

Abstract
Background
The portfolio of hyaluronic acid (HA) fillers and the techniques of administration have evolved in recent years. The latest innovation in the Vycross® range was the introduction of VYC‐25L (Juvéderm Volux®; Allergan plc), a first‐in‐class filler effective for chin and facial lower third remodeling. The aim here was to provide clinicians who are starting to use VYC‐25L with key advice, and to standardize procedures so that optimal and predictable outcomes can be obtained.
Methods
A multidisciplinary group of experts in esthetic medicine from Spain and Portugal reviewed the properties, treatment paradigms, administration techniques, and potential complications of VYC‐25L, on the basis of which they drafted consensus recommendations for its clinical use.
Results
The consensus panel provided specific recommendations focusing on the patient profile, dose, administration techniques, and the complications of VYC‐25L and their management. The panel identified five different profiles of patients who may benefit from VYC‐25L, and they drafted recommendations aimed to facilitate the treatment of these patients, namely, microgenia (women/men), masculinization (men), rejuvenation (women/men), facial laxity (women/men), and submental convexity (women/men). In terms of their safety, no specific recommendations were made beyond those established for other HA fillers.
Conclusions
The evolution of esthetic medicine makes it necessary to update the clinical recommendations that guide patient assessment and treatment with the new HA fillers developed. The current consensus document addresses relevant issues related to the use of VYC‐25L on different types of patient, in an attempt to standardize procedures and help specialists obtain predictable results.
Keywords: facial rejuvenation, hyaluronic acid, myomodulation, Vyc‐25L, Vycross
1. INTRODUCTION
Esthetic medicine is continuously evolving, providing specialists with constant challenges. The development of new classes of products, new indications and procedures, and the evolution of treatment paradigms, in conjunction with a better understanding of facial anatomy and its aging, make it necessary to adopt more comprehensive approaches to facial rejuvenation, and to update guidelines.
Over the past few years, the number of minimally invasive esthetic procedures has increased dramatically. 1 Based on a survey conducted by the International Society of Aesthetic Plastic Surgery, more than 13.6 million non‐surgical procedures were performed worldwide in 2019. 1 Moreover, more than 4.3 million of minimally invasive hyaluronic acid (HA) esthetic procedures were performed that year, representing an increase of 15.7% from 2018. 1
Hyaluronic acid fillers are mainly used to fill rhytides and folds, or to restore/correct soft tissue loss caused by either disease or aging. 2 , 3 , 4 HA is a high molecular weight, natural, and linear glycosaminoglycan that is present in all mammals. 5 , 6 Due to its physicochemical properties, HA is one of the most hygroscopic molecules in nature and hydrated HA can contain up to 1000‐fold more water than its own weight. 7 Some specific features of HA influence its properties as a filler, such as polymer chain length, HA concentration, degree of cross‐linking, or the cross‐linking technology used, which affect its duration, extrusion force, and elastic Modulus (G'). These phenomena define the distinct products and the indications for which they may be employed. 6 , 8 , 9 , 10 , 11 , 12
One of the most recent generation of fillers was created using the patented Vycross® technology (Allergan, Inc.), which utilizes a proprietary mixture of high and lower molecular weight HA. 13 VYC‐25L (Juvéderm Volux®; Allergan plc) represents the latest innovation in the Vycross® range, combining high G' (resistance to deformation) and high cohesivity HA, 14 properties that make it an ideal filler to create and restore facial volume. In clinical practice, VYC‐25L has been successfully used to restore and create facial volume in patients with chin retrusion 15 , 16 and for other esthetic indications. 17 Moreover, when used for chin augmentation in patients with chin retrusion, its effects persist for at least 18 months. 16
It is not only effectiveness but also the safety of new HA products that must be considered. Thus, it is particularly important to study the bio‐integration and tolerability of HA fillers after their injection. 18 Tissue bio‐integration of VYC‐25L was assessed recently in a prospective, non‐comparative, open‐label, and multicenter study carried out on subjects who underwent facial rejuvenation treatment of the lower third of the face. 19 According to this study, partial bio‐integration of VYC‐25L was evident 48 h after treatment and the HA had fully integrated into the tissue 30 days after injection.
Although we have data from clinical studies about the good efficacy and safety profile of VYC‐25L, there is only limited knowledge about its use in daily practice. This manuscript aims to provide guidelines for the best way to use VYC‐25L in clinical practice, focusing mainly on three issues: (1) the best patient profile; (2) patient‐tailored treatment approaches to improve esthetic outcomes; and (3) the prevention of adverse events and potential complications. Thus, in this article we shall establish consensus‐based recommendations to provide doctors with a reference framework extracted from the available data and the panel's clinical experience.
2. METHODS
A multidisciplinary group of experts in esthetic medicine from Spain and Portugal convened to discuss the use of VYC‐25L in clinical practice. Meetings took place using a virtual platform from April 3 to May 26, 2020.
Different topics emerged as core concerns, including patient profiles, injection techniques, indications, and potential complications (Table 1). As a result, the authors drafted this consensus document based on their experience and opinions, and on a literature search of PubMed conducted in using the search terms “Hyaluronic acid” OR “Dermal Fillers” OR “Aesthetics” OR “Tissue bio‐integration” OR “complications.” Articles on human subjects in English, French, Portuguese, or Spanish were selected. Moreover, the references cited in the selected articles were also reviewed to identify additional relevant reports. In addition, relevant national and international guidelines were also reviewed.
TABLE 1.
The session's objectives and the issues considered as key points for the Consensus document about the use of VYC‐25L (Juvéderm Volux®; Allergan plc) in clinical practice
| Session objectives and key points |
|---|
|
Patient profile:
|
|
Tailored treatment approach
|
|
Safety
|
Consensus was achieved by discussing the expert panel's opinions, and considering their clinical experiences and the currently available scientific evidence. An initial document was drafted as a result of these meetings, and it was reviewed by the members of the expert panel. Feedback from the panel was taken into consideration until the greatest level of consensus was achieved and the final text was validated. During the structured consensus‐based decision‐making process, panel members voted on the draft statements and recommendations. The extent of agreement was determined at the end of the session held on May 26, 2020 (Table 2).
TABLE 2.
Classification of the agreement in the consensus decision‐making process
| Level of consensus | Extent of agreement as a percentage |
|---|---|
| Strong consensus | >95% of the participants agree |
| Consensus | >75%‐≤95% of the participants agree |
| Majority agreement | >50%‐≤75% of the participants agree |
| No consensus | ≤50% of the participants agree |
Adapted from the German Association of the Scientific Medical Societies (AWMF)—Standing Guidelines Commission. 33
3. RESULTS
3.1. Patient profile
Choosing the appropriate patients for treatment with VYC‐25L is essential to obtain optimal esthetic results. Prior to any treatment, it is crucial to perform an exhaustive examination to determine why the patient wants to undergo esthetic treatment and to establish “realistic” treatment goals. 20
According to the expert opinion, the first step is to identify whether the patient is a suitable candidate for a lower third intervention.
Recommendation 1 (Strong consensus): It is essential to establish whether the facial proportions and facial angles make the patient a good candidate for treatment. Evaluating the different measurements and characteristics of the jaw is crucial to determine the best patient profile to be treated.
An individual's facial beauty is determined by the harmony of its proportions and symmetry. 21 Symmetry and balance are two relevant aspects that should be taken into consideration during the patient's facial assessment and diagnosis. 22 Among the different facial angles, the glabella‐subnasale‐pogonion angle may be considered as the most important one. The mean value of the glabella‐subnasale‐pogonion angle ranges from 165º to 175º. 23
In addition, the "WAY" paradigm may be a valuable tool to diagnose and treat aging in the mid‐ and lower third of the face. 24 This paradigm takes into consideration different aspects of facial aging, including the appearance of the jaw contour (“W”); the prejowl (“A”); and the tear trough, palpebromalar area, and nasojugal groove (“Y”) regions.
Table 3 summarizes the most important measurements to take into account.
Recommendation 2 (Strong consensus): The most suitable patients for an intervention with VYC‐25L in the lower third are patients with microgenia (women and men), and those undergoing masculinization (men) or rejuvenation of the lower third, mainly the jawline (women and men).
TABLE 3.
Different measurements and characteristics of the jaw to be taken into account
| Examination | Description |
|---|---|
| Dental occlusion | Pay special attention to class II malocclusion as this may be due to any combination of the jaw, tooth, and lip position. In these patients, the upper jaw (maxilla) can be too far forward or more usually, the lower jaw (mandible) is too far back. 34 |
| Evaluation of facial angles | Glabella‐subnasale‐pogonion angle: Describe the angle of facial convexity, which is formed by connecting the soft tissue glabella, subnasale and soft tissue pogonion. 35 , 36 This value ranges from 165º to 175º. 34 , 35 |
| Evaluation of the effective jaw length | Evaluate the distance between the condilion and gnation, or between the condilion and pogonion (both are acceptable). The mean (±standard deviation) of the effective jaw length from the condilion to gnation is 120.2 (±5.3) mm in women and 132.3 (±6.8) mm in men. 37 |
| Evaluation of the chin | Analyze the previously described facial angles. |
| Evaluation of muscle activity | It is very important to assess the depressor anguli oris, mentalis and masseter muscle activity, in addition to that of the superficial musculoaponeurotic system. |
| Evaluation of skin laxity and submental fat |
Evaluating these aspects may be important when addressing combined treatments (neck + submental fat). It is important to maintain good skin integrity and structure. The "WAY" paradigm* may be a useful method to diagnose skin laxity and facial aging. 24 |
*WAY refers to the appearance of: the jaw contour (“W”); the prejowl (“A”); and the tear trough, palpebromalar area and nasojugal groove (“Y”).
In addition to those profiles mentioned above, other patients that may obtain significant benefit from such a procedure are as follows:
Patients with facial laxity (Majority agreement):
Patients with thick subcutaneous cellular tissue in the upper and middle third of the face (myomodulation of the levator muscles due to their tightening effect).
Patients with a "heavy face" who have sagging tissues (skin/subcutaneous cellular tissue) in the upper and middle third of the face.
Patients with a double chin (Majority agreement).
Recommendation 3 (Strong consensus): Due to the product's characteristics 1 , VYC‐25L is especially well suited for creating and restoring facial volume in areas where strong muscles are present, such as the chin and jaw, and to add bone support.
3.2. Treatment
The introduction of new products onto the market often requires new treatment paradigms to be devised. These new paradigms aim to establish comprehensive approaches focused more on achieving patient beautification than on treating individual facial deficiencies. Due to the increasing popularity of minimally invasive esthetic procedures, it is necessary to create a "common language" that can be used not only to describe treatment approaches but also to communicate among specialists around the world. The medical codes developed by de Maio (MD Codes®: 31) are specific injection guidelines that enable optimal esthetic outcomes to be achieved. The MD Codes® represent precise anatomical sites and procedures for the injection of HA fillers, referring to the Cheek (Ck); Temple (T); Chin (C); Jowls (Jw); Forehead (F); Lateral orbital (O); Eyebrow (E); Tear trough (Tt); Glabella (G); Nasolabial fold (NL); Marionette line (M); Lip (Lp); and Nose (N). 26
Recommendation 4 (Strong consensus): High‐quality, standardized photographs should be used. The panel recommends taking photographs at angles of 0 º, 45 º, and 90º (right and left). If possible, it would be preferable to obtain three‐dimensional (3D) images.
Recommendation 5 (Strong consensus): The recommendation is to use a customized 7‐point protocol with women, which includes the following treatment areas: zygomatic arch; lateral lower cheek/parotid area; labiomental angle; chin apex; mandible angle; lower prejowl; and lower anterior chin (see Figure 1).
Recommendation 6 (Strong consensus): The recommendation is to use a customized 9‐point protocol with men, which includes the following treatment areas: zygomatic arch; lateral lower cheek/parotid area; labiomental angle; chin apex; lateral lower chin; mandible angle; pre‐auricular area; lower prejowl; and lower anterior chin (see Figure 2).
Recommendation 7: Despite its main indication for lower third facial treatments, due to its characteristics VYC‐25L may also be effectively used for facial contouring at other locations:
FIGURE 1.

Customized 7‐point preferred protocol pattern recommended for women (adapted from de Maio: 26 ): Ck1, Zygomatic arch; Ck4, Lateral lower cheek/parotid area; Jw1, Mandible angle; Jw4, Lower prejowl; Jw5, Lower anterior Chin; C1, Labiomental angle; C2, Chin apex. This photograph has been reprinted with permission from Allergan plc, Dublin, Ireland
FIGURE 2.
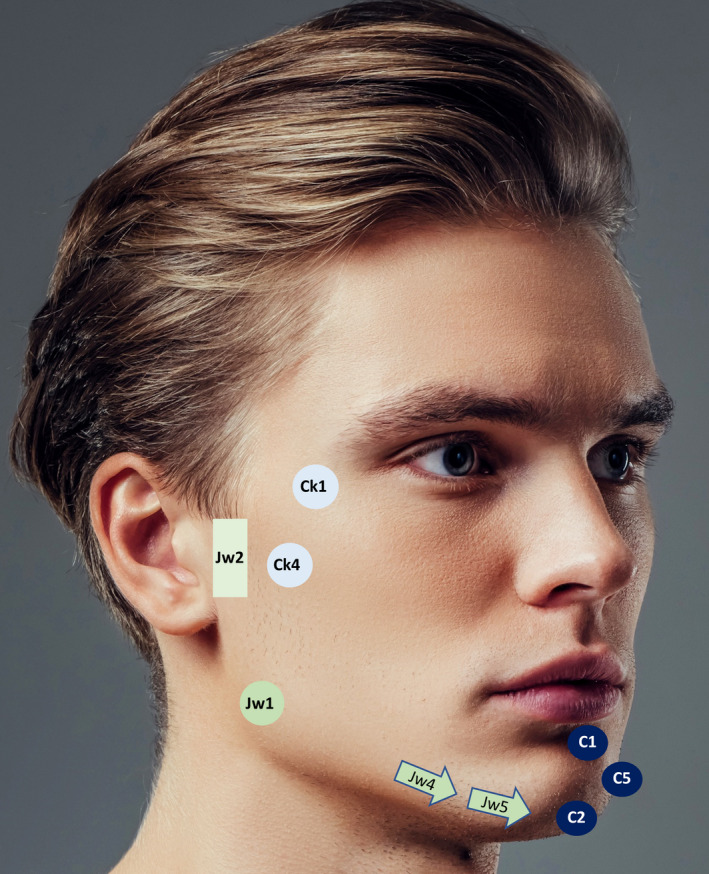
Customized 9‐point preferred protocol pattern recommended for men (adapted from de Maio: 26 ). Ck1, Zygomatic arch; Ck4, Lateral lower cheek/parotid area; Jw1, Mandible angle; Jw2, Pre‐auricular area; Jw4, Lower prejowl; Jw5, Lower anterior Chin; C1, Labiomental angle; C2, Chin apex; C5, Lateral lower chin. This photograph has been reprinted with permission from Allergan plc, Dublin, Ireland
-
i.
Temple – based on the MD Codes®. 26
-
•
Anterior temple: Strong consensus.
-
•
Posterior temple: No consensus.
-
•
-
ii.
Cheek – based on the MD Codes®. 26
-
•
Zygomatic arch: Strong consensus.
-
•
Zygomatic eminence: No consensus.
-
•
AnteVromedial cheek: Majority agreement.
-
•
The panel addressed the esthetic management of 7 different situations, namely, beautification (women); masculinization (men); microgenia (women and men); rejuvenation (women and men); and submental convexity (women and men).
-
1
Women
Different treatment approaches were assessed in women, including beautification; microgenia; rejuvenation; and submental fat convexity (Table 4).
-
2
Men
TABLE 4.
Overview of the main panel recommendations and considerations about the treatment strategies for women. Each point identified in this table corresponds to those defined in the MD codes® 26
| Indication | Recommendation |
|---|---|
| Beautification |
|
| Microgeniaa |
|
| Rejuvenation |
|
| Submental fat |
|
Abbreviations: C1, Labiomental angle; C2, Chin apex; C4, Anterior chin/soft tissue pogonion; C5, Lateral lower chin; Ck1, Zygomatic arch; Ck2, Zygomatic eminence; Ck3, Anteromedial cheek; Ck4, Lateral lower cheek/parotid area; Jw1, Mandible angle; Jw3, Mandible body; Jw4, Lower prejowl; Jw5, Lower anterior chin; T1, Anterior temple; HA, Hyaluronic acid; SMAS, Superficial musculoaponeurotic system.
aMicrogenia is usually associated with maxillary and mandibular atrophy in both men and women.
The treatment indications for men included masculinization; microgenia; rejuvenation; and submental fat convexity (Table 5).
-
3
Other considerations
TABLE 5.
Overview of the panel's main recommendations and considerations regarding the treatment strategies for men. Each point identified in this table correspond to those defined in the MD codes® 26
| Indication | Recommendation |
|---|---|
| Masculinization |
|
| Microgeniaa |
|
| Rejuvenation |
|
| Submental fat |
|
Abbreviations: C1, Labiomental angle; C2, Chin apex; C3, Anterior chin; C4, Anterior chin/soft tissue pogonion; C5, Lateral lower chin; Ck1, Zygomatic arch; Ck2, Zygomatic eminence; Ck4, Lateral lower cheek/parotid area; Jw1, Mandible angle; Jw3, Mandible body; Jw4, Lower prejowl; Jw5, Lower anterior chin; T1, Anterior temple; HA, Hyaluronic acid; SMAS, Superficial musculoaponeurotic system.
aMicrogenia is usually associated to maxillary and mandibular atrophy in both women and men.
*There was no consensus on this issue. The panel's opinions ranged from those who do not treat these points to those who treat them with other HA fillers like VYC‐17.5L, as well as those who treat them with VYC‐25L.
Besides the specific treatment strategies recommended for men and women, other issues that should be taken into consideration include dose/plane; learning curve; and warnings (Table 6). These were discussed along with additional aspects of the treatments, and the consensus reached regarding the MD Codes®, the areas to be injected, the dose, the depth, and the administration technique are summarized in Table 7. In terms of the amount of filler to be used, the volume administered should be customized depending on the patient's sex, age, and facial structure. It is advisable to start with volumes of 0.3–0.5 cc for each MD Code® treated and the panel recommended that a volume of 0.5 ml per/MD Code® should not be exceeded. In addition, it was considered that treatment can be performed in either one or two sessions, depending on the patient's specific characteristics.
TABLE 6.
Overview of the panel recommendations about safety. Each point identified in this table corresponds to those defined in the MD codes® 26
| Indication | Recommendation/Considerations |
|---|---|
| Dose/Plane |
|
| Learning curve |
|
| Warnings |
|
Abbreviations: C, Chin; C2, Chin apex; C4, Anterior chin/soft tissue pogonion; C5, Lateral lower chin; C6, Lateral chin; Jw1, Mandible angle; Jw, Jaw; Jw4, Lower prejowl; Jw5, Lower anterior chin; SMAS, Superficial musculoaponeurotic system.
aMicrogenia is usually associated to maxillary and mandibular atrophy in both women and men.
TABLE 7.
Overview of the MD Codes, injection areas, depth, injection device, and dose of VYC‐25 L to be used (adapted from de Maio 26 )
| MD Codes™ | Injection area | Target layer | Tool | Delivery | Volume per site (ml)a |
|---|---|---|---|---|---|
| Ck1 | Zygomatic arch | Supraperiostialb | Needle | Bolus | 0.1+0.1+0.1 |
| Ck4 | Lateral lower cheek/parotid area | Subcutaneous | Cannula | Fanning | 0.5 |
| Jw1 | Mandible angle | Supraperiostealb | Needlec | Bolus | 0.5 |
| Mandible angle | Subcutaneous | Cannula | Bolus | 0.5 | |
| Jw2* | Pre‐auricular area | Subcutaneous | Cannula | Bolus | 0.5 |
| Jw4 | Lower prejowl | Subcutaneous | Cannula | Bolus | 0.5 |
| Jw5 | Lower anterior chin | Subcutaneous | Cannula | Bolus | 0.5 |
| C1 | Labiomental angle | Subcutaneous | Cannula | Bolus | 0.5 |
| C2 | Chin apex | Subcutaneous | Cannula | Bolus | 0.3 to 0.5 |
| Chin apex | Supraperiostealb | Needlec | Bolus | 0.3 to 0.5 | |
| C5* | Lateral lower chin | Supraperiostealb | Needlec | Bolus | 0.3 to 0.5 |
aRecommended volumes were determined based on the panel's clinical experience.
bDo not inject into the cartilage or bone but rather at the level of the cartilage or bone.
cAspiration is highly recommended when injecting with a needle at the level of the bone.
*Only in men.
3.3. Safety
According to panel's experience, no unexpected adverse events have been observed with VYC‐25L.
Recommendation 8 (strong consensus): To prevent serious adverse events and undesirable outcomes, in addition to the filler's characteristics, it is extremely important to have an exhaustive knowledge of facial anatomy and of the aging process. Moreover, a complete medical history should be obtained from the patient and the procedure and technique should be carefully documented (dose, plane, administration, and treatment patterns).
4. DISCUSSION
The new products developed for esthetic medicine are designed to address new indications or to improve the results of existing ones, often associated with new procedures and altered treatment paradigms. These advances represent a constant challenge for specialists who must keep up with the new alternatives and the novel approaches available. Moreover, as new products emerge on the market, the clinical experience in using them is initially limited, which makes it necessary to draw up new clinical guidelines that can help specialists who are new to these procedures and those who have less experience with the products to incorporate them into their clinical arsenal.
To date, there are few studies that have evaluated the efficacy and safety of VYC‐25L in patients who undergo minimally invasive esthetic procedures. 15 , 16 , 17 , 27 A prospective, single‐blind, randomized, multicenter, international, controlled study evaluated the efficacy and safety of VYC‐25L when used to restore and create facial volume in the chin and jaw areas of subjects with chin retrusion. 15 , 16 The data showed that VYC‐25L achieved optimal esthetic outcomes with a good safety profile, making it an alternative to surgical interventions to increase chin projection and jaw volume. Moreover, the use of VYC‐25L was associated with good patient and specialist satisfaction. 15 , 16
A retrospective, single‐center study was also carried out on adult patients who underwent treatment of the lower third of the face with VYC‐25L. 27 Again, this study showed a good safety profile and high patient satisfaction in terms of chin and jawline sculpting. 27 In another retrospective, single‐center study, this time on patients who underwent a minimally invasive rhinoplasty, VYC‐25L, demonstrated good efficacy and a good safety profile, in association with good patient satisfaction. 17 In addition to clinical outcomes, tissue integration is an important aspect of HA fillers. Heterogeneous patterns are evident upon ultrasound examination, with no residual anechoic/hypoechoic areas, indicative of the full integration of VYC‐25L into the tissue 30 days after injection. 19
Irrespective of the technique used, facial analysis is the cornerstone to achieve optimal outcomes, which critically depends on understanding the underlying anatomy and the clinical implications of facial aging. 28 Moreover, when considering facial muscles, it is important not only to focus on the treatment results at rest but also in movement. The effectiveness of the HA fillers in modulating muscle activity has been described previously. 29 It was proposed that the HA fillers can mechanically alter muscle contraction by either facilitating or blocking their action. 29
Although HA filler injection is considered a safe procedure, the rising popularity of dermal fillers has led to an increase in the number of complications associated with their use. 30 , 31 Several early and late onset complications have been associated with the use of HA fillers, including local injection site reactions, infection, hypersensitivity, technical and placement errors, skin discoloration, and vascular conditions. 30 , 31 , 32
Finally, as a limitation of the current consensus, it should be noted that VYC‐25L is a relatively new product, and thus, clinical experience with it is limited to the short‐ to mid‐term. Nevertheless, there is evidence suggesting it has a good safety and efficacy profile 15 , 16 , 17 and that VYC‐25L has a very good bio‐integration profile as reflected by its partial tissue bio‐integration 48 h after treatment and total integration 30 days after filler injection. 19 However, all consensus documents, and perhaps this one in particular, must be considered within an evolving environment, and therefore, this document should be regularly revised to implement novel findings as they occur and future evidence as it becomes available.
5. CONCLUSIONS
To achieve optimal esthetic outcomes, clinicians must have an exhaustive knowledge of facial anatomy, filler characteristics, injection techniques, and, in particular, the patients best suited for an intervention. According to the panel's recommendations, VYC‐25L represents a valuable option to treat patients with microgenia (women and men), and for masculinization (men) and rejuvenation of the lower third of the face (women and men). Guidelines are laid out for how these patients should be treated and how they should be managed. Regarding safety, the incidence of complications is low, the majority of adverse events are mild, and no unexpected adverse events have been observed with VYC‐25L. This consensus highlights relevant points that may help professionals to undertake esthetic procedures with VYC‐25L safely and effectively. Moreover, it could serve as a basis to standardize procedures, which may help achieve optimal and predictable esthetic results.
CONFLICT OF INTERESTS
Dr Segurado, Dr Urdiales‐Gálvez, Dr Benítez, Dr Carrasco, Dr Escoda, Dr Farollch, and Dr Uva all received research grants to cover the costs of medical writing services and publication fees, honoraria for lectures, and travel support to attend educational meetings from Allergan, an AbbVie company. Dr Díaz, Dr Figueiredo, Dr Ortíz, and Dr Sebastian received honoraria for lectures and travel support to attend educational meetings from Allergan, an AbbVie company.
ETHICAL APPROVAL
Authors declare human ethics approval was not needed for this study.
AUTHOR CONTRIBUTIONS
M.A.S. and F.U.G. designed and directed the project, the main conceptual ideas, and proof outline. P.A.B, S.C., and I.D. drafted the manuscript, literature search, and designed the tables and figures. N.E., L.F.P., and V.F. performed literature search, funding acquisition, and project administration; F.O., M.C.S., and L.U. involved in critical review and edition of the manuscript. All authors reviewed the results and approved the final version of the manuscript.
ACKNOWLEDGMENTS
Medical writing services were provided by Ciencia y Deporte S.L. and Editorial Assistance by BiomedRed S.L. Support for this assistance was funded by Allergan Aesthetic, an AbbVie company.
Segurado MA, Urdiales‐Gálvez F, Benítez PA, et al. An expert consensus report on the clinical use of the Vycross® hyaluronic acid VYC‐25 L filler. J Cosmet Dermatol. 2021;20:3156–3165. 10.1111/jocd.14398
Segurado and Urdiales‐Gálvez contributed equally to this work and should be considered equivalent first authors.
ENDNOTE
VYC‐25L combines the highest elastic Modulus (G’) HA, which reflects the elasticity of the material when deformed, and it has the highest cohesivity currently available on the market 30 .
DATA AVAILABILITY STATEMENT
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
REFERENCES
- 1. https://www.isaps.org/wp‐content/uploads/2020/12/Global‐Survey‐2019.pdf ‐ Accessed May 12, 2021.
- 2. Brandt FS, Cazzaniga A. Hyaluronic acid gel fillers in the management of facial aging. Clin Interv Aging. 2008;3(1):153‐159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Carruthers J, Cohen SR, Joseph JH, Narins RS, Rubin M. The science and art of dermal fillers for soft‐tissue augmentation. J Drugs Dermatol. 2009;8(4):335‐350. [PubMed] [Google Scholar]
- 4. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;12(6):295‐316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tezel A, Fredrickson GH. The science of hyaluronic acid dermal fillers. J Cosmet Laser Ther. 2008;10(1):35‐42. Erratum in: J Cosmet Laser Ther. 2014; 16(1):45. [DOI] [PubMed] [Google Scholar]
- 6. Gutowski KA. Hyaluronic acid fillers: science and clinical uses. Clin Plast Surg. 2016;43(3):489‐496. [DOI] [PubMed] [Google Scholar]
- 7. Laurent TC, Fraser JRE. Hyaluronan. FASEB J. 1992;6:2397‐2404. [PubMed] [Google Scholar]
- 8. Stocks D, Sundaram H, Michaels J, Durrani MJ, Wortzman MS, Nelson DB. Rheological evaluation of the physical properties of hyaluronic acid dermal fillers. J Drugs Dermatol. 2011;10(9):974‐980. [PubMed] [Google Scholar]
- 9. Segura S, Anthonioz L, Fuchez F, Herbage B. A complete range of hyaluronic acid filler with distinctive physical properties specifically designed for optimal tissue adaptations. J Drugs Dermatol. 2012;11(1 Suppl):s5‐8. [PubMed] [Google Scholar]
- 10. Mansouri Y, Goldenberg G. Update on hyaluronic acid fillers for facial rejuvenation. Cutis. 2015;96(2):85‐88. [PubMed] [Google Scholar]
- 11. Greene JJ, Sidle DM. The hyaluronic acid fillers: current understanding of the tissue device interface. Facial Plast Surg Clin North Am. 2015;23(4):423‐432. [DOI] [PubMed] [Google Scholar]
- 12. Micheels P, Sarazin D, Tran C, Salomon D. Effect of different crosslinking technologies on hyaluronic acid behavior: a visual and microscopic study of seven hyaluronic acid gels. J Drugs Dermatol. 2016;15(5):600‐606. [PubMed] [Google Scholar]
- 13. Philipp‐Dormston WG, Hilton S, Nathan M. A prospective, open‐label, multicenter, observational, postmarket study of the use of a 15 mg/mL hyaluronic acid dermal filler in the lips. J Cosmet Dermatol. 2014;13(2):125‐134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Pierre S, Liew S, Bernardin A. Basics of dermal filler rheology. Dermatol Surg. 2015;41(Suppl 1):S120‐S126. [DOI] [PubMed] [Google Scholar]
- 15. Ogilvie P, Sattler G, Gaymans F, et al. Safe, effective chin and jaw restoration with VYC‐25L hyaluronic acid injectable gel. Dermatol Surg. 2019;45(10):1294‐1303. [DOI] [PubMed] [Google Scholar]
- 16. Ogilvie P, Benouaiche L, Philipp‐Dormston WG, et al. VYC‐25L Hyaluronic acid injectable gel is safe and effective for long‐term restoration and creation of volume of the lower face. Aesthet Surg J. 2020;40(9):NP499‐NP510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Bertossi D, Malchiodi L, Albanese M, Nocini R, Nocini P. Nonsurgical rhinoplasty with the novel hyaluronic acid filler VYC‐25L: results using a nasal grid approach. Aesthet Surg J. 2021;41(6):NP512‐NP520. 10.1093/asj/sjaa196 [DOI] [PubMed] [Google Scholar]
- 18. Tran C, Carraux P, Micheels P, Kaya G, Salomon D. In vivo biointegration of three hyaluronic acid fillers in human skin: a histological study. Dermatology. 2014;228(1):47‐54. [DOI] [PubMed] [Google Scholar]
- 19. Urdiales‐Gálvez F, Barres‐Caballer J, Carrasco‐Sánchez S. Ultrasound assessment of tissue integration of the crosslinked hyaluronic acid filler VYC‐25L in facial lower‐third aesthetic treatment: a prospective multicenter study. J Cosmet Dermatol. 2021;20(5):1439‐1449. 10.1111/jocd.13632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Urdiales‐Gálvez F, Delgado NE, Figueiredo V, et al. Preventing the complications associated with the use of dermal fillers in facial aesthetic procedures: an expert group consensus report. Aesthetic Plast Surg. 2017;41(3):667‐677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Milutinovic J, Zelic NN. Evaluation of facial beauty using anthropometric proportions. ScientificWorldJournal. 2014;2014:428250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Farolch‐Prats L, Nome‐Chamorro C. Facial contouring by using dermal fillers and botulinum toxin a: a practical approach. Aesthetic Plast Surg. 2019;43(3):793‐802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Park C, Lee M, Jung Y. Photogrammetric facial analysis of attractive celebrities using the glabella for planning rhinoplasty and analyzing surgical outcomes. Arch Aesthetic Plast Surg. 2018;24:105‐110. Available in: https://e‐aaps.org/journal/view.php?doi= 10.14730/aaps.2018.24.3.105 Accessed May 12, 2021. [DOI] [Google Scholar]
- 24. Farollch Prats L, Mirada Donisa E, Villanueva C. "WAY": A practical means to identify and treat the aging process. J Cosmet Dermatol. 2021;20(6):1837‐1845. 10.1111/jocd.13782 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Pierre S, Liew S, Bernardin A. Basics of dermal filler rheology. Dermatol Surg. 2015;41(Suppl 1):S120‐S126. [DOI] [PubMed] [Google Scholar]
- 26. de Maio M. MD Codes™: A methodological approach to facial aesthetic treatment with injectable hyaluronic acid fillers. Aesthetic Plast Surg. 2021;45(2):690‐709. 10.1007/s00266-020-01762-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Bertossi D, Robiony M, Lazzarotto A, Giampaoli G, Nocini R, Nocini PF. Nonsurgical redefinition of the chin and jawline of younger adults with a hyaluronic acid filler: results evaluated with a grid system approach. Aesthet Surg J. 2021;41(9):1068‐1076. 10.1093/asj/sjaa179 [DOI] [PubMed] [Google Scholar]
- 28. Little JW. Volumetric perceptions in midfacial aging with altered priorities for rejuvenation. Plast Reconstr Surg. 2000;105(1):252‐266. [DOI] [PubMed] [Google Scholar]
- 29. de Maio M. Myomodulation with injectable fillers: an innovative approach to addressing facial muscle movement. Aesthetic Plast Surg. 2018;42(3):798‐814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Urdiales‐Gálvez F, Delgado NE, Figueiredo V, et al. Treatment of soft tissue filler complications: expert consensus recommendations. Aesthetic Plast Surg. 2018;42(2):498‐510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Ortiz AE, Ahluwalia J, Song SS, Avram MM. Analysis of U.S. Food and Drug Administration data on soft‐tissue filler complications. Dermatol Surg. 2020;46(7):958‐961. [DOI] [PubMed] [Google Scholar]
- 32. Park TH, Seo SW, Kim JK, Chang CH. Clinical experience with hyaluronic acid‐filler complications. J Plast Reconstr Aesthet Surg. 2011;64(7):892‐896. [DOI] [PubMed] [Google Scholar]
- 33. German Association of the Scientific Medical Societies (AWMF) . Standing Guidelines Commission. AWMF guidance manual and rules for guideline development. English version. Available in: http://www.awmf.org/leitlinien/awmf‐regelwerk.html ‐ Accessed January 20, 2021.
- 34. Batista KB, Thiruvenkatachari B, Harrison JE, O'Brien KD. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children and adolescents. Cochrane Database Syst Rev. 2018. 13:(3):CD003452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Legan HL, Burstone CJ. Soft tissue cephalometric analysis for orthognathic surgery. J. Oral Surg. 1980;38(10):744‐751. [PubMed] [Google Scholar]
- 36. Anić‐Milosević S, Lapter‐Varga M, Slaj M. Analysis of the soft tissue facial profile by means of angular measurements. Eur J Orthod. 2008;30(2):135‐140. [DOI] [PubMed] [Google Scholar]
- 37. McNamara JA Jr. A method of cephalometric evaluation. Am J Orthod. 1984;86(6):449‐469. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.