

Abstract
Background
Every year, more than 800,000 people die by suicide, three‐quarters of which are males. Economic factors influence suicide rates, but a worldwide perspective of their impact according to age and sex is lacking.
Method
We queried publicly available datasets on economic factors and on suicide rates stratified according to sex and age, from 1991 to 2017, for 175 countries. Thus, we analyzed approximately 21 million deaths by suicide using a multivariable regression model approach.
Results
Every 1% increase in global unemployment rates is associated with a 1% upsurge in male deaths by suicide (Relative risk (RR) = 1.01 [CI 95% 1.00–1.01] with respect to females) or 5000 excess male deaths. A 1% higher unemployment rate also exerts age‐specific effects on suicide rates, since, among adults aged 30–59, the suicide rate is increased by 2–3%. Lastly, for every 1000 US dollar increase in the GDP per capita, suicide rates are reduced by 2% (RR = 0.98 [0.98–0.98]), corresponding to a reduction of 14,000–15,000 suicide deaths per year globally.
Conclusions
Males who have lost their jobs in adulthood are those at higher risk of suicide and to whom financial support measures should be delivered in a timely manner.
INTRODUCTION
Suicide is a complex phenomenon arising from the interaction between individual characteristics (Mościcki, 1997), social, cultural, and environmental conditions (Värnik, 2012; Ying & Chang, 2009), claiming one life every forty seconds (WHO | Suicide Data, n.d.) Although represented virtually on a global scale, suicide rates vary profoundly according to geographical region (Liu, 2009; Snowdon, 2018), ethnic group (Garlow et al., 2005; McKenzie et al., 2003), religion, and spirituality (Colucci & Martin, 2008), sex (Gvion & Apter, 2012), age (Agerbo, 2005; Dervic et al., 2008; A. Erlangsen, 2004; Fässberg et al., 2012), access to lethal methods (Florentine & Crane, 2010), and preventive strategies (Mann et al., 2005; Milner & De Leo, 2010). Moreover, macroeconomic factors (e.g., Gross Domestic Product—GDP—per capita and unemployment rate) have been proposed as suicide rate modulating factors (Berk et al., 2006; Blakely, 2003; Fountoulakis et al., 2013). For instance, some single‐country studies provide evidence of a link between suicide and unemployment (Chan et al., 2014; Fountoulakis, 2020), and that increases in GDP might be temporally associated with a reduction of suicide rates (Mattei & Pistoresi, 2019). However, there is considerable heterogeneity in population stratification (per sex (Demirci et al., 2020) or age range (Ásgeirsdóttir et al., 2020; Basta et al., 2018; Hempstead & Phillips, 2015; Khang et al., 2005; Pompili et al., 2014)) and in the time periods considered (Chang et al., 2009; Fountoulakis et al., 2014; Nordt et al., 2015; Soleymani & Yip, 2020) by each study, and this hinders the possibility of conducting robust meta‐analyses of these findings. Two important studies (Huikari et al., 2019; Nordt et al., 2015), limited to some countries, evidenced how unemployment rates may affect suicide rates, and this effect may be modulated by gender (Qin et al., 2000, 2003a), but a worldwide perspective on the association between suicide and unemployment is still lacking. The identification of fine‐grained demographic differences in suicide rates is a necessary step to develop targeted public health interventions (Horton, 2018). For example, shedding light on the effect of unemployment on suicide rates of specific age ranges could provide policy‐makers with essential indicators for the optimal allocation of anti‐suicidal resources. Given the importance of such data in the light of the economic crisis due to the COVID‐19 pandemic, we queried publicly available datasets regarding economic factors and suicide rates stratified according to sex and age, from 1991 to 2017, for 175 countries, and conducted global and per income class statistical analyses while accounting for possible underreporting of deaths, to provide an up‐to‐date and comprehensive picture.
METHODS
Dataset preparation
Data on rates of death by suicide per 100,000 persons, stratified according to (i) sex, (ii) seventeen five‐year age ranges (10–14, through 90–94), (iii) calendar year (from 1990 to 2017), and (iv) country, were retrieved from the Global Burden of Disease Study (Global Burden of Disease (GBD), 2014). Gross domestic product (GDP) per capita referred to the 2010 US dollar value, and unemployment rates per country and calendar year were downloaded from the World Bank website (World Bank Group—International Development, Poverty, & Sustainability, n.d.). Data retrieved from the Global Burden of Disease and the World Bank website were matched, and countries (n = 20) for which either data on suicide or unemployment rates were missing were excluded from further analyses. Unemployment rates were available from 1991: we thus excluded information on suicide rates in 1990. To account for increased suicide rates due to heat waves (Basagaña et al., 2011; Page et al., 2007; Thompson et al., 2018), we extracted the corresponding data from The International Disaster Database (EM‐DAT | The International Disasters Database, n.d.). Given the frequency of the phenomena, we focused our analysis only on heat waves involving more than one region/large city of any country or that claimed more than 100 lives (total number of heat waves considered, n = 63). To account for possible underreporting of deaths by suicide, we downloaded data on major episodes of political violence (ethnic/civil violence or ethnic/civil war) from the Center for Systemic Peace website (CSP, —Major Episodes of Political Violence, 1946–2013, n.d.) and in order to identify those countries where attempted suicide is considered a misdemeanor, we referred to (Mishara and Weisstub, 2016). In total, our analyses covered on average 5.14 billion [SD, 0.62] people per year (Figure S1a). These corresponded to 786.310 [SD, 26 thousand] suicides per year (35.3% [SD, 2.81] females—Figure S1b).
Statistical analysis
Our analysis comprised 175 states (Table S1), in the years from 1991 to 2017, grouped by income class according to the ranges proposed by the World Bank (which are based on GDP per capita referred to the 2010 US dollar value, World Bank Group—International Development, Poverty, & Sustainability, n.d.). For each year‐country match, suicide rates were aggregated according to sex and to seventeen five‐year age ranges (from 10 to 14, from 15 to 19, …, from 90 to 94). Multivariable regression models based on negative binomial distributions (distributions used to analyze count data with overdispersion) were applied (Zeileis et al., 2008) to identify the association between suicide and unemployment rates. We then compared several regression models and chose the one with the lowest Bayesian Information Criterion (BIC) (Raftery, 1995) as the regression model that best explained suicide rates. The most accurate model for the description of yearly global suicide rates, and suicide rates in relation to income class, is composed of the following variables: sex, age, the occurrence of violent events (e.g., civil wars), the yearly unemployment rate, and GDP per capita, the interaction between sex and age, unemployment and sex, and unemployment and age (for further details, see Methods S1).
GDP was divided by 1000 in order to avoid having regression coefficients on a very small order of magnitude, which can make the interpretation of the model β coefficient estimates more cumbersome (also less intuitive). The analyses were conducted using RStudio 3.5.3 (R Core Team (2019). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, n.d.) and the glmmTMB package (Brooks et al., 2017); figures were produced with the ggplot2 package (Wickham, 2009).
RESULTS
Global suicide rates and possible confounders
Among the available variables retrieved for this study, we identified sex, age, the interaction between sex and age, the presence of episodes of political violence (i.e., civil war or ethnic violence), the Gross Domestic Product per capita referred to the 2010 US Dollar value, the unemployment rate, and its interactions with sex and age to be significant in determining the global suicide rates.
Several confounding factors needed to be accounted for before assessing the role of unemployment rates on suicide rates: first of all, global suicide rates are heavily influenced by age and sex, as has been previously reported (Conwell et al., 2002; De Leo et al., 2009; Szanto et al., 2020): This analysis indicates that, globally, males die by suicide 1.63 times more than females (relative risk—henceforth RR—confidence interval 95%: [1.57–1.70]), but this risk is also influenced by age, as adult males die by suicide approximately twice as much as adult females (ages 25–29, RR = 2.19 [2.09–2.30]; ages 45–49, RR = 2.00 [CI 95% 1.91–2.10], Figure 1b, Table S2A). Despite this difference between the sexes, both females and males show an increase in completed suicides with increasing age (between ages 15–19 RR = 5.42‐fold [5.17–5.69]; between ages 45–49, RR = 6.63 [6.33–6.95]; between ages 80–84, RR = 18.13 [17.33–18.98]—reference age for relative risk estimation is 10–14—Table S2A, Figure 1b). It has been reported that daily suicide rates might increase during heat waves (Basagaña et al., 2011; Page et al., 2007; Thompson et al., 2018); however, we found that on a calendar year basis, rates are not much affected, and thus the possible confounding effect of heat waves on increasing yearly global suicide rates is not significant. Other macro‐level environmental factors with limited effect, if any, were not included in the model (e.g., draught, see (Qi et al., 2014)). Furthermore, we also focused our attention on two factors that might be associated with the underreporting of suicide deaths: we tested whether countries where attempting suicide is a misdemeanor (Mishara & Weisstub, 2016) report on average lower suicide rates. It turned out that considering this factor in the regression model does not improve the fit, and thus, at least globally, it does not significantly affect suicide rates. Instead, major episodes of political violence (CSP—Major Episodes of Political Violence, 1946–2013, n.d.) (e.g., civil wars and ethnic wars) are significantly associated with lower suicide rates (RR = 0.83 [0.81–0.86]), likely mirroring an underreporting of suicide deaths due to institutional instability. We did not include religious affiliation in our models for its loose association with religious commitment and unreliable estimation (e.g., see Rushing et al., 2013).
FIGURE 1.
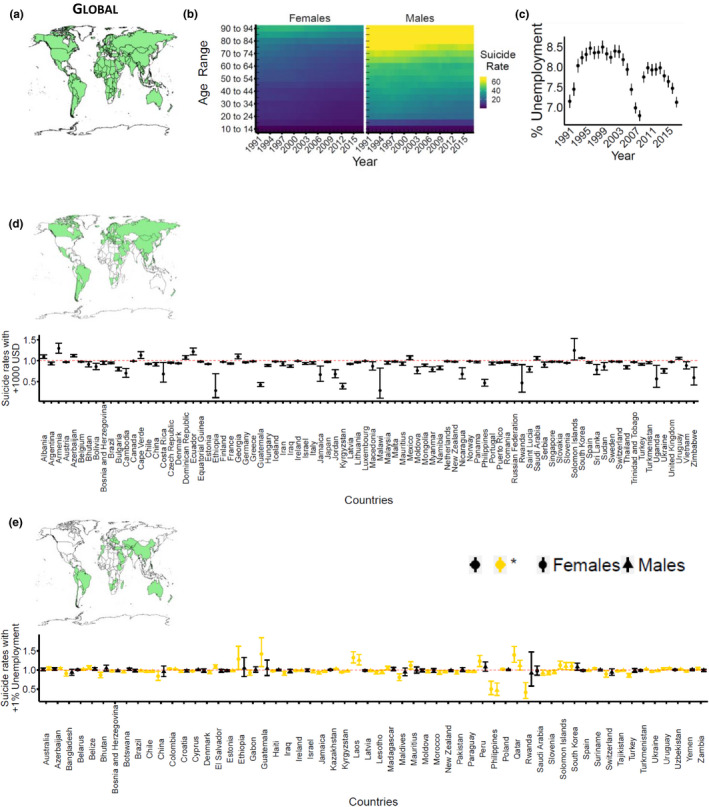
Suicide rates in the world, (a) countries considered in our global analysis of suicide rates (in green). (b) suicide rates per sex, year (x‐axis), and age range (y‐axis). The labels of the age ranges representing the second half of each decade (15 to 19, 25 to 29, etc.) are omitted for ease of reading. Each tile color refers to median suicide rates per year and age range across the countries considered. Higher rates correspond to the increasing yellow color of the tile. (c) unemployment rate per year (point range = mean and confidence interval). (d, e) represent the relative risk of death by suicide conveyed by macroeconomic factors. The horizontal red dashed line corresponds to RR = 1, which is the limit for which a variable is either protective (RR < 1) or harmful (RR > 1). For four countries (Burundi, Djibouti, Guinea, and Kuwait), the role of GDP/unemployment rate on suicide deaths could not be reliably estimated, and thus, we excluded these countries from this figure. (d) the relative risk of death by suicide with an increase of 1000 US dollars (USD) in gross domestic product per capita. For ease of reading, the countries for which the risk is reported (in green on the map) are only those for which an increment of 1000 USD in GDP significantly affects suicide rates. (e) the relative risk of death by suicide with a +1% unemployment rate for females and males. For ease of reading, the countries for which the risk is reported (in green on the map) are those where unemployment rates significantly alter suicide rates in females or males or both. For each country, both sexes are reported; the first errorbar (for each country) is referred to females. Sex/sexes for which unemployment rates significantly alter suicide rates are colored in yellow. When considering the role of unemployment rates in determining suicide rates, each interaction of unemployment rate (with age, with sex, or unemployment alone) needs to be considered together with the other interactions involving unemployment, since the relative risk conveyed by a variable is dependent on the relative risks given by all the other interactions of that variable. That is, although for some countries the increase in unemployment rate seems to be protective for males/females or both, this RR has to be weighed against the role of said increase for different age ranges to evince the overall influence of an increase in unemployment. For example, the model reports that a 1% increase in unemployment rates is associated with a 1% decrease in female suicide rates in Brazil. In that case, this reduction has to be weighed against the role of a 1% increase in unemployment rate for individuals belonging to a specific age range, say 45–49, which means that this increase is associated with a 4% increase in suicide rates (thus, evidencing that a 1% percent increase in the unemployment rate is linked to a 3% increase in suicide rates of females aged 45–49)
Global suicide rates and macroeconomic factors
After having considered the possible confounding effects of the previous factors, we assessed the influence of macroeconomic factors in determining a change in yearly suicide rates: we thus included the yearly Gross Domestic Product per capita (measured in terms of the 2010 US dollar value) in the predictive model to test whether this factor might influence suicide rates. In this way, we evidenced that GDP may play a significant role in reducing the rate of suicide: for every 1000 US dollar increase in the GDP per capita, suicide rates are reduced by 2% (RR = 0.98 [0.98–0.98], Table S2B). That is, if the world GDP per capita were to increase by 1000 USD, this rise would be associated with a reduction of 14,000–15,000 suicide deaths per year globally (i.e., 2% of the yearly number of deaths by suicide—approximately 800,000). We also applied the predictive model at the single country level. This analysis evidenced a statistically significant risk reduction associated with increasing GDP per capita for the majority of high‐income countries, with the notable exceptions of Australia and the United States, for which an increase in GDP per capita is not significantly linked to a change (neither a reduction nor an increase) in suicide rates (the countries for which an increase in GDP per capita is associated with a change in suicide rates are shown in Figure 1d). We then assessed the influence of unemployment on suicide rates. We found that unemployment affects male and female suicide rates differently, while also exerting age‐specific effects: a 1% higher unemployment rate increases the suicide rate in males by 1% (1.01 [CI 95% 1.00–1.01], Figure 1b,c, Table S2C) with respect to females; considering the effect of unemployment on males alone, this would correspond to more than 5,000 excess male deaths by suicide every year. Moreover, although all age ranges are significantly affected by higher unemployment rates, adults (males and females) between 30 and 59 years of age suffer an increase in suicide rate that is 2–3% higher than individuals aged 10–14 (ages 30–34, RR = 1.02 [1.02–1.03]; ages 45–49, RR = 1.03 [1.02–1.03]; ages 55–59, RR = 1.02 [1.02–1.03], Figure 1b,c, Table S2C). Thus, considering the age and sex‐specific effects of unemployment on suicide, globally, males aged 30–59 die by suicide more than females of the same age range, and more than male adolescents during times of rising unemployment rates. However, a global mean cannot be adopted as a rule of thumb, as there are several exceptions to this sex specificity in suicide: in Ethiopia, a 1% increase in unemployment rates significantly affects only female suicide rates; this is evident also for some middle‐income countries like Guatemala and Peru. There are also a few exceptions in the boreal hemisphere, like Qatar and South Korea (Figure 1e).
Suicide and macroeconomic factors per income class
Suicide rates vary tremendously based on the geo‐economic regions in which people are living. To assess differences in suicide rates and their relationship with unemployment rates according to general economic conditions, we assigned each country to an income class for each year (low, lower‐middle, upper‐middle, or high income), according to the ranges based on Gross Domestic Product per capita at the 2010 US dollar value proposed by the World Bank (World Bank Group ‐ International Development, Poverty, & Sustainability, n.d.). The low‐income class includes countries with GDP per capita less than 1006 USD; the lower‐middle class has GDP per capita equal to 1006 USD or more but less than 3976 USD; the upper‐middle class equal to 3976 USD but less than 12,276 USD; the high‐income class countries are characterized by a GDP per capita greater than 12,276 USD. We found that suicide rates of each income class fit well to the same regression model previously employed to described global suicide rates. Despite significant differences in suicide rates among countries grouped within the same income class (except for high‐income countries—intercept term in Table S2A), in all the income classes considered, males die by suicide more frequently than females (in low‐income countries, RR = 2.07 [1.89–2.27]; in lower‐middle‐income countries, RR = 1.62 [1.50–1.74]; in upper‐middle countries RR = 1.53 [1.41–1.67]; in high‐income countries RR = 1.52 [1.38–1.68], Figure 2b,e,h,k), with significant differences between the sexes that are influenced also by age. Throughout all the income classes, suicide rates rise significantly with age, although the increases differ between income classes (Figure 2b,e,h,k, Table S2A). Similar to what we evidenced at the global level, also at the income class level, yearly suicide rates are not significantly increased by heat waves or by the legal status of suicide. On the other hand, the presence of civil/ethnic wars/violence is associated with lower suicide rates in all income classes, except for high‐income countries (low‐income countries, RR = 0.86 [0.82–0.90]; lower‐middle income, RR = 0.93 [0.88–0.99]; upper‐middle income RR = 0.88 [0.85–0.92]; high income, RR = 1.06 [0.95–1.18], Table S2B). At the global level, GDP per capita exerts a slight, but significant, influence in reducing suicide rates. At the income class level, this effect is larger for low‐income countries, where for every 1000 USD increase in GDP per capita suicide rates are reduced by almost 30% (RR = 0.71 [0.67–0.75]), whereas, in lower‐middle and upper‐middle countries suicide rates are reduced by 5% (lower‐middle countries, RR = 0.95 [0.94–0.96]; upper‐middle countries, RR = 0.95 [0.94–0.95]) and in high‐income countries by 2%, (RR = 0.98, [0.98–0.98], Table S2B). Regarding the influence of unemployment rates on completed suicide rates, we evidence that unemployment significantly affects males more than females, especially in the high‐income class (RR = 1.04 [1.03–1.04], Figure 2b,c), but also in upper‐middle‐income countries (RR = 1.01 [1.00–1.02], Figure 2e,f). In low and lower‐middle‐income countries, unemployment rates do not affect male suicide rates more than in females; instead, as previously described, some countries (e.g., Ethiopia and Guatemala) report increased unemployment‐associated suicide rates in females (Figure 2h,i,k,l, Table S2B,C). Considering the influence of unemployment on suicide rates stratified according to age ranges, there is no significant effect of said influence in most of the age ranges in high‐income countries, except for people aged 40–44 (RR = 1.01, [1.00–1.03]), whereas 45–49 (RR = 1.02, [1.00–1.03]) and 90–94 (RR = 0.99, [0.97–1.00], Table S2C). On the other hand, in low, lower‐middle, and upper‐middle‐income countries, a rise in unemployment rates significantly increases suicide rates in virtually all age ranges, with a larger effect on middle‐aged people (e.g., age 45–49, low‐income countries RR = 1.03 [1.02–1.04]; lower‐middle RR = 1.04 [1.03–1.04]; upper‐middle RR = 1.04 [1.03–1.05]; Figure 2, Table S2C). Since death reporting may be inaccurate in some countries, we repeated the analysis described above also on 94 countries which have good or excellent reporting of causes of death, with the aim of confirming the results obtained with the complete dataset. We retrieved the rating of death reporting from Naghavi et al., (2017). Despite the exclusion of 81 countries (mostly belonging to the low or lower‐middle income class), the results obtained with the analysis considering all of the 175 countries are substantially confirmed (Tables S3 and S4).
FIGURE 2.
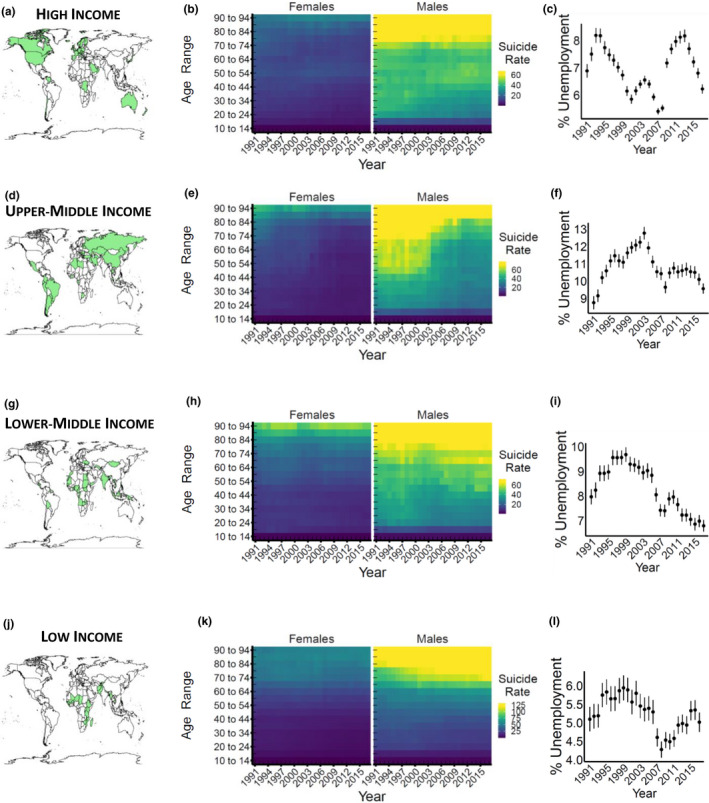
Suicide rates stratified per income classes. (a) high‐income class countries (in 2010, green) considered in our analysis. (b) suicide rates per sex, year (x‐axis), and age range (y‐axis). The labels of the age ranges representing the second half of each decade (15 to 19, 25 to 29, etc.) are omitted for ease of reading. Each tile color refers to median suicide rates per year and age range across the countries considered. Higher rates correspond to the increasing yellow color of the tile. (c) unemployment rate per year (point range = mean and confidence interval). The panels d–l are replicas of the panels described above, for countries of different income classes
DISCUSSION
The impact of unemployment on suicide rates
In this study, we queried several datasets to investigate the relationship between suicide rates and macroeconomic factors in 175 countries during a 27‐year period. First, we replicated the previously reported demographic differences in suicide rates, showing that males have a 1.5‐fold to twofold higher risk of dying by suicide with respect to females (Fountoulakis, 2020; Mościcki, 1994; Värnik, 2012) and that age is the most important demographic factor correlated to higher suicide rates, with death by suicide being 10–20 times more frequent in men and women over 65 years old (De Leo et al., 2009; A. Erlangsen, 2004; Qin et al., 2003b) than in adolescents. Second, we accounted for possible confounders such as the occurrence of heat waves or episodes of political violence. We highlight that during civil/ethnic wars/violence, suicide rates decline, an effect that we believe might reflect a reduced reporting of deaths due to institutional instability, rather than a real reduction in fatalities. Moreover, in line with previous studies involving single countries (Fountoulakis, 2020; Khang et al., 2005) or of geographically or income‐defined super regions (Chang et al., 2009; Fountoulakis et al., 2014; Huikari et al., 2019; Nordt et al., 2015), we evidenced an upsurge in suicide rates that is temporally closely linked (i.e., does not present a previously reported 6‐month lag (Nordt et al., 2015)) to that of unemployment rates. Also, by leveraging on the large, almost global, population considered in this study, we were able to identify specific subgroups of the world population that are at a higher risk of dying by suicide during times of unemployment: a 1% increase in global unemployment rates is associated to a 1% global rise of suicide rates in the male population with respect to females. Moreover, we showed that unemployment takes its toll especially on adults aged 30 to 60, for whom the risk of dying by suicide is increased by up to 3–4%. Although the relative risk is rather small, when considered against the global number of deaths by suicide per year (more than 800,000, WHO | Suicide Data, n.d.) a 1% increase in the number of completed suicides corresponds to the loss of more than 8000 lives.
The impact of gross domestic product on suicide rates
Despite the significant differences in suicide rates among countries belonging to different income classes, there was no definitive evidence supporting a protective role of gross domestic product (Huikari et al., 2019; Nordt et al., 2015). Here, we showed that at the global level, a 1000 US dollar increase in gross domestic product per capita is associated with a reduction in the suicide rate by 2%. This effect was particularly marked for low‐income countries (average GDP per capita <1006 USD, with an average decrease of 29% in suicide rates), and for lower‐middle‐income countries (GDP per capita higher than 1006 USD but less than 3976 USD, reduction by up to 5%). This implies that with a more precise unemployment rate forecasting (Askitas & Zimmermann, 2009; Montgomery et al., 1998), it would be possible to deliver financial support to those at higher risk of suicide after having lost their jobs in a more timely manner. This analysis indicates that the high‐risk category includes males who have lost their jobs in adulthood (30–59, Table S2). However, given the width of this sub‐population, we suggest also considering other individual factors known to be significant predictors of suicide risk and that can be simply assessed when allocating resources, such as whether the recipient is a relative of a person who died by suicide (Annette Erlangsen et al., 2017), is widowed/single (Fässberg et al., 2012), is being/has been evicted (Rojas & Stenberg, 2016). The precise weight of these factors cannot be established at the population level, but their estimation should be a priority to the field to provide the best possible social care to those in need and to prevent suicide during times of economic uncertainty. Moreover, GDP reflects a nation's prosperity and not necessarily its welfare, although the two are to some extent correlated (Fleurbaey, 2009). In fact, a wealthy nation has also more resources to invest in social and health welfare. Therefore, it is not possible to indicate with certainty that a “more money to the unemployed” policy (which would not increase GDP per capita) would reduce suicide rates in nations with well‐developed welfare systems. However, it is noteworthy that a support policy, at present, of delivering 1000 US dollars to 500 people at high risk of suicide, with the prediction of saving at least 1 life, would economically cost less than 1 death by suicide (which is estimated to cost, directly and indirectly, at least 500,000 US dollars (Kennelly, 2007; O’Dea & Tucker, 2005; Shepard et al., 2016)); in addition to the incommensurable human cost of losing a life to suicide.
Limitations
The accuracy of any estimation, including the ones presented herein, is primarily determined by data quality, especially when a plethora of factors, each with a small effect, interact to determine a clinical impact. Studies such as the present are subject to aggregation bias since the net effect of unemployment on an individual's health is modulated by several factors in the person's milieu for which it is not possible to account for. In the light of this, it should be considered that the reported effects of unemployment on deaths by suicide are very likely to be underestimated. Considering the above limitations, the establishment of a worldwide consortium aimed at collecting psychological autopsies and social information on suicide deaths with single‐person resolution would provide immeasurable benefits to the enactment of specifically tailored prevention strategies.
CONCLUSIONS
By leveraging on an unprecedented amount of suicide data with a resolution at the single country, gender, and multiple age range levels, this analysis provides precise estimates of the burden of unemployment on suicide rates. This study reveals that increases in the unemployment rates are associated with higher rates of deaths by suicide in males as well as working‐age males and females. This evidence can help policy‐makers implement economic support funds and programs to prevent upsurges in suicide rates among those who have sustained job loss.
ETHICS STATEMENT
All data were anonymous and aggregated at the source, therefore, Ethics Committee approval was unnecessary. Guidelines of the Declaration of Helsinki and further revisions were followed.
CREDIT CONTRIBUTIONS
Nicola Meda contributed to conceptualization (Lead), formal analysis (Lead), investigation (Lead), methodology (Equal), software (Lead), visualization (Equal), writing—original draft (Equal), and writing—review and editing (Equal). Alessandro Miola contributed to investigation (Equal), methodology (Equal), supervision (Equal), and writing—review and editing (Equal). Irene Slongo contributed to conceptualization (Equal), investigation (Equal), methodology (Equal), and writing—review and editing (Equal). Mauro Agostino Zordan contributed to investigation (Equal), methodology (Equal), software (Equal), supervision (Equal), and writing—review and editing (Equal). Fabio Sambataro contributed to investigation (Equal), methodology (Equal), supervision (Lead), and writing—review and editing (Equal).
CONFLICTS OF INTEREST
None.
Supporting information
Supplementary Material
ACKNOWLEDGEMENTS
The Global Burden of Disease Study received funding from the Bill and Melinda Gates Foundation. The funders had no roles in the design, conduct, analysis, or submission of the present study.
The datasets generated and analyzed in the present study are available from the Global Burden of Disease Collaborative Network datasets, http://ghdx.healthdata.org/gbd‐results‐tool, the World Bank website https://tcdata360.worldbank.org/topics, the Center for Systemic Peace website https://www.systemicpeace.org/ , and the International Disaster Database https://www.emdat.be/. The compiled dataset is available at https://www.researchgate.net/profile/Nicola_Meda and https://doi.org/10.17632/g4syfn24nw.1. Any use of the dataset provided by the authors must adhere to the guidelines adopted by the acknowledged sources. R Code will be made available by the corresponding author on reasonable request. Open Access funding provided by Universita degli Studi di Padova within the CRUI‐CARE Agreement. [Correction added on May 11, 2022, after first online publication: CRUI‐CARE Funding statement has been added.]
Funding Information
This research received no specific grant from any funding agency, commercial, or not‐for‐profit sectors
REFERENCES
- Agerbo, E. (2005). Midlife suicide risk, partner’s psychiatric illness, spouse and child bereavement by suicide or other modes of death: A gender specific study. Journal of Epidemiology & Community Health, 59(5), 407–412. 10.1136/jech.2004.024950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ásgeirsdóttir, H. G. , Valdimarsdóttir, U. A. , Nyberg, U. , Lund, S. H. , Tomasson, G. , Þorsteinsdóttir, Þ. K. , Ásgeirsdóttir, T. L. , & Hauksdóttir, A. (2020). Suicide rates in Iceland before and after the 2008 Global Recession: A nationwide population‐based study. European Journal of Public Health, 30, 1102–1108. 10.1093/eurpub/ckaa121 [DOI] [PubMed] [Google Scholar]
- Askitas, N. , & Zimmermann, K. F. (2009). Google econometrics and unemployment forecasting. SSRN Electronic Journal, 10.2139/ssrn.1480251 [DOI] [Google Scholar]
- Basagaña, X. , Sartini, C. , Barrera‐Gómez, J. , Dadvand, P. , Cunillera, J. , Ostro, B. , Sunyer, J. , & Medina‐Ramón, M. (2011). Heat waves and cause‐specific mortality at all ages. Epidemiology, 22(6), 765–772. 10.1097/EDE.0b013e31823031c5 [DOI] [PubMed] [Google Scholar]
- Basta, M. , Vgontzas, A. , Kastanaki, A. , Michalodimitrakis, M. , Kanaki, K. , Koutra, K. , Anastasaki, M. , & Simos, P. (2018). Suicide rates in Crete, Greece during the economic crisis: The effect of age, gender, unemployment and mental health service provision. BMC Psychiatry, 18(1), 356. 10.1186/s12888-018-1931-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berk, M. , Dodd, S. , & Henry, M. (2006). The effect of macroeconomic variables on suicide. Psychological Medicine, 36(2), 181–189. 10.1017/S0033291705006665 [DOI] [PubMed] [Google Scholar]
- Blakely, T. A. (2003). Unemployment and suicide. Evidence for a causal association? Journal of Epidemiology & Community Health, 57(8), 594–600. 10.1136/jech.57.8.594 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks, M. E. , Kristensen, K. , Benthem, K. J. , Magnusson, A. , Berg, C. W. , Nielsen, A. , Skaug, H. J. , Mächler, M. , & Bolker, B. M. (2017). GlmmTMB balances speed and flexibility among packages for zero‐inflated generalized linear mixed modeling. The R Journal, 9(2), 378. 10.32614/RJ-2017-066 [DOI] [Google Scholar]
- Chan, C. H. , Caine, E. D. , You, S. , Fu, K. W. , Chang, S. S. , & Yip, P. S. F. (2014). Suicide rates among working‐age adults in South Korea before and after the 2008 economic crisis. Journal of Epidemiology and Community Health, 68(3), 246–252. 10.1136/jech-2013-202759 [DOI] [PubMed] [Google Scholar]
- Chang, S.‐S. , Gunnell, D. , Sterne, J. A. C. , Lu, T.‐H. , & Cheng, A. T. A. (2009). Was the economic crisis 1997–1998 responsible for rising suicide rates in East/Southeast Asia? A time–trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Social Science & Medicine, 68(7), 1322–1331. 10.1016/j.socscimed.2009.01.010 [DOI] [PubMed] [Google Scholar]
- Colucci, E. , & Martin, G. (2008). Religion and spirituality along the suicidal path. Suicide and Life‐Threatening Behavior, 38(2), 229–244. 10.1521/suli.2008.38.2.229 [DOI] [PubMed] [Google Scholar]
- Conwell, Y. , Duberstein, P. R. , & Caine, E. D. (2002). Risk factors for suicide in later life. Biological Psychiatry, 52(3), 193–204. 10.1016/S0006-3223(02)01347-1 [DOI] [PubMed] [Google Scholar]
- CSP . (n.d.). CSP ‐ Major Episodes of Political Violence, 1946–2013. Retrieved from http://www.systemicpeace.org/warlist/warlist.htm. 20 September 2020.
- De Leo, D. , Draper, B. , & Krysinska, K. (2009). Suicidal elderly people in clinical and community settings: Risk factors, treatment and suicide prevention. 703–719.Oxford University Press. [Google Scholar]
- Demirci, Ş. , Konca, M. , Yetim, B. , & İlgün, G. (2020). Effect of economic crisis on suicide cases: An ARDL bounds testing approach. International Journal of Social Psychiatry, 66(1), 34–40. 10.1177/0020764019879946 [DOI] [PubMed] [Google Scholar]
- Dervic, K. , Brent, D. A. , & Oquendo, M. A. (2008). Completed suicide in childhood. Psychiatric Clinics of North America, 31(2), 271–291. 10.1016/j.psc.2008.01.006 [DOI] [PubMed] [Google Scholar]
- EM‐DAT . (n.d.). The international disasters database. Retrieved from https://www.emdat.be/. 20 September 2020
- Erlangsen, A. (2004). Loss of partner and suicide risks among oldest old: A population‐based register study. Age and Ageing, 33(4), 378–383. 10.1093/ageing/afh128 [DOI] [PubMed] [Google Scholar]
- Erlangsen, A. , Runeson, B. , Bolton, J. M. , Wilcox, H. C. , Forman, J. L. , Krogh, J. , Shear, M. K. , Nordentoft, M. , & Conwell, Y. (2017). Association between spousal suicide and mental, physical, and social health outcomes: A longitudinal and nationwide register‐based study. JAMA Psychiatry, 74(5), 456. 10.1001/jamapsychiatry.2017.0226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fässberg, M. M. , van Orden, K. A. , Duberstein, P. , Erlangsen, A. , Lapierre, S. , Bodner, E. , Canetto, S. S. , Leo, D. D. , Szanto, K. , & Waern, M. (2012). A systematic review of social factors and suicidal behavior in older adulthood. International Journal of Environmental Research and Public Health, 9(3), 722–745. 10.3390/ijerph9030722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleurbaey, M. (2009). Beyond GDP: The quest for a measure of social welfare. Journal of Economic Literature, 47(4), 1029–1075. 10.1257/jel.47.4.1029 [DOI] [Google Scholar]
- Florentine, J. B. , & Crane, C. (2010). Suicide prevention by limiting access to methods: A review of theory and practice. Social Science & Medicine, 70(10), 1626–1632. 10.1016/j.socscimed.2010.01.029 [DOI] [PubMed] [Google Scholar]
- Fountoulakis, K. N. (2020). Suicides in Greece before and during the period of austerity by sex and age group: Relationship to unemployment and economic variables. Journal of Affective Disorders, 260, 174–182. 10.1016/j.jad.2019.09.001 [DOI] [PubMed] [Google Scholar]
- Fountoulakis, K. N. , Kawohl, W. , Theodorakis, P. N. , Kerkhof, A. J. F. M. , Navickas, A. , Höschl, C. , Lecic‐Tosevski, D. , Sorel, E. , Rancans, E. , Palova, E. , Juckel, G. , Isacsson, G. , Jagodic, H. K. , Botezat‐Antonescu, I. , Warnke, I. , Rybakowski, J. , Azorin, J. M. , Cookson, J. , Waddington, J. , … Lopez‐Ibor, J. (2014). Relationship of suicide rates to economic variables in Europe: 2000–2011. British Journal of Psychiatry, 205(6), 486–496. 10.1192/bjp.bp.114.147454 [DOI] [PubMed] [Google Scholar]
- Fountoulakis, K. N. , Koupidis, S. A. , Siamouli, M. , Grammatikopoulos, I. A. , & Theodorakis, P. N. (2013). Suicide, recession, and unemployment. The Lancet, 381(9868), 721–722. 10.1016/S0140-6736(13)60573-5 [DOI] [PubMed] [Google Scholar]
- Garlow, S. J. , Purselle, D. , & Heninger, M. (2005). Ethnic Differences in patterns of suicide across the life cycle. American Journal of Psychiatry, 162(2), 319–323. 10.1176/appi.ajp.162.2.319 [DOI] [PubMed] [Google Scholar]
- Global Burden of Disease (GBD) . (2014, March 29). Institute for Health Metrics and Evaluation. http://www.healthdata.org/gbd [Google Scholar]
- Gvion, Y. , & Apter, A. (2012). Suicide and suicidal behavior. Public Health Reviews, 34(2), 9. 10.1007/BF03391677 [DOI] [Google Scholar]
- Hempstead, K. A. , & Phillips, J. A. (2015). Rising suicide among adults aged 40–64 years. American Journal of Preventive Medicine, 48(5), 491–500. 10.1016/j.amepre.2014.11.006 [DOI] [PubMed] [Google Scholar]
- Horton, R. (2018). Offline: In defence of precision public health. The Lancet, 392(10157), 1504. 10.1016/S0140-6736(18)32741-7 [DOI] [PubMed] [Google Scholar]
- Huikari, S. , Miettunen, J. , & Korhonen, M. (2019). Economic crises and suicides between 1970 and 2011: Time trend study in 21 developed countries. Journal of Epidemiology and Community Health, 73(4), 311–316. 10.1136/jech-2018-210781 [DOI] [PubMed] [Google Scholar]
- Kennelly, B. (2007). The economic cost of suicide in Ireland. Crisis, 28(2), 89–94. 10.1027/0227-5910.28.2.89 [DOI] [PubMed] [Google Scholar]
- Khang, Y.‐H. , Lynch, J. W. , & Kaplan, G. A. (2005). Impact of economic crisis on cause‐specific mortality in South Korea. International Journal of Epidemiology, 34(6), 1291–1301. 10.1093/ije/dyi224 [DOI] [PubMed] [Google Scholar]
- Liu, K. (2009). Suicide rates in the world: 1950–2004. Suicide and Life‐Threatening Behavior, 39(2), 204–213. 10.1521/suli.2009.39.2.204 [DOI] [PubMed] [Google Scholar]
- Mann, J. J. , Apter, A. , Bertolote, J. , Beautrais, A. , Currier, D. , Haas, A. , Hegerl, U. , Lonnqvist, J. , Malone, K. , Marusic, A. , Mehlum, L. , Patton, G. , Phillips, M. , Rutz, W. , Rihmer, Z. , Schmidtke, A. , Shaffer, D. , Silverman, M. , Takahashi, Y. , … Hendin, H. (2005). Suicide prevention strategies: a systematic review. JAMA, 294(16), 2064. 10.1001/jama.294.16.2064 [DOI] [PubMed] [Google Scholar]
- Mattei, G. , & Pistoresi, B. (2019). Unemployment and suicide in Italy: Evidence of a long‐run association mitigated by public unemployment spending. The European Journal of Health Economics, 20(4), 569–577. 10.1007/s10198-018-1018-7 [DOI] [PubMed] [Google Scholar]
- McKenzie, K. , Serfaty, M. , & Crawford, M. (2003). Suicide in ethnic minority groups. British Journal of Psychiatry, 183(2), 100–101. 10.1192/bjp.183.2.100 [DOI] [PubMed] [Google Scholar]
- Milner, A. , & De Leo, D. (2010). Suicide research and prevention in developing countries in Asia and the Pacific. Bulletin of the World Health Organization, 88(10), 795–796. 10.2471/BLT.09.070821 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mishara, B. L. , & Weisstub, D. N. (2016). The legal status of suicide: A global review. International Journal of Law and Psychiatry, 44, 54–74. 10.1016/j.ijlp.2015.08.032 [DOI] [PubMed] [Google Scholar]
- Montgomery, A. L. , Zarnowitz, V. , Tsay, R. S. , & Tiao, G. C. (1998). Forecasting the U.S. unemployment rate. Journal of the American Statistical Association, 93(442), 478–493. 10.1080/01621459.1998.10473696 [DOI] [Google Scholar]
- Mościcki, E. K. (1994). Gender differences in completed and attempted suicides. Annals of Epidemiology, 4(2), 152–158. 10.1016/1047-2797(94)90062-0 [DOI] [PubMed] [Google Scholar]
- Mościcki, E. K. (1997). Identification of suicide risk factors using epidemiologic studies. Psychiatric Clinics of North America, 20(3), 499–517. 10.1016/S0193-953X(05)70327-0 [DOI] [PubMed] [Google Scholar]
- Naghavi, M. , Abajobir, A. A. , Abbafati, C. , Abbas, K. M. , Abd‐Allah, F. , Abera, S. F. , Aboyans, V. , Adetokunboh, O. , Afshin, A. , Agrawal, A. , Ahmadi, A. , Ahmed, M. B. , Aichour, A. N. , Aichour, M. T. E. , Aichour, I. , Aiyar, S. , Alahdab, F. , Al‐Aly, Z. , Alam, K. , … Murray, C. J. L. (2017). Global, regional, and national age‐sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet, 390(10100), 1151–1210. 10.1016/S0140-6736(17)32152-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nordt, C. , Warnke, I. , Seifritz, E. , & Kawohl, W. (2015). Modelling suicide and unemployment: A longitudinal analysis covering 63 countries, 2000–11. The Lancet Psychiatry, 2(3), 239–245. 10.1016/S2215-0366(14)00118-7 [DOI] [PubMed] [Google Scholar]
- O’Dea, D. J. , & Tucker, S. (2005). The cost of suicide to society. Ministry of Health. [Google Scholar]
- Page, L. A. , Hajat, S. , & Kovats, R. S. (2007). Relationship between daily suicide counts and temperature in England and Wales. British Journal of Psychiatry, 191(2), 106–112. 10.1192/bjp.bp.106.031948 [DOI] [PubMed] [Google Scholar]
- Pompili, M. , Vichi, M. , Innamorati, M. , Lester, D. , Yang, B. , De Leo, D. , & Girardi, P. (2014). Suicide in Italy during a time of economic recession: Some recent data related to age and gender based on a nationwide register study. Health & Social Care in the Community, 22(4), 361–367. 10.1111/hsc.12086 [DOI] [PubMed] [Google Scholar]
- Qi, X. , Hu, W. , Mengersen, K. , & Tong, S. (2014). Socio‐environmental drivers and suicide in Australia: Bayesian spatial analysis. BMC Public Health, 14(1), 681. 10.1186/1471-2458-14-681 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qin, P. , Agerbo, E. , & Mortensen, P. B. (2003a). Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: A National Register‐Based Study of All Suicides in Denmark, 1981–1997. American Journal of Psychiatry, 160(4), 765–772. 10.1176/appi.ajp.160.4.765 [DOI] [PubMed] [Google Scholar]
- Qin, P. , Agerbo, E. , & Mortensen, P. B. (2003b). Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: A National Register‐Based Study of All Suicides in Denmark, 1981–1997. American Journal of Psychiatry, 160(4), 765–772. 10.1176/appi.ajp.160.4.765 [DOI] [PubMed] [Google Scholar]
- Qin, P. , Agerbo, E. , Westergård‐Nielsen, N. , Eriksson, T. , & Mortensen, P. B. (2000). Gender differences in risk factors for suicide in Denmark. British Journal of Psychiatry, 177(6), 546–550. 10.1192/bjp.177.6.546 [DOI] [PubMed] [Google Scholar]
- R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing. (n.d.) [Google Scholar]
- Raftery, A. E. (1995). Bayesian model selection in social research. Sociological Methodology, 25, 111. 10.2307/271063 [DOI] [Google Scholar]
- Rojas, Y. , & Stenberg, S.‐Å. (2016). Evictions and suicide: A follow‐up study of almost 22 000 Swedish households in the wake of the global financial crisis. Journal of Epidemiology and Community Health, 70(4), 409–413. 10.1136/jech-2015-206419 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rushing, N. C. , Corsentino, E. , Hames, J. L. , Sachs‐Ericsson, N. , & Steffens, D. C. (2013). The relationship of religious involvement indicators and social support to current and past suicidality among depressed older adults. Aging & Mental Health, 17(3), 366–374. 10.1080/13607863.2012.738414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shepard, D. S. , Gurewich, D. , Lwin, A. K. , Reed, G. A. , & Silverman, M. M. (2016). Suicide and suicidal attempts in the United States: Costs and policy implications. Suicide and Life‐Threatening Behavior, 46(3), 352–362. 10.1111/sltb.12225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snowdon, J. (2018). Differences between patterns of suicide in East Asia and the West. The importance of sociocultural factors. Asian Journal of Psychiatry, 37, 106–111. 10.1016/j.ajp.2018.08.019 [DOI] [PubMed] [Google Scholar]
- Soleymani, M. , & Yip, P. S. F. (2020). Assessing the impact of the economic crises in 1997 and 2008 on suicides in Hong Kong, Taiwan and South Korea using a strata‐bootstrap algorithm. Journal of Applied Statistics, 47(4), 666–684. 10.1080/02664763.2019.1650008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szanto, K. , Galfalvy, H. , Kenneally, L. , Almasi, R. , & Dombrovski, A. Y. (2020). Predictors of serious suicidal behavior in late‐life depression. European Neuropsychopharmacology, 40, 85–98. 10.1016/j.euroneuro.2020.06.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson, R. , Hornigold, R. , Page, L. , & Waite, T. (2018). Associations between high ambient temperatures and heat waves with mental health outcomes: A systematic review. Public Health, 161, 171–191. 10.1016/j.puhe.2018.06.008 [DOI] [PubMed] [Google Scholar]
- Värnik, P. (2012). Suicide in the world. International Journal of Environmental Research and Public Health, 9(3), 760–771. 10.3390/ijerph9030760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO (n.d.). Suicide data. Retrieved from https://www.who.int/mental_health/prevention/suicide/suicideprevent/en/. 20 September 2020.
- Wickham, 2009 Wickham, H. (2009). Ggplot2. Springer New York. 10.1007/978-0-387-98141-3 [DOI] [Google Scholar]
- World Bank Group . (n.d.). International Development, Poverty, & Sustainability. [Text/HTML]. World Bank. Retrieved from https://www.worldbank.org/. 20 September 2020. [Google Scholar]
- Ying, Y. , & Chang, K. (2009). A study of suicide and socioeconomic factors. Suicide and Life‐Threatening Behavior, 39(2), 214–226. 10.1521/suli.2009.39.2.214 [DOI] [PubMed] [Google Scholar]
- Zeileis, A. , Kleiber, C. , & Jackman, S. (2008). Regression models for count data in R . Journal of Statistical Software, 27(8). 10.18637/jss.v027.i08 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material