the PAE + dysmorphic subgroup and the no/low PAE group, and both PAE subgroups and the no/low PAE group scored below the average range on the measures.
Phonological and semantic processing skills
Three studies reported on two different tasks related to access and retrieval of lexical items. All three compared outcomes of adolescents with PAE and no/low PAE. Doyle et al. (2018) and Panczakiewicz et al. (2016) reported on the same participants. Furtado and de Sa Roriz (2016) identified a difference for semantic verbal fluency, but not for phonemic verbal fluency. Doyle et al. (2018) and Panczakiewicz et al. (2016) identified group differences for two word‐generation measures (semantic only, and semantic and initial letter combined) and a speeded naming measure. Panczakiewicz et al. (2016) found that age did not interact with the outcome for word generation.
Verbal working memory
Two studies reported on a digit span task. Howell et al. (2006) included subgroups within the PAE group (± dysmorphic). Both Howell et al. (2006) and Furtado and de Sa Roriz (2016) found no between‐group differences for digit span (total: forwards and backwards).
Verbal learning and memory
Four studies administered three different tasks related to verbal learning and memory. All four compared outcomes of adolescents with PAE and no/low PAE. Panczakiewicz et al. (2016) reported data for different subgroups in both the PAE and no/low PAE groups (male and female), and Coles et al. (2010) and Lewis et al. (2015) reported data for subgroups within the PAE group (± dysmorphic, and heavy and moderate). For verbal processing skills that underlie and support communication skills, semantic processing as well as verbal learning and memory were the most commonly reported measures. Group differences were identified for these measures across most studies, with the PAE groups demonstrating weaker skills than the no/low PAE groups.
Panczakiewicz et al. (2016) identified differences between the PAE and no/low PAE groups for a word‐level memory measure (memory for names) and a text‐level memory measure (narrative memory). For outcomes related to word‐list learning, Furtado and de Sa Roriz (2016) found no differences between groups for any of the measures. In contrast, Coles et al. (2010) identified group differences between both PAE subgroups (± dysmorphic) and the no/low PAE group for four of six measures (total recall, trial 8, long‐term storage, consistent long‐term retrieval), and between the PAE + dysmorphic subgroup and the no/low PAE group for the remaining two of six measures (learning slope and delayed recall). Lewis et al. (2015), who included heavy and moderate PAE subgroups, and whose no/low PAE group had the highest threshold for no/low PAE, identified differences between the PAE + heavy subgroup and the no/low PAE group for three of five measures (short delay recall, long delay recall and recognition discrimination).
Panczakiewicz et al. (2016) identified that age did not interact with memory outcomes. When controlling for IQ, Coles et al. (2010) found that the results changed for total recall only, and only between the PAE – dysmorphic subgroup and the no/low PAE group. Coles et al. (2010) also examined forgetting across groups by analyzing delayed recall in the context of total recall, long‐term storage and consistent long‐term retrieval. There was no difference between groups for forgetting. When Lewis et al. (2015) controlled for socioeconomic status, maternal vocabulary and maternal smoking in pregnancy, differences between the groups remained. Lewis et al. also identified that outcomes were not related to prenatal exposure to marijuana or cocaine.
Written language skills
Reading
Two studies reported on reading using three different measures. McLachlan et al. (2014) compared outcomes among adolescents with FASD and no/low PAE, while Howell et al. (2006) compared outcomes between PAE subgroups (± dysmorphic) and a no/low PAE group. McLachlan et al. (2014) identified differences between the FASD and no/low PAE groups for their reading measure (combined score for identification of letters, word reading, and sentence‐level reading comprehension). Howell et al. (2006) also identified a difference for one reading measure (combined score for receptive vocabulary and text‐level reading) between the PAE + dysmorphic subgroup and the no/low PAE group, but not for another reading measure (non‐word and word‐reading).
Spelling
Just one study reported on spelling. Howell et al. (2006), who included two PAE subgroups (± dysmorphic), did not identify a difference between groups in their post‐hoc tests. However, in our analysis, we identified a difference between the PAE + dysmorphic subgroup and the no/low PAE group for single‐word spelling.
Discussion
We synthesized the published, peer‐reviewed literature on oral and written communication skills of adolescents who have PAE compared with those with no/low PAE. Studies included in this review demonstrated that participants with PAE generally had weaker skills in vocabulary and semantic knowledge, semantic processing, verbal learning and memory, as well as reading and spelling compared with those with no/low PAE. However, these findings were inconsistent across studies and measures. For the domain of oral language, two studies found between‐group differences on all measures of semantic knowledge and organization, and another found differences on all tasks but only for the comparison between adolescents with PAE plus dysmorphic features and those with no/low PAE. One found no difference on any task. For verbal processing skills, one study found differences on semantic verbal fluency but not phonemic verbal fluency, verbal IQ, working memory, or verbal learning and memory. Another study found differences on verbal IQ, for just adolescents with PAE plus dysmorphic features compared with those with no/low PAE, but not for working memory. Two studies found differences on both tasks administered (semantic verbal fluency and rapid naming, and semantic verbal fluency and learning and memory, respectively). Another study identified differences on all six subtests of a verbal learning and memory task; however, on two of these subtests, between group differences were not observed for the comparison involving the PAE group who did not have dysmorphic features. A further study identified differences for three out of five subtests of a verbal learning and memory task, but only for comparisons involving adolescents with heavy levels of PAE and those with no/low PAE. For written language skills, one study found between group differences for reading, while the other reported differences for spelling and one of two reading tasks, but only for comparisons involving adolescents with PAE plus dysmorphic features. Studies were rated as having either good or strong quality.
In line with the findings of previous systematic reviews, methodological differences for the included studies potentially contributed to mixed findings. Together, with the small number of studies identified and included, this limits our capacity to draw robust conclusions from the extant literature. We identified inconsistency in the definitions used to allocate participants to groups based on PAE levels. No safe level of PAE has been identified, methods used to assess PAE vary, and the effect of alcohol on the foetus can be influenced by other exposures, timing and dose of PAE, as well as individual differences in alcohol metabolism (Popova et al. 2017). Misclassification of participants is likely to have also occurred within the included studies due to caregiver‐fears of stigmatization as well as memory and recall bias (Sayal 2007). Furthermore, assessment and diagnostic guidelines for FASD differ internationally. Accordingly, it is possible that the definitions used to allocate research participants to PAE groups will continue to lack consistency. To determine the source of variation in communication profiles of individuals with and without PAE, it will be important that there is consistency in the ways in which PAE is assessed and defined in future research.
Previous systematic reviews related to individuals with FASD or PAE and which reported communication outcomes emphasize a need to consider additional confounding factors. While socioeconomic status (SES) was considered in most studies in this review, most reported on adolescents from medium and low socioeconomic strata, highlighting a dearth of knowledge related to higher SES groups. Given that PAE is also associated with educational attainment and economic advantage (Hutchinson et al. 2013, McCormack et al. 2017, Muggli et al. 2016), research with groups from medium to high SES will contribute to a better understanding of the effects of PAE on communication skills. This review revealed that little is known about the communication skills of adolescents with PAE in relation to caregiving and trauma backgrounds. We further identified that most studies lacked data related to the languages spoken of the participants. The languages used, as well as the culture and caregiving environment of a child heavily influences language skill development (Norbury and Sparks 2013). Therefore, it is important that future research considers and accounts for these variables.
We identified that participants were assessed predominantly using tasks that draw on semantic knowledge and organization. Vocabulary knowledge is enriched within the lexicon, and the breadth, depth and organization of semantic knowledge promotes the ability to efficiently appreciate and convey meaning (Levelt 1995). Semantic knowledge is fundamental to educational and occupational success (Lowe et al. 2018). In this review, we found that expressive vocabulary skills were generally weaker among adolescents with PAE compared with those with no/low PAE. Receptive vocabulary skills are also important when examining semantic skills; however, data for receptive vocabulary were not reported in any of the included studies.
Semantic knowledge and organization were also assessed on other measures such as similarities, sentence recognition, paraphrasing, semantic processing and reading comprehension. Across most studies, adolescents with PAE performed more poorly than those with no/low PAE. This may reflect the influence of their weaker expressive vocabulary knowledge on more complex word‐ and sentence‐level language‐based tasks and highlights the importance of examining vocabulary and semantic skills comprehensively.
Word learning involves the encoding and mapping of phonological (sound based) and semantic representations of words (Brackenbury and Pye 2005). Phonological representations are encoded using phonological memory skills (Gathercole 2006). Semantic representations, which are thought to develop through syntactic, semantic, pragmatic and social–cognitive cues, map onto their respective phonological representations (Brackenbury and Pye 2005, Stackhouse and Wells 1997). A robust measure of phonological memory skills is non‐word repetition (Gathercole 2006); however, none of the included studies reported non‐word repetition data. Individual subtest data for digit span forwards, also a measure of phonological memory (Rasmussen 2005), was also not reported. Research with 9‐year‐old children with PAE and no/low PAE has shown that the patterns of neural activation involved in phonological memory differ, indicating atypical phonological skills among those with PAE (Diwadkar et al. 2013). Further, the transition from visual to verbal memory strategies, which draws on phonological memory skills, occurs in late childhood and early adolescence among children with FASD, which is much later than for children without FASD (Rasmussen et al. 2009). The lack of evidence about phonological memory skills identified in this review makes it difficult to draw conclusions about if, and how, phonological memory skills of adolescents with PAE compare with those with no/low PAE, and how they relate to word learning and semantic knowledge.
In the studies included in this review, participants were also assessed on verbal working‐memory and verbal learning and memory measures. While we identified no between‐group differences in verbal working memory, there was an identified trend for verbal learning and memory skills to decrease according to the presence of dysmorphology (Coles et al. 2010) and the level of PAE (Lewis et al. 2015). Age‐related specialization of neural systems that underlies memory skills occurs across childhood and adolescence (Bathelt et al. 2018). However, PAE is associated with smaller brain volumes and atypical brain structures, including those important for memory (Chen et al. 2012, Willoughby et al. 2008). Therefore, a growth deficit related to PAE might contribute to atypical neural development and weaker verbal learning and memory skills among adolescents with PAE.
Using different methods, Lewis et al. (2015) and Coles et al. (2010), whose studies differed on sample size, participant age, assessment task and PAE definitions, examined the deficits underlying weaker learning and memory performance among their PAE groups. Coles et al. (2010) suggested that memory difficulties among their participants with PAE are linked to encoding problems rather than a tendency to forget learned information. Lewis et al. (2015) suggested that memory difficulties among their participants with PAE are linked to problems with retention as well as inefficient strategies to access and retrieve words. Further, as discussed by Lewis et al. (2015) and Furtado and de Sa Roriz (2016), a semantic clustering strategy, which can support memory and recall, is used less frequently and effectively by individuals who have PAE. The findings in this review for verbal fluency show that semantic information is accessed and retrieved less efficiently by adolescents with PAE. A specific deficit in semantic skills was posited by Furtado and de Sa Roriz (2016) as being a key consequence of PAE, given that semantic verbal fluency was the only verbal measure in their study in which group differences were identified, and that children who have FASD have abnormal neural activation of a language processing area in the temporal lobe (Sowell et al. 2007). Access to and retrieval of words is complex, and thought to be supported by the robustness of stored phonological and semantic representations as well as the ability to use retrieval cues (Brackenbury and Pye 2005, Levelt 1995). While limited, our findings indicate that in assessment of memory and learning skills with adolescents with PAE, it is important to consider both lexical storage and retrieval strategies.
Few studies in this review examined reading and spelling skills. However, those that did indicated that adolescents with PAE perform more poorly. As reading requires skills in both the decoding of graphemes, as well as in receptive language, weaknesses in one or both can compromise reading ability (Nation 2019). Howell et al. (2006) identified that the receptive vocabulary and text‐level reading comprehension score was lower among adolescents with PAE. As these participants’ scores for non‐word and word reading were similar for both groups, albeit below the expected level for their age, it is likely that receptive language skills, rather than decoding skills, underlie the between‐group difference for the reading scores. This is supported by our findings in the domain of semantic knowledge. In addition, Doyle et al. (2018) showed that adolescents with PAE have weaker rapid naming skills, which has implications for decoding, word recognition and reading fluency (Norton and Wolf 2012). As a result, both reading and spelling skills can be compromised. Our findings highlight that for adolescents with PAE, assessment should consider phonological processing, decoding and receptive language skills, and the impact these have on literacy skill development.
Several studies included in this review reported on communication measures that draw on grammar comprehension and expression. For example, tasks involving sentence and text levels of language require grammatical skills, in addition to semantic and memory skills, to support language processing (Levelt 1995). However, none of the studies used measures of grammar, nor reported directly on grammatical skills. Therefore, it is unclear how the grammatical skills of adolescents who have PAE compare with those with no/low PAE, and what implications there are for their communication ability.
Implications for clinical practice and research
Our findings are important to functioning and well‐being in adolescence and have implications for clinicians working across a variety of settings. For example, in a school setting, students who lack competence in oral and written communication skills are likely to have problems with the comprehension and production of both oral and written texts (Lowe et al. 2018, Nippold et al. 2009). As a result, a student may have difficulty extending and demonstrating their knowledge, and in turn, meeting the requirements of the school curriculum. A pilot speech–language pathology intervention study with 9‐year‐old students with FASD revealed that gains in language and literacy skills can be made (Adnams et al. 2007), suggesting an important role for speech–language pathologists within schools to deliver services to improve language and literacy outcomes of students with PAE and FASD. However, there is a dearth of research investigating language and literacy interventions for adolescent students who have PAE. Given our findings that adolescents with PAE have difficulties with both oral and written communication skills, and that completing school is important to adolescent students who have FASD (Duquette et al. 2006), future research investigating the effectiveness of language and literacy interventions is required to inform clinical practice.
Our findings are also relevant to social and emotional well‐being. Language skills are critical to supporting the recognition and labelling of emotions (Griffiths et al. 2020). Among children and adolescents with FASD, strengths in emotion recognition support adaptive functioning in the classroom (Crawford et al. 2020), and expressive vocabulary skills are associated with social perspective‐taking (Stevens et al. 2015). Given that social and emotional well‐being are areas of identified difficulty for children and adolescents who have PAE (Coggins et al. 2007, Kjellmer and Olswang 2013, Schonfeld et al. 2005), it is imperative that assessment and service provision with them includes consideration of communication skills.
Weak communication skills also have implications for forensic contexts, compromising psycho‐legal abilities and, potentially, success in rehabilitation and educational programmes (McLachlan et al. 2014, Rost and McGregor 2012). Adolescents and adults who have either or both FASD and language deficits are over‐represented, yet often under‐identified, in justice settings (Kippin et al. 2018, McLachlan et al. 2019). Therefore, it is critical that the communication demands of forensic contexts are understood by the justice workforce, and that policies and practices are introduced that better enable the identification and response to an individual's communication needs (Kippin et al. 2018, Rost and McGregor 2012). For example, providing neurocognitive assessment upon an individual's entry into the justice system can support more responsive rehabilitation efforts and more equitable outcomes for young people with PAE (Reid et al. 2020).
A common finding amongst the research identified in this review is that many of the scores, for both the PAE and no/low PAE groups, did not fall into impaired thresholds as used in FASD diagnostic guidelines, despite there being significant differences between groups as well as potential for functional communication problems. According to the revised Institute of Medicine Guideline for diagnosing FASD (Hoyme et al. 2016), impairment of a neurocognitive skill is defined as a score of ≥ 1.5 SDs below the mean while in both the Scottish and Australian Guidelines (Bower and Elliott 2016, Scottish Intercollegiate Guidelines Network 2019) impairment is defined as a score of ≥ 2 SDs below the mean. Our findings highlight the possibility that many adolescents who have PAE may not meet criteria for a FASD diagnosis based on their language and communication scores, while if they meet criteria based on scores for other diagnostic domains, they may not have their oral and written communication needs prioritized.
In the identification of communication impairments more broadly, in both clinical practice and research, there is no one cut‐off score that is used universally (Bishop et al. 2016). It is important that consideration is given as to whether test scores are significantly different to those of their peers, and that, in addition to caregiver and teacher reports, direct assessment incorporates activities that are meaningful and relevant to the individual, to account for the functional impacts of communication difficulties (Bishop et al. 2016, Westby and Washington 2017). In this review, we identified that just one study (McLachlan et al. 2014) considered functional assessment, in which supplemental language items specific to the Canadian legal system were incorporated into assessment of psycho‐legal abilities. Given that all the study participants were involved with the Canadian legal system, the supplemental items have practical relevance to the identification of specific psycho‐legal abilities needed to participate in the Canadian criminal justice system. In research and clinical practice related to PAE, comprehensive and direct assessment of communication skills using both standardized and functional tasks is important and should not be underestimated.
A further limitation that may arise from these thresholds for impairment is the lack of clarity regarding their appropriacy to warrant a neurodevelopmental disorder diagnosis among peoples from non‐dominant languages and cultures (Bishop et al. 2016, Norbury and Sparks 2013). The language(s) used by an individual to communicate, as well as assessment methods, should be carefully considered when planning and delivering assessment services to ensure that an individual's communication skills are appropriately and accurately examined.
Speech–language pathologists have a key role to play in assessment and intervention with individuals who have PAE (Popova et al. 2014). Further, speech–language pathology assessment is recommended in assessment guidelines for FASD (Bower and Elliott 2016, Hoyme et al. 2016, Scottish Intercollegiate Guidelines Network 2019). Increased speech–language pathology involvement in clinical practice and research related to PAE and FASD is likely to advance a more nuanced understanding of the communication profiles of adolescents with PAE. This is important to inform more targeted assessment, supports and interventions into the future.
Strengths and limitations
We set a specific age range for inclusion in this review and followed a systematic process to search for and review studies. Our search was broad, including terms drawn from the speech, language and literacy literature, as well as terms relating to cognitive processing skills that underlie communication skills. While we did not select PubMed in the initial search strategy, we included it in an additional search and found no further records that met the inclusion criteria.
We did not conduct a meta‐analysis due to the limited number of studies identified, few studies reporting data for each outcome, as well as the methodological variations such as the PAE definitions used to allocate participants to groups. While we identified a small knowledge base with equivocal findings, we identified that the most assessed skills, which were semantic knowledge, semantic processing, and verbal learning and memory, were commonly weaker among adolescents with PAE compared with those with no/low PAE.
CONCLUSIONS
There has been limited investigation of oral and written communication skills of adolescents with PAE compared with those with no/low PAE. Variability between studies, as well as the limited research base, make it difficult to compare study results and draw conclusions. However, our results highlight that adolescents with PAE have weaker skills in some areas of oral and written communication, as well as in verbal processing skills that underlie and support communication skills, compared with those with no/low PAE. Both oral and written communication skills in the adolescent years underpin social and educational development and support the transition to becoming more independent. Our results emphasize that for adolescents with PAE, communication skills in both oral and written modalities should be comprehensively understood in assessment and when planning interventions.
DECLARATION OF INTEREST
None.
AVAILABILITY
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Supporting information
Table S1. PsycInfo search strategy (19 March 2019).
Table S2. Study and participant characteristics for included studies that reported on the same participant groups in table 1.
Table S3. Quality assessment of seven included studies.
Kippin, N. R. , Leitão, S. , Watkins, R. , & Finlay‐Jones, A. . Oral and written communication skills of adolescents with prenatal alcohol exposure (PAE) compared with those with no/low PAE: A systematic review. International Journal of Language & Communication Disorders. 2021;56:694–718. 10.1111/1460-6984.12644
Funding information
FASD Research Australia CRE PhD scholarship and Australian Government Research Training Program PhD Scholarship (NRK); FASD Research Australia CRE (National Health and Medical Research Council of Australia grant number 1110341) (RW/AFJ).
NOTES
REFERENCES
- Adnams, C.M. , Sorour, P. , Kalberg, W.O. , Kodituwakku, P. , Perold, M.D. , Kotze, A. , et al. (2007) Language and literacy outcomes from a pilot intervention study for children with fetal alcohol spectrum disorders in South Africa. Alcohol, 41, 403–414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bathelt, J. , Gathercole, S.E. , Johnson, A. & Astle, D.E. (2018) Differences in brain morphology and working memory capacity across childhood. Developmental Science, 21, e12579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becker, M. , Warr‐Leeper, G.A. & Leeper, H.A. (1990) Fetal alcohol syndrome: a description of oral motor, articulatory, short‐term memory, grammatical, and semantic abilities. Journal of Communication Disorders, 23, 97–124. [DOI] [PubMed] [Google Scholar]
- Bishop, D.V.M. , Snowling, M.J. , Thompson, P.A. & Greenhalgh, T. & CATALISE CONSORTIUM (2016) CATALISE: a multinational and multidisciplinary Delphi consensus study. Identifying language impairments in children. PLoS One, 11, e0158753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blakemore, S.J. (2018) Inventing ourselves: The secret life of the teenage brain. London, United Kingdom: Transworld Publishers. [Google Scholar]
- Bower, C. & Elliott, E.J. (2016) Australian guide to the diagnosis of fetal alcohol spectrum disorder (FASD): Report to the Australian Government Department of Health.
- Brackenbury, T. & Pye, C. (2005) Semantic deficits in children with language impairments: issues for clinical assessment. Language, Speech, & Hearing Services in Schools, 36, 5–16. [DOI] [PubMed] [Google Scholar]
- Buschke, H. & Fuld, P.A. (1974) Evaluating storage, retention and retrieval in disordered memory and learning. Neurology, 24, 1019–1025. [DOI] [PubMed] [Google Scholar]
- Chen, X. , Coles, C.D. , Lynch, M.E. & Hu, X. (2012) Understanding specific effects of prenatal alcohol exposure on brain structure in young adults. Human Brain Mapping, 33, 1663–1676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chudley, A.E. , Conry, J. , Cook, J.L. , Loock, C. , Rosales, T. & Leblanc, N. (2005) Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis. Canadian Medical Association Journal, 172, S1–S21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coggins, T.E. , Timler, G.R. & Olswang, L.B. (2007) A state of double jeopardy: impact of prenatal alcohol exposure and adverse environments on the social communicative abilities of school‐age children with fetal alcohol spectrum disorder. Language, Speech, & Hearing Services in Schools, 38, 117–127. [DOI] [PubMed] [Google Scholar]
- Cohen, J. (1988) Statistical power analysis for the behavioural sciences, second edition. Mahwah, Lawrence Erlbaum Associates. [Google Scholar]
- Coles, C.D. , Lynch, M.E. , Kable, J.A. , Johnson, K.C. & Goldstein, F.C. (2010) Verbal and nonverbal memory in adults prenatally exposed to alcohol. Alcoholism: Clinical and Experimental Research, 34, 897–906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crawford, A. , Te Nahu, L.T.H. , Peterson, E.R. , McGinn, V. , Robertshaw, K. & Tippett, L. (2020) Cognitive and social/emotional influences on adaptive functioning in children with FASD: Clinical and cultural considerations. Child Neuropsychology, 26, 1112–1144. [DOI] [PubMed] [Google Scholar]
- Dahl, R.E. , Allen, N.B. , Wilbrecht, L. & Suleiman, A.B. (2018) Importance of investing in adolescence from a developmental science perspective. Nature, 554, 441–450. [DOI] [PubMed] [Google Scholar]
- Day, N.L. , Helsel, A. , Sonon, K. & Goldschmidt, L. (2013) The association between prenatal alcohol exposure and behavior at 22 years of age. Alcoholism: Clinical and Experimental Research, 37, 1171–1178. [DOI] [PubMed] [Google Scholar]
- De Beer, M. , Kritzinger, A. & Zsilavecz, U. (2010) Young children with fetal alcohol spectrum disorder—Communication profiles. South African Journal of Communication Disorders, 57, 33–42. [DOI] [PubMed] [Google Scholar]
- Delis, D.C. , Kaplan, E. & Kramer, J.H. (2001) The Delis–Kaplan executive function system (DKEFS): Examiner's Manual. San Antonio, TX: Psychological Corporation. [Google Scholar]
- Delis, D.C. , Kramer, J.H. , Kaplan, E. & Ober, B.A. (1994) The California Verbal Learning Test, Children's version. New York: Psychological Corporation. [Google Scholar]
- Dennis, M. , Francis, D.J. , Cirino, P.T. , Schachar, R. , Barnes, M.A. & Fletcher, J.M. (2009) Why IQ is not a covariate in cognitive studies of neurodevelopmental disorders. Journal of the International Neuropsychological Society, 15, 331–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DEPARTMENT OF HEALTH . 2020. Standard drinks guide. [Online]. Available: https://www.health.gov.au/health‐topics/alcohol/about‐alcohol/standard‐drinks‐guide [Accessed 27 November].
- Diniz, L.F.M. , Cruz, M.D.F.D. , Torres, V.D.M. & Cosenza, R.M. (2000) O teste de aprendizagem auditivo‐verbal de Rey: normas para uma populacao brasileira. Revista Brasileira de Neurologia, 3, 79–83. [Google Scholar]
- Diwadkar, V.A. , Meintjes, E.M. , Goradia, D. , Dodge, N.C. , Warton, C. , Molteno, C.D. , et al. (2013) Differences in cortico‐striatal‐cerebellar activation during working memory in syndromal and nonsyndromal children with prenatal alcohol exposure. Human Brain Mapping, 34, 1931–1945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doyle, L.R. , Moore, E.M. , Coles, C.D. , Kable, J.A. , Sowell, E.R. , Wozniak, J.R. , et al. (2018) Executive functioning correlates with communication ability in youth with histories of heavy prenatal alcohol exposure. Journal of the International Neuropsychological Society, 24, 1026–1037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duquette, C. , Stodel, E. , Fullarton, S. & Hagglund, K. (2006) Persistence in high school: Experiences of adolescents and young adults with fetal alcohol spectrum disorder. Journal of Intellectual and Developmental Disability, 31, 219–231. [DOI] [PubMed] [Google Scholar]
- Elliott, C.D. (2007) Differential ability scales, second edition (DAS‐II). (San Antonio, TX: Harcourt Assessment; ). [Google Scholar]
- Flak, A.L. , Su, S. , Bertrand, J. , Denny, C.H. , Kesmodel, U.S. & Cogswell, M.E. (2014) The association of mild, moderate, and binge prenatal alcohol exposure and child neuropsychological outcomes: A meta‐analysis. Alcoholism: Clinical and Experimental Research, 38, 214–226. [DOI] [PubMed] [Google Scholar]
- Furtado, E.F. & De Sa Roriz, S.T. (2016) Inattention and impulsivity associated with prenatal alcohol exposure in a prospective cohort study with 11‑years‑old Brazilian children. European Child & Adolescent Psychiatry, 25, 1327–1335. [DOI] [PubMed] [Google Scholar]
- Gathercole, S.E. (2006) Nonword repetition and word learning: The nature of the relationship. Applied Psycholinguistics, 27, 513–543. [Google Scholar]
- Glass, L. , Graham, D.M. , Akshoomoff, N. & Mattson, S.N. (2015) Cognitive factors contributing to spelling performance in children with prenatal alcohol exposure. Neuropsychology, 29, 817–828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffiths, S. , Goh, S.K.Y. & Norbury, C.F. & TEAM., T. S . (2020) Early language competence, but not general cognitive ability, predicts children's recognition of emotion from facial and vocal cues. PeerJ, 12, e9118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grisso, T. (1998) Instruments for assessing understanding and appreciation of Miranda rights. Sarasota, FL: Professional Resources Press. [Google Scholar]
- Hendricks, G. , Malcolm‐Smith, S. , Adnams, C. , Stein, D.J. & Donald, K.A.M. (2019) Effects of prenatal alcohol exposure on language, speech and communication outcomes: A review longitudinal studies. Acta Neuropsychiatrica, 31, 74–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry, J. , Sloan, M. & Black‐Pond, C. (2007) Neurobiology and neurodevelopmental impact of childhood traumatic stress and prenatal alcohol exposure. Language, Speech, and Hearing Services in Schools, 38, 99–108. [DOI] [PubMed] [Google Scholar]
- Howell, K.K. , Lynch, M.E. , Platzman, K.A. , Smith, G.H. & Coles, C.D. (2006) Prenatal alcohol exposure and ability, academic achievement, and school functioning in adolescence: A longitudinal follow‐up. Journal of Pediatric Psychology, 31, 116–126. [DOI] [PubMed] [Google Scholar]
- Hoover, H.D. , Hieronymus, A.N. , Frisbie, D.A. & Dunbar, S.B. (1996) Iowa test of basic skills. Itasca, IL: Riverside Publishing. [Google Scholar]
- Hoyme, H.E. , Kalberg, W.O. , Elliott, A.J. , Blankenship, J. , Buckley, D. , Marais, A. , et al. (2016) Updated clinical guidelines for diagnosing fetal alcohol spectrum disorders. Pediatrics, 138, e2 0154256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hutchinson, D. , Moore, E.A. , Breen, C. , Burns, L. & Mattick, R.P. (2013) Alcohol use in pregnancy: prevalence and predictors in the. Longitudinal Study of Australian children Drug & Alcohol Review, 32, 475–482. [DOI] [PubMed] [Google Scholar]
- Hyter, Y.D. (2007) Understanding children who have been affected by maltreatment and prenatal alcohol exposure. Language, Speech, & Hearing Services in Schools, 38, 93–98. [DOI] [PubMed] [Google Scholar]
- Iosub, S. , Fuchs, M. , Bingol, N. & Gromisch, D.S. (1981) Fetal alcohol syndrome revisited. Pediatrics, 68, 475–479. [PubMed] [Google Scholar]
- Irner, T.B. (2012) Substance exposure in utero and developmental consequences in adolescence: A systematic review. Child Neuropsychology, 18, 521–549. [DOI] [PubMed] [Google Scholar]
- Kambeitz, C. , Klug, M.G. , Greenmyer, J. , Popova, S. & Burd, L. (2019) Association of adverse childhood experiences and neurodevelopmental disorders in people with fetal alcohol spectrum disorders (FASD) and non‐FASD controls. BMC Pediatrics, 19, 498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kippin, N.R. , Leitao, S. , Watkins, R. , Finlay‐Jones, A. , Condon, C. , Marriott, R. , et al. (2018) Language diversity, language disorder, and fetal alcohol spectrum disorder among youth sentenced to detention in Western Australia. International Journal of Law and Psychiatry, 61, 40–49. [DOI] [PubMed] [Google Scholar]
- Kjellmer, L. & Olswang, L.B. (2013) Variability in classroom social communication: performance of children with fetal alcohol spectrum disorders and typically developing peers. Journal of Speech, Language, and Hearing Research, 56, 982–993. [DOI] [PubMed] [Google Scholar]
- Kmet, L.M. , Lee, R.C. & Cook, L.S. (2004) Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Canada: Alberta Heritage Foundation for Medical Research. [Google Scholar]
- Kodituwakku, P. , Coriale, G. , Fiorentino, D. , Arago´N, A.S. , Kalberg, W.O. , Buckley, D. , et al. (2006) Neurobehavioral characteristics of children with fetal alcohol spectrum disorders in communities from Italy: Preliminary results. Alcoholism: Clinical and Experimental Research, 30, 1551–15661. [DOI] [PubMed] [Google Scholar]
- Korkman, M. , Kirk, U. & Kemp, S. (2007) NEPSY‐II Clinical and interpretive manual. San Antonio, TX: Harcourt Assessment. [Google Scholar]
- Lange, S. , Probst, C. , Gmel, G. , Rehm, J. , Burd, L. & Popova, S. (2017) Global prevalence of fetal alcohol spectrum disorder among children and youth: A systematic review and meta‐analysis. JAMA Pediatrics, 171, 948–956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, L. , Packer, T.L. , Tang, S.H. & Girdler, S. (2008) Self‐management education programs for age‐related macular degeneration: A systematic review. Australasian Journal on Ageing, 27, 170–176. [DOI] [PubMed] [Google Scholar]
- Lemoine, P. , Harousseau, H. , Borteyru, J.P. & Menuet, J.C. (2003) Children of alcoholic parents — Observed anomalies: discussion of 127 cases. Therapeutic Drug Monitoring, 25, 132–136. [DOI] [PubMed] [Google Scholar]
- Levelt, W.J.M. (1995) The ability to speak: from intentions to spoken words. European Review, 3, 13–23. [Google Scholar]
- Lewis, C.E. , Thomas, K.G.F. , Dodge, N.C. , Molteno, C.D. , Meintjes, E.M. , Jacobson, J.L. , et al. (2015) Verbal learning and memory impairment in children with. Fetal Alcohol Spectrum Disorders. Alcoholism: Clinical and Experimental Research, 39, 724–732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lowe, H. , Henry, L. , Muller, L.‐M. & Joffe, V.L. (2018) Vocabulary intervention for adolescents with language disorder: A systematic review. International Journal of Language & Communication Disorders, 53, 199–217. [DOI] [PubMed] [Google Scholar]
- Lynch, M.E. , Kable, J.A. & Coles, C.D. (2017) Effects of prenatal alcohol exposure in a prospective sample of young adults: mental health, substance use, and difficulties with the legal system. Neurotoxicology and Teratology, 64, 50–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattson, S.N. , Bernes, G.A. & Doyle, L.R. (2019) Fetal alcohol spectrum disorders: a review of the neurobehavioral deficits associated with prenatal alcohol exposure. Alcoholism: Clinical and Experimental Research, 43, 1046–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattson, S.N. & Riley, E.P. (1999) Implicit and explicit memory functioning in children with heavy prenatal alcohol exposure. Journal of the International Neuropsychological Society, 5, 462–471. [DOI] [PubMed] [Google Scholar]
- Mattson, S.N. , Riley, E.P. , Gramling, L. , Delis, D.C. & Jones, K.L. (1998) Neuropsychological comparison of alcohol‐exposed children with or without physical features of Fetal Alcohol Syndrome. Neuropsychology, 12, 146–153. [DOI] [PubMed] [Google Scholar]
- McCormack, C. , Hutchinson, D. , Burns, L. , Wilson, J. , Elliott, E. , Allsop, S. , et al. (2017) Prenatal alcohol consumption between conception and recognition of pregnancy. Alcoholism: Clinical and Experimental Research, 41, 369–378. [DOI] [PubMed] [Google Scholar]
- McLachlan, K. , Flannigan, K. , Temple, V. , Unsworth, K. & Cook, J.L. (2020) Difficulties in daily living experienced by adolescents, transition‐aged youth, and adults with fetal alcohol spectrum disorder. Alcoholism: Clinical and Experimental Research, 44(8), 1609–1624. [DOI] [PubMed] [Google Scholar]
- McLachlan, K. , McNeil, A. , Pei, J. , Brain, U. , Andrew, G. & Oberlander, T.F. (2019) Prevalence and characteristics of adults with fetal alcohol spectrum disorder in corrections: A Canadian case ascertainment study. BMC Public Health, 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLachlan, K. , Roesch, R. , Viljoen, J.L. & Douglas, K.S. (2014) Evaluating the psycholegal abilities of young offenders with. Fetal Alcohol Spectrum Disorder. Law and Human Behavior, 38, 10–22. [DOI] [PubMed] [Google Scholar]
- Mclaughlin, S.A. , Thorne, J.C. , Jirikowic, T. , Waddington, T. , Lee, A.K.C. & Astley Hemingway, S.J. (2019) Listening difficulties in children with fetal alcohol spectrum disorders: More than a problem of audibility. Journal of Speech, Language, and Hearing Research, 62, 1532–1548. [DOI] [PubMed] [Google Scholar]
- Moher, D. , Liberati, A. , Tetzlaff, J. & Altman, D.G. & THE PRISMA GROUP (2009) Preferred reporting items for systematic reviews and meta‐analyses: The PRISMA statement. PLOS Medicine, 6, e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muggli, E. , O'Leary, C. , Donath, S. , Orsini, F. , Forster, D. , Anderson, P.J. , et al. (2016) Did you ever drink more?” A detailed description of pregnant women's drinking patterns. Bmc Public Health [Electronic Resource], 16, 683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nation, K. (2019) Children's reading difficulties, language, and reflections on the simple view of reading. Australian Journal of Learning Difficulties, 24, 47–73. [Google Scholar]
- NATIONAL HEALTH AND MEDICAL RESEARCH COUNCIL (1999) How to review the evidence: Systematic identification and review of the scientific literature. Canberra, AUS: NHMRC. [Google Scholar]
- NATIONAL INSTITUTE ON ALCOHOL ABUSE AND ALCOHOLISM . 2020. What is a standard drink? [Online]. Available: https://www.niaaa.nih.gov/alcohols‐effects‐health/overview‐alcohol‐consumption/what‐standard‐drink [Accessed 6 November]. [Google Scholar]
- Netelenbos, N. , Sanders, J.L. , Dei, S.O. & McDonald, S. (2020) A case for early screening: prenatal alcohol risk exposure predicts risk for early childhood communication delays. Journal of Developmental & Behavioral Pediatrics, 41(7), 559–564. [DOI] [PubMed] [Google Scholar]
- Nippold, M.A. (2016) Later language development: School‐age children, adolescents, and young adults, 4th edition. Austin, Texas, Pro‐Ed. [Google Scholar]
- Nippold, M.A. , Mansfield, T.C. , Billow, J.L. & Tomblin, J.B. (2009) Syntactic development in adolescents with a history of language impairments: A follow up investigation. American Journal of Speech–Language Pathology, 18, 241–251. [DOI] [PubMed] [Google Scholar]
- Norbury, C.F. & Sparks, A. (2013) Difference or disorder? Cultural issues in understanding neurodevelopmental disorders. Developmental Psychology, 49, 45–58. [DOI] [PubMed] [Google Scholar]
- Norton, E.S. & Wolf, M. (2012) Rapid automatized naming (RAN) and reading fluency: implications for understanding and treatment of reading disabilities. Annual Review of Psychology, 63, 427–452. [DOI] [PubMed] [Google Scholar]
- O'Keeffe, L.M. , Greene, R.A. & Kearney, P.M. (2014) The effect of moderate gestational alcohol consumption during pregnancy on speech and language outcomes in children: A systematic review. Systematic Reviews, 3, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Leary, C. , Zubrick, S.R. , Taylor, C.L. , Dixon, G. & Bower, C. (2009) Prenatal alcohol exposure and language delay in 2‐year‐old children: The importance of dose and timing on risk. Pediatrics, 123, 547–554. [DOI] [PubMed] [Google Scholar]
- Olson, H.C. , Feldman, J.J. , Streissguth, A.P. , Sampson, P.D. & Bookstein, F.L. (1998) Neuropsychological deficits in adolescents with fetal alcohol syndrome: clinical findings. Alcoholism: Clinical and Experimental Research, 22, 1998–2012. [PubMed] [Google Scholar]
- Panczakiewicz, A.L. , Glass, L. , Coles, C.D. , Kable, J.A. , Sowell, E.R. , Wozniak, J.R. , et al. (2016) Neurobehavioral deficits consistent across age and sex in youth with prenatal alcohol exposure. Alcoholism: Clinical and Experimental Research, 40, 1971–1981 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patton, G.C. , Sawyer, S.M. , Santelli, J.S. , Ross, D.A. , Afifi, R. , Allen, N.B. , et al. (2016) Our future: a Lancet commission on adolescent health and wellbeing. Lancet, 387, 2423–2478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popova, S. , Lange, S. , Burd, L. , Shield, K. & Rehm, J. (2014) Cost of speech–language interventions for children and youth with foetal alcohol spectrum disorder in Canada. International Journal of Speech–Language Pathology, 16, 571–581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popova, S. , Lange, S. , Probst, C. , Gmel, G. & Rehm, J. (2017) Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta‐analysis. Lancet Global Health, 5, e290–e299. [DOI] [PubMed] [Google Scholar]
- Popova, S. , Lange, S. , Shield, K. , Burd, L. & Rehm, J. (2019) Prevalence of fetal alcohol spectrum disorder among special subpopulations: a systematic review and meta‐analysis. Addiction, 114, 1150–1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popova, S. , Lange, S. , Shield, K. , Mihic, A. , Chudley, A.E. , Mukherjee, R.A.S. , et al. (2016) Comorbidity of fetal alcohol spectrum disorder: A systematic review and meta‐analysis. Lancet, 387, 978–87. [DOI] [PubMed] [Google Scholar]
- Price, A. , Cook, P.A. , Norgate, S. & Mukherjee, R. (2017) Prenatal alcohol exposure and traumatic childhood experiences: A systematic review. Neuroscience & Biobehavioral Reviews, 80, 89–98. [DOI] [PubMed] [Google Scholar]
- Proven, S. , Ens, C. & Beaudin, P.G. (2014) The language profile of school‐aged children with fetal alcohol spectrum disorder (FASD). Canadian Journal of Speech–Language Pathology & Audiology, 37, 268–279. [Google Scholar]
- Rasmussen, C. (2005) Executive functioning and working memory in fetal alcohol spectrum disorder. Alcoholism: Clinical and Experimental Research, 29, 1359–1367. [DOI] [PubMed] [Google Scholar]
- Rasmussen, C. & Bisanz, J. (2009) Executive functioning in children with fetal alcohol spectrum disorders: profiles and age‐related differences. Child Neuropsychology, 15, 201–215. [DOI] [PubMed] [Google Scholar]
- Rasmussen, C. , Pei, J. , Manji, S. , Loomes, C. & Andrew, G. (2009) Memory strategy development in children with foetal alcohol spectrum disorders. Developmental Neurorehabilitation, 12, 207–214. [DOI] [PubMed] [Google Scholar]
- Reid, N. , Kippin, N. , Passmore, H. & Finlay‐Jones, A. (2020) Fetal alcohol spectrum disorder: the importance of assessment, diagnosis and support in the Australian justice context. Psychiatry, Psychology and Law, 27, 265–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rost, G.C. & McGregor, K.K. (2012) Miranda rights comprehension in young adults with specific language impairment. American Journal of Speech–Language Pathology, 21, 101–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sayal, K. (2007) Alcohol consumption in pregnancy as a risk factor for later mental health problems. Evidence Based Mental Health, 10, 98. [DOI] [PubMed] [Google Scholar]
- Schonfeld, A.M. , Mattson, S.N. & Riley, E.P. (2005) Moral maturity and delinquency after prenatal alcohol exposure. Journal of Studies on Alcohol, 66, 545–554. [DOI] [PubMed] [Google Scholar]
- SCOTTISH INTERCOLLEGIATE GUIDELINES NETWORK (2019) Children and young people exposed prenatally to alcohol: A national clinical guideline. Edinburgh, UK: SIGN. [Google Scholar]
- Skorka, K. , McBryde, C. , Copley, J. , Meredith, P.J. & Reid, N. (2020) Experiences of children with fetal alcohol spectrum disorder and their families: A critical review. Alcoholism: Clinical and Experimental Research, 44, 1175–1188. [DOI] [PubMed] [Google Scholar]
- Sowell, E.R. , Lu, L.H. , O'Hare, E.D. , McCourt, S.T. , Mattson, S.N. , O'Connor, M.J. et al. (2007) Functional magnetic resonance imaging of verbal learning in children with heavy prenatal alcohol exposure. Brain Imaging, 18, 635–639. [DOI] [PubMed] [Google Scholar]
- Spencer, S. (2018) Multidisciplinary perspectives on adolescence. In: Spencer, S. (Ed.) Supporting adolescents with language disorders. UK: J & R Press. [Google Scholar]
- Stackhouse, J. & Wells, B. (1997) Children's speech and literacy difficulties: A psycholinguistic framework. London, UK, Whurr Publishers. [Google Scholar]
- Stevens, S.A. , Dudek, J. , Nash, K. , Koren, G. & Rovet, J. (2015) Social perspective taking and empathy in children with Fetal Alcohol Spectrum Disorders. Journal of the International Neuropsychological Society, 21, 74–84. [DOI] [PubMed] [Google Scholar]
- Vaurio, L. , Riley, E.P. & Mattson, S.N. (2011) Neuropsychological comparison of children with heavy prenatal alcohol exposure and an IQ‐matched comparison group. Journal of the International Neuropsychological Society, 17, 463–473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- VERITAS HEALTH INNOVATION Covidence systematic review software. Melbourne, Australia. [Google Scholar]
- Viner, R.M. , Ozer, E.M. , Denny, S. , Marmot, M. , Resnick, M. , Fatusi, A. , et al. (2012) Adolescent Health 2: Adolescence and the social determinants of health. Lancet, 379, 1641–1652. [DOI] [PubMed] [Google Scholar]
- Wagner, R.K. & Torgesen, J.K. (1987) The nature of phonological processing and its causal role in the acquisition of reading skills. Psychological Bulletin, 101, 192–212. [Google Scholar]
- Wechsler, D. (1991) Wechsler Intelligence Scale for Children, third edition (WISC‐III). United States of America, Psychological Corporation. [Google Scholar]
- Wechsler, D. (1992) Wechsler Individual Achievement Test, first edition. New York: Psychological Corporation. [Google Scholar]
- Westby, C. & Washington, K.N. (2017) Using the international classification of functioning, disability and health in assessment and intervention of school‐aged children with language impairments. Language, Speech, & Hearing Services in Schools, 48, 137–152. [DOI] [PubMed] [Google Scholar]
- Wilkinson, G.S. & Robertson, G.J. (2006) Wide range achievement test, fourth edition. Lutz, FL: Psychological Assessment Resources. [Google Scholar]
- Willford, J.A. , Richardson, G.A. , Leech, S.L. & Day, N.L. (2004) Verbal and visuospatial learning and memory function in children with moderate prenatal alcohol exposure. Alcoholism: Clinical and Experimental Research, 28, 497–507. [DOI] [PubMed] [Google Scholar]
- Willoughby, K.A. , Sheard, E.D. , Nash, K. & Rovet, J. (2008) Effects of prenatal alcohol exposure on hippocampal volume, verbal learning, and verbal and spatial recall in late childhood. Journal of the International Neuropsychological Society, 14, 1022–1033. [DOI] [PubMed] [Google Scholar]
- Wyper, K.R. & Rasmussen, C.R. (2011) Language impairments in children with fetal alcohol spectrum disorder. Canadian Society of Clinical Pharmacology and Therapeutics, 18, e364–e376. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. PsycInfo search strategy (19 March 2019).
Table S2. Study and participant characteristics for included studies that reported on the same participant groups in table 1.
Table S3. Quality assessment of seven included studies.